
The Mojo Programme Tallaght - hse.ie · The Mojo pilot programme worked with three groups of men on...
53
The Mojo Programme Tallaght Men at risk to suicide: An interagency response Final Report Evaluation Burtenshaw Kenny Associates December 2013 Burtenshaw Kenny Associates
Transcript of The Mojo Programme Tallaght - hse.ie · The Mojo pilot programme worked with three groups of men on...

The Mojo Programme Tallaght Men at risk to suicide: An interagency response
Final Report Evaluation
Burtenshaw Kenny Associates
December 2013
Burtenshaw KennyAssociates

2
Table of Contents
Executive Summary ....................................................................................................................... 3
1. Introduction .......................................................................................................................... 7
1.1 Evaluation: Terms of Reference....................................................................................... 7 1.2 Objectives of the Mojo Programme .................................................................................. 8 1.3 Methodology .................................................................................................................. 9 1.4 Acknowledgements....................................................................................................... 10
2. Context ............................................................................................................................... 11
2.1 Mental Health and Suicide in Ireland ............................................................................. 11 2.2 Unemployment ............................................................................................................. 12 2.3 Interagency Working .................................................................................................... 12
3. Mojo Overview .................................................................................................................... 14
3.1 History and Rationale for Mojo ...................................................................................... 14 3.2 Mojo ............................................................................................................................ 15 3.3 Organisations involved in Mojo ...................................................................................... 20
4. Evaluation Findings - Mojo Programme ................................................................................. 22
4.1 Group Based Training ................................................................................................... 22 4.2 Care Planning and Link Working .................................................................................... 25 4.3 Mojo Outcomes for Participants ..................................................................................... 25 4.4 Mojo outcomes for Partners .......................................................................................... 29 4.5 Mojo outcomes for key external stakeholders ................................................................. 29 4.6 Post Mojo .................................................................................................................... 30
5. Evaluation findings - Mojo approach ..................................................................................... 32
5.1 Preparation and development phase .............................................................................. 32 5.2 Recruitment and selection ............................................................................................. 33 5.3 Interagency Structure ................................................................................................... 35 5.4 Co-ordination and Management .................................................................................... 36 5.5 Collaborative working ................................................................................................... 38 5.6 Communication ............................................................................................................ 39
6. Overview ............................................................................................................................. 41
6.1 Overall ......................................................................................................................... 41 6.2 Mojo Programme .......................................................................................................... 41 6.3 Mojo Approach ............................................................................................................. 44
7. Final Recommendations ....................................................................................................... 47
7.1 Mojo Programme Recommendations .............................................................................. 47 7.2 Mojo Approach Recommendations ................................................................................. 47 7.3 Expansion of Mojo ........................................................................................................ 48 7.4 Policy considerations .................................................................................................... 48
9. Appendix 2: Advisory Group Members ................................................................................... 51
10. Appendix 3: Sample Poster ............................................................................................... 52

3
Executive Summary
Introduction This report presents the final evaluation of the pilot phase of the Mojo programme, an interagency
response for men who are affected by unemployment and/or the recession and who are finding it
difficult to cope. The evaluation is based on an eighteen month external formative evaluation process. This executive summary will provide a short synopsis of the pilot programme, its background,
content, outcomes and recommendations.
The Mojo Programme was initiated and subsequently managed by South Dublin County Partnership
(SDCP - formerly known as Dodder Valley Partnership) and is funded by the National Office for Suicide Prevention (NOSP).
Mojo originated from work that was done by Suicide Action West Tallaght, an interagency group
established to respond to growing concerns about the level of male death by suicide in West Tallaght. Following their initial research and successful application for funding, the Mojo programme was
initiated.
Mojo focuses on targeting men (aged 25 and older with a priority on those over 40). It is becoming
more evident nationally that this cohort of men is increasingly at risk of suicide. A Programme Coordinator, with the support of senior level stakeholders from a range of statutory and non statutory
organisations worked together to research, plan and design the Mojo programme. Leaders and
champions emerged with significant, recognised experience in the areas of mental health and collaborative working. Their input helped to inform the programme, give credibility and encourage
key stakeholders to actively engage in Mojo.
The initial planning and development phase took place over a twelve month period from August 2011 to August 2012. The lead in time helped to ensure that the programme was based on best practice. It
also ensured that stakeholders were actively involved in agreeing the programme structure, its
management and implementation. This senior level group continued to meet to advise on the programme roll out through their participation in the Advisory Group, the Care Planning Group and
task specific working groups. They were also actively involved in supporting the implementation of the Mojo pilot by co facilitating a number of training sessions throughout 2012 and 2013.
Mojo Programme The Mojo pilot programme worked with three groups of men on a ten/twelve week basis.1 Each Mojo
programme was based on working with participants as part of a) group based training and b) on a
one to one basis with designated link workers to develop and support the implementation of a care plan.
The group training element of the programme took place over two sessions per week. One session
focused on mental health and wellbeing underpinned by Wellness Recovery Action Planning (WRAP)
and other specialised sessions focussing on mental health resilience. The other session provided information and support to access a range of services to help the men return to work or education. A
fitness programme was incorporated into the second and third Mojo programmes in order to increase the men’s involvement in physical activity. Agencies involved in Mojo worked with Mojo staff to
implement the programme. The mental health and wellbeing aspect of the programme was led by an
agency representative who was trained and experienced in delivering WRAP. 2
1 Mojo 1 and 2 ran over twelve weeks, with Mojo 3 running over ten weeks 2 WRAP is based on an evidenced based programme www.copelandcenter.com

4
The care planning and link working element of Mojo used the Mental Health Recovery Star
assessment and care planning tool, widely used in the UK, to care plan and case manage participants.3 The primary role of this element of the programme was to link individual participants
into agreed services, co-ordinate service delivery, liaise with other key workers as required, provide feedback to participants, ensure documentation was complete and to develop care plans. Five senior
staff from four organisations in addition to the Mojo programme Co-ordinator were trained and
worked with participants on this element of the programme.
An outcome of the initial Mojo programme was the establishment of a Men’s Shed as a post programme support. This was not included in the original plan or objectives for Mojo but was a
response initiated by the men, with the support of Mojo organisers, to provide a space where health and wellbeing supports for men were available. This Men’s Shed is available to all men across South
County Dublin, who have an interest in engaging in activities that support health and wellbeing.
SDCP is responsible for managing the programme and providing the training space for the groupwork
elements of the programme. A Programme Co-ordinator is employed by SDCP on a part time basis to support management and co-ordination. Additional funding was secured for Mojo 2 and 3 to employ a
part time Project Support Worker who had responsibility for implementing elements of the
programme and to support the establishment of the Men’s Shed. In addition to the part time staff employed, the agencies involved in Mojo (over twenty two), played an instrumental part in delivering
the group training and care planning aspects of the programme. These organisations are outlined in section 3.3, and range from statutory and voluntary sector organisations involved in mental health
care and provision such as HSE Tallaght Mental Health Service, Threshold Training Network and Shine, to education and training organisations such as Tallaght Adult Education Service, South Dublin
Sports Partnership. There was no cost to Mojo for all of the time given by the organisations involved
to plan, oversee, deliver or care plan. This substantial contribution was incorporated by agencies involved as part of their commitment to the programme.
Programme Outcomes
The Mojo pilot programme was an exceptionally successful preventative/early intervention Programme. It was designed and delivered collaboratively with key stakeholders to a very high level
to one of the most vulnerable groups to suicide, in Irish society. The programme met all of the objectives set and expanded on elements of the programme as it rolled out. The time taken to plan
and the high calibre of the agency representatives, lead agency (SDCP) and Programme Co-ordinator was instrumental in the success of Mojo.
The Mojo pilot engaged with thirty six men vulnerable men, which exceeded the initial target of thirty. All three pilots targeted men, most of whom had a history of employment prior to the recession and
who were experiencing mental health challenges. The majority of Mojo participants were over the age of 40, with almost a third previously employed in the construction sector and most of whom had low
education levels. There are substantial national challenges to respond appropriately and support this
group, particularly for men who were previously self employed.
Of particular importance to note is the high retention level of participants at 89%, which was consistent across all programmes. In addition, the progression rate for participants either on to
another service or back to employment post the programme was 70%. These achievements are in excess of accepted national retention and progression rates. It is particularly notable given the
voluntary nature of participation (no allowances were paid to participants), the level of commitment
that was required (two mornings per week), and the personal and health challenges experienced by participants.
The outcomes for participants, their partners and key external stakeholders are outlined in detail in
sections 4.3, 4.4 and 4.5 of this report and there was a high level of consistency across all three Mojo
3 www.outcomesstar.org.uk

5
programmes. In summary, participants who engaged in Mojo had an increased ability to manage their
mental health, physical health and self care. The evaluation found that participants, often for the first time, were learning how to manage and take control of their health. In addition participants self
esteem and trust in others increased following participation on this programme. The enjoyment and sense of belonging were also key outcomes for the participants involved. These were largely due to
the facilitators’ delivery of the project and the atmosphere created which allowed them to fully
participate. The evaluation also found that the men involved in Mojo are taking positive steps to build on Mojo and progress onto other opportunities. This is exceptionally positive. The evaluation found
that partners of the participants highlighted that the men became more open, spoke more about their concerns and worries and were less angry. It also found that external stakeholders were exceptionally
positive about the programme, the quality and involvement of medical professionals from the outset gave Mojo increased credibility. Stakeholders are keen that the lessons learned from Mojo are
considered nationally, as the programme as a whole in their view was unique, innovative and very
successful.
The evaluation also found that the quality of management and staffing was key to this programme. The interagency approach requires dedication, time and commitment from participating agencies.
This was achieved, however maintaining this intensive level of engagement will require a sustained
stream of funding in the mid to long term.
Recommendations The following recommendations are made to inform the future development and expansion of the
Mojo:
A. Mojo Programme
Retain the current structure of the Mojo programme to include group based training (which
includes WRAP and resilience building and Information Provision) alongside careplanning and link working.
Mojo should run over 12 weeks, with two three hour group training elements and with
physical exercise included in the Programme. Consolidate progress by focusing more on pathways to employment/education/training as part
of the information provision element of the project.
Consider specific programmes targeting taxi drivers and Travellers as these presented as
particularly vulnerable groups of men who informed the initial rationale for the programme. While strategies have been put in place to attract these groups, they have not engaged in the
programme to date. Therefore, their needs have not been met. Different strategies maybe
required to attract these groups given cultural and work patterns (e.g. taxi drivers working at night). Therefore, specific programmes maybe more effective in responding to the needs of
these men. The Mental Health Recovery Star tool should continue to be used to underpin care planning.
Participants should continue to have one to one meetings at least twice during each project.
The way that link workers share progress, updates and concerns with GP and other referrers
should be considered further to ensure that referrers are aware of progress. This may not
always be appropriate but in some instances could help participant progress.
Continue to develop the tracking system for participants when they leave the Mojo
programme. The position of the post Mojo Men’s Shed needs to be clarified and clearly agreed as it is
likely to require long-term resourcing if it is to develop further.
The Mojo Programme should be retained in Tallaght on account of the population it serves,
established demand, work already completed to establish the programme, and the level of service/supports available in the area. This will require long term secured resourcing.

6
B. Mojo Approach Recommendations
A more effective plan to respond to the increasing demand for places on Mojo projects is
required, especially for those referred well in advance of the commencement of the
programme. Examine the mental health policy and practices of agencies particularly those with a remit for
employment supports and services (primarily the Department of Social Protection and the
Local Employment Service) to identify how these agencies can take on a more central,
supportive role within Mojo. This could help to support increased participation and buy in from these agencies in Mojo more locally.
Retain the Advisory group and Working Group structure in future Mojo programmes.
Give further consideration to how the learning and work within Mojo can contribute to the
work of the agencies involved. For example utilising the Recovery Star tool.
C. Expansion of Mojo
Prior to considering the expansion of Mojo the costs involved in the programme should be
established and evaluated.
Taking cost/benefit into account, plan to expand Mojo to other specific cohorts in Tallaght
such as taxi drivers, Traveller men, men with who were previously self-employed, younger people (possibly in conjunction with Jigsaw), and women. The Programme will require
adjustments for same. Taking cost/benefit into account, plan to run Mojo as a pilot in an area with a similar profile
and level of service to Tallaght. This would test the programme but only minimal structural
changes would be required. Consider the adjustments to the Programme to run in a rural area which would be less likely
to have the developed services and supports that exist in Tallaght.
Review the Mojo Reference Manual in the context of rolling out the programme outside of
Tallaght.
Any expansion of the Programme will require dedicated Co-ordination with wide ranging skills
levels and experience. In particular experience of achieving outcomes through interagency working at senior level, understanding and experience of working with disadvantaged target
groups, mental health and supporting progression to employment/training or further education is important to implement the role (as outlined in section 5.2).
D. Policy considerations
Mojo has demonstrated that unemployed men who are experiencing a number of complex
health and social issues are willing to voluntarily engage in well run programmes that help
them plan their progress. There are substantial gaps in supports and services available to those who were previously
self-employed. As they are not automatically entitled to social welfare support or services,
their status is often uncertain as they are not working but not officially classified as unemployed. Mojo provides an effective model for supporting this particularly isolated and
vulnerable cohort.
The employment support system faces national challenges in supporting men over 40 with
relatively low levels of education in their return to full time and sustained employment. This cohort is large due to the decline in the construction sector. There are even greater
challenges when this cohort experience mental health issues. Mojo serves as a particularly appropriate strategy to meet the needs of this cohort.
The employment support system at present focuses on results and outputs. The experience
of Mojo demonstrates that the system needs to consider the impact of its processes on the
mental health of men who have been affected by the recession and unemployment. The Mojo model should therefore be drawn upon to promote a greater understanding of mental
health across all relevant state agencies.
7
Research has identified the cohorts served by Mojo as being particularly vulnerable to suicide.
The learning from Mojo should be strongly integrated into the new National Suicide
Prevention Strategy being developed by NOSP. The feasibility of scaling up Mojo as part of suicide prevention more widely should be assessed.
1. Introduction This report presents the final evaluation of Mojo - an interagency response to support men in Tallaght
who are affected by the recession and/or unemployment who are at risk to suicide initiated by the South Dublin County Partnership (SDCP - formerly known as Dodder Valley Partnership). The vision of
Mojo is to reduce the number of male suicides in Tallaght. It is funded as a pilot initiative through the National Office for Suicide Prevention (NOSP).
There were 3 Mojo Programmes with 3 separate groups of men in distress:
Mojo 1: September - December 2012
Mojo 2: January - May 2013
Mojo 3: June - October 2013
Initially, the funding for this programme was committed until December 2013, but new additional
funding was recently secured from NOSP until June, 2014.
This is the final report from a five stage evaluation process, which is partly based on the aggregated
results of the previous reports. Stage 1 was a Base Line Report. This was followed by three further formative evaluations that followed each individual programme. This evaluation process commenced
in June 2012 and concluded in December 2013.
Underlying all of this is the Mojo Reference Manual, which outlines the aims and objectives as well as
the programme and organisational structure. It also provides guidelines and protocols which underpin the implementation of the project along with a range of forms which helped to monitor progress and
process. This Reference Manual was developed prior to the programme evaluation as part of the programme planning phase.
This report should be read in conjunction with the Mojo Reference Manual, the baseline evaluation report, and the three formative evaluation reports.
1.1 Evaluation: Terms of Reference
The following was agreed as the evaluation terms of reference:
1. A summary of the progress on outputs to date.
2. An ongoing formative evaluation up until October 31st 2013 so as to ensure that:
Lessons are learned and captured.
Learning is disseminated.
Continuous improvement and development will be prioritised.

8
The evaluation focused on:
Strategic learning.
Identifying what is working (or not) in order to inform the implementation of the
Programme.
Making changes and adapting the work based on learning from what has happened
to date.
3. The development of an internal monitoring system to track developments and provide an
information base that can be easily accessible. This includes assessing:
The impact of the Programme on the participants and their families.
The interagency network established to support the mental health of men who find
themselves in difficult economic circumstances.
The effectiveness of the Programme’s internal structure such as programme
coordination, the Advisory Group, and the ad-hoc working groups.
The impact of the Programme on participating organisations.
The development and impact of a communications strategy to publicise services and
available supports.
The links between frontline services and whether they lead to improved outcomes for
men ‘in distress.’
The following deliverables were agreed:
Consultation with the Advisory Group, the key workers, the referral agencies and the
Programme management.
Consulting with the Programme participants.
Providing draft interim (written and verbal) reports to the Programme Coordinator,
including conclusions and recommendations every four months.
Providing a final written report, including conclusions and recommendations.
1.2 Objectives of the Mojo Programme
The stated objectives are to have a responsive Programme to men ‘in distress’ by means of:
Developing strong cross-agency working relationships.
Developing inter-agency work methods and key working protocols.
Creating an integrated service that improve all round access to appropriate counselling, financial and welfare advice, and employment and training support.
Improving links and supports to GPs.
Developing frontline staff capacity and response through the delivery of appropriate
training projects to the target group.

9
Monitor and evaluate outcomes and outputs.
As intended outcomes, the Programme would establish an effective and efficient interagency
operation with a key working model for our target group as well as a referral system primed to respond to our target group’s needs. More specifically, the intended outcomes for the men involved
include:
Engagement with a group process that is supportive and responsive to their
needs.
Receiving information on available services and supports.
Support in accessing relevant services and supports.
Support in developing a personal recovery plan.
Clarity on how they may access support in the long-term.
1.3 Methodology
In May 2012, the SDCP commissioned an external evaluation of the Mojo Programme. This evaluation agreed the terms of reference which are outlined in Section 1.1. A range of quantitative and
qualitative methodologies were agreed to deliver the evaluation which commenced in June, 2012 and
is finalised in this report of December, 2013. An evaluation sub-group, comprising two Advisory Group members and the Programme Co-ordinator, was in place to oversee and inform the evaluation
process. The Programme Co-ordinator liaised between the Project and the evaluators. A baseline report was completed in advance of the first Mojo project. In addition, evaluation reports for Mojo 1,
Mojo 2 and Mojo 3 are available and were used to inform the development of Mojo as it progressed.
The following evaluation methods were adopted:
Documentary Review: All of the material produced from the inception of the programme until October, 2013 was reviewed. This included a Mojo reference manual; minutes of meetings; materials produced and designed; the
recovery star tool used to support care planning; and, programme schedules. Evaluation sheets
completed by participants at the end of each training session were also reviewed as were evaluation sheets completed by trainers. In addition, “Reach Out” the National Strategy for Action on Suicide
Prevention 2005-2014, the National Office for Suicide Prevention Annual Report 2012 and other key documents were assessed.
Focus Groups:
Two focus groups were held with participants on each project, one at an early stage and the
other towards the end of each project. In total, six focus groups took place with men while they engaged on the project.
Two focus groups were held with men six months after they completed the project.
Four focus groups were held with the Advisory Group.
Three focus groups took place with the Care Planning Group.
Survey:
Three online surveys were completed by members of the Advisory Group towards the end of
each project. On average, 12 Advisory Group members completed each survey.

10
One to one interviews:
The Project Co-ordinator was interviewed both at the beginning and end of each project.
These were supplemented by regular telephone conversations and email communication.
One to one interviews were held with the Project Support Worker at the beginning and end of
the second and third Mojo project.
One to one interviews took place with seven men, selected according to differing ages, link
workers and experiences by the evaluator through participant records as they participated in the project.
Telephone interviews took place with three partners of participants.
The following one to one interviews took place with key stakeholders linked to the Mojo Programme:
Gerry Raleigh Director of the National Office for Suicide Prevention
Paula Forrest National Office for Suicide Prevention
Professor Tom O’Dowd Public Health and Primary Care, Tallaght Hospital
Professor Veronica O’ Kane
Department of Psychiatry, Tallaght Hospital and Trinity College Dublin
Dr Peter Whitty Head of Tallaght Mental Health Service
Dr Hester O’Connor HSE Managing Psychologist Tallaght/Kildare
Dr Oliver Quinn GP
Aine Moloney HSE Physiotherapist
Anna Lee CEO, South Dublin County Partnership
Samantha Whelan Project Manager, Headway
Emma Freeman Manager of Tallaght Jigsaw
Throughout the report, the assessments/conclusions reached are based on combining evaluation methodologies (e.g. evaluation sheets, focus groups, one to one interviews) unless otherwise stated.
1.4 Acknowledgements
This report has been prepared with the full cooperation and assistance of all of agencies involved in
the Mojo Advisory Group, South Dublin County Partnership and the Mojo Programme Co-ordinator.
We would like to thank all the stakeholders who readily and willingly engaged in the evaluation process over an eighteen month period.
In particular we would like to express our sincere thanks to the men involved in the three pilot Mojo
projects, who participated so willingly and openly in this process. Their openness, engagement and
honesty were invaluable to the process.
Finally we also thank Derek McDonnell, the Mojo Programme Co-ordinator and the evaluation sub group (Derek, Marjo Moonen and Nuala Whelan) for their guidance and support in the completion of
this report.
Rita Burtenshaw, MSc. Susan Bookle, MBS
Burtenshaw Kenny Associates

11
2. Context
2.1 Mental Health and Suicide in Ireland
The level of death by suicide in Ireland is increasingly recognised as a key concern nationally. In 2010, the most recent year that figures are available, there were 485 deaths by suicide in Ireland.4
This equates to almost ten deaths per week of which approximately 80% are men. While the figures showed a slight decline on the previous year, the level of death by suicide particularly amongst young
men, is very high by EU standards. In addition, there are substantial deaths recorded by men aged
40-49 and women 50-59 nationally.
The rate of self-harm was 12% higher in 2012 than in 2007 the year prior to the onset of the recession. As self harm is a recognised as one of the greatest predictors of suicide this increase is
concerning.5
Factors such as unemployment, economic deprivation, substance misuse, and isolation are linked to
suicide. There is increasing awareness and emphasis being placed on the link between the recession and associated unemployment to death by suicide. The need to prioritise suicide prevention
programmes during economic recession has been recommended in recent studies carried out by the
National Suicide Research Foundation.6 While to date most of the national discourse has tended to concentrate on the levels amongst young people there is a growing awareness nationally of the
vulnerability to men over the age of 40 to death by suicide.7
The National Office for Suicide Prevention (NOSP) oversees and monitors “Reach Out” - the current national strategy guiding suicide prevention in Ireland. It has a role to oversee the development of
responses with regard to:
General population levels
Targeted groups
Response to suicide when/where it occurs
Ongoing research.
This strategy was developed a number of years ago, prior to the onset of the current recession.
Therefore, the level of unemployment and its impact on mental health was not to the forefront of this national strategy. However, this strategy outlines the need to build on existing initiatives and to pilot
new initiatives that work directly with local and national groups representing unemployed people.8
A new strategy is currently being developed by NOSP. It is likely that this will build on work and
learning to date which includes: work to roll out evidence based suicide prevention training programmes such as ASSIT and Safetalk, developing county wide prevention/response plans and to
build on the role and to increase the numbers of Suicide Resource Officers nationally. In addition the changed external environment and those most at risk of suicide is also a key consideration.
4 National Office for Suicide Prevention, Annual Report 2012
5 The Irish Association of Suicidology Newsletter, Volume 9, Issue 2, Autumn/Winter 2013 Page 18 6 ibid 7 National Suicide Research Centre, Second report of the suicide support and information system, 2013 8 National Office for Suicide Prevention, Reach Out Irish National Strategy for Action on Suicide Prevention, 2005-2014, Page 64

12
2.2 Unemployment
Ireland is experiencing the most devastating recession in living memory. Since 2008, unemployment
and substantial cuts in public finances have been experienced year on year. While initial signs of stabilisation and growth are occurring, the standardised unemployment rate in November 2013 was
12.5% with 406,200 people on the live register. This is in contrast to the early 2000s when Ireland
experienced full employment prior to the onset of the recession.
Unemployment has impacted more substantially on some cohorts and sectors than others. Construction related industries in particular experienced significant job losses. At the height of the
construction boom, the industry employed almost 400,000 people. This has declined to a little over
100,000.9 While initial signs of growth are being experienced, indications are pointing to a slow but steady economic recovery. It is not projected that the construction sector will increase to pre-
recession levels in the future. Unemployment amongst young people is amongst one of the highest in Europe at 29% compared to 8% in Germany. This is significant because high numbers of well
educated, highly skilled young people are competing for jobs in an increasingly highly skilled and competitive labour market. It is believed that the future economic growth of the country rests on a
knowledge based economy. Therefore there is most likely to be a significant displacement of lower
skilled, less educated people from the labour market which includes large proportions of former construction employees. This presents severe challenges for unemployed men who worked in low and
semi skilled positions in the past.
The services and supports available to unemployed people to engage in up skilling and training have,
and are continuing to change. FAS the former national training authority has merged with the Department of Social Protection. The voluntary nature of engagement in the Local Employment
Service, who previously targeted the most socially excluded, has also changed. Job path, the newly establishing system of contracting regionally based employment supports is currently being
established. Increasingly the emphasis is being placed on employment support providers working with
large numbers of people to achieve employment outcomes. This is largely to respond to the huge volumes of people who are currently unemployed nationally. However, services are increasingly based
on mandatory engagement of unemployed people and services funding is increasingly linked to sustained placement levels.
2.3 Interagency Working
In recent years, increasing emphasis is being placed on agencies from across sectors working
together to respond to complex issues. This is echoed in the most recent NOSP annual report where the National Director of Mental Health Services has stressed the need “to ensure that partner agencies continue to work together to avoid duplication, improve integration of programmes and develop local plans at a community level.” 10
There are a number of definitions of interagency working in the literature but one concise definition that can apply relates to a well-defined relationship or agreement entered into by two or more
agencies to achieve common goals. While there are a wide range of models, they contain a number of identifiable common factors that include:
Leadership
Commitment to interagency working at agency and individual level
Involvement of the right stakeholders
Adequate resources
9 The Irish Construction Industry in 2012 (Society of Chartered Surveyors) 10 NOSP Annual Report 2012

13
Good communication
Training and/or experience of interagency working
Shared clarity in relation to roles, responsibility and remit
A level of flexibility or responsiveness.
In addition, the role of the Co-ordinator or facilitator can also be crucial in successful interagency working.

14
3. Mojo Overview
3.1 History and Rationale for Mojo
Suicide Action West Tallaght, a collaborative interagency initiative under the auspices of RAPID, was successful in securing funding through Dormant Accounts. This funding was allocated to employ a Co-
ordinator to develop a plan to respond to a number of suicides that had occurred in the West Tallaght area. One of the initial tasks for the Co-ordinator was to conduct a needs analysis which identified
that young men and taxi drivers were particular at risk groups in the Tallaght area.
Suicide Action West Tallaght expanded its membership at this time and moved from a largely
community and voluntary sector initiative to a more interagency initiative that included more statutory representatives such as HSE Suicide Resource Officer, MABS, local schools, and elected
representatives. Work was rolled out to increase services in the area and to develop responses
targeted at young people and men particularly those affected by the recession or recently made unemployed. In 2010, South Dublin County Partnership (SDCP) assumed responsibility for the
employment of the Co-ordinator, managed and sustained this initiative while becoming increasingly involved in community health initiatives across Tallaght.
In 2011, opportunities existed to apply for funding through the National Office for Suicide Prevention (NOSP) and through Headstrong to support locally based initiatives. Both funding opportunities
required broader geographical catchment areas than the existing West Tallaght area. Other stakeholders, particularly state agencies also had a preference for expanding the geographic focus.
The Co-ordinator of Suicide Action West Tallaght submitted two parallel applications respectively to:
a) Headstrong - to develop a Jigsaw project aimed at young people under the age of 25 in the Tallaght/Clondalkin catchment area
b) National Office for Suicide Prevention - to establish a collaborative approach to providing
integrated services and supports for men over 25 who had recently been made unemployed
or were distressed as a result of the recession (targeting the wider Tallaght catchment of SDCP). This is now known as the Mojo Programme - a preventative support programme for
men at risk which is the subject of this evaluation.
Both applications were successful. NOSP, which had largely focussed on funding larger, national initiatives, was supportive of the Mojo Programme as a more localised initiative that had the support
of key strategic partners such as the HSE and community voluntary sector organisations. The aim of
providing more integrated statutory and community based supports for men experiencing distress as a result of the recession and/or unemployment was also of keen interest to NOSP.
In tandem, the Jigsaw initiative has been established. The Jigsaw Manager is located in SDCP, is
employed by SDCP and seconded to Headstrong having previously worked as the Co-ordinator of
Suicide Action West Tallaght. While both Mojo and Jigsaw are run independently, both Programme Co-ordinators liaise regularly including with a wider group of SDCP staff, communicating progress and
sharing their experiences in establishing both initiatives
15
3.2 Mojo
The Mojo Programme is a pilot programme funded by NOSP. It was developed to support men who
are affected by unemployment and/or the recession in Tallaght which has increased their risk of ‘distress’.11 This distress is evidenced by higher levels of mental health concerns and can range from
an initial, first experience of lower level mental health issues to substantial mental health concerns
including severe depression and self harm. Due to their mental health distress, such men are at higher risk of suicide.
Mojo was developed as a pilot preventative programme. Significant research took place to inform the
programme design, which was carried out by the Mojo Co-ordinator. Through action research key
issues for men locally were identified including the services and supports already in place and possible programme tools. The content of the programme was based on best practice/research. This initial
period was also used to build relationships and commitment to Mojo amongst key stakeholders. Senior level stakeholders were identified and targeted for participation in Mojo. Leaders emerged,
with significant expertise and profile in the area of mental health. Their input helped inform the programme, give credibility and encourage key stakeholders to actively engage in Mojo. The role and
experience of SCDP was central to engaging stakeholders. The Advisory Group and initial working
groups were established to consider and agree the Mojo programme elements. This time was also used to agree how the agencies would work together and protocols based on recognised best
practice were adapted to underpin client information sharing and interagency working. The name and branding for the programme was also agreed. This was important to attract men to the programme.
While the Mojo pilot programme builds on successful practice from other mental health and inter-agency initiatives, the programme as a whole is new, unique to Tallaght and developed by
stakeholders involved with the support of the Co-ordinator. This preparatory work to design and agree the programme took place over a nine month period from August, 2011 to May, 2012.
The pilot programme was divided into three projects that each initially aimed to include 10 men. However, higher numbers were recruited in response to demand. Each project lasted between 10 and
12 weeks.12
The Mojo Programme aims to respond to the men’s mental health and wellbeing needs as well as to support their education/employment progression.
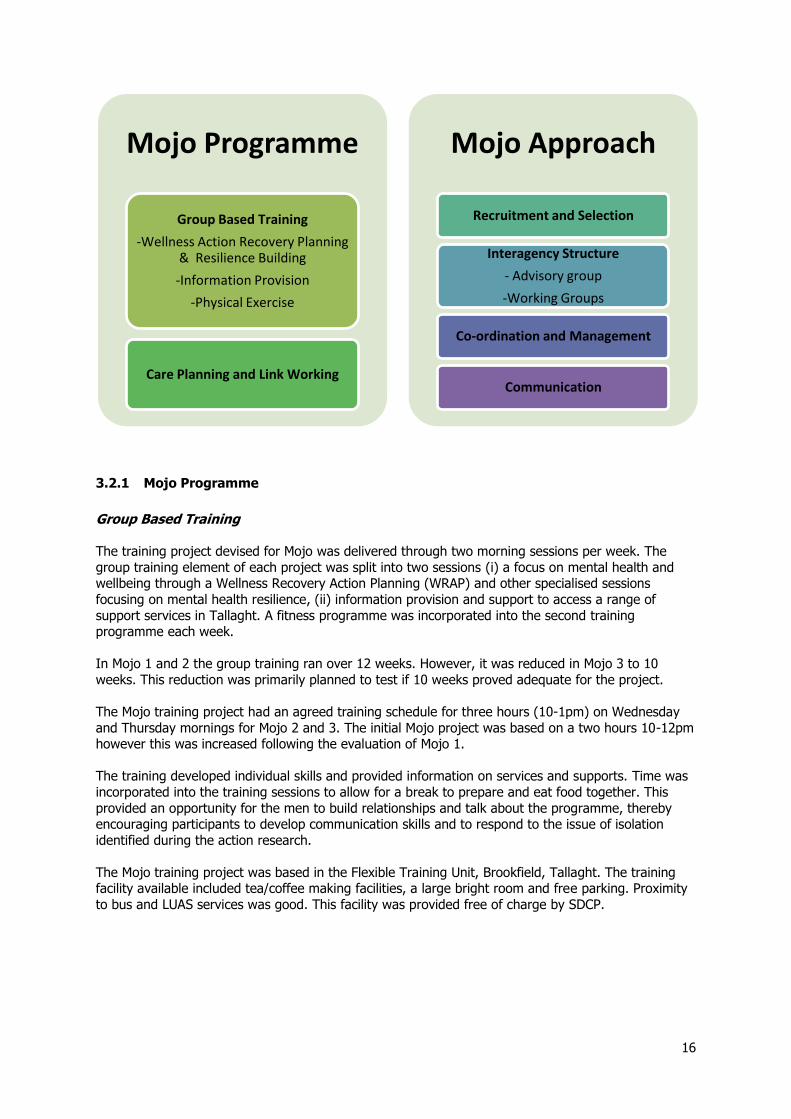
There are a number of components to Mojo, which are presented as follows:
11 Taken from Mojo Project manual 12 Mojo 1 and 2 took place over 12 weeks; Mojo 3 took place over 10 weeks.
16
3.2.1 Mojo Programme
Group Based Training The training project devised for Mojo was delivered through two morning sessions per week. The
group training element of each project was split into two sessions (i) a focus on mental health and wellbeing through a Wellness Recovery Action Planning (WRAP) and other specialised sessions
focusing on mental health resilience, (ii) information provision and support to access a range of
support services in Tallaght. A fitness programme was incorporated into the second training programme each week.
In Mojo 1 and 2 the group training ran over 12 weeks. However, it was reduced in Mojo 3 to 10
weeks. This reduction was primarily planned to test if 10 weeks proved adequate for the project.
The Mojo training project had an agreed training schedule for three hours (10-1pm) on Wednesday
and Thursday mornings for Mojo 2 and 3. The initial Mojo project was based on a two hours 10-12pm however this was increased following the evaluation of Mojo 1.
The training developed individual skills and provided information on services and supports. Time was
incorporated into the training sessions to allow for a break to prepare and eat food together. This
provided an opportunity for the men to build relationships and talk about the programme, thereby encouraging participants to develop communication skills and to respond to the issue of isolation
identified during the action research.
The Mojo training project was based in the Flexible Training Unit, Brookfield, Tallaght. The training facility available included tea/coffee making facilities, a large bright room and free parking. Proximity
to bus and LUAS services was good. This facility was provided free of charge by SDCP.
Mojo Programme
Group Based Training
-Wellness Action Recovery Planning & Resilience Building
-Information Provision
-Physical Exercise
Care Planning and Link Working
Mojo Approach
Recruitment and Selection
Interagency Structure
- Advisory group
-Working Groups
Co-ordination and Management
Communication

17
a) WRAP & Resilience Building
WRAP is an established evidenced based approach aimed at supporting people experiencing mental
health issues. WRAP shifts the focus of mental health care from “symptom control” to prevention and recovery. It helps people take responsibility for their own wellness by using a number of self-help
techniques and to utilise support from family, friends, and service providers. WRAP supports people
to identify what makes them well, to use their own wellness tools to relieve difficult feelings and maintain wellness. It has a number of key elements which include: wellness toolbox, daily
maintenance plan, identifying triggers and action plan, identifying early warning signs and action plan, when things are breaking down and action plan, crisis planning, post crisis planning.13 This
programme is recognised internationally as being very successful in working to respond to mental health challenges.
As part of the preparation to establish Mojo, five Advisory Group (AG) members participated in training on WRAP. In addition, another AG member was already a practicing WRAP facilitator. The
WRAP element of Mojo was led by two trainers at all times. The lead trainer in all Mojo programmes was consistent and had experience of delivering WRAP. As Mojo rolled out, further WRAP training
amongst agencies took place. This is outlined in Section 4.1.1. below. The WRAP and resilience
building element of the training took place on Wednesday mornings. As Mojo developed additional elements were added to the WRAP sessions to enhance and compliment them. These included
mindfulness, managing anxiety, men’s role in the family, social supports and self-esteem. The Copeland Centre, who oversee the implementation of WRAP in Ireland, is supportive of Mojo adding
to WRAP as part of the programme as long as fidelity to WRAP was maintained. Therefore, as the programme evolved WRAP was complimented by a range of additional elements to support mental
health resilience.
b) Information Provision and Physical exercise
The information provision and support aspect of the training programme was delivered by relevant
service providers, a number of whom are directly involved in the Advisory Group with others linked to the programme through their respective agencies’ involvement. These sessions aim to provide men
with an opportunity to become aware of services and supports available to them in Tallaght, to clarify how to access services, and to raise questions directly with service providers. These sessions included
inputs from the Local Employment Service, Tallaght Adult Education Service (Dublin and Dunlaoighre
Education and Training Board), the Department of Social Protection, MABS, and the Volunteering Centre. The information provision aspect of the training took place on Thursday mornings.
Mojo 2 and 3 included an hour of physical exercise to end the Thursday morning sessions. This aimed
to increase awareness and give men experience of physical fitness.
A sample training programme is outlined in appendix one.
Care Planning and Link working Four members of the Advisory Group were involved in care planning and link working (formerly key
working) with participants throughout each project. In addition, a colleague of one AG member and
the Programme Co-ordinator were also involved. All Mojo participants were allocated a link worker. The primary role of this element of the programme served to link individual participants into agreed
services, co-ordinate service delivery, liaise with other key workers as required, provide feedback to the participants, ensure documentation was complete and to develop care plans. The individual care
plans identify individual needs. Care plans aim to act as a practical response to presenting issues and clarify the progression path towards work, education and/or other services.
In July 2012, it was agreed that the Mental Health Recovery Star would be trialled as a key assessment and care planning tool for participants on the Programme. This is one of a set of tools
13 Taken from www.wrapireland.ie and www.copelandcenter.com

18
developed in the UK for care planning, which has become more widely used and recognised as a way
of working with clients in Ireland by health professionals. None of the agencies in Tallaght had used the Recovery Star in their work to date. With the exception of one link worker, all participated in
training delivered by the originators of the Recovery Star from the UK. Interviews highlighted that not all link workers had previous experience of key working and using care planning tools.
Using the recovery star, participants and care planners awards a score from one to ten, with ten being highest across ten areas.
Managing mental health
Physical health and self care
Living skills
Social networks
Work
Relationships
Addictive behaviour
Responsibilities
Identity and self esteem
Trust and hope
A visual star is used to work with clients to determine which score is appropriate to their situation and this aids discussion and planning to work to increase the areas that require prioritisation. The star is
used at intervals to determine if progress has been made or if other areas require prioritisation.
Throughout the Mojo pilot phase the link workers met as the Care Planning Group to discuss
participant progression and to support link workers in their work with the men. The protocols agreed at project design phase, underpinned how information would be shared.
19
3.2.2 Mojo Approach
Recruitment and Selection Agreed criteria for participation on the Mojo Programme specified that men should be:
a) Directly affected by the recession and/or unemployment, which has increased their risk of distress
b) Motivated to work on change so that they can improve their work and social life c) Aged 25 years or older (if the course is oversubscribed, men aged 40 and over will be given
preference) d) Reside in the Tallaght area (changed to South Dublin County)
e) Have the capacity to take personal responsibility for themselves and agree to attend the full
12 week programme.
A number of methods including posters and flyers were developed to inform and promote the Mojo project. These were slightly adapted from project to project, but were visible and widely distributed
amongst stakeholders to publicise across Tallaght and through relevant national forums. GP surgeries
were targeted as part of the publicity for each project. (See appendix three for a sample poster)
At the initial stages the Co-ordinator met with the GP network in the area to highlight the programme and build links with GPs. This took considerable time to organise and took place as part of the initial
programme planning phase and was supported by key Advisory Group members. Links with GPs were established through this process which was important given their access to the programme target
group.
It was anticipated from the outset that the agencies involved in Mojo would play a key role in
supporting the recruitment process in addition to self-referral. All applicants were called for a short interview with the Project Co-ordinator to discuss Mojo prior to taking up their place.
Interagency Structure
The interagency aspect of the programme is central to Mojo. This includes the development of relationships, increased understanding, and referrals between agencies. In particular, linking the HSE
services to those in the community and matching labour market and therapeutic services more closely
to men’s requirements is a key aspect of the Programme.
a) Advisory Group
An Advisory Group (AG) composed of agencies from statutory, community and voluntary sector organisations in Tallaght was established to advise and guide the Mojo Programme. In addition, ad
hoc Working Groups were developed to progress specific aspects of the Programme.
b) Working Groups
As outlined in section 3.2 interagency protocols were agreed at an early stage to underpin
collaborative working. These protocols were developed by a Protocol Development Working Group
comprised of AG members who considered existing information sharing protocols (e.g. those developed by Equal Ballymun, Hidden Harm Northern Ireland, ARM, and the South Dublin Children’s
Services Committee) which were then adapted to fit with Mojo requirements. The reference manual developed as part of the project development phase outlines the detail of the protocols agreed, in
addition to detailed terms of reference which underpins the role and functioning of all management/co-ordination aspects of the programme.
Three working groups have been established to date: the PDG working group (outlined above), the care planning and link working group and a post Mojo working group.
20
Co-ordination and Management
South Dublin County Partnership (SDCP) is responsible for managing the programme and providing
the training space in the Flexible Training Unit, Brookfield. A Programme Co-ordinator is employed by SDCP on a part-time basis to support management and co-ordination. He is line managed by, and
reports to, the CEO of SDCP. In late 2012, additional funding was secured from NOSP to provide
administration support, and to employ a part-time Project Support Worker, who was responsible for implementing elements of the programme and supporting the development of the Men’s Shed which
is outlined in more detail in section 4.4.1.
Communications As this is a newly established programme, a range of communication tools and mechanisms were
envisaged from the outset. This included the development of a communication strategy to publicise services and supports.
3.3 Organisations involved in Mojo
Tallaght has a number of well established services and supports which include:-
Community Addiction Response (CARP): Provides a range of services and supports to drug
users. Department of Social Protection: There is a local DSP office providing a range of social welfare
and training supports. Tallaght Adult Education Service (Dublin and Dunlaoighre Education and Training Board formerly the VEC): Provides a broad range of adult educational services (including BTEI and VTOS)
which are primarily aimed at the long-term unemployed.
General Practitioners: There are currently 42 GPs on the network list that provide GP services in
the Tallaght area.
HSE Mental Health Service: Provides a range of supports to people experiencing mental health issues.
HSE Primary Care Teams: Teams of health professionals working together to provide a co-ordinated health service in Tallaght. The PCT social worker responds to non-emergency referrals for
suicide ideation. An anxiety clinic management group has been established in Tallaght.
HSE Support after self harm: A HSE service that provides follow up in a community setting to
people presenting to Tallaght A&E with self harm and/or suicide ideation.
Jobstown Assisting Drug Dependency (JADD): A purpose built drug treatment centre which offers a range of services and supports to drug users and their families. A men’s support group and
mentoring service is part of the service offered through JADD.
Pieta House: A non-profit organisation providing a specialist treatment programme for people who
have suicidal ideation or who participate in self-harming behaviours. There is a free outreach service operating in Tallaght, with three therapists offering 16 hours of counselling per week.
Shine: The national organisation working to support people who experience schizophrenia.
South Dublin County Partnership: Provides a range of support targeting socially excluded people. There are a number of targeted services to support people to progress into the labour market. These
include (a) the Flexible Training Unit which offers intensive training for unemployed men. This training project is adapted to meet participant needs; and, (b) the Local Employment Service which

21
offers mediation supports and a range of services for the unemployed in Tallaght. Further, the SDCP
have considerable experience in leading and supporting interagency collaborative initiatives.
South Dublin Sports Partnership: Provides a range of supports to engage people in physical activity. This includes Link 2 B Active which offers unemployed people the opportunity to use local
sports facilities at low rates (gyms, swimming pools, all weather pitches, Pilates, zumba).
South Dublin County Council Social Work: Works with people who are experiencing housing
issues locally. Tallaght Local Drugs Task Force: Co-ordinates responses to alcohol and drug addiction in line with the National Drugs Strategy.
Threshold Training Network: Provides a training project, cafe, and other supports to people experiencing mental health issues.
Village Counselling Service: Operates a confidential counselling service from two locations in
Tallaght. There are 140 counselling sessions available per week. All staff are ASSIT trained.
In addition, the area has a range of other relevant services such as Citizens Information Service,
Volunteer Centre, Money Advice and Budgeting Service, Family Resource Centre, Tallaght Hospital, and Tallaght IT.
The funding for the Mojo Programme through the National Office for Suicide Prevention was due to
expire on 31 December 2013. However NOSP, due to their interest in the initial outcomes emerging
from the formative evaluation process, have allocated additional resources to extend the pilot until June 2014. This will allow for two additional Mojo projects and to extend the employment of the Co-
ordinator. Longer term financial support is not committed at this point.

22
4. Evaluation Findings - Mojo Programme
This section outlines the evaluation findings in relation to:
4.1 Group Based Training
This section aims to outline the Group Based Training elements of Mojo. This includes a brief description and assessment of WRAP and of the information provision aspect of training
4.1.1 WRAP & Resilience building
The WRAP programme ran on Wednesday mornings and was primarily based on the Wellness and Recovery Action Planning programme (WRAP) - an established evidence-based approach to
supporting people experiencing mental health issues outlined in Section 3.2.1. It concentrated on mental health, wellness, understanding and responding to triggers. However this element of the Mojo
project was refined and added to as the programme rolled out to include and emphasise topics such
as anxiety, men’s role in the family, social supports, self-esteem, and mindfulness. These adaptations were honed by feedback from participants and reflection at the end of each Mojo project. As outlined
in section 3.2.1 these additions elements of the programme. The Copeland Centre, through their Advanced WRAP Facilitator, was made aware that Mojo were adding to WRAP, while also retaining
the fidelity of the programme.
Attendance by participants on the WRAP and Resilience Building element of the programme averaged
eight men per week across all three Mojo projects. The evaluation of each project highlighted that this element of the programme was exceptionally popular and that the participants found it very
beneficial. It was highlighted that this part of the programme gave participants an understanding of how to understand and manage their emotions, combat anxiety, and deal with anger. The men
interviewed highlighted that for the vast majority it was the first time that they had explored their
behaviours and feelings. WRAP and Resilience Building enabled them to develop the skills to respond constructively to difficulties as they emerged.
Mojo Programme
Group Based Training
-Wellness Action Recovery Planning & Resilience Building
-Information Provision
-Physical Exercise
_
Care Planning and Link Working

23
Wednesdays were very beneficial. A lot of great things were covered. I know that I can talk, that it’s ok. The WRAP programme was very interesting. In the beginning I thought that part wouldn’t be for me and I didn’t know if I would stick it out, but as it went on I really looked forward to Wednesdays. I realise that I have worked physically and very hard all my life to earn a living for me and my family but I never worked on myself to develop emotionally. That has been a big learning. Men in general that I know have the same gap but women are much more in tune with themselves”
Quote from participant, November 2012 ”I now understand stress. I didn’t really know that was mainly why I wasn’t sleeping. I also learnt that it’s really, really, important to deal with. WRAP was great.”
Quote from participant, September 2013 “Mojo has given me a language to help describe how I feel. That has been great. I didn’t have that before and didn’t really know what was going on, and what to do. The way WRAP was delivered made it easy for me to ask questions and to tease things out. I feel much more in control.”
Quote from participant, September 2013
Participants across all three projects linked their engagement and the general success of the
Wednesday sessions to the training delivery method. The experience and processes used by the lead
facilitator to engage and work with the group were especially noted. As stated in Section 3.2.1, participants in Mojo 1 had 24 hours of WRAP and Resilience Building, Mojo 2 (36 hours) and Mojo 3
(30 hours). Irrespective of the time allocated, the participants on all Mojo projects indicated that they would have benefitted from additional sessions. This was linked to their enjoyment and learning
gained from this element of the programme.
In addition to providing WRAP to Mojo participants, the organisers of Mojo have provided three WRAP
courses to frontline staff working in Tallaght and Clondalkin in 2013. These staff members were primarily from Tallaght Adult Mental Health Service, Traveller CDPs, and South Dublin County Council
and community organisations. These (four x three hour) sessions enabled workers to develop their
own plan and provided the first step to becoming a WRAP trainer. As the lead facilitator on Mojo WRAP and the Mojo Co-ordinator participated in Advanced Facilitator Training they can also now train
the trainers. Therefore, their participation at the initial WRAP training, experience of delivering WRAP as part of Mojo and further WRAP training is developing the skills within Tallaght to train staff and to
roll out WRAP with clients who experience mental health challenges in a variety of settings.
4.1.2 Information Provision and Physical Exercise
The Thursday morning training sessions focused on providing information on available services and
supports. These sessions were initially of two hour duration but were increased to three following the Mojo 1 evaluation. Since the employment of the Project Support Worker, these sessions were
organised as part of his brief. Sessions were delivered by relevant agencies who were mainly involved in the Advisory Group. Thirteen facilitators delivered this aspect of the programme in Mojo 1 and 2,
with ten in Mojo 3 (as it was a shorter programme). Following from the Mojo 2 evaluation, increased
emphasis was placed on providing information on education, training and returning to work.
Participants across all Mojo projects were also very satisfied with the Thursday morning training sessions. They liked the information provision element and it provided an opportunity to raise
questions directly to services. Feedback on the process was largely highlighted as positive and it was generally felt that the agencies connected with the group providing information in an easily accessible
way. Interviews highlighted that this aspect of Mojo made participants more aware and confident in
accessing services and supports. Mojo 2 and 3 participants were particularly keen to get information on next steps, particularly education/training in order to return to the employment ladder. However,
24
at times, participants felt that there was a great deal of information to take in during a short space of
time.
A number of men in Mojo 3 expressed concerns relating to the level of understanding that employment support agencies have of their needs, interests and experiences. It was highlighted
when men had interviews with employers, they felt that their experience, interest and skills did not fit
the positions and differed significantly from the initial interviews with employment support agencies. The men highlighted how demoralising this could be in adding to a sense of hopelessness at times.
However, they also outlined that Mojo helped them to raise questions with agencies and to take more control of their future.
Men who had been self-employed highlighted the anomalies that they experience when trying to
access state support. Due to their status they are not automatically entitled to any welfare supports
when spouses work due to the level of their PRSI contributions which are lower than PRSI. They are unclear about their status as they are not officially “unemployed” and yet are not in the workplace.
This has a major impact not only financially but emotionally. This was particularly acute for the older men who ran their own business for many years. Such issues were primarily highlighted in Mojo 1.
As with Mojo 2 an additional hour was allocated to Mojo 3 (Mojo 1 ran for two hours, Mojo 2 and 3 ran for three on Thursdays). This was used to develop a physical exercise programme, led by South
Dublin Sports Partnership (SDSP), and ran by an independent trainer who works for SDSP in a nearby gym. This element of the programme allowed participants to engage in physical activity in a
structured, supported way. For some participants it had been a long time since they engaged in physical exercise, others were more physically active. However, the majority of men in Mojo 2 and 3
did not exercise regularly.
The physical exercise component of the session had mixed responses, but generally there was
agreement that time taken to increase physical activity is positive with some continuing to build their fitness and paying more attention to their diet as a result of this aspect of the Programme.
“I was stuck in a boring job for 20 years. Nobody asked me my point of view; I just turned up and felt like a machine. I was made redundant at Christmas, I didn’t know what to do, where to turn. I was panicked. The timing of Mojo was great; I started in February and am looking forward. I want to work but don’t want to go back into that type of environment. I want to learn and have a job that matters, that is what I would like help with.”
Quote from participant, March 2013 “There is a lot of information out there. I now have my CV updated and have started to really look for jobs. I even went for an interview last week. I didn’t get the job but I am back out there which is as a result of Mojo.”
Quote from participant, September 2013 “Going to the gym was great. I had stopped looking after myself physically. Doing a bit of weight training made me feel positive. It was good to get out with the lads, have a chat, do some exercise and go home. I am now much more open to physical exercise and can see how it might help.”
Quote from participant, November 2012

25
4.2 Care Planning and Link Working
This section aims to outline and assess the care planning and link working element of Mojo. All Mojo
participants were allocated a link worker and the Mental Health Recovery Star was used to underpin
the care planning process.14 The care planning process aims to agree a plan to work to identify priorities and agree on ways to address issues/challenges that are blocking progression. The
Recovery Star provides a framework to guide and support care planning.
Six link workers were allocated participants to support through the care planning process. Throughout
Mojo, the way that workers linked and worked with participants changed. Initially, workers checked in three times on a one to one basis with weekly telephone calls. By Mojo 3 this contact had reduced to
two one to one meetings and telephone calls on a needs basis as it was discerned from Mojo 1 and 2 that link workers did not find weekly contact necessary.
The care planning and link working element of the programme was very successful in Mojo 1 and 2.
However, in Mojo 3 this aspect was less successful with the majority of participants in interview
outlining dissatisfaction. Only 55% of participants completed the Recovery Star Process, in contrast to Mojo 1 and 2 where all participants were fully engaged in this process. It is not fully clear why this
was the case but it could be attributed to a) the reduced time frame of Mojo 3 from 12 to 10 weeks; b) the complexities presented by participants on Mojo; c) the increasing pressures on link workers
due to cuts in their own services and increased demand; d) running the programme over the summer
period which is traditionally the time when people take leave/holidays; and, e) challenges associated with maintaining intensive commitment to Mojo.
Throughout the Mojo pilot phase the link workers met as the Care Planning Group. Overall, these
meetings were seen to support the care planning process and the link workers. Those involved in link
working are key individuals within Mojo, as all are actively engaged with the Advisory Group. One particular issue that did emerge in Mojo 3, which tested the definition of child protection, was
addressed effectively by applying the established protocols.
4.3 Mojo Outcomes for Participants
This section outlines the outcomes for participants involved in Mojo. It is based on the interviews, focus groups, evaluation sheets, and an overall assessment of the Recovery Star.
“Before I started Mojo I felt like I was looking in at the world. It was like a foggy window and I was looking in. Now I feel part of the world around me. I am part of wider society. It’s very hard to describe how positive this feels.”
Quote from participant, September 2013
The following visual star outlines the combined assessment from the Recovery Star tool used to guide the link working and care planning process for the three Mojo projects. Green indicates the
assessment for all participants at commencement of the programme, and blue at the end of the
programme. Positive change occurred across all elements for participants who used the tool. The combined report available from all three Mojo programmes highlights that a substantial increase was
recorded for 54% of participants with 29% indicating a small increase and 17% recording no change.15
14 The terms of reference for the link workers is outlined in the Mojo Reference Manual. Full details on the recovery star are available from www.staronline.org.uk or from the Mojo Co-ordinator. 15 The combined recovery star report provides the data used in this section of the report. It is based on the overall assessment of clients of the three Mojo pilot programmes.

26
Across each scale there were different levels of change. Physical health and self-care and managing mental health scored highest with 83% and 79% of men respectively outlining an increased score.
Identity & self-esteem increased for 71% of participants and social networks increased for 75% of participants. The lowest increases occurred in living skills - increases for 33% of participants;
however the initial assessment indicated that the original baseline was high. The following outcomes
for participants on the project were established:
Participants across all three projects highlighted that they understood stress and anxiety much
more clearly as a result of Mojo. This linked to the recovery star where 79% of the men overall experienced an increase in their ability to manage their mental health.
“I got what I wanted and so much more from this project. I was in a very bad place. I am more confident, I can go to the Square. Before this I just sat in all day so getting out and being here in itself was a real achievement. However, the biggest thing is that I am now a real father. Before this when I saw my son, I put him in front of the TV and turned on play station, now we go to the park, go to the cinema we even went swimming. I feel so happy that I can be a real dad. Mojo gave that to me. I am determined to keep going.”
Quote from participant, November 2012
Men also experienced significant progress in physical health and self care with an increase
recorded for 83% of the participants. Interviews highlighted that men placed more emphasis on their appearance and that the physical exercise component to the project was an important

27
factor in supporting this. This was also visible when meeting with the men at various stages
throughout the evaluation process as a number looked healthier and took more care of their appearance.
“I know what stress is now and that it can kill. I mind myself much more and Mojo has taught me that it’s ok to look after myself and that this is very actually very important to do”
Quote from participant, September 2013
“I hit a bad patch last week. In the past when this happened I spiralled down and started to drink. Then I would go really off the rails often for months. This time I focussed on getting through the weekend and got myself together to go to Mojo on Wednesday. I am proud that I managed to do this and am starting to come out the other side. I kept thinking of WRAP and meeting the lads. I know now that there are other ways to deal with stresses and bad times”
Quote from participant, May 2013
Participants highlighted strongly at interview that their self-esteem and identity had improved
since the commencing Mojo and had increased for 71% of participants. This was consistent
across all projects. Participants noted that they had a greater sense of themselves and awareness of how to respond in different situations. They also indicated that they were able to
challenge and ask questions more effectively.
“I have always been really quiet, I don’t say much. This has a big impact, at school I never spoke, in relationships I didn’t say much - I have been ignored my whole life because of my shyness. However, I should say I was! I can’t believe what’s happened in Mojo - I keep hearing myself speak and I have lots to say. I have never said so much!! I was in such a bad place last Christmas before Mojo, my marriage broke down. Now I am talking, asking questions, enjoying the banter - it’s like there is a new, more confident me. My mental health is so much better and I have hope for the future again.”
Quote from participant, March 2013
“My client’s mood picked up noticeably. He has experienced substantial loss which has impacted on every aspect of his life. For the first time he is really talking about this. While we haven’t discussed the day to day detail of the project, but he tells me how positive the project is. I think that it has “Given him his Mojo back!” He is not as angry and meeting with other men in the context of the project is very beneficial as this man was very isolated. I would certainly refer again as this has been exceptionally positive.”
Quote from interview with senior stakeholder who referred onto the project, November 2012
Participants in all projects highlighted that social networking increased through interview.
The Recovery Star highlighted that social networking increased for 75% of men overall.
The men involved in Mojo highlighted increasing ability to trust. On commencing Mojo a
number of participants were very angry and found it difficult to envisage change. However, on finishing the project a number highlighted through interview that they were now regaining
control and were more optimistic. Overall, the Recovery Star noted a 71% increase in trust
and hope.
“ Before Mojo I was so angry at what happened to me. I couldn’t deal with it. Mojo has helped me to let go. I am accepting that things have changed and while some things are not fair, I am moving on. This wouldn’t have happened without Mojo.
Quote from participant, November 2012

28
Participants also highlighted their increased motivation to work. This was measured by a
58% increase overall. However, a number of men outlined that agencies supporting job seekers needed to start listening to men like them and respond more appropriately to their
needs.
“I am back looking for jobs again. I got my CV done and I even got an interview last week. I didn’t get the job, but I am back out there trying again. This is major. I have a course lined up after Mojo so I think that will keep me focussed on building up my skills.” “I had an interview yesterday. I really concentrated on getting ready, thinking about what to say, how I looked and so on. I had to get two buses there and when I arrived I found out that the job was completely different to what I had been told. It is not a job that I have any interest, skill in or could really do well. I was so disappointed and then I got angry. What a waste of time and money. Was anybody listening? Why shove me in there is it just to tick a box? However I thought of WRAP. I need to ask these questions but I am determined not to be as angry as I would have been. I am also going to keep on looking now.”
Quotes from focus group, September 2013
Participants highlighted that they enjoyed Mojo. They found it relaxing, enjoyable, and fun.
This was largely in part to the facilitator’s delivery of the project and the atmosphere created
which allowed them to fully participate. Interviews had highlighted that many had not laughed regularly prior to their participation on Mojo.
The men also outlined that they are taking steps to build on Mojo and progress onto other
opportunities. This is exceptionally positive.
29
4.4 Mojo outcomes for Partners
The partners interviewed all outlined deep concerns about the mental health and wellbeing of their partners prior to their participation on Mojo. They were exceptionally positive about Mojo and the
impact that it had not only for their partners themselves but more generally. The assessment of the
interviews highlighted that:
The men benefited immensely, from Mojo, the were generally more positive, less isolated, felt
more confident, had made friends, were managing their mental health much better and were more optimistic for the future. This fits with the participant assessment outlined in the
previous section.
The men were more open and spoke more to their partners about their concerns, worries and
discussed plans for the future. As a result of Mojo, the men were more engaged at home with their children. They were
more involved and interested in their lives, interests and challenges.
Mojo gave participants time to reflect, to come to terms with unemployment and isolation
that they experienced since becoming unemployed. The partners outlined that the men were less angry and happier. They had changed and were
far more optimistic and able to deal with challenges more effectively.
“ I didn’t really know what Mojo was about when he started. I didn’t expect him to come on so much. He has changed for the better, he has far more energy, is happy and home life is much better. The difference is amazing.” “My husband has really opened up. He talks alot more about himself, how he is feeling and he uses different language to express himself. He definitely learned that through Mojo. Overall his attitude is much more open to new things, new ideas a new future. I think that this programme has supported him through a really tough time and he is in a much better place since he started on Mojo.”
Quotes from interviews December 2012 and July 2013
4.5 Mojo outcomes for key external stakeholders
The assessment of the interviews of referrers to the programme, and key external stakeholders highlighted that:
Those interviewed were not aware of a similar programme in Ireland. While elements of Mojo
exist, the programme as a whole is, in their view, unique.
Many community based programmes, offer alternatives to medical treatment, this programme
is however actively working with medical professionals and is complimentary to treatment. Mojo is the only community based programme that the Tallaght Mental Health Service refers
to. This is due to the quality of the programme, the involvement of medical professionals in
the design and roll out of the programme and the outcomes from the men involved.
Stakeholders became aware of the programme through colleagues involved in Mojo, the co-
ordinator and Mojo posters. They liked the name, the way that the programme was promoted and the professionalism that underpinned the work.
Mojo fills a real need. There are very limited options available for men who require a
programme to address their mental health and future employment/training needs. Mojo also provides an opportunity for men with varying degrees of mental health issues, from
differing socio economic backgrounds to engage in a programme. This was seen to be very
positive.
Men referred to Mojo positively engaged in the programme. The men became more engaged
in their recovery, opened up, became more positive in their outlook and less angry. They also
30
displayed greater levels of confidence in their abilities. This fits with the assessment by
participants and their partners. Stakeholders noted significant change in their attitude and behaviours over the twelve weeks
that the men engaged in Mojo. For some of the men referred it was the first time that they
had completed a programme which was a significant achievement. The management and co-ordination of the programme was seen to be very efficient and
effective.
All stakeholders interviewed outlined that they would refer to the Mojo projects in the future,
and that they are very keen that this programme continues to develop and be sustained into the future. It is agreed that this programme fills a real need and that the pilots to date
appear to have worked very successfully.
Stakeholders are keen to ensure that the lessons learnt through Mojo are used to influence
national and regional policy and delivery to men at risk of suicide. The profile and impact of Mojo is understood. The collaboration between stakeholders from
across sectors has been very successful. This is particularly notable in the current climate
where resources are generally decreasing and competition for funding exists.
4.6 Post Mojo
This section outlines the progression of participants following their involvement in the Mojo Programme.
4.6.1 Men’s Shed
Plans to establish a Men’s Shed commenced in 2013 as a post programme support for men. This was not included in the original plan or objectives for Mojo, but emerged in Mojo 1 as the men were
fearful of becoming isolated once the project ended. They were aware of the idea of Men’s Sheds and proposed that one be established as part of the programme to support men finishing the programme
and, more generally, as a support for men with mental health challenges. Funding was secured
through NOSP to employ the Project Support Worker who as part of his role supports the development of the Men’s Shed. It is envisaged that the Men’s Shed will be self-sustaining over time.
As part of the establishment of the Mojo Men’s Shed, discussions took place with two existing Men’s
Sheds in Tallaght. It was agreed that given the population and focus of the existing Men’s Shed, that the Mojo Men’s Shed would concentrate on providing a health and wellbeing space for men. While it
aims to engage Mojo participants; it is also open to all men who have an interest in engaging in
activities that support health and wellbeing.
South Dublin County Council was very supportive in identifying a suitable venue - Ardmore Community Centre. This centre contains excellent facilities and is rented to Mojo at a very reasonable
rate.
At the time of the final interviews for the evaluation (October 2013), a core group of eight to ten men
from both Mojo 1 and 2 attend the Men’s Shed on a weekly basis. They have bonded well and use the Men’s Shed primarily as a social space to meet up and tackle isolation. At the time of the
evaluation, the men from Mojo 3 have not started to attend, and it is not clear from the interviews
whether they will begin to link with the Men’s Shed. A facilitator has been employed to develop a more structured work plan for the Men’s Shed but there are concerns that the momentum to develop
the Men’s Shed is declining on the part of both the men and organisers. Numbers are relatively low and the ability of the men to lead and organise is relatively weak.
“Thanks to Mojo I have reconnected with the world again” “The Men’s Shed is one of the highlights of my week. There are great relationships and

31
friendships between the men. It doesn’t matter if you did Mojo 1 or 2 or at all - we have all gelled really well. We can relate to each other. I know when I come here that I can talk, I will be listened to and nobody will judge” “Since I started on Mojo things for me are much better. I get help when I’m down. In the past I just stayed in and self-harmed. I haven’t self-harmed since I became involved with Mojo.” “I have continued to build up my confidence. I am going back to school, I left very early and my reading and writing is very bad. I just found out that I have a place. It’s brilliant. I can honestly say that I wouldn’t have taken that step if I hadn’t become involved on Mojo. It has really changed me.”
Quotes from Men’s Shed focus group September 2013
4.6.2 Progression – Links with other Services and Employment
As of 2 December 2013, the following information was available to determine the progression of participants:
Mojo 1 Mojo 2 Mojo 3 Total
Threshold
Training
3 1 2 6
Tallaght Adult Education
Service
1 1 2
Employment 3 1 (temporary) 4
Community
Employment
1 1 (applied) 2
Training 1 (FETAC level 5 community
involvement)
1 (Aspire internship) 1 (Barber course) 1 (Aware skills
building)
4
Flexible Training Unit
1 2 3
Masters
Education
1 1
Headway 1 1
Dun Laoighaire
Central Remedial Clinic
1 1
Treatment 1 1
Overall, of the 36 men who completed Mojo, 25 have progressed to another service. This is a
progression rate of 70% which is far in excess of accepted national norms. Furthermore, on average
ten men continue attend the Men’s Shed each week. Up to four men have also accessed the Village Counselling Service who had not received counselling support prior to their involvement on Mojo.16 It
must be remembered that prior to Mojo these men were very vulnerable and a large number were very isolated with little connection to the outside world.
16 There is the possibility of overlap e.g. a participant who has progressed to a course, attends the mens shed and engages in
counselling.
32
5. Evaluation findings - Mojo approach
This section outlines the evaluation findings in relation to:
5.1 Preparation and development phase
The initial nine months of the programme were spent developing Mojo. The programme design was
based on research and consideration of what was possible to deliver locally. The Mojo Co-ordinator played a central role in gathering information, identifying key stakeholders locally and engaging them
in the programme. Champions emerged with a national profile, expertise and connectivity with a keen
interest in the programme. This helped to encourage and engage stakeholders locally and to give the programme credibility. In addition, the role of SCDP was important. This Partnership has significant
experience of leading collaborative responses which also helped to engage key stakeholders in the programme. Critical to engaging and encouraging participation was an agreement with DSP that
participation in the programme would not affect welfare entitlements. This initial period was
important in a) agreeing the programme design, b) gaining commitment to participate in the delivery of the programme and in c) establishing the programme structure. This foundation secured
ownership and buy- in and also enabled the programme to roll out within a defined agreed structure. The outputs of this phase are outlined in the Mojo reference manual which underpins the programme.
Mojo Approach
Preparation and development phase
Recruitment and Selection
Interagency Structure
- Advisory group
-Working Groups
Co-ordination and Management
Communication
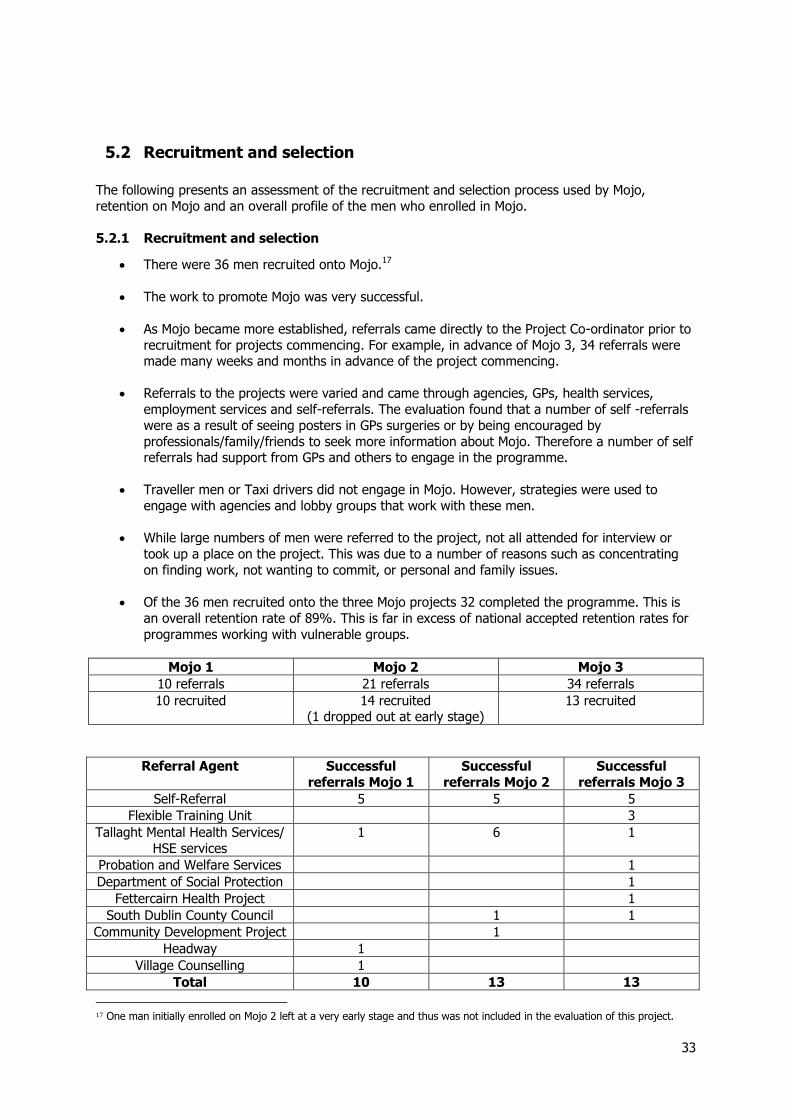
33
5.2 Recruitment and selection
The following presents an assessment of the recruitment and selection process used by Mojo,
retention on Mojo and an overall profile of the men who enrolled in Mojo.
5.2.1 Recruitment and selection
There were 36 men recruited onto Mojo.17
The work to promote Mojo was very successful.
As Mojo became more established, referrals came directly to the Project Co-ordinator prior to
recruitment for projects commencing. For example, in advance of Mojo 3, 34 referrals were made many weeks and months in advance of the project commencing.
Referrals to the projects were varied and came through agencies, GPs, health services,
employment services and self-referrals. The evaluation found that a number of self -referrals
were as a result of seeing posters in GPs surgeries or by being encouraged by
professionals/family/friends to seek more information about Mojo. Therefore a number of self referrals had support from GPs and others to engage in the programme.
Traveller men or Taxi drivers did not engage in Mojo. However, strategies were used to
engage with agencies and lobby groups that work with these men.
While large numbers of men were referred to the project, not all attended for interview or
took up a place on the project. This was due to a number of reasons such as concentrating
on finding work, not wanting to commit, or personal and family issues.
Of the 36 men recruited onto the three Mojo projects 32 completed the programme. This is
an overall retention rate of 89%. This is far in excess of national accepted retention rates for
programmes working with vulnerable groups.
Mojo 1 Mojo 2 Mojo 3
10 referrals 21 referrals 34 referrals
10 recruited 14 recruited (1 dropped out at early stage)
13 recruited
Referral Agent Successful
referrals Mojo 1
Successful
referrals Mojo 2
Successful
referrals Mojo 3
Self-Referral 5 5 5
Flexible Training Unit 3
Tallaght Mental Health Services/
HSE services
1 6 1
Probation and Welfare Services 1
Department of Social Protection 1
Fettercairn Health Project 1
South Dublin County Council 1 1
Community Development Project 1
Headway 1
Village Counselling 1
Total 10 13 13
17 One man initially enrolled on Mojo 2 left at a very early stage and thus was not included in the evaluation of this project.
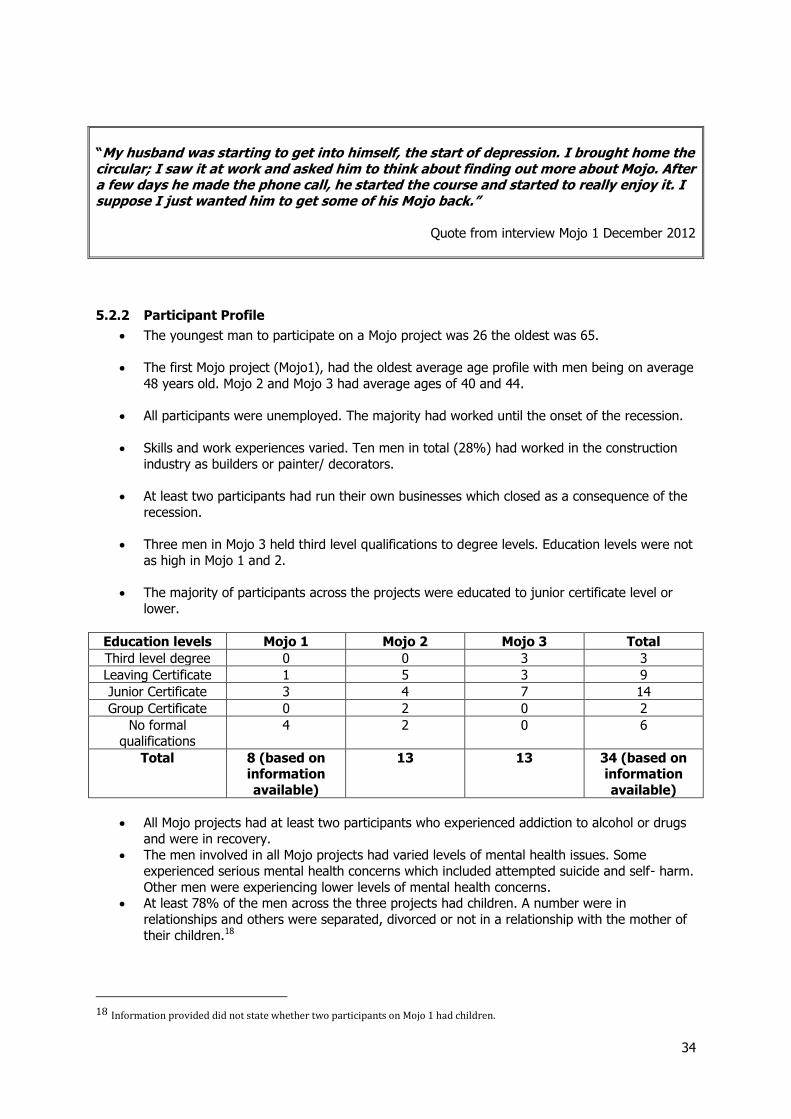
34
“My husband was starting to get into himself, the start of depression. I brought home the circular; I saw it at work and asked him to think about finding out more about Mojo. After a few days he made the phone call, he started the course and started to really enjoy it. I suppose I just wanted him to get some of his Mojo back.”
Quote from interview Mojo 1 December 2012
5.2.2 Participant Profile
The youngest man to participate on a Mojo project was 26 the oldest was 65.
The first Mojo project (Mojo1), had the oldest average age profile with men being on average
48 years old. Mojo 2 and Mojo 3 had average ages of 40 and 44.
All participants were unemployed. The majority had worked until the onset of the recession.
Skills and work experiences varied. Ten men in total (28%) had worked in the construction
industry as builders or painter/ decorators.
At least two participants had run their own businesses which closed as a consequence of the
recession.
Three men in Mojo 3 held third level qualifications to degree levels. Education levels were not
as high in Mojo 1 and 2.
The majority of participants across the projects were educated to junior certificate level or
lower.
Education levels Mojo 1 Mojo 2 Mojo 3 Total
Third level degree 0 0 3 3
Leaving Certificate 1 5 3 9
Junior Certificate 3 4 7 14
Group Certificate 0 2 0 2
No formal qualifications
4 2 0 6
Total 8 (based on information
available)
13 13 34 (based on information
available)
All Mojo projects had at least two participants who experienced addiction to alcohol or drugs
and were in recovery.
The men involved in all Mojo projects had varied levels of mental health issues. Some
experienced serious mental health concerns which included attempted suicide and self- harm.
Other men were experiencing lower levels of mental health concerns. At least 78% of the men across the three projects had children. A number were in
relationships and others were separated, divorced or not in a relationship with the mother of
their children.18
18 Information provided did not state whether two participants on Mojo 1 had children.
35
Men across the three projects highlighted the role that partners and children played in
encouraging and supporting them to participate in Mojo.
“When things were booming, a lot of men like me worked 60-70 hours per week. We didn’t see our kids. We didn’t really know them but we provided for them well. Now we know them really well and almost spend too well at times! So in that way its great being off the treadmill. But it’s hard, really hard. Yesterday it was so hot; I couldn’t even buy the kids an ice cream. That makes me feel bad; my kids do without all the time. Your male pride goes, you spiral down and it becomes hard to see a way out. There must be a balance not an either/or?” “I’m very angry about what’s happened to this country. People like us are just left. Our sense of pride, sense of who we are, what we can do, our routine is just gone. After a while you just don’t know what to do, how to make it better.”
Quotes from focus group, July 2013
5.3 Interagency Structure
This section outlines an assessment of the Advisory Group and other Working Groups.
5.3.1 Advisory Group
An Advisory Group (AG) of representatives from statutory, community, and voluntary sectors working
in Tallaght was established at the commencement of the initiative. AG members were selected based on their experience of supporting mental health, general health, training, education, housing,
employment, financial, social inclusion, or working with men more generally. This occurred at the initial stages of the programme as part of Mojo development and planning. The agencies involved are
outlined in Section 3.3. Tallaght has a strong history of collaborative working, and has been at the
forefront of a number of collaborative initiatives. The SDCP is well established and has managed a number of collaborative initiatives since its establishment over 20 years ago. The AG also secured the
participation and involvement of a representative from Ballymun who has longstanding and recognised experience in supporting collaborative processes.
The AG at an early point agreed their overall aim as well as objectives, outputs, and outcomes as part
of the preparation and development phase. This is detailed in the Mojo Reference Manual. The group
met 17 times (approximately every four to six weeks throughout) from evaluation commencement until conclusion. The AG is chaired by a SDCP representative whose agreed role is outlined in the
Reference Manual. The Programme Co-ordinator supports the chairperson in organising the meetings and minutes with agendas circulated in advance. Meetings generally lasted no longer than an hour
and a half and took place at lunchtime with refreshments available. Time at the beginning of each
meeting is allocated for a brief overview of the role and services provided by one of the AG members on a rotating basis. This aims to build a working knowledge as well as trust between AG members.
The majority of time is allocated to discussing Mojo progress/challenges with space designated for group members to discuss a concern/issue relevant to stakeholders.
Attendance at the AG meetings has been high with an average of between 10 and 13 per meeting
(including the Programme Co-ordinator).19 There are currently 12 organisations represented on the
AG (see appendix two) with eighteen representatives20. Mojo has been very successful in retaining representatives at senior and middle management levels to participate in meetings. Although General
Practitioners (GPs) are not represented on the AG other mechanisms facilitated links with the local GP network. Challenges exist in securing the consistent engagement of labour market support agencies
19 This is based on the initial meeting held in December 2011, and the five meetings held in 2012 20 Representatives from different sections of the HSE and SCDP attend the AG.

36
such as the Department of Social Protection following a number of attempts to secure their
engagement. The core group attending AG meetings are those most actively involved in delivering the projects with the men. However, the last pilot project also found that representatives with key
roles in providing mental health and education supports also participated regularly. There are however, a number of AG members on the mailing list who have not attended many or any meetings.
These include services representing drug users, Traveller men, and the DSP.
5.3.2 Working Groups
Working groups were established to carry out defined roles as outlined in the Mojo Reference Manual.
They disbanded when their role was fulfilled. Protocol – Interagency Information Sharing As outlined in Section 3.2.2, as part of the planning phase, a Working Group was established to
develop interagency information sharing and key working protocols - Protocol Development Group (PDG). The PDG had the role of exploring and making recommendations in relation to interagency
protocols, information sharing, and key working protocols. These protocols are outlined in the
Reference Manual and are based on similar protocols developed in other parts of the country.
Care Planning and Link Working Group
The Care Planning and Link Working group outlined in Section 4.3 was established at the commencement of Mojo 1 and continued to meet since. This group has had consistent attendance
and participation from the AG representatives involved.
Post Mojo
A post Mojo pilot sub group was established in July 2013 with representatives from the AG working
alongside the Co-ordinator. This group met once and has not met since NOSP granted additional funding to extend the pilot phase.
5.4 Co-ordination and Management
As outlined in Section 3.2.2, the SDCP is responsible for managing the programme with the support
of the Programme Co-ordinator whom it employs. The CEO of SDCP is an active member of the Advisory Group, with a senior staff member acting as the AG chairperson. The majority of meetings
and training in relation to Mojo are held on SDCP premises. SDCP played a key role at the initial stages in identifying the stakeholders to target for participation in Mojo and used established
relationships to inform and encourage stakeholders to participate on the programme.
The SDCP are responsible for overseeing and reporting on the funding for the Mojo Programme which
was received through NOSP. In July 2012, the recruitment of a part time Co-ordinator for the Mojo Programme was advertised on a 21 hours per week basis. The core purpose of the post required the
holder to “develop, implement and monitor an inter-agency programme aimed at supporting men ‘at risk’ of suicide because of the recession and or unemployment.” Two elements of the original job
description stated duties and responsibilities which were changed. Firstly, it was originally envisaged
that the Co-ordinator would assess and key work all programme participants. And secondly, to liaise with other agencies in relation to individual care-plans and conduct outreach work where appropriate.
These roles were assumed by the CPG and agreed as part of the planning phase.
The Mojo Programme Co-ordinator has worked on the Programme since the planning stage and has
overseen its implementation with a contract renewed on a monthly basis. The Co-ordinator accesses frequent informal support through the CEO of SDCP and the AG chairperson. In addition, more formal

37
meetings take place between the Mojo Co-ordinator and the CEO on request. External support is also
available. The role involves:
Overall Programme Co-ordination
Programme design
Managing and supporting the Project Support Worker
Promoting and securing referrals onto Mojo
Overseeing and managing the participant recruitment process
Co-facilitating the Wednesday morning training sessions
Link working and supporting men on the project
Organising and supporting the Advisory Group
Organising and supporting the Care Planning Group
Reporting to NOSP
Communicating the programme at key events
Planning strategically for the programme
Funding applications
Administration, with support from SDCP
Funding accessed from NOSP in late 2012, helped to secure a) administration support through SDCP;
and, b) support to deliver aspects of the training project and to establish a ‘men’s shed’ through the
employment of a Project Support Worker to progress aspects of Mojo as it develops.
The Project Support Worker employed in February 2013 was actively involved on the AG and was a trainer/link worker on Mojo 1 prior to his employment. The Project Support Worker retained the
representation of the Village Counselling Service on the AG and was a link worker with participants on
Mojo 2 and 3. In September 2013, his hours were reduced to allow for specialist facilitation skills to plan for the Men’s Shed.
While additional staffing helped to support the Co-ordinator in his role, the demands of the
Programme cannot be underestimated.
“We need to acknowledge the role of the Co-ordinator. He is really committed and really good at managing the Advisory Group. This has been pivotal”
Quote from interview with senior stakeholder, May 2013.

38
5.5 Collaborative working
Collaborative working and developing more integrated systems for men at risk of suicide are a central
part of the Mojo Programme. Throughout the pilot phase a range of agencies have been involved in:-
Participating on management and advisory structures.
Participating on working group structures.
Participating and organising training.
Distributing project information
Supporting project recruitment
Facilitating and leading on aspects of the training project.
Link working and case manage participants.
Supporting the project to communicate its work and progress.
Three online surveys were carried out with Advisory Group members throughout the evaluation process and as shown in the focus groups it is clear that the organisations involved in Mojo are
increasingly working with each other.
Collaboration has occurred in a number of ways - referrals to and from organisations, information
sharing and working outside of direct Mojo auspices. It is noted that the AG has played a key role in supporting increased working and collaborations. All the organisations who completed the last online
survey (September 2013) expressed that they have become more aware of the work and role of the organisations involved in Mojo as a result of their involvement in the initiative. Advisory Group
meetings were seen to play the key role in supporting this increased awareness. The organisations
most involved and who regularly participate in Mojo have higher engagement with the other agencies. However it must be noted that some agencies are specialist and therefore there may not be
a need for them to work with other organisations on an on-going basis.
“Since becoming involved in Mojo I have become more enabled to pick up the phone to
make appropriate referrals. I have become more aware of services and more comfortable
to make referrals. This is not limited to one service; I contact and work closely with a
number that I didn’t before Mojo.”
Quote from Advisory Group focus group, October 2013
“Our organisation is quite specific as we run a structured programme for fifteen weeks. Mojo has made our organisation more aware of other supports that are in the community. This is really helpful and supports transition into other services.”
Quote from Advisory Group focus group, October 2013
The most recent survey (outlined in the evaluation report for Mojo 3) also highlighted that 90% of respondents indicated that levels of understanding, awareness and links with Mojo by other staff
members within their organisation was either very good or good. This increased from a previous 75%
39
in March 2013 in the Mojo 2evaluation. There was also a high level of respondents indicating that the
organisations involved in Mojo actively work to increase co-operation and collaboration.
Throughout the evaluation process it has been highlighted that the role that GPs play is important to the success of Mojo. While GPs are not actively involved at AG level, the Programme is well
connected to local GPs through the GP network. The HSE representatives on the AG have played a
key role in supporting this development. This has led to referrals onto the Programme and promotion of the programme through GP surgeries as highlighted in Section 5.1.1.
“I saw Mojo in my doctor’s surgery. There was a poster and I talked to my doctor about it. I then made the call and here I am. I don’t look up the internet or any of that, so catchy posters are the way to get to men like me. Having the poster in the doctor’s was a great idea.”
Quote from focus group, July 2013
5.6 Communication
This section assesses the project’s internal and external communication.
5.6.1 Internal Communication
The primary connector for communicating to all stakeholders involved in the programme was the
Programme Co-ordinator with back up support available from South Dublin County Partnership administration. Minutes taken at all advisory and care planning meetings are emailed in advance of
scheduled meetings. Frequent communication occurs between meetings to monitor progress and work agreed upon. This was in the form of telephone calls, email, face to face meetings, and
distributing draft documents for consideration. Interviews highlighted that communication and progress updates from the Co-ordinator are frequent, clear, and have significantly helped the project
to progress. This was backed up by the most recent online survey with AG members on Mojo 3 where
100% of respondents rated communication as either very good or excellent.
5.6.2 External communication
A website has been developed (www.mojo-programme.org). While update maintenance of the website is required, it offers an opportunity for widening communication.
The National Office for Suicide Prevention, who fund Mojo, require regular updates on progress provided in the form of requested reports and verbal updates which are prepared by the Programme
Co-ordinator.
The Programme Co-ordinator, with the support of AG members has presented the Mojo Programme at a number of regional and national forums. In addition requests for information about the Mojo
Programme and its processes are increasingly requested. Among the forums at which Mojo was
presented and discussed:
The Psychiatrist from Tallaght Mental Health Unit and the Programme Co-ordinator made a
presentation at the Irish Medical Times conference in June 2012.
South Dublin County Council, through the Mayor, invited the Programme Co-ordinator to
speak at World Health Day on 10 October 2012. This event was highlighted in the local press.
The Project Co-ordinator made a presentation on the Mojo Programme as part of NOSP
conference in September 2012.
The Project Co-ordinator spoke at the launch of NOSP’s annual report 2012. This provided a
very high profile opportunity for the Mojo model and its outcomes to be presented to a

40
widespread national audience of key stakeholders. An interview with TV3 also took place after
the conference.
The HSE primary care Social Worker and Project Co-ordinator presented the Mojo Programme
at a cross border Social Work conference in October 2012.
The Programme Co-ordinator, following an invitation from Professor O’Dowd, participated in a
men’s health forum in October 2012.
Meetings were held with organisations such as the Traveller Health Programme, Eden, and
Jigsaw to explore how Mojo links and fits with these programmes.
Mojo entered the Aontas Star awards to highlight the work of the programme. However, the
application was not successful.
The Project Co-ordinator participated on NOSP prevention panel in 2013, which provided
Mojo with an opportunity not only to work with NOSP but also to disseminate key lessons
from Mojo. A new national suicide prevention strategy is being planned and may provide
opportunities for Mojo to communicate its model and outcomes.
The Project Co-ordinator was also selected to present Mojo at the Irish Public Health
Conference in October. This provided a very important platform for Mojo to present the Programme.
Requests for information came from a number of sources: Grow Suicide Prevention Community Project Offaly, Traveller Men’s Health Worker - Carlow, Rathmines Pembroke
Community Partnership, and Susan Beaton (specialist Australian consultant).
In addition, a range of articles on Mojo were issued in the local and regional press.
As outlined in Section 3 and in line with Mojo 1 and 2, the Programme Co-ordinator developed posters and flyers to promote Mojo for recruitment which were distributed to a wide range of
organisations both locally and nationally. As mentioned earlier, the name of the programme and
associated branding was carefully considered. The need to attract and not alienate the target group was a key consideration. Interviews with participants and stakeholders highlighted that the name has
proven to be very catchy, memorable and appropriate.
While there was no explicit objective set to promote Mojo externally, opportunities emerged
throughout the programme. This was beneficial in gaining support from senior stakeholders and in highlighting the work and progress with funders throughout the lifetime of the programme.
An objective was set at the Mojo Programme’s outset to communicate available services and
supports. While this does constitute part of the training element of Mojo and via AG meetings, a written leaflet or on-line resource is not available which would benefit the Programme.

41
6. Overview
6.1 Overall
Mojo has been an exceptionally successful prevention/early intervention Programme. In a two year period it has managed to implement an interagency collaborative programme that effectively
responded to the needs of one of the most vulnerable groups in Irish society – Men who are affected by the recession and are at risk of suicide.
Mojo has met all of the objectives that it initially set and gone on to expand elements of the
Programme to respond to participant needs and opportunities. The Programme has been run with three successive groups of men and has attained notable and consistent success with each group.
Interviews highlighted that while elements of the Mojo Programme exist in other programmes, as a whole, Mojo is both unique and well-balanced.
At the outset, while building on earlier work, Mojo took almost a year to plan the programme and to ensure that key elements were in place and functioning effectively. An agreement with the DSP that
participant’s welfare entitlements would not be affected by their participation on the programme was critical and helped to secure participation. This planning phase benefited the programme and was
essential to ensure that there was a clear and agreed vision for Mojo amongst stakeholders. This also
extended to incorporating key lessons from other programmes, agreeing roles, and a devising a master project plan. The reference manual which outlines the systems, agreements and structure to
implement the plan is a key resource which outlines the process and structure that underpins Mojo. These were all crucial in the success of the Programme.
The mix of group based training and one to one care planning combined available expertise and other
resources to provide a very effective balance to meet the men’s needs. The formative evaluation
process informed and honed the roll out of Mojo as training progressed. A number of tools such as evaluation sheets, focus group processes and online surveys are in place and can be adapted for use
in future programmes.
This interagency approach requires dedication, time, and commitment from agencies. This has been
achieved, however maintaining this intensive level of engagement will require a sustained stream of funding in the mid to long term.
6.2 Mojo Programme
The Mojo Programme comprises three distinct components. First group based training which is
underpinned by Wellness Recovery Action Planning (WRAP) and resilience building, the second information provision and physical exercise. The third concerns care planning and link working. This
section of the report also highlights the outcomes achieved by participants involved on the Mojo Programme including their post Mojo progress.
6.2.1 Group Based Training
The distinctive focus of WRAP and resilience building, specifically on mental health and wellbeing, and
the focus on information regarding services and supports were clear and maximised benefits for participants. As an exercise in group based training, WRAP provided a clear, evidence based
programme for the mental health and wellbeing component of Mojo to build on. It also provided opportunities for the agencies to train to deliver elements of WRAP.
It was exceptionally beneficial that Mojo could rely on an experienced WRAP facilitator from an associated agency to lead this throughout the pilot phase. The experienced course organisers devised
42
further appropriate modules when needed e.g. mindfulness, the participants’ family role. This
enhanced and developed this element of the group based training. Feedback from participants for this aspect of the programme was consistently very positive. This is significant given the lack of self
development experience of the men, and the resistance of men more generally to engage in self awareness programmes.
The information sessions proved to be successful. The agencies involved in Mojo were very involved in this aspect of the programme and provided staff to deliver on this element. This helped to promote
Mojo and increase awareness within organisations. Feedback from participants across all three projects was also very positive, with the enhancement of Mojo 3 to include more information on
available education/employment support being a very positive development. However, there remains substantial national challenges in supporting middle aged men who had been primarily employed in
unskilled/manual work or with skills that are difficult to transfer, who have low levels of education and
mental health issues, to actually return to the workplace. The participants raised these concerns along with the difficulties of finding meaningful, developmental opportunities.
The training element of the three Mojo projects, built lasting bonds between the men. This proved to
be very beneficial for participants who had had limited social opportunities outside of their home. This
group development helped individual men to positively engage and build trust. The initial research had identified the substantial social isolation that men experience when out of the workplace and
experiencing mental health issues.
The group based training, while designed by the Mojo supporting agencies involved, was based on an assessment of training available and the experience of those involved of working with vulnerable
target groups.
The evaluation concludes that Mojo 2, which ran for twelve weeks, six hours per week, is the optimal
model for the training element of the programme. In comparison to the ten week programme, the additional time gave participants an additional twelve hours of groupwork, more time to process the
information presented and more opportunities to engage with key working. In the context of the
profile of men targeted for participation, this additional face to face support time was beneficial.
6.2.2 Care Planning and Link Working
The care planning and link working provided an individual one to one element of the Programme. The
Recovery Star provided a comprehensive evidence based tool for link workers and participants to
inform and advise care plans. Overall, the care planning element was very successful in Mojo 1 and 2, with high levels of engagement and very positive participant/link worker feedback. However, it was
not as successful in Mojo 3. It is not possible to determine exactly why this was the case, but it is likely that a combination of the substantial workload of link workers, challenging and complex
participants, the summer season, fatigue, and Mojo’s own intensive demands were all factors.
The support structure of the Care Planning Group, helped provide link workers with feedback and
other support throughout the process. The protocols developed were applied and helped resolve issues as they emerged. However, it is important to ensure that responses to issues, particularly
those underpinned by legislative regulation, such as child protection, are clearly agreed and understood.
This element of the Programme would have been further enhanced by clearer and ongoing channel of communication with referral agencies e.g. GPs. to discuss care plans and monitor progress.

43
6.2.3 Outcomes for Participants
The outcomes for the men involved in Mojo have been consistent throughout all 3 Mojo projects. The
Recovery Star provides a quantifiable approach to measure change. Notable and significant changes are recorded particularly in the men’s ability to manage or improve each of the following:
Mental health
Physical Health and self-care
Identity and self-esteem Social Networks
Trust and hope
It must be noted that outcomes varied according to the individual. Interviews also highlighted the
positive influence that the Programme had on addictive behaviour and relationships with children and partners. The isolation levels of a number of men prior to their involvement on Mojo was highlighted
at interview stage, so the impact of men socialising, learning new skills and gathering information in an organised/controlled environment cannot be underestimated.
6.2.4 Outcomes for partners
Partners highlighted that Mojo had a very positive impact on the men involved in the programme. They identified that they were more open, less isolated, less angry, able to manage their mental
health issues more effectively and overall more positive. They also highlighted that the programme
had a broader impact on the family as a whole. The men became more interested and engaged in family life. In general relationships between the men and partners interviewed were stronger and
happier since their participation in Mojo.
6.2.5 Outcomes for key external stakeholders
The interviews with external stakeholders about the Mojo programme were very positive. They
identified that programmes of this type were not readily available and in their view unique in construct. The programme was seen to be exceptionally well planned and delivered. The involvement
of senior level experts in mental health at project design phase was of immense benefit to the programme as it ensured that best practice was incorporated and identified key champions for the
programme.
Stakeholders highlighted exceptionally positive impacts for men that they referred and that they
would continue to refer and promote Mojo. It is exceptionally notable that Mojo is the only community based service that Tallaght Mental Health Services refer into. Stakeholders outlined a
need for the programme to continue in Tallaght beyond its pilot phase, and to influence key national strategies that underpin responses to mental health and employment. All of the stakeholders
interviewed were highly complementary of the programme and its impact during this pilot phase.
6.2.6 Post Mojo
While the establishment of a Men’s Shed was not an original objective, this development has proved
to be a positive legacy aspect. Ten men are actively engaging in the Men’s Shed on a regular basis
and they appreciate that this forum provides a space to meet, learn new things, focus on their health and develop new friendships. These men are primarily from Mojo 1 and 2. It is important to note that
participants on Mojo 2 and 3 were younger and displayed greater desire to return to the workforce.

44
The development of a strong vibrant Men’s Shed requires substantial work to sustain and while a
great deal has been done to secure the longer term future of the Men’s Shed, how it is integrated with the Mojo programme requires clarification.
The progression of participants since engaging on Mojo is very impressive. 70% of the highly
vulnerable men, who participated in Mojo, have made significant progress in acquiring further
training, education and employment, following a 10 to 12 week programme. This is in excess of accepted progressions for programmes of this type. It is important to continue to monitor this.
6.3 Mojo Approach
6.3.1 Recruitment and Selection
The programme to date has engaged with 36 men which exceeded the original threshold of 30. The
high retention level (89%) was consistent across all three projects and is a very successful achievement. It is particularly notable given the voluntary nature of participation (no allowances were
paid to participants), the level of commitment that was required (two mornings per week), and the personal and health challenges experienced by participants. This rate exceeds accepted national
retention levels for a programme of this type.
The Mojo programme indicates that there are large numbers of men, who are affected by the
recession and/or otherwise unemployed in Tallaght who are interested in engaging in the Programme. All three projects run to date, have targeted middle aged men having a history of
employment prior to the recession and experiencing mental health issues. The majority of Mojo
participants were aged over 40 with almost a third previously employed in the construction sector. Education levels were generally low with 65% having completed their education at junior certificate
level or lower. A small number had been self-employed and had lost their business in the recession. These men were particularly vulnerable as they were not automatically entitled to social welfare
payments or a range of supports/services that are linked to these payments and thereby not then
technically registered as unemployed.
Despite targeting there were no participants from the Traveller community or from among current or former taxi drivers, both particular target cohorts at the beginning of the Programme. However,
following contact with Traveller organisations it was suggested that a male-specific Traveller Programme may be more successful in engaging with this group of men.
Referral levels progressively increased as each pilot project rolled out. In advance of Mojo 3 recruitment, large numbers of referrals were made. Referrals came from a range of sources and it is
notable that the majority came from health professionals via GPs and the HSE. The Advisory Group played a key role in supporting the referral process through respective agencies. GP promotion and
information was important in encouraging a number of men across all three Mojo projects to
participate in the Programme. In addition, family support in self-referral also played a key role in encouraging men to engage with the Programme.
6.3.2 Interagency Structure
The process to plan, design and implement Mojo, at all stages involved a range of stakeholders who had the collective expertise and commitment to working with vulnerable men. The role of the Co-
ordinator, with the recognised experience of SDCP in interagency working, was central to this
process. Thus a more integrated approach to responding to their mental health and employment support needs could be provided. At a time when resourcing has been substantially reduced across
the board, it can be increasingly challenging to engage agencies in interagency working. In addition challenges exist in engaging stakeholders across the state and voluntary sectors and those holding
different perspectives on complex issues such as mental health and employment. On average 10 to
13 representatives, many at senior level, participated at the AG every four to six weeks.

45
While collaborative working is well-established in Tallaght, the evaluation found that a number of
agencies and individual representatives did not have a history of working together in Tallaght prior to Mojo. The SDCP played a key role in supporting the collaborative process. They hosted and chaired
the AG meetings and their experience of developing collaborative processes helped to develop the interagency element of the programme. Mojo progressed. However, the engagement of health
related agencies was higher than those with an employment focus. Their ability to provide the
supports, skills and connectivity to enable these men to make progress to re-engage with the workplace and up-skill is of great importance.
Concerning the inter-agency structure, this evaluation concludes the following:
The commitment of recognised leaders in the area of mental health and collaborative
working, informed the programme design, helped agencies to buy into the programme, gave
it credibility and championed the programme as it rolled out.
The leadership of SDCP and its credibility and expertise in inter agency work was an
important contributory factor to establishing and sustaining the interagency element of the programme.
The commitment level of a substantial number of key agencies to Mojo is high. While all the
appropriate stakeholders are involved, employment support agencies could be more significantly engaged.
The structures are in place and support the interagency working.
Leadership for the development and implementation of Mojo is evident amongst the range of
agencies involved.
An open, honest, trusting way of working is in place.
The level of awareness amongst agencies of the services and supports available in Tallaght
has increased and there is a greater understanding of the respective role of agencies more generally. This has significantly improved links between frontline services.
Resourcing was committed to support this project to date which has contributed to the
success of the interagency dimension.
Communication internally and externally has been very consistent and effective.
Agencies engaged in training and were open to new methods of working, and were able to
adapt as Mojo rolled out.
The men, who engaged on Mojo, received direct engagement with services that was largely
positive and individually focused. This helped to maximise their progress.
6.3.3 Co-ordination and Management
Mojo is a project of SDCP. SDCP is skilled and experienced in managing and supporting staff as well
as managing interagency programmes and coordinating interagency strategies.
The role that the Programme Co-ordinator played in the initial design of the programme, developing
and leading the overall implementation of this programme was crucial. Interagency collaborative projects of this standard require high quality staffing. Mojo has benefited from a Co-ordinator who
has marshalled the development of the Programme. The achievements and standard of work are
46
particularly notable, particularly given that the post was part-time. His ability to work effectively with
agencies at senior level, design programmes, to plan and to communicate were all central to the programme. In addition his understanding of mental health and employment issues, ability to
implement collaboratively and to engage and empathise with the men involved was also of great value.
6.3.4 Communication
Internal and external communication provided a high level of awareness of Mojo. It was also instrumental to ensuring that key stakeholders were involved in Mojo. Communication was largely led
by the Project Co-ordinator. Further work to develop the website and to ensure that there is a clear strategy to publicise available supports and services would benefit Mojo into the future.

47
7. Final Recommendations
7.1 Mojo Programme Recommendations
Retain the current structure of the Mojo programme to include group based training (which
includes WRAP and resilience building and Information Provision) alongside care planning and link working.
Mojo should run over 12 weeks, with two three hour group training elements and with
physical exercise included in the Programme.
Consider specific programmes targeting taxi drivers and Travellers as these presented as
particularly vulnerable groups of men who informed the initial rationale for the programme. While strategies have been put in place to attract these groups, they have not engaged in the
programme to date. Therefore, their needs have not been met. Different strategies maybe required to attract these groups given cultural and work patterns (e.g. taxi drivers working at
night). Therefore, specific programmes maybe more effective in responding to the needs of
these men.
Consolidate progress to focus more on pathways to employment/education/training as part of
the information provision element of the project.
The Mental Health Recovery Star tool should continue to be used to underpin care planning.
Participants should continue to have one to one meetings at least twice during each project.
The way that link workers share progress, updates and concerns with GP and other referrers
should be considered further to ensure that referrers are aware of progress. This may not
always be appropriate but in some instances could help participant progress.
Continue to develop the tracking system for participants when they leave the Mojo
programme.
The position of the post Mojo Men’s Shed needs to be clarified and clearly agreed as it is
likely to require long-term resourcing if it is to develop further.
The Mojo Programme should be retained in Tallaght on account of the population it serves,
established demand, work already completed to establish the programme, and the level of
service/supports available in the area. This will require long term secured resourcing.
7.2 Mojo Approach Recommendations
A more effective plan to respond to the increasing demand for places on Mojo projects is
required, especially for those referred well in advance of the commencement of the programme.
Examine the mental health policy and practices of agencies particularly those with a remit for
employment supports and services (primarily the Department of Social Protection and the
Local Employment Service) to identify how these agencies can take on a more central,
leadership role within Mojo. This could help to support increased participation and buy in from these agencies in Mojo more locally.
Retain the Advisory group and Working Group structure in future Mojo programmes.
Give further consideration to how the learning and work within Mojo can contribute to the
work of the agencies involved. For example utilising the Recovery Star tool.

48
7.3 Expansion of Mojo
Prior to considering the expansion of Mojo the costs involved in the programme should be
established and evaluated.
Taking cost/benefit into account, plan to expand Mojo to other specific cohorts in Tallaght
such as taxi drivers, Traveller men, men with who were previously self-employed, younger
people (possibly in conjunction with Jigsaw), and women. The Programme will require
adjustments for same.
Taking cost/benefit into account, plan to run Mojo as a pilot in an area with a similar profile
and level of service to Tallaght. This would test the programme but only minimal structural changes would be required.
Consider the adjustments to the Programme to run in a rural area which would be less likely
to have the developed services and supports that exist in Tallaght.
Review the Mojo Reference Manual in the context of rolling out the programme outside of
Tallaght.
Any expansion of the Programme will require dedicated Co-ordination with wide ranging skills
levels and experience. In particular experience of achieving outcomes through interagency working at senior level, understanding and experience of working with disadvantaged target
groups, mental health and supporting progression to employment/training or further
education is important to implement the role (as outlined in section 5.2).
7.4 Policy considerations
Mojo has demonstrated that unemployed men who are experiencing a number of complex
health and social issues are willing to voluntarily engage in well run programmes that help
them plan their progress.
There are substantial gaps in supports and services available to those who were previously
self-employed. As they are not automatically entitled to social welfare support or services,
their status is often uncertain as they are not working but not officially classified as unemployed. Mojo provides an effective model for supporting this particularly isolated and
vulnerable cohort.
The employment support system faces national challenges in supporting men over 40 with
relatively low levels of education in their return to full time and sustained employment. This
cohort is large due to the decline in the construction sector. There are even greater challenges when this cohort experience mental health issues. Mojo serves as a particularly
appropriate strategy to meet the needs of this cohort.
The employment support system at present focuses on results and outputs. The experience
of Mojo demonstrates that the system needs to consider the impact of its processes on the
mental health of men who have been affected by the recession and unemployment. Mojo model should therefore be drawn upon to promote a greater understanding of mental health
across all relevant state agencies.
Research has identified the cohorts served by Mojo as being particularly vulnerable to suicide.
The learning from Mojo should be strongly integrated into the new National Suicide
Prevention Strategy being developed by NOSP. The feasibility of scaling up Mojo as part of suicide prevention more widely should be assessed.

49
8. Appendix One: Sample Training Schedule
Mojo 3 Wednesdays: Date Part 1
10 – 11.15
Break
11.15 -11.45
Part 2
11.45 –
13:00
Facilitator
July 10th
Introduction to WRAP Comfort agreements
specific to WRAP. Assigning Mojo Contact
Workers
Social space Team building Derek, Des , Patrice, Annmarie and Niamh
July 17th
Understanding Anxiety
Social space
Understanding Anxiety
Derek and Patrice
July 24th
Key concepts of WRAP
Social space
Understanding Mental Health
Angela, Derek and
Veronica
July 31st
Wellness recovery plan and tools
Social space
Our role in the family
Angela and Derek
Aug 7th
Daily maintenance
Social space Self-esteem
Angela and Patrice
Aug 14th
Understanding triggers
Social space Social
Supports
Angela and Niamh
Aug 21st
Early warning signs
Social space How the brain
works
Angela and Derek
Aug 28th
When things start breaking down
Social space
Mindfulness
Angela and Derek
Sep 4th
Crisis and post crisis
planning
Social space Goal planning
Angela and Niamh
Sep 11th
Review of WRAP
Social space Developing WRAP plan
Angela, Derek, Des, Patrice and Niamh
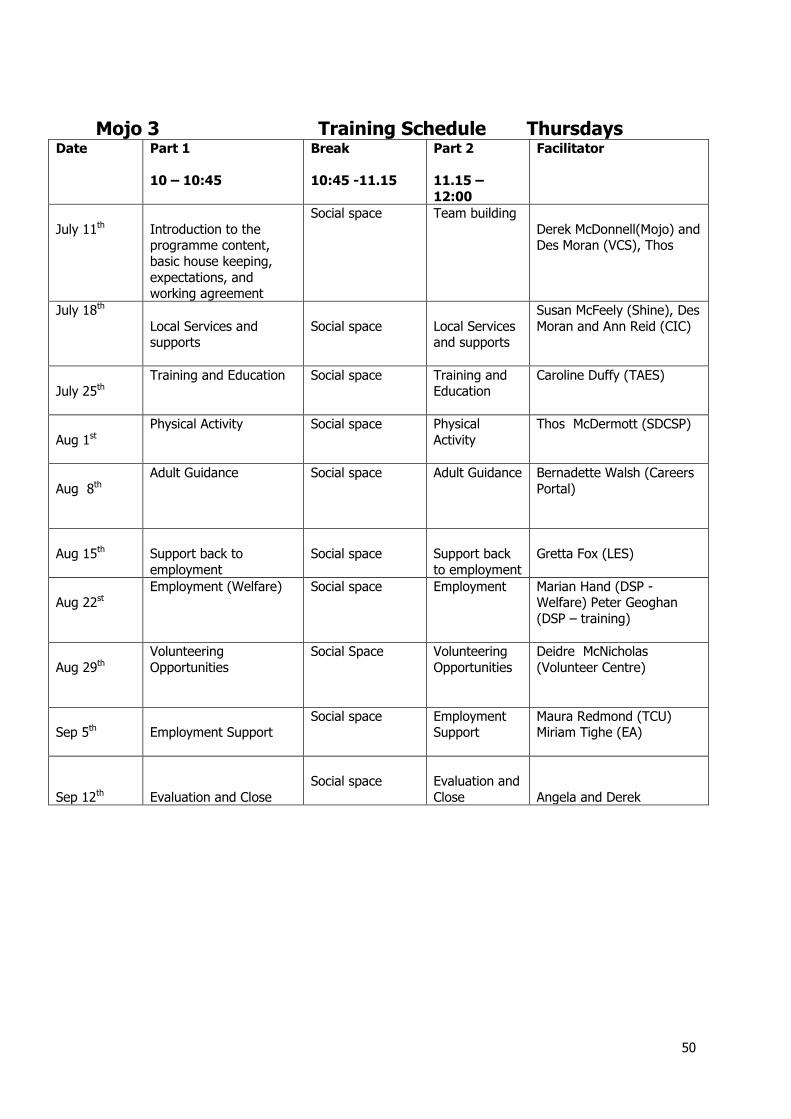
50
Mojo 3 Training Schedule Thursdays
Date Part 1
10 – 10:45
Break
10:45 -11.15
Part 2
11.15 –
12:00
Facilitator
July 11th
Introduction to the programme content,
basic house keeping,
expectations, and working agreement
Social space Team building
Derek McDonnell(Mojo) and Des Moran (VCS), Thos
July 18th
Local Services and supports
Social space
Local Services and supports
Susan McFeely (Shine), Des
Moran and Ann Reid (CIC)
July 25th
Training and Education Social space Training and Education
Caroline Duffy (TAES)
Aug 1st
Physical Activity Social space Physical
Activity
Thos McDermott (SDCSP)
Aug 8th
Adult Guidance Social space Adult Guidance Bernadette Walsh (Careers
Portal)
Aug 15th
Support back to
employment
Social space
Support back
to employment
Gretta Fox (LES)
Aug 22st
Employment (Welfare) Social space Employment Marian Hand (DSP - Welfare) Peter Geoghan
(DSP – training)
Aug 29th
Volunteering
Opportunities
Social Space Volunteering
Opportunities
Deidre McNicholas
(Volunteer Centre)
Sep 5th
Employment Support
Social space Employment Support
Maura Redmond (TCU) Miriam Tighe (EA)
Sep 12th
Evaluation and Close
Social space
Evaluation and
Close
Angela and Derek

51
9. Appendix 2: Advisory Group Members
Name Organisation Sector
Martin Berrige Tallaght Adult Education Service, Workplace Education Co-ordinator
Education
Tony Condron
JAAD, Counsellor Service Users
Julie Cruikshank HSE, Transformation Development Officer
Social Inclusion
Liz Dunne
CARP , Youth Worker Youth
Peter Geoghan
Department of Social Protection
Employment
Gretta Fox Local Employment Service
Employment
Angela Keegan Threshold Training Network , Manager
Direct service provider
Enda Dowling Pieta House, Counselling Psychologist
Mental Health
Anna Lee DVP Manager Integration and Communication
Thos McDermott South Dublin Sports Partnership, Coordinator
Sports/Activity (Link 2B Active)
Susan McFeely
Shine, Manager Mental Health
Niamh Millikan
SDCC, Social Worker Housing
Marjo Moonen DVP, Positive Action Manager
Integration and Communication
Des Moran Village Counselling Service, Manager
Mental Health
Hester O’Connor
HSE Clinical Psychologist Mental Health
Veronica O’Keane Tallaght Mental Health Service, Psychiatrist
Mental Health
Eileen O’Rourke Flexible Training Unit, DVP, Manager
Training/Employment
Patrice Reilly HSE , Primary Healthcare Social Worker
Public Health
Nuala Whelan Ballymun Job Centre, Manager
Interagency working

52
10. Appendix 3: Sample Poster

53


















