The neuropathology of the vegetative state after an acute brain insult
12
Brain (2000), 123, 1327–1338 The neuropathology of the vegetative state after an acute brain insult J. Hume Adams, 1 D. I. Graham 1 and Bryan Jennett 2 University Departments of 1 Neuropathology and Correspondence to: J. Hume Adams, University 2 Neurosurgery, Institute of Neurological Sciences, South Department of Neuropathology, Institute of Neurological Glasgow University Hospitals NHS Trust, Glasgow, UK Sciences, Southern General Hospital, South Glasgow University Hospitals NHS Trust, 1345 Govan Road, Glasgow G51 4TF, UK Summary The vegetative state is often described clinically as loss of function of the cortex while the function of the brainstem is preserved. In an attempt to define the structural basis of the vegetative state we have undertaken a detailed neuropathological study of the brains of 49 patients who remained vegetative until death, 1 month to 8 years after an acute brain insult. Of these, 35 had sustained a blunt head injury and 14 some type of acute non-traumatic brain damage. In the traumatic cases the commonest structural abnormalities identified were grades 2 and 3 diffuse axonal injury (25 cases, 71%). The thalamus was abnormal in 28 cases (80%), and in 96% of the cases who survived for more than 3 months. Other abnormalities included ischaemic damage in the neocortex (13 cases, Keywords: vegetative state; head injury; cerebral hypoxia Abbreviations: DAI diffuse axonal injury; TCI total contusion index Introduction In the quarter of a century since Jennett and Plum described and named the persistent vegetative state (Jennett and Plum, 1972), there has been continued and increasing interest in the medical, ethical and legal aspects of the condition (McLean, 1999). Its essential clinical features are loss of any meaningful cognitive responsiveness, presumed lack of awareness and therefore of consciousness, while there is spontaneous breathing and a range of reflex responses as well as periods of wakefulness (eyes open). It is often described as loss of function in the cerebral cortex while the function of the brainstem is preserved (Jennett, 1997). Although the vegetative state may characterize the end-stage of progressive dementing conditions in children and in adults, most interest has focused on the vegetative state resulting from an acute brain insult. Some such patients may recover to a degree after having been diagnosed as being vegetative. In the Multi-Society Task Force review of the world literature (Multi-Society Task Force, 1994), half of the patients who © Oxford University Press 2000 37%) and intracranial haematoma (nine cases, 26%). In the non-traumatic cases there was diffuse ischaemic damage in the neocortex in nine cases (64%) and focal damage in four (29%); the thalamus was abnormal in every case. There were cases in both groups where the cerebral cortex, the cerebellum and the brainstem were of structurally normal appearance. In every case, however, there was profound damage to the subcortical white matter or to the major relay nuclei of the thalamus, or both. These lesions render any structurally intact cortex unable to function because connections between different cortical areas via the thalamic nuclei are no longer functional, and there is also extensive damage to afferent and efferent cerebral connections. were vegetative at 1 month after a head injury had regained consciousness after a year, as had one-third of those who were vegetative for 3 months. The potential for recovery was much less after non-traumatic insults. The Task Force, and more recently the Royal College of Physicians of London (Royal College of Physicians Working Party, 1996) have therefore recommended that the vegetative state should not be declared permanent until a year after a head injury, but after 3 months following non-traumatic insults according to the Task Force and after 6 months according to the London report. Neuropathologists have also been intrigued by the vegetative state if only because, particularly in patients who survive for only a few months, the brain may appear normal or virtually so to the naked eye. Indeed, the underlying structural changes responsible for the vegetative state may be rather subtle to elucidate even with microscopy. In the present paper we describe the neuropathological
Transcript of The neuropathology of the vegetative state after an acute brain insult

Brain (2000), 123, 1327–1338
The neuropathology of the vegetative state after anacute brain insultJ. Hume Adams,1 D. I. Graham1 and Bryan Jennett2
University Departments of 1Neuropathology and Correspondence to: J. Hume Adams, University2Neurosurgery, Institute of Neurological Sciences, South Department of Neuropathology, Institute of NeurologicalGlasgow University Hospitals NHS Trust, Glasgow, UK Sciences, Southern General Hospital, South Glasgow
University Hospitals NHS Trust, 1345 Govan Road,Glasgow G51 4TF, UK
SummaryThe vegetative state is often described clinically as loss offunction of the cortex while the function of the brainstem ispreserved. In an attempt to define the structural basisof the vegetative state we have undertaken a detailedneuropathological study of the brains of 49 patients whoremained vegetative until death, 1 month to 8 years afteran acute brain insult. Of these, 35 had sustained a blunthead injury and 14 some type of acute non-traumaticbrain damage. In the traumatic cases the commoneststructural abnormalities identified were grades 2 and 3diffuse axonal injury (25 cases, 71%). The thalamus wasabnormal in 28 cases (80%), and in 96% of the cases whosurvived for more than 3 months. Other abnormalitiesincluded ischaemic damage in the neocortex (13 cases,
Keywords: vegetative state; head injury; cerebral hypoxia
Abbreviations: DAI � diffuse axonal injury; TCI � total contusion index
IntroductionIn the quarter of a century since Jennett and Plum describedand named the persistent vegetative state (Jennett and Plum,1972), there has been continued and increasing interest inthe medical, ethical and legal aspects of the condition(McLean, 1999). Its essential clinical features are loss ofany meaningful cognitive responsiveness, presumed lack ofawareness and therefore of consciousness, while there isspontaneous breathing and a range of reflex responses aswell as periods of wakefulness (eyes open). It is oftendescribed as loss of function in the cerebral cortex whilethe function of the brainstem is preserved (Jennett, 1997).Although the vegetative state may characterize the end-stageof progressive dementing conditions in children and in adults,most interest has focused on the vegetative state resultingfrom an acute brain insult. Some such patients may recoverto a degree after having been diagnosed as being vegetative.In the Multi-Society Task Force review of the world literature(Multi-Society Task Force, 1994), half of the patients who
© Oxford University Press 2000
37%) and intracranial haematoma (nine cases, 26%).In the non-traumatic cases there was diffuse ischaemicdamage in the neocortex in nine cases (64%) and focaldamage in four (29%); the thalamus was abnormal inevery case. There were cases in both groups where thecerebral cortex, the cerebellum and the brainstem wereof structurally normal appearance. In every case, however,there was profound damage to the subcortical whitematter or to the major relay nuclei of the thalamus, orboth. These lesions render any structurally intact cortexunable to function because connections between differentcortical areas via the thalamic nuclei are no longerfunctional, and there is also extensive damage to afferentand efferent cerebral connections.
were vegetative at 1 month after a head injury had regainedconsciousness after a year, as had one-third of those whowere vegetative for 3 months. The potential for recovery wasmuch less after non-traumatic insults. The Task Force, andmore recently the Royal College of Physicians of London(Royal College of Physicians Working Party, 1996) havetherefore recommended that the vegetative state should notbe declared permanent until a year after a head injury, butafter 3 months following non-traumatic insults accordingto the Task Force and after 6 months according to theLondon report.
Neuropathologists have also been intrigued by thevegetative state if only because, particularly in patients whosurvive for only a few months, the brain may appear normalor virtually so to the naked eye. Indeed, the underlyingstructural changes responsible for the vegetative state maybe rather subtle to elucidate even with microscopy.
In the present paper we describe the neuropathological

1328 J. H. Adams et al.
findings in 49 patients who had remained in the vegetativestate for more than 1 month after acute brain damage; in 35cases the cause had been a blunt head injury and in theremaining 14 some type of hypoxic event.
Material and methodsThe cases will be presented in two groups—those where thevegetative state was brought about by a head injury andthose where there was another cause. Most of the caseshave been taken from the records of the Department ofNeuropathology of this Institute while six were kindly referredto us by Dr J. B. Brierley, lately of the MRC Laboratoriesnear Carshalton. All had survived for at least 1 month afterthe acute event, as had all of the cases in the Multi-SocietyTask Force report (Multi-Society Task Force, 1994).
The clinical records available were reviewed by one of us(B.J.) in order to confirm that the patients had been vegetativeat the time of death. Some of these records were from severalyears ago before recent diagnostic criteria were established.In certain cases some judgement was involved in decidingthat the patient had been vegetative, but when there wasdoubt the case was rejected.
Group 1 (traumatic cases)This consisted of 35 patients who had sustained a blunt headinjury (Adams et al., 1999). There were 32 males and threefemales with an age range of 7–75 years (average 38 years).The cause of injury in 17 patients was a road traffic accident,in nine an assault, in six a fall and in three the precisecircumstance of the head injury was not known. Eleven casessurvived for less than 3 months, 11 for between 3 monthsand a year and 13 for more than a year. Particular attentionwas paid to whether or not the patient had talked after hisinjury (Reilly et al., 1975); if the patient had talked but hadnot been completely rational, the lucid interval was definedas being partial.
Group 2 (non-traumatic cases)Of the 14 patients in this group, 11 were male and threewere female. The age range was from 2 to 58 years (average32 years). Survival was less than 3 months in six patients,between 3 months and a year in six and greater than a yearin two. Five of the patients had experienced an intra-operativeor postoperative cardiac arrest, three an acute episode ofhypotension and two acute circulatory failure induced bydrugs. There was one case of asphyxia, one of smokeinhalation, one of severe bronchospasm and one of severeintracranial infection.
NeuropathologyAll brains were fixed in 10% formal saline for a minimumof 3 weeks prior to dissection, after which a full macroscopic
and microscopic examination was undertaken in each case(Adams et al., 1980). After transecting the rostral brainstem,the cerebral hemispheres were cut into coronal sections 1 cmthick. The cerebellar hemispheres were cut at right angles tothe folia and multiple horizontal sections were taken of thebrainstem. In all but four cases, large bilateral blocks of thefrontal, parietal, occipital and temporal lobes (three levelsincorporating the basal ganglia and the hippocampalstructures), each cerebellar hemisphere and the brainstem(three levels) were embedded in celloidin and sections stainedwith cresyl violet and by Heidenhain’s method for myelin.The remaining pieces of corpus callosum and brainstem wereembedded in paraffin wax. In the four cases where celloidinstudies were not undertaken, representative blocks were takenfrom all lobes of the cerebral hemispheres, the corpuscallosum, the basal ganglia and the hippocampal structures(at least at two levels), the cerebellum (both hemispheres)and the brainstem (at least at three levels). Paraffin sectionswere routinely stained with haematoxylin and eosin and bythe Luxol fast blue/cresyl violet technique. When consideredappropriate, sections were stained by the Palmgren techniquefor axons and other stains including immunohistochemistryfor astrocytes (GFAP, 1 : 3000; Dako, Ely, Cambs., UK) andmacrophages (CD68, 1 : 200; Dako), which were developedwith PAP or Vectastain ABC kit, respectively, and visualizedwith diaminobenzidine.
The severity of ischaemic brain damage was graded inboth groups. In the traumatic cases it occurred mainly in theneocortex and was classified as severe when the lesions werediffuse or multifocal, or took the form of infarcts withinspecific arterial territories, and moderate when ischaemicdamage was limited to arterial boundary zones, singly or incombination with subtotal infarction in the distribution ofarterial territories (Graham et al., 1989). In the non-traumaticcases the ischaemic damage was always severe; it was gradedeither as diffuse when there was widespread neuronal lossthroughout the affected structure, or focal when there werelines of demarcation between normal and abnormal tissue as,for example, with ischaemic damage in arterial boundaryzones. The criterion of pressure necrosis in one or bothparahippocampal gyri was used as evidence that theintracranial pressure had been high during life as a result ofa supratentorial expanding lesion (Adams and Graham, 1976).
In the traumatic cases surface contusions were assessedsemi-quantitatively using the total contusion index (TCI).This takes into account the depth and extent of the contusionsin various parts of the brain: 0 means that there were nocontusions, a contusion index of less than 9 is indicative ofminimal contusions, while one of more than 37 is indicativeof severe contusions (Adams et al., 1985b). Diffuse axonalinjury (DAI) was graded and in this series most exampleswere of the more severe grades 2 and 3. In grade 3 there arefocal lesions in the corpus callosum and in the dorsolateralsegment(s) of the rostral brainstem and in grade 2 there is afocal lesion only in the corpus callosum. In grade 1, there isagain axonal damage diffusely throughout the white matter,

Vegetative state 1329
but there are no focal lesions in the corpus callosum or inthe brainstem (Adams et al., 1985a, 1989).
Only traumatic haematomas thought to be sufficiently largeto act as significant intracranial expanding lesions (more than35 ml) were recorded. The great majority of the haematomasso recorded had been evacuated surgically before death.
ResultsGroup 1 (traumatic cases)The principal features are given in Table 1. Three of thepatients had experienced a lucid interval—two total and onepartial. All of the patients with lucid intervals had developedintracranial haematomas, one of whom had also sustained apostoperative cardiac arrest.
The commonest structural abnormalities identified in thebrains were grades 2 and 3 DAI (25 cases, 71%). Unlike theacute haemorrhagic lesions (Fig. 1) that are the characteristicfocal features of DAI in patients who survive for only ashort time after their injury, the lesions were shrunken,granular and sometimes cystic (Fig. 2). They often retainedan orange-yellow colour because of the persistence ofhaemosiderin. They were not all visible macroscopically—in 15 of the 25 cases, one or both of the focal lesions wereidentifiable only microscopically (Table 1). With increasingsurvival the bulk of the white matter became reduced andthere was enlargement of the ventricular system (Fig. 2A).Of the 10 patients without grades 2 or 3 DAI, seven haddeveloped intracranial haematomas and nine had sustainedmoderate or severe ischaemic brain damage. There were alsothree cases of grade 1 DAI: in two of these there was, inaddition, ischaemic damage in the cerebral cortex, and inone of these diffuse ischaemic damage in the thalamus also.In the third there was focal ischaemic damage in the thalamus.
Moderate or severe ischaemic brain damage was presentin 15 (43%) of the traumatic cases. In six it was centred onarterial boundary zones in the cerebral hemispheres (Fig. 3),in four the ischaemic brain damage was diffuse, in two itaffected specific arterial territories (Fig. 2A) and in one itwas multifocal. In two there was diffuse neuronal loss in thethalamus without there being any neocortical damage. Theintracranial pressure had been high in all but two of thepatients who sustained ischaemic brain damage. In six of the15 cases with ischaemic damage there was major extracranialinjuries that might have contributed to an inadequate cerebralblood flow.
Intracranial haematomas had developed in nine (26%) ofthe cases—six subdural haematomas, one extraduralhaematoma and two cases with bilateral intracerebralhaematomas. In all but one patient the intracranial pressurehad been high and all the subdural and extradural haematomashad been evacuated during life.
The intracranial pressure had been high in 25 (71%)of the patients. Only eight of these had an intracranialhaematoma.
In five cases (14%) there were abnormalities in thebrainstem other than the focal lesions that are a feature ofDAI. The intracranial pressure had been high in all of them.The lesions were in the midline in four cases and lateral (ina cerebral peduncle) in one. In all of these cases the lesionswere small and non-haemorrhagic.
The TCI ranged from 0 to 21 (median 3.9), i.e. in not onecase could contusions be classified as severe and in eightthey were absent. If surface contusions are excluded, theneocortex was abnormal in only 13 of the cases and thistook the form of ischaemic damage; this was diffuse in onlyfour cases. There were no identifiable abnormalities in thecerebral cortex resulting from DAI.
The subcortical white matter was abnormally pale andgranular in texture in 29 cases (83%), this being diffuse inall 28 patients with DAI. Focal damage to subcortical whitematter was seen in two patients who had sustained ischaemicbrain damage (Figs 2A and 3).
The thalamus was abnormal in 28 cases (80%), in 25 ofwhich the damage was diffuse. This took the form oftransneuronal change or ischaemic damage. In two of thecases with ischaemic damage there was no cortical ischaemicdamage. In the other three cases there was focal infarctionas a consequence of raised intracranial pressure and acompromised circulation through the posterior cerebralarteries or as part of the pattern of focal ischaemic braindamage. In DAI, retrograde thalamic degeneration occurs asa result of widespread axonal damage and takes some 3months to develop. On the other hand, thalamic damageassociated with ischaemia is apparent shortly after the hypoxicevent. In DAI there is atrophy due to shrinkage of nervecells and an astrocytosis in the lateral and ventral nuclei withrelative sparing of the anterior and dorsomedial nuclei, thepulvinar, the centromedian nuclei and lateral geniculatebodies. In contrast, in cases in which the thalamic damageis attributable to ischaemia, there is neuronal loss andastrocytosis in the anterior and dorsomedial nuclei withrelative sparing of the lateral and ventral nuclei. These twomain patterns correspond to those described in cases ofdiffuse degeneration of the cerebral white matter in severedementia after head injury (Strich, 1956) and in long survivalafter cardiac arrest (Brierley et al., 1971; Cole and Cowie,1987).
There was a low incidence of fracture of the skull (12cases, 34%). With the passage of time there was a trend forthe brain weight to fall and for the ventricles to enlarge.
Group 2 (non-traumatic cases)The structural abnormalities in these cases, given in Table 2,cover the spectrum of brain damage brought about by anacute hypoxic episode (Auer and Benveniste, 1997). Themost common abnormality was diffuse damage in theneocortex (nine cases, 64%). This took the form of laminarnecrosis, more severe in the depths of sulci than on theircrests, and increasing in intensity from the frontal to the

1330 J. H. Adams et al.T
able
1Tr
aum
atic
case
s.T
hepr
inci
pal
clin
ical
and
neur
opat
holo
gica
lfe
atur
esin
35pa
tien
tsw
hosu
rviv
edin
ave
geta
tive
stat
efo
r1
mon
thor
mor
eaf
ter
ahe
adin
jury
Cas
eA
geSe
xC
ause
Surv
ival
Luc
idSk
ull
Bra
inIn
trac
rani
alIC
P�T
CI
DA
IIB
DA
bnor
mal
ities
Hyd
roce
phal
usno
.(y
ears
)fr
actu
rew
eigh
tha
emat
oma
(g)
Neo
cort
exSC
WM
Tha
lam
usB
rain
stem
157
MR
TA5
wN
oY
es14
50IC
HY
es19
No
�C
No
DN
o–
236
MR
TA6
wN
oY
es15
40N
oN
o4
3M
mN
oC
DN
oN
o–
39
MR
TA7
wN
oN
o14
30N
oY
es0
3m
No
No
DN
oN
o�
418
MR
TA7
wN
oY
es14
90N
oY
es3
3M
mN
oC
DN
oN
o–
532
MR
TA7
wN
oN
o15
00N
oN
o3
3M
mN
oC
DN
oN
o�
�6
38M
Fall
8w
PN
o12
50SD
He
Yes
71
No
CD
FM
–7
59M
Ass
ault
8w
No
No
1370
No
No
43
MN
oC
DT
No
–8
47M
Ass
ault
8w
No
No
1390
No
No
63
MN
oC
DN
oN
o�
943
MFa
ll10
wN
oY
es13
50N
oY
es14
No
�C
,B
ZN
oF
No
�10
24M
RTA
10w
No
Yes
1520
SDH
eY
es16
1�
�C
,B
ZD
DN
o�
�11
29M
Fall
12w
No
No
1650
No
No
03
MN
oN
oD
No
No
–12
15F
Fall
3m
NK
No
1160
No
No
43
MN
oC
DT
No
–13
65M
RTA
3m
NK
Yes
1440
No
Yes
151
�C
,B
ZD
DM
��
�14
18M
RTA
3m
No
Yes
1160
No
Yes
193
m�
C,
FD
TN
o�
1527
MR
TA4
mN
oY
es14
30SD
He
No
62
m�
�C
DD
No
–16
31M
RTA
6m
No
No
1300
No
Yes
63
Mm
No
CD
TN
o�
�17
42M
Ass
ault
9m
No
No
1270
No
Yes
03
Mm
No
No
DT
No
��
1858
MR
TA9
mN
oN
o15
50N
oY
es0
3m
No
No
DT
No
��
1956
MR
TA9
mN
oN
o11
90N
oY
es4
3M
No
CD
TN
o�
�20
75F
Ass
ault
11m
No
No
1260
No
No
02
MN
oN
oD
TN
o�
�21
50M
Ass
ault
1y
No
No
1260
SDH
eY
es4
No
�C
,B
ZF
DM
��
2249
MA
ssau
lt1
yT
No
1070
SDH
eY
es9
No
��
C,
AT
FF
L�
�23
34F
RTA
1y
6m
No
No
1070
No
Yes
213
Mm
�C
,D
DD
No
��
2464
MA
ssau
lt1
y6
mN
oY
es11
50N
oY
es3
2M
No
CD
TN
o�
�25
27M
NK
1y
6m
No
No
1130
No
No
03
Mm
No
No
DN
oN
o�
�26
18M
Ass
ault
2y
No
No
1200
No
Yes
63
Mm
No
CD
TN
o�
�27
44M
NK
2y
2m
No
Yes
1300
No
Yes
63
Mm
No
CD
TN
o�
�28
61M
NK
2y
3m
No
No
1350
ICH
Yes
6N
o�
�C
,D
No
DN
o�
�29
52M
RTA
2y
4m
No
No
NK
No
Yes
03
Mm
�A
TD
,F
DN
o�
�30
7M
RTA
2y
5m
No
Yes
NK
No
Yes
33
MN
oC
DT
M�
�31
56M
Ass
ault
3y
No
No
1260
No
No
03
MN
oN
oD
TN
o�
�32
15M
RTA
3y
No
No
1140
No
Yes
20N
o�
�C
,D
No
DN
o�
��
338
MFa
ll4
yT
Yes
670
ED
He
Yes
4N
o�
�C
,D
No
DN
o�
��
3420
MR
TA6
yN
oN
o10
20N
oY
es3
3M
m�
C,
BZ
DD
No
��
3542
MFa
ll8
y6
mN
oN
o12
20SD
He
Yes
143
M�
C,
BZ
DD
No
��
�
Cau
se:
RTA
�ro
adtr
affic
acci
dent
.Su
rviv
al:
w�
wee
k(s)
;m
�m
onth
(s);
y�
year
(s).
Luc
id:
T�
tota
llylu
cid
imm
edia
tely
afte
rin
jury
;P
�pa
rtia
llylu
cid;
NK
�no
tkn
own.
Bra
inw
eigh
t:N
K�
not
know
n.In
trac
rani
alha
emat
oma:
SDH
�su
bdur
alha
emat
oma;
ED
H�
extr
adur
alha
emat
oma;
ICH
�in
trac
ereb
ral
haem
atom
a;e
�ev
acua
ted.
ICP�
�ra
ised
intr
acra
nial
pres
sure
.T
CI
�to
tal
cont
usio
nin
dex.
DA
I�
diff
use
axon
alin
jury
:1,
2,3
indi
cate
grad
e;m
�fo
cal
lesi
ons
seen
only
mic
rosc
opic
ally
;M
�fo
cal
lesi
ons
seen
mac
rosc
opic
ally
;M
m�
one
lesi
onse
enm
acro
scop
ical
ly,
the
othe
ron
lym
icro
scop
ical
ly.
IBD
�is
chae
mic
brai
nda
mag
ein
cere
bral
cort
ex:
��
mod
erat
e;�
��
seve
re.
Neo
cort
ex:
BZ
�is
chae
mic
brai
nda
mag
ein
arte
rial
boun
dary
zone
s;A
T�
isch
aem
icbr
ain
dam
age
inar
teri
alte
rrito
ries
;D
�di
ffus
eda
mag
e;F
�fo
cal
dam
age;
C�
cont
usio
ns(f
orse
veri
tyse
eT
CI)
.SC
WM
�su
bcor
tical
whi
tem
atte
r:D
�di
ffus
eda
mag
e;F
�fo
cal
dam
age
inre
latio
nto
isch
aem
icda
mag
e.T
hala
mus
:F
�fo
cal
dam
age;
T�
tran
sneu
rona
lda
mag
e;D
�di
ffus
eis
chae
mic
dam
age.
Bra
inst
em:
M�
foca
lda
mag
ein
mid
line;
L�
late
ral
dam
age.
Hyd
roce
phal
us:
��
slig
hten
larg
emen
tof
the
vent
ricu
lar
syst
em;
��
�m
oder
ate;
��
��
seve
re.

Vegetative state 1331
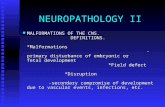
Fig. 1 Acute DAI. There are focal haemorrhagic lesions in (A)the corpus callosum and in (B) the dorsolateral part of the rostralbrainstem. Reproduced, with permission, from Adams et al. (1977).
occipital poles often with selective sparing of the calcarinecortex. With the passage of time the affected cortex becamerather granular and shrunken, there was a reduction in thebulk of the white matter and there was ventricular enlargement(Fig. 4). In three cases the ischaemic damage was restrictedto arterial boundary zones of the type known to be associatedwith an acute episode of hypotension (Adams et al., 1966).In the one case with ischaemic damage in more than onearterial territory, there had been an intracranial expandinglesion in the form of an abscess in the left frontal lobebrought about by a localized penetrating head injury that hadinitially not caused a disturbance of consciousness. As canbe seen from Table 2, there were variable abnormalities inthe caudate nucleus, the putamen, the globus pallidus andthe cerebellum, but in every case there was profound diffuseneuronal loss in each thalamus and hippocampus. In eightcases there were variable minor abnormalities in thebrainstem, the most common being focal changes in thesubstantia nigra or in some of the major motor nuclei. Innone of the cases was there histological evidence to suggestthat the intracranial pressure had been high (Adams andGraham, 1976).
Fig. 2 DAI. (A) Table 1, case 29: survival 2 years 4 months aftera head injury. The corpus callosum is narrowed because of an oldfocal lesion. There is also an old shrunken infarct in the leftmiddle cerebral arterial territory. There is enlargement of theventricular system. (B) Table 1, case 19: survival 9 months after ahead injury. There is a shrunken cystic lesion in the dorsolateralpart of the rostral brainstem. B is reproduced, with permission,from Adams et al. (1977).
There was only one case in which the neocortex wasstructurally of normal appearance (case 12). This patienthad been accidentally incarcerated in a hermetically sealedmotorized vehicle and there was a possibility that there hadbeen carbon monoxide in the atmosphere. The most dramaticabnormality was extensive damage to the subcortical whitematter associated with widespread destruction of axons andloss of myelin, and reactive changes in astrocytes andmicroglia. In this patient there were also diffuse abnormalitiesin the thalamus and in the hippocampi.
As with the patients in group 1, there was a trend for thebrain weight to decrease and for the ventricles to enlarge assurvival increased.

1332 J. H. Adams et al.
Fig. 3 Table 1, case 21: survival 1 year after a head injury. Thereis an old infarct in the boundary zone between the anterior andmiddle cerebral arterial territories.
DiscussionThere have in the past been many reports of disorders ofconsciousness after acute brain insults, usually of hypoxiccausation (French, 1952; Adams et al., 1966; Brierley et al.,1971; Ingvar et al., 1978; Dougherty et al., 1981; Cole andCowie, 1987; Relkin et al., 1990). Very few publications,however, have specifically addressed the underlying basis ofthe persistent vegetative state. An exception is the review ofthe literature by Kinney and Samuels of cases of the vegetativestate of traumatic and non-traumatic causation (Kinney andSamuels, 1994). Precise clinical details and duration ofsurvival were not defined in this review and not all of thecases would be accepted as being vegetative using currentcriteria. They concluded, however, that the vegetative stateresults from widespread and bilateral damage to (i) thecerebral cortex itself; (ii) the thalamus; or (iii) many of theintra- and subcortical connections (via axonal injury and/ordemyelination of the cerebral hemispheric white matter).They present three diagrams: one with diffuse destruction ofthe cerebral cortex only, one with diffuse damage to thesubcortical white matter only and one with diffuse damageto each thalamus only. We have never seen a case in whichthere was diffuse hypoxic damage to the cerebral cortexwithout there being correspondingly severe damage in eachthalamus. Kinney and colleagues reported a single case ofthe vegetative state in a young woman who survived for 10years after cardiopulmonary arrest (Kinney et al., 1994). Inthis patient the damage to the cerebral cortex was in theparasagittal regions, i.e. in arterial boundary zones, and muchof the neocortex was spared. There was, however, severebilateral thalamic damage and they suggested that this maysometimes be more important than cortical damage in theproduction of the vegetative state. A similar case has beenreported by Jellinger (Jellinger, 1994).
The concept that axons may be damaged directly at the
time of a head injury has a long and chequered history. Strichwas the first to suggest that it could be an important factorwhen she described the neuropathological findings in a seriesof cases with ‘severe post-traumatic dementia’ in which therewas widespread Wallerian-type degeneration in subcorticalwhite matter and in descending tracts in the brainstem andspinal cord (Strich, 1956). She was of the opinion that therehad been disruption of axons at the time of injury broughtabout by shearing strains. In support of this view was thework of Holbourn (Holbourn, 1943, 1945) and of Pudenzand Shelden (Pudenz and Shelden, 1946) on shearing injuryand the fact that in patients with this type of brain damagethere are gross and permanent neurological abnormalitiesfrom the moment of injury. The observations of Strich andher opinion as to the pathogenesis of axonal damage werealso supported by Peerless and Rewcastle (Peerless andRewcastle, 1967) and by Zimmerman and colleagues(Zimmerman et al., 1978), both groups describing examplesof shearing injury, and by ourselves (Adams et al., 1977) inan account of 19 patients found post-mortem to have ‘diffusedamage to white matter of immediate impact type’. Others,however, were of the opinion that the damage to axons wassecondary to factors such as hypoxia and ischaemia, brainswelling, or damage to the brainstem secondary to a highintracranial pressure brought about by an intracranialexpanding lesion (Jellinger and Seitelberger, 1970; Jellinger,1977; Peters and Rothemund, 1977).
The final proof that axons could be damaged at the timeof a head injury came about as a result of experimentalstudies in non-human primates when it was shown that axonaldamage identical to the type already known to occur in mancould be produced by non-impact angular acceleration of thehead (Adams et al., 1982; Gennarelli et al., 1982). At thattime we introduced the term ‘diffuse axonal injury’, now theinternationally accepted term (Gennarelli et al., 1998) todescribe this type of brain damage resulting from a headinjury. On the basis of this controlled experimental model,three grades of severity of DAI were defined and wereapplied to man (Adams et al., 1989). In the most severe form(grade 3) there are, in addition to microscopical evidence ofwidespread damage to axons in all parts of the brain, focallesions in the corpus callosum and in the dorsolateral sector(s)of the rostral brainstem. In grade 2 there is a focal lesiononly in the corpus callosum, while in grade 1 there are nofocal lesions (Adams et al., 1989). There were three caseswith grade 1 DAI in the present series and in all three therewas also ischaemic brain damage; this grade of DAI may bea cause of persistent disability after a head injury (B. Jennett,personal communication), but, on its own, does not appearto be a cause of the vegetative state.
The focal lesions of DAI can often be seen macroscopically,but sometimes only on microscopic examination. In earlierstudies the identification of axonal injury was dependent onsilver staining techniques to identify axonal swellings (the‘retraction’ balls of Cajal), but more recently immuno-histochemical methodology using an antibody to the precursor

Vegetative state 1333
Tab
le2
Non
-tra
umat
icca
ses.
The
prin
cipa
lcl
inic
alan
dne
urop
atho
logi
cal
feat
ures
in14
pati
ents
who
surv
ived
ina
vege
tati
vest
ate
for
mor
eth
an4
wee
ksaf
ter
anac
ute
non-
trau
mat
icce
rebr
alin
sult
Cas
eA
geSe
xC
ause
Surv
ival
Bra
inIC
P�H
ydro
ceph
alus
Abn
orm
aliti
esno
.(y
ears
)w
eigh
t(g
)
Neo
cort
exSC
WM
Cau
date
Puta
men
Glo
bus
Tha
lam
usH
ippo
cam
pus
Cer
ebel
lum
Bra
inst
emnu
cleu
spa
llidu
s
142
MPo
st-o
p.C
A4
w13
75N
o�
DN
oD
DD
DD
Dm
22.
5M
Intr
a-op
.C
A4
w12
50N
o�
�D
No
DD
DD
DD
m3
30M
Intr
acra
nial
8w
1420
No
��
BZ
FN
oD
DD
DD
No
infe
ctio
n:co
nvul
sion
:hy
pot.
446
FPo
st-o
p.C
A8
w12
00N
oN
oB
ZN
oN
oD
DD
DF
No
544
MD
rugs
/alc
ohol
:10
w13
00N
o�
�D
No
DD
No
DD
Dm
hypo
t.6
22F
Car
diom
yopa
thy
11w
1320
No
�B
ZN
oN
oN
oN
oD
DD
No
(pre
gnan
cy):
hypo
t.7
24M
Cer
ebra
lab
sces
s/4
m14
20N
o�
�A
TF
DN
oF
DD
Dm
men
ingi
tis8
48M
Bro
msu
lpht
hale
in5
m12
50N
o�
��
DA
DD
DD
DD
mC
A9
58M
Bro
ncho
spas
m5
m11
00N
o�
�D
AD
DD
DD
Dm
CA
1048
MSm
oke
inha
latio
n7
m11
10N
o�
�D
AD
DD
DD
Dm
1117
MPo
st-o
p.C
A9
mN
KN
o�
��
DA
DD
DD
DD
m12
21M
Asp
hyxi
a–
seal
ed10
m14
60N
oN
oN
oD
LM
No
No
DD
DB
ZN
ove
hicl
e(?
CO
)13
38M
Stab
wou
nd:
1y
9m
1050
No
��
DA
DD
DD
DD
No
hypo
t.,co
nvul
sion
s14
2F
Post
-op.
CA
4y
515
No
��
�D
AD
DD
DD
DN
o
Cau
se:
CA
�ca
rdia
car
rest
;hy
pot.
�an
acut
eep
isod
eof
hypo
tens
ion;
CO
�po
ssib
lepr
esen
ceof
carb
onm
onox
ide.
Surv
ival
:w
�w
eek(
s);
m�
mon
th(s
);y
�ye
ar(s
).B
rain
wei
ght:
NK
�no
tkn
own.
ICP�
�ra
ised
intr
acra
nial
pres
sure
.H
ydro
ceph
alus
:�
�sl
ight
enla
rgem
ent
ofth
eve
ntri
cula
rsy
stem
;�
��
mod
erat
e;�
��
�se
vere
.N
eoco
rtex
:D
�di
ffus
ehy
poxi
cda
mag
e;B
Z�
hypo
xic
dam
age
inar
teri
albo
unda
ryzo
nes;
AT
�hy
poxi
cda
mag
ein
arte
rial
terr
itori
es.
SCW
M�
subc
ortic
alw
hite
mat
ter:
F�
foca
lda
mag
ein
rela
tion
toda
mag
eto
the
neoc
orte
x;A
�as
troc
ytos
is;
DL
M�
diff
use
loss
ofm
yelin
.In
all
othe
rco
lum
ns:
D�
diff
use
hypo
xic
dam
age;
F�
foca
lda
mag
e;B
Z�
dam
age
inar
teri
albo
unda
ryzo
nes;
m�
min
imal
abno
rmal
ities
iden
tified
only
mic
rosc
opic
ally
.

1334 J. H. Adams et al.
Fig. 4 Table 2, case 8: survival 5 months after an episode ofcardiac arrest. The cerebral cortex is thin and granular. Thethalamus is small and there is enlargement of the ventricularsystem. Reproduced with permission from Graham (1992).
protein of β-amyloid has rendered the identification of axonalinjury much more reliable (Gentleman et al., 1993; Sherriffet al., 1994). Indeed, it would now appear that grade 1 DAIis of frequent occurrence in head injuries (Gentleman et al.,1995). There is now, as a result of these more recent studies,a structural basis to account for persisting minimal clinicalsequelae after what appeared to have been only a minorhead injury (Oppenheimer, 1968; Clark, 1974; Blumbergset al., 1994).
Whether or not there is total disruption of axons at themoment of injury, as had originally been suggested byStrich (Strich, 1956) and subsequently supported by otherinvestigators, has been controversial. In ultrastructural studiesof the brains of non-human primates subjected to shear-strains identical to those known to produce DAI in the brain,disruption immediately after injury has been seen (Maxwellet al., 1993). Such primary axotomy, however, is uncommonand there is increasing recognition of damaged axonsundergoing a process of secondary axotomy (Maxwell et al.,1997). The axons undergo a sequence of events: initiallythere is focal swelling of axons (Maxwell et al., 1995; Pettusand Povlishock, 1996) and thereafter swelling of axonalmitochondria (Pettus et al., 1994; Maxwell et al., 1995;Pettus and Povlishock, 1996), the development of nodal blebs(Maxwell et al., 1991) and/or a focal decrease in theinternodal axonal diameter. This is followed by loss of axonalmicrotubules (Maxwell, 1995, 1996; Pettus and Povlishock,1996; Jafari et al., 1997; Povlishock et al., 1997) andalterations of the intra-axonal relationships of neurofilaments(Pettus and Povlishock, 1996; Jafari et al., 1997). Next, thereis involution of the internodal axolemma (Povlishock, 1992;Pettus et al., 1994; Maxwell et al., 1995) followed byseparation of the axolemma from the internal aspect of themyelin sheath (Maxwell et al., 1995), the development ofaxonal swellings (Maxwell et al., 1991, 1995; Povlishock,1992), the development of myelin intrusions (Povlishock
et al., 1983; Maxwell et al., 1995) and finally axonalseparation (Povlishock, 1992; Jafari et al., 1997) to formaxonal (‘retraction’) bulbs. Subsequently, more severemorphological changes take place including axonal ruptureand Wallerian-type degeneration (Strich, 1956). This has ledto the concept of secondary axotomy in the pathogenesis ofDAI. In a review of the literature, Maxwell and colleaguesconcluded that, whereas primary axotomy could be identifiedwithin 60 min of injury, secondary axotomy required aminimum of 4 h to develop (Maxwell et al., 1997).
Whether or not axons are disrupted at the moment ofinjury in patients who sustain DAI, they are clearly renderedimmediately dysfunctional and temporary changes ofconduction in damaged axons now seem the most likelycause of transient disturbances of consciousness after a headinjury (concussion). Further clinicopathological studies haveestablished that there are many differences between patientswith the more severe grades of DAI compared with othertypes of head injury. For example, the former never experiencea lucid interval; they have a low incidence of fracture ofthe skull, traumatic intracranial haematomas and increasedintracranial pressure; and surface contusions are seldomsevere—all features of the present series (Table 1).
The occurrence of structural changes in the thalamus inassociation with DAI is dependent on the length of survivalof the patient because it is transneuronal in origin and takesabout 3 months to appear. Thus, in the present series thethalamus appeared normal on microscopical examination insix of the seven patients with DAI who survived for 12weeks or less after their injuries, notwithstanding the presenceof widespread damage to subcortical white matter (Table 1).There is no rational explanation for the fact that there wasno transneuronal change in the thalamus of traumatic case25 who survived in a vegetative state for 18 months as aresult of DAI despite there being diffuse degeneration in thesubcortical white matter. This was the only patient in thetraumatic group who survived for 3 months or more in whomthere were no identifiable abnormalities in the thalamus. Inthe traumatic group the thalamus was abnormal in 28 (80%)of all cases and in 96% of those who survived for more than3 months.
The importance of grades 2 and 3 DAI as a cause of thevegetative state after head injury is evident from Table 1,these being a feature of 71% of the cases in the present series.
Moderate to severe ischaemic brain damage, particularlyin the patients with intracranial haematomas or extracranialinjuries, was also common (43%). It has long been knownthat ischaemic damage is not uncommon in patients withfatal head injuries (Graham et al., 1978), particularly if theintracranial pressure has been high (Graham et al., 1987,1989). In the series of 151 unselected non-missile headinjuries published by Graham and colleagues, moderate tosevere ischaemic brain damage was observed in 96 cases(64%) (Graham et al., 1978). Its pathogenesis, namely aregional or global failure of cerebral blood flow, is likely to

Vegetative state 1335
be similar to the cause of the brain damage in some of thenon-traumatic cases to be discussed in the next section.
A striking feature in the traumatic cases of the vegetativestate is the low incidence of damage to the brainstem (14%);in all five cases with this type of brain damage it was slightand never haemorrhagic. This confirms the view we haveheld for a long time that patients who develop classicsecondary haemorrhage and infarction in the brainstem as aresult of an acute intracranial expanding lesion survive foronly a short time. Thus, a post-traumatic vegetative statemay occur in patients in whom both the cerebral cortex andbrainstem are intact.
The causes and patterns of hypoxic brain damage inpatients who have sustained an acute circulatory catastrophehave long been an interest of neuropathologists and clinicians(Adams et al., 1966; Dougherty et al., 1981; Cole and Cowie,1987; Kinney and Samuels, 1994). The classic example isthe brain damage brought about by a period of true cardiacarrest. This takes the form of diffuse neuronal necrosis inthe regions of selective vulnerability. In the neocortex thereis laminar necrosis, more severe in the depths of sulci thanon their crests, and tending to increase in severity from thefrontal to the occipital poles, but often with some sparing ofthe medial occipital cortex. There is also diffuse neuronalnecrosis in the hippocampal and amygdaloid structures, inthe major relay nuclei of the thalamus, in the Purkinje cellsof the cerebellum and, variably, in other structures in thedeep grey matter. Essentially similar patterns of brain damagemay occur as a result of other types of hypoxic insultsuch as status epilepticus, carbon monoxide poisoning andasphyxia (Auer and Benveniste, 1997), and hypoglycaemia(Auer et al., 1989). This diffuse pattern of ischaemic damagewas found in nine of the cases of the non-traumatic vegetativestate (Table 2). The second pattern of brain damage is focal.Here the classic example is brain damage brought about bya short episode of profound hypotension (Adams et al., 1966;Torvik and Jorgensen, 1969; Auer and Benveniste, 1997)when ischaemic damage is confined to the arterial boundaryzones in the cerebral and cerebellar hemispheres. The affectedzones tend to be wedge-shaped with their base on the surfaceand their apex deep within the brain, e.g. adjacent to the angleof a lateral ventricle. There is almost always involvementof the thalamus and there is variable involvement of thehippocampal structures and the deep grey matter. This patternof brain damage was present in three of the non-traumaticcases (Table 2). Another type of focal ischaemic brain damageis, because of local factors compromising the blood flowthrough individual arteries, restricted to specific arterialterritories. There was one case of this type in the presentseries; there were also variable ischaemic lesions in otherstructures, but damage to the thalamus was diffuse (Table 2).
In one case (case 12 in Table 2) there were no abnormalitiesin the cerebral cortex, the principal abnormality being severedestruction of the subcortical white matter of the typeassociated with carbon monoxide poisoning (Lapresle andFardeau, 1966; Vuia, 1967; Auer and Benveniste, 1997), and
Fig. 5 Carbon monoxide poisoning: survival 21 days. Thecerebral cortex is intact but there is extensive destruction of thesubcortical white matter. (A) Heidenhain’s stain for myelin, (B)cresyl violet. Bar � 1 cm.

1336 J. H. Adams et al.
there was the unconfirmed possibility that there could havebeen some carbon monoxide in the vehicle in which he hadbecome accidentally sealed. An almost identical case ofconfirmed carbon monoxide poisoning (Fig. 5) that we havereported (Hart et al., 1988) would have been included in thispaper had the patient survived in a vegetative state for theadditional few days required to fulfil the criterion of amonth’s survival. In both cases, there was diffuse neuronalloss in the thalamus. It is of some interest that we have neverseen or encountered a case of the vegetative state caused byhypoglycaemia. It would appear, therefore, that most suchcases either die less than a month after the episode or makevarying degrees of recovery. However, one of us (B.J.) hasseen a clinical case of a teenager who survived for severalyears in a vegetative state after hypoglycaemia. Somecertainly remain severely disabled (Kalimo and Olsson, 1980;Auer et al., 1989).
In patients who sustain severe brain damage as a result ofsome catastrophic circulatory event, there is characteristicallyminimal or no damage in the brainstem, as was the case inthe present series.
Thus, as in the traumatic group of cases, there are patientsin the non-traumatic group where the vegetative state waspresent without there being diffuse damage to the cerebralcortex or severe damage in the brainstem. Diffuse neuronalloss in the thalamus was, however, a common factor in all.
The Multi-Society Task Force recognized that the potentialfor recovery from the vegetative state was greater aftertraumatic than non-traumatic insults (Multi-Society TaskForce, 1994). This may be related to the differing types ofdamage sustained by neurons in the thalamus. In acutehypoxic episodes the neurons that are lost have undergoneischaemic necrosis and will therefore never function again.In contrast, in DAI there is no actual loss of neurons, onlytransneuronal degeneration. If there is any delayed restorationof function in the axons damaged at the time of the originalinjury, the substrate of thalamic neurons is still there and,conceivably, may be able to function again. Anotherdifference between the traumatic and non-traumatic caseswas the frequency of diffuse ischaemic damage in theneocortex: this occurred in 64% of the non-traumatic casesbut in only 11% of the traumatic cases. The respective figuresfor any type of ischaemic damage in the neocortex were 93and 37%.
We also have considerable experience of the neuro-pathological abnormalities in patients who remained severelydisabled but not vegetative as a result of an acute braininsult. In some of these brains there were lesions similar tothose found in some of the vegetative patients, particularlyin the traumatic group, in that some severely disabled patientshad grades 2 or 3 DAI including damage to the thalamus.The severity of the damage may have been more severe inthe vegetative patients but, as yet, we have been unable todevise a quantitative method to measure damage to axons.
It is clear from the present account of 49 clinicallyconfirmed patients who were in a vegetative state for 1 month
or more, that this condition can occur in patients in whomthere are no identifiable structural abnormalities in thecerebral cortex, the cerebellum or the brainstem. The featurescommon to all are widespread destruction of the white matterof the cerebral hemispheres and/or the thalamus. With oneexception (case 25)—and we cannot account for this—all ofthe patients with DAI in whom no abnormalities could beidentified in the thalamus had not survived long enough fortransneuronal degeneration to have occurred. Diffuse damageto subcortical white matter was, however, common to allpatients. In all of the patients in whom the vegetative statehad been produced by some hypoxic episode, there wasdiffuse and severe damage to each thalamus. It must thereforebe concluded that the fundamental structural abnormality inpatients with the vegetative state is subcortical and is relatedto damage to the white matter of the cerebral hemispheresand/or the thalamus. These lesions do, however, renderany structurally intact cortex unable to function becauseconnections between different cortical areas via the thalamicnuclei are no longer viable, and there is also extensivedamage to afferent and efferent cerebral connections.
ReferencesAdams JH, Graham DI. The relationship between ventricular fluidpressure and the neuropathology of raised intracranial pressure.Neuropathol Appl Neurobiol 1976; 2: 323–32.
Adams JH, Brierley JB, Connor RC, Treip CS. The effects ofsystemic hypotension upon the human brain. Clinical andneuropathological observations in 11 cases. Brain 1966; 89: 235–68.
Adams JH, Mitchell DE, Graham DI, Doyle D. Diffuse braindamage of immediate impact type. Brain 1977; 100: 489–502.
Adams JH, Graham DI, Scott G, Parker LS, Doyle D. Brain damagein fatal non-missile head injury. J Clin Pathol 1980; 33: 1132–45.
Adams JH, Graham DI, Murray LS, Scott G. Diffuse axonal injurydue to nonmissile head injury in humans: an analysis of 45 cases.Ann Neurol 1982; 12: 557–63.
Adams JH, Doyle D, Graham DI, Lawrence AE, McLellan DR.Microscopic diffuse axonal injury in cases of head injury. Med SciLaw 1985a; 25: 265–9.
Adams JH, Doyle D, Graham DI, Lawrence AE, McLellan DR,Gennarelli TA, et al. The contusion index: a reappraisal in human andexperimental non-missile head injury. Neuropathol Appl Neurobiol1985b; 11: 299–308.
Adams JH, Doyle D, Ford I, Gennarelli TA, Graham DI, McLellanDR. Diffuse axonal injury in head injury: definition, diagnosis andgrading. Histopathology 1989; 15: 49–59.
Adams JH, Jennett B, McLellan DR, Murray LS, Graham DI. Theneuropathology of the vegetative state after head injury. J ClinPathol 1999; 52: 804–6.
Auer RN, Benveniste H. Hypoxia and related conditions. In: GrahamDI, Lantos PL, editors. Greenfield’s neuropathology, Vol. 1, 6th ed.London: Arnold; 1997. p. 263–314.

Vegetative state 1337
Auer RN, Hugh J, Cosgrove E, Curry B. Neuropathologic findingsin three cases of profound hypoglycemia. Clin Neuropathol 1989;8: 63–8.
Blumbergs PC, Scott G, Manavis J, Wainwright H, Simpson DA,McLean AJ. Staining of amyloid precursor protein to study axonaldamage in mild head injury. Lancet 1994; 344: 1055–56.
Brierley JB, Graham DI, Adams JH, Simpson JA. Neocortical deathafter cardiac arrest: a clinical, neurophysiological, and neuro-pathological report of two cases. Lancet 1971; 2: 560–5.
Clark JM. Distribution of microglial clusters in the brain after headinjury. J Neurol Neurosurg Psychiatry 1974; 37: 463–74.
Cole G, Cowie VA. Long survival after cardiac arrest: case reportand neuropathological findings. Clin Neuropathol 1987; 6: 104–9.
Dougherty JH Jr, Rawlinson DG, Levy DE, Plum F. Hypoxic-ischemic brain injury and the vegetative state: clinical andneuropathologic correlation. Neurology 1981; 31: 991–7.
French JD. Brain lesions associated with prolonged unconsciousness.Arch Neurol Psychiat 1952; 68: 727–40.
Gennarelli TA, Thibault LE, Adams JH, Graham DI, Thompson CJ,Marcincin RP. Diffuse axonal injury and traumatic coma in theprimate. Ann Neurol 1982; 12: 564–74.
Gennarelli TA, Thibault LE, Graham DI. Diffuse axonal injury: animportant form of traumatic brain damage. Neuroscientist 1998; 4:202–15.
Gentleman SM, Nash MJ, Sweeting CJ, Graham DI, Roberts GW.β-amyloid precursor protein (βAPP) as a marker for axonal injuryafter head injury. Neurosci Lett 1993; 160: 139–44.
Gentleman SM, Roberts GW, Gennarelli TA, Maxwell WL, AdamsJH, Kerr S, et al. Axonal injury: a universal consequence of fatalclosed head injury? Acta Neuropathol (Berl) 1995; 89: 537–43.
Graham DI. Hypoxia and vascular disorders. In: Adams JH, DuchenLW, editors. Greenfield’s neuropathology. 5th ed. London: EdwardArnold; 1992. p. 153–268.
Graham DI, Adams JH, Doyle D. Ischaemic brain damage in fatalnon-missile head injuries. J Neurol Sci 1978; 39: 213–34.
Graham DI, Lawrence AE, Adams JH, Doyle D, McLellan DR. Braindamage in non-missile head injury secondary to high intracranialpressure. Neuropathol Appl Neurobiol 1987; 13: 209–17.
Graham DI, Ford I, Adams JH, Doyle D, Teasdale GM, LawrenceAE, et al. Ischaemic brain damage is still common in fatal non-missile head injury. J Neurol Neurosurg Psychiatry 1989; 52: 346–50.
Hart IK, Kennedy PG, Adams JH, Cunningham NE. Neurologicalmanifestation of carbon monoxide poisoning. Postgrad Med J 1988;64: 213–6.
Holbourn AHS. Mechanics of head injuries. Lancet 1943; 2: 438–41.
Holbourn AHS. The mechanics of brain injuries. Br Med Bull 1945;3: 147–9.
Ingvar DH, Brun A, Johansson L, Samuelsson SM. Survival aftersevere cerebral anoxia with destruction of the cerebral cortex: theapallic syndrome. Ann NY Acad Sci 1978; 315: 184–214.
Jafari SS, Maxwell WL, Neilson M, Graham DI. Axonal cytoskeletal
changes after non-disruptive axonal injury. J Neurocytol 1997; 26:207–21.
Jellinger K. Pathology and pathogenesis of apallic syndromesfollowing closed head injuries. In: Dalle Ore G, Gerstenbrand F,Lucking CH, Peters F, Peters UH, editors. The Apallic syndrome .Berlin: Springer-Verlag; 1977. p. 88–103.
Jellinger KA. The brain of Karen Ann Quinlan [letter]. N Engl JMed 1994; 331: 1378–9.
Jellinger K, Seitelberger F. Protracted post-traumatic encephalo-pathy: pathology, pathogenesis and clinical implications. J NeurolSci 1970; 10: 51–94.
Jennett B. A quarter century of the vegetative state: an internationalperspective. J Head Trauma Rehabil 1997; 12: 1–12.
Jennett B, Plum F. Persistent vegetative state after brain damage.A syndrome in search of a name. Lancet 1972; 1: 734–7.
Kalimo H, Olsson Y. Effects of severe hypoglycemia on the humanbrain. Neuropathological case reports. Acta Neurol Scand 1980; 62:345–56.
Kinney HC, Samuels MA. Neuropathology of the persistentvegetative state. A review. [Review]. J Neuropathol Exp Neurol1994; 53: 548–58.
Kinney HC, Korein J, Panigrahy A, Dikkes P, Goode R.Neuropathological findings in the brain of Karen Ann Quinlan. Therole of the thalamus in the persistent vegetative state. N Engl JMed 1994; 330: 1469–75.
Lapresle J, Fardeau M. The leukoencephalopathies caused by carbonmonoxide poisoning. Study of sixteen anatomo-clinical observations.[French]. Acta Neuropathol (Berl) 1966; 6: 327–48.
McLean SA. Legal and ethical aspects of the vegetative state. J ClinPathol 1999; 52: 490–3.
Maxwell WL. Microtubular changes in axons after stretch injury[abstract]. J Neurotrauma 1995; 12: 363.
Maxwell WL. Histopathological changes at central nodes of Ranvierafter stretch-injury. Microsc Res Tech 1996; 34: 522–35.
Maxwell WL, Irvine A, Graham DI, Adams JH, Gennarelli TA,Tipperman R, et al. Focal axonal injury: the early axonal responseto stretch. J Neurocytol 1991; 20: 157–64.
Maxwell WL, Watt C, Graham DI, Gennarelli TA. Ultrastructuralevidence of axonal shearing as a result of lateral acceleration of thehead in non-human primates. Acta Neuropathol (Berl) 1993; 86:136–44.
Maxwell WL, McCreath BJ, Graham DI, Gennarelli TA.Cytochemical evidence for redistribution of membrane pumpcalcium-ATPase and ecto-Ca-ATPase activity, and calcium influxin myelinated nerve fibres of the optic nerve after stretch injury.J Neurocytol 1995; 24: 925–42.
Maxwell WL, Povlishock JT, Graham DI. A mechanistic analysisof nondisruptive axonal injury: a review. [Review]. J Neurotrauma1997; 14: 419–40.
Multi-Society Task Force on PVS. Medical aspects of the persistentvegetative state. [Review]. N Engl J Med 1994; 330: 1572–9.

1338 J. H. Adams et al.
Oppenheimer DR. Microscopic lesions in the brain following headinjury. J Neurol Neurosurg Psychiatry 1968; 31: 299–306.
Peerless SJ, Rewcastle NB. Shear injuries of the brain. Can MedAssoc J 1967; 96: 577–82.
Peters G, Rothemund E. Neuropathology of the traumatic apallicsyndrome. In: Dalle Ore G, Gerstenbrand F, Lucking CH, Peters F,Peters UH, editors. The Apallic syndrome. Berlin: Springer-Verlag;1977. p. 78–87.
Pettus EH, Povlishock JT. Characterization of a distinct set of intra-axonal ultrastructural changes associated with traumatically inducedalteration in axolemmal permeability. Brain Res 1996; 25: 722: 1–11.
Pettus EH, Christman CW, Giebel ML, Povlishock JT. Traumaticallyinduced altered membrane permeability: its relationship totraumatically induced reactive axonal change. J Neurotrauma 1994;11: 507–22.
Povlishock JT. Traumatically induced axonal injury: pathogenesisand pathobiological implications. [Review]. Brain Pathol 1992; 2:1–12.
Povlishock JT, Becker DP, Cheng CL, Vaughan GW. Axonal changein minor head injury. J Neuropathol Exp Neurol 1983; 42: 225–42.
Povlishock JT, Marmarou A, McIntosh T, Trojanowski JQ, Moroi J.Impact acceleration injury in the rat: evidence for focal axolemmalchange and related neurofilament sidearm alteration. J NeuropatholExp Neurol 1997; 56: 347–59.
Pudenz RH, Shelden CH. The lucite calvarium – a method for
direct observation of the brain: II. Cranial trauma and brainmovement. J Neurosurg 1946; 3: 487–505.
Reilly PL, Graham DI, Adams JH, Jennett B. Patients with headinjury who talk and die. Lancet 1975; 2: 375–7.
Relkin NR, Petito CK, Plum F. Coma and the vegetative stateassociated with thalamic injury after cardiac arrest [abstract]. AnnNeurol 1990; 28: 221–2.
Royal College of Physicians Working Party. The permanentvegetative state. J R Coll Physicians Lond 1996; 30: 119–21.
Sherriff FE, Bridges LR, Sivaloganathan S. Early detection ofaxonal injury after human head trauma using immunocytochemistryfor β-amyloid precursor protein. Acta Neuropathol (Berl) 1994; 87:55–62.
Strich SJ. Diffuse degeneration of the cerebral white matter in severedementia following head injury. J Neurol Neurosurg Psychiatry 1956;19: 163–85.
Torvik A, Jorgensen L. Ischaemic cerebrovascular diseases in anautopsy series. 2. Prevalence, location, pathogenesis, and clinicalcourse of cerebral infarcts. J Neurol Sci 1969; 9: 285–320.
Vuia O. Subcortical leukoencephalopathy caused by CO poisoning.[French]. Acta Neuropathol (Berl) 1967; 7: 305–14.
Zimmerman RA, Bilaniuk LT, Genneralli T. Computed tomographyof shearing injuries of the cerebral white matter. Radiology 1978;127: 393–6.
Received September 14, 1999. Revised November 29, 1999.Accepted December 10, 1999