THE MANAGEMENT OF ACUTE POISONING · THE MANAGEMENT OF ACUTE POISONING G. G. COLLEE AND G. C....
12
British Journal of Anaesthesia 1993; 70: 562-573 REVIEW ARTICLE THE MANAGEMENT OF ACUTE POISONING G. G. COLLEE AND G. C. HANSON Self poisoning is among the most common causes of non-traumatic coma in patients younger than 35 yr, and accounts for approximately 10% of all acute medical admissions [8]. Anaesthetists may become involved in the care of these patients during emergency resuscitation or in the intensive care unit. In the U.S.A., acute self poisoning accounts for 5-30 % of admissions to medical intensive care units [21,23]. Classification Self-poisoning accounts for 95% of all poison- related admissions. It is slightly commoner in females (female to male ratio approximately = 1.3:1) with a peak incidence in females younger than 25 yr, and between 20 and 35 yr for males [8]. About 50 % of all overdoses involve a mixture of agents [8, 10, 21]. Self-poisoning is often an impulsive act with no clear intent to die and with a previous history of similar episodes [33]. Accidental poisoning occurs predominantly in chil- dren younger than 5 yr, and may be with medicines (usually those prescribed to a parent) or household products. Each year accidental poisoning in children accounts for about 24000 hospital admissions in England and Wales [5]. Only about 15% of the children presented to hospital with accidental poisoning develop symptoms from the agent ingested [23]. Fatal accidental poisoning is rare [35]. Non-accidental poisoning may occur as an extension of the syndrome of child abuse, usually in children younger than 30 months. This may be more common than is generally accepted [7], and has a fatal outcome more commonly than cases of accidental poisoning [23]. Homicidal poisoning is encountered rarely in clini- cal practice. Diagnosis Diagnosis is usually made from the history and circumstantial evidence. However, patients' state- ments about the nature and the quantity of the poison ingested are unreliable [39]. Witnesses, family, friends and ambulance personnel should be interviewed to establish details regarding the prob- (Br. J. Anaesth. 1993; 70: 562-573) KEY WORDS Tox/crty: drugs. able agents ingested and approximate time of ingestion. Alcohol is often taken in combination with one or more other agents. Isolated signs and symptoms are of little diagnostic value in any poisoning incident, but identification of the agent can often be surmised from the history and examination. Various combinations of signs may be suggestive of specific commonly ingested poisons [11]; however, there is a poor correlation between drugs suspected on admission and those actually detected in the blood [21]. The agents used in deliberate self-poisoning undergo changing patterns, with various agents going in and out of vogue. Currently in the U.K., the agents encountered most commonly in deliberate self-poisoning are the benzo- diazepines, paracetamol, aspirin and tricyclic anti- depressants [8]. Car exhaust poisoning is the method of suicide used most often by men aged 15—44 yr [29]. Toxicological screening should be considered in the urgent investigation of coma when the history, examination and biochemical analysis do not yield a diagnosis. About 50% of patients attending a casualty department with coma of unknown aetiology may be self-poisoning cases [10]. Appropriate samples should be collected early in the initial management of these patients so that they are available later if required for either diagnostic or medico-legal purposes. These samples should in- clude : Gastric contents: 50 ml of vomit, aspirate or the first portion of a gastric lavage. Urine: 50 ml of the first sample voided after admission. Blood: 10 ml of lithium-heparinized blood, 10 ml of blood without anticoagulant, and 2 ml of fluorided blood for ethanol assay. Care should be taken to avoid the use of swabs containing alcohol. Ideally, all of these samples should be collected before administration of any medications which may confuse toxicological analysis. Routine biochemical and haematological investi- gations may, rarely, suggest a diagnosis of acute poisoning. More often they provide a helpful baseline for later comparison. Many poisons cause fluid and electrolyte imbalance, renal or hepatic impairment, or acid—base imbalance. The majority of patients admitted after acute GEORGE G. COLLEE, M.B., CH.B., F.R.C.ANAES., Department of An- aesthesia, St Bartholomew's Hospital, London EC1A 7BE. GILLIAN C. HANSON, M.B., F.R.C.P., F.R.C.ANAES., Whipps Cross Hospital, Whipps Cross Road, Leytonstone, London Ell 1NR. Correspondence to G.C.H.
Transcript of THE MANAGEMENT OF ACUTE POISONING · THE MANAGEMENT OF ACUTE POISONING G. G. COLLEE AND G. C....
British Journal of Anaesthesia 1993; 70: 562-573
REVIEW ARTICLE
THE MANAGEMENT OF ACUTE POISONING
G. G. COLLEE AND G. C. HANSON
Self poisoning is among the most common causes ofnon-traumatic coma in patients younger than 35 yr,and accounts for approximately 10% of all acutemedical admissions [8]. Anaesthetists may becomeinvolved in the care of these patients duringemergency resuscitation or in the intensive care unit.In the U.S.A., acute self poisoning accounts for5-30 % of admissions to medical intensive care units[21,23].
ClassificationSelf-poisoning accounts for 95% of all poison-
related admissions. It is slightly commoner infemales (female to male ratio approximately = 1.3:1)with a peak incidence in females younger than 25 yr,and between 20 and 35 yr for males [8]. About 50 %of all overdoses involve a mixture of agents [8, 10,21]. Self-poisoning is often an impulsive act with noclear intent to die and with a previous history ofsimilar episodes [33].
Accidental poisoning occurs predominantly in chil-dren younger than 5 yr, and may be with medicines(usually those prescribed to a parent) or householdproducts. Each year accidental poisoning in childrenaccounts for about 24000 hospital admissions inEngland and Wales [5]. Only about 15% of thechildren presented to hospital with accidentalpoisoning develop symptoms from the agent ingested[23]. Fatal accidental poisoning is rare [35].
Non-accidental poisoning may occur as an extensionof the syndrome of child abuse, usually in childrenyounger than 30 months. This may be more commonthan is generally accepted [7], and has a fatal outcomemore commonly than cases of accidental poisoning[23].
Homicidal poisoning is encountered rarely in clini-cal practice.
DiagnosisDiagnosis is usually made from the history and
circumstantial evidence. However, patients' state-ments about the nature and the quantity of thepoison ingested are unreliable [39]. Witnesses,family, friends and ambulance personnel should beinterviewed to establish details regarding the prob-
(Br. J. Anaesth. 1993; 70: 562-573)
KEY WORDSTox/crty: drugs.
able agents ingested and approximate time ofingestion. Alcohol is often taken in combination withone or more other agents.
Isolated signs and symptoms are of little diagnosticvalue in any poisoning incident, but identification ofthe agent can often be surmised from the history andexamination. Various combinations of signs may besuggestive of specific commonly ingested poisons[11]; however, there is a poor correlation betweendrugs suspected on admission and those actuallydetected in the blood [21]. The agents used indeliberate self-poisoning undergo changing patterns,with various agents going in and out of vogue.Currently in the U.K., the agents encountered mostcommonly in deliberate self-poisoning are the benzo-diazepines, paracetamol, aspirin and tricyclic anti-depressants [8]. Car exhaust poisoning is the methodof suicide used most often by men aged 15—44 yr [29].
Toxicological screening should be considered inthe urgent investigation of coma when the history,examination and biochemical analysis do not yield adiagnosis. About 50% of patients attending acasualty department with coma of unknown aetiologymay be self-poisoning cases [10]. Appropriatesamples should be collected early in the initialmanagement of these patients so that they areavailable later if required for either diagnostic ormedico-legal purposes. These samples should in-clude :
Gastric contents: 50 ml of vomit, aspirate or thefirst portion of a gastric lavage.
Urine: 50 ml of the first sample voided afteradmission.
Blood: 10 ml of lithium-heparinized blood, 10 mlof blood without anticoagulant, and 2 ml of fluoridedblood for ethanol assay. Care should be taken toavoid the use of swabs containing alcohol.Ideally, all of these samples should be collectedbefore administration of any medications which mayconfuse toxicological analysis.
Routine biochemical and haematological investi-gations may, rarely, suggest a diagnosis of acutepoisoning. More often they provide a helpfulbaseline for later comparison. Many poisons causefluid and electrolyte imbalance, renal or hepaticimpairment, or acid—base imbalance.
The majority of patients admitted after acute
GEORGE G. COLLEE, M.B., CH.B., F.R.C.ANAES., Department of An-aesthesia, St Bartholomew's Hospital, London EC1A 7BE.GILLIAN C. HANSON, M.B., F.R.C.P., F.R.C.ANAES., Whipps CrossHospital, Whipps Cross Road, Leytonstone, London Ell 1NR.
Correspondence to G.C.H.
THE MANAGEMENT OF ACUTE POISONING 563
poisoning are conscious on arrival at the hospital;however, in unconscious patients organic braindamage should always be suspected if the history ofpoisoning is unsatisfactory and the depth of comadoes not improve within 12 h.
MANAGEMENT
Before consideration of the active management of thepoisoned patient, it should be emphasized that, forthe majority of poisoned patients, only supportivecare is needed. This led one reviewer to comment"It cannot be repeated too often that the primaryobject of the treatment of acute poisoning is not tocollect as much ' poison' from the patient as possible,but to save life when this is threatened and to relievepain and suffering... i.e to save the patient, not toregain the poison" [22].
Immediate measuresInitial resuscitation in comatose patients should be
conducted with the usual priorities: A-B—C-D—E:Airway. Provide one if the patient's upper airway
is obstructed. Protect the airway if the cough and gagreflexes are obtunded and secure the airway, whennecessary, with tracheal intubation (this may includepatients with marginally adequate protective reflexeswho require gastric lavage).
Breathing. Assess the ventilatory efforts and assistwhere necessary. Assess gas exchange. Look forevidence of aspiration of gastric contents, toxic gasesor foreign substances.
Circulation. Establish i.v. access early. Assessperipheral perfusion and begin resuscitation asrequired. Connect electrocardiographic monitoringand examine a rhythm strip.
Collect samples for future toxicological analysis ifrequired.
Document the available history before ambulancepersonnel, relatives, etc. leave the hospital, and thelevel of coma.
Examine the patient thoroughly for associatedinjuries (e.g. pressure area necrosis), medical con-ditions which may have precipitated the overdose(e.g. toxic psychosis) or which may produce coma(e.g. hypoglycaemia).
Measures to limit absorption
The conventional belief that, after ingestion ofpoisons other than corrosives or petroleum distil-lates, the stomach should be routinely emptied byemesis or gastric lavage has been questioned byseveral authors [25, 27, 37].
Emesis should be induced only in fully consciouspatients. It is less traumatic for the conscious patientthan gastric lavage and is therefore the preferredtechnique of gastric emptying for children. However,the recovery of gastric contents by ipecacuanha-induced emesis is generally less than 50% [28, 37].Syrup of ipecacuanha followed by an adequatevolume of water induces vomiting in 90-95% ofpatients within 20-30 min, in both adults and
children [13,32]. Evidence that this emesis sig-nificantly reduces the absorption of commonlyingested poisons is less convincing. Therefore,although it only rarely causes serious sequelae, it isprobably of little or no benefit to the majority ofpoisoned patients. The decision to empty theconscious patient's stomach by inducing emesisshould be dependent upon the specific history ofprobable toxins, the estimated dose and the timesince ingestion, rather than an automatic response toa history of acute poisoning.
Gastric aspiration and lavage is the only suitableway of emptying the stomach in the presence ofobtunded laryngeal and pharyngeal reflexes. Airwayprotection is an essential part of the procedure. Inthe semi-conscious patient, airway protection maybe achieved by placing the patient in the left-lateral,head-down position in the presence of an experi-enced anaesthetist with suction apparatus immedi-ately to hand. In patients with more severelyobtunded reflexes, it is safer to opt for electivetracheal intubation before gastric lavage.
Gastric aspiration and lavage via a wide-boreorogastric tube is indicated within 4 h of seriouspoisoning (i.e. the patient is comatose) with any ofthe commonly ingested poisons. The technique hasbeen well described elsewhere [26]. Because thehistory is usually unreliable and gastric emptying isdelayed by many poisons (notably aspirin and thetricyclic antidepressants), gastric lavage should beconsidered in any seriously poisoned patient up to12 h after ingestion [12]. Conversely, with drugswhich do not delay gastric emptying and which areabsorbed rapidly from the gastrointestinal tract (e.g.paracetamol), gastric lavage may be ineffective aslittle as 2-4 h after ingestion.
Activated charcoal is a powerful, non-specificadsorbent which may be administered orally or via agastric tube. Irreversibly binding the drugs withinthe bowel reduces blood concentration both byreducing drug absorption and by creating a negativediffusion gradient between the gut lumen and theblood, whereby drug diffuses from the circulationinto the gut lumen—so called "gastrointestinaldialysis" [18]. It may be appropriate, therefore, toadminister activated charcoal long after the originalpoisoning, and repeated administration is advocatedas a safe, cheap and effective method of reducingdrug concentrations in the blood. It is of demon-strable benefit after poisoning with several com-monly ingested drugs, including aspirin [20] andparacetamol [19]. Anecdotal reports support the useof repeated administration of activated charcoal aftera variety of other poisons. Enthusiasm for theserelatively unproven uses, however, must be temperedby reports of serious consequences of pulmonaryaspiration of activated charcoal [9, 24] and the minorrisk of gastrointestinal obstruction after its use [36].Furthermore, there are theoretical limitations. Drugelimination with activated charcoal is less effective inpatients with severely impaired gastrointestinalmotility—particularly relevant after poisoning withsalicylates or with agents which have a significantanticholinergic action. Kirshenbaum and colleagueshave questioned the clinical efficacy of multiple-dose
564 BRITISH JOURNAL OF ANAESTHESIA
charcoal therapy after salicylate poisoning [16]. It issuggested also that clearance of parenterally admin-istered medications used to treat intoxicated patientsis increased by the charcoal, perhaps making treat-ment less effective.
Further pharmacokinetdc data on the clearance ofspecific poisons are needed to determine the rationaluse of repeated charcoal regimens in a variety ofclinical settings. Meanwhile, it provides a relativelysafe technique of proven benefit in limiting drugabsorption when given soon after ingestion of specificpoisons. It is also probably of benefit in repeateddoses in carefully selected clinical circumstances.Drugs which are well adsorbed to activated charcoalinclude benzodiazepines, antidepressants, anti-convulsants, barbiturates and theophylline. Sali-cylates and paracetamol are moderately welladsorbed.
Supportive careAll but a small minority of unconscious poisoned
patients recover with supportive care alone. Con-servative therapy is aimed at preventing complica-tions such as hypoxaemia, aspiration, hypotension,acid—base and electrolyte imbalance, hypothermia,convulsions and the consequences of unconscious-ness, whilst awaiting spontaneous elimination of thepoison via the liver, kidneys, lungs and gut.
Respiratory complications are the commonestcauses of death after acute poisoning, and immediatemanagement must give priority to the airway,ventilation and prevention of aspiration. Havingestablished an airway, it is important to assess theprotective reflexes and consider the need for trachealintubation. Whether or not gastric lavage is con-sidered appropriate, a nasogastric tube should beinserted to prevent gastric dilatation. Hypo-ventilation is common after poisoning with sedatives,hypnotics, analgesics and many other drugs andchemicals. Hypoxia and hypercapnia may cause orpotentiate cardiac arrhythmias or may exacerbateincreased intracranial pressure, and should thereforebe treated promptly. Specific antidotes may play arole in reducing the need for mechanical ventilationafter poisoning with opioids or benzodiazepines (seeNeurological complications).
Continued observation is essential in order todetect deterioration in the conscious level requiringa reappraisal of the need for airway protection ormechanical ventilation. Nurses should be givenspecific criteria by which to assess the need for re-referral to an anaesthetist. All patients requiringmechanical ventilation or tracheal intubation shouldbe transferred to an intensive care unit for furthermonitoring.
Patients may present after long periods of res-piratory depression, having already developed as-piration pneumonia or hypostatic pneumonia. Themainstay of treatment comprises endobronchialaspiration, physiotherapy and antibiotics.
Cardiovascular complications include hypotension,cardiac arrhythmias and cardiac arrest. A carefulassessment of the patient's cardiovascular statusshould be made soon after presentation. The major
factors contributing to hypotension in the presenceof normal sinus rhythm are peripheral vasodilatationand myocardial depression, and the majority ofpatients respond to adequate intravascular volumerepletion. In young, previously healthy patients,invasive monitoring is rarely required.
Arrhythmias may be caused by the toxin (e.g.poisoning with tricyclic antidepressants), hypoxia orhypercapnia, or may be secondary to the effects ofthe toxin on acid—base or electrolyte balance. A 12-lead ECG should be performed to provide a baselineand, in selected patients, continuous ECG moni-toring is required. Patients suffering cardiac arrest asa direct result of a circulating toxin may be resistantto attempts to re-establish sinus rhythm. It istherefore worth persisting with external cardiacmassage for longer than may otherwise be consideredappropriate. Particular caution should be exercisedin attributing any significance to the presence offixed dilated pupils, which may reflect merely theactions of the toxin rather than any cerebraldysfunction.
Renal complications may result from the directeffects of the toxin (e.g. in aspirin, paracetamol orheavy metal poisoning), from a period of hypo-tension, from rhabdomyolysis with myoglobinuria,or from sepsis related to aspiration pneumonia. Forfurther information beyond the scope of this article,the reader is referred to an extensive review ofnephrotoxins by Abuelo [1].
Myoglobinuria should be suspected in any patientwith evidence of a prolonged period of coma beforeadmission (i.e. pressure area discolouration withpoor capillary refill), with a history of prolongedseizures or with tissue hypoxia (e.g. from carbonmonoxide poisoning).
Any comatose or hypotensive patient, or anypatient with a history of poisoning with a knownnephrotoxin, should be catheterized, and the urineoutput maintained at least at 0.5 ml kg"1 h"1. This isachieved with volume resuscitation in the firstinstance followed, if necessary, by an infusion ofdopamine in a small dose (2-4 ug kg"1 min"1) and thejudicious use of diuretics. Urinalysis before in-tervention may aid diagnosis by pointing to a renal orpre-renal cause, and occasionally by displaying thegranular casts of acute tubular necrosis or theeosinophils of an acute interstitial nephritis.
When rhabdomyolysis is suspected, urinalysis ofmyoglobin should be performed, but treatmentshould be started promptly without awaiting theresults of urinalysis. Urine output should be main-tained at least at 1.5-2 ml kg"1 h"1 with aggressivevolume loading and mannitol, and the urinary pHshould be kept greater than 6.5 in order to preventmyoglobin from precipitating in the renal tubules.Loop diuretics have the theoretical disadvantage ofacidifying the urine, therefore mannitol is preferredfor maintaining the diuresis. Blood samples shouldbe taken for measurement of the urea, creatinine,potassium, calcium and creatine phosphokinaseconcentrations. In severe cases, hypocalcaemia mayresult from a shift of extracellular calcium intoinjured muscle. Serum potassium concentrationsmay increase rapidly because of muscle breakdown,
THE MANAGEMENT OF ACUTE POISONING 565
necessitating early intervention with calcium, glu-cose and insulin infusion, or dialysis.
Hepatic and gastrointestinal complications. Gastricstasis may occur in any comatose patient, or inresponse to anticholinergic or opioid effects. Earlydecompression with a nasogastric tube should beperformed to reduce the risk of regurgitation andaspiration. Stress ulcer prophylaxis may also beappropriate in selected patients.
Fulminant hepatic failure is a well recognizedcomplication of serious poisoning with paracetamol,carbon tetrachloride or Amanita phalloides. Thesepatients require early referral to a specialist liverunit.
Neurological complications include depression ofconscious level, seizures, cerebral oedema and per-ipheral nerve injuries as a result of prolongedpressure. It is important to exclude metabolic ortraumatic causes, and any patient whose level ofconsciousness appears inappropriately depressed forthe history of poisoning should be suspected ofhaving an intracranial haemorrhage. Lateralizingsigns are rarely attributable directly to the toxin.
Correct nursing care is essential to protect thepatient from the complications of prolonged coma.The presence of pressure area necrosis, neuro-praxias, comeal abrasions and other sequelae ofcoma must be documented on admission to the unit,both to alert the nurses to areas requiring specialattention, and to provide medico-legal protection.The role of specific antagonists such as naloxone andflumazenil to antagonize central nervous systemdepression is controversial [2]. Reversal of coma canundoubtedly make management of the patient easier;however, acute antagonism of opioids with naloxone,or of benzodiazepines with flumazenil, may provokesevere withdrawal reactions. Antagonism of benzo-diazepines with the specific antagonist, flumazenil,may be counterproductive in patients who havetaken a mixture of drugs. For example, in thecommonly encountered poisoning with both tricyclicantidepressants and benzodiazepines, acute antag-onism of the benzodiazepines may induce seizureswhich had previously been suppressed. Moreover,for both antagonists the action of the antagonism isshort-lived, therefore the patient may become coma-tose unexpectedly as the antagonist wears off.
Seizures may result from metabolic disturbance,cerebral hypoxia, or as a direct toxic effect (e.g. afterpoisoning with tricyclic antidepressants or theo-phylline). Urgent control is essential and is usuallyachieved initially with i.v. diazepam. Thereafter,consideration must be given to further anti-convulsant therapy (e.g. with phenytoin, pheno-barbitone or clonazepam). Resistant subjects mayrequire an infusion of thiopentone. Some of theseagents cause further respiratory depression andelective tracheal intubation and artificial ventilationmay be necessary. Detection of further seizures maybe difficult in the patient undergoing ventilation, andmonitoring should include continuous recordingwith a cerebral function monitor if neuromuscularblockers are used.
Cerebral oedema should be anticipated in anypatient who has suffered a hypoxic cardiac arrest, a
period of profound hypotension or severe carbonmonoxide poisoning. Treatment to prevent sec-ondary brain injury should include elective intu-bation and mechanical ventilation to moderatehypocapnia, with careful control of cerebral per-fusion pressure by maintaining the mean arterialpressure within the normal range for that patient,and by avoiding fluid overload. Mannitol and loopdiuretics may have a role after specialist consultation,and in severe cases intracranial pressure monitoringmay be appropriate to direct therapy.
Metabolic complications may take almost any formin acute poisoning. The concentrations of urea,electrolytes and blood glucose should be checkedroutinely. In some patients, blood-gas analysis isalso required.
Hypothermia is a common complication of pro-longed coma outside hospital, and may be exacer-bated by drugs which prevent the usual responses ofvasoconstriction and shivering. Passive rewarmingshould be achieved with warm blankets. Activeexternal rewarming is discouraged, as it may produceperipheral vasodilatation when cardiac function isstill depressed by a reduced core temperature. I.v.fluids should be warmed and, during artificialventilation, warm water bath humidifiers should beadded to the breathing system. In extreme cases(< 32 °C) resistant to these techniques, it may benecessary to rewarm actively with warm water gastricor bladder instillation or by peritoneal lavage.Temperature should be monitored centrally (oeso-phageal or nasopharyngeal) and the ECG should bemonitored for arrhythmias.
Hyperthermia may occur in acute intoxicationwith, for example, tricyclic antidepressants, cocaineor amphetamines, or as part of the syndrome ofneuroleptic malignant syndrome after phenothiazineoverdosage. In severe cases, active cooling withsedation, paralysis and ventilation with unheatedgases may be required to control core temperature.
Measures to enhance elimination of the poison
Fewer than 5 % of cases of acute poisoning merittreatment with specific techniques to increase drugelimination [34]. "Gastrointestinal dialysis" withactivated charcoal has already been discussed, andfor those drugs which are readily adsorbed toactivated charcoal it provides the safest mechanismof enhancing drug clearance. More invasive tech-niques are rarely justified. In cases of seriouspoisoning, specialist advice should be sought fromthe regional poisons centre.
Forced diuresis should be considered only for thosepatients in whom toxicological analysis has demon-strated the presence in the blood of a toxic agent insufficient amount to cause severe poisoning. Briskdiuresis maintains a small concentration gradientbetween the renal tubular fluid and the renalcapillary bed, thereby minimizing tubular re-absorption of toxins. Manipulation of the urinarypH may further decrease tubular reabsorption of thetargeted drug by ensuring that it remains mostly inthe ionized form. Therefore, for weak acids (such assalicylates or barbiturates), forced alkaline diuresis ismost effective, whilst for weak bases (such as
566 BRITISH JOURNAL OF ANAESTHESIA
phencyclidine) forced acid diuresis is more ap-propriate. The technique is ineffective for drugswhich are strongly protein-bound (e.g. tricyclicantidepressants, carbamazepine, phenytoin) orwhich have a large apparent volume of distribution(e.g. paracetamol, lithium, tricylic antidepressants).Regimens to establish a forced alkaline or forced aciddiuresis have been described well elsewhere [34].The technique, however, carries significant risk ofcausing fluid overload with pulmonary oedema orcerebral oedema, or of causing severe disturbance ofelectrolyte and acid-base balance. This risk isaccentuated in the elderly, or those with cardiac orrenal impairment, and should be balanced againstthe likelihood of significantly altering the patient'sclinical outcome.
Extracorporeal elimination techniques—haemo-dialysis and haemoperfusion—have not yet beenassessed adequately clinically in acute poisoning, andthere remain many difficulties in assessing theefficacy of these invasive techniques [4, 38]. Theiruse should currently be limited to a carefully selectedgroup of patients, and specialist help should alwaysbe sought. For extracorporeal elimination techniquesto be helpful the following criteria are suggested [4]:(1) The drug or toxin should either diffuse readilythrough the dialysis membrane or be readily takenup by an absorbant. Protein-bound drugs and largemolecules are removed inefficiently by dialysis, andcan be removed more effectively by haemoperfusion(in which the blood is passed directly over sorbentparticles to which toxins or drugs are adsorbed bysurface forces). However, although salicylates areprotein-bound, the plasma binding sites are satu-rated quickly even at normal therapeutic plasmaconcentrations, therefore a large proportion of thedrug exists in the unbound form.(2) A significant proportion of the poison should bepresent in the plasma water, or be capable of rapidequilibration with it. Drugs with a large volume ofdistribution and high lipid solubility are thereforedifficult to eliminate. If movement of the drug fromthe extravascular compartment back into the intra-vascular compartment is slower than the plasmaclearance achieved, a rebound of the plasma concen-tration occurs on stopping dialysis/haemoperfusion.(3) The pharmacological effect of the toxin shouldbe directly related to its concentration in the blood.(4) Dialysis or haemoperfusion should add sig-nificantly to other body mechanisms of elimination.
Peritoneal dialysis achieves considerably less clear-ance of plasma than can be achieved with haemo-dialysis, and has no established role in the man-agement of acute poisoning.
Haemodialysis or haemoperfusion has a clearlyestablished role in the treatment of severe salicylateoverdosage or poisoning with death cap mushrooms(Amanita phalloides) [4]. Clearance of alcohol, ethan-olj barbiturates, anticonvulsants, benzodiazepines,lithium, cardiac glycosides and many other lesscommonly encountered poisons can certainly beenhanced with extracorporeal techniques; however,it remains unclear if this influences clinical outcomefavourably. Clearance of paracetamol and the tri-cyclic antidepressants is not enhanced by haemo-
dialysis or haemoperfusion, and extracorporeal elim-ination techniques have no role in the managementof patients after poisoning with these agents.
Use of specific antidotes
The toxic effects after poisoning with specificagents may be decreased or prevented by admin-istration of their specific antidotes. Such antidotesmay directly influence the metabolism of the poison,preventing or reducing the formation of harmfulmetabolites (e.g. acetylcysteine in paracetamolpoisoning), may compete for drug receptor sites (e.g.flumazenil in benzodiazepine overdose; naloxone inopioid overdose) or may bind with the poison toform less toxic chelates which are more easilyexcreted (e.g. Fab fragments in severe cardiacglycoside overdosage). A broader definition of anantidote includes any substance which can favour-ably influence the onset, severity or duration of thetoxic effects of a poison. The currently availableantidote therapies and their clinical use has recentlybeen reviewed comprehensively by Lheureux, Even-Adin and Askenasi [17] and emergency departmentsshould keep a reference list of antidotes and theirmode of administration for quick reference.
FEATURES AND TREATMENT OF SPECIFIC POISONS
It is proposed not to give here detailed aspects ofmanagement, but to provide a ready, practicalreferral list, and to point out aspects of care peculiarto specific intoxicants.
Analgesics
Salicylate intoxicationA large number of salicylate preparations are
available to the community, many of which do notmention the name "aspirin". Oil of wintergreen ismethyl salicylate and is highly toxic.
Pharmacology. In normal therapeutic doses, acetylsalicylic acid is de-acetylated by plasma esterases andeliminated by conjugation. The volume of distri-bution is normally low but, when metabolic acidosisdevelops, tissue penetration increases.
In salicylate intoxication, prolongation of elim-ination occurs, the conjugation padiway rapidlybecomes saturated and elimination is by the clearanceof free salicylate via the kidneys. Salicylate clearanceis pH-dependent, increasing 10-fold from a serumpH of 6 to that of 7.5.
Salicylates have a contradictory effect on acid-basebalance. CNS stimulation of the respiratory centremay lead to respiratory alkalosis, whereas salicylateitself results in the accumulation of organic acidmetabolites. The interaction between these twoelements is variable and can be assessed only byfrequent measurement of blood-gas tensions andacid-base state. Other important metabolic effectsare hypo- or hyperglycaemia, and hypokalaemia fromcompensatory renal excretion.
There is increased risk of permeability-relatedoedema, although left ventricular failure may alsooccur secondary to cardiac arrhythmias, hypo-kalaemia or fluid overload. Clotting defects may
THE MANAGEMENT OF ACUTE POISONING 567
TABLE I. Summary of management of salicylate poisoning
Mild intoxicationObserve fluid balance.Forced diuresis with large fluid turnover (4 litre/24 h).Repeat salicylate concentration measurement 2 h later to check that concentration is decreasing.
Moderate-severe intoxicationAdmit to ITU regardless of the level of consciousness.Administer activated charcoal orally or via a nasogastric tube: 5 g 4-hourly for six doses.Observe airway, venrilatory frequency, mental state and core temperature.Insert central venous pressure mnmilaMeasure acid-base balance 2-hourly.Forced alkaline diuresis.Maintain careful fluid balance charts and observe for fluid overload, pulmonary oedema and pulmonary aspiration.Haemodialyse if:1. "Severe" concentration does not decrease after 2 h of therapy.2. "Moderate" concentration increases to the "severe" range after 2 h of therapy.3. Onset of acute renal failure or pulmonary oedema secondary to fluid overload, unresponsive to diuretic therapy.
200
140
1024 36 48
Time after ingestion (h)60
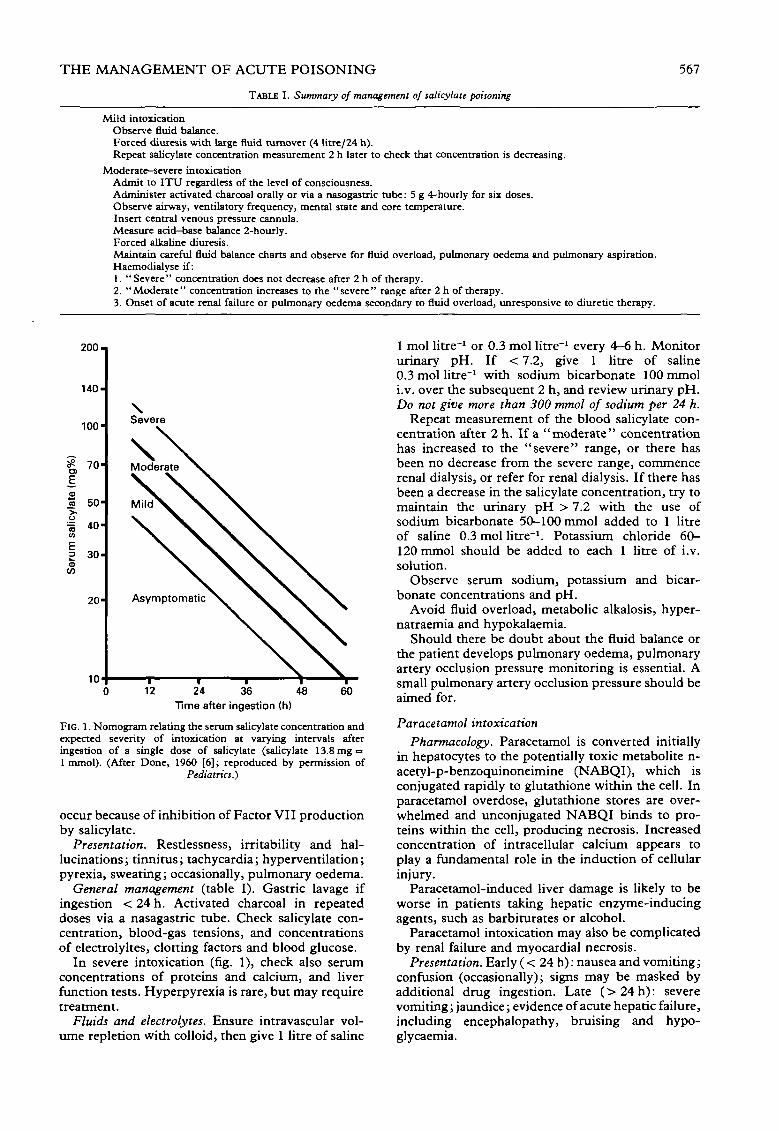
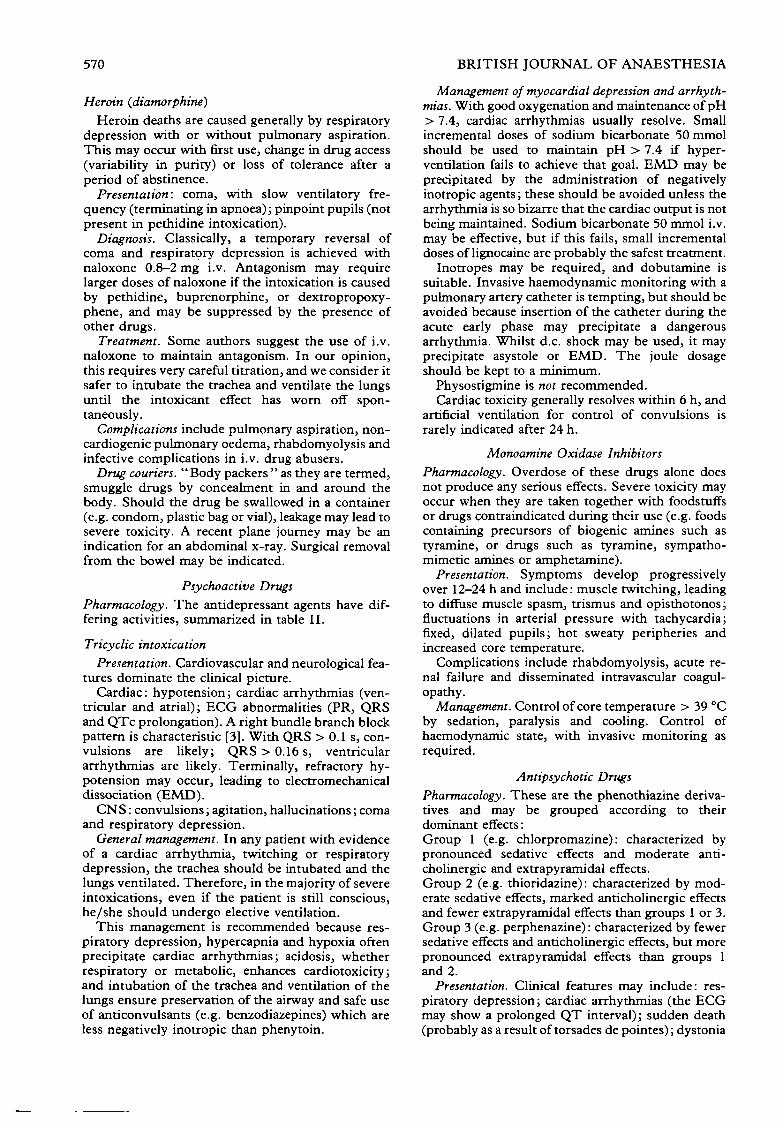
FIG. 1. Nomogram relating the serum salicylate concentration andexpected severity of intoxication at varying intervals afteringestion of a single dose of salicylate (salicylate 13.8 mg =1 mmol). (After Done, 1960 [6]; reproduced by permission of
Pediatrics.)
occur because of inhibition of Factor VII productionby salicylate.
Presentation. Restlessness, irritability and hal-lucinations; tinnitus; tachycardia; hyperventilation;pyrexia, sweating; occasionally, pulmonary oedema.
General management (table I). Gastric lavage ifingestion < 24 h. Activated charcoal in repeateddoses via a nasagastric tube. Check salicylate con-centration, blood-gas tensions, and concentrationsof electrolyltes, clotting factors and blood glucose.
In severe intoxication (fig. 1), check also serumconcentrations of proteins and calcium, and liverfunction tests. Hyperpyrexia is rare, but may requiretreatment.
Fluids and electrolytes. Ensure intravascular vol-ume repletion with colloid, then give 1 litre of saline
1 mol litre"1 or 0.3 mol litre"1 every 4-6 h. Monitorurinary pH. If < 7.2, give 1 litre of saline0.3 mol litre"1 with sodium bicarbonate 100 mmoli.v. over the subsequent 2 h, and review urinary pH.Do not give more than 300 mmol of sodium per 24 h.
Repeat measurement of the blood salicylate con-centration after 2 h. If a "moderate" concentrationhas increased to the "severe" range, or there hasbeen no decrease from the severe range, commencerenal dialysis, or refer for renal dialysis. If there hasbeen a decrease in the salicylate concentration, try tomaintain the urinary pH > 7.2 with the use ofsodium bicarbonate 50-100 mmol added to 1 litreof saline 0.3 mol litre"1. Potassium chloride 60-120 mmol should be added to each 1 litre of i.v.solution.
Observe serum sodium, potassium and bicar-bonate concentrations and pH.
Avoid fluid overload, metabolic alkalosis, hyper-natraemia and hypokalaemia.
Should there be doubt about the fluid balance orthe patient develops pulmonary oedema, pulmonaryartery occlusion pressure monitoring is essential. Asmall pulmonary artery occlusion pressure should beaimed for.
Paracetamol intoxicationPharmacology. Paracetamol is converted initially
in hepatocytes to the potentially toxic metabolite n-acetyl-p-benzoquinoneimine (NABQI), which isconjugated rapidly to glutathione within the cell. Inparacetamol overdose, glutathione stores are over-whelmed and unconjugated NABQI binds to pro-teins within the cell, producing necrosis. Increasedconcentration of intracellular calcium appears toplay a fundamental role in the induction of cellularinjury.
Paracetamol-induced liver damage is likely to beworse in patients taking hepatic enzyme-inducingagents, such as barbiturates or alcohol.
Paracetamol intoxication may also be complicatedby renal failure and myocardial necrosis.
Presentation. Early (< 24 h): nausea and vomiting;confusion (occasionally); signs may be masked byadditional drug ingestion. Late (>24h) : severevomiting; jaundice; evidence of acute hepatic failure,including encephalopathy, bruising and hypo-glycaemia.
568 BRITISH JOURNAL OF ANAESTHESIA
450
- 400
Brf)
co
rat
CCDUcou"5
tarn
oCOCOaCO
ECOCOa_
350
300
250
200
150
100
50
6 7 8 9 10Time after ingestion (h)
11 12
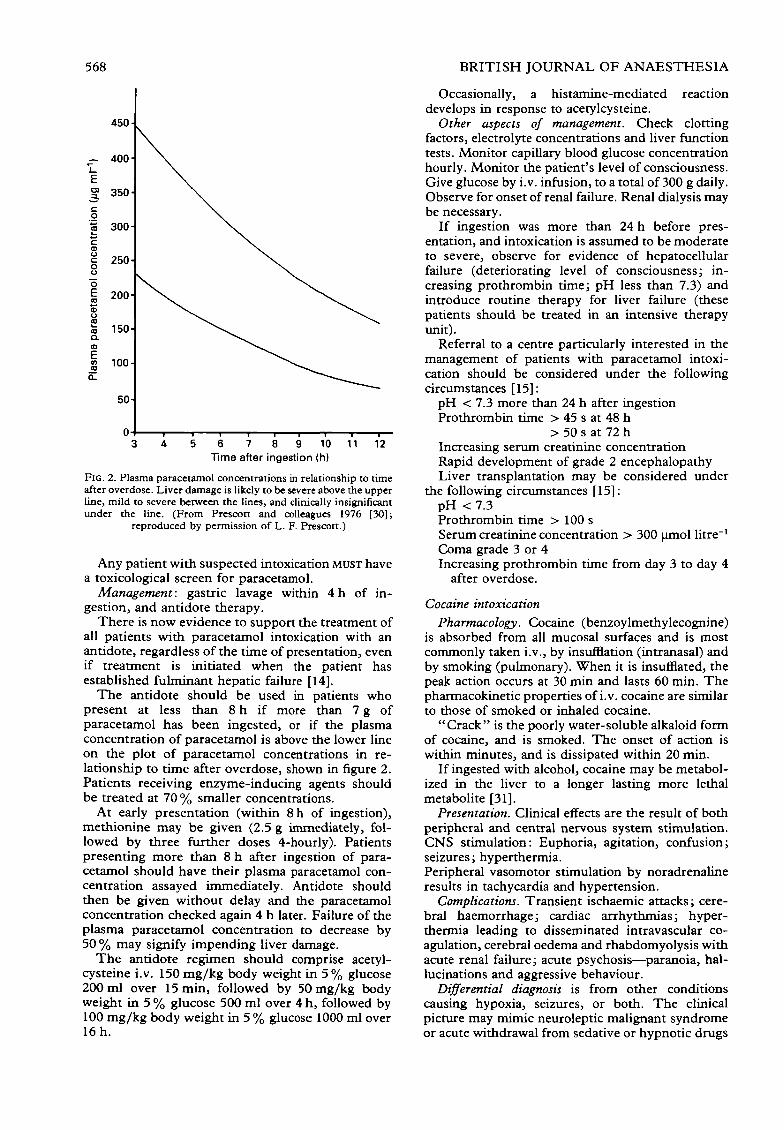
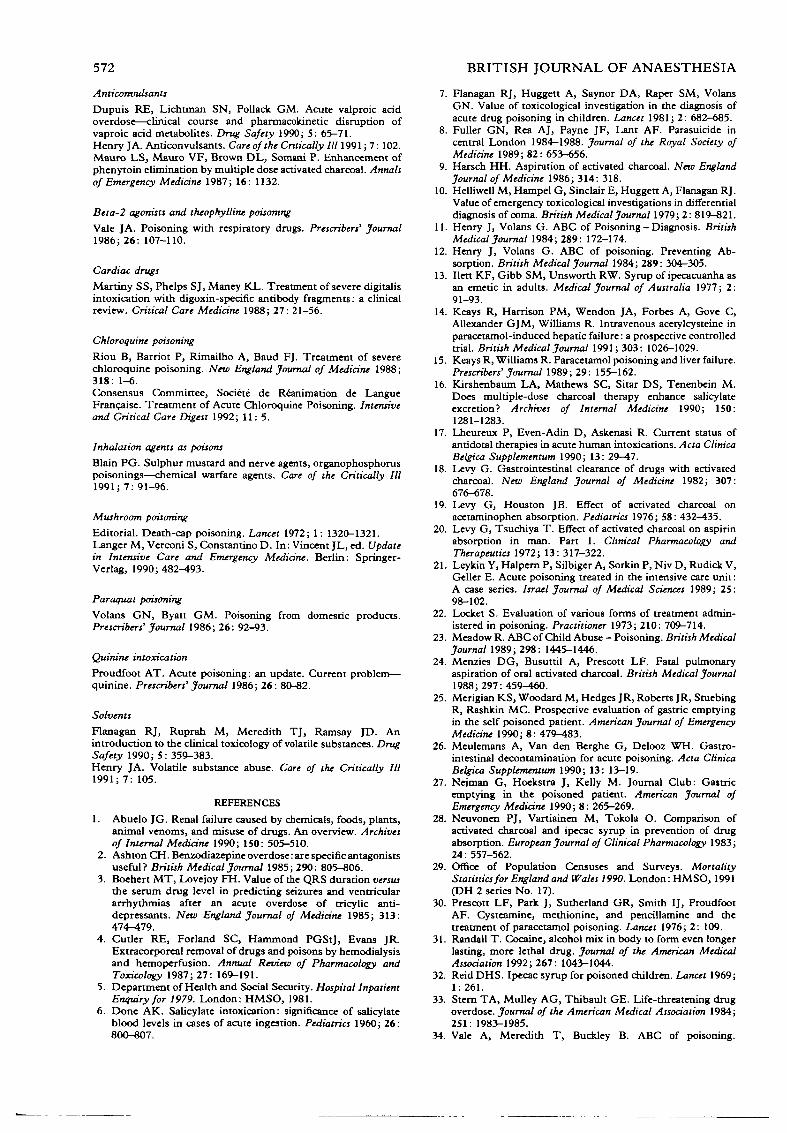
FIG. 2. Plasma paracetamol concentrations in relationship to timeafter overdose. Liver damage is likely to be severe above the upperline, mild to severe between the lines, and clinically insignificantunder the line. (From Prescott and colleagues 1976 [30];
reproduced by permission of L. F. Prescott.)
Any patient with suspected intoxication MUST havea toxicological screen for paracetamol.
Management: gastric lavage within 4 h of in-gestion, and antidote therapy.
There is now evidence to support the treatment ofall patients with paracetamol intoxication with anantidote, regardless of the time of presentation, evenif treatment is initiated when the patient hasestablished fulminant hepatic failure [14].
The antidote should be used in patients whopresent at less than 8 h if more than 7 g ofparacetamol has been ingested, or if the plasmaconcentration of paracetamol is above the lower lineon the plot of paracetamol concentrations in re-lationship to time after overdose, shown in figure 2.Patients receiving enzyme-inducing agents shouldbe treated at 70% smaller concentrations.
At early presentation (within 8h of ingestion),methionine may be given (2.5 g immediately, fol-lowed by three further doses 4-hourly). Patientspresenting more than 8 h after ingestion of para-cetamol should have their plasma paracetamol con-centration assayed immediately. Antidote shouldthen be given without delay and the paracetamolconcentration checked again 4 h later. Failure of theplasma paracetamol concentration to decrease by50 % may signify impending liver damage.
The antidote regimen should comprise acetyl-cysteine i.v. 150 mg/kg body weight in 5 % glucose200 ml over 15 min, followed by 50 mg/kg bodyweight in 5 % glucose 500 ml over 4 h, followed by100 mg/kg body weight in 5 % glucose 1000 ml over16 h.
Occasionally, a histamine-mediated reactiondevelops in response to acetylcysteine.
Other aspects of management. Check clottingfactors, electrolyte concentrations and liver functiontests. Monitor capillary blood glucose concentrationhourly. Monitor the patient's level of consciousness.Give glucose by i.v. infusion, to a total of 300 g daily.Observe for onset of renal failure. Renal dialysis maybe necessary.
If ingestion was more than 24 h before pres-entation, and intoxication is assumed to be moderateto severe, observe for evidence of hepatocellularfailure (deteriorating level of consciousness; in-creasing prothrombin time; pH less than 7.3) andintroduce routine therapy for liver failure (thesepatients should be treated in an intensive therapyunit).
Referral to a centre particularly interested in themanagement of patients with paracetamol intoxi-cation should be considered under the followingcircumstances [15]:
pH < 7.3 more than 24 h after ingestionProthrombin time > 45 s at 48 h
> 50 s at 72 hIncreasing serum creatinine concentrationRapid development of grade 2 encephalopathyLiver transplantation may be considered under
the following circumstances [15]:pH < 7.3Prothrombin time > 100 sSerum creatinine concentration > 300 umol litre"1
Coma grade 3 or 4Increasing prothrombin time from day 3 to day 4
after overdose.
Cocaine intoxicationPharmacology. Cocaine (benzoylmethylecognine)
is absorbed from all mucosal surfaces and is mostcommonly taken i.v., by insufflation (intranasal) andby smoking (pulmonary). When it is insufflated, thepeak action occurs at 30 min and lasts 60 min. Thepharmacokinetic properties of i.v. cocaine are similarto those of smoked or inhaled cocaine.
" Crack " is the poorly water-soluble alkaloid formof cocaine, and is smoked. The onset of action iswithin minutes, and is dissipated within 20 min.
If ingested with alcohol, cocaine may be metabol-ized in the liver to a longer lasting more lethalmetabolite [31].
Presentation. Clinical effects are the result of bothperipheral and central nervous system stimulation.CNS stimulation: Euphoria, agitation, confusion;seizures; hyperthermia.Peripheral vasomotor stimulation by noradrenalineresults in tachycardia and hypertension.
Complications. Transient ischaemic attacks; cere-bral haemorrhage; cardiac arrhythmias; hyper-thermia leading to disseminated intravascular co-agulation, cerebral oedema and rhabdomyolysis withacute renal failure; acute psychosis—paranoia, hal-lucinations and aggressive behaviour.
Differential diagnosis is from other conditionscausing hypoxia, seizures, or both. The clinicalpicture may mimic neuroleptic malignant syndromeor acute withdrawal from sedative or hypnotic drugs
THE MANAGEMENT OF ACUTE POISONING 569
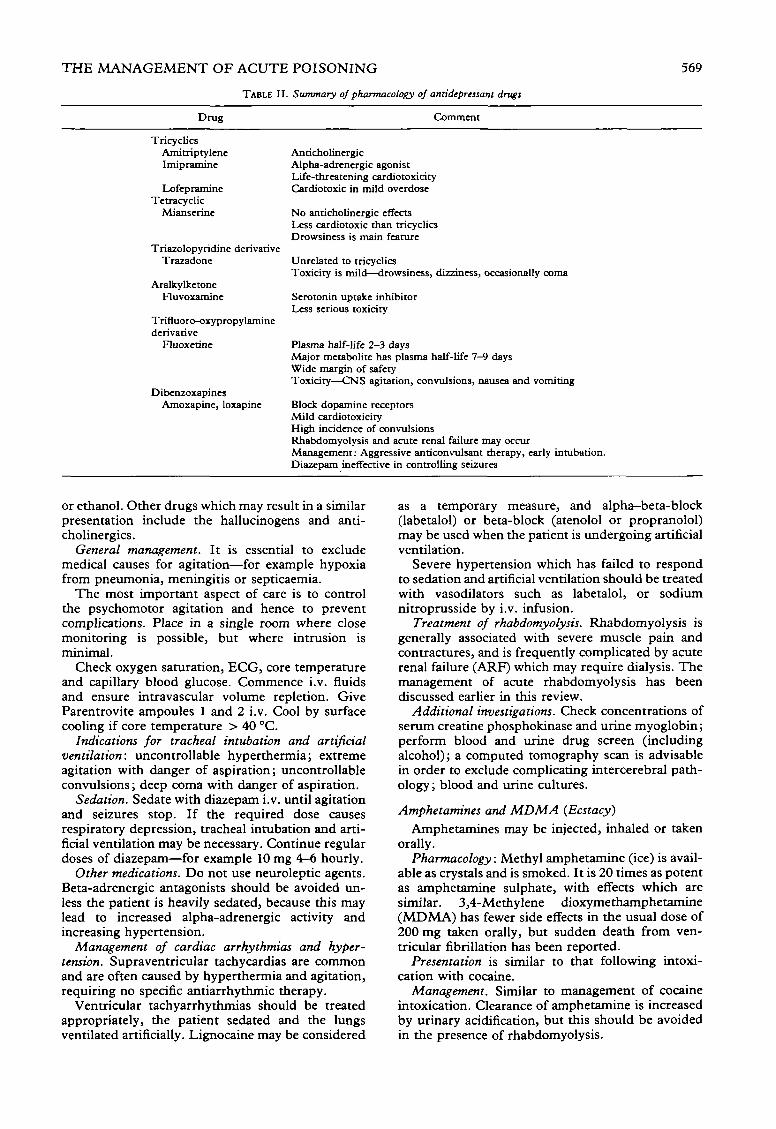
TABLE II. Summary of pharmacology of antidepressam drugs
Drug Comment
TricyclicsAmitriptyleneImipraminc
LofepramineTetracyclic
Mi anserine
Triazolopyridine derivativeTrazadone
AralkylketoneFluvoxamine
Trifluoro-oxypropylaminederivative
Fluoxetine
D ibenzoxapinesAmoxapine, loxapine
AnticholinergicAlpha-adrenergic agonistLife-threatening cardiotoxicityCardiotoxic in mild overdose
No anticholincrgic effectsLess cardiotoxic than tricyclicsDrowsiness is main feature
Unrelated to tricyclicsToxicity is mild—drowsiness, dizziness, occasionally coma
Serotonin uptake inhibitorLess serious toxicity
Plasma half-life 2-3 daysMajor metabolite has plasma half-life 7-9 daysWide margin of safetyToxicity—CNS agitation, convulsions, nausea and vomiting
Block dopamine receptorsMild cardiotoxicityHigh incidence of convulsionsRhabdomyolysis and acute renal failure may occurManagement: Aggressive anticonvulsant therapy, early intubation.Diazepam ineffective in controlling seizures
or ethanol. Other drugs which may result in a similarpresentation include the hallucinogens and anti-cholinergics.
General management. It is essential to excludemedical causes for agitation—for example hypoxiafrom pneumonia, meningitis or septicaemia.
The most important aspect of care is to controlthe psychomotor agitation and hence to preventcomplications. Place in a single room where closemonitoring is possible, but where intrusion isminimal.
Check oxygen saturation, ECG, core temperatureand capillary blood glucose. Commence i.v. fluidsand ensure intravascular volume repletion. GiveParentrovite ampoules 1 and 2 i.v. Cool by surfacecooling if core temperature > 40 °C.
Indications for tracheal intubation and artificialventilation: uncontrollable hyperthermia; extremeagitation with danger of aspiration; uncontrollableconvulsions; deep coma with danger of aspiration.
Sedation. Sedate with diazepam i.v. until agitationand seizures stop. If the required dose causesrespiratory depression, tracheal intubation and arti-ficial ventilation may be necessary. Continue regulardoses of diazepam—for example 10 mg 4—6 hourly.
Other medications. Do not use neuroleptic agents.Beta-adrenergic antagonists should be avoided un-less the patient is heavily sedated, because this maylead to increased alpha-adrenergic activity andincreasing hypertension.
Management of cardiac arrhythmias and hyper-tension. Supraventricular tachycardias are commonand are often caused by hyperthermia and agitation,requiring no specific antiarrhythmic therapy.
Ventricular tachyarrhythmias should be treatedappropriately, the patient sedated and the lungsventilated artificially. Lignocaine may be considered
as a temporary measure, and alpha—beta-block(labetalol) or beta-block (atenolol or propranolol)may be used when the patient is undergoing artificialventilation.
Severe hypertension which has failed to respondto sedation and artificial ventilation should be treatedwith vasodilators such as labetalol, or sodiumnitroprusside by i.v. infusion.
Treatment of rhabdomyolysis. Rhabdomyolysis isgenerally associated with severe muscle pain andcontractures, and is frequently complicated by acuterenal failure (ARF) which may require dialysis. Themanagement of acute rhabdomyolysis has beendiscussed earlier in this review.
Additional investigations. Check concentrations ofserum creatine phosphokinase and urine myoglobin;perform blood and urine drug screen (includingalcohol); a computed tomography scan is advisablein order to exclude complicating intercerebral path-ology; blood and urine cultures.
Amphetamines and MDMA (Ecstacy)Amphetamines may be injected, inhaled or taken
orally.Pharmacology: Methyl amphetamine (ice) is avail-
able as crystals and is smoked. It is 20 times as potentas amphetamine sulphate, with effects which aresimilar. 3,4-Methylene dioxymethamphetamine(MDMA) has fewer side effects in the usual dose of200 mg taken orally, but sudden death from ven-tricular fibrillation has been reported.
Presentation is similar to that following intoxi-cation with cocaine.
Management. Similar to management of cocaineintoxication. Clearance of amphetamine is increasedby urinary acidification, but this should be avoidedin the presence of rhabdomyolysis.
570 BRITISH JOURNAL OF ANAESTHESIA
Heroin (diamorphine)Heroin deaths are caused generally by respiratory
depression with or without pulmonary aspiration.This may occur with first use, change in drug access(variability in purity) or loss of tolerance after aperiod of abstinence.
Presentation: coma, with slow ventilatory fre-quency (terminating in apnoea); pinpoint pupils (notpresent in pethidine intoxication).
Diagnosis. Classically, a temporary reversal ofcoma and respiratory depression is achieved withnaloxone 0.8-2 mg i.v. Antagonism may requirelarger doses of naloxone if the intoxication is causedby pethidine, buprenorphine, or dextropropoxy-phene, and may be suppressed by the presence ofother drugs.
Treatment. Some authors suggest the use of i.v.naloxone to maintain antagonism. In our opinion,this requires very careful titration, and we consider itsafer to intubate the trachea and ventilate the lungsuntil the intoxicant effect has worn off spon-taneously.
Complications include pulmonary aspiration, non-cardiogenic pulmonary oedema, rhabdomyolysis andinfective complications in i.v. drug abusers.
Drug couriers. "Body packers" as they are termed,smuggle drugs by concealment in and around thebody. Should the drug be swallowed in a container(e.g. condom, plastic bag or vial), leakage may lead tosevere toxicity. A recent plane journey may be anindication for an abdominal x-ray. Surgical removalfrom the bowel may be indicated.
Psychoactive DrugsPharmacology. The antidepressant agents have dif-fering activities, summarized in table II.
Tricyclic intoxicationPresentation. Cardiovascular and neurological fea-
tures dominate the clinical picture.Cardiac: hypotension; cardiac arrhythmias (ven-
tricular and atrial); ECG abnormalities (PR, QRSand QTc prolongation). A right bundle branch blockpattern is characteristic [3]. With QRS > 0.1 s, con-vulsions are likely; QRS > 0.16 s, ventriculararrhythmias are likely. Terminally, refractory hy-potension may occur, leading to electromechanicaldissociation (EMD).
CNS: convulsions; agitation, hallucinations; comaand respiratory depression.
General management. In any patient with evidenceof a cardiac arrhythmia, twitching or respiratorydepression, the trachea should be intubated and thelungs ventilated. Therefore, in the majority of severeintoxications, even if the patient is still conscious,he/she should undergo elective ventilation.
This management is recommended because res-piratory depression, hypercapnia and hypoxia oftenprecipitate cardiac arrhythmias; acidosis, whetherrespiratory or metabolic, enhances cardiotoxicity;and intubation of the trachea and ventilation of thelungs ensure preservation of the airway and safe useof anticonvulsants (e.g. benzodiazepines) which areless negatively inotropic than phenytoin.
Management of myocardial depression and arrhyth-mias. With good oxygenation and maintenance of pH> 7.4, cardiac arrhythmias usually resolve. Smallincremental doses of sodium bicarbonate 50 mmolshould be used to maintain pH > 7.4 if hyper-ventilation fails to achieve that goal. EMD may beprecipitated by the administration of negativelyinotropic agents; these should be avoided unless thearrhythmia is so bizarre that the cardiac output is notbeing maintained. Sodium bicarbonate 50 mmol i.v.may be effective, but if this fails, small incrementaldoses of lignocaine are probably the safest treatment.
Inotropes may be required, and dobutamine issuitable. Invasive haemodynamic monitoring with apulmonary artery catheter is tempting, but should beavoided because insertion of the catheter during theacute early phase may precipitate a dangerousarrhythmia. Whilst d.c. shock may be used, it mayprecipitate asystole or EMD. The joule dosageshould be kept to a minimum.
Physostigmine is not recommended.Cardiac toxicity generally resolves within 6 h, and
artificial ventilation for control of convulsions israrely indicated after 24 h.
Monoamine Oxidase InhibitorsPharmacology. Overdose of these drugs alone doesnot produce any serious effects. Severe toxicity mayoccur when they are taken together with foodstuffsor drugs contraindicated during their use (e.g. foodscontaining precursors of biogenic amines such astyramine, or drugs such as tyramine, sympatho-mimetic amines or amphetamine).
Presentation. Symptoms develop progressivelyover 12-24 h and include: muscle twitching, leadingto diffuse muscle spasm, trismus and opisthotonos;fluctuations in arterial pressure with tachycardia;fixed, dilated pupils; hot sweaty peripheries andincreased core temperature.
Complications include rhabdomyolysis, acute re-nal failure and disseminated intravascular coagul-opathy.
Management. Control of core temperature > 39 °Cby sedation, paralysis and cooling. Control ofhaemodynamic state, with invasive monitoring asrequired.
Antipsychotic DrugsPharmacology. These are the phenothiazine deriva-tives and may be grouped according to theirdominant effects:Group 1 (e.g. chlorpromazine): characterized bypronounced sedative effects and moderate anti-cholinergic and extrapyramidal effects.Group 2 (e.g. thioridazine): characterized by mod-erate sedative effects, marked anticholinergic effectsand fewer extrapyramidal effects than groups 1 or 3.Group 3 (e.g. perphenazine): characterized by fewersedative effects and anticholinergic effects, but morepronounced extrapyramidal effects than groups 1and 2.
Presentation. Clinical features may include: res-piratory depression; cardiac arrhythmias (the ECGmay show a prolonged QT interval); sudden death(probably as a result of torsades de pointes); dystonia

THE MANAGEMENT OF ACUTE POISONING 571
(generally relieved by procyclidine 5-10 mg i.v.);coma and convulsions; hypothermia; neurolepticmalignant syndrome (confusion, muscle pain andrigidity, rhabdomyolysis, fever).
General management: supportive care; maintainpH > 7.4; ensure a normal serum potassium con-centration.
Management of torsades de pointes: d.c. shock andcardiac pacing 20 beat min"1 greater than thepatient's sinus rhythm; infusion of isoprenaline2-6 ug min"1 may be tried whilst pacing is es-tablished.
Sedative and Hypnotic Agents
Benzodiazepine overdosage
Death is caused by respiratory depression andaspiration of vomitus, but note that these drugs areoften taken in combination with other drugs, result-ing in a confusing clinical picture.
In our opinion, flumazenil should not be used fortreatment because it may precipitate convulsions oracute withdrawal syndromes, and it has a short half-life (1-2 h), making repetitive doses and continuedmonitoring necessary.
Management: supportive care with intubation andventilation if required.
Carbon monoxide poisoning
In England and Wales, approximately 1000 peopledie every year from carbon monoxide poisoning.Most of these patients do not reach hospital.Common sources of carbon monoxide are car exhaustfumes, improperly maintained and ventilated heatingsystems, smoke from fires, and household gas.
Pharmacology. Carbon monoxide has an affinityfor haemoglobin which is 200-250 times that ofoxygen. Carbon monoxide combines with haemo-globin to form carboxyhaemoglobin, and the affinityfor oxygen of the remaining haem is increased.Carbon monoxide toxicity is caused by cellularanoxia, and possibly also inhibition of cellularrespiration as a result of binding to other haemproteins. The elimination half-life of carbon mon-oxide is reduced from 250 min when the subject isbreathing air, to 59 min breathing 100% oxygen,and is reduced further to 22 min when 100 % oxygenis breathed at 2.2 atm.
The severity of poisoning depends on the con-centration of carbon monoxide in the air, theduration of exposure and the person's general health.
Presentation. Repeated exposure: headache;fatigue; poor memory and concentration; dizzinessand paraesthesia; visual disturbances; chest pain;diarrhoea and abdominal pain.Acute exposure: carboxyhaemoglobin < 10%—generally no symptoms; carboxyhaemoglobin> 60 %—coma, leading to cardiorespiratory arrest.
Late sequelae may include neuropsychiatricsequelae which may develop weeks after exposure(memory loss, impaired intellect, signs of cerebellarand mid-brain damage).
Signs of poisoning include: cherry red skin, coma,hyper-reflexia, convulsions and cardiac arrhythmias.
General management. Remove from site; admin-ister 100% oxygen via tight fitting face mask
(where there is respiratory depression or difficultywith airway control, intubate the trachea andventilate the lungs with 100% oxygen); in cases ofsevere poisoning, assume cerebral oedema and treataccordingly.
Indications for hyperbaric oxygen therapy in-clude: a conscious patient with a carboxy-haemoglobin > 20 %; depressed level of conscious-ness, but able to maintain airway; recovery ofconsciousness after an initial carboxyhaemoglobin >40%.
Contraindications to hyperbaric oxygen therapyvia a single person chamber include: artificialventilation; inability to maintain an airway;hypovolaemia or dependence on cardiac inotropes;cardiac arrhythmias potentially requiring urgentintervention; asthma.
These contraindications arise because of thepractical difficulties of managing such patients insingle person hyperbaric oxygen chambers, and thelimited availability of compressed air chambers inwhich medical attendants can also be pressurized.All patients fulfilling die indications for hyperbaricoxygen therapy should be discussed with the regionalhyperbaric oxygen facility. (The availability ofhyperbaric oxygen facilities may be ascertained bycontacting the Diving Diseases Research Centre,who provide a 24-h service. Tel.: 0752-261-910.)
Lithium intoxicationPharmacology. This metal is eliminated by the
kidney, therefore renal failure may lead to accumu-lation. Other circumstances which may lead totoxicity when lithium is being used for treatmentinclude dehydration and concomitant administrationof non-steroidal anti-inflammatory agents ordiuretics.
Presentation. Neurological: confusion, agitation;hyper-reflexia, hypertonia, tremor; ataxia; con-vulsions.Gastrointestinal: vomiting.Metabolic: hyponatraemia; diabetes insipidus; renalfailure.
The therapeutic range in blood is lithium1.0-1.4 mmol litre"1. In acute poisoning the lithiumconcentration is generally > 5.0 mmol litre"1.
General management: gastric lavage up to 4 h afteringestion; forced diuresis. In the presence of neuro-logical symptoms, renal failure, or both, haemo-dialysis should be performed.
APPENDIX
OTHER POISONINGS
Space docs not allow for details about other poisons. Readers arereferred to the following texts for further information on themanagement of specific poisons:
Alcohols and elhylene glycolBuckley BM, Vale JA. Poisoning by alcohols and ethylene glycol.Prescribers' Journal 1986; 26: 109-114.Galliot M, Astier A, Vu Bien D, Gamier R, Likforman J,Bismuth C. Treatment of ethylene glycol poisoning with in-travenous 4-methylpyrazole. New England Journal of Medicine1988; 319: 97-100.
572
AnticonvulsantsDupuis RE, Lichtman SN, Pollack GM. Acute valproic acidoverdose—clinical course and pharmacokinetic disruption ofvaproic acid metabolites. Drug Safety 1990; 5: 65-71.Henry JA. Anticonvulsants. Care of the Critically III 1991; 7: 102.Mauro LS, Mauro VF, Brown DL, Somani P. Enhancement ofphenytoin elimination by multiple dose activated charcoal. Annalsof Emergency Medicine 1987; 16: 1132.
Beta-2 agonists and theophylline poisoningVale JA. Poisoning with respiratory drugs. Prescribers' Journal1986; 26: 107-110.
Cardiac drugsMartiny SS, Phelps SJ, Maney KL. Treatment of severe digitalisintoxication with digoxin-specific antibody fragments: a clinicalreview. Critical Care Medicine 1988; 27: 21-56.
Chloroquim poisoningRiou B, Barriot P, Rimailho A, Baud FJ. Treatment of severechloroquine poisoning. New England Journal of Medicine 1988;318: 1-6.Consensus Committee, Societe de Reanimation de LangueFrancaise. Treatment of Acute Chloroquine Poisoning. Intensiveand Critical Care Digest 1992; 11: 5.
Inhalation agents as poisonsBlain PG. Sulphur mustard and nerve agents, organophosphoruspoisonings—chemical warfare agents. Care of the Critically III1991; 7: 91-96.
Mushroom poisoningEditorial. Death-cap poisoning. Lancet 1972; 1: 1320-1321.I .anger M, Verconi S, Constantino D. In: Vincent JL, ed. Updatein Intensive Care and Emergency Medicine. Berlin: Springer-Verlag, 1990; 482^193.
Paraquat poisoningVolans GN, Byart GM. Poisoning from domestic products.Prescribers' Journal 1986; 26: 92-93.
Quinine intoxicationProudfoot AT. Acute poisoning: an update. Current problem—quinine. Prescribers' Journal 1986; 26: 80-82.
SolventsFlanagan RJ, Ruprah M, Meredith TJ, Ramsay JD. Anintroduction to the clinical toxicology of volatile substances. DrugSafety 1990; S: 359-383.Henry JA. Volatile substance abuse. Care of the Critically III1991; 7: 105.
REFERENCES1. Abuelo JG. Renal failure caused by chemicals, foods, plants,
nnimnl venoms, and misuse of drugs. An overview. Archivesof Internal Medicine 1990; ISO: 505-510.
2. Ashton CH. Benzodiazepine overdose: are specific antagonistsuseful? British Medical Journal 1985; 290: 805-806.
3. Boehert MT, Lovejoy FH. Value of the QRS duration versusthe serum drug level in predicting seizures and ventriculararrhythmias after an acute overdose of tricylic anti-depressants. New England Journal of Medicine 1985; 313:474-479.
4. Cutler RE, Forland SQ Hammond PGStJ, Evans JR.Extracorporeal removal of drugs and poisons by hemodialysisand hemoperfusion. Annual Review of Pharmacology andToxicology 1987; 27: 169-191.
5. Department of Health and Social Security. Hospital InpatientEnquiry for 1979. London: HMSO, 1981.
6. Done AK. Salicylate intoxication: significance of salicylateblood levels in cases of acute ingestion. Pediatrics 1960; 26:800-807.
BRITISH JOURNAL OF ANAESTHESIA
7. Flanagan RJ, Huggett A, Saynor DA, Raper SM, VolansGN. Value of toxicological investigation in the diagnosis ofacute drug poisoning in children. Lancet 1981; 2: 682-685.
8. Fuller GN, Rea AJ, Payne JF, Lant AF. Parasuicide incentral London 1984-1988. Journal of the Royal Society ofMedicine 1989; 82: 653-656.
9. Harsch HH. Aspiration of activated charcoal. New EnglandJournal of Medicine 1986; 314: 318.
10. Helliwell M, Hampel G, Sinclair E, Huggett A, Flanagan RJ.Value of emergency toxicological investigations in differentialdiagnosis of coma. British Medical Journal 1979; 2: 819-821.
11. Henry J, Volans G. ABC of Poisoning - Diagnosis. BritishMedical Journal 1984; 289: 172-174.
12. Henry J, Volans G. ABC of poisoning. Preventing Ab-sorption. British Medical Journal 1984; 289: 304-305.
13. Ilett KF, Gibb SM, Unsworth RW. Syrup of ipecacuanha asan emetic in adults. Medical Journal of Australia 1977; 2:91-93.
14. Keays R, Harrison PM, Wendon JA, Forbes A, Gove C,Allexander GJM, Williams R. Intravenous acerylcysteine inparacetamol-induced hepatic failure: a prospective controlledtrial. British Medical Journal 1991; 303: 1026-1029.
15. Keays R, Williams R. Paracetamol poisoning and liver failure.Prescribers'Journal 1989; 29: 155-162.
16. Kirshenbaum LA, Mathews SC, Sitar DS, Tenenbcin M.Does multiple-dose charcoal therapy enhance salicylateexcretion? Archives of Internal Medicine 1990; 150:1281-1283.
17. Lheureux P, Even-Adin D, Askenasi R. Current status ofantidotal therapies in acute human intoxications. Ada ClinicaBelgica Supplcmentum 1990; 13: 29-47.
18. Levy G. Gastrointestinal clearance of drugs with activatedcharcoal. New England Journal of Medicine 1982; 307:676-678.
19. Levy G, Houston JB. Effect of activated charcoal onacetaminophen absorption. Pediatrics 1976; 58: 432-435.
20. Levy G, Tsuchiya T. Effect of activated charcoal on aspirinabsorption in man Part 1. Clinical Pharmacology andTherapeutics 1972; 13: 317-322.
21. Leykin Y, Halpem P, Silbiger A, Sorkin P, Niv D, Rudick V,Geller E. Acute poisoning treated in the intensive care unit:A case series. Israel Journal of Medical Sciences 1989; 25:98-102.
22. Locket S. Evaluation of various forms of treatment admin-istered in poisoning. Practitioner 1973; 210: 709-714.
23. Meadow R. ABC of Child Abuse - Poisoning. British MedicalJournal 1989; 298: 1445-1446.
24. Menzies DG, Busuttil A, Prescott LF. Fatal pulmonaryaspiration of oral activated charcoal. British Medical Journal1988; 297: 459-460.
25. Merigian KS, Woodard M, Hedges JR, Roberts JR, StuebingR, Rashkin MC. Prospective evaluation of gastric emptyingin the self poisoned patient. American Journal of EmergencyMedicine 1990; 8: 479-483.
26. Meulemans A, Van den Berghe G, Delooz WH. Gastro-intestinal decontamination for acute poisoning. Ada ClinicaBelgica Supplementum 1990; 13: 13-19.
27. Nejman G, Hoekstra J, Kelly M. Journal Club: Gattricemptying in the poisoned patient. American Journal ofEmergency Medicine 1990; 8: 265-269.
28. Neuvonen PJ, Vartiainen M, Tokola O. Comparison ofactivated charcoal and ipecac syrup in prevention of drugabsorption. European Journal of Clinical Pharmacology 1983;24: 557-562.
29. Office of Population Censuses and Surveys. MortalityStatistics for England and Wales 1990. London: HMSO, 1991(DH 2 series No. IT).
30. Prescott LF, Park J, Sutherland GR, Smith IJ, ProudfootAF. Cysteamine, methionine, and pencillamine and thetreatment of paracetamol poisoning. Lancet 1976; 2: 109.
31. Randall T. Cocaine, alcohol mix in body to form even longerlasting, more lethal drug. Journal of the American MedicalAssociation 1992; 267: 1043-1044.
32. Reid DHS. Ipecac syrup for poisoned children. Lancet 1969;1: 261.
33. Stem TA, Mulley AG, Thibault GE. Life-threatening drugoverdose. Journal of the American Medical Association 1984;251: 1983-1985.
34. Vale A, Meredith T, Buckley B. ABC of poisoning.

THE MANAGEMENT OF ACUTE POISONING 573
Eliminating poisons. British Medical Journal 1984; 289:366-369.
35. Vale JA, Meredith TJ, Proudfoot AT. Syrup of ipecacuanha:is it really useful? British Medical Journal 1986; 293:1321-1322.
36. Watson WA, Cremer KF, Chapman JA. Gastrointestinalobstruction associated with multiple-dose charcoal. Journal ofEmergency Medicine 1986; 4: 401-407.
37. Wheeler-Usher DH, Wanke LA, Bayer MJ. Gastric emp-
tying. Risk versus benefit in the treatment of acute poisoning.Medical Toxicology 1986; 1: 142-153.
38. Winchester JF, Gelfland MC. Hemoperfusion in drugintoxication: clinical and laboratory aspects. Drug MetabolismReviews 1978; 8: 69-104.
39. Wright N. An assessment of the unreliability of the historygiven by self-poisoned patients. Clinical Toxicology 1980; 16:381-384.