The Not-So-Gentle Summer Febreze
44
The Not-So-Gentle Summer Febreze Omar Malas MD Practical Updates in Anesthesiology, February 4 th , 2020 Department of Anesthesiology Michigan Medicine
Transcript of The Not-So-Gentle Summer Febreze
The Not-So-Gentle Summer Febreze
Omar Malas MD Practical Updates in Anesthesiology, February 4th, 2020
Department of AnesthesiologyMichigan Medicine

Disclosures
• None
Case
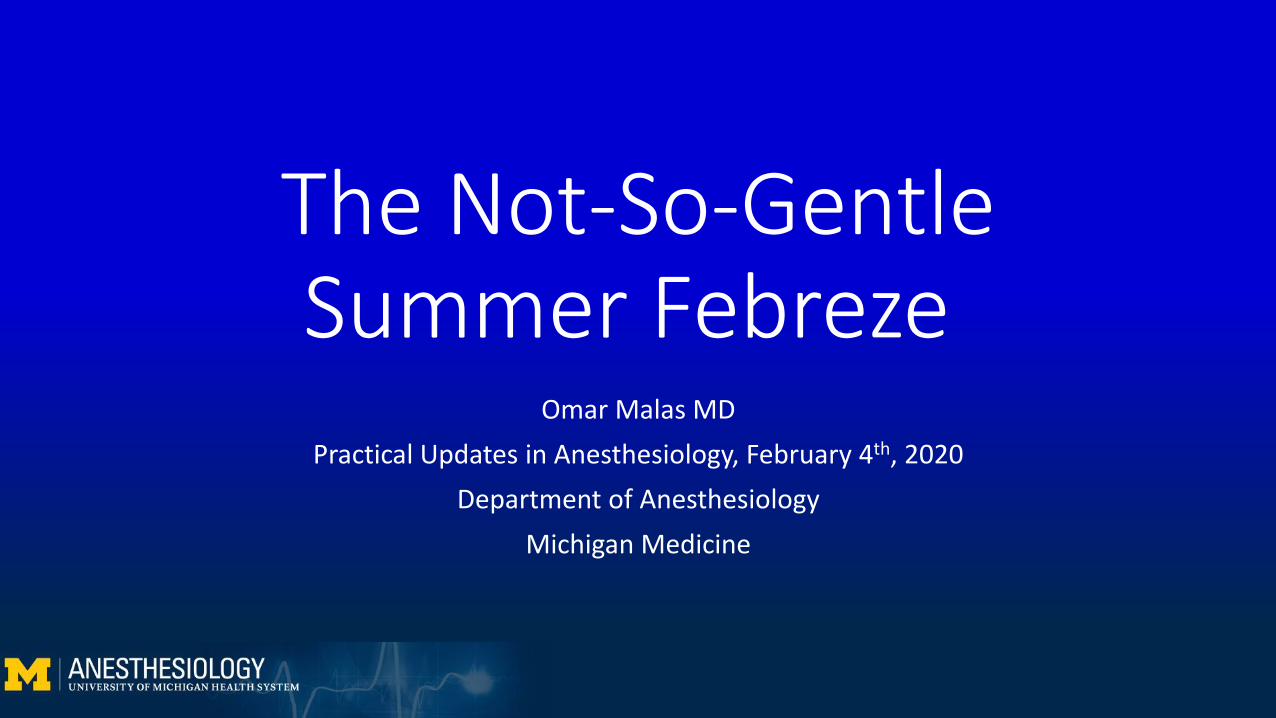
• 74 yo 84kg Male presents for segment IVb/V partial hepatectomy
• PMHx: cholangiocarcinoma s/p chemotherapy, COPD, Type II DM, HTN
• PSHx: Bilateral cataract extraction, liver biopsy, L subclavian central venous port placement
Casaccia M, Andorno E, Di Domenico s, et al. Laparoscopic liver resection for hepatocellular carcinoma in cirrhotic patients. Feasibility of nonanatomic resection in difficult tumor locations. Journal of Minimal Access Surgery. 2011;7(4): 222-226.

Case
• Meds: Aspirin 81mg qday, Metformin 500mg BID, Metoprolol succinate 75mg qday, simvastatin 20mg qday
• Allergies: None• SHx: Former smoker, Quit 2002 (30 pack-year), former EtOH abuse,
quit 1972

Perioperative Course• Pre-operative management
• T7/8 thoracic epidural, no complications• Right radial A-line
• Induction• Fentanyl 50mcg, lidocaine 60mg, propofol 120mg, rocuronium 70mg• Grade 2M, 2a view with Mac 4 VL, 8.0mm ETT at 22cm• 16g and 14g placed
• Maintenance• Isoflurane at 0.8-1 MAC, intermittent fentanyl and rocuronium boluses• Goals: judicious fluid management, low CVP to decrease bleeding

Intraoperative Course• 1030 – 1130: Relieved for lecture• 1110: Surgical resection complete, 600cc IV fluids given• 1130: Midway through closing, hemodynamically stable, estimated blood
loss 850cc, IV fluids 1800cc• 1136: Surgical dressing complete, pt has 1/4 TOF• 1137: 4mg/kg (360mg) Sugammadex given

Hemodynamic Collapse• 1139:
• A-line reading 41/30 mmHg, no pulse oximetry reading• A-line transducer appropriately positioned• No femoral or carotid pulses palpable

Differential Diagnosis
• STEMI/NSTEMI• PE• Venous air embolism• Anaphylaxis• Epidural bolus• Hemorrhage • Neurogenic shock• Respiratory arrest• Pneumothorax• Sepsis
• Dysrhythmia• Medication overdose/error• Hypoglycemia• Pulmonary HTN• Severe MR• Ventricular septal rupture• Ventricular free wall rupture• Chordae tendineae or papillary muscle
rupture• Cardiac tamponade

OutlineI. Case IntroductionII. Anaphylaxis
I. DefinitionII. PathophysiologyIII. DiagnosisIV. Causal AgentsV. OR considerationsVI. SeverityVII. Treatment
III. SugammadexI. Brief historyII. Anaphylactic incidenceIII. Cross reactivity
IV. Case FinaleV. Questions
Anaphylaxis – Definition
Sampson HA, Muñoz-Furlong A, Campbell RL, et al. Second symposium on the definition and management of anaphylaxis: Summary report—Second National Institute of Allergy and Infectious Disease/Food Allergy and Anaphylaxis Network symposium. J. Allergy Clin. Immunol.2006;117(2):391–397.
“Anaphylaxis is a serious allergic reaction that is rapid in onset and may cause death”

Anaphylaxis – Pathophysiology
• Allergic reactions: IgE, complement, nonimmunologic mast cell activation
• Initial exposure• IgE antibodies produced by B cells in response to allergen • Clinically silent
Dewachter P, Mouton-Faivre C, Emala CW. Anaphylaxis and Anesthesia Controversies and New Insights. Anesthesiol. J. Am. Soc. Anesthesiol. 2009;111(5):1141–1150.

Anaphylaxis – Pathophysiology
Ali MR. Anaphylaxis. Slideshare.net. 2015; accessed 9/18/18
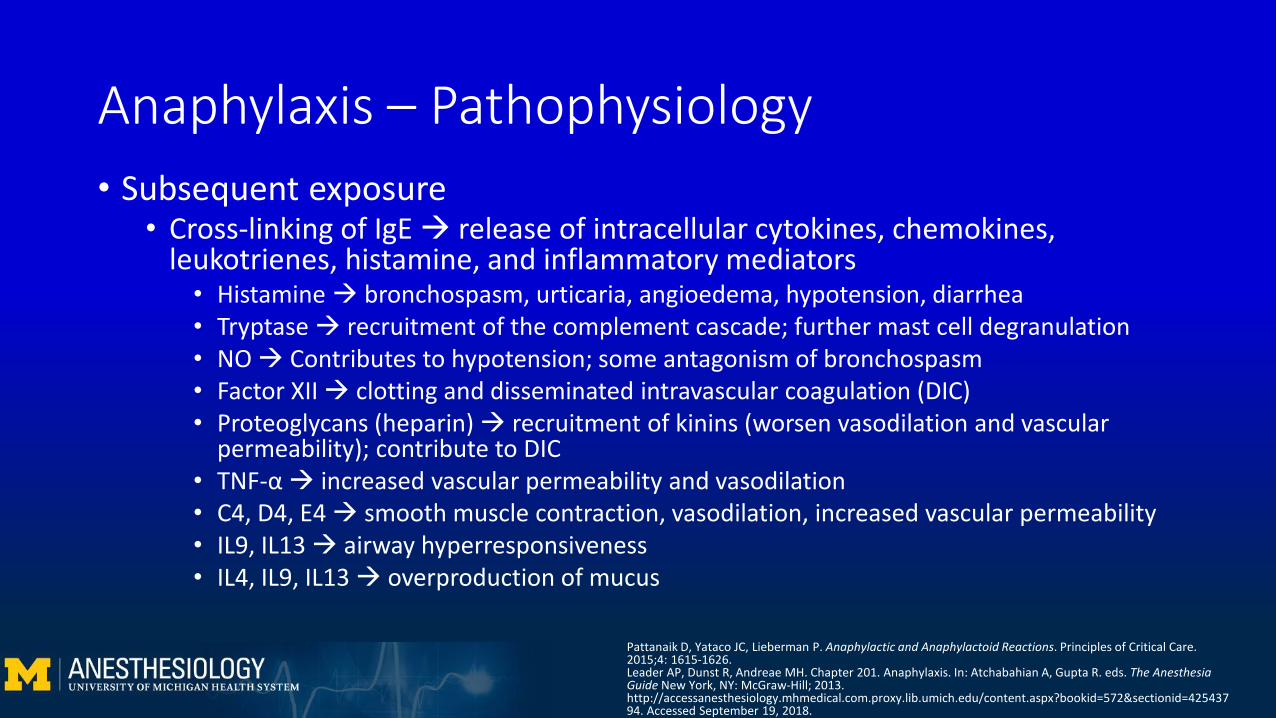
Anaphylaxis – Pathophysiology • Subsequent exposure
• Cross-linking of IgE release of intracellular cytokines, chemokines, leukotrienes, histamine, and inflammatory mediators
• Histamine bronchospasm, urticaria, angioedema, hypotension, diarrhea• Tryptase recruitment of the complement cascade; further mast cell degranulation• NO Contributes to hypotension; some antagonism of bronchospasm• Factor XII clotting and disseminated intravascular coagulation (DIC)• Proteoglycans (heparin) recruitment of kinins (worsen vasodilation and vascular
permeability); contribute to DIC• TNF-α increased vascular permeability and vasodilation• C4, D4, E4 smooth muscle contraction, vasodilation, increased vascular permeability• IL9, IL13 airway hyperresponsiveness• IL4, IL9, IL13 overproduction of mucus
Pattanaik D, Yataco JC, Lieberman P. Anaphylactic and Anaphylactoid Reactions. Principles of Critical Care. 2015;4: 1615-1626.Leader AP, Dunst R, Andreae MH. Chapter 201. Anaphylaxis. In: Atchabahian A, Gupta R. eds. The Anesthesia Guide New York, NY: McGraw-Hill; 2013. http://accessanesthesiology.mhmedical.com.proxy.lib.umich.edu/content.aspx?bookid=572§ionid=42543794. Accessed September 19, 2018.

Anaphylactic vs Anaphylactoid ReactionsAnaphylactic Anaphylactoid
Mechanism IgE-mediated mast cell activation Complement-mediated direct mast cell activation
Clinical Presentation Same Same
Clinical Manifestation More severe* Less severe*
Histamine Elevated Elevated
Tryptase Elevated Elevated or unchanged
Specific IgE assays Positive Negative
Sensitization required? Yes No
Intradermal Skin testing Positive Negative
Mertes PM, Laxenaire M-C, Alla F. Anaphylactic and Anaphylactoid Reactions Occurring during Anesthesia in France in 1999–2000. Anesthesiol. J. Am. Soc. Anesthesiol. 2003;99(3):536–545.Lagopoulos V, Gigi E. Anaphylactic and anaphylactoid reactions during the perioperative period. Hippokratia. 2011;15(2):138–140.

Anaphylaxis – Clinical Features
Leader AP, Dunst R, Andreae MH. Chapter 201. Anaphylaxis. In: Atchabahian A, Gupta R. eds. The Anesthesia Guide New York, NY: McGraw-Hill; 2013. Shutterstock.comWebMD.com

Anaphylaxis – Diagnosis
Sampson HA, Muñoz-Furlong A, Campbell RL, et al. Second symposium on the definition and management of anaphylaxis: Summary report—Second National Institute of Allergy and Infectious Disease/Food Allergy and Anaphylaxis Network symposium. J. Allergy Clin. Immunol.2006;117(2):391–397.

Anaphylaxis – Diagnosis
Sampson HA, Muñoz-Furlong A, Campbell RL, et al. Second symposium on the definition and management of anaphylaxis: Summary report—Second National Institute of Allergy and Infectious Disease/Food Allergy and Anaphylaxis Network symposium. J. Allergy Clin. Immunol.2006;117(2):391–397.
1. Unknown allergen for that patient
2. Known allergen for that patient
+ or

Anaphylaxis – Causal Agents• Overall incidence between 1:3500 and 1:20,000 anesthetics
• Female predominant (2:1)• Neuromuscular blocking agents (NMBA)
• 50-70% of periop anaphylaxis • Quaternary ammonium IgE mediated reaction• Benzylisoquinolines non-IgE mediated reactions
• Natural rubber latex• 5-15% of periop anaphylaxis
• Antibiotics• Up to 15% of periop anaphylaxis• Penicillins and cephalosporins responsible for 70% of periop anaphylaxis from
antibiotics
Leo ED, Donne PD, Calogiuri GF, Macchia L, Nettis E. Focus on the agents most frequently responsible for perioperative anaphylaxis. Clin. Mol. Allergy. 2018;16(1):16.Kroigaard M, Garvey LH, Gillberg L, et al. Scandinavian Clinical Practice Guidelines on the diagnosis, management and follow-up of anaphylaxis during anaesthesia*. Acta Anaesthesiol. Scand.2007;51(6):655–670.

Anaphylaxis – OR Considerations
• Signs and symptoms may be masked by OR circumstances• Tachycardia
• Masked by cholinergic drugs, beta blockers, bradycardia associated with GA
• Hypotension• Blamed on induction agents, opioids, beta blockers, NMBAs
• Urticaria• May be missed as patient is covered by drapes
• Respiratory: laryngeal edema, cough, bronchospasm• Masked by intubation and mechanical ventilation
De Feo G, Parente R, Triggiani M. Pitfalls in anaphylaxis. Curr. Opin. Allergy Clin. Immunol. 2018;18(5):382.
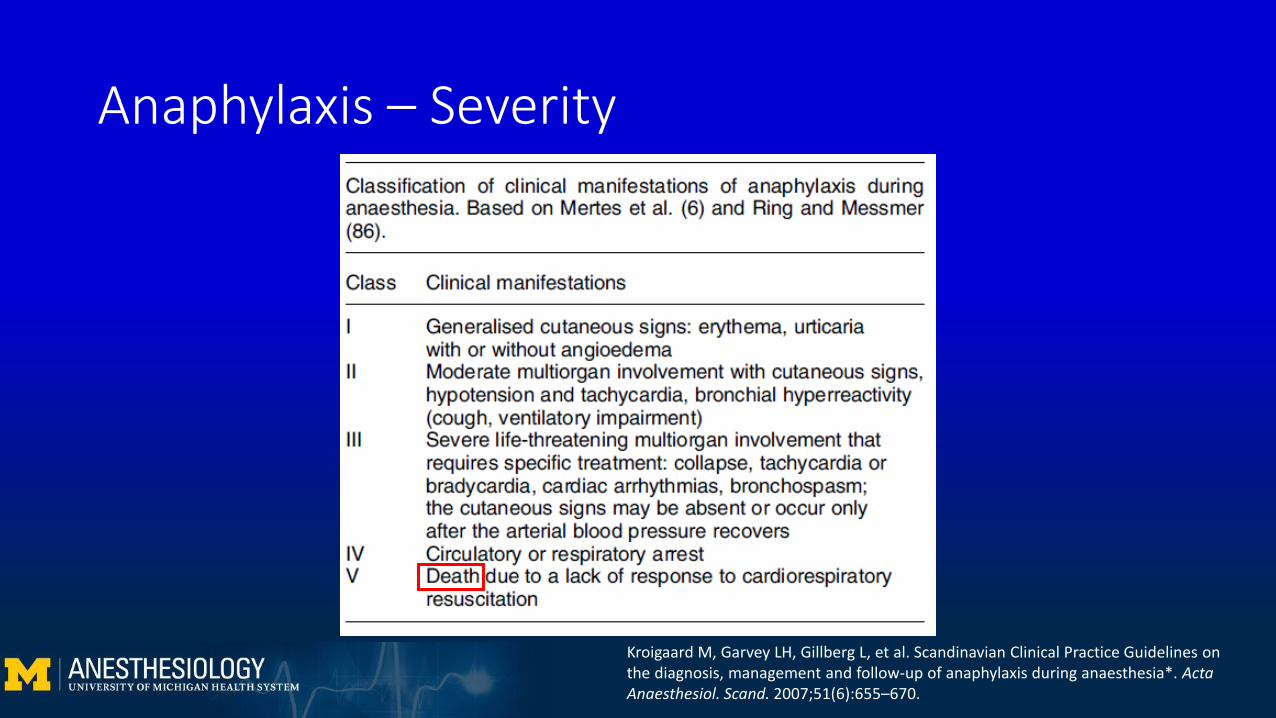
Anaphylaxis – Severity
Kroigaard M, Garvey LH, Gillberg L, et al. Scandinavian Clinical Practice Guidelines on the diagnosis, management and follow-up of anaphylaxis during anaesthesia*. ActaAnaesthesiol. Scand. 2007;51(6):655–670.

Anaphylaxis – Severity
Kroigaard M, Garvey LH, Gillberg L, et al. Scandinavian Clinical Practice Guidelines on the diagnosis, management and follow-up of anaphylaxis during anaesthesia*. ActaAnaesthesiol. Scand. 2007;51(6):655–670.
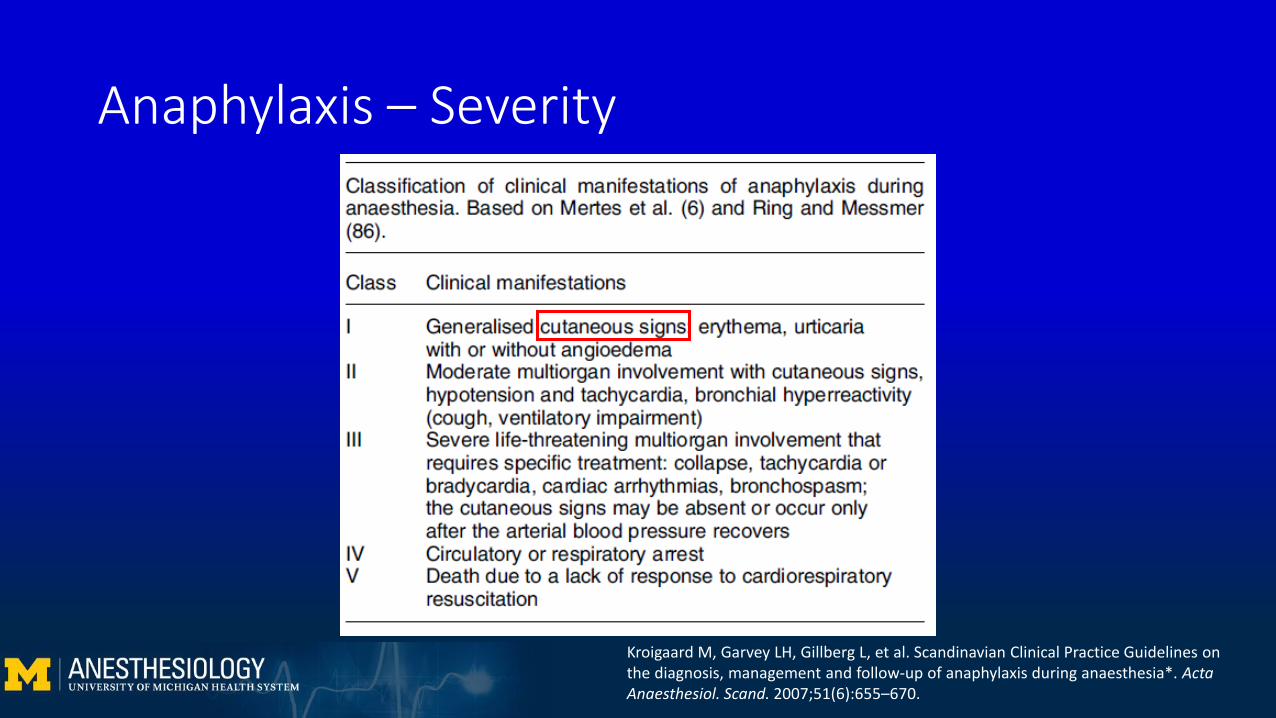
Anaphylaxis – Severity
Kroigaard M, Garvey LH, Gillberg L, et al. Scandinavian Clinical Practice Guidelines on the diagnosis, management and follow-up of anaphylaxis during anaesthesia*. ActaAnaesthesiol. Scand. 2007;51(6):655–670.

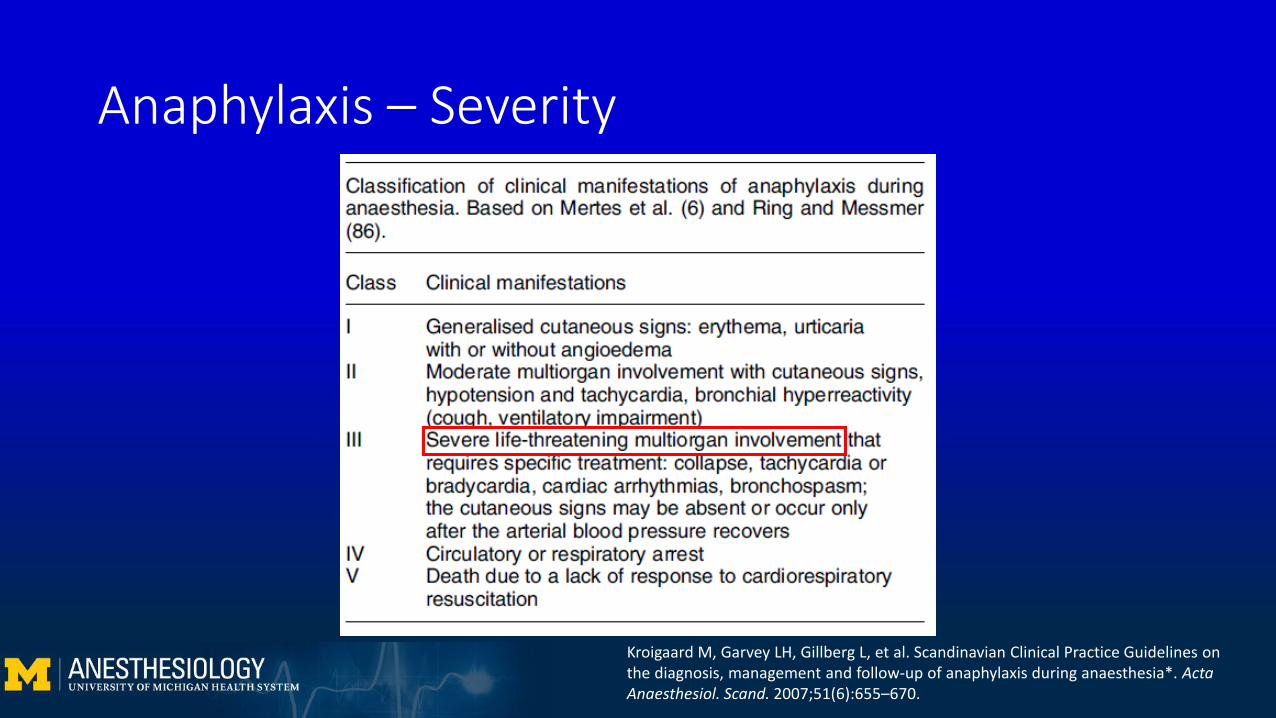
Anaphylaxis – Severity
Kroigaard M, Garvey LH, Gillberg L, et al. Scandinavian Clinical Practice Guidelines on the diagnosis, management and follow-up of anaphylaxis during anaesthesia*. ActaAnaesthesiol. Scand. 2007;51(6):655–670.
Anaphylaxis – Severity
Kroigaard M, Garvey LH, Gillberg L, et al. Scandinavian Clinical Practice Guidelines on the diagnosis, management and follow-up of anaphylaxis during anaesthesia*. ActaAnaesthesiol. Scand. 2007;51(6):655–670.
Anaphylaxis – Predictors of Severity
1. Rapid onset• Often IV and mucous membrane exposure
2. Delayed cutaneous signs • Subcutaneous tissue vasoconstriction in response to systemic hypotension• May only appear after normalization of BP
3. Bradycardia due to Bezold-Jarisch reflex• Cardioinhibitory reflex from the LV• Extreme hypovolemia bradycardia to allow LV to fill• Importance of recognition; avoiding atropine
Dewachter P, Mouton-Faivre C, Emala CW. Anaphylaxis and anesthesia controversies and new insights. Anesthesiol. J. Am. Soc. Anesthesiol. 2009;111(5):1141–1150.

Anaphylaxis – Treatment• Stop administering drug• CALL FOR HELP• A-B-C’s, ACLS if indicated• *EPINEPHRINE*• Oxygen, secure airway• Fluid resuscitation• Vasopressors• H1 and H2 blockers• Corticosteroids• Patient positioning• Observation
Sampson HA, Muñoz-Furlong A, Campbell RL, et al. Second symposium on the definition and management of anaphylaxis: Summary report—Second National Institute of Allergy and Infectious Disease/Food Allergy and Anaphylaxis Network symposium. J. Allergy Clin. Immunol.2006;117(2):391–397.
Anaphylaxis – Definitive Diagnosis
1. Clinical signs and symptoms2. Elevated tryptase +/- histamine
• Tryptase more sensitive and specific for anaphylaxis• Note: it is a send-out lab
• Drawn at time of the event and within 1-3hrs of symptom onset; follow until normal (~24hrs later)
3. Skin testing• Wait for 4-6 weeks to avoid false negative due to mast cell depletion• Prick vs intradermal testing
Dewachter P, Mouton-Faivre C, Emala CW. Anaphylaxis and anesthesia controversies and new insights. Anesthesiol. J. Am. Soc. Anesthesiol.2009;111(5):1141–1150.Leader AP, Dunst R, Andreae MH. Chapter 201. Anaphylaxis. In: Atchabahian A, Gupta R. eds. The Anesthesia Guide New York, NY: McGraw-Hill; 2013. http://accessanesthesiology.mhmedical.com.proxy.lib.umich.edu/content.aspx?bookid=572§ionid=42543794. Accessed September 19, 2018.

OutlineI. Case IntroductionII. Anaphylaxis
I. DefinitionII. PathophysiologyIII. DiagnosisIV. Causal AgentsV. OR considerationsVI. SeverityVII. Treatment
III. SugammadexI. Brief historyII. Anaphylactic incidenceIII. Cross reactivity
IV. Case FinaleV. Questions
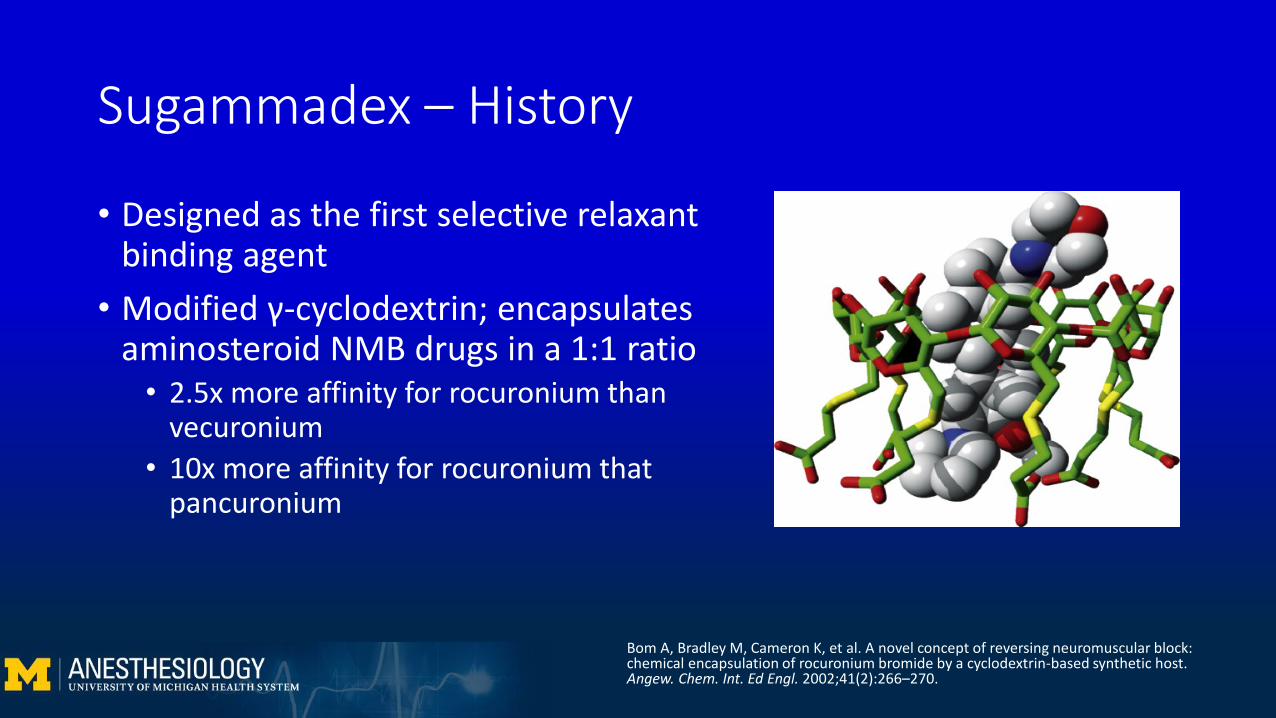
Sugammadex – History
• Designed as the first selective relaxant binding agent
• Modified γ-cyclodextrin; encapsulates aminosteroid NMB drugs in a 1:1 ratio
• 2.5x more affinity for rocuronium than vecuronium
• 10x more affinity for rocuronium that pancuronium
Bom A, Bradley M, Cameron K, et al. A novel concept of reversing neuromuscular block: chemical encapsulation of rocuronium bromide by a cyclodextrin-based synthetic host. Angew. Chem. Int. Ed Engl. 2002;41(2):266–270.
Sugammadex – Timeline
• 1990s: Dr. Bom identifies cyclodextrins as potential molecules for selective rocuronium binding
• 1999: First batch of Org 25969 (sugammadex) produced• 2001: Sugammadex structure and reversal function patented• 2005: First human studies performed• 2008: EU approves sugammadex; FDA concerned about bleeding, QT,
and anaphylactic risk• 2010: Japan approves sugammadex• 2015: December 15th, FDA approves sugammadex
Murphy, G. The Development and Regulatory History of Sugammadex in the United States. APSF Newsletter. 2016; 30(3):53-54. Takazawa T, Miyasaka K, Sawa T, Ilda H. The current status of sugammadex usage and the occurrence of sugammadex-induced anaphylaxis in Japan. APSF Newsletter. 2018;33(1):1–12.
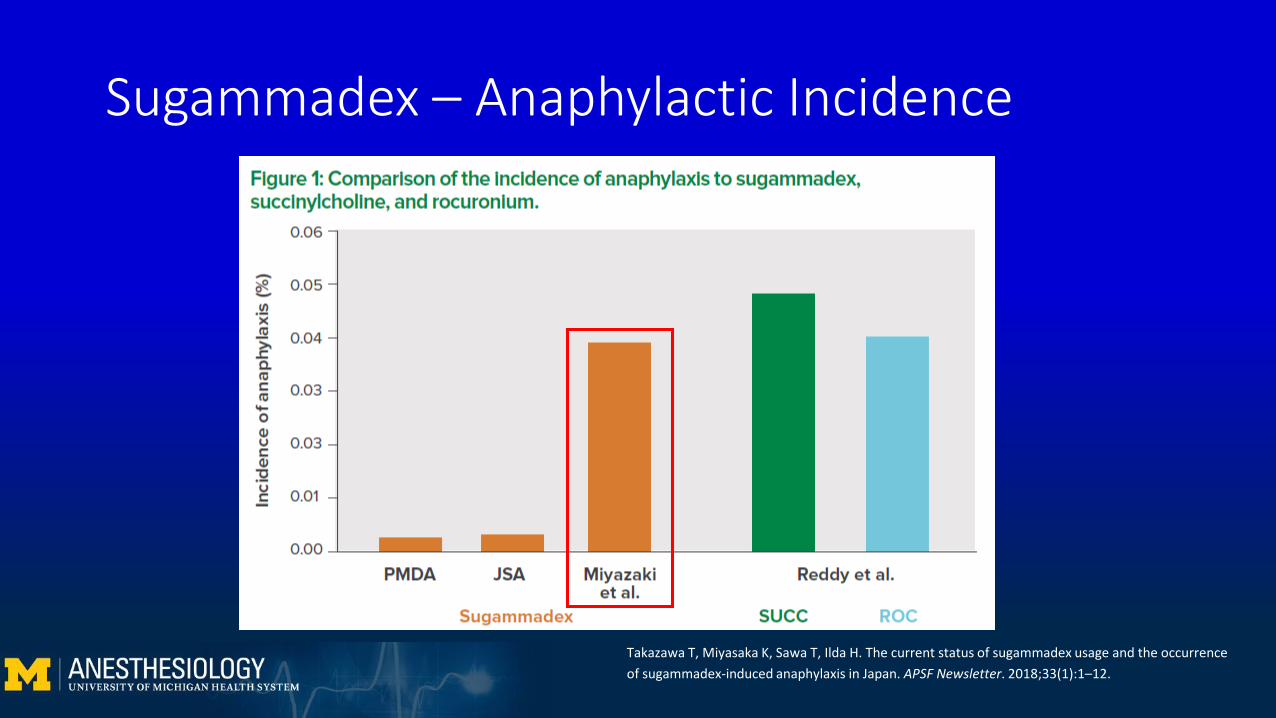
Takazawa T, Miyasaka K, Sawa T, Ilda H. The current status of sugammadex usage and the occurrence of sugammadex-induced anaphylaxis in Japan. APSF Newsletter. 2018;33(1):1–12.
Sugammadex – Anaphylactic Incidence

Sugammadex – Anaphylatic Considerations
• Dose-dependent response• Higher doses produce more significant reactions
• Occurs within 5 minutes of administration• Given typically at the end of the case to facilitate emergence
• May need to re-establish anesthesia to avoid awareness
• Sugammadex anaphylaxis often happens without prior exposure• Thought to be due to cross-reactivity
Munro IC, Newberne PM, Young VR, Bär A. Safety assessment of γ-cyclodextrin. Regul. Toxicol. Pharmacol.2004;39:3–13.O’Donnell R, Hammond J, Soltanifar S. A confirmed case of sugammadex-induced anaphylaxis in a UK hospital. BMJ Case Rep. 2017;2017:bcr-2017-220197.
Sugammadex – Cross-reactivity• We consume 4.1g/person/day of cyclodextrins• Cyclodextrins are everywhere
Marcolino VA, Zanin GM, Durrant LR, Benassi MDT, Matioli G. Interaction of Curcumin and Bixin with β-Cyclodextrin: Complexation Methods, Stability, and Applications in Food. J. Agric. Food Chem. 2011;59(7):3348–3357. Li Z, Wang M, Wang F, et al. γ-Cyclodextrin: a review on enzymatic production and applications. Appl. Microbiol. Biotechnol. 2007;77(2):245. Munro IC, Newberne PM, Young VR, Bär A. Safety assessment of γ-cyclodextrin. Regul. Toxicol. Pharmacol. 2004;39:3–13.

Brunning A. Periodic graphics: The chemistry of air fresheners. Chem & Engin News. 2018;96(8):27. Li Z, Wang M, Wang F, et al. γ-Cyclodextrin: a review on enzymatic production and applications. Appl. Microbiol. Biotechnol. 2007;77(2):245.

Sugammadex – More Anaphylaxis to Come?
• Reactions are dose-dependent• Patient may develop IgE antibodies without significant reactions• Big molecule, not readily absorbed via mucus membranes and skin
• West are heavy users of processed foods• More likely to have IgE antibodies• Counter-argument: frequent mast-cell degranulation from foods in small
doses acts to desensitize patients to Sugammadex
Takazawa T, Miyasaka K, Sawa T, Ilda H. The current status of sugammadex usage and the occurrence of sugammadex-induced anaphylaxis in Japan. APSF Newsletter. 2018;33(1):1–12. FDA Adverse Event Reporting System (FAERS) Public Dashboard. Sugammadex sodium. https://www.fda.gov/Drugs/GuidanceComplianceRegulatoryInformation/Surveillance/AdverseDrugEffects/default.htm. Updated June 4, 2018. Accessed August 8, 2018.

Case Finale
• 1140: • Staff STAT called• 100% oxygen, manual bagging• Chest compressions initiated• 1mg epinephrine administered• Urticarial rash noted on upper chest
• 1142: • ROSC, BP 166/78 mmHg, peak pressures <20 cmH2O
• 1145:• Labs drawn, tryptase elevated to 43ng/ml (normal <11.5ng/ml)
Aftermath
• Grade IV anaphylaxis high on our differential• Diphenhydramine 50mg, famotidine 20mg, and hydrocortisone
100mg given IV; albuterol administered via ETT• ABG: 7.26/57/210/25.6, Lactate 2.0 4.0• CXR showed RUL opacity consistent with collapse, no pneumothorax
or rib fractures• Intra-op TEE: normal biventricular function, no obvious valvular
disease, no pericardial effusion

Aftermath
• Taken to SICU intubated for observation; extubated 2 hours later• Tryptase at 1hr still elevated to 21ng/ml; 10hr later 7.2ng/ml• Never required epinephrine gtt
• Unremarkable post-op course, discharged POD #5• Lost to follow-up, did not complete confirmatory skin testing
Conclusion
• Anaphylaxis is a serious, life-threatening allergic reaction• Rapid recognition of characteristic signs (rash, bronchospasm,
hemodynamic collapse) is important for appropriate management• OR and GA can mask some of the characteristic signs and symptoms• The mainstay of therapy: A-B-Cs (ACLS if indicated), epinephrine, fluids• Many cognitive aids are available

Conclusion
• For definitive diagnosis, obtain tryptase levels at 0, 1, and 24hrs; schedule skin testing 4-6 weeks later
• Sugammadex anaphylaxis can happen without prior exposure• Reactions typically occur within 5 minutes of administration• Reactions are dose-dependent• Consider observing for a few minutes to avoid hemodynamic collapse

Special thanks
Dr. Sathish KumarDr. Norah Naughton
References1. Casaccia M, Andorno E, Di Domenico s, et al. Laparoscopic liver resection for hepatocellular carcinoma in cirrhotic patients.
Feasibility of nonanatomic resection in difficult tumor locations. Journal of Minimal Access Surgery. 2011;7(4): 222-226.2. Sampson HA, Muñoz-Furlong A, Campbell RL, et al. Second symposium on the definition and management of anaphylaxis:
Summary report—Second National Institute of Allergy and Infectious Disease/Food Allergy and Anaphylaxis Network symposium. J. Allergy Clin. Immunol. 2006;117(2):391–397.
3. Dewachter P, Mouton-Faivre C, Emala CW. Anaphylaxis and Anesthesia Controversies and New Insights. Anesthesiol. J. Am. Soc. Anesthesiol. 2009;111(5):1141–1150.
4. Pattanaik D, Yataco JC, Lieberman P. Anaphylactic and Anaphylactoid Reactions. Principles of Critical Care. 2015;4: 1615-1626.5. Leader AP, Dunst R, Andreae MH. Chapter 201. Anaphylaxis. In: Atchabahian A, Gupta R. eds. The Anesthesia Guide New York, NY:
McGraw-Hill; 2013. http://accessanesthesiology.mhmedical.com.proxy.lib.umich.edu/content.aspx?bookid=572§ionid=42543794. Accessed September 19, 2018.
6. Ali MR. Anaphylaxis. Slideshare.net. 2015; accessed 9/18/187. Mertes PM, Laxenaire M-C, Alla F. Anaphylactic and Anaphylactoid Reactions Occurring during Anesthesia in France in 1999–2000.
Anesthesiol. J. Am. Soc. Anesthesiol. 2003;99(3):536–545.8. Lagopoulos V, Gigi E. Anaphylactic and anaphylactoid reactions during the perioperative period. Hippokratia. 2011;15(2):138–140. 9. Leo ED, Donne PD, Calogiuri GF, Macchia L, Nettis E. Focus on the agents most frequently responsible for perioperative
anaphylaxis. Clin. Mol. Allergy. 2018;16(1):16.10.Kroigaard M, Garvey LH, Gillberg L, et al. Scandinavian Clinical Practice Guidelines on the diagnosis, management and follow-up of
anaphylaxis during anaesthesia*. Acta Anaesthesiol. Scand. 2007;51(6):655–670. 11.De Feo G, Parente R, Triggiani M. Pitfalls in anaphylaxis. Curr. Opin. Allergy Clin. Immunol. 2018;18(5):382.12.Anaphylactic Reaction (Systemic Hypersensitivity Reaction). Michigan Medicine Clinical Practice Guidelines.
www.med.umich.edu/i/michart/2018CPGS.html. 2018. Accessed 9/22/18.
References13. Meek T, May A, Ferguson K, et al. Anaphylaxis. Association of Anesthetists of Great Britain and Ireland. www.aagbi.org/safety/qrh. May 2018.
Accessed 9/22/18.14. Howard SK, Chu LF, Goldhaber-Fiebert SN, et al. Emergency Manual: Cogitive aids for perioperative critical events.
http://emergencymanual.Stanford.edu. 2016;3. Accessed 9/22/18.15. Tremper KK, Mace JJ, Gombert JM, et al. Design of a Novel Multifunction Decision Support Display for Anesthesia Care: AlertWatch® OR. BMC
Anesthesiol. 2018;18(1):1616. Bom A, Bradley M, Cameron K, et al. A novel concept of reversing neuromuscular block: chemical encapsulation of rocuronium bromide by a
cyclodextrin-based synthetic host. Angew. Chem. Int. Ed Engl. 2002;41(2):266–270. 17. Murphy, G. The Development and Regulatory History of Sugammadex in the United States. APSF Newsletter. 2016; 30(3):53-54. 18. Takazawa T, Miyasaka K, Sawa T, Ilda H. The current status of sugammadex usage and the occurrence of sugammadex-induced anaphylaxis in Japan.
APSF Newsletter. 2018;33(1):1–12. 19. K.C. Min, P. Bondiskey, Schulz V, Woo T, Assaid C, Yu W, et al. Evaluation of hypersensitivity incidence following sugammadex administration in healthy
subjects: a randomized controlled trial. Br J Anaesth. 2008. 20. Miyazaki Y, Sunaga H, Kida K, et al. Incidence of anaphylaxis associated with sugammadex. Anesth. Analg. 2018;126(5):1505–1508.21. Munro IC, Newberne PM, Young VR, Bär A. Safety assessment of γ-cyclodextrin. Regul. Toxicol. Pharmacol. 2004;39:3–13. 22. O’Donnell R, Hammond J, Soltanifar S. A confirmed case of sugammadex-induced anaphylaxis in a UK hospital. BMJ Case Rep. 2017;2017:bcr-2017-
220197.23. Marcolino VA, Zanin GM, Durrant LR, Benassi MDT, Matioli G. Interaction of Curcumin and Bixin with β-Cyclodextrin: Complexation Methods, Stability,
and Applications in Food. J. Agric. Food Chem. 2011;59(7):3348–3357. 24. Li Z, Wang M, Wang F, et al. γ-Cyclodextrin: a review on enzymatic production and applications. Appl. Microbiol. Biotechnol. 2007;77(2):245. 25. Brunning A. Periodic graphics: The chemistry of air fresheners. Chem & Engin News. 2018;96(8):27.
26. FDA Adverse Event Reporting System (FAERS) Public Dashboard. Sugammadex sodium. https://www.fda.gov/Drugs/GuidanceComplianceRegulatoryInformation/Surveillance/AdverseDrugEffects/default.htm. Updated June 4, 2018. Accessed August 8, 2018.

Questions?
https://www.google.com/url?sa=i&rct=j&q=&esrc=s&source=images&cd=&cad=rja&uact=8&ved=2ahUKEwjIsu3iw9bdAhUj2oMKHXrGDL8QjRx6BAgBEAU&url=https%3A%2F%2Fwww.pinterest.com%2Fpin%2F326722147950669631%2F&psig=AOvVaw3N041Pbq243Hp2Eif4Vlzi&ust=1537977761722048