CLINICAL PHARMACOLOGY OF ANTIBACTERIAL AGENTS. Actions of antibacterial drugs on bacterial cells.
Upload
mohamed-naguibCategory
view
212download
0
Ombewtsepin
tat“sdTicdnR“ohfs
J
Ms2
2
The Pharmacology of Commonly Used Chemical Agents
Mohamed Naguib
N
itTp
“Wars are not acts of God. They are caused by man, byman-made institutions, by the way in which man has or-ganized his society. What man has made, man canchange.”
Speech by Frederick Moore Vinson (1890-1953) at Ar-lington National Cemetery (Memorial Day, 1945)
f all forms of warfare, chemical warfare isprobably one of the most brutal created by
ankind. Originally, simple techniques such asurning materials to produce acrid smoke to blindnemies and polluting enemy water supplies withaste were used. During the Peloponnesian War in
he 5th century BC, Spartans used bombs made ofulphur and pitch to conquer the enemy. In medi-val times, soldiers sometimes threw bodies oflague victims over the walls of besieged cities, ornto water wells. World War I advanced the tech-iques of chemical warfare.Probably nearly 70 different chemicals or mix-
ures of chemicals are thought to be stockpiled asgents for chemical warfare.1 A 1969 United Na-ions report defines chemical warfare agents aschemical substances, whether gaseous, liquid orolid, which might be employed because of theirirect toxic effects on man, animals and plants. . . .”he Chemical Weapons Convention defines chem-
cal weapons as “any chemical which, through itshemical effect on living processes, may causeeath, temporary loss of performance, or perma-ent injury to people and animals.” The U.S. Armyegulation 380-86 states that a chemical agent isa chemical substance intended for use in militaryperations to kill, seriously injure, or incapacitateumans through its chemical properties.” Excludedrom this classification are riot-control agents,moke, and incendiary agents. Incendiary agents
From the Department of Anesthesia, University of Iowa, Roy. and Lucille A. Carver College of Medicine, Iowa City, IA.
Address reprint requests to Mohamed Naguib, MB, BCh,Sc, FFARCSI, MD, Department of Anesthesia-6JCP, Univer-
ity of Iowa, Roy J. and Lucille A. Carver College of Medicine,00 Hawkins Drive, Iowa City, IA 52242-1009.E-mail: [email protected]© 2003 Elsevier Inc. All rights reserved.0277-0326/03/2204-0000$30.00/0
adoi:10.1053/S0277-0326(03)00040-0
30 Seminars in Anesthesia, Perioperative Medici
uch as napalm and phosphorus are not consideredhemical warfare agents because they achieve theirffect through thermal injury.
CLASSIFICATION OF CHEMICAL WARFAREAGENTS
Chemical agents used in warfare may be classi-ed as follows:
● Nerve agents● Blistering agents (vesicants)● Cyanogenic compounds● Choking agents● Toxins● Psychomimetic agents
erve Agents
Nerve agents are highly toxic compounds thatrreversibly inhibit cholinesterases. Althoughoxic, these agents are not nearly equally potent.he lethal concentration for VX is 500 times lessotent than hydrogen cyanide, a highly toxic com-ound. The physical and biological properties oferve agents are shown in Table 1. Nerve agentsere first developed in the 1930’s by the German
hemist Gerhard Schrader. The organophosphatesarin, soman, VX, GF, and tabun are the mostowerful nerve agents (Fig 1). Tabun (GA), sarinGB), soman (GD), and GF (the “G-agents”) arectually fluorinated cyanide-containing organo-hosphates. They are colorless and odorless vola-ile liquids whose vapors are heavier than air. TheG” indicates that they originated in Germany.2
he “V-agents” (VX) are sulfur-containing or-anophosphates, are less volatile, and act throughirect skin contact. The “V” means venomous.2
he use of sarin in the terrorist attacks againstivilians in Japan in 1994 and 1995 resulted ineveral fatalities and hundreds of casualties.3
Acetylcholine is the primary neurotransmitter ofhe cholinergic system, and its duration of activitys regulated through hydrolysis by acetylcholines-erase (AChE). (For a detailed account on AChE,ee Naguib et al4 and Soreq and Seidman).5 There
sce
fi
pnwcsp(apt“TgdTcs
tits
re three known types of cholinesterase enzymes,ne and Pain, Vol 22, No 4 (December), 2003: pp 230-238

namely AChE, butyrylcholinesterase (BChE), anderythrocyte-ChE. AChE is a type B carboxylester-ase that hydrolyzes acetylcholine at neuronal cho-linergic synapses and at neuromuscular junctionsinto choline and acetic acid. In addition, AChE hasother functions such as nerve-growth promotion6
and modulation of acetylcholine receptors.7 BChE
is a serine hydrolase. AChE and BChE arise fromdifferent genes and have about 50% sequence iden-tity. BChE is widely distributed in the nervoussystem, indicating a possible role in neural func-tion.8 BChE catalyses the hydrolysis of succinyl-choline and mivacurium. Erythrocyte-ChE activityreflects AChE but not BChE activity. The physio-
Table 1. Physical and Toxicological Properties of Nerve Agents and Mustard Gas
Boiling Point (°C)Vapor Pressure
(mmHg at 25°C) Odor
Toxicity
Vapor (LCt50)mg/min/m3
Liquid(LD50) g/70 kg
Nerve agentsTabun (GA) 230 0.037 (at 20°C) Fruity 400 1Sarin (GB) 158 2.1 Odorless 100 1.7Soman (GD) 198 0.4 Oil of camphor 50 0.35GF 92 0.06 Odorless — —VX 298 0.0007 Odorless 10 0.01
VesicantsMustard gas 277 0.072 (at 20°C) Faint smell of mustard
or garlic1500 100
Lewisite 190 0.39 Geranium 1300 3.5Hydrogen cyanide 25.7 740 Bitter almonds 2500–5000 7
LCt50 � the lethal concentrations in 50% of individuals exposed by inhalation.LD50 � the lethal dose in 50% of individuals exposed.Reproduced from Sidell et al.2
Fig 1. The chemical structure of nerve agents.
231PHARMACOLOGY OF COMMON CHEMICALS

logical function of erythrocyte-ChE is not yetknown.
Nerve agents irreversibly inhibit AChE every-where in the body. They inhibit AChE, BChE, anderythrocyte-ChE.9 Acetylcholine accumulates. Inrats, histochemical staining for AChE demon-strates that sarin exposure reduces AChE in thecerebral cortex, striatum, and olfactory bulb.10
Nerve agents also activate choline acetyltrans-ferase in the central nervous system,11 causingaugmentation of acetylcholine availability beyondthat produced by AChE inhibition alone.11 Accu-mulated acetylcholine in turn stimulates cholin-ergic synapses via nicotinic and muscarinic recep-tors, resulting in cholinergic toxicity. Nerve agentsalso appear to have a direct effect on many recep-tors. For instance, nerve agents can antagonizeGABA (�-aminobutyric acid) neurotransmission12
and bind to nicotinic, cardiac muscarinic, and glu-tamate NMDA (N-methyl-D-aspartate) receptorsdirectly.13,14 In rats, 30% and 60% inhibitions oferythrocyte-ChE were noted after repeated expo-sures to both the low and high doses, respec-tively.10 After irreversible inhibition of erythro-cyte-ChE and BChE, regeneration of enzymes oc-curs after 120 and 50 days, respectively.15 It hasbeen shown that knockout mice with no AChE aremore sensitive to VX than mice that have AChE.This indicates that the presence of AChE providesprotection against VX toxicity.9
The amount, duration, and route of exposure tonerve agents are important factors in determiningthe severity of the victim’s clinical course. Afterinhalation of nerve agents, respiratory, cardiovas-cular, and central nervous system manifestations ofcholinergic toxicity (shortness of breath, bronchor-rhea, wheezing, bradycardia, heart block, dys-rhythmias, hypotension, fasciculations, tremors,and convulsions) are followed by cardiorespiratorycollapse and death within minutes. A single expo-sure of rats to sarin at 1 � LD50 causes seizuresand extensive brain damage within 24 hours.16 Bycontrast, dermal exposure causes local muscletwitching, weakness, delayed paralysis, respiratoryfailure, and eventually death. Dermal exposureconstitutes the highest risk to healthcare personnelshould there be direct contact with contaminatedclothing and patients.
Nerve agents are believed to exert severe long-term consequences as manifested by altered neu-romuscular function, predisposition to convul-
sions, and impaired psychomotor performance thatpersists more than 1 year after nonlethal exposure.1
Approximately 1 � LD50 of soman causes long-lasting epileptic seizure activity and severe braindamage in rats.17,18 At much lower doses, somaninduces behavioral alterations that are not associ-ated with histopathological changes in the brain ofrats.19,20 The epileptic activity induced by highdoses of soman in laboratory animals can be pre-vented by pretreatment with atropine (a muscarinicreceptor antagonist) and pralidoxime (an oximethat reactivates cholinesterases by removing thephosphate group bound to the esteratic site ofcholinesterases). Also effective are benzodiaz-epines in treating convulsions and reversible cho-linesterase inhibitors that cross the blood–brainbarrier.17,21,22
After exposure to nerve agents, treatment con-sists of decontamination, administration of musca-rinic receptor antagonists with mainly peripheral(atropine) or central (benactyzine, scopolamine)activity, reversal of cholinesterase inhibition withpralidoxime,23,24 treatment of convulsions, andcorrection of metabolic abnormalities. Aqueous so-dium hydroxide or calcium hypochlorite is used fordecontamination. The latter is the standard decon-taminant for VX. Because of limited experiencewith nerve-agent casualties, it has been recom-mended that only repeated administration of dosesof atropine as high as 10 to 20 mg in the first 2 or3 hours and up to 50 mg in a 24-hour period willprovide an adequate control of the toxic symp-toms.25 Others26 recommend repeated intravenousadministration of 2 mg of atropine for adults and0.02 mg/kg atropine for children until pupillarydilatation occurs. Individuals at risk may self-ad-minister repeated injections of atropine until thefull effect of atropine is seen (flushed and dry skin,pupillary dilatation, increased heart rate, and ces-sation of bronchoconstriction and bronchorrhea).25
In conjunction with atropine, Singh et al27 recom-mended intravenous administration of 2 g of pra-lidoxime over 15 to 30 minutes followed by aninfusion (7.5 mg/kg/h). Because of their low lipidsolubility, oximes are only effective in the periph-eral nervous system and not in the central nervoussystem. Sometimes the organophosphate-AChEcomplex becomes resistant to reactivation byoxime therapy in a process termed “aging.”25 Ag-ing is an irreversible reaction. The half-time foraging of soman-AChE complex is �1 minute and
232 MOHAMED NAGUIB
that for sarin, soman, GF, and VX are 5, 6, 7.5, and48 hours, respectively.25,28-31
H oximes are recent and promising antidotes tonerve agents because they are able to protect ex-perimental animals from toxic effects and improvethe survival of animals poisoned with supralethaldoses.32 They appear more effective against nerve-agent poisoning than the currently used oximes,pralidoxime, and obidoxime.32 H-series oximes ap-pear to have a range of activity: reactivation ofAChE, blockage of ganglia and muscarinic recep-tors, stimulation of vasopressor and respiratorycentre receptors, chemical combination withagents, restoration of neuromuscular transmission,retardation of the formation of the aged inhibitor–enzyme complex, and (or) inhibition of the releaseof acetylcholine.24,32
Pretreatment with pyridostigmine is now recom-mended by the North Atlantic Treaty Organizationas the prophylactic measure of choice.2 At firstglance, it might appear contradictory to use aninhibitor to protect an enzyme from another inhib-itor. However, the explanation is simple: (1) AChEbound to pyridostigmine is not available for bind-ing with nerve agents; (2) the interaction of AChEand pyridostigmine is reversible; and (3) AChEbound to pyridostigmine can be easily reactivatedby oximes. However, pretreatment with pyridostig-mine does not appear to be equally effectiveagainst all nerve agents. In animals, pyridostig-mine pretreatment improved survival against so-man and tabun exposure but not against sarin orVX.31,33
Administration of exogenous preparations ofBChE appears to provide protection against nerveagents in animals.34-36 There is also evidence thatthe use of monoclonal antibodies37,38 and protease
inhibitors39 such as suramin may be therapeuticallyor prophylactically useful against nerve agents.
Blistering Agents (vesicants)
A vesicant is an agent that produces vesicle orblisters. Several have been used.
Mustard Gas
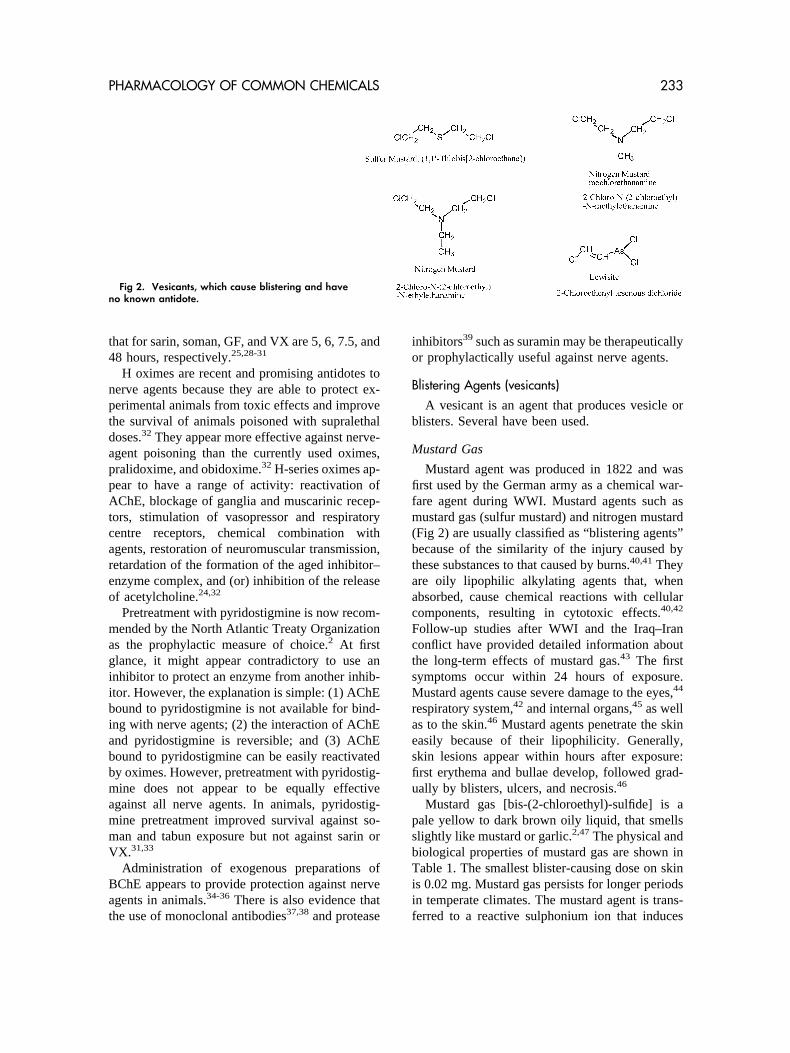
Mustard agent was produced in 1822 and wasfirst used by the German army as a chemical war-fare agent during WWI. Mustard agents such asmustard gas (sulfur mustard) and nitrogen mustard(Fig 2) are usually classified as “blistering agents”because of the similarity of the injury caused bythese substances to that caused by burns.40,41 Theyare oily lipophilic alkylating agents that, whenabsorbed, cause chemical reactions with cellularcomponents, resulting in cytotoxic effects.40,42
Follow-up studies after WWI and the Iraq–Iranconflict have provided detailed information aboutthe long-term effects of mustard gas.43 The firstsymptoms occur within 24 hours of exposure.Mustard agents cause severe damage to the eyes,44
respiratory system,42 and internal organs,45 as wellas to the skin.46 Mustard agents penetrate the skineasily because of their lipophilicity. Generally,skin lesions appear within hours after exposure:first erythema and bullae develop, followed grad-ually by blisters, ulcers, and necrosis.46
Mustard gas [bis-(2-chloroethyl)-sulfide] is apale yellow to dark brown oily liquid, that smellsslightly like mustard or garlic.2,47 The physical andbiological properties of mustard gas are shown inTable 1. The smallest blister-causing dose on skinis 0.02 mg. Mustard gas persists for longer periodsin temperate climates. The mustard agent is trans-ferred to a reactive sulphonium ion that induces
Fig 2. Vesicants, which cause blistering and haveno known antidote.
233PHARMACOLOGY OF COMMON CHEMICALS

DNA damage42 and generates reactive oxygen spe-cies.48 These effects may increase the likelihood ofdeveloping malignant diseases.49 The incidence ofmalignant diseases is greater for mustard gas thanfor any other chemical warfare agent.
There is no effective treatment for mustard-agent intoxication. Wearing protective clothingwhile decontaminating both casualties and re-sponders immediately after contact are still therecommended measures of choice.50,51 Clothesshould be removed, the skin should be decontam-inated and washed with soap and water, and con-taminated hair should be shaved off. Eyes shouldbe frequently rinsed with saline solution. N-acetyl-cysteine appears to be effective against sulfur-mustard-induced lung injury in experimental ani-mal models.52
Arsines
Organoarsenic-based chemical warfare agentsinclude 10-chloro-9-10-dihydrophenarsazine, di-phenyl arsine chloride, diphenylcyanoarsine, and2-chlorovinyldichloroarsine (lewisite) (Fig 2).53
Lewisite (also known as agent L) is a potent toxicvesicant that reacts with the sulfhydryl groups ofproteins through its arsenic group. It seems thatinhibition of the carbohydrate metabolism andDNA damage constitute major factors in arsenicalpoisoning.50,54 Pure lewisite is a colorless liquidand causes severe chemical burns upon direct con-tact with tissue. The physical and biological prop-erties of lewisite are shown in Table 1. Injuriescaused by lewisite are similar to those caused bymustard agents. However, unlike mustard gas,symptoms in lewisite poisoning occur immedi-ately. Moist tissues such as the eyes, respiratorytract, and axillary areas are particularly affected.50
Skin damage is treated in the same way asexposure to mustard agents. A specific antidote(dimercaptopropanol, BAL, British Anti Lewisite)gives good protection against local injuries to skin,mucous membrane, and systemic poisoning.55
Cyanogenic Compounds
Hydrogen cyanide and cyanogen chloride (for-merly known as blood agents) are the main chem-ical agents in this class. Recognition of the toxiceffects of cyanide dates back to 1786, when thefamous synthetic chemist, Scheele, died acciden-tally from inhaling cyanide vapors that he hadsynthesized. There are no confirmed reports of this
substance being used in chemical warfare, possiblybecause it is difficult to achieve adequate concen-trations outdoors. On the other hand, the concen-tration of hydrogen cyanide may rapidly reachlethal concentrations if it is released in a confinedspace. A dose of 300 mg/m3 is immediately le-thal.56 Industrial intoxications infrequently occurbecause of the widespread use of cyanide com-pounds in electroplating, plastics manufacture, fu-migation of ships, and gold mining.57 At roomtemperature, hydrogen cyanide is a colorless liquidthat smells of almonds and boils at 26°C (Table1).56 The most important route of poisoning isthrough inhalation. Both gaseous and liquid hydro-gen cyanide also can be absorbed through theskin.56
Cyanide inhibits the mitochondrial respiratorychain enzyme cytochrome oxidase, resulting inhistotoxic hypoxia. It binds to ferrocytochromea3
58 to inhibit electron transport, mitochondrialoxygen utilization, and cellular respiration.59 Allbody organs are adversely affected, especiallythose with high oxygen requirements, such as theheart and brain.59 Cyanide also has neurotoxicproperties. Oxidative stress plays a pivotal role incyanide-induced neurodegeneration.60 Cyanidestimulates N-methyl-D-aspartate receptors,61 mobi-lizes intracellular calcium stores,62 and inducesseveral reactions that generate reactive oxygenspecies and nitric oxide,63 resulting in either cellnecrosis or apoptosis.64
Cyanogenic compounds may produce acute orsubacute toxicity. Acute cyanide toxicity is lethal,resulting in respiratory failure and death.65 Thediagnosis of cyanide poisoning is difficult. Thedifferential diagnosis includes carbon monoxidepoisoning, hypoglycemia, metabolic disturbances,and the postictal state.66 Signs of cyanide poison-ing include headache, vertigo, agitation, confu-sion, coma, convulsions, respiratory failure, anddeath.2,65 On exposure to lethal concentrations,there is no time for symptoms to develop andexposed persons may present with sudden collapseand death. Increased lactate concentrations associ-ated with cardiovascular collapse suggest cyanideintoxication. Immediate treatment includes admin-istration of 100% oxygen, assisted ventilation, cor-rection of acidosis, and hemodynamic support.White67 recommends the following antidote regi-men: “(1) intravenous administration of 1250 mgsodium thiosulphate over 10 min, which converts
234 MOHAMED NAGUIB

cyanide to nontoxic thiocyanate; (2) intravenousadministration of 300 mg sodium nitrite over 10min, which converts hemoglobin to methemoglo-bin [cyanide ions have higher affinity for methe-moglobin than for hemoglobin]; and (3) intrave-nous administration of 400 mg hydroxycobalaminover 20 min in order to form cyanocobalamin[even though the efficacy of hydroxycobalamin isquestionable]. Dicobalt edetate (300-600 mg intra-venous, repeated as necessary) is reserved for sec-ond-line treatment because of its side-effects (hy-pertension and nausea).”
Choking Agents
During WWI, chlorine (Cl2) and phosgene(COCl2) gases were used as chemical warfareagents. Currently, most of the chemical warfareagents are either liquids or solids. Chlorine is agreenish-yellow gas with a pungent smell. Chlo-rine reacts with water and liberates hypochlorousacid, hydrochloric acid, and oxygen free radicals,all of which cause tissue damage. Chlorine forms ahighly reactive free Cl� radical that induces cellulartoxicity and damage.
Phosgene is a colorless nonflammable gas, andits odor is similar to that of newly mown hay.2 Itwas produced by John Davy in 1812 and was firstused on the battlefield by the German army in1917. Phosgene is slightly soluble in water and ishydrolyzed slowly by moisture to form hydrochlo-ric acid. The acyl chloride moiety, which is a partof the phosgene molecule, is very unstable andreactive. One of the characteristics of the chockingagents is the latent formation of life-threatening,noncardiogenic pulmonary edema. Leukotrienesappear to be involved in the pathogenesis of pul-monary edema, which can be attenuated or eveninhibited by pretreatment with drugs that increaseadenosine 3�,5�-cyclic monophosphate concentra-tions,68 leukotriene inhibitors, and glutathione.69
After phosgene exposure, a patient may be free ofsymptoms for up to 48 hours before pulmonaryedema becomes apparent. Common initial symp-toms include mild irritation of the eyes, lacrima-tion, coughing, choking, tightness in the chest,nausea, vomiting, and headache.
Victims exposed only to phosgene gas do notpose significant risks of secondary contaminationto others unless they have been have contaminatedwith liquid phosgene. There is no antidote forchlorine and phosgene, mainly because of the for-
mation of free radicals with these agents. Themanagement of chlorine and phosgene toxicity islargely supportive.
Toxins
Toxins are toxic chemical compounds synthe-sized in nature by living organisms.
Botulinum Toxins
Botulinum toxin, produced by the bacteria Clos-tridium botulinum, is considered to be the mostpoisonous substance ever known.70 Botulinumtoxin is also known also as agent X.2 Arnon et al71
estimated that if 1 g of this toxin is aerosolized, itwould kill �1 million people. The toxin is a pro-tein available in 7 (designated A through G) dif-ferent forms. The most poisonous is type A (mo-lecular weight � 150,000 D). The lethal dose ofbotulinum toxin for a 70-kg human is estimated tobe approximately 0.7 �g if inhaled or 70 �g ifingested.71,72 In the former USSR, attempts weremade to splice the botulinum toxin gene from C.botulinum into other bacteria. All botulinum toxins(which include tetanus and botulinum toxins) in-hibit exocytosis via the cleavage of SNARE pro-teins (SNAP25, syntaxin 1, or synaptobrevin)73,74
SNARE is essential for docking synaptic vesiclesinto the presynaptic membrane before acetylcho-line release.73,74 The only specific treatment forbotulism is passive immunization with antitoxin,but once the victim has become poisoned (if notimmunized) there is no antidote. Botulism prefer-entially affects the cranial nerves, followed bygeneralized weakness and respiratory failure.66,75
Therapy for botulism consists of supportive careand passive immunization with equine antitoxin.(For a more extensive account on botulinum toxin,see Arnon et al.71)
Ricin
Ricin is a heterodimeric plant toxin isolatedfrom the bean of the caster oil, Ricinus communis.It is considered a very potent toxin.76 Ricin is alsoreferred to as agent W in the military arena.2 Itinhibits ribosome proteins, and the toxic dose forhumans is about 0.1-1.0 �g/kg, depending on themode of administration.2 It was used in the famous“umbrella tip” assassination of the Bulgarian jour-nalist Georgy Markov.77 Ricin causes vascularleak syndrome, characterized by hypoalbumine-mia, pulmonary edema, and death.78 A variety of
235PHARMACOLOGY OF COMMON CHEMICALS

ricin antitoxins are currently being investi-gated.79,80
Shellfish Toxins
At least 4 toxins (saxitoxin, ciguatoxin, tetrodo-toxin, and domoic acid) cause shellfish poison-ing.81 Paralytic shellfish poisoning is a seriousillness with significant neurological symptoms. Re-covery is usually complete and uncomplicated, butin severe cases it may result in respiratory paralysisand death. Polyclonal and monoclonal antibodiesare under investigation.82
Psychomimetic Agents
Hallucinogenic drugs such as lysergic acid di-ethylamide (LSD) can induce severe incapacita-tion.83 LSD is a semisynthetic analog of alkaloidsfound in plants and fungi. The aerosolized dose ofLSD that incapacitates 50% of exposed individuals(ID50) is estimated to be 6 �g/kg.84 LSD is unsta-ble, and it is doubtful that it can be used forchemical warfare. Nonetheless, there are other sta-ble chemical substances with effects similar toLSD that have chemical warfare potential. Theseinclude 3-quinuclidinyl benzilate (BZ) and a re-lated potent glycolate. Both are anticholinergicagents with psychomimetic properties. BZ (Fig 3)is a potent anticholinergic drug that is 25 timesmore potent than atropine. The ID50 for BZ is 6�g/kg.2 Less than 1 mg of BZ can produce an acutebrain syndrome characterized by delirium lastingfor 2 to 3 days, which can be reversed by phy-sostigmine and other anticholinesterases.2
CONCLUSIONS
Chemical warfare is an insidious form of war-fare. Not only individuals but also the environmentare vulnerable to these agents. The risks and long-term effects on the soil and groundwater are un-known, but chemical agents can affect both theeconomy and the food supply.85 Level C personal
protective equipment can provide protection dur-ing chemical warfare. Sophisticated detectionequipment is now available to monitor levels ofchemical warfare agents. With the growing aware-ness of the threat of the potential use of chemicalagents in the U.S., both the Occupational Safetyand Health Administration and the Joint Commis-sion on Accreditation of Healthcare Organizationshave issued new requirements for hospitals to in-crease their preparedness.86,87
REFERENCES
1. Volans GN, Karalliedde L: Long-term effects of chemicalweapons. Lancet 360:S35-S36, 2002 (suppl)
2. Sidell FR, Takafuji ET, Franz DR: Medical Aspects ofChemical and Biological Warfare. Washington, DC, Office ofThe Surgeon General, Department of the Army, 1997
3. Morita H, Yanagisawa N, Nakajima T, et al: Sarin poi-soning in Matsumoto, Japan. Lancet 346:290-293, 1995
4. Naguib M, Flood P, McArdle JJ, et al: Advances inneurobiology of the neuromuscular junction: implications forthe anesthesiologist. Anesthesiology 96:202-231, 2002
5. Soreq H, Seidman S: Acetylcholinesterase–new roles foran old actor. Nat Rev Neurosci 2:294-302, 2001
6. Sternfeld M, Ming G, Song H, et al: Acetylcholinesteraseenhances neurite growth and synapse development throughalternative contributions of its hydrolytic capacity, core protein,and variable C termini. J Neurosci 18:1240-1249, 1998
7. Sung JJ, Kim SJ, Lee HB, et al: Anticholinesterase in-duces nicotinic receptor modulation. Muscle Nerve 21:1135-1144, 1998
8. Darvesh S, Hopkins DA, Geula C: Neurobiology of bu-tyrylcholinesterase. Nat Rev Neurosci 4:131-138, 2003
9. Duysen EG, Li B, Xie W, et al: Evidence for nonacetyl-cholinesterase targets of organophosphorus nerve agent: super-sensitivity of acetylcholinesterase knockout mouse to VX le-thality. J Pharmacol Exp Ther 299:528-535, 2001
10. Henderson RF, Barr EB, Blackwell WB, et al: Responseof rats to low levels of sarin. Toxicol Appl Pharmacol 184:67-76, 2002
11. Khan WA, Dechkovskaia AM, Herrick EA, et al: Acutesarin exposure causes differential regulation of choline acetyl-transferase, acetylcholinesterase, and acetylcholine receptors inthe central nervous system of the rat. Toxicol Sci 57:112-120,2000
12. Rocha ES, Santos MD, Chebabo SR, et al: Low concen-trations of the organophosphate VX affect spontaneous andevoked transmitter release from hippocampal neurons: toxico-logical relevance of cholinesterase-independent actions. Toxi-col Appl Pharmacol 159:31-40, 1999
13. Albuquerque EX, Deshpande SS, Kawabuchi M, et al:Multiple actions of anticholinesterase agents on chemosensitivesynapses: molecular basis for prophylaxis and treatment oforganophosphate poisoning. Fundam Appl Toxicol 5:S182-S203, 1985 (suppl)
14. Santos MD, Pereira EF, Aracava Y, et al: Low concen-trations of pyridostigmine prevent soman-induced inhibition ofGABAergic transmission in the central nervous system: in-
Fig 3. BZ, a benzilate and a potent glycolate that hashallucinating properties similar to LSD.
236 MOHAMED NAGUIB

volvement of muscarinic receptors. J Pharmacol Exp Ther 304:254-265, 2003
15. Grob D, Harvey AM: The effects and treatment of nervegas poisoning. Am J Med 14:52-63, 1953
16. Abdel–Rahman A, Shetty AK, Abou–Donia MB: Acuteexposure to sarin increases blood brain barrier permeability andinduces neuropathological changes in the rat brain: dose-re-sponse relationships. Neuroscience 113:721-741, 2002
17. Lallement G, Veyret J, Masqueliez C, et al: Efficacy ofhuperzine in preventing soman-induced seizures, neuropatho-logical changes and lethality. Fundam Clin Pharmacol 11:387-394, 1997
18. McDonough JH, Jr, Shih TM: Neuropharmacologicalmechanisms of nerve agent-induced seizure and neuropathol-ogy. Neurosci Biobehav Rev 21:559-579, 1997
19. Sirkka U, Nieminen SA, Ylitalo P: Neurobehavioraltoxicity with low doses of sarin and soman. Methods Find ExpClin Pharmacol 12:245-250, 1990
20. Baille V, Dorandeu F, Carpentier P, et al: Acute expo-sure to a low or mild dose of soman: biochemical, behavioraland histopathological effects. Pharmacol Biochem Behav 69:561-569, 2001
21. Lennox WJ, Harris LW, Anderson DR, et al: Successfulpretreatment/therapy of soman, sarin and VX intoxication. DrugChem Toxicol 15:271-283, 1992
22. Carpentier P, Foquin A, Rondouin G, et al: Effects ofatropine sulphate on seizure activity and brain damage pro-duced by soman in guinea-pigs: ECoG correlates of neuropa-thology. Neurotoxicology 21:521-540, 2000
23. Sellin LC, McArdle JJ: Multiple effects of 2,3-butane-dione monoxime. Pharmacol Toxicol 74:305-313, 1994
24. Rousseaux CG, Dua AK: Pharmacology of HI-6, anH-series oxime. Can J Physiol Pharmacol 67:1183-1189, 1989
25. Dunn MA, Sidell FR: Progress in medical defenseagainst nerve agents. JAMA 262:649-652, 1989
26. Nzerue MC: Lassa fever: review of virology, immuno-pathogenesis, and algorithms for control and therapy. Cent AfrJ Med 38:247-252, 1992
27. Singh S, Chaudhry D, Behera D, et al: Aggressive atro-pinisation and continuous pralidoxime (2-PAM) infusion inpatients with severe organophosphate poisoning: experience ofa northwest Indian hospital. Hum Exp Toxicol 20:15-18, 2001
28. Karczmar AG: Acute and long lasting central actions oforganophosphorus agents. Fundam Appl Toxicol 4:S1-S17,1984 (suppl)
29. Michel HO, Hackley BE, Jr, Berkowitz L, et al: Ageingand dealkylation of Soman (pinacolylmethylphosphonofluo-ridate)-inactivated eel cholinesterase. Arch Biochem Biophys121:29-34, 1967
30. Sidell FR, Groff WA: The reactivatibility of cholin-esterase inhibited by VX and sarin in man. Toxicol Appl Phar-macol 27:241-252, 1974
31. Dirnhuber P, French MC, Green DM, et al: The protec-tion of primates against soman poisoning by pretreatment withpyridostigmine. J Pharm Pharmacol 31:295-299, 1979
32. Kassa J: Review of oximes in the antidotal treatment ofpoisoning by organophosphorus nerve agents. J Toxicol ClinToxicol 40:803-816, 2002
33. Gordon JJ, Leadbeater L, Maidment MP: The protectionof animals against organophosphate poisoning by pretreatmentwith a carbamate. Toxicol Appl Pharmacol 43:207-216, 1978
34. Doctor BP, Blick DW, Caranto G, et al: Cholinesterasesas scavengers for organophosphorus compounds: protection ofprimate performance against soman toxicity. Chem Biol Inter-act 87:285-293, 1993
35. Maxwell DM, Castro CA, De La Hoz DM, et al: Pro-tection of rhesus monkeys against soman and prevention ofperformance decrement by pretreatment with acetylcholinester-ase. Toxicol Appl Pharmacol 115:44-49, 1992
36. Raveh L, Grunwald J, Marcus D, et al: Human butyryl-cholinesterase as a general prophylactic antidote for nerve agenttoxicity. In vitro and in vivo quantitative characterization. Bio-chem Pharmacol 45:2465-24674, 1993
37. Lenz DE, Brimfield AA, Hunter KW, Jr, et al: Studiesusing a monoclonal antibody against soman. Fundam ApplToxicol 4:S156-S164, 1984 (suppl)
38. Lenz DE, Yourick JJ, Dawson JS, et al: Monoclonalantibodies against soman: characterization of soman stereoiso-mers. Immunol Lett 31:131-135, 1992
39. Cowan FM, Broomfield CA, Lenz DE, et al: Protectiveaction of the serine protease inhibitor N-tosyl-L-lysine chloro-methyl ketone (TLCK) against acute soman poisoning: J ApplToxicol 21:293-296, 2001
40. Dacre JC, Goldman M: Toxicology and pharmacology ofthe chemical warfare agent sulfur mustard. Pharmacol Rev48:289-326, 1996
41. Graham JS, Schomacker KT, Glatter RD, et al: Efficacyof laser debridement with autologous split-thickness skin graft-ing in promoting improved healing of deep cutaneous sulfurmustard burns. Burns 28:719-730, 2002
42. Lakshmana Rao PV, Vijayaraghavan R, Bhaskar AS:Sulphur mustard induced DNA damage in mice after dermaland inhalation exposure. Toxicology 139:39-51, 1999
43. Bijani K, Moghadamnia AA: Long-term effects of chem-ical weapons on respiratory tract in Iraq-Iran war victims livingin Babol (North of Iran). Ecotoxicol Environ Saf 53:422-424,2002
44. Varma SD, Devamanoharan PS, Ali AH, et al: Cornealdamage by half mustard (2-chloroethyl ethyl sulfide, CEES) invitro preventive studies: a histologic and electron microscopicevaluation. J Ocul Pharmacol Ther 14:413-421, 1998
45. Maisonneuve A, Callebat I, Debordes L, et al: Biologicalfate of sulphur mustard in rat: toxicokinetics and disposition.Xenobiotica 23:771-780, 1993
46. Momeni AZ, Enshaeih S, Meghdadi M, et al: Skin man-ifestations of mustard gas. A clinical study of 535 patientsexposed to mustard gas. Arch Dermatol 128:775-780, 1992
47. Borak J, Sidell FR: Agents of chemical warfare: sulfurmustard. Ann Emerg Med 21:303-308, 1992
48. Eldad A, Ben Meir P, Breiterman S, et al: Superoxidedismutase (SOD) for mustard gas burns. Burns 24:114-119,1998
49. Fox M, Scott D: The genetic toxicology of nitrogen andsulphur mustard. Mutat Res 75:131-168, 1980
50. Watson AP, Griffin GD: Toxicity of vesicant agentsscheduled for destruction by the Chemical Stockpile DisposalProgram. Environ Health Perspect 98:259-280, 1992
51. Reutter S: Hazards of chemical weapons release duringwar: new perspectives. Environ Health Perspect 107:985-990,1999
237PHARMACOLOGY OF COMMON CHEMICALS

52. Anderson DR, Byers SL, Vesely KR: Treatment of sulfurmustard (HD)-induced lung injury. J Appl Toxicol 20:S129-S132, 2000 (suppl)
53. Henriksson J, Johannisson A, Bergqvist PA, et al: Thetoxicity of organoarsenic-based warfare agents: in vitro and invivo studies. Arch Environ Contam Toxicol 30:213-219, 1996
54. Aposhian HV, Hsu CA, Hoover TD: DL- and meso-dimercaptosuccinic acid: in vitro and in vivo studies with so-dium arsenite. Toxicol Appl Pharmacol 69:206-213, 1983
55. Vilensky JA, Redman K: British anti-Lewisite (dimer-caprol): an amazing history. Ann Emerg Med 41:378-383, 2003
56. Sidell FR, Borak J: Chemical warfare agents: II. Nerveagents. Ann Emerg Med 21:865-871, 1992
57. Koenig R: Environmental disasters. Wildlife deaths are agrim wake-up call in Eastern Europe. Science 287:1737-1738,2000
58. Jones MG, Bickar D, Wilson MT, et al: A re-examina-tion of the reactions of cyanide with cytochrome c oxidase.Biochem J 220:57-66, 1984
59. Borron SW, Baud FJ: Acute cyanide poisoning: clinicalspectrum, diagnosis, and treatment. Arh Hig Rada Toksikol47:307-322, 1996
60. Kanthasamy AG, Borowitz JL, Pavlakovic G, et al:Dopaminergic neurotoxicity of cyanide: neurochemical, histo-logical, and behavioral characterization. Toxicol Appl Pharma-col 126:156-163, 1994
61. Patel MN, Yim GK, Isom GE: Blockade of N-methyl-D-aspartate receptors prevents cyanide-induced neuronal injuryin primary hippocampal cultures: Toxicol Appl Pharmacol 115:124-129, 1992
62. Yang CW, Borowitz JL, Gunasekar PG, et al: Cyanide-stimulated inositol 1,4,5-trisphosphate formation: an intracellu-lar neurotoxic signaling cascade. J Biochem Toxicol 11:251-256, 1996
63. Gunasekar PG, Sun PW, Kanthasamy AG, et al: Cya-nide-induced neurotoxicity involves nitric oxide and reactiveoxygen species generation after N-methyl-D-aspartate receptoractivation. J Pharmacol Exp Ther 277:150-155, 1996
64. Bonfoco E, Krainc D, Ankarcrona M, et al: Apoptosisand necrosis: two distinct events induced, respectively, by mildand intense insults with N-methyl-D-aspartate or nitric oxide/superoxide in cortical cell cultures: Proc Natl Acad Sci USA92:7162-7166, 1995
65. Greer JJ, Carter JE: Effects of cyanide on the neuralmechanisms controlling breathing in the neonatal rat in vitro.Neurotoxicology 16:211-215, 1995
66. Martin CO, Adams HP, Jr: Neurological aspects of bio-logical and chemical terrorism: a review for neurologists. ArchNeurol 60:21-25, 2003
67. White SM: Chemical and biological weapons. Implicationsfor anaesthesia and intensive care. Br J Anaesth 89:306-324, 2002
68. Sciuto AM, Strickland PT, Kennedy TP, et al: Intratrachealadministration of DBcAMP attenuates edema formation in phos-gene-induced acute lung injury. J Appl Physiol 80:149-157, 1996
69. Sciuto AM, Strickland PT, Kennedy TP, et al: Protectiveeffects of N-acetylcysteine treatment after phosgene exposurein rabbits. Am J Respir Crit Care Med 151:768-772, 1995
70. Gill DM: Bacterial toxins: a table of lethal amounts.Microbiol Rev 46:86-94, 1982
71. Arnon SS, Schechter R, Inglesby TV, et al: Botulinumtoxin as a biological weapon: medical and public health man-agement. JAMA 285:1059-1070, 2001
72. Albin RL: Basal ganglia neurotoxins. Neurol Clin 18:665-680, 2000
73. Schiavo G, Matteoli M, Montecucco C: Neurotoxinsaffecting neuroexocytosis. Physiol Rev 80:717-766, 2000
74. Naguib M, Magboul MM: Adverse effects of neuromus-cular blockers and their antagonists. Drug Saf 18:99-116, 1998
75. Townes JM, Cieslak PR, Hatheway CL, et al: An out-break of type A botulism associated with a commercial cheesesauce. Ann Intern Med 125:558-563, 1996
76. Lord JM, Roberts LM, Robertus JD: Ricin: structure,mode of action, and some current applications. Faseb J 8:201-208, 1994
77. Crompton R, Gall D: Georgi Markov–death in a pellet.Med Leg J 48:51-62, 1980
78. Soler–Rodriguez AM, Ghetie MA, Oppenheimer–MarksN, et al: Ricin A-chain and ricin A-chain immunotoxins rapidlydamage human endothelial cells: implications for vascular leaksyndrome. Exp Cell Res 206:227-234, 1993
79. Miller DJ, Ravikumar K, Shen H, et al: Structure-baseddesign and characterization of novel platforms for ricin andshiga toxin inhibition. J Med Chem 45:90-98, 2002
80. Lemley PV, Thalley BS, Stafford DC: Prophylactic andtherapeutic efficacy of an avian antitoxin in ricin intoxication.Ther Immunol 2:59-66, 1995
81. Watters MR: Organic neurotoxins in seafoods. Clin Neu-rol Neurosurg 97:119-124, 1995
82. Usleber E, Dietrich R, Burk C, et al: Immunoassaymethods for paralytic shellfish poisoning toxins. J AOAC Int84:1649-1656, 2001
83. Kinston W, Rosser R: Disaster: effects on mental andphysical state. J Psychosom Res 18:437-456, 1974
84. Ketchum JS: Detection of LSD. Am J Psychiatry 125:1447-1448, 1969
85. Stellman JM, Stellman SD, Weber T, et al: A geographicinformation system for characterizing exposure to agent orangeand other herbicides in Vietnam. Environ Health Perspect 111:321-328, 2003
86. 1910.120. CP. Washington, DC, Government PrintingOffice, 1995
87. Joint Commission on Accreditation of Healthcare Orga-nizations: Comprehensive Accreditation Manual for Hospitals.Chicago, IL, Oakbrook Terrace, 1996
238 MOHAMED NAGUIB