
The Peaks Unit: Developing an Integrated Treatment Model Dr Todd Hogue Paper presented at: Care not...
30
The Peaks Unit: Developing an Integrated Treatment Model Dr Todd Hogue Paper presented at: Care not containment: Interventions for mentally disordered individuals 24-25 June 2004, Royal Moat House Hotel Nottingham, UK [email protected]
-
Upload
rosanna-fields -
Category
Documents
-
view
220 -
download
1
Transcript of The Peaks Unit: Developing an Integrated Treatment Model Dr Todd Hogue Paper presented at: Care not...
The Peaks Unit: Developing an Integrated Treatment Model
Dr Todd HoguePaper presented at:
Care not containment: Interventions for mentally disordered individuals
24-25 June 2004, Royal Moat House Hotel
Nottingham, UK
DSPD: The Challenge
• Untreatable?• Psychopathy • Personality Disorder
• Difficult to manageImpulsive Aggressive Manipulative Predatory
Volatile Attention Seeking Needy Violent
Vulnerable Emotionally Labile Self Harming

What Kind of Patients?
• A couple of examples…
Case 1 - JP
• Age – 31• Wounding: Life 7yr min• Mother – mental health
problems• Farther – alcoholic and
violent• Q: brain damage at birth• 2-3 hyperactive/
behavioural problems
• Family separation 6yrs
• 6 sexual abuse?• 7 challenging behaviour• 9 special school/homes
– Threaten knife, impulsive, aggressive, social isolation
• 11 repeat self-harm• 12 violent attack – family• 17 violence, threat with
knife, fire setting, cruelty to animals
• 20 attempt - strangle resident
• 20-23 aimless lifestyle, heavy drinking, casual sex
Case 1 - JP
• History:– Assaults, breech of peace,
affray, imp-police– Repeat institutional
violence and threats to kill• Index:
– wounding with intent– alcohol – paid for sex– violent urge to kill– Strangles, assaults– Victim escapes
• Violent fantasies• Voices / visions• Religious fixation: Jewish• Gender dysphoria –
attempted self castration• Poor institutional
behaviour– Moved, seg, hospital unit
• Neuropsychological problems?
• Little “treatment”• PD: Borderline, ASPD,
Paranoid

Case 2 -JU
• Age – 33• Rape – 6yrs• ‘raging’ family violence• 6 - in care • 7-9 attempts to foster
or return home• Early conduct disorder• Boarding school to 16
• 16+: acquisitive offences
• 19: endanger life – arson
• 27: assault partner, controlled drugs
• Index offence– Drug induced psychosis?– Belief of Ying/Yang– Rape of stranger(?) – Allows her to go

Case 2 - JU
• Axis I– ADHD, cannabis,
amphetamine dependence, A-I psychotic disorder
• Axis II – Schizotypal, Antisocial,
Borderline, Histrionic, Narcissistic
• High Psychopathy• High / very high risk
• Substance use• Callousness• Impulsivity• Failure to manage violence• Limited treatment – none
on sexual offending• Denial of sexual motivation• Released on licence –
failed• Likely to be detained
beyond sentence length

The Task
• An integrated approach to assessment and treatment
Personality Disorder
An enduring pattern… deviates markedly from the expectations of the individual’s culture.
Manifested in: – cognitive, – affective, – interpersonal functioning – impulse control
… inflexible and pervasive across personal and social situations
... leads to clinically significant distress or impairment… pattern is stable and or long duration … onset traced to adolescence or early childhood

Risk / Violence Assessment
• Identifying risk factors: the RISK of WHAT happening with WHO in WHAT SITUATION(S)
• How does the individual function?– Interpersonal– Intrapersonal– Core beliefs– Bio-Physiological
• Linking individual functioning with risk factors

The Risk - Personality Link
• Look for repeating patterns reflective of risk and consistent over time
• Risk predictors > dynamic factors > personality• Hypothesise individual factors linked to risk and
personality • Predict interaction style of PD as it relates to
parallel risk related behaviour• Repeatedly revisit formulation of risk / PD link

What is an integrated model?
• Whole person assessment
• Multiple assessments
• MDT working
• Team decisions
• Agreed targets
• Information fed into Individual Development Plan (IDP)

Conceptual Background
• An Integrated Approach to Treatment – Livesley (2003)
• Good Lives – Ward (2002)
• Hierarchy of Need – Linehan (1993)
• Therapeutic Community Principles• Case Formulation • Structuring Clinical Judgment
– Goal Attainment Scaling
INDIVIDUALISED ASSESSMENT
• Whole Person Approach
• Comprehensive Assessment
• Identify Dynamic Factors
• Target deficits/Criminogenic needs
• Treatment Hierarchy/Prioritise needs

Patient Focused
• Client Centred
• Needs and deficits
• Strengths and abilities
• Patient involvement
• Motivational structure
• Collaborative

Pragmatic difficulties with traditional ways of working
• Single model (Medical)
• Hierarchical decision making
• Multiple formulations
• Different perceptions of patients
• Little patient involvement
• No central resource or document

Integrated Treatment Plan
• Integrate assessment information
• Case formulation
• Shared treatment formulation
• Individual development plan
• Coherent and consistent documentation

Integrated Regime
• A “normalised” day
• Multidisciplinary working across interventions
• Consistent clinical teams
• Therapy teams – linked to each patient
• Routine / timing to facilitate clinical practice
• Agreed team decisions.

ASSESSMENT
WARD
MOTIVATIONBuilding the relationship and therapeutic alliance
First stage assessment
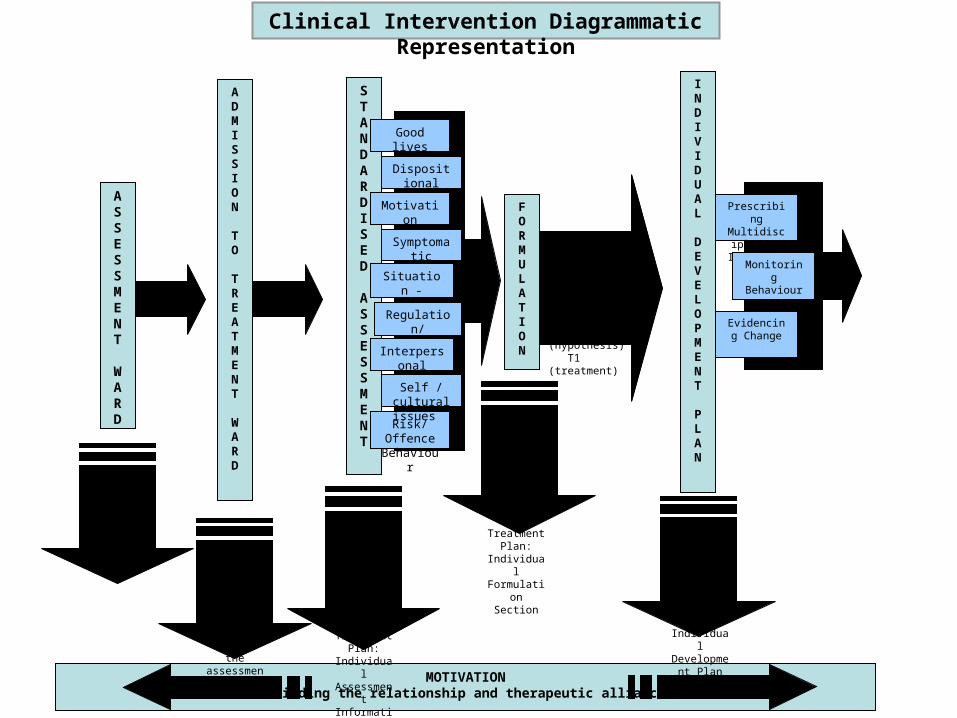
Clinical Intervention Diagrammatic Representation

DSPD Core Assessment
Three critical components
• High Risk – More likely than not• Severe Personality Disorder
– Very High Psychopathy– High Psychopathy & 1 PD – 2 different PDs
• Functional Risk / PD Link

STANDARDISED
ASSESSMENT
ASSESSMENT
WARD
ADMISSION
TO
TREATMENT
WARD
MOTIVATIONBuilding the relationship and therapeutic alliance
First stage assessment
Individual Development
Plan for engagement
with the assessment
process
Risk/Offence Behaviour
Second stage assessmentRecorded in Integrated
Treatment Plan: Individual
Assessment Information
Section
Good lives
Motivation
Symptomatic
Dispositional
Situation -environment
Regulation/ control
Interpersonal
Self / cultural issues
Clinical Intervention Diagrammatic Representation

Individual Assessment Information
• Physical health• Symptomatic factors• Situational/
Environmental factors• Regulation / Control
factors• Neuropsychological
assessment
• Dispositional traits• Interpersonal factors• Self system• Risk / Offending
issues• Mental health factors
(axis I)

STANDARDISED
ASSESSMENT
ASSESSMENT
WARD Reviewed and
agreed by therapy team. Transferred to
Integrated Treatment Plan:
Individual Formulation
Section
ADMISSION
TO
TREATMENT
WARD
MOTIVATIONBuilding the relationship and therapeutic alliance
First stage assessment
Individual Development
Plan for engagement
with the assessment
process
Treatment Needs & Pathway
What & Why?How?
When? N1 (need) H1 (hypothesis) T1 (treatment)
FORMULATION
Risk/Offence Behaviour
Second stage assessmentRecorded in Integrated
Treatment Plan: Individual
Assessment Information
Section
Good lives
Motivation
Symptomatic
Dispositional
Situation -environment
Regulation/ control
Interpersonal
Self / cultural issues
Clinical Intervention Diagrammatic Representation
Individual Case formulation
• Case formulation model• What, why, how & when • Areas of strengths and weaknesses • Multiple issues, systems and formulations• Hypotheses (testable)• Integrate motivational issues• Diagrammatic representation• Agreed “Team formulation”
STANDARDISED
ASSESSMENT
ASSESSMENT
WARD Reviewed and
agreed by therapy team. Transferred to
Integrated Treatment Plan:
Individual Formulation
Section
ADMISSION
TO
TREATMENT
WARD
MOTIVATIONBuilding the relationship and therapeutic alliance
Prescribing Multidisciplinary
Intervention
Monitoring Behaviour
Evidencing Change
INDIVIDUAL DEVELOPMENT
PLAN
Recorded in Integrated
Treatment Plan: Individual
Development Plan Section
First stage assessment
Individual Development
Plan for engagement
with the assessment
process
Treatment Needs & Pathway
What & Why?How?
When? N1 (need) H1 (hypothesis) T1 (treatment)
FORMULATION
Risk/Offence Behaviour
Second stage assessmentRecorded in Integrated
Treatment Plan: Individual
Assessment Information
Section
Good lives
Motivation
Symptomatic
Dispositional
Situation -environment
Regulation/ control
Interpersonal
Self / cultural issues
Clinical Intervention Diagrammatic Representation
Individual development plan
• Focuses on treatment need• Aim of interventions• Objectives
GroupIndividualEnvironmental
• Specified “success criteria”• Regular – identified review process• Evidenced evaluation

STANDARDISED
ASSESSMENT
ASSESSMENT
WARD Reviewed and
agreed by therapy team. Transferred to
Integrated Treatment Plan:
Individual Formulation
Section
N2 (need)H2 (hypothesis)T2 (treatment)
Reviewed by Therapy
Team (CPA)
ADMISSION
TO
TREATMENT
WARD
MOTIVATIONBuilding the relationship and therapeutic alliance
Prescribing Multidisciplinary
Intervention
Monitoring Behaviour
Evidencing Change
INDIVIDUAL DEVELOPMENT
PLAN
Recorded in Integrated
Treatment Plan: Individual
Development Plan Section
First stage assessment
Individual Development
Plan for engagement
with the assessment
process
Treatment Needs & Pathway
What & Why?How?
When? N1 (need) H1 (hypothesis) T1 (treatment)
FORMULATION
Risk/Offence Behaviour
Second stage assessmentRecorded in Integrated
Treatment Plan: Individual
Assessment Information
Section
Good lives
Motivation
Symptomatic
Dispositional
Situation -environment
Regulation/ control
Interpersonal
Self / cultural issues
Clinical Intervention Diagrammatic Representation

Individual treatment formulation
Includes: • Responsivity & therapeutic engagement issues • Clear hierarchy of need• Identified treatment options• Clear alternatives pathways
Structuring Clinical Judgment:Clinical Progress
• How to evidencing change• Pulling information from different sources
together• Clear criteria and understanding –
treatment needs and targets• Clearly defined goals• Goal Attainment Scaling (GAS) Model• Structure to guide clinicians

Summary
• Matches integrated model principles• Multidisciplinary • Actively involves and includes the patient• Shared Team view of:
– Patients’ needs and strengths– Shared “team” formulation – Hierarchy of treatment provision– Clear treatment pathways
• Single source documentation


















