The mucosubstances rectal biopsies patients ulcerative Crohn's · Gut, 1970, 11, 229-234...
6
Gut, 1970, 11, 229-234 The diagnostic value of mucosubstances in rectal biopsies from patients with ulcerative colitis and Crohn's disease M. I. FILIPE AND IAN DAWSON From the Department of Clinical Histochemistry, Westminster Medical School, London SUMMARY Sixty-two biopsies from 36 patients with ulcerative colitis and 29 biopsies from 15 patients with Crohn's disease were studied with special reference to the content of neutral, acid non-sulphated and sulphated mucosubstances. A marked decrease was found in muco- substance in patients with active ulcerative colitis and was related to the intensity of inflam- mation in the lamina propria but not to the duration of the disease. In patients with active Crohn's disease there was no corresponding decrease. Techniques for mucosubstances appear to be of value in differentiating between the two diseases in rectal biopsies. The importance of rectal biopsy in the diagnosis and follow up of ulcerative colitis and Crohn's disease of the large intestine has been emphasized by Matts (1961), Gonzalez-Licea and Yardley (1966), and others. Biopsy also has an important role in attempts to separate these two diseases. There are, however, limitations to the value of conventional histology; for example the histo- logical lesions found in ulcerative colitis are not always specific and can be inseparable from those seen in other inflammations such as bacillary dysentery. Nor is histology always helpful in the differential diagnosis between ulcerative colitis and Crohn's disease when pathological features of both are present (Lewin and Swales, 1966). For these reasons many workers have turned to histochemical or ultrastructural techniques for the further evaluation of such biopsies. Ultra- structural changes have been described as of value in detecting disease activity (Gonzalez- Licea and Yardley, 1966) but none have so far been described which are diagnostic of ulcerative colitis or of Crohn's disease. Monis and Mendeloff (1965) described characteristic changes in the distribution of NADP-linked dehydrogenases and non-specific esterases in ulcerative colitis, but these findings have not been confirmed by other workers (Van Noorden, Thayer, Yesner, and Spiro, 1967; Melnyk, Braucher, and Kirsner, 1967; Filipe, 1968), and there are no ultra- structural changes at the epithelial cell apex to correlate with them. Other workers have turned to a study of mucosal mucins in colectomy specimens from ulcerative colitis (Greco, Lauro, Fabbrini, and Torsoli, 1967) and ulcerative colitis and Crohn's disease (Hellstrom and Fisher, 1967). This seems a profitable line of approach, bearing in mind that rectal biopsy is easy and relatively innocuous and is being increasingly used by clinicians as a complement to clinical, radiological, and sig- moidoscopic investigations. It was decided to review all rectal biopsies of confirmed cases of ulcerative colitis and Crohn's disease of the large bowel seen in the Vincent Square Laboratories of Westminster Hospital over the past ten years, using histochemical techniques for muco- substances to assess their value as an aid to definitive differential diagnosis between the two conditions. Material and Methods The studies presented here were on rectal biopsies from patients treated at the Gordon Hospital (Westminster Group) during the period 1958 to 1968 and in all of them a diagnosis of either ulcerative colitis or Crohn's disease of the large on October 2, 2020 by guest. Protected by copyright. http://gut.bmj.com/ Gut: first published as 10.1136/gut.11.3.229 on 1 March 1970. Downloaded from
Transcript of The mucosubstances rectal biopsies patients ulcerative Crohn's · Gut, 1970, 11, 229-234...

Gut, 1970, 11, 229-234
The diagnostic value of mucosubstances inrectal biopsies from patients with ulcerativecolitis and Crohn's disease
M. I. FILIPE AND IAN DAWSONFrom the Department of Clinical Histochemistry, Westminster Medical School, London
SUMMARY Sixty-two biopsies from 36 patients with ulcerative colitis and 29 biopsies from15 patients with Crohn's disease were studied with special reference to the content of neutral,acid non-sulphated and sulphated mucosubstances. A marked decrease was found in muco-substance in patients with active ulcerative colitis and was related to the intensity of inflam-mation in the lamina propria but not to the duration of the disease. In patients with activeCrohn's disease there was no corresponding decrease. Techniques for mucosubstances appearto be of value in differentiating between the two diseases in rectal biopsies.
The importance of rectal biopsy in the diagnosisand follow up of ulcerative colitis and Crohn'sdisease of the large intestine has been emphasizedby Matts (1961), Gonzalez-Licea and Yardley(1966), and others. Biopsy also has an importantrole in attempts to separate these two diseases.There are, however, limitations to the value ofconventional histology; for example the histo-logical lesions found in ulcerative colitis are notalways specific and can be inseparable from thoseseen in other inflammations such as bacillarydysentery. Nor is histology always helpful in thedifferential diagnosis between ulcerative colitisand Crohn's disease when pathological features ofboth are present (Lewin and Swales, 1966).For these reasons many workers have turned to
histochemical or ultrastructural techniques forthe further evaluation of such biopsies. Ultra-structural changes have been described as ofvalue in detecting disease activity (Gonzalez-Licea and Yardley, 1966) but none have so farbeen described which are diagnostic of ulcerativecolitis or ofCrohn's disease. Monis and Mendeloff(1965) described characteristic changes in thedistribution of NADP-linked dehydrogenasesand non-specific esterases in ulcerative colitis,but these findings have not been confirmed byother workers (Van Noorden, Thayer, Yesner, andSpiro, 1967; Melnyk, Braucher, and Kirsner,1967; Filipe, 1968), and there are no ultra-
structural changes at the epithelial cell apex tocorrelate with them.
Other workers have turned to a study ofmucosal mucins in colectomy specimens fromulcerative colitis (Greco, Lauro, Fabbrini, andTorsoli, 1967) and ulcerative colitis and Crohn'sdisease (Hellstrom and Fisher, 1967). This seemsa profitable line of approach, bearing in mind thatrectal biopsy is easy and relatively innocuousand is being increasingly used by clinicians as acomplement to clinical, radiological, and sig-moidoscopic investigations. It was decided toreview all rectal biopsies of confirmed cases ofulcerative colitis and Crohn's disease of the largebowel seen in the Vincent Square Laboratories ofWestminster Hospital over the past ten years,using histochemical techniques for muco-substances to assess their value as an aid todefinitive differential diagnosis between the twoconditions.
Material and Methods
The studies presented here were on rectal biopsiesfrom patients treated at the Gordon Hospital(Westminster Group) during the period 1958to 1968 and in all of them a diagnosis of eitherulcerative colitis or Crohn's disease of the large
on October 2, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.11.3.229 on 1 M
arch 1970. Dow
nloaded from

230 M. I. Filipe and Ian Dawson
Disease Histology
Acute Chronic Quiescent Fulminant Non- Normal Typical BorderlineActive specific (Group (Groups
])1 2.3)1
Ulcerative colitis (36 patients)11 32 2 3 13 1
Total 62 rectal biopsies
Crohn's disease (15 patients)5 4 15 5
Total 29 rectal biopsies
Table I Histological classification ofthe cases studied'According to classification of Lewin and Swales (1966)
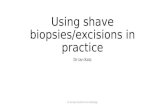
Fig. 1 Normal rectal mucosa to show sulphatedmucosubstance (dark staining high iron diamine andalcian blue) predominantly in the lower two-thirdsand a mixture ofsulphated and acid non-sulphatedmucosubstance in the upper third. x 60
intestine was confirmed histologically in colec-tomy specimens.
All patients on whom a rectal biopsy was
performed but no operation specimen was avail-able for pathological confirmation are excluded.A total of 91 rectal biopsies from 51 patients ful-filled these conditions. Thirty-six patients (62rectal biopsies) suffered from ulcerative colitisand 15 (29 rectal biopsies) were cases of Crohn'sdisease affecting the large bowel. All specimenswere initially fixed in 10% formalin, embeddedin paraffin, and stained with haematoxylin andeosin.The 62 rectal biopsies from cases of ulcerative
colitis were divided into six categories accordingto the histological findings using the classificationof Dawson and Pryse-Davies (1959). The 29rectal biopsies from patients with Crohn's diseasewere also divided in four groups according to thehistological type of lesions observed, broadlybased on that of Lewin and Swales (1966).The classification of mucosubstances is con-
fused (Spicer, Leppi, and Stoward, 1965) and itis not proposed to discuss it here. Epithelialmucosubstances are probably all glycopoly-
peptides in which carbohydrates are linked to theside chains of amino acids forming the poly-peptide strand through covalent bonds (Jeanloz,1960, 1963; Gottschalk, 1962). The carbohydrateunits are either disaccharides or polysaccharidesof low molecular weight, often with a terminalsialic acid group. Histocnemical techniquesidentify the carbohydrate as opposed to the poly-peptide component, and allow a simple classi-fication into neutral, acid non-sulphated, andsulphated mucosubstances. The following tech-niques have been used on sections from theoriginal paraffin blocks. Periodic acid-Schiff totest for neutral mucosubstances, alcian blue atpH 2.5 followed by periodic acid-Schiff to testfor acid non-sulphated and neutral muco-substances (Mowry and Morard, 1957), and highiron diamine followed by alcian blue at pH 2.5for acid sulphated and acid non-sulphated muco-substances (Spicer, 1965).The amount of mucosubstance present was
estimated semiquantitatively on a visual basisusing a scale from 0 to + + + with + ±1++ +representing the normal.
Results
CLINICAL FINDINGSThe age at first onset of symptoms lay between13 and 78 years (mean 45.5) for 36 patients withulcerative colitis, with a fairly even scatterbetween the third, fourth, and fifth decades and aconsiderable number beginning in the seventhdecade, and between 11 and 50 years (mean 30.5)for 15 cases with Crohn's disease with a maximumincidence in the second and third decades. Theduration of symptoms up to 'the time of biopsyvaried from one month to 23 years in colitics,being less than four years in the majority, andin Crohn's disease it varied from four to 27 years,being four to eight years in the majority. The sexincidence was equal in both ulcerative colitis andCrohn's disease.
HISTOLOGICAL FINDINGSThere were 62 biopsies from 36 patients withulcerative colitis, classified as shown in Table I.In some patients who had more than one biopsythe_histological pattern changed as the diseaseprogressed. There were 29 biopsies from 15patients with Crohn's disease classified as shownin Table I.
HISTOCHEMICAL FINDINGSIn the normal adult rectal mucosa the lower two-thirds of the crypt contains goblet cells with apredominance of sulphated mucosubsfances butno neutral mucosubstance, while the goblet cellsof surface epithelium and the upper one-third
on October 2, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.11.3.229 on 1 M
arch 1970. Dow
nloaded from

The diagnostic value of mucosubstances in rectal biopsies
Amount of Mucus (No. of Cases)
Histology o/+ +I++Io ++/+++ Variable Totalo/+/+ +1+ + +
Ulcerative ColitisAcute 4 5 2 11Chronic active 18 9 5 32Quiescent 2 2Fulminant 1 1 1 3Non-specific lesions 1 1 2 13Normal 11 1
Total 23 26 7 6 62
Crohn's DiseaseTypical lesion 1 13 1 15Borderline cases 5 5Non-specific lesions 5 5Normal 4 4
Total 1 27 1 29
Table II Variations in the amount of mucosubstancein mucosa in relation to the histological picture1+ +
Fig. 2 Rectal mucosa in chronic active ulcerativecolitis. (Haematoxylin and eosin) x 52.
Amount ofMucus
Ulcerative Colitis Crohn's Disease
Histology oI+/++ ++/+++ o/+l++ ++I+++Inflammatory or Variable or VariableInfiltrate
Heavy 29 7 1 7Moderate 11 7 0 11Mild ornormal 5 3 1 9Total 45 17 2 27
Table III Relationship between the amount of mucusin the mucosa and the degree ofinflammation in laminapropria
contain a mixture of sulphated and non-sulphatedacid mucosubstances, with a variable smallamount of neutral mucosubstance (Figure 1). Therectal mucosa of children aged from 2 days to 8years shows a similar pattern (Filipe, 1969).An attempt was made to classify any alteration
in the amount of mucosubstance in the biopsiesin terms of sulphated, acid non-sulphated, orneutral mucosubstance. In any general reductionin the amount of mucosubstance, both sulphatedand acid non-sulphated mucosubstances decrease,but this reduction affects the non-sulphated lessthan the sulphated. No increases above normalwere found in any mucosubstances.
Table II shows the semiquantitative findingsfor mucosubstances related to the different histo-logical patterns in ulcerative colitis and inCrohn's disease. In both diseases where polypoidzones were present in the biopsies non-polypoidzones were chosen without extensive ulcerationfor the estimations, since it was found that poly-poid zones invariably contained abundantmucosubstances, and severely ulcerated zoneshave insufficient mucosa for reliable estimates.The findings show clearly a decrease in muco-substances in the majority of cases of ulcerativecolitis but no corresponding decrease in Crohn'sdisease (Figures 2 to 6).A correlation of the amount of mucosubstance
present with the duration of disease was nextattempted but no positive correlation could befound. An attempt to correlate the amountof mucosubstance with the degree of inflam-mation in the lamina propria was (Table III)more successful. In the colitic group, 36 of the 62rectal biopsies had a heavy inflammatory cellularinfiltrate in the lamina propria (Fig. 2), and 29in this group had a marked generalized decreasein mucosubstance and four a patchy decrease(Fig. 3), while only three had normal amounts.Eighteen biopsies showed a moderate inflam-matory infiltrate of which 11 showed a markeddecrease in mucosubstances, while seven showedslight decreases. Eight showed mild inflammatory
Fig. 3 Serial section of biopsy in Fig. 2 to showthe marked decrease in mucosubstance. (High irondiamine and alcian blue) x 51.
on October 2, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.11.3.229 on 1 M
arch 1970. Dow
nloaded from

232 M. L Filipe and Ian Dawson
Fig. 4 Rectal muicosa in acute ulcerative colitis.There is a marked decrease in mucosubstancealthough many gland elements remain. (High irondiamine and alcian blue) x 49.
Fig. 5 Rectal mucosa in Crohn's disease showingmoderate inflammation in lamina propria. There werecharacteristic lesions in submucosa and serosa.(Haematoxylin and eosin) x 36.
infiltrate, and three of these showed moderatedecrease in mucosubstances. In the group withCrohn's disease, although eight biopsies showedsevere and 21 moderate or mild inflammatorychanges in the lamina propria (Figs 5 and 6), themucosubstances were reduced only in two of thebiopsies.
Finally those patients were considered fromwhom two or more biopsies were available atintervals and an attempt made to was correlate theamount of mucosubstance present with the pro-gression, or regression, of the disease as judgedhistologically. It was found that, in general, heal-ing and mucosal regeneration with diminutionof inflammatory reaction, parallel an increase inmucosubstances (Figures 7 and 8).
It will be clear from these findings that mostcases of ulcerative colitis show a decrease inmucosubstance while most cases with Crohn'sdisease do not. Fourteen out of the 91 biopsies,all diagnosed as ulcerative colitis, showed anormal mucosubstance content which on thissupposition was not in keeping with the histo-logical diagnosis. Before regarding these as adefinite negative correlation it was decided toreview both the original biopsies and the opera-tion specimens, since in the laboratory theseparation of large intestinal Crohn's diseasefrom ulcerative colitis was only made with anyconfidence after 1963.Of these 14 cases, three were reclassified as
Crohn's disease, three confirmed as ulcerativecolitis while eight still defied positive identifica-tion, falling into types II and III of Lewin andSwales (1966) in which there are macroscopicRand microscopic features suggestive, but notconclusive, of Crohn's disease. The experience ina considerable number of such cases points toconclusion that where, after considering theclinical history, radiology, and histology of aresected colon, there is still doubt as to whetherthe condition is Crohn's disease or colitis, thedisease will behave as Crohn's disease rather thancolitis. If this be accepted, then the normal muco-substance is in keeping with this opinion.
Discussion
When a patient presents with clinical evidence ofproctitis or colitis, and specific bacterial orprotozoal inflammation can be excluded, thediagnosis usually rests between non-specificproctitis, ulcerative colitis, and Crohn's disease,and then rectal biopsy is often performed toelucidate it. Although there are specific histologicalfeatures which may allow of a definite diagnosis
Fig. 6 Serial section of biopsy in Fig. 5 to shownormal content of mucosubstance. (High irondiamine and alcian blue) x 36.
on October 2, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.11.3.229 on 1 M
arch 1970. Dow
nloaded from

The diagnostic value of mucosubstances in rectal biopsies
*W'
Fig. 7 Rectal mucosa from the same patient as
Fig. 2, biopsy taken three years later. There isconsiderable healing but still some evidence ofactivity. (Haematoxylin and eosin) x 35.
Fig. 8 Serial section of biopsy in Fig. 7. Theregenerated epithelium contains mucosubstances butthere is still a diminution in the zone of active disease.(High iron diamine and alcian blue) x 40.
of Crohn's disease or of ulcerative colitis (Lock-hart-Mummery and Morson, 1960; Janowitzand Present, 1966; Hawk and Turnbull, 1966;Gonzalez-Licea and Yardley, 1966) two prob-lems commonly arise. First the biopsy may
show only 'non-specific inflammation' and thediagnosis remains in doubt; second even whenthe clinical and radiological findings make itclear that the patient suffers either from ulcerativecolitis or from Crohn's disease, the biopsy doesnot always differentiate clearly between them(Lewin and Swales, 1966). Both aspects of thisproblem are being studied but only the second isreported on and discussed here.
Certain definite conclusions can be drawn fromthe observations. In biopsies from patients with
proven ulcerative colitis, if assessment of muco-substances is made in zones free from severeulceration or polypoidal hyperplasia, there is amoderate or marked diminution in sulphated andacid non-sulphated mucosubstances in nearly allcases. This reduction bears a definite relationshipto the degree of inflammatory cellular infiltrationof the lamina propria, but not to the duration ofthe disease. This finding in rectal biopsies issimilar to that described in colectomy specimens(Hellstrom and Fisher, 1967; Greco et al, 1967;Filipe, 1969) and may at first be thought toparallel the observation that rectal involvementis more common in colitis than in Crohn's disease.In this series, however, as in that of Hawk andTurnbull (1966), histologicaLxectal involvementin Crohn's disease; with inflammatory change inthe lamina propria, is common but reduction inmucosubstances is rare, pointing to an essentialand significant difference between the two condi-tions. This difference, though not absolute, is ofconsiderable help in differential diagnosis. Sucha difference is perhaps not surprising sinceulcerative colitis is primarily a diffuse mucosalinflammation, whereas Crohn's disease ofteninvolves the whole thickness of the bowel wallwithout such severe mucosal damage (Morson,1966).The differences in amount and type of muco-
substance seen in the different histologicalpatterns of ulcerative colitis are not sufficient toallow these patterns to be distinguished on histo-chemical grounds alone, but in general it may besaid that in fulminating and acute active cases ofshort duration the decrease in mucosubstances isslight or moderate, and that in chronic activecases it is moderate or severe, and in quiescentcases tends to revert again towards normal. Thesefindings may be of value in assessing the progressof the disease and the effects of medical treatment.When the mucosubstances present were con-
sidered in terms of their neutral, acid non-sulphated, and sulphated content, no loss ofmucosubstance was found to differ sharplybetween sulphated and acid non-sulphated,though in general the mucosubstances whichremained seem to be rather more acid non-sulphated than sulphated. This might be ex-plained by the relative immaturity of newlyformed cells following an alteration in cellularturnover due to damage of the regenerating zonein the fundus of the crypt (Greco et al, 1967).The differences are not sufficiently distinct to beof any diagnostic value.
In conclusion, it is felt that the addition ofinvestigations for mucosubstances to the con-ventional histological assessment on rectalbiopsies helps materially in the distinction ofulcerative colitis, in which mucosubstances aremarkedlyreduced, from Crohn's disease, in whichthey are present in normal or slightly reducedamounts. This distinction remains in the presenceof marked inflammation of the lamina propriaand equivocal histology. Current studies on the
233 on O
ctober 2, 2020 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.11.3.229 on 1 March 1970. D
ownloaded from

234 M. L Filipe and Ian Dawson
mucosubstances in non-specific proctitis may helpfurther in the differential diagnosis of procto-colitis on rectal biopsy.
Our thanks are due to the surgical staff of the GordonHospital, Westminster Group, under whose care thepatients were, to Miss Jean Sowden for technicalassistance, to the Photographic Department of West-minster Medical School for the finished prints, and toMiss Jill Ashby for secretarial help. One of us (M.I.F.)was in receipt of a grant from the British EmpireCancer Campaign which we gratefully acknowledge.
References
Dawson, I. M. P., and Pryse-Davies, J. (1959). The developmentof carcinoma of the large intestine in ulcerative colitis.Brit. J. Surg., 47, 113-128.
Filipe, M. I. (1968). Some aspects of the histochemical enzymedistribution in colon and rectum. Normal and pathological.In Symposium for Histochemistry, Hamburg, September1968.
Filipe, M. I. (1969). Value of histochemical reactions for muco-substances in the diagnosis of certain pathological condi-tions of the colon and rectum. Gut, 10, 577-586.
Gonzalez-Licea, A., and Yardley, J. H. (1966). Nature of thetissue reaction in ulcerative colitis. Light and electronmicroscopic findings. Gastroenterology, 51, 825-840.
Gottschalk, A. (1962). The relation between structure and functionin some glycoproteins. Perspect. Biol. Med., 5, 327-337.
Greco, V., Lauro, G., Fabbrini, A., and Torsoli, A. (1967).Histochemistry of the colonic epithelial mucins in normalsubjects and in patients with ulcerative colitis. A qualitativeand histophotometric investigation. Gut, 8, 491-496.
Hawk, W. A., and Turnbull, R. B., Jr. (1966). Primary ulcerativedisease of the colon. Gastroenterology, 51, 802-805.
Helistrom, H. R., and Fisher, E. R. (1967). Estimation of mucosalmucin as an aid in the differentiation of Crohn's diseaseof the colon and chronic ulcerative colitis. Amer. J. clin.Path., 48, 259-268.
Janowitz, H. D., and Present, D. H. (1966). Granulomatouscolitis: pathogenic concepts. Gastroenterology, 51, 778-787.
Jeanloz, R. W. (1960). The nomenclature of mucopolysaccharides.Arthr. and Rheum., 3, 233-237.
Jeanloz, R. W. (1963). Recent developments in the biochemistryof amino sugars. Advanc. Enzymol., 25, 433-456.
Lewin, K., and Swales, J. D. (1966). Granulomatous colitis andatypical ulcerative colitis. Histological features, behaviour,and prognosis. Gastroenterology, 50, 211-223.
Lockhart-Mummery, H. E., and Morson, B. C. (1960). Crohn'sdisease (regional enteritis) of the large intestine and itsdistinction from ulcerative colitis. Gut, 1, 87-105.
Matts, S. G. F. (1961). The value of rectal biopsy in the diagnosisof ulcerative colitis. Quart. J. Med., 30, 393-407.
Melnyk, C. S., Braucher, R. E., and Kirsner, J. B. (1967).Regeneration of the human colon mucosa. Morphologicaland histochemical study. Gastroenterology, 52, 985 997.
Monis, B., and Mendeloff, A. I. (1965). Studies in ulcerativecolitis: TPN-linked dehydrogenases and nonspecificesterases in rectal biopsy specimens. Gastroenterology, 48,173-184.
Morson, B. C. (1966). Discussion to Symposium-Newer bio-logical concepts in ulcerative colitis and related diseases.Gastroenterology, 51, 807-808.
Mowry, R. W., and Morard, J. C. (1957). The distribution of acidmucopolysaccharides in normal kidneys, as shown by thealcian blue-Feulgen (AB-F) and alcian blue-periodic acid-Schiff (AB-PAS) stains. (Abstract.) Amer. J. Path., 33,620 621.
Van Noorden, S., Thayer, W. R. Jr, Yesner, R., and Spiro, H. M.(1967). Some histochemical studies on intestinal epitheliumwith particular reference to ulcerative colitis and otherinflammatory cond;tions. J. Path. Bact., 94, 13-18.
Spicer, S. S. (1965). Diamine methods for differentiating muco-substances histochemically. J. Histochem. Cytochem., 13,211-234.
Spicer, S. S., Leppi, T. J., and Stoward, P. J. (1965). Suggestionsfor a histochemical terminology of carbohydrate-rich tissuecomponents. J. Histochem. Cytochem, 13, 599-603.
on October 2, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.11.3.229 on 1 M
arch 1970. Dow
nloaded from