The Movement Disorders Society criteria for the diagnosis of Parkinson’s disease dementia: their...
11
ORIGINAL COMMUNICATION The Movement Disorders Society criteria for the diagnosis of Parkinson’s disease dementia: their usefulness and limitations in elderly patients Miche `le Kiesmann • Jean-Baptiste Chanson • Julien Godet • Thomas Vogel • Laetitia Schweiger • Saı ¨d Chayer • Georges Kaltenbach Received: 25 March 2013 / Revised: 5 June 2013 / Accepted: 20 June 2013 Ó Springer-Verlag Berlin Heidelberg 2013 Abstract The aim of this study was to assess the per- formance of the Movement Disorders Society (MDS) cri- teria for the diagnosis of Parkinson’s disease dementia (PDD) in the elderly, and also to evaluate the relevance of applying other tests in this patient population. The MDS criteria include a first short part in checklist form, and a second part which is used as a basis for reference and consists of an in-depth neuropsychological examination. Forty consecutive PD patients presenting with cognitive complaints were enrolled. An assessment was made of the performances of the MDS checklist compared with the MDS exhaustive cognitive examination which was used as a basis for reference, and with other cognitive tests including the Mattis Dementia Rating Scale (MDRS), the French version of the Grober and Buschke test, the verbal fluency test, the Rey–Osterreith complex figure and the paced auditory serial addition test. Out of a total of 40 PD subjects (mean age: 80.5 ± 4.9 years), 20 were diagnosed with PDD according to the checklist and 31 on the basis of the exhaustive examination, i.e. with 11 more patients diagnosed via the latter. The sensitivity of the checklist for the diagnosis of PDD was 0.64, with a specificity of 1.00. The use of the MDRS for PDD diagnosis with a cut-off at B120 showed a sensitivity of 0.80 and a specificity of 1.00, while at B132 it displayed a sensitivity of 1.00 and a specificity of 0.444. The specificity of the checklist for the diagnosis of PDD in the elderly was confirmed, but it was lacking in sensitivity. It was also found that the MDRS could be helpful in the diagnosis and screening of PDD. Keywords Parkinson’s disease Dementia Cognitive disorder Memory Elderly Introduction Parkinson’s disease (PD) has been reported to affect more than 1 % of elderly patients over the age of 65 years, and 2.6 % of those between 85 and 89 years [1]. Some studies [2–5] have found that between 22 and 48 % of the patients with PD have cognitive disorders, and that Parkinson’s disease dementia (PDD) may develop in up to 80 % of surviving PD patients after 20 years [6–8]. It is considered that 3 to 4 % of cases of dementia are due to PDD in the general population, and that 32 % of all subjects with PD have dementia [5]. Factors associated with PDD include psychiatric disorders, advanced age, excessive daytime somnolence, falls, urinary incontinence, moderate dysar- thria and severely impaired motor function [8]. PDD is basically distinguished from Lewy body dementia by the chronology of clinical events, and from Alzheimer’s dis- ease by the neuropsychological profile at the onset of the disease [9]. The cognitive disorders in PD patients pre- dominate in regard to executive and visuo-spatial M. Kiesmann (&) T. Vogel L. Schweiger G. Kaltenbach Department of Geriatrics, Robertsau Hospital, Strasbourg University Hospitals, 83 rue Himmerich, Strasbourg 67091, France e-mail: [email protected] J.-B. Chanson Department of Neurology, Hautepierre Hospital, Strasbourg University Hospitals, Strasbourg, France J. Godet Department of Public Health, Biostatistics and Methodology Sector, Strasbourg University Hospitals, Strasbourg, France S. Chayer Department of Clinical Research, Civil Hospital, Strasbourg University Hospitals, Strasbourg, France 123 J Neurol DOI 10.1007/s00415-013-7018-8
-
Upload
thomas-vogel -
Category
Documents
-
view
215 -
download
0
Transcript of The Movement Disorders Society criteria for the diagnosis of Parkinson’s disease dementia: their...

ORIGINAL COMMUNICATION
The Movement Disorders Society criteria for the diagnosisof Parkinson’s disease dementia: their usefulness and limitationsin elderly patients
Michele Kiesmann • Jean-Baptiste Chanson •
Julien Godet • Thomas Vogel • Laetitia Schweiger •
Saıd Chayer • Georges Kaltenbach
Received: 25 March 2013 / Revised: 5 June 2013 / Accepted: 20 June 2013
� Springer-Verlag Berlin Heidelberg 2013
Abstract The aim of this study was to assess the per-
formance of the Movement Disorders Society (MDS) cri-
teria for the diagnosis of Parkinson’s disease dementia
(PDD) in the elderly, and also to evaluate the relevance of
applying other tests in this patient population. The MDS
criteria include a first short part in checklist form, and a
second part which is used as a basis for reference and
consists of an in-depth neuropsychological examination.
Forty consecutive PD patients presenting with cognitive
complaints were enrolled. An assessment was made of the
performances of the MDS checklist compared with the
MDS exhaustive cognitive examination which was used as
a basis for reference, and with other cognitive tests
including the Mattis Dementia Rating Scale (MDRS), the
French version of the Grober and Buschke test, the verbal
fluency test, the Rey–Osterreith complex figure and the
paced auditory serial addition test. Out of a total of 40 PD
subjects (mean age: 80.5 ± 4.9 years), 20 were diagnosed
with PDD according to the checklist and 31 on the basis of
the exhaustive examination, i.e. with 11 more patients
diagnosed via the latter. The sensitivity of the checklist for
the diagnosis of PDD was 0.64, with a specificity of 1.00.
The use of the MDRS for PDD diagnosis with a cut-off at
B120 showed a sensitivity of 0.80 and a specificity of 1.00,
while at B132 it displayed a sensitivity of 1.00 and a
specificity of 0.444. The specificity of the checklist for the
diagnosis of PDD in the elderly was confirmed, but it was
lacking in sensitivity. It was also found that the MDRS
could be helpful in the diagnosis and screening of PDD.
Keywords Parkinson’s disease � Dementia � Cognitive
disorder � Memory � Elderly
Introduction
Parkinson’s disease (PD) has been reported to affect more
than 1 % of elderly patients over the age of 65 years, and
2.6 % of those between 85 and 89 years [1]. Some studies
[2–5] have found that between 22 and 48 % of the patients
with PD have cognitive disorders, and that Parkinson’s
disease dementia (PDD) may develop in up to 80 % of
surviving PD patients after 20 years [6–8]. It is considered
that 3 to 4 % of cases of dementia are due to PDD in the
general population, and that 32 % of all subjects with PD
have dementia [5]. Factors associated with PDD include
psychiatric disorders, advanced age, excessive daytime
somnolence, falls, urinary incontinence, moderate dysar-
thria and severely impaired motor function [8]. PDD is
basically distinguished from Lewy body dementia by the
chronology of clinical events, and from Alzheimer’s dis-
ease by the neuropsychological profile at the onset of the
disease [9]. The cognitive disorders in PD patients pre-
dominate in regard to executive and visuo-spatial
M. Kiesmann (&) � T. Vogel � L. Schweiger � G. Kaltenbach
Department of Geriatrics, Robertsau Hospital, Strasbourg
University Hospitals, 83 rue Himmerich, Strasbourg 67091,
France
e-mail: [email protected]
J.-B. Chanson
Department of Neurology, Hautepierre Hospital,
Strasbourg University Hospitals, Strasbourg, France
J. Godet
Department of Public Health, Biostatistics and Methodology
Sector, Strasbourg University Hospitals, Strasbourg, France
S. Chayer
Department of Clinical Research, Civil Hospital, Strasbourg
University Hospitals, Strasbourg, France
123
J Neurol
DOI 10.1007/s00415-013-7018-8

functions. In their mild form, they may be detected only in
the course of specialized assessment; when they are severe,
they are overtly expressed in the form of attention disor-
ders. New diagnostic criteria for PDD have been proposed
by the Movement Disorders Society (MDS) [10], and are
divided into several parts including a preliminary simpli-
fied checklist [11]. Elderly PD patients have not been
specifically studied until now, although they have a high
risk of developing PDD.
In this study, an investigation of cognitive functions was
carried out in elderly PD patients with cognitive complaints
who were under standard medical care, and who had a
degree of cognitive impairment that affected their daily
lives. The main aim was to assess the performance of the
MDS criteria including the shortened checklist and the
exhaustive reference examination for the diagnosis of
PDD, and to compare these tools with other cognitive tests.
Patients and methods
Patients
PD patients with cognitive complaints who had attended the
Strasbourg geriatric center for a fixed period of 2 years were
selected for potential inclusion in the study. The inclusion
criteria were as follows: patient age C65 years, PD diag-
nosed according to the United Kingdom Parkinson’s Disease
Society Brain Bank (UKPDSBB) criteria [12], and stable
motor function. Eligible patients had to complain of cogni-
tive disorders which had direct consequences on their
everyday activities, as it has been found that the incidence of
objective cognitive decline appears to be significantly higher
in subjects with subjective complaints [13]. To ensure that
the cognitive deficits would in all probability lead to prob-
lems in activities of daily living (ADL), a clinical dementia
rating scale (CDR) [14–16] score[0.5 was required as part
of the inclusion criteria, also taking into account the fact that
reduced mobility interferes with ADL especially in the
elderly. The CDR scale is based on a comparison between the
patients’ capacities before and after the onset of the disease
with the aid of a referent. The mini-mental state examination
(MMSE) [17] score had to amount to [16 to ensure the
exclusion of patients with overly severe cognitive disorders.
However, the inclusion of patients subject to hallucinations
without significant emotional impact was permitted, as was a
case of PD-associated psychosis treated with low-dose
atypical neuroleptics. Biological analyses (blood cell count
and measurement of urea, creatinine, electrolytes, proteins,
TSH and vitamin B12 in the serum) as well as brain imaging
(CT scan or MRI) were respectively carried out within 6 and
12 months prior to entry into the study to rule out any
alternative diagnosis for dementia.
The exclusion criteria included the lack of impact of
cognitive impairment on the patients’ ADL, exclusion
criteria for PD according to the UKPDSBB, dementia due
to a cause other than PD, delirium that had occurred
\3 months before study inclusion, severe depressive syn-
drome accounting for the disorders observed, previous
major stroke, anticholinergic treatment, lack of feasibility
for carrying out the tests that were part of the study, or the
impossibility to provide the patient with detailed infor-
mation about the study.
All the patients were recruited from the Strasbourg
University Hospitals’ geriatric center by a neurologist with
experience in the field of PD and dementia, and a geria-
trician. The study was approved of by the Strasbourg
University Hospitals’ scientific committee and the local
ethics committee. It was then registered with the advisory
committee on the treatment of research information in the
health sector under No. IDRCB.2010-A00113-36, and also
with Clinical Trials. Gov. under No. NCT01113242.
Informed consent was obtained from all the patients prior
to their inclusion in the study.
Methods
The preliminary selection of potentially eligible subjects
was carried out by an experienced neurologist (MK), and
included the following: a physical and neurological
examination, application of the diagnostic criteria for PD
data collection on PD-specific characteristics, medical
history, treatments, and the results of biological analyses
and brain imaging. The patient was orally informed about
the study protocol at the time he or she was given the
informed consent form and information notice. The CDR
scale, which was scored out of five, and the geriatric
depression scale (GDS) [18, 19], which was scored out of
30, were both applied. Patients who had obtained a score
C22 on the GDS were excluded from the study, as this
score over-corresponded to a state of severe depression,
which could have interfered with the diagnosis of PDD.
The MMSE, scored out of 30, was also performed. Cog-
nitive assessment included literal verbal fluency over 2 min
for the letter P to evaluate executive function [20, 21], and
is included among the eight items on the MDS checklist.
The 2-min time frame was specifically chosen as it was
better adapted to the advanced age of the study subjects
who tended to react more slowly than younger individuals.
Following this pre-selection phase, the definitive patient
selection took place 2 weeks later: study inclusion was
determined by the neurologist who received the dated and
signed informed consent form, plus information on the
patient’s educational background from the age of 6 years.
The Hoehn and Yahr rating scale (H&Y) [22] was then
applied, scored out of five; while the instrumental activities
J Neurol
123

of daily living (IADL) were evaluated for the patient’s
capacity to use the telephone, means of public transport,
organize the budget and manage medicinal drug intake,
with a maximum score of 37 for these particular items,
which are more useful indicators than basic everyday
activities [23]. The Pill questionnaire was not used due to
the high proportion of institutionalized subjects in this
study population. The assessment based on the Unified
Parkinson’s Disease Rating Scale score for Part III, motor
function [24], was only partial and focused on an evalua-
tion of the rigidity of the neck and the upper and lower
limbs, right and left hand finger tapping tested separately
and the patient’s ability to get up from a chair, with a
maximum score of 32. Cognitive assessment, which was
adapted to the evaluation of PD-associated cognitive dis-
orders, included the Mattis Dementia Rating Scale
(MDRS) [25, 26], scored out of 144, an instrument for the
assessment of impaired executive function and in particular
for the evaluation of PD-associated cognitive disorders [27,
28]. The global score is considered to be normal if it
reaches [136/144 on the MDS; a copy of the Rey–Oster-
reith Complex Figure (ROCF), scored out of 36, was also
used for the assessment of visuo-constructive capacity [29].
A follow-up visit took place 2 weeks later with a neu-
ropsychologist, and included the French version of Grober
and Buschke’s 16-item Free and Cued Selective Remind-
ing Test with immediate recall (FCSRT–IR) [30]. This test
is used for assessing immediate recall (IR) capacity: in all,
three free recalls (FR) out of 48, three cued recalls (CR),
and the sum of three total recalls (TR) out of 48, with the
calculation of the number of off-list intrusions for the
exploration of recent episodic memory. Total FR is fre-
quently altered in PD patients, while cue-induced memory
is rarely affected. The Paced Auditory Serial Addition Test
in 4 s (PASAT) [31] was used for the evaluation of
attention capacity and executive function, thereby com-
pleting the cognitive assessment. The modified French
version of this test of the capacity for sustained attention
was used [32], and the result expressed in the number of
positive responses out of 60.
The values obtained for the different tests used were
expressed in percentiles (pc) of the normal population
adapted for age and educational level. A value within the
worst 10 pc for the reference population was considered
abnormal. The MDS criteria were applied by a neurologist
(JBC) who had not performed any previous assessment in
this study in order to differentiate between the two groups,
i.e. patients likely to have PDD and those with a probable
absence of PDD.
In this study, the final diagnosis of PDD was based on an
exhaustive cognitive assessment. This evaluation included
the testing of those cognitive functions that are more fre-
quently associated with PDD, as recommended by the MDS
[10]. PDD was diagnosed if abnormal results were observed
for at least two of the following functions or domains:
memory, executive functions, visuo-spatial capacities, and
attention. Memory impairment was defined by abnormal
results in either the total FR sub-score of the FCSRT–IR, or
the MDRS memory subtest. Executive functions were
considered impaired if at least two tests were abnormal
among the MDRS overall score, the verbal fluency score
and the PASAT score. Impairment of visuo-spatial capacity
was determined if either the copy of the ROCF or the
MDRS subtest for visuo-constructive function was abnor-
mal. Attention deficit was defined by abnormal results in at
least one of the following: the MDRS attention subtest, the
IR of the FCSRT–IR, or fluctuations of attention determined
by variability in performance over time in the different tasks
involving attention, independently of motor function fluc-
tuations. The classification into normal and abnormal was
carried out by the same neurologist (JBC), based on the
results of the cognitive tests, classified by domains.
The patients likely to have PDD as determined by the
MDS checklist met all the following criteria: diagnosis of
PD established before the development of cognitive defi-
cits, MMSE score\26, impact on the IADL (i.e. an IADL
score[5), at least two errors amongst the MMSE attention
sub-scores or the seven backwards test with two incorrect
replies; negative results for the visuo-construction test with
failed copy of pentagons; for memory, FR for three words
considered altered if one word was forgotten, and executive
function impairment determined via literal fluency for the
letter P over 2 min if the result was within the worst 10 pc.
Absence of major depression, absence of delirium and
absence of other abnormalities that could obscure diagnosis
completed the rating sheet for probable PDD. However, the
presence of apathy, depressed mood, delusions or excessive
daytime sleepiness could also be indicative of a diagnosis
of probable PDD insofar as application of the MDS criteria
for PDD diagnosis were concerned.
Statistical analysis
All statistical analyses were performed using R statistical
software (version 2.15.1 http://www.R-project.org/). PDD
and PD patients’ characteristics were compared using non-
parametric tests. The Kruskal–Wallis or the Mann–Whit-
ney test was used where appropriate to compare continuous
variables. Fisher’s exact test was performed on nominal
variables. Sensitivity, specificity, positive (PPV) and neg-
ative predictive values (NPV) and area under the receiver
operating characteristic (ROC) curve were determined
using the caret (version 5.15-048) and ROC (version 1.0-4)
R packages from the Comprehensive R Archive Network
repository. The level of statistical significance was set at
5 %.
J Neurol
123
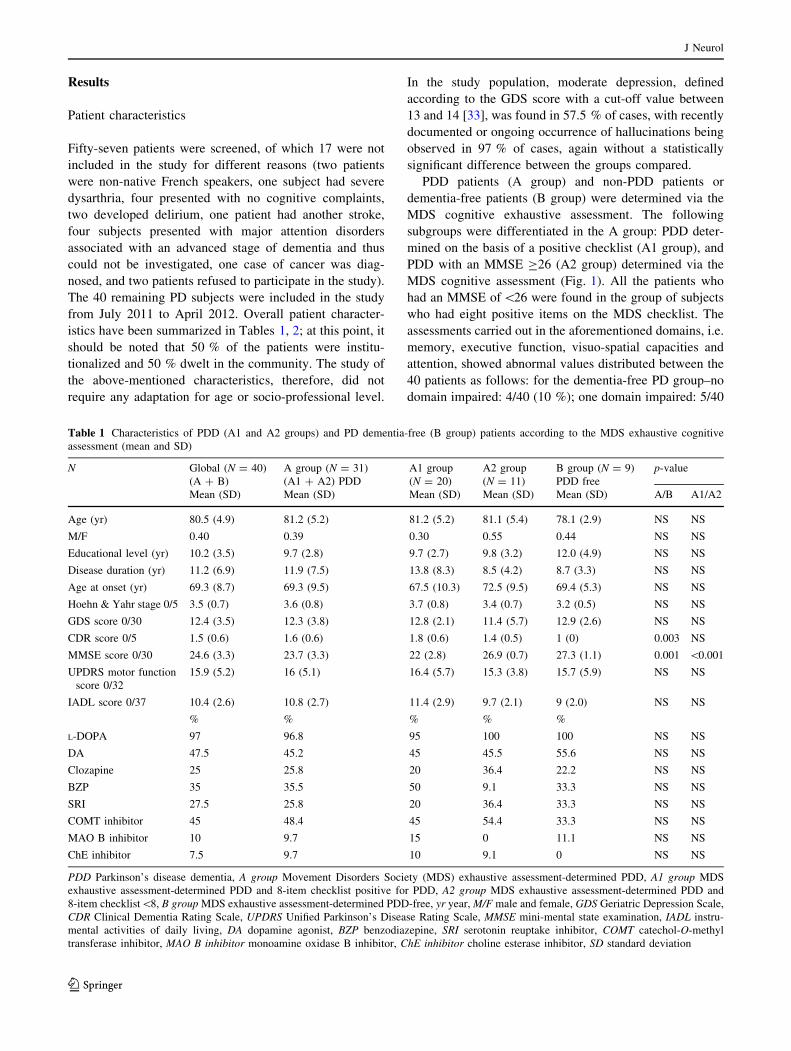
Results
Patient characteristics
Fifty-seven patients were screened, of which 17 were not
included in the study for different reasons (two patients
were non-native French speakers, one subject had severe
dysarthria, four presented with no cognitive complaints,
two developed delirium, one patient had another stroke,
four subjects presented with major attention disorders
associated with an advanced stage of dementia and thus
could not be investigated, one case of cancer was diag-
nosed, and two patients refused to participate in the study).
The 40 remaining PD subjects were included in the study
from July 2011 to April 2012. Overall patient character-
istics have been summarized in Tables 1, 2; at this point, it
should be noted that 50 % of the patients were institu-
tionalized and 50 % dwelt in the community. The study of
the above-mentioned characteristics, therefore, did not
require any adaptation for age or socio-professional level.
In the study population, moderate depression, defined
according to the GDS score with a cut-off value between
13 and 14 [33], was found in 57.5 % of cases, with recently
documented or ongoing occurrence of hallucinations being
observed in 97 % of cases, again without a statistically
significant difference between the groups compared.
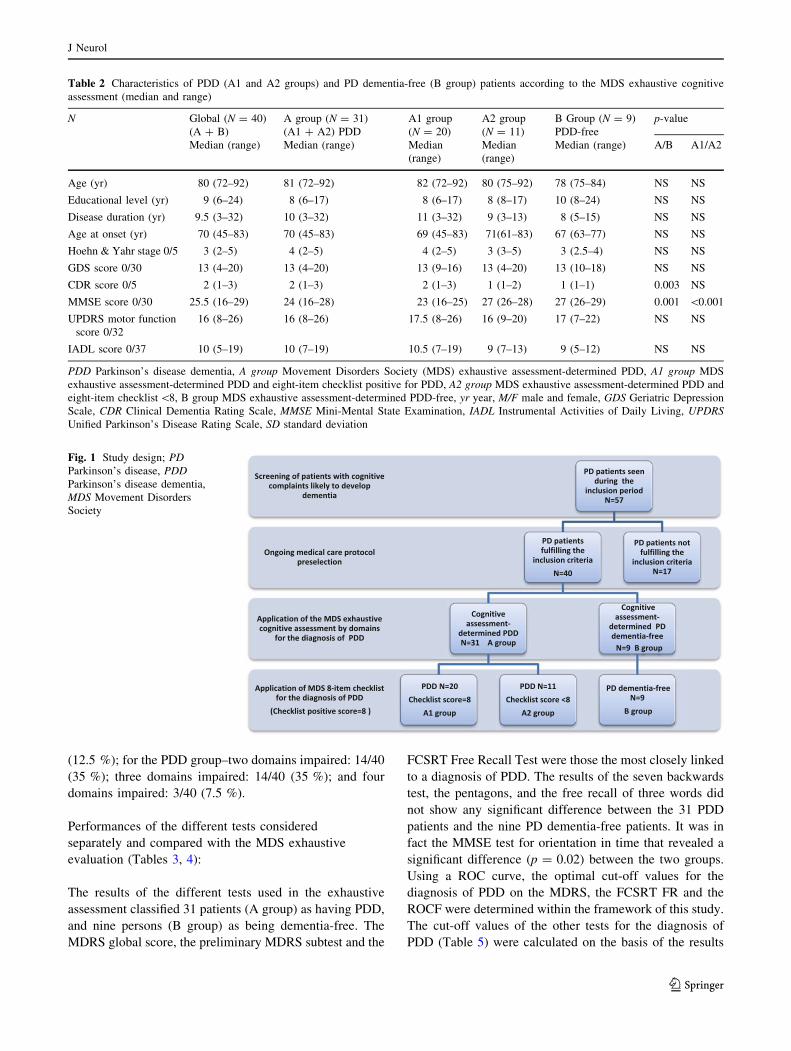
PDD patients (A group) and non-PDD patients or
dementia-free patients (B group) were determined via the
MDS cognitive exhaustive assessment. The following
subgroups were differentiated in the A group: PDD deter-
mined on the basis of a positive checklist (A1 group), and
PDD with an MMSE C26 (A2 group) determined via the
MDS cognitive assessment (Fig. 1). All the patients who
had an MMSE of\26 were found in the group of subjects
who had eight positive items on the MDS checklist. The
assessments carried out in the aforementioned domains, i.e.
memory, executive function, visuo-spatial capacities and
attention, showed abnormal values distributed between the
40 patients as follows: for the dementia-free PD group–no
domain impaired: 4/40 (10 %); one domain impaired: 5/40
Table 1 Characteristics of PDD (A1 and A2 groups) and PD dementia-free (B group) patients according to the MDS exhaustive cognitive
assessment (mean and SD)
N Global (N = 40)
(A ? B)
A group (N = 31)
(A1 ? A2) PDD
A1 group
(N = 20)
A2 group
(N = 11)
B group (N = 9)
PDD free
p-value
Mean (SD) Mean (SD) Mean (SD) Mean (SD) Mean (SD) A/B A1/A2
Age (yr) 80.5 (4.9) 81.2 (5.2) 81.2 (5.2) 81.1 (5.4) 78.1 (2.9) NS NS
M/F 0.40 0.39 0.30 0.55 0.44 NS NS
Educational level (yr) 10.2 (3.5) 9.7 (2.8) 9.7 (2.7) 9.8 (3.2) 12.0 (4.9) NS NS
Disease duration (yr) 11.2 (6.9) 11.9 (7.5) 13.8 (8.3) 8.5 (4.2) 8.7 (3.3) NS NS
Age at onset (yr) 69.3 (8.7) 69.3 (9.5) 67.5 (10.3) 72.5 (9.5) 69.4 (5.3) NS NS
Hoehn & Yahr stage 0/5 3.5 (0.7) 3.6 (0.8) 3.7 (0.8) 3.4 (0.7) 3.2 (0.5) NS NS
GDS score 0/30 12.4 (3.5) 12.3 (3.8) 12.8 (2.1) 11.4 (5.7) 12.9 (2.6) NS NS
CDR score 0/5 1.5 (0.6) 1.6 (0.6) 1.8 (0.6) 1.4 (0.5) 1 (0) 0.003 NS
MMSE score 0/30 24.6 (3.3) 23.7 (3.3) 22 (2.8) 26.9 (0.7) 27.3 (1.1) 0.001 \0.001
UPDRS motor function
score 0/32
15.9 (5.2) 16 (5.1) 16.4 (5.7) 15.3 (3.8) 15.7 (5.9) NS NS
IADL score 0/37 10.4 (2.6) 10.8 (2.7) 11.4 (2.9) 9.7 (2.1) 9 (2.0) NS NS
% % % % %
L-DOPA 97 96.8 95 100 100 NS NS
DA 47.5 45.2 45 45.5 55.6 NS NS
Clozapine 25 25.8 20 36.4 22.2 NS NS
BZP 35 35.5 50 9.1 33.3 NS NS
SRI 27.5 25.8 20 36.4 33.3 NS NS
COMT inhibitor 45 48.4 45 54.4 33.3 NS NS
MAO B inhibitor 10 9.7 15 0 11.1 NS NS
ChE inhibitor 7.5 9.7 10 9.1 0 NS NS
PDD Parkinson’s disease dementia, A group Movement Disorders Society (MDS) exhaustive assessment-determined PDD, A1 group MDS
exhaustive assessment-determined PDD and 8-item checklist positive for PDD, A2 group MDS exhaustive assessment-determined PDD and
8-item checklist\8, B group MDS exhaustive assessment-determined PDD-free, yr year, M/F male and female, GDS Geriatric Depression Scale,
CDR Clinical Dementia Rating Scale, UPDRS Unified Parkinson’s Disease Rating Scale, MMSE mini-mental state examination, IADL instru-
mental activities of daily living, DA dopamine agonist, BZP benzodiazepine, SRI serotonin reuptake inhibitor, COMT catechol-O-methyl
transferase inhibitor, MAO B inhibitor monoamine oxidase B inhibitor, ChE inhibitor choline esterase inhibitor, SD standard deviation
J Neurol
123
(12.5 %); for the PDD group–two domains impaired: 14/40
(35 %); three domains impaired: 14/40 (35 %); and four
domains impaired: 3/40 (7.5 %).
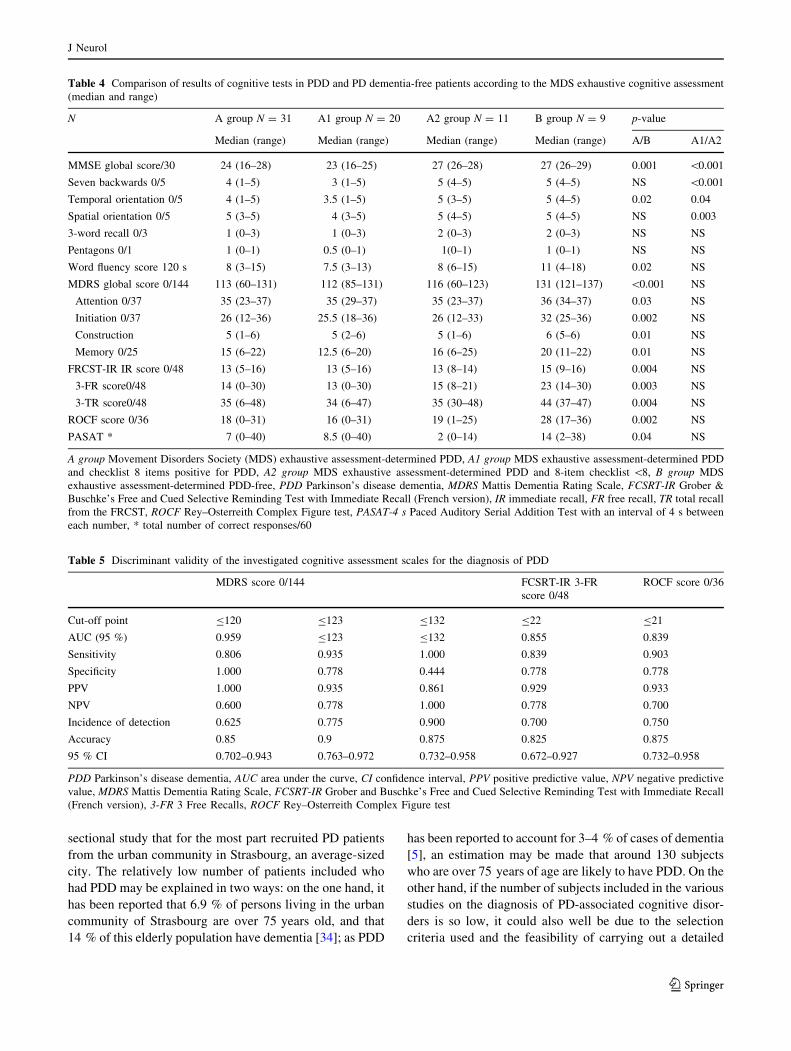
Performances of the different tests considered
separately and compared with the MDS exhaustive
evaluation (Tables 3, 4):
The results of the different tests used in the exhaustive
assessment classified 31 patients (A group) as having PDD,
and nine persons (B group) as being dementia-free. The
MDRS global score, the preliminary MDRS subtest and the
FCSRT Free Recall Test were those the most closely linked
to a diagnosis of PDD. The results of the seven backwards
test, the pentagons, and the free recall of three words did
not show any significant difference between the 31 PDD
patients and the nine PD dementia-free patients. It was in
fact the MMSE test for orientation in time that revealed a
significant difference (p = 0.02) between the two groups.
Using a ROC curve, the optimal cut-off values for the
diagnosis of PDD on the MDRS, the FCSRT FR and the
ROCF were determined within the framework of this study.
The cut-off values of the other tests for the diagnosis of
PDD (Table 5) were calculated on the basis of the results
Table 2 Characteristics of PDD (A1 and A2 groups) and PD dementia-free (B group) patients according to the MDS exhaustive cognitive
assessment (median and range)
N Global (N = 40)
(A ? B)
A group (N = 31)
(A1 ? A2) PDD
A1 group
(N = 20)
A2 group
(N = 11)
B Group (N = 9)
PDD-free
p-value
Median (range) Median (range) Median
(range)
Median
(range)
Median (range) A/B A1/A2
Age (yr) 80 (72–92) 81 (72–92) 82 (72–92) 80 (75–92) 78 (75–84) NS NS
Educational level (yr) 9 (6–24) 8 (6–17) 8 (6–17) 8 (8–17) 10 (8–24) NS NS
Disease duration (yr) 9.5 (3–32) 10 (3–32) 11 (3–32) 9 (3–13) 8 (5–15) NS NS
Age at onset (yr) 70 (45–83) 70 (45–83) 69 (45–83) 71(61–83) 67 (63–77) NS NS
Hoehn & Yahr stage 0/5 3 (2–5) 4 (2–5) 4 (2–5) 3 (3–5) 3 (2.5–4) NS NS
GDS score 0/30 13 (4–20) 13 (4–20) 13 (9–16) 13 (4–20) 13 (10–18) NS NS
CDR score 0/5 2 (1–3) 2 (1–3) 2 (1–3) 1 (1–2) 1 (1–1) 0.003 NS
MMSE score 0/30 25.5 (16–29) 24 (16–28) 23 (16–25) 27 (26–28) 27 (26–29) 0.001 \0.001
UPDRS motor function
score 0/32
16 (8–26) 16 (8–26) 17.5 (8–26) 16 (9–20) 17 (7–22) NS NS
IADL score 0/37 10 (5–19) 10 (7–19) 10.5 (7–19) 9 (7–13) 9 (5–12) NS NS
PDD Parkinson’s disease dementia, A group Movement Disorders Society (MDS) exhaustive assessment-determined PDD, A1 group MDS
exhaustive assessment-determined PDD and eight-item checklist positive for PDD, A2 group MDS exhaustive assessment-determined PDD and
eight-item checklist \8, B group MDS exhaustive assessment-determined PDD-free, yr year, M/F male and female, GDS Geriatric Depression
Scale, CDR Clinical Dementia Rating Scale, MMSE Mini-Mental State Examination, IADL Instrumental Activities of Daily Living, UPDRS
Unified Parkinson’s Disease Rating Scale, SD standard deviation
Fig. 1 Study design; PD
Parkinson’s disease, PDD
Parkinson’s disease dementia,
MDS Movement Disorders
Society
J Neurol
123

obtained via the reference list established according to
MDS criteria, i.e. the exhaustive cognitive assessment
(Table 5).
MDS checklist performance for the diagnosis of PDD
compared with the MDS exhaustive evaluation:
All the patients who met the diagnostic criteria for PDD
according to the MDS checklist had an MMSE score of
\26 (A1 group), while all the remaining subjects (A2 and
B groups) had an MMSE score C26. The application of the
MDS checklist resulted in a diagnosis of dementia in 20
patients, i.e. in 50 % of the study population. No between-
group difference was found for the characteristics exam-
ined, and no readjustment for age or educational level was
required. The extremely low p-values for the CDR scale
and the MMSE, the seven backwards test and the verbal
fluency test were explained by the fact that these were
selection criteria. Variables such as the global score on the
MDRS, the MDRS memory test, the ROCF and the 16-item
free and cued recall test were the most determinant in
differentiating between the MDS checklist-positive group
(A1 group) and the other PDD subjects with an MMSE
C26 (A2 group) based on the results of the MDS
exhaustive cognitive assessment. The specificity of the
checklist compared with that of the exhaustive evaluation
was 1, and its sensitivity amounted to 0.645. The accuracy
was 0.725, with a 95 % CI (0.561, 0.854), positive pre-
dictive value (PPV) of 1, negative predictive value (NPV)
0.450, and prevalence 0.775.
The characteristics of the patients who fulfilled either
the checklist criteria or those of the exhaustive evaluation
recommended by the MDS were compared. The compari-
son between the checklist–positive dementia group
(n = 20) or the A1 group and the PDD subgroup with an
MMSE C26 identified via the exhaustive assessment
(n = 11) or the A2 group showed that the item, orientation
in space, scored on the MMSE was significantly associated
with the diagnosis of PDD via the checklist, with a p value
of 0.0033.
Discussion
To the authors’ knowledge, this is the first study to apply the
MDS criteria for the diagnosis of PDD to a patient popu-
lation of such an advanced age using a detailed method of
cognitive assessment. This was a monocentric cross-
Table 3 Comparison of results of cognitive tests in PDD and PD dementia-free patients according to the MDS exhaustive cognitive assessment
(mean and SD)
N A Group N = 31 A1 group N = 20 A2 group N = 11 B group N = 9 p-value
Mean (SD) Mean (SD) Mean (SD) Mean (SD) A/B A1/A2
MMSE global score/30 23.7 (3.3) 22 (2.8) 26.9 (0.7) 27.3 (1.1) 0.001 \0.001
Seven backwards 0/5 3.5 (1.5) 2.8 (1.5) 4.8 (0.4) 4.6 (0.5) NS \0.001
Temporal orientation0/5 3.8 (1.2) 3.5 (1.3) 4.5 (0.7) 4.8 (0.4) 0.02 0.04
Spatial orientation 0/5 4.4 (0.8) 4.1 (0.8) 4.9 (0.3) 4.7 (0.5) NS 0.003
3-word recall 0/3 1.5 (1.4) 1.4 (1.7) 1.7 (0.9) 2 (1.0) NS NS
Pentagons 0/1 0.8 (1.4) 0.8 (1.8) 0.8 (0.4) 0.9 (0.3) NS NS
Word fluency score 120 s 7.7 (3) 7 (2.9) 8.9 (2.9) 10.8 (3.9) 0.02 NS
MDRS global score 0/144 110.5 (13.7) 109.9 (11.2) 111.17 (18.0) 130.1 (5.6) \0.001 NS
Attention 0/37 34.1 (2.9) 34.1 (2.3) 34 (3.9) 35.9 (1.2) 0.03 NS
Initiation 0/37 25.6 (5.1) 26.1 (5.0) 24.8 (5.4) 32 (3.6) 0.002 NS
Construction 0/6 4.6 (1.3) 4.6 (1.1) 4.6 (1.6) 5.7 (0.5) 0.01 NS
Memory 0/25 14.5 (5.5) 12.9 (4.5) 17.2 (6.3) 18.8 (4.0) 0.01 NS
FRCST-IR IR score 0/48 12.2 (2.4) 12.2 (2.8) 12.1 (1.6) 14.6 (2.2) 0.004 NS
3-FR score0/48 13.8 (6.9) 13.1 (8.0) 15.1 (3.9) 22.9 (5.6) 0.003 NS
3-TR score0/48 33.3 (10.4) 31.2 (11.8) 37 (6.0) 43.3 (3.4) 0.004 NS
ROCF score 0/36 16.3 (7.4) 15.7 (7.7) 17.4 (6.9) 27.2 (6.6) 0.002 NS
PASAT* 7.9 (8.9) 9.7 (10.1) 4.6 (5.2) 16.9 (12.8) 0.04 NS
A group Movement Disorders Society (MDS) exhaustive assessment-determined PDD, A1 group MDS exhaustive assessment-determined PDD
and eight-item checklist positive for PDD, A2 group MDS exhaustive assessment-determined PDD and 8-item checklist \8, B group MDS
exhaustive assessment-determined PD dementia-free, PDD Parkinson’s disease dementia, MDRS Mattis Dementia Rating Scale, FCSRT-IR
Grober & Buschke’s Free and Cued Selective Reminding Test with Immediate Recall (French version), IR immediate recall, FR free recall, TR
total recall from the FRCST, ROCF Rey–Osterreith Complex Figure test, PASAT-4 s Paced Auditory Serial Addition Test with an interval of 4 s
between each number, * total number of correct responses/60, SD standard deviation
J Neurol
123
sectional study that for the most part recruited PD patients
from the urban community in Strasbourg, an average-sized
city. The relatively low number of patients included who
had PDD may be explained in two ways: on the one hand, it
has been reported that 6.9 % of persons living in the urban
community of Strasbourg are over 75 years old, and that
14 % of this elderly population have dementia [34]; as PDD
has been reported to account for 3–4 % of cases of dementia
[5], an estimation may be made that around 130 subjects
who are over 75 years of age are likely to have PDD. On the
other hand, if the number of subjects included in the various
studies on the diagnosis of PD-associated cognitive disor-
ders is so low, it could also well be due to the selection
criteria used and the feasibility of carrying out a detailed
Table 4 Comparison of results of cognitive tests in PDD and PD dementia-free patients according to the MDS exhaustive cognitive assessment
(median and range)
N A group N = 31 A1 group N = 20 A2 group N = 11 B group N = 9 p-value
Median (range) Median (range) Median (range) Median (range) A/B A1/A2
MMSE global score/30 24 (16–28) 23 (16–25) 27 (26–28) 27 (26–29) 0.001 \0.001
Seven backwards 0/5 4 (1–5) 3 (1–5) 5 (4–5) 5 (4–5) NS \0.001
Temporal orientation 0/5 4 (1–5) 3.5 (1–5) 5 (3–5) 5 (4–5) 0.02 0.04
Spatial orientation 0/5 5 (3–5) 4 (3–5) 5 (4–5) 5 (4–5) NS 0.003
3-word recall 0/3 1 (0–3) 1 (0–3) 2 (0–3) 2 (0–3) NS NS
Pentagons 0/1 1 (0–1) 0.5 (0–1) 1(0–1) 1 (0–1) NS NS
Word fluency score 120 s 8 (3–15) 7.5 (3–13) 8 (6–15) 11 (4–18) 0.02 NS
MDRS global score 0/144 113 (60–131) 112 (85–131) 116 (60–123) 131 (121–137) \0.001 NS
Attention 0/37 35 (23–37) 35 (29–37) 35 (23–37) 36 (34–37) 0.03 NS
Initiation 0/37 26 (12–36) 25.5 (18–36) 26 (12–33) 32 (25–36) 0.002 NS
Construction 5 (1–6) 5 (2–6) 5 (1–6) 6 (5–6) 0.01 NS
Memory 0/25 15 (6–22) 12.5 (6–20) 16 (6–25) 20 (11–22) 0.01 NS
FRCST-IR IR score 0/48 13 (5–16) 13 (5–16) 13 (8–14) 15 (9–16) 0.004 NS
3-FR score0/48 14 (0–30) 13 (0–30) 15 (8–21) 23 (14–30) 0.003 NS
3-TR score0/48 35 (6–48) 34 (6–47) 35 (30–48) 44 (37–47) 0.004 NS
ROCF score 0/36 18 (0–31) 16 (0–31) 19 (1–25) 28 (17–36) 0.002 NS
PASAT * 7 (0–40) 8.5 (0–40) 2 (0–14) 14 (2–38) 0.04 NS
A group Movement Disorders Society (MDS) exhaustive assessment-determined PDD, A1 group MDS exhaustive assessment-determined PDD
and checklist 8 items positive for PDD, A2 group MDS exhaustive assessment-determined PDD and 8-item checklist \8, B group MDS
exhaustive assessment-determined PDD-free, PDD Parkinson’s disease dementia, MDRS Mattis Dementia Rating Scale, FCSRT-IR Grober &
Buschke’s Free and Cued Selective Reminding Test with Immediate Recall (French version), IR immediate recall, FR free recall, TR total recall
from the FRCST, ROCF Rey–Osterreith Complex Figure test, PASAT-4 s Paced Auditory Serial Addition Test with an interval of 4 s between
each number, * total number of correct responses/60
Table 5 Discriminant validity of the investigated cognitive assessment scales for the diagnosis of PDD
MDRS score 0/144 FCSRT-IR 3-FR
score 0/48
ROCF score 0/36
Cut-off point B120 B123 B132 B22 B21
AUC (95 %) 0.959 B123 B132 0.855 0.839
Sensitivity 0.806 0.935 1.000 0.839 0.903
Specificity 1.000 0.778 0.444 0.778 0.778
PPV 1.000 0.935 0.861 0.929 0.933
NPV 0.600 0.778 1.000 0.778 0.700
Incidence of detection 0.625 0.775 0.900 0.700 0.750
Accuracy 0.85 0.9 0.875 0.825 0.875
95 % CI 0.702–0.943 0.763–0.972 0.732–0.958 0.672–0.927 0.732–0.958
PDD Parkinson’s disease dementia, AUC area under the curve, CI confidence interval, PPV positive predictive value, NPV negative predictive
value, MDRS Mattis Dementia Rating Scale, FCSRT-IR Grober and Buschke’s Free and Cued Selective Reminding Test with Immediate Recall
(French version), 3-FR 3 Free Recalls, ROCF Rey–Osterreith Complex Figure test
J Neurol
123

cognitive examination in this specific, i.e. very elderly
patient population. This view is corroborated by the studies
of Riedel et al. [35] (GEPAD) and Balzer-Geldsetzer et al.
[36] (DEMPARK). The first study found that 229 patients
had PDD, i.e. 29 % of the PD population investigated
diagnosis of dementia established by an MMSE score B24,
global clinical impression and DSM IV criteria, whereas in
the latter study the number of patients diagnosed with PDD
amounted to just 78, i.e. 13.1 % of the 604 PD patients who
had been selected on the basis of a detailed cognitive
examination carried out within the same urban community,
but one which was much larger than that examined in the
present work.
The relative utility of the checklist has been confirmed
in the present study for the diagnosis of PDD in an elderly
PD population although it has its limitations as a screening
instrument. However, there is a widespread need for a brief
yet reliable diagnostic method to help diagnose PDD
patients who are at a relatively advanced stage of their
disease. Not only would a short method be simpler and thus
more feasible to apply, but as these attention disorders will
continue to worsen in this elderly PDD population it will
become increasingly more difficult for them to be capable
of undergoing an in-depth neuropsychological assessment.
In this regard, reports have been published in the literature
on the diagnostic method proposed by Emre et al. and
Dubois et al. [10, 11], and several other studies have also
investigated the sensitivity and specificity of the checklist
for the diagnosis of PDD.
Using an in-depth neuropsychological examination as
reference, Barton et al.’s study [37] classified 15 subjects
out of 91 PD patients as suffering from PDD (mean age:
66.3 ± 9.7 years). It should, however, be mentioned that
these authors had expressly not respected definite cut-off
values for the cognitive assessment, and that the specificity
amounted to 1. The sensitivity of the checklist was only
46 %, with a prevalence of 7.7 %. The study by Riedel et al.
[35] on the assessment of PD-associated disorders with an
MMSE of B24 also showed a sensitivity of only 50 %.
In Di Battista et al.’s study [38] using the DSM IV cri-
teria for the diagnosis of PDD as reference, the checklist
was validated with a sensitivity of 78 % and a specificity of
95.5 % for a 12 % prevalence of PDD in 76 subjects (mean
age: 69.3 ± 8.5 years), i.e. nine cases of PDD (mean age:
77 ± 5.4 years) with a PPV of 70 %, an NPV of 97 %, and
an accuracy of 93.4 %. Nine cases of PDD were determined
using the checklist and seven cases of PDD with the DSM
IV criteria. The latter study is the only one in which the
checklist overestimated the diagnosis of PDD. In fact, use of
the checklist tends to result in an underestimation of the
number of PDD cases rather than the opposite. It has been
suggested that the sensitivity of the checklist could be
improved upon if depression, apathy, hallucinations and
delusions were to be considered characteristics in support of
a diagnosis of PDD [37, 39]; moreover, the results of the
present study did not reveal any significant differences in
this regard: all the patients in fact had at least one psychi-
atric disorder at inclusion in this study. Thus, it was not the
lack of data on psychiatric or behavioral disorders that
declassified patients likely to have PDD. In the present
study, the PDD patients classified by the checklist (A1
group) were at a stage of dementia in which temporo-spatial
orientation disorders had developed. As regards the MMSE
orientation subtest, among the patients with PDD (A group),
the A2 group was found to be better oriented in time and
space than the A1 group, with a significant difference of
0.04 and 0.003 respectively. Also of note, as regards the
MMSE orientation subtest the dementia-free PD patients (B
group) were better temporally oriented than the 31 PDD
subjects (A group), with a significant difference of 0.02. In
fact, the diagnosis of PDD is strongly linked to the devel-
opment of disorientation [35]; at this point, it is suggested
that the checklist could include a temporal orientation item
to determine the progressive impairment of temporo-spatial
perception, as was observed in the present study. It can be
considered that the cognitive deficits determined via the
eight-item checklist tended to be more severe in PD
patients: however, the latter was not sufficiently sensitive
for the diagnosis of PDD because 11 out of the 31 patients
with at least two cognitive domains impaired were excluded
using this method. Attention disorders were therefore
determined by the item, disorientation on the MMSE, which
characterizes the advanced stages of PDD.
In Dujardin et al.’s study [40] involving 41 PDD patients
(mean age: 73.95 ± 5.27 years) out of a total PD patient
population of 188 subjects (mean age: 69.10 ± 8.68 years),
validity was based on an adaptation of the MDS checklist
which included a five-word test, the Pill questionnaire and
an assessment of specific behavioral disorders—halluci-
nations, depression and motivational state. The shortened
approach developed by Dujardin et al. was compared with
an in-depth neuropsychological examination as recom-
mended by the MDS, and showed a sensitivity of 65.85 %
(95 % CI = 49.41–79.92 %) and a specificity of 94.56 %
(95 % CI = 89.56–97.62 %). An MMSE score B26, ver-
bal fluency B7, the five-word recall test, the score on the
Pill questionnaire and age C70 years showed improved
sensitivity at 85.37 % (95 % CI = 76.69–89.25 %) with-
out overly reducing specificity at 83.67 % (95 %
CI = 76.69–89.25 %). In the present study, this threshold
of B26 only permitted five patients to be reclassified in the
group of dementia patients instead of the 11 PDD subjects
diagnosed via the exhaustive assessment, taking into
account the fact that the five-word test was not used in the
MDS checklist in the present study. Moreover, two out of
these five patients were not classified as demented by the
J Neurol
123

exhaustive list. Hoops et al.’s study [41] investigated the
validity of the Montreal Cognitive Assessment test [42]
and the MMSE for the detection of mild cognitive
impairment (MCI) and PDD. These authors showed an
optimal cut-off point of between 24 and 25 for the diag-
nosis of PDD via the MMSE, with a sensitivity of 29 %,
specificity of 99 %, PPV of 83 %, NPV of 88 %. In the
present study, the MDS checklist displayed a better sensi-
tivity for an optimal specificity of 1, with an MMSE of
\26. In Biundo et al.’s study [43], the cut-off score, in
agreement with the MDS criteria for differentiation
between PDD and PD without the presence of cognitive
impairment, had a value of\25.9 for 15 PDD patients with
an average age of 70.3 years (±7.6 years) out of 104
consecutive PD patients, with a PPV of 80 %. With a
sensitivity of 0.645 for the checklist results, the present
study showed that it had a fairly low capacity for detecting
patients suffering from PDD when they had an MMSE
score of C26.
This study proposes that the evaluation of the cognitive
domains be based on the MDS exhaustive reference method
or gold standard. The choice of subtests with the 3-FRs
seemed to be of interest for the diagnosis of dementia,
whatever its etiology [44], while the memory subtest, which
explores visual memory, verbal recall and fluctuating
attention, displayed an excellent capacity to establish a
diagnosis of dementia [28]. The utility of the Rey–Osterrieth
Complex Figure for the exploration of visuo-constructive
capacities was confirmed for its use in the assessment of PD-
associated cognitive disorders [43]. In the present study, the
choice of at least one abnormal test result out of two for
classifying a cognitive domain as being impaired rather than
two abnormal test results can be explained by the fact that it is
thereby possible to avoid underestimating the number of
domains that have been impaired, all the more as the tests
used to assess a domain have been specifically adapted to the
assessment of states of dementia. The choice of two abnor-
mal test results out of three for classifying the executive
function cognitive domain as impaired is explained by the
fact that as the PASAT has frequently failed to adequately
assess dementia, it is thereby possible to avoid overesti-
mating executive dysfunction. This approach permitted 31
patients to be classified as having PDD, and for nine patients
to be considered dementia-free, although the latter group
nevertheless experienced problems regarding ADL. How-
ever, it is commonly known that PD-associated cognitive
impairment has a progressively negative effect on PD
patients’ capacity to deal with ADL, even in the absence of
dementia [23]. As regards the PDD-free group, the criteria
for the assessment of mild cognitive impairment (MCI),
which were not applied in the present study, would have
allowed cognitive impairment to be classified between MCI
and normal. In a predominantly PD patient population,
around 10 % of patients have been found to progress from
the non-demented to the demented stage each year [45].
This study also attempted to establish optimal cut-off
values for the diagnosis of PDD using other cognitive tests.
The ROC curve showed a clear relationship between PDD
diagnosis and the MDRS score. However, a circularity bias
was present as the global score on the MDRS rating scale,
the construction score and the memory score were included
in the diagnostic criteria on the reference list. At this point,
it should also be recalled that the values were expressed in
pc (the reference was in percentiles such as \10 pc), and
the threshold values of previous studies did not serve as a
basis in the present case for differentiating between normal
and demented patients. The MDRS explored the executive
functions and contributed to establishing the diagnosis of
PDD. The results of the MDRS in the present study were
fairly similar to those previously published in the literature,
but with slight differences. Mean values of 109.5 ± 11.2
(A1 group) versus 110.5 ± 13.7 (A group) were found,
whereas in Llebaria et al.’s study [28] which investigated a
younger and less educated patient population
(77.6 ± 5 years; 6.4 ± 4 years in PDD patients), the mean
value for subjects classified as having PDD amounted to
105 ± 14.30. Using the CDR scale and the DSM IV cri-
teria as diagnostic reference tools, a diagnostic cut-off
value of 123 for the MDRS was proposed by these authors.
This value corresponded to a sensitivity of 92.65 % and a
specificity of 91.4 %, a PPV of 83.3 %, and an NPV of
96.4 %. In Martinez-Martin et al.’s study [46], the diag-
nostic criteria for PDD in a population of 85 PDD patients
(mean age: 71.9 ± 6.3 years) based on the CDR scale and
the DSM IV criteria were found to be less sensitive than
those proposed by the MDS. Using the MDS in-depth
neuropsychological examination as a basis for reference
which did not include the MDRS to avoid a circularity bias,
an optimal cut-off value of B132 on the MDRS scale has
been proposed by Matteau et al. [47] for the diagnosis of
PDD (n = 6; mean age: 73.5 ± 7.7 years), with a sensi-
tivity of 1 and a specificity of 1. In the latter study, the
neuropsychological examination was better adapted to a
diagnosis of MCI rather than to that of PDD, and classified
as PDD patients all subjects who presented with a depen-
dent state. The cut-off point of 132 in the present study
showed a sensitivity of 1 with a low specificity; the cut-off
point of 120 appears to correspond to a discriminatory
value for the diagnosis of PDD, and that of 132 to a dis-
criminatory value for the screening of PDD. The use of the
checklist criteria could suffice for the diagnosis of severe
PDD, and that of the MDRS for the diagnosis of PDD in
patients who do not fulfill the checklist conditions. How-
ever, the difficulty lies in determining which persons
actually have disease and who remain undiagnosed among
the group classified as PDD-free for an MMSE score of
J Neurol
123
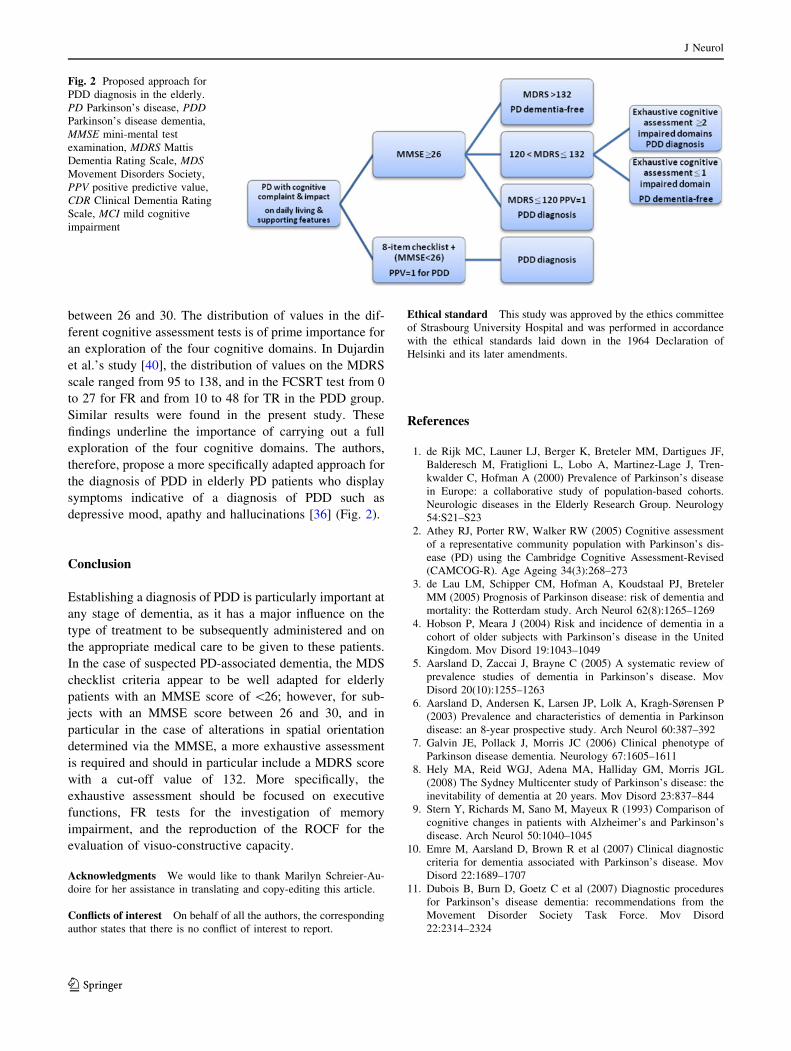
between 26 and 30. The distribution of values in the dif-
ferent cognitive assessment tests is of prime importance for
an exploration of the four cognitive domains. In Dujardin
et al.’s study [40], the distribution of values on the MDRS
scale ranged from 95 to 138, and in the FCSRT test from 0
to 27 for FR and from 10 to 48 for TR in the PDD group.
Similar results were found in the present study. These
findings underline the importance of carrying out a full
exploration of the four cognitive domains. The authors,
therefore, propose a more specifically adapted approach for
the diagnosis of PDD in elderly PD patients who display
symptoms indicative of a diagnosis of PDD such as
depressive mood, apathy and hallucinations [36] (Fig. 2).
Conclusion
Establishing a diagnosis of PDD is particularly important at
any stage of dementia, as it has a major influence on the
type of treatment to be subsequently administered and on
the appropriate medical care to be given to these patients.
In the case of suspected PD-associated dementia, the MDS
checklist criteria appear to be well adapted for elderly
patients with an MMSE score of \26; however, for sub-
jects with an MMSE score between 26 and 30, and in
particular in the case of alterations in spatial orientation
determined via the MMSE, a more exhaustive assessment
is required and should in particular include a MDRS score
with a cut-off value of 132. More specifically, the
exhaustive assessment should be focused on executive
functions, FR tests for the investigation of memory
impairment, and the reproduction of the ROCF for the
evaluation of visuo-constructive capacity.
Acknowledgments We would like to thank Marilyn Schreier-Au-
doire for her assistance in translating and copy-editing this article.
Conflicts of interest On behalf of all the authors, the corresponding
author states that there is no conflict of interest to report.
Ethical standard This study was approved by the ethics committee
of Strasbourg University Hospital and was performed in accordance
with the ethical standards laid down in the 1964 Declaration of
Helsinki and its later amendments.
References
1. de Rijk MC, Launer LJ, Berger K, Breteler MM, Dartigues JF,
Balderesch M, Fratiglioni L, Lobo A, Martinez-Lage J, Tren-
kwalder C, Hofman A (2000) Prevalence of Parkinson’s disease
in Europe: a collaborative study of population-based cohorts.
Neurologic diseases in the Elderly Research Group. Neurology
54:S21–S23
2. Athey RJ, Porter RW, Walker RW (2005) Cognitive assessment
of a representative community population with Parkinson’s dis-
ease (PD) using the Cambridge Cognitive Assessment-Revised
(CAMCOG-R). Age Ageing 34(3):268–273
3. de Lau LM, Schipper CM, Hofman A, Koudstaal PJ, Breteler
MM (2005) Prognosis of Parkinson disease: risk of dementia and
mortality: the Rotterdam study. Arch Neurol 62(8):1265–1269
4. Hobson P, Meara J (2004) Risk and incidence of dementia in a
cohort of older subjects with Parkinson’s disease in the United
Kingdom. Mov Disord 19:1043–1049
5. Aarsland D, Zaccai J, Brayne C (2005) A systematic review of
prevalence studies of dementia in Parkinson’s disease. Mov
Disord 20(10):1255–1263
6. Aarsland D, Andersen K, Larsen JP, Lolk A, Kragh-Sørensen P
(2003) Prevalence and characteristics of dementia in Parkinson
disease: an 8-year prospective study. Arch Neurol 60:387–392
7. Galvin JE, Pollack J, Morris JC (2006) Clinical phenotype of
Parkinson disease dementia. Neurology 67:1605–1611
8. Hely MA, Reid WGJ, Adena MA, Halliday GM, Morris JGL
(2008) The Sydney Multicenter study of Parkinson’s disease: the
inevitability of dementia at 20 years. Mov Disord 23:837–844
9. Stern Y, Richards M, Sano M, Mayeux R (1993) Comparison of
cognitive changes in patients with Alzheimer’s and Parkinson’s
disease. Arch Neurol 50:1040–1045
10. Emre M, Aarsland D, Brown R et al (2007) Clinical diagnostic
criteria for dementia associated with Parkinson’s disease. Mov
Disord 22:1689–1707
11. Dubois B, Burn D, Goetz C et al (2007) Diagnostic procedures
for Parkinson’s disease dementia: recommendations from the
Movement Disorder Society Task Force. Mov Disord
22:2314–2324
Fig. 2 Proposed approach for
PDD diagnosis in the elderly.
PD Parkinson’s disease, PDD
Parkinson’s disease dementia,
MMSE mini-mental test
examination, MDRS Mattis
Dementia Rating Scale, MDS
Movement Disorders Society,
PPV positive predictive value,
CDR Clinical Dementia Rating
Scale, MCI mild cognitive
impairment
J Neurol
123

12. Hughes AJ, Daniel SE, Kilford L, Lees AJ (1992) Accuracy of
clinical diagnosis of idiopathic Parkinson’s disease: a clinic-
pathological study of 100 cases. J Neurol Neurosurg Psychiatry
55:181–184
13. Dujardin K, Duhamel A, Delliaux M, Thomas-Anterion C,
Destee A, Defebvre L (2010) Cognitive complaints in Parkin-
son’s disease: its relationship with objective cognitive decline.
J Neurol 257:79–84
14. Hughes CP, Berg L, Danzinger WL, Coben LA, Martin RL
(1982) A new clinical scale for the staging of dementia. Br J
Psychiatry 140:566–572
15. Morris JC (1993) The Clinical Dementia Rating (CDR): current
version and scoring rules. Neurology 43:2412–2414
16. Williams MM, Roe CM, Morris JC (2009) Stability of the
Clinical Dementia Rating: 1979–2007. Arch Neurol 66(6):
773–777
17. Folstein MF, Folstein SE, McHugh PR (1975) ‘‘Mini-mental
state’’. A practical method for grading the cognitive state of
patients for the clinician. J Psychiatr Res 12:189–199
18. McDonald WM, Holtzheimer PE, Haber M, Vitek JL, McW-
horter K, Delong M (2006) Validity of the 30-item geriatric
depression scale in patients with Parkinson’s disease. Mov Disord
21:1618–1622
19. Schrag A, Barone P, Brown RG et al (2007) Depression rating
scales in Parkinson’s disease: critique and recommendations.
Mov Disord 22(8):1077–1092
20. Cardebat D, Doyon B, Puel M, Goulet P, Joanette Y (1990)
Formal and semantic lexical evocation in normal subjects. Per-
formance and dynamics of production as a function of sex, age
and educational level. Acta Neurol Belg 90(4):207–217
21. Godefroy O, ‘Groupe de Reflexion sur l’Evaluation des Fonctions
Executives’ (2008) Fonctions executives et pathologies neuro-
logiques et psychiatriques. Solal, Marseille
22. Hoehn MM, Yahr MD (1967) Parkinsonism: onset, progression,
and mortality. Neurology 17:427–442
23. Rosenthal E, Brennan L, Xie S, Hurtig H, Milber J, Weintraub D,
Karlawish J, Siderowf A (2010) Association between cognition
and function in patients with Parkinson disease with and without
dementia. Mov Disord 25(9):1170–1176
24. Fahn S, Elton RL, The UPDRS Development Committee (1987)
Unified Parkinson’s disease rating scale. In: Fahn S, Marsden CD,
Calne D, Goldstein M (eds) Recent developments in Parkinson’s
disease. Macmillan Health Care Information, Florham Park,
pp 153–163
25. Mattis S (1976) Mental status examination for organic mental
syndrome in the elderly patient. In: Bellak L, Karasy T (eds)
Geriatric psychiatry. Grune and Stratton, New York, pp 77–121
26. Mattis S (1988) Dementia rating scale: professional manual.
Psychological Assessment Resources, Odessa
27. Brown GG, Rahill AA, Gorell JM, McDonald C, Brown SJ,
Sillanpaa M et al (1999) Validity of the dementia rating scale in
assessing cognitive function in Parkinson’s disease. J Geriatr
Psychiatry Neurol 12(4):180–188
28. Llebaria G, Pagonobarraga J, Kulisevsky J, Garcia-Sanchez C,
Pascual-Sedano B, Gironell A, Martinez-Corral M (2008) Cut-off
score of the Mattis dementia rating scale for screening dementia
in Parkinson’s disease. Mov Disord 23:1546–1550
29. Machulda MM, Ivnik RJ, Smith GE, Ferman TJ, Boeve BF,
Knopman D et al (2007) Mayo’s older Americans normative
studies: visual form discrimination and copy trial of the Rey–
Osterrieth complex figure. J Clin Exp Neuropsychol 29:377–384
30. Van der Linden M, Coyette F, Poitrenaud J, et al (2004)
L’epreuve de rappel libre/rappel indice0 a 16 items (RL/RI-16).
In: Van der Linden M, Grenem (eds) L’evaluation des troubles de
la memoire. Marseille, Solal, pp 25–47.
31. Gronwall C (1977) Paced auditory serial-addition task: a measure
of recovery from concussion. Percept Mot Skills 44:367–373
32. Naeagele B, Mazza S. Paced auditory serial-addition task: version
francaise dite modifiee. Editions Solal.
33. Wancata J, Alexandrowicz R, Marquart B, Weiss M, Friedrich F
(2006) The criterion validity of the geriatric depression scale: a
systematic review. Acta Psychiatr Scand 114:398–410
34. Conseil General du Bas-Rhin/Departmental Council of the Lower
Rhine. Diagnostic departemental: les seniors. Pole aide a la
personne. 2007; http://www.bas-rhin.fr
35. Riedel O, Klotsche J, Spottke A, Deuschl G, Forstl H, Henn F,
Heuser I, Oertel W, Reichmann H, Riederer P, Trenkwalder C,
Dodel R, Wittchen H-U (2008) Cognitive impairment in 873
patients with idiopathic Parkinson’s disease. Results from the
German Study on Epidemiology of Parkinson’s Disease with
Dementia (GEPAD). J Neurol 255:255–264
36. Balzer-Geldsetzer M, Ferreira Braga da Costa A-S, Kronenburger
M et al (2011) Parkinson’s disease and dementia. A longitudinal
study (DEMPARK). Neuroepidemiology 37:168–176
37. Barton B, Grabli D, Bernard B, Czernecki V, Goldman JG,
Stebbins G, Dubois B, Goetz CG (2012) Clinical validation of
Movement Disorder Society : recommended diagnostic criteria
for Parkinson’s disease with dementia. Mov Disord 27:248–253
38. Di Battista ME, Giustini P, Bernardi S, Stirpe P, Vanacore N,
Meco G (2011) A simplified algorithm may lead to overestimate
dementia in PD. A clinical and epidemiological study using cri-
teria for PD-D proposed by the Movement Disorders Task Force.
J Neural Transm 118:1609–1612
39. Dujardin K, Sockeel P, Delliaux M, Destee A, Defebvre L (2009)
Apathy may herald cognitive decline and dementia in Parkinson’s
disease. Mov Disord 24:2391–2397
40. Dujardin K, Dubois B, Tison F, Durif F, Bourdeix I, Pere JJ,
Duhamel A, Executive study group (2010) Parkinson’s disease
dementia can be easily detected in routine clinical practice. Mov
Disord 25:2769–2776
41. Hoops S, Nazem S, Siderowf AD, Duda JE, Xie SX, Stern MB,
Weintraub D (2009) Validity of the MoCA and MMSE in the
detection of MCI and dementia in Parkinson disease. Neurology
73:1738–1745
42. Nasreddine ZS, Phillips NA, Bedirian V et al (2005) The Mon-
treal Cognitive Assessment, MoCA: a brief screening tool for
mild cognitive impairment. J Am Geriatr Soc 53:695–699
43. Biundo R, Weis L, Pilleri M, Facchini S, Formento-Dojot P,
Vallelunga A, Antonini A (2013) Diagnostic and screening power
of neuropsychological testing in detecting mild cognitive
impairment in Parkinson’s disease. J Neural Transm 120:627–633
44. Grober E, Sanders AE, Hall C, Lipton RB (2010) Free and cued
selective reminding identifies very mild dementia in primary care.
Alzheimer Dis Assoc Disord 24:284–290
45. Aarsland D, Kurz MW (2010) The epidemiology of dementia
associated with Parkinson’s disease. Brain Pathol 20(3):633–639
46. Martinez-Martin P, Falup-Pecurariu C, Rodriguez-Blazquez C,
Serrano-Duenas M, Carod Artal FJ, Rojo Abuin JM, Aarsland D
(2011) Dementia associated with Parkinson’s disease: applying
the Movement Disorder Society Task Force criteria. Parkinson-
ism Relat Disord 17:621–624
47. Matteau E, Dupre N, Langlois M, Provencher P, Simard M
(2012) Clinical validity of the Mattis dementia rating scale-2 in
Parkinson disease with MCI and dementia. J Geriatr Psychiatry
Neurol 25:100–106
J Neurol
123