
Lecture 1 code version Copyright © BSAC 2007 BSAC Clubmark The ‘How to’ guide..
The PHE CPE Toolkit and the need to detect Carbapenemase-Producing Enterobacteriaceae
Professor Neil Woodford
Antimicrobial Resistance & Healthcare Associated Infections (AMRHAI) Reference Unit
© Crown copyright
2 BSAC, 8th July 2014 © Crown Copyright
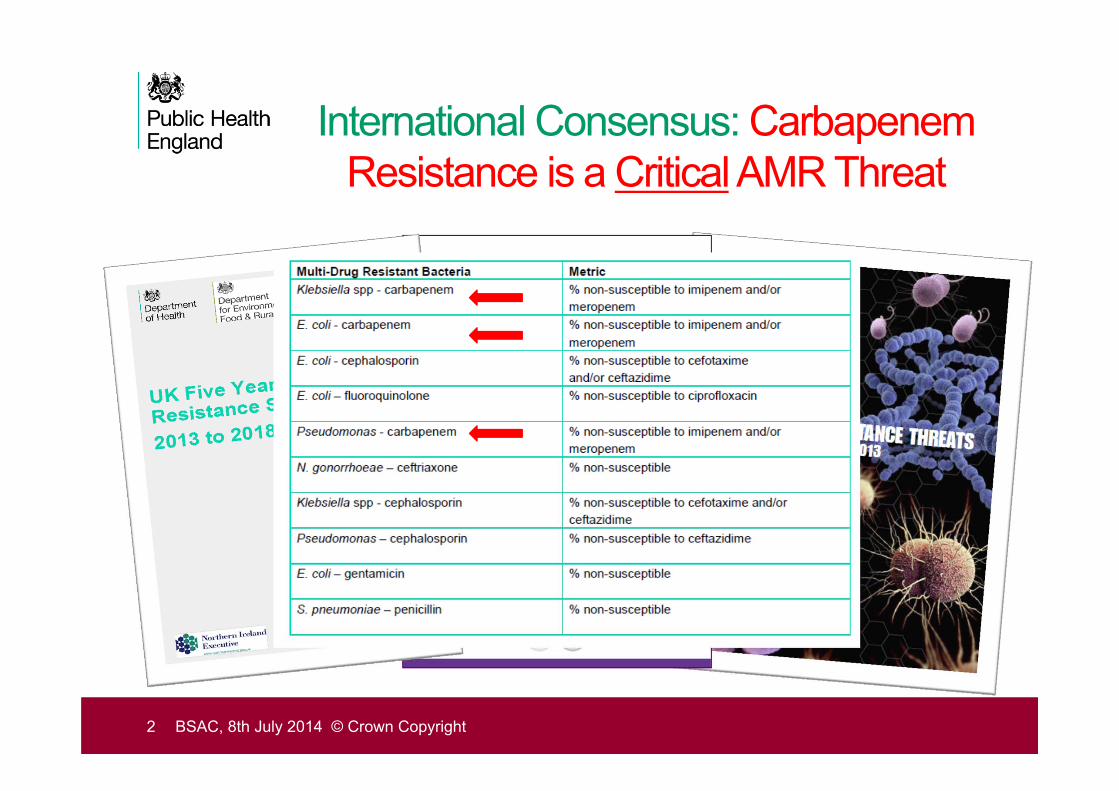
International Consensus: CarbapenemResistance is a CriticalAMR Threat
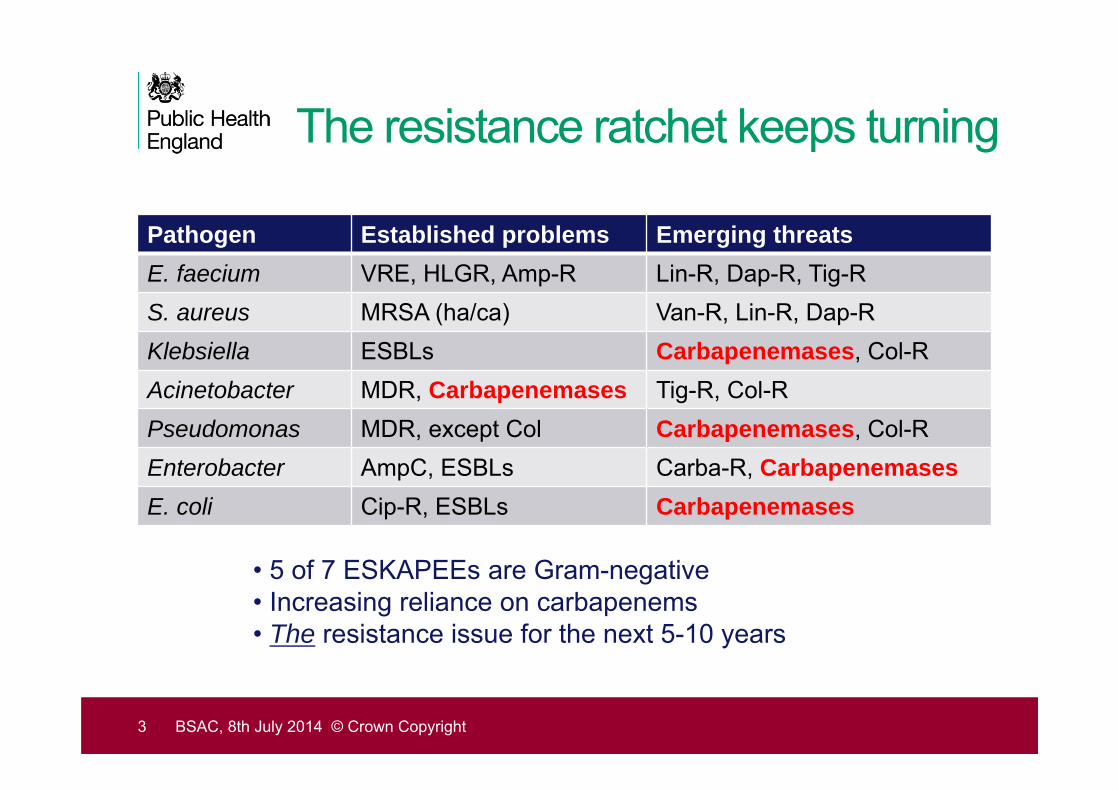
The resistance ratchet keeps turning
Pathogen Established problems Emerging threatsE. faecium VRE, HLGR, Amp-R Lin-R, Dap-R, Tig-RS. aureus MRSA (ha/ca) Van-R, Lin-R, Dap-RKlebsiella ESBLs Carbapenemases, Col-RAcinetobacter MDR, Carbapenemases Tig-R, Col-RPseudomonas MDR, except Col Carbapenemases, Col-REnterobacter AmpC, ESBLs Carba-R, CarbapenemasesE. coli Cip-R, ESBLs Carbapenemases
• 5 of 7 ESKAPEEs are Gram-negative• Increasing reliance on carbapenems• The resistance issue for the next 5-10 years
3 BSAC, 8th July 2014 © Crown Copyright
KPC
OXA-48NDM
VIM IMP
The “Big 5” carbapenemases
4 BSAC, 8th July 2014 © Crown Copyright
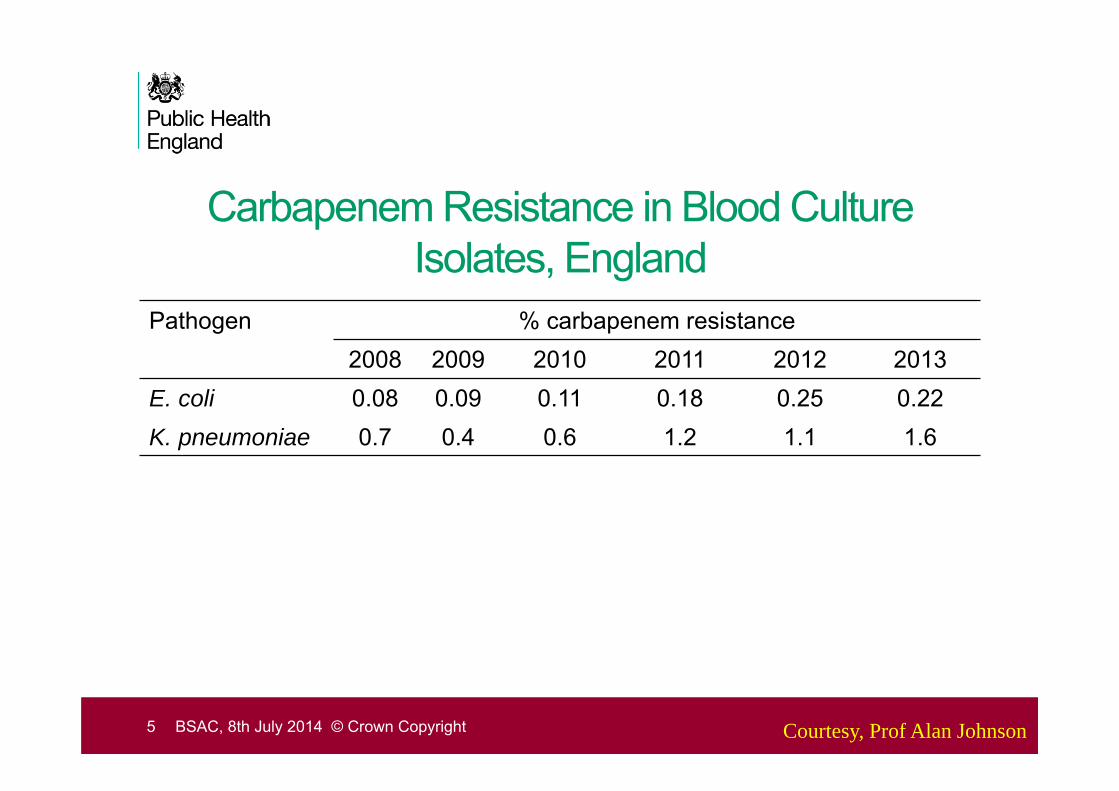
Carbapenem Resistance in Blood Culture Isolates, England
Pathogen % carbapenem resistance2008 2009 2010 2011 2012 2013
E. coli 0.08 0.09 0.11 0.18 0.25 0.22K. pneumoniae 0.7 0.4 0.6 1.2 1.1 1.6
5 BSAC, 8th July 2014 © Crown Copyright Courtesy, Prof Alan Johnson
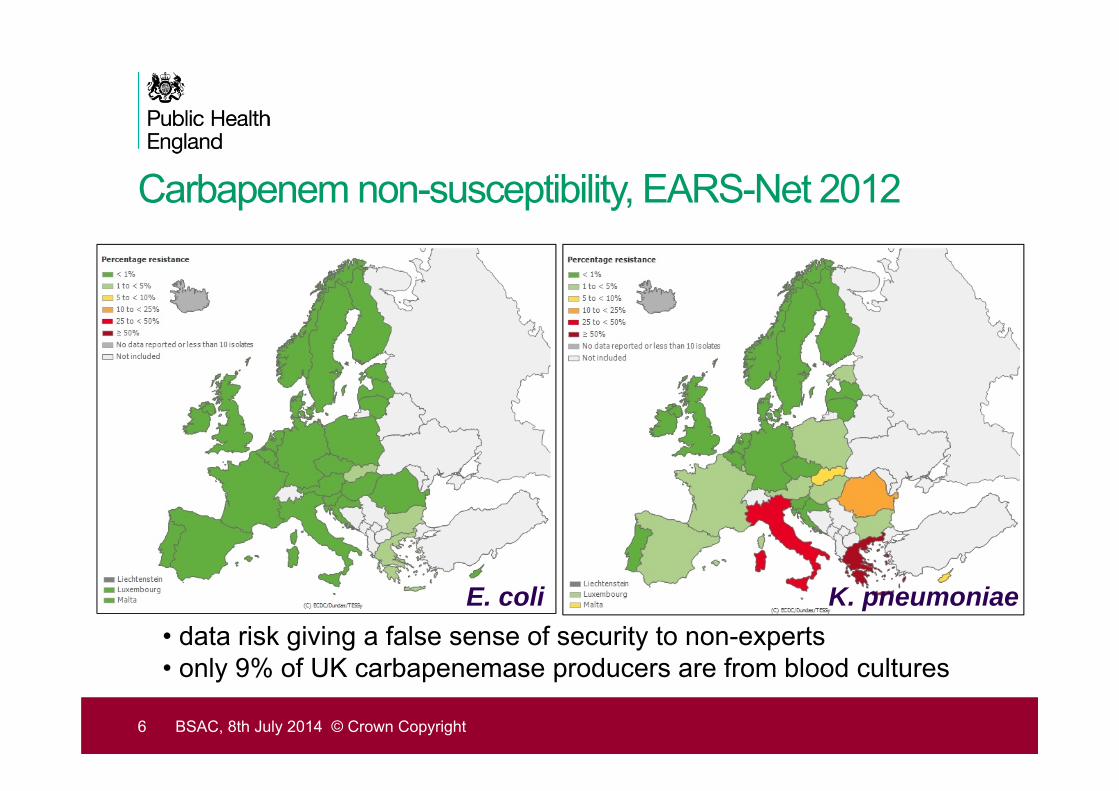
Carbapenem non-susceptibility, EARS-Net 2012
6 BSAC, 8th July 2014 © Crown Copyright
K. pneumoniaeE. coli• data risk giving a false sense of security to non-experts• only 9% of UK carbapenemase producers are from blood cultures
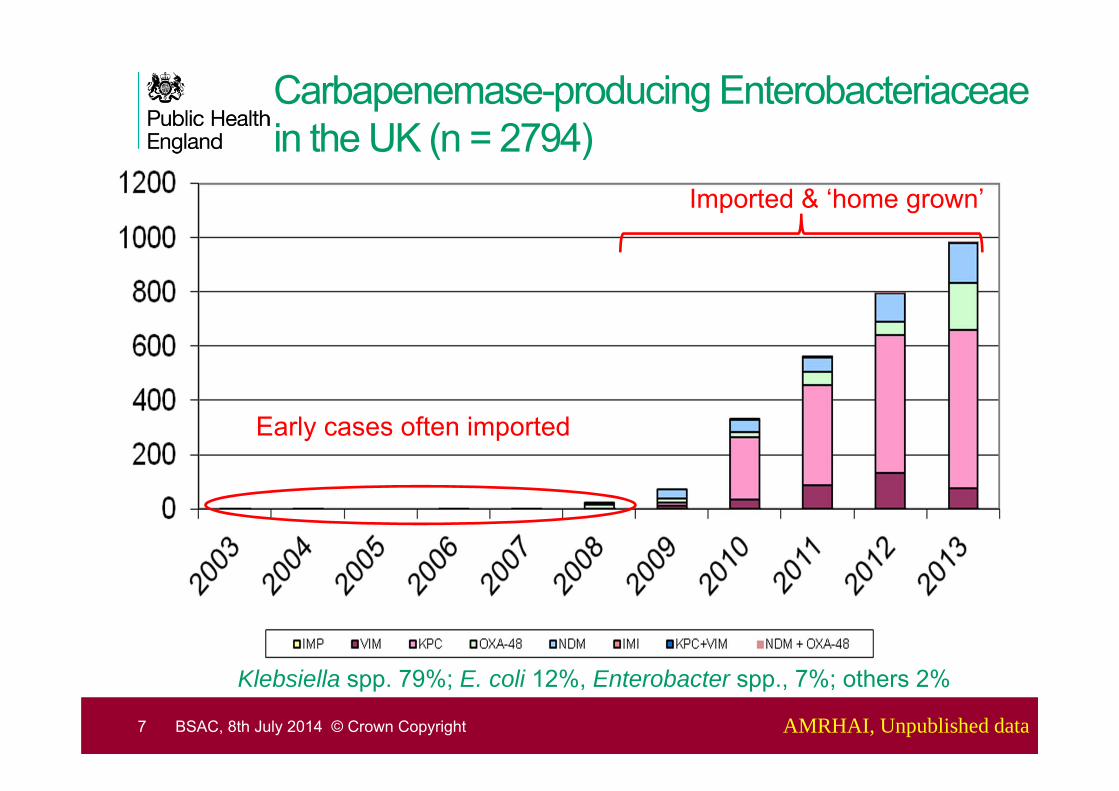
Carbapenemase-producing Enterobacteriaceae in the UK (n = 2794)
Early cases often imported
Imported & ‘home grown’
Klebsiella spp. 79%; E. coli 12%, Enterobacter spp., 7%; others 2%
7 AMRHAI, Unpublished dataBSAC, 8th July 2014 © Crown Copyright

The spread of CPE in the UK
8 AMRHAI, Unpublished dataBSAC, 8th July 2014 © Crown Copyright
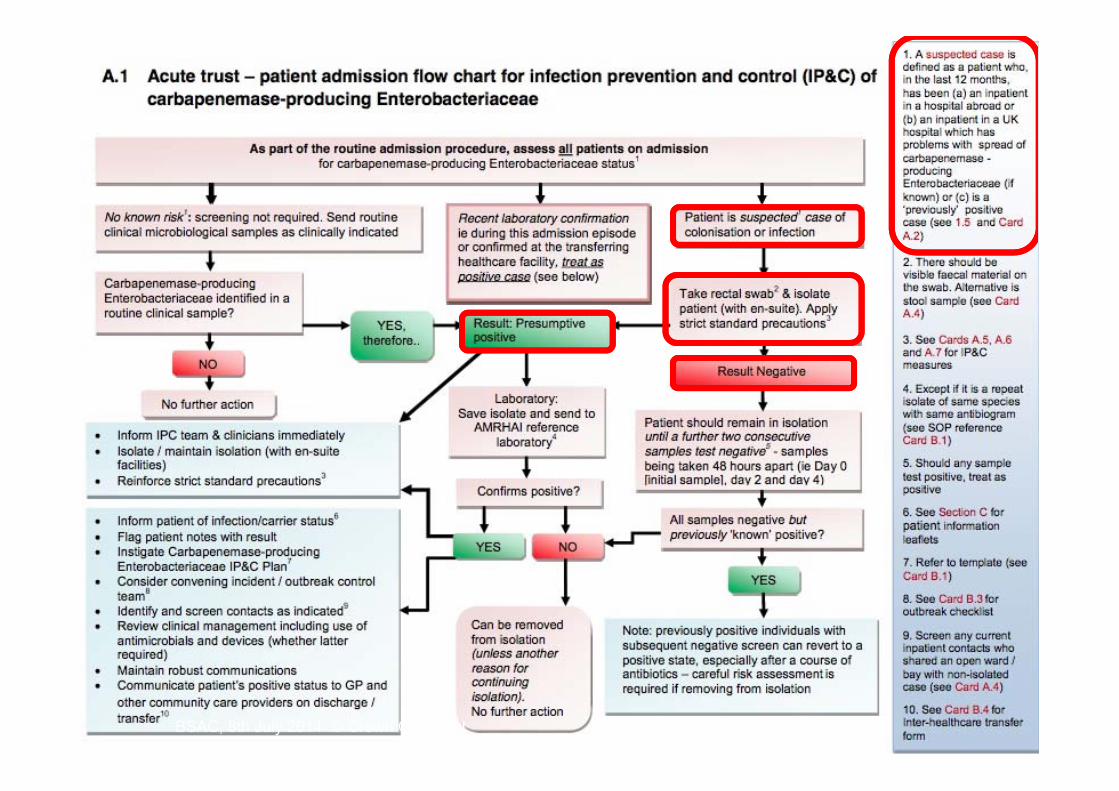
Limiting the impact of carbapenemases
• Detecting resistance in the clinical laboratory is essential for identifying infected / colonized patients:
1. appropriate patient management
2. rapid implementation of infection control procedures
3. Prevent onwards transmission
• But how ?
9 BSAC, 8th July 2014 © Crown Copyright
BSAC, 8th July 2014 © Crown Copyright
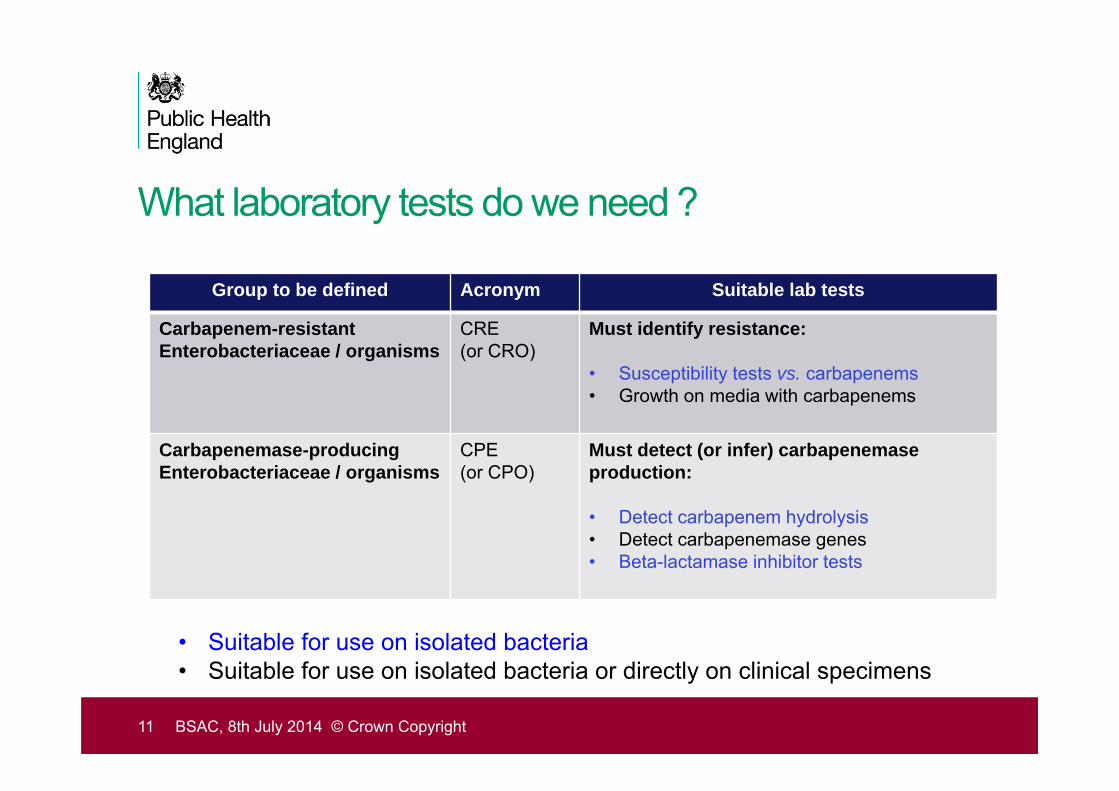
What laboratory tests do we need ?
Group to be defined Acronym Suitable lab tests
Carbapenem-resistant Enterobacteriaceae / organisms
CRE(or CRO)
Must identify resistance:
• Susceptibility tests vs. carbapenems• Growth on media with carbapenems
Carbapenemase-producing Enterobacteriaceae / organisms
CPE (or CPO)
Must detect (or infer) carbapenemaseproduction:
• Detect carbapenem hydrolysis• Detect carbapenemase genes• Beta-lactamase inhibitor tests
11 BSAC, 8th July 2014 © Crown Copyright
• Suitable for use on isolated bacteria• Suitable for use on isolated bacteria or directly on clinical specimens
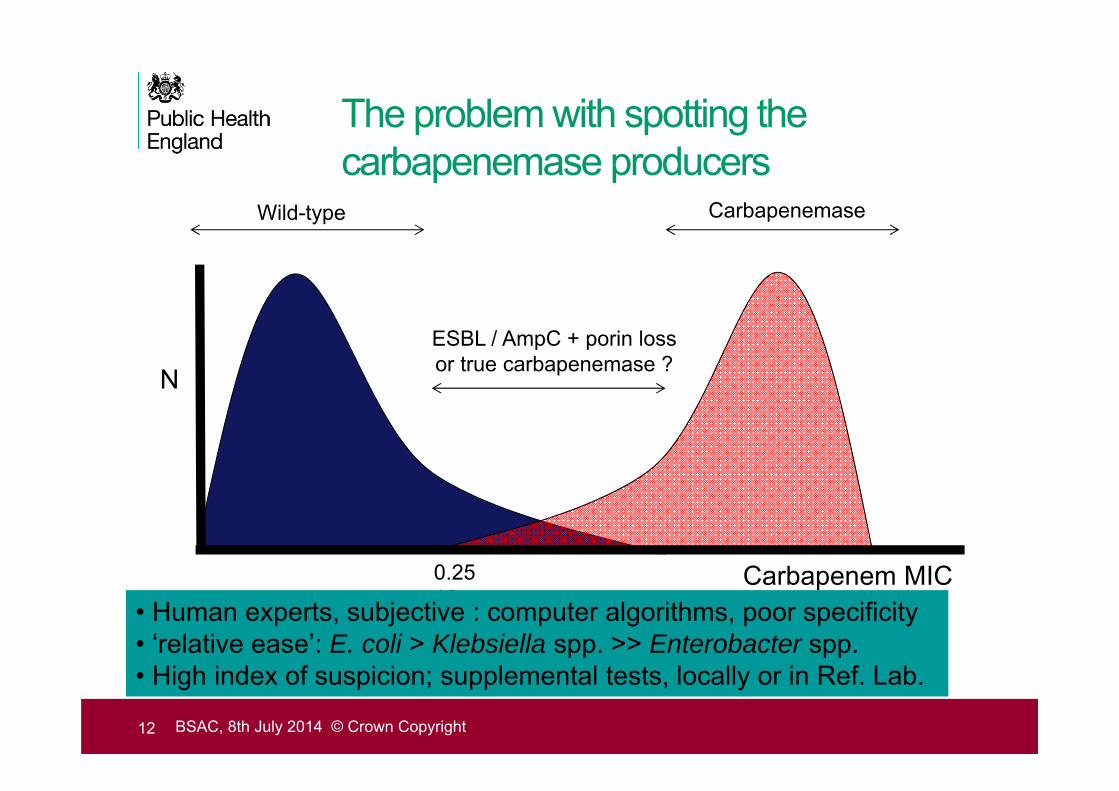
The problem with spotting the carbapenemase producers
Carbapenem MIC
N
0.25 16
Wild-type Carbapenemase
ESBL / AmpC + porin lossor true carbapenemase ?
• Human experts, subjective : computer algorithms, poor specificity• ‘relative ease’: E. coli > Klebsiella spp. >> Enterobacter spp.• High index of suspicion; supplemental tests, locally or in Ref. Lab.
12 BSAC, 8th July 2014 © Crown Copyright
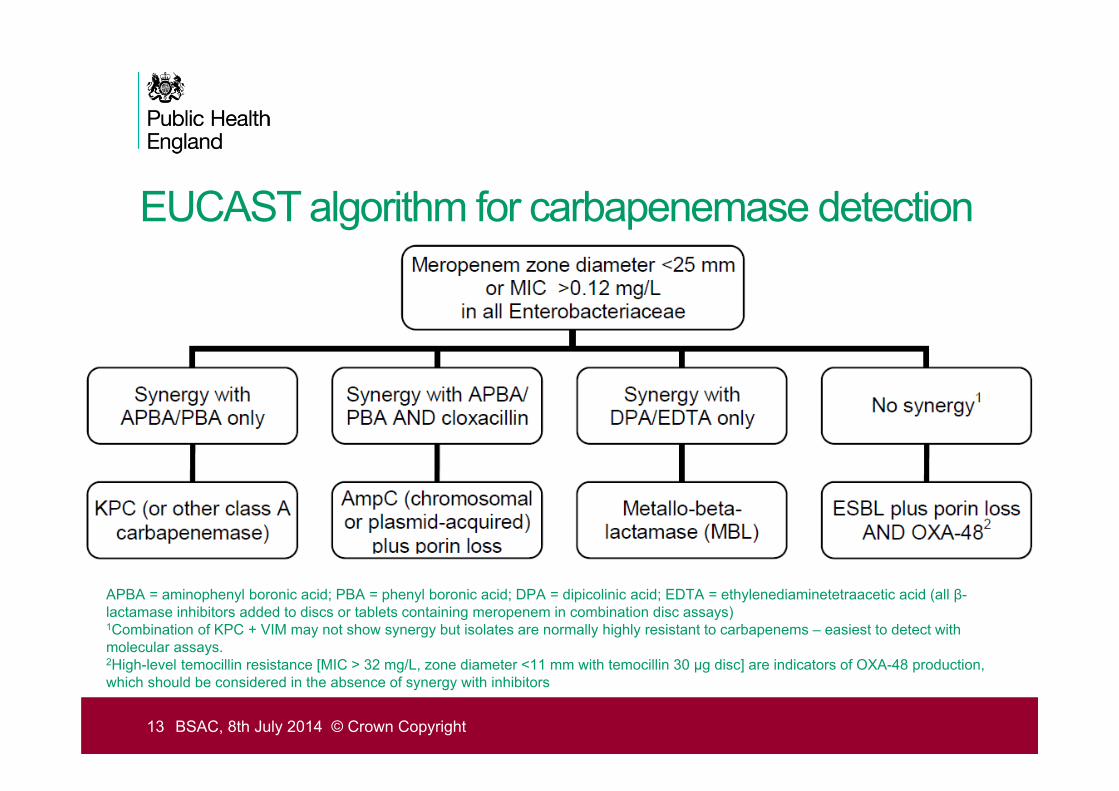
EUCAST algorithm for carbapenemase detection
13 BSAC, 8th July 2014 © Crown Copyright
APBA = aminophenyl boronic acid; PBA = phenyl boronic acid; DPA = dipicolinic acid; EDTA = ethylenediaminetetraacetic acid (all β-lactamase inhibitors added to discs or tablets containing meropenem in combination disc assays)1Combination of KPC + VIM may not show synergy but isolates are normally highly resistant to carbapenems – easiest to detect withmolecular assays.2High-level temocillin resistance [MIC > 32 mg/L, zone diameter <11 mm with temocillin 30 μg disc] are indicators of OXA-48 production, which should be considered in the absence of synergy with inhibitors
Limiting the impact of carbapenemases
• Detecting resistance in the clinical laboratory is too slow if using traditional AST methods and supplemental tests
• RAPID diagnostics are essential for identifying infected / colonized patients:
1. appropriate patient management
2. rapid implementation of infection control procedures
3. Prevent onwards transmission
14 BSAC, 8th July 2014 © Crown Copyright
Commercial systems
• Increasing numbers of products for a growing market
• Phenotypic detection of hydrolysis• Colorimetric e.g. Rosco Diagnostica Rapid CARB Screen kit;
bioMerieux Rapidec• MALDI-ToF
• Molecular detection of resistance genes • Coverage of ‘big five’ carbapenemases varies • Range from ‘yes/no’ tests to ‘full’ group differentiation• None will find novel carbapenemases
15BSAC, 8th July 2014 © Crown Copyright
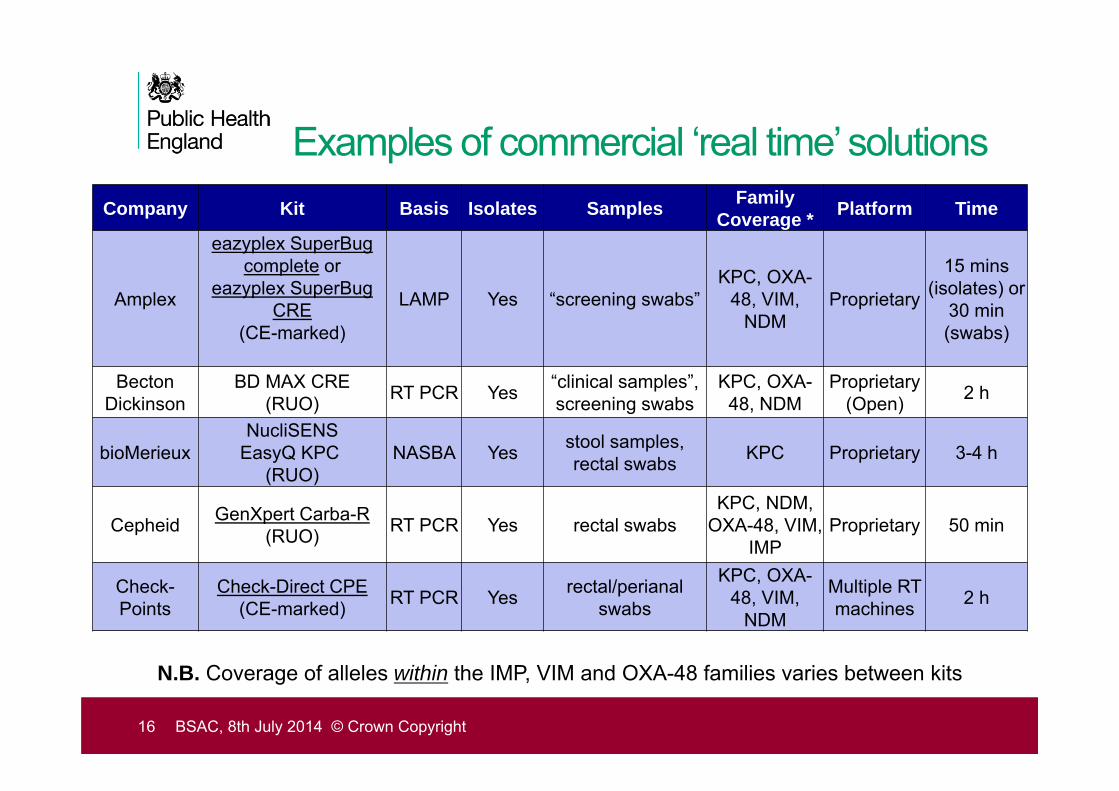
Examples of commercial ‘real time’ solutionsCompany Kit Basis Isolates Samples Family
Coverage * Platform Time
Amplex
eazyplex SuperBug complete or
eazyplex SuperBugCRE
(CE-marked)
LAMP Yes “screening swabs”KPC, OXA-
48, VIM, NDM
Proprietary
15 mins(isolates) or
30 min (swabs)
Becton Dickinson
BD MAX CRE (RUO) RT PCR Yes “clinical samples”,
screening swabsKPC, OXA-
48, NDMProprietary
(Open) 2 h
bioMerieuxNucliSENS
EasyQ KPC(RUO)
NASBA Yes stool samples, rectal swabs KPC Proprietary 3-4 h
Cepheid GenXpert Carba-R(RUO) RT PCR Yes rectal swabs
KPC, NDM, OXA-48, VIM,
IMPProprietary 50 min
Check-Points
Check-Direct CPE(CE-marked) RT PCR Yes rectal/perianal
swabs
KPC, OXA-48, VIM,
NDM
Multiple RT machines 2 h
16 BSAC, 8th July 2014 © Crown Copyright
N.B. Coverage of alleles within the IMP, VIM and OXA-48 families varies between kits
Rapid Diagnostics to Guide Empiric Therapy
• Rapid tests for mechanisms = surrogates for rapid AST
• Absence of a resistance mechanism doesn’t confirm susceptibility• cannot indicate appropriate empiric therapy
• Presence of a resistance mechanism used to infer likely resistance• indicates potentially inappropriate empiric therapy
• Carbapenemase detected: carbapenem NOT suitable as sole agent
• (Confirming susceptibility = prime criterion for appropriate therapy)
17 BSAC, 8th July 2014 © Crown Copyright
There isn’t a single ‘best’ detection method…
• because of the diversity of carbapenemases
• their different molecular classes
• the variation between genes within major families
• all hydrolyze carbapenems, but have no other shared properties
• because of the diversity of host strains
• level of resistance is contigent on e.g. porin status etc.
18 BSAC, 8th July 2014 © Crown Copyright
Better use of resources for better patient care
19 BSAC, 8th July 2014 © Crown Copyright
• Local AST results analysed regionally on daily basis (e.g. AMWEB)*
• Daily request for MDR bacteria• Regional testing in specialist lab• Timely feedback to local lab• Better IPC / patient management
• Positive isolates sent to national reference lab for further study
*Ironmonger et al. JAC 2013 doi: 10.1093/jac/dkt181
Hawkey, Woodford & Ironmonger
20 BSAC, 8th July 2014 © Crown Copyright
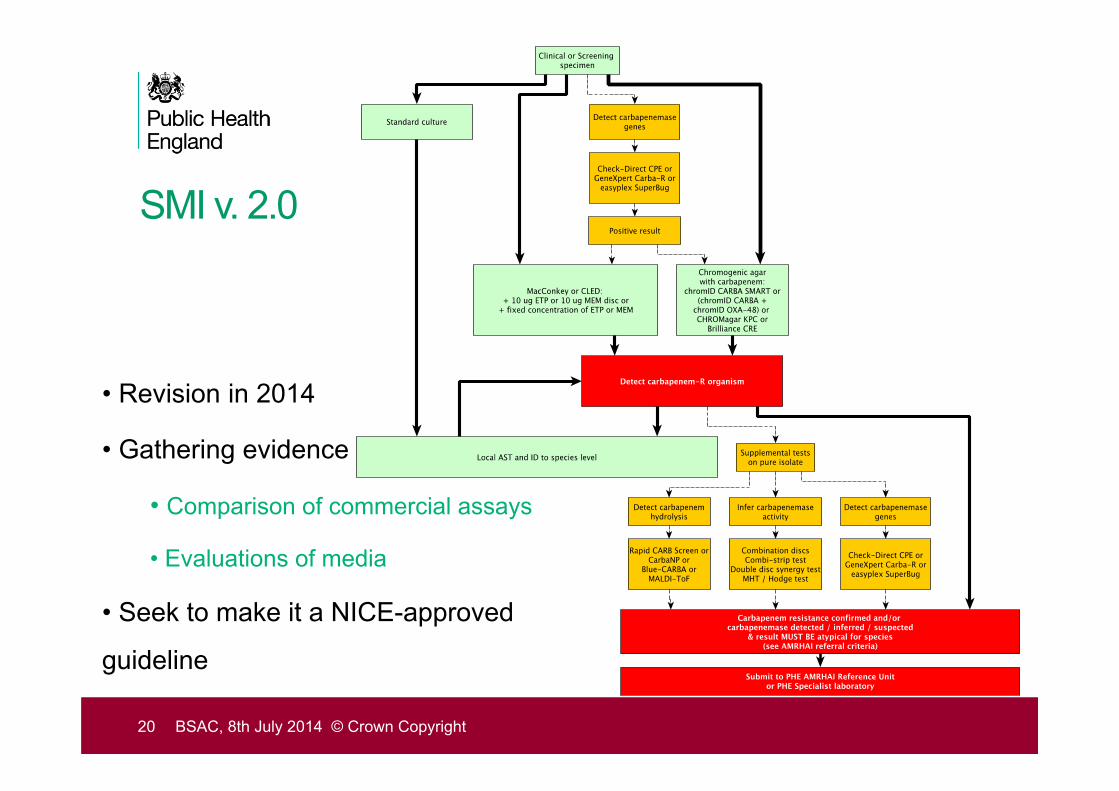
• Revision in 2014
• Gathering evidence
• Comparison of commercial assays
• Evaluations of media
• Seek to make it a NICE-approved
guideline
SMI v. 2.0















![.g¼ Ïï¬Diver's guide guma- Ä] › pdf › taikendiving_seimei.pdf · l. 2. (bsac bsac confirmation bsac dive with us bsac 3. bsac bsac bsac bsac japan & 4. 5. bsac 7. bsac bsac](https://static.fdocuments.us/doc/165x107/60bd74eca725ab1ff12f7e75/g-divers-guide-guma-a-pdf-a-taikendiving-l-2-bsac-bsac.jpg)
