The investment you make in yourself today will determine ... · P E R S O N A L S E L F HE L P M A...
136
PERSONAL SELF HELP MANUAL "The investment you make in yourself today will determine the quality of your life in the days and years to come." Author Unknown OWNER: ____________________________________________________ IMPORTANT DISCLAIMER: Before starting any health / fitness / wellness program, all individuals should consult with their physician or primary health care provider. All information, provided by the publisher, in this handbook is of general nature for your own personal use. No material in this handbook is to be taken as medical, health, wellness or fitness advice. This material is not a treatment plan, a recommendation, or a course of action for any individual. The publisher and / or it’s associates are not liable or responsible, in whole or in part, to any person, or entity for any injury, or damage, or loss of any sort, caused or alleged to be caused directly or indirectly by the use, practice or dissemination of any of the techniques, information, or ideas presented in this handbook. It remains your responsibility to evaluate the complete usefulness of the handbook. Some information on various charts are referenced to their credited sources.
Transcript of The investment you make in yourself today will determine ... · P E R S O N A L S E L F HE L P M A...

PERSONAL SELF HELP MANUAL
"The investment you make in yourself today will determine the quality of your life in the days and years to come." Author Unknown OWNER: ____________________________________________________ IMPORTANT DISCLAIMER: Before starting any health / fitness / wellness program, all individuals should consult with their physician or primary health care provider. All information, provided by the publisher, in this handbook is of general nature for your own personal use. No material in this handbook is to be taken as medical, health, wellness or fitness advice. This material is not a treatment plan, a recommendation, or a course of action for any individual. The publisher and / or it’s associates are not liable or responsible, in whole or in part, to any person, or entity for any injury, or damage, or loss of any sort, caused or alleged to be caused directly or indirectly by the use, practice or dissemination of any of the techniques, information, or ideas presented in this handbook. It remains your responsibility to evaluate the complete usefulness of the handbook. Some information on various charts are referenced to their credited sources.

Personal Self Help Manual E-book
INDEX Section Topics General Section Chart # Page # 1. Confidentiality Form – 8 2. 2008 Annual Calendar Form – 9 3. Blank Monthly Calendar Form – 10 4. Blank Daily Calendar Form – 11 5. Blank Weekly Calendar Form – 12 6. Dates to Remember Form – 13 7. Weights and Measures Form – 14 8. Websites, User Names etc. Form – 15 9. Meal Planner Form – 16 10. Full Day Meal Planner Form – 17 11. Table Seating Plan Form – 18 12. Movie List Form – 19 13. Birthstone Gift Form – 20 14. Laundry Labels Sheet #1 – 21 15. Laundry Labels Sheet #2– 22 16. Laundry Labels Sheet #3 – 23 17. Daily Food Guide– General Section - 24 18. Recipe Index– 25 19. Recipe Blank Cards – 26 20. Recipe Blank Cards Sheet 2 – 27 21. Recipe Blank Sheet 3 – 28 22. Statutory Holiday Planner– 29 23. Pet Record Chart– 30 24. Pet Dedication– 31 25. Pet Stories & Pictures– 32 26. Pet Memories & Pictures– 33 27. Christmas Holiday Plan – 34 28. Christmas Budget – 35 29. Christmas Card List - 36 30. Christmas Gift Shopping - 37

Health Section 31. Medical Alerts Form – 39 32. Medical History Form – 40 33. Medication Form – 41 34. Daily Health Form – 42 35. Daily Health Sheet 2 Form – 43 36. Blood Pressure Record Form – 44 37. Medical Tests Record Form – 45 38. Medical Health Contacts Form – 46 39. Food Diary Form – 47 40. Men & Woman Weight & Height Chart – 48 41. Metric Weights Men & Woman– 49 42. Calories in Alcohol Drink – 50 43. Child’s Health Record– 51 Fitness Section 44. Exercise Schedule Form – 53 45. Daily Fitness Chart – 54 46. Daily Fitness Chart – 55 47. Daily Total Progress Chart – 56 48. Monthly Total Progress Chart – 57 49. Annual Personal Progress Chart – 58 50. Food Energy Counts Chart – 59 51. Fitness Contacts – 60 52. Body Mass Index Chart – 61 53. Activity Fitness Chart – 62 54. Calories Burnt During Activities Chart – 63 55. Record Child’s Growth Chart – 64 Wellness Section
56. Gratitude Exercise Info – 66 57. Gratitude Exercise Form – 67 58. My Goals Form – 68 59. Make Changes Form – 69 60. Decisions Pros & Cons Form – 70 61. Balanced Lifestyle Plan Form – 71 62. Achievement, Successes Form – 72 63. Areas for Improvement Form – 73 64. Wellness Contacts – 74 65. Daily / Weekly Diary– 75 66. Problem Solver– 76

Financial Section 67. Finances Checklist Form – 78 68. Monthly Payments Form– 79 69. Record of Bill Payments Form– 80 70. Quarterly, Semi/Annual Expenses Form– 81 71. Basic Monthly Expenses Form– 82 72. Basic Semi/Annual Expenses Form– 83 73. Financial Contacts Form– 84 74. Bank Reconciliation Form Sheet #1– 85 75. Bank Reconciliation Form Sheet #2– 86 76. House & Mortgage Information – 87 Organization Section 77. Confidential Information Checklist Form – 89 78. Event Planner Form – 90 79. Grocery Shopping Form – 91 80. Things to Do Form – 92 81. Detailed Contact Information – 93 82. Family, Friends & Co-Worker Gift List – 94 83. Daily Organizer – 95 84. Personal Property Inventory Sheet 1– 96 85. Personal Property Inventory Sheet 2– 97 86. Personal Property Inventory Sheet 3– 98 87. Personal Property Inventory Sheet 4 - 99 88. Shopping Websites – 100 89. Contact Information – 101 Family Section 90. Fire Home Escape Form – 103 91. Our Family Chart – 104 92. Family Birthday Chart – 105 93. Family Weekly Schedule Chart – 106 94. Company/Guests/Visitors Chart – 107 95. Personal Contacts – 108 96. Family Traditions – 109 97. Positive Reward System Chart – 110 98. ‘Find It Treasure” Cutout Cards – 111 99. Family Tree Sheet 1– 112 100. Family Tree Sheet 2– 113 101. Family Tree Sheet 3– 114

102. Family Tree Sheet 4– 115 103. Family Tree Beginning– 116 104. Family Tree Index– 117 105. Family Tree (Grand) Children– 118 106. Family Tree Siblings/Nieces-Nephew– 119 107. School Days Book Cover– 120 108. School Days Index– 121 109. School Days Grades K-13-122 110. School Days Awards/Achievements– 123
Travel Section 111. Travel Itinerary Form – 125 112. Items to Pack Form – 126 113. Reminders Form – 127 114. Places I have Visited Form – 128 115. Daily Vacation Itinerary Form – 129 116. Travel Contacts – 130 117. Vacation Budget – 131 118. Vacation Scheduler – 132 119. Vehicle Log – 133 Journaling Section 120. Journaling Form - 135

PERSONAL SELF HELP MANUAL - SECTIONS
PAGE # SECTION TOPIC

GENERAL SECTION
TABLE OF CONTENTS
PAGE # TOPIC / DESCRIPTION / TITLE

THIS
PERSONAL SELF HELP MANUAL
BELONGS TO:
Enter your name here:_________________________________________________________________ Your personal health is very private and confidential. You may wish to have certain loved ones, friends or Health Care Providers have reference to the information that you have recorded into your manual. Here is a section for you to list person (s) whom you permit to have access to the contents in your manual. Enter a list of person(s) whom you permit to have access to your manual:
NAME RELATIONSHIP TO YOU
1). ________________________________________________________________________________
2.) _______________________________________________________________________________
3.) _______________________________________________________________________________
4.) _______________________________________________________________________________
5.) _______________________________________________________________________________
6.) _______________________________________________________________________________
7.) _______________________________________________________________________________
8.) _______________________________________________________________________________
9.) _______________________________________________________________________________
10.) _______________________________________________________________________________
2008 ANNUAL CALENDAR – GENERAL
PUBLIC HOLIDAYS ANNUAL NOTES New Year's Day Jan. 1 ___________________________________ Family Day Feb. 18 Good Friday March 21 ___________________________________ Easter Sunday March 23 Victoria Day May 19 ___________________________________ Canada Day July 1 Labour Day Sept. 1 ___________________________________ Thanksgiving Day Oct. 13 Remembrance Day Nov. 11 ___________________________________ Christmas Dec. 25 Boxing Day Dec. 26 ___________________________________

MONTHLY CALENDAR:_____________________________
SUN MON TUE WED THUR FRI SAT
NOTES:

DAILY CALENDAR:_____________________________
Time Task

WEEKLY CALENDAR:_____________________________ DAY TIME

DATES TO REMEMBER
DATE EVENT TO REMEMBER

WEIGHTS & MEASURES
Volume Conversions Imperial Metric
1/4 teaspoon (tsp) 1.25 ml (milliliter) 1/2 tsp 2.5 ml 1 tsp 5 ml 1 tablespoon (tbsp) 15 ml 1/4 cup 60 ml
1/3 cup 75 ml 1/2 cup 125 ml 2/3 cup 150 ml 3/4 cup 175 ml 1 cup 250 ml 1 1/8 cups 275 ml 1 1/4 cups 300 ml
1 1/2 cups 350 ml 1 2/3 cups 400 ml 1 3/4 cups 450 ml 2 cups 500 ml 2 1/2 cups 600 ml 3 cups 750 ml 3 2/3 cups 900 ml 4 cups 1 liter
METRIC CONVERSTIONS Multiply By To Get Fluid Ounces 29.57 grams Ounces (dry) 28.35 grams Grams 0.0353 ounces Grams 0.0022 pounds Kilograms 2.21 pounds Pounds 453.6 grams Pounds 0.4536 kilograms Quarts 0.946 liters Quarts (dry) 67.2 cubic inches Quarts (liquid) 57.7 cubic inches Liters 1.0567 quarts Gallons 3,785 cubic centimeters Gallons 3.785 liters
Weights Measurements Imperial Metric Imperial Metric
1/2 ounce (oz) 15 g (grams)1/4 in (inch) 5 mm (millimeter)
1 oz 25 g 1/2 in 1 cm (centimeter) 2 oz 50 g 1 in 2.5 cm
3 oz 75 g 2 in 5 cm 4 oz 100 g 3 in 7 cm 6 oz 175 g 4 in 10 cm 7 oz 200 g 5 in 12 cm 8 oz 250 g 6 in 15 cm 9 oz 275 g 7 in 18 cm 10 oz 300 g 8 in 20 cm 12 oz 350 g 9 in 23 cm 1 lb (pound) 500 g 10 in 25 cm 1 1/2 750 g 11 in 28 cm
2 lb 1 kg (kilogram)
12 in (1 foot)
30 cm
Oven Heat Conversions Fahrenheit Celsius Oven Heat
225º 110º very cool 250º 120º very cool 275º 140º cool 300º 150º cool 325º 160º moderate
350º 180º moderate 375º 190º moderately hot 400º 200º moderately hot 425º 220º hot 450º 230º very hot

INTERNET WEBSITE LOG-IN, USER-NAME, PASSWORDS
WEBSITE ADDRESS
WEBSITE TITLE
EMAIL ADDRESS
USER NAME
PASSWORD COMMENTS NOTES

MEAL (MAIN) PLANNER - GENERAL
DAY: TIME: DATE: ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ DAY: TIME: DATE: ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ DAY: TIME: DATE: ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ DAY: TIME: DATE: ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ DAY: TIME: DATE: ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ DAY: TIME: DATE: ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ DAY: TIME: DATE: _______________________________________________________________________________________________________________________________________________________________________________________________________________________________________

DAILY MEAL PLANNER - GENERAL
DATE:_______________________ DAY:_______________________________
BREAKFAST TIME: ___________ ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ LUNCH TIME: ___________ ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ DINNER TIME: ___________ ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ DRINKS / SNACKS TIME: ___________ ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ ENTERTAINMENT TIME: ___________ ____________________________________________________________ ____________________________________________________________ ____________________________________________________________
TABLE SEATING PLAN - GENERAL
PLAN GUEST SEATING ARRANGEMENTS ON TABLE OF CHOICE BELOW

MOVIE LIST- GENERAL
DATE MOVIES VIEWED MOVIES TO WATCH LIST

GIFT REFERENCE GENERAL MONTH ZODIAC SIGN BIRTHSTONE FLOWER January Capricorn * Dec 22 – Jan 20 Garnet Carnation/Snowdrop
February Aquarius *Jan 21 – Feb 18 Amethyst Violet/Primrose March Pisces * Feb 19 – Mar 20 Aquamarine Jonquil/Daffodil April Aries *Mar 21 – Apr 20 Diamond Sweet Pea/Daisy
May Taurus * Apr 21 – May 21 Emerald Lily/Hawthorne June Gemini * May 22 – Jun 21 Pearl Rose/Honeysuckle July Cancer * Jun 22 – Jul 22 Ruby Larkspur/Water Lily
August Leo *Jul 23 – Aug 23 Peridot Poppy/Gladiolus September Virgo * Aug 24 – Sep 22 Sapphire Aster/Morning Glory October Libra *Sep 23 – Oct 23 Opal Calendula/Cosmos
November Scorpio * Oct 24 – Nov 22 Topaz Chrysanthemum December Sagittarius *Nov 23 – Dec 21 Turquoise Narcissus/Holly ANNIVERSARY TRADITIONAL MODERN First Paper Clocks Second Cotton China Third Leather/Muslin Crystal/Glass Fourth Silk/Fruit/Flowers Electrical Fifth Wood Silverware Sixth Iron Wood Seventh Copper/Wool Desk Set Eighth Bronze Linen/Lace Ninth Pottery/China Leather Tenth Tin/Aluminum Diamond Eleventh Steel Fashion Jewelry Twelfth Linen/Silk Pearls/Gems Thirteenth Lace Fur/Fabrics Fourteenth Ivory Gold Jewelry Fifteenth Crystal Watches Twentieth China Platinum Twenty-Fifth Silver Silver Thirtieth Pearl Diamond Thirty-Fifth Coral/Jade Jade Fortieth Ruby Ruby Forty-Fifth Sapphire Sapphire Fiftieth Gold Gold Fifty-Fifth Emerald Emerald Sixtieth Diamond Diamond

LAUNDRY LABELS SHEET 1 - GENERAL NOTE: SYSTEM OF DOTS INDICATES TEMPERATURE RANGE FOR ALL WASH PROCEDURES.
WASH SYMBOL
CARE INSTRUCTIONS INSTRUCTIONS AS FOLLOWS…..
Machine Wash, Normal Garment to be laundered through the use of hottest available water, detergent or
soap, agitation, and a machine designed for this purpose.
Machine Wash, Cold Initial water temperature should not exceed 30C or 65 to 85F.
Machine Wash, Warm Initial water temperature should not exceed 40C or 105F.
Machine Wash, Hot Initial water temperature should not exceed 50C or 120F.
Machine Wash, Hot Initial water temperature should not exceed 60C or 140F.
Machine Wash, Hot Initial water temperature should not exceed 70C or 160F.
Machine Wash, Hot Initial water temperature should not exceed 95C or 200F.
Machine Wash, Permanent Press
Garment can be machine laundered only on the setting designed to preserve Permanent Press with cool down or cold rinse prior to reduced spin.
Machine Wash, Gentle or Delicate
Garment can be machine laundered only on the setting designed for gentle agitation and/or reduced time for delicate items.
Hand Wash Garment can be laundered through the use of water, detergent or soap and gentle hand manipulation.
Do Not Wash Garment can not be safely laundered by any process. Seek Dry Clean instructions.
NOTE: All (98+%) washable textiles are safe in some type of bleach. IF BLEACH IS NOT MENTIONED OR REPRESENTED BY A SYMBOL, ANY BLEACH MAY BE USED.
BLEACH SYMBOL
CARE INSTRUCTIONS INSTRUCTIONS AS FOLLOWS…..
Bleach When Needed Any commercially available bleach product can be used in the laundering process.
Non-Chlorine Bleach When Needed
Only a non-chlorine, color-safe bleach may be used in the laundering process. Chlorine bleach can not be used.
Do Not Bleach No bleach product can be used. The garment is not colorfast or structurally able to withstand any bleach.

LAUNDRY LABELS SHEET 2 - GENERAL NOTE: SYSTEM OF DOTS INDICATING TEMPERATURE RANGE IS THE SAME FOR ALL DRY PROCEDURES.
DRY SYMBOL CARE INSTRUCTIONS INSTRUCTIONS AS FOLLOWS…..
Tumble Dry, Normal A machine dryer can be regularly used at the hottest available temperature
setting.
Tumble Dry, Normal, Low Heat
A machine dryer can be regularly used at a maximum of Low Heat setting.
Tumble Dry, Normal, Medium Heat
A machine dryer can be regularly used at a maximum of Medium Heat setting.
Tumble Dry, Normal, High Heat
A machine dryer can be regularly used at a High Heat setting.
Tumble Dry, Normal, No Heat A machine dryer can be regularly used only at No Heat or Air Only setting.
Tumble Dry, Permanent Press
A machine dryer can be regularly used only at the Permanent Press setting.
Tumble Dry, Gentle A machine dryer can be regularly used only at the Gentle setting.
Do Not Tumble Dry A machine dryer can not be used. Seek alternate drying method symbol.
Do Not Dry A machine dryer can not be used. Seek alternate drying method symbol.
Line Dry Hang damp garment from line or bar, in or out doors.
Drip Dry Hang dripping wet garment from line or bar, in or out doors, without hand
shaping or smoothing.
Dry Flat Lay out horizontally for drying.
Dry In Shade Usually added to Line or Drip Dry. Dry away from direct sunlight.
WIRING SYMBOL
CARE INSTRUCTIONS INSTRUCTIONS AS FOLLOWS…..
Do Not Wring Do not wring as wiring will cause damage to item.

LAUNDRY LABELS SHEET 3 - GENERAL NOTE: IF IRONING IS NOT A NECESSARY, REGULAR CARE PROCEDURE IT NEED NOT BE MENTIONED. NOTE: SYSTEM OF DOTS INDICATING TEMPERATURE RANGE IS THE SAME FOR ALL IRONING PROCEDURES.
IRON SYMBOL CARE INSTRUCTIONS INSTRUCTIONS AS FOLLOWS…..
Iron, Any Temperature, Steam or Dry
Regular ironing may be needed and can be performed at any available temperature with or without steam is acceptable.
Iron, Low Regular ironing, steam or dry, can be performed at Low setting (110C, 230F)
only.
Iron, Medium Regular ironing, steam or dry, can be performed at Medium setting (150C,
300F).
Iron, High Regular ironing, steam or dry, can be performed at High setting (200C,
290F).
Do Not Steam Steam ironing will harm garment, but regular dry ironing at indicated
temperature setting is acceptable.
Do Not Iron Item can not be smoothed or finished with an iron.
DRY CLEAN SYMBOL
CARE INSTRUCTIONS INSTRUCTIONS AS FOLLOWS…..
Dry clean Dry Clean, any solvent, any cycle any moisture, any heat.
Dry clean, Any Solvent Dry Clean, any solvent. Usually used with other restrictions on proper dry
cleaning procedure.
Dry clean, Petroleum Solvent Only
Dry Clean using only petroleum solvent. Usually used with other restrictions.
Dry clean, Any Solvent Except Trichloroethylene
Any dry cleaning solvent other than trichloroethylene can be safely used.
Dry clean, Short Cycle Can be used with A, P, or F solvent restriction.
Dry clean, Reduced Moisture Can be used with A, P, or F solvent restriction.
Dry clean, Low Heat Can be used with A, P, or F solvent restriction.
Dry clean, No Steam Can be used with A, P, or F solvent restriction.
Do Not Dry clean Garment can not be commercially dry cleaned.

DAILY FOOD GUIDE - GENERAL RECOMMENDED (REFERENCED CANADA’S FOOD GUIDE) NUMBER OF FOOD GUIDE SERVINGS PER DAY:
SERVINGS FOR CHILDREN TEENS ADULTS Sex Girls & Boys Females Males Females Males Females Males
Age in years 2-3 4-8 9-13 14-18 19-50 51+ Vegetables and Fruit 4 5 6 7 8 7-8 8-10 7 7
Grain Products 3 4 6 6 7 6-7 8 6 7 Milk and Alternatives 2 2 3-4 3-4 3-4 2 2 3 3 Meat and Alternatives 1 1 1-2 2 3 2 3 2 3
Vegetables and Fruit Daily Servings;
→ Fresh, frozen or canned vegetables 125ml / ½ cup → Leafy vegetables cooked: 125ml / ½ cup Raw ; 250ml / 1 cup → Fresh, frozen or canned fruit 1 fruit or 125 ml / ½ cup → 100% juice 125 ml / ½ cup
Grain Products Daily Servings; → Bread 1 slice 35g → ½ Bagel 45g → Flat breads ½ Pita or ½ tortilla / 35g → Cooked rice, bulgur or quinoa 125 ml / 1/2 cup → Cereal Cold: 30g Hot: 175 ml / 3/4 cup → Cooked pasta, couscous 125 ml / ½ cup
Milk and Alternatives Daily Servings;
→ Milk or powdered milk (reconstituted) 250 ml / 1 cup → Canned milk, evaporated 125 ml / ½ cup → Fortified soy beverage 250 ml / 1 cup → Yogurt 175 g / ¾ cup → Kefir 175 g / ¾ cup → Cheese 50 g / 1.5 oz
Meat and Alternatives Daily Servings;
→ Cooked fish, shellfish, poultry, lean meat 75g / 2.5 oz / 125ml / ½ cup → Cooked legumes 175ml / ¾ cup → Tofu 150 g or 175 ml / ¾ cup → Eggs 2 → Peanut or nut butters 30ml / 2 tbsp → Shelled nuts and seeds 60 ml / ¼ cup

RECIPE INDEX - GENERAL
PAGE# RECIPE PAGE# RECIPE

RECIPE CARDS - GENERAL
PAGE#_____Title: __________________________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________
PAGE#_____Title: __________________________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________

RECIPE CARDS - GENERAL
Title: _____________________ PAGE#____ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________
Title: _____________________ PAGE#_________________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________
Title: _____________________ PAGE#_________________________ ____________________ ____________________ ____________________ ____________________ ____________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________
Title: _____________________ PAGE#_________________________ ____________________ ____________________ ____________________ ____________________ ____________________ ___________________________________________ ___________________________________________ ___________________________________________ ___________________________________________ ___________________________________________ ___________________________________________ ___________________________________________ ___________________________________________ ___________________________________________ ___________________________________________
RECIPE SHEET 3 - GENERAL
Title: __________________________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ ____________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________

STATUTORY HOLIDAY PLANS - GENERAL
STATUTORY HOLIDAY:________________________________ DATE/DAY:_____________________
CARD/PARTY INVITATION LIST GIFT LIST NAME CARD / INVITATION NAME GIFT
PARTY BUDGET: $__________________________________ PARTY INVITATIONS:________________________________ PARTY THEME:_______________________________________________________________________________________ ___________________________________________________________________________________________________ PARTY SUPPLIES:____________________________________________________________________________________ ___________________________________________________________________________________________________
RESERVATIONS / PRIVATE DINNER PLANS OCCASION NAME/NUMBER OF GUESTS DATE TIME

PET RECORD CHART - GENERAL PET’S NAME:_____________________________________________________________________________________________________________ BREED:_____________________________________________________ SEX: MALE FEMALE COLOUR:____________________________________________________ I.D. NUMBER:___________________ DATE OF BIRTH:______________________________________________ PLACE OF BIRTH:_____________________________ OWNER’S NAME:______________________________________________ OWNER’S ADDRESS:__________________________ VETERINARY CLINIC:______________________________________________________________________________________________________ VETERINARY ADDRESS:____________________________________________________________________________________________________ VETERINARY PHONE NUMBER:______________________________________________________________________________________________
VACCINATION DATE AGE DATE AGE DATE AGE DATE AGE DATE AGE Distemper-Hepatitis-CAV2 Parainfluenza Leptospirosis Parvovirus Coronavirus Bordetella Lyme Disease Giardia Rabies
HEALTH RECORD APPOINTMENTS DATE INCIDENT DATE REASON
PET DEDICATION/ in memory of……. - GENERAL
DATE:______________________________
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
PAGE #_________________________

PET STORIES AND PICTURES - GENERAL
DATE STORY DATE STORY

PET MEMORIES AND PICTURES - GENERAL
MEMORIES_______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

CHRISTMAS HOLIDAY PLAN - GENERAL ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ ___________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ ___________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ ___________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

CHRISTMAS COSTS / BUDGET - GENERAL
√ DESCRIPTION COST √ DESCRIPTION COST
SECTION ONE Christmas tree ----------------$________ Tree decorations---------------$________ Outdoor decorations-----------$________ Inside decorations-------------$________ Christmas flowers-------------$________ TOTAL---------------------------$________
SECTION TWO Smoke detectors------------------------$________Fire extinguishers-----------------------$________Carbon monoxide detector--------------$________Flashlights-------------------------------$________Batteries--------------------------------$________ TOTAL------------------------------------$________
SECTION THREE Christmas dinner ------------- $________ Extra groceries----------------$________ Baking goods-------------------$________ Holiday treats------------------$________ Ginger Bread House------------$________ TOTAL---------------------------$________
SECTION FOUR Presents--------------------------------$________ Wrapping paper-------------------------$________ Bows, ribbon, tags----------------------$________ Boxes, gift bags-------------------------$________ Crafts, jars, tins-------------------------$________TOTAL------------------------------------$________
SECTION FIVE Alcohol beverages------------- $________ Mix for beverages--------------$________ Entertainment snacks----------$________ TOTAL---------------------------$________
SECTION SIX Shipping paper & tape------------------ $________ Cost of freight to ship parcels----------$________ Christmas cards & stamps--------------$________TOTAL------------------------------------$________
SECTION SEVEN Christmas parties--------------$________ Entertainment, movies---------$________ New Years Eve Party-----------$________ TOTAL---------------------------$________
SECTION EIGHT Babysitters----------------------------- $________ Donations-------------------------------$________ Party clothes----------------------------$________TOTAL------------------------------------$________

CHRISTMAS CARD LIST - GENERAL Name ______________________________ Address ______________________________ City / Province / State ______________________________ Postal Code / Zip Code ______________________________
Name ______________________________ Address ______________________________ City / Province / State ______________________________ Postal Code / Zip Code ______________________________
Name ______________________________ Address ______________________________ City / Province / State ______________________________ Postal Code / Zip Code ______________________________
Name ______________________________ Address ______________________________ City / Province / State ______________________________ Postal Code / Zip Code ______________________________
Name ______________________________ Address ______________________________ City / Province / State ______________________________ Postal Code / Zip Code ______________________________
Name ______________________________ Address ______________________________ City / Province / State ______________________________ Postal Code / Zip Code ______________________________
Name ______________________________ Address ______________________________ City / Province / State ______________________________ Postal Code / Zip Code ______________________________
Name ______________________________ Address ______________________________ City / Province / State ______________________________ Postal Code / Zip Code ______________________________
Name ______________________________ Address ______________________________ City / Province / State ______________________________ Postal Code / Zip Code ______________________________
Name ______________________________ Address ______________________________ City / Province / State ______________________________ Postal Code / Zip Code ______________________________
Name ______________________________ Address ______________________________ City / Province / State ______________________________ Postal Code / Zip Code ______________________________
Name ______________________________ Address ______________________________ City / Province / State ______________________________ Postal Code / Zip Code ______________________________
Name ______________________________ Address ______________________________ City / Province / State ______________________________ Postal Code / Zip Code ______________________________
Name ______________________________ Address ______________________________ City / Province / State ______________________________ Postal Code / Zip Code ______________________________
Name ______________________________ Address ______________________________ City / Province / State ______________________________ Postal Code / Zip Code ______________________________

CHRISTMAS GIFT SHOPPING LIST - GENERAL
NAME GIFT COST PURCHASE AT…

HEALTH SECTION
TABLE OF CONTENTS
PAGE # TOPIC / DESCRIPTION / TITLE

MEDICAL ALERT CONDITIONS / ALLERGIES MEDICAL ALERT CONITIONS
ALLERGIES
EMERGENCY PHONE NUMBERS
IN CASE OF AN EMERGENCY CALL PHONE
NUMBER RELATION
TO ME NAME
NAME
FAMILY DOCTOR
HOSPITAL
POLICE
FIRE
HEALTH CARE PROVIDER
PHARMACY
OTHER
OTHER
IMPORTANT NUMBERS
HEALTH CARE NUMBER
OTHER INSURANCE NUMBER
OTHER NUMBER
MEDICAL HISTORIES
MY MEDICAL HISTORY FAMILY MEDICAL HISTORY

MEDICATIONS - HEALTH
DATE MEDICATION HOW MANY?
AMOUNT? DIRECTIONS / INSTRUCTIONS
COMPLETED?

DAILY RECORD - HEALTH Date: From________________________ To_____________________________
DAY LIST
SLEEP DETAILS
NOTE TODAY’S FEELINGS
LIST TODAY’S
SYMPTOMS
LIST TODAY’S MEDICATION
RECORD APPOINTMENTS
AND NOTES
SUN DATE
MON DATE
TUE DATE
WED DATE
THU DATE
FRI DATE
SAT
JOURNAL NOTES:

DAILY RECORD SHEET 2 - HEALTH DATE: FROM:___________________________________________ TO:_________________________________________
DAY LIST
TODAY’S FOODS
LIST TODAY’S
EXERCISES
RECORD CALORIEIN-TAKE
RECORD CALORIES
BURNT OFF
RECORD TODAY’S WEIGHT
SUN
MON
TUE
WED
THU
FRI
SAT
WEEKLY TOTALS

BLOOD PRESSURE RECORD - HEALTH
DATE BLOOD PRESSURE
DATE BLOOD PRESSURE
DATE BLOOD PRESSURE
DATE BLOOD PRESSURE

MEDICAL TESTS COMPLETED - RECORD - HEALTH
DATE TEST COMPLETED RESULTS

MEDICAL HEALTH CONTACTS - HEALTH
Name:____________________________________________ Phone: ____________________________________
Reason for Contact:__________________________________________________________________________________
Fax: _____________________________________________ e-Mail: ___________________________________
Mail: _____________________________________________________________________________________________
Mail :______________________________________________________________________________________________
Notes:_____________________________________________________________________________________________
Name:____________________________________________ Phone: ____________________________________
Reason for Contact:__________________________________________________________________________________
Fax: _____________________________________________ e-Mail: ___________________________________
Mail: _____________________________________________________________________________________________
Mail :______________________________________________________________________________________________
Notes:_____________________________________________________________________________________________
Name:____________________________________________ Phone: ____________________________________
Reason for Contact:__________________________________________________________________________________
Fax: _____________________________________________ e-Mail: ___________________________________
Mail: _____________________________________________________________________________________________
Mail :______________________________________________________________________________________________
Notes:_____________________________________________________________________________________________

FOOD DIARY - HEALTH Keep a food diary to monitor eating habits that may be related to other issues. Review to observe any patterns.
DATE FOOD OR DRINK
AMOUNT TIME PLACE ALONE OR WITH SOMEONE
ACTIVITY FEELINGS

WEIGHT CHARTS – HEALTH
Weight Chart for Women Weight Chart for Men
Height Small Frame Medium Frame Large Frame
4'10" 102-111 109-121 118-131
4'11" 103-113 111-123 120-134
5'0" 104-115 113-126 122-137
5'1" 106-118 115-129 125-140
5'2" 108-121 118-132 128-143
5'3" 111-124 121-135 131-147
5'4" 114-127 124-138 134-151
5'5" 117-130 127-141 137-155
5'6" 120-133 130-144 140-159
5'7" 123-136 133-147 143-163
5'8" 126-139 136-150 146-167
5'9" 129-142 139-153 149-170
5'10" 132-145 142-156 152-173
5'11" 135-148 145-159 155-176
6'0" 138-151 148-162 158-179
Weight in pounds, based on ages 25-59 with the lowest mortality rate (indoor clothing weighing 3 pounds and shoes with 1" heels)
Weight in pounds, based on ages 25-59 with the lowest mortality rate(indoor clothing weighing 5 pounds and shoes with 1" heels)
DATE NAME AGE WEIGHT HEIGHT COMMENTS
Height Small Frame Medium Frame Large Frame
5'2" 128-134 131-141 138-150
5'3" 130-136 133-143 140-153
5'4" 132-138 135-145 142-156
5'5" 134-140 137-148 144-160
5'6" 136-142 139-151 146-164
5'7" 138-145 142-154 149-168
5'8" 140-148 145-157 152-172
5'9" 142-151 148-160 155-176
5'10" 144-154 151-163 158-180
5'11" 146-157 154-166 161-184
6'0" 149-160 157-170 164-188
6'1" 152-164 160-174 168-192
6'2" 155-168 164-178 172-197
6'3" 158-172 167-182 176-202
6'4" 162-176 171-187 181-207

METRIC WEIGHTS & MEASURES - HEALTH
Desirable Weights (Kilograms) Men Women
Height(cms) Small Frame
Medium Frame
Large Frame
Height(cms) Small Frame Medium Frame
Large Frame
157.5 50.7-54.4 53.5-57.1 57.1-63.9 147.5 41.7-44.4 43.5-48.5 47.1-53.9 160 52.1-55.8 54.8-60.3 58.5-65.3 150 42.6-45.8 44.4-49.9 48.0-55.3 162.5 53.5-57.1 56.2-61.6 59.8-67.1 152.5 43.5-47.1 45.8-51.2 49.4-56.7 165 54.8-58.5 57.8-63.0 61.2-68.9 155 44.9-48.5 47.1-52.6 50.8-58.0 167.5 56.2-60.3 59.0-64.8 62.6-70.7 157.5 46.2-49.9 48.5-53.9 52.1-59.4 170 58.0-62.1 60.7-66.6 64.4-73.0 160 47.6-51.2 49.9-55.3 53.5-60.7 172.5 59.8-63.9 62.6-68.9 66.6-75.2 162.5 49.0-52.6 51.2-57.1 54.9-62.6 175 61.6-65.7 64.4-70.7 68.4-77.1 165 50.3-53.9 52.6-58.9 56.7-64.4 178 63.4-68.0 66.6-72.5 70.3-78.9 167.5 51.6-55.8 54.4-61.2 58.5-66.2 180 65.3-69.8 68.0-74.8 72.1-81.1 170 53.5-57.6 56.2-63.0 60.3-68.0 183 67.1-71.6 69.8-77.1 75.3-83.4 172.5 54.8-59.4 58.0-64.8 62.1-69.8 185.5 68.9-73.4 71.6-79.3 76.1-85.7 175 57.1-61.2 59.8-66.6 63.9-71.6 188 70.7-75.7 73.4-81.6 78.4-87.9 178 58.9-63.5 61.6-68.4 65.7-73.9 190.5 72.5-77.5 75.7-83.9 80.7-90.2 180 60.7-65.3 63.5-70.3 67.5-76.2 193 74.3-79.3 78.0-86.1 82.5-92.5 183 62.6-67.1 65.3-72.1 69.4-78.4
DATE NAME HEIGHT WEIGHT DOWN UP COMMENTS

CALORIES IN ALCOHOLIC DRINKS - HEALTH Beer Ready Reckoner
Regular : 5% alcohol Calories Alcohol (g) Carbohydrate
Glass : 7 fl oz 80 8.5 4
Glass/Bottle/Can : 12 fl oz 140 14 10
Bottle/Can : 16 fl oz 185 19 11
Bottle : 22 fl oz 260 26 20
Bottle : 32 fl oz 370 37 28
Bottle : 40 fl oz 470 47 35
Light : 4.2% alcohol
Glass : 7 fl oz 65 7 4
Glass/Bottle/Can : 12 fl oz 110 12 6
Bottle/Can : 16 fl oz 145 16 8
Bottle : 22 fl oz 200 22 11
Low Alcohol : 2.3% alcohol
Glass : 7 fl oz 45 4 3
Glass/Bottle/Can : 12 fl oz 75 7 6
Spirits, Brandy, Whisky Includes: Brandy, Rum, Whisky, Gin, Bourbon, Scotch, Tequila, Vodka, Bacardi, Haig, Mainstay, Southern Comfort
Average 80 proof (40% alcohol) Calories Alcohol (g) Carbohydrate
1/2 shot : 3/4 fl oz 33 5 0
1 shot : 1 1/2 fl oz 65 9.5 0
Double shot : 3 fl oz 130 19 0
1/2 Bottle, 375ml 810 120 0
Coolers & Premixed Cocktails
Calories Alcohol (g) Carbohydrate
Barcardi Silver, 4.9 %, 12 fl. oz 235 14 35
Bartles & James Malt Based Coolers, 3.9 %, 12 fl. oz, av.all flavors 225 11 41
Cruzan Island Cocktails, 5%, 12 fl. oz, av. all flavors 270 14 43
Jack Daniels Country Cocktails, 5.9%, 12 fl. oz, av all flavours 170 10 25
Seagram’s Coolers, 3.2%, 12 fl. oz, av. all flavours 230 12 36
Smirnoff Ice, 5%, 330 ml 225 13 33
The Club, 4 fl. oz, av. all flavours 240 11 38
Table Wine Ready Reckoner
Average All Varieties (11.5% Alcohol) Calories Alcohol (g) Carbohydrate
4 fl. oz (1/2 large wine glass) 85 11 2
6 fl. oz serve (3/4 large wine glass) 125 16 3
1/2 Carafe/Bottle, 375ml 265 34 6
1 Bottle, 750ml Note: Wines contain nil fat.
530 68 13

CHILD’S HEALTH RECORD - HEALTH FOR COMPLETE RECORDS & ROUTINE IMMUNIZATION SCHEDULES, please refer to Canadian Immunization Guide, Seventh Edition, 2006 (Chart below is for record keeping only)
VACCINATION DATE DATE DATE DATE DATE Diphtheria, tetanus, acellular pertussis and inactivated polio virus vaccine (DTaP-IPV): DTaP-IPV(± Hib)
Haemophilus influenzae type b conjugate vaccine (Hib)
Measles, mumps and rubella vaccine (MMR)
Varicella vaccine (Var)
Hepatitis B vaccine (HB:
Pneumococcal conjugate vaccine - 7-valent (Pneu-C-7)
Meningococcal C conjugate vaccine (Men-C)
Influenza vaccine (Inf)
Inactivated polio virus (IPV)
CHILDHOOD ILLNESSES AND ACCIDENTS ILLNESS/ACCIDENT MEDICATION/EXRAYS DATE ILLNESS/ACCIDENT MEDICATION/EXRAYS DATE
HOSPITAL VISITS: (NOTES) ______________________________________________________________ __________________________________________________________________________________________________________________________________________________________________________

FITNESS SECTION
TABLE OF CONTENTS
PAGE # TOPIC / DESCRIPTION / TITLE

PHYSICAL , PHYSIO, BREATHING & RELAXATION EXERCISES - SCHEDULE
DAY TIME PHYSICAL /
PHYSIO BREATHING RELAXATION
SUN
DATE:_______
MORNING:__________ AFTERNOON:________ EVENING:___________
MON
DATE:_______
MORNING:__________ AFTERNOON:________ EVENING:___________
TUE
DATE:_______
MORNING:__________ AFTERNOON:________ EVENING:___________
WED
DATE:_______
MORNING:__________ AFTERNOON:________ EVENING:___________
THU
DATE:_______
MORNING:__________ AFTERNOON:________ EVENING:___________
FRI
DATE:_______
MORNING:__________ AFTERNOON:________ EVENING:___________
SAT
DATE:_______
MORNING:__________ AFTERNOON:________ EVENING:___________

DAILY FITNESS
DATE:________________________________ DAY:_________________________________
DECRIBE YOUR ENERGY LEVEL BEFORE YOUR WORKOUT? (Scale 1-10 1 is low)
DESCRIBE YOUR ENERGY LEVEL AFTER YOUR WORKOUT? (Scale 1-10 1 = low)
GENERAL EXERCISE
Duration / Time
Energy used up / burned
STRETCHEXERCISE
Duration / Time
Energy used up / burned
TOTALS TOTALS
CARDIO EXERCISE Duration /
Time Energy used up /
burned STRENGTH /
TRAINING Duration /
Time Energy used up /
burned
TOTALS TOTALS
RELAXATION EXERCISE
Duration / Time
Energy used up / burned
BREATHING EXERCISES
Duration / Time
Energy used up / burned
TOTALS TOTALS ENERGY CONSUMED: _________ MINUS (-) ENERGY USED: __________ = TODAY’S TOTAL _____________

DAILY FITNESS PART 2 - FITNESS
DAY:_______________________________ DATE:________________________________ PLAN YOUR GOALS FOR TODAY HOW DID YOU SLEEP?
HOW DO YOU FEEL TODAY?
MEDICATIONS VITAMINS / SUPPLEMENTS GLASSES OF WATER 1. 2. 3. 4. 5. 6. 7. 8. 9.
List the foods you ate today. Record the energy count in foods (calories, carbs, fibers, etc.) BREAKFAST ENERGY
TOTAL: [ _______ ]
LUNCH ENERGY
TOTAL: [ _______ ]
DINNER ENERGY
TOTAL: [ _______ ]
SNACKS ENERGY
TOTAL: [ _______ ]
NOTES ON HEALTH NOTES ON FITNESS
DAILY TOTALS PROGRESS - FITNESS
MONTH __________
ENERGY (CALORIES) CONSUMED
[ - MINUS ] ENERGY (CALORIES)
USED (BURNED) UP
[ = ] ENERGY (CALORIES) PER DAY
WEIGHT
-/+
INCHES
-/+ 1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
TOTALS

MONTHLY TOTALS PROGRESS - FITNESS
MONTH START
WEIGHT
ENERGY USED UP (CALORIES
BURNED)
END WEIGHT
WEIGHT -/+
INCHES -/+
1 2 3 4 5 6 7 8 9 10 11 12 TOTALS
NOTES / GOALS: ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

ANNUAL PERSONAL PROGRESS - FITNESS
MEASUREMENT BEFORE JAN FEB MAR APR MAY JUNWeight Bust Arms Waist Hips Thighs Calves B.M.I. (Body Mass Index) Cholesterol Resting Heart Rate Personal Fat Scale/Budget
MEASUREMENT JUL AUG SEP OCT NOV DEC AFTER
Weight Bust Arms Waist Hips Thighs Calves B.M.I. (Body Mass Index) Cholesterol Resting Heart Rate Personal Fat Scale/Budget

FOOD ENERGY COUNT - FITNESS
FOOD ITEM CALORIES FAT (GRAMS) % FAT SODIUM (mgs.)

FITNESS CONTACTS - FITNESS
Name:____________________________________________ Phone: ____________________________________
Reason for Contact:__________________________________________________________________________________
Fax: _____________________________________________ e-Mail: ___________________________________
Mail: _____________________________________________________________________________________________
Mail :______________________________________________________________________________________________
Notes:_____________________________________________________________________________________________
Name:____________________________________________ Phone: ____________________________________
Reason for Contact:__________________________________________________________________________________
Fax: _____________________________________________ e-Mail: ___________________________________
Mail: _____________________________________________________________________________________________
Mail :______________________________________________________________________________________________
Notes:_____________________________________________________________________________________________
Name:____________________________________________ Phone: ____________________________________
Reason for Contact:__________________________________________________________________________________
Fax: _____________________________________________ e-Mail: ___________________________________
Mail: _____________________________________________________________________________________________
Mail :______________________________________________________________________________________________
Notes:_____________________________________________________________________________________________

BODY MASS INDEX CHART- FITNESS The table below has already done the math and metric conversions. To use the table, find the appropriate height in the left-hand column. Move across the row to the given weight. The number at the top of the column is the BMI for that height and weight.
BMI (kg/m2)
19 20 21 22 23 24 25 26 27 28 29 30 35 40
Height (in.)
Weight (lb.)
58 91 96 100 105 110 115 119 124 129 134 138 143 167 191
59 94 99 104 109 114 119 124 128 133 138 143 148 173 198
60 97 102 107 112 118 123 128 133 138 143 148 153 179 204
61 100 106 111 116 122 127 132 137 143 148 153 158 185 211
62 104 109 115 120 126 131 136 142 147 153 158 164 191 218
63 107 113 118 124 130 135 141 146 152 158 163 169 197 225
64 110 116 122 128 134 140 145 151 157 163 169 174 204 232
65 114 120 126 132 138 144 150 156 162 168 174 180 210 240
66 118 124 130 136 142 148 155 161 167 173 179 186 216 247
67 121 127 134 140 146 153 159 166 172 178 185 191 223 255
68 125 131 138 144 151 158 164 171 177 184 190 197 230 262
69 128 135 142 149 155 162 169 176 182 189 196 203 236 270
70 132 139 146 153 160 167 174 181 188 195 202 207 243 278
71 136 143 150 157 165 172 179 186 193 200 208 215 250 286
72 140 147 154 162 169 177 184 191 199 206 213 221 258 294
73 144 151 159 166 174 182 189 197 204 212 219 227 265 302
74 148 155 163 171 179 186 194 202 210 218 225 233 272 311
75 152 160 168 176 184 192 200 208 216 224 232 240 279 319
76 156 164 172 180 189 197 205 213 221 230 238 246 287 328
Body weight in pounds according to height and body mass index.
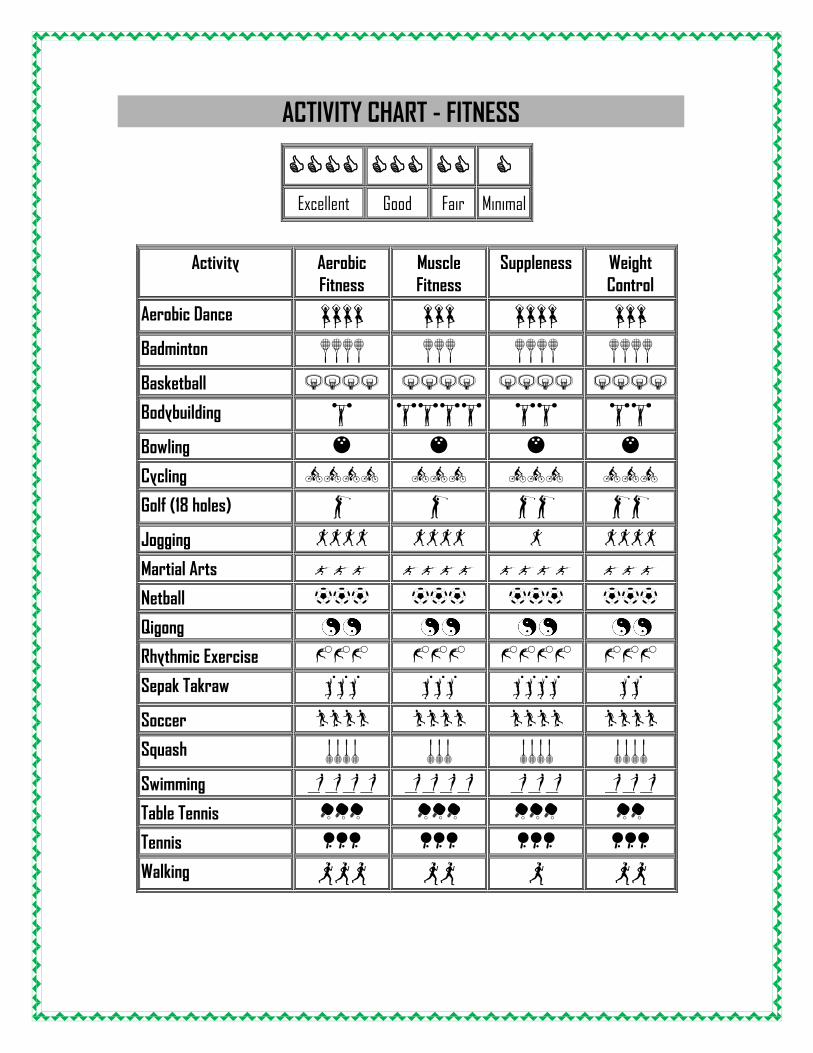
ACTIVITY CHART - FITNESS
Activity Aerobic Fitness
Muscle Fitness
Suppleness Weight Control
Aerobic Dance Badminton Basketball
Bodybuilding Bowling
Cycling
Golf (18 holes) Jogging
Martial Arts
Netball
Qigong Rhythmic Exercise
Sepak Takraw Soccer
Squash Swimming Table Tennis
Tennis
Walking
Excellent Good Fair Minimal

TIMED CALORIES BURNT - FITNESS
Activity 15min 30min 45min 60min Activity 15min 30min 45min 60min
Aerobics (High-Impact) 165 320 500 660 Martial Arts 180 328 485 645
Aerobics (Low-Impact) 135 270 400 540 Racquetball 110 225 340 450
Basketball (Game-playing) 140 280 430 550 Rock Climbing (Ascending) 192 388 540 722
Baseball/Softball 92 159 240 317 Rowing Machine 150 350 475 650
Circuit Training(with weights)
185 320 455 580 Running (10min mile pace) 180 360 540 730
Cycling (6mph) 75 130 190 240 Running (8min mile pace) 225 450 670 925
Cycling (12mph) 100 200 300 410 Sex (Ave. Pace) 24 49 75 97
Cycling (15mph) 150 320 480 600 Skate Boarding 85 165 237 317
Cross-Country Skiing 145 300 450 600 Ski Machine 125 280 425 575
Dancing (Swing) 110 205 293 390 Snow Shoeing (General) 140 290 405 535
Dancing (Line) 65 138 195 258 Soccer 140 270 415 555
Downhill Skiing 100 200 300 400 Surfing 48 97 146 195
Elliptical Trainer 235 548 690 905 Stair Climber 155 310 460 618
Football 140 280 390 530 Swimming (freestyle) 130 250 380 510
Golf (Walking) 45 115 170 230 Tennis (singles) 110 225 350 450
Golf (Carrying Clubs) 80 170 260 340 Ultimate Frisbee 55 105 174 222
Handball 165 325 490 655 Volleyball 48 90 144 190
Hiking (Avg Incline) 105 190 280 360 Walking (flat, 17min mile pace)
65 130 200 275
Hockey 142 290 420 555 Walking (hills, 17min mile pace)
90 180 260 380
Horseback Riding (General)
65 130 195 260 Water Aerobics 70 140 210 280
Ice Skating (General) 110 225 340 445 Water Skiing 95 205 312 415
In-line Skating 150 300 450 600 Weeding a Garden 90 160 230 320
Jump Rope 170 290 460 620 Weight Training 130 270 385 510
Other: Wrestling (5 min match) 115 180 290 387
Other: Yoga 70 120 185 240

CHILD GROWTH CHART- FITNESS
NAME DATE AGE WEIGHT HEIGHT COMMENTS

WELLNESS SECTION
TABLE OF CONTENTS
PAGE # TOPIC / DESCRIPTION / TITLE

GRATITUDE EXPERIENCE – WELLNESS EXERCISE Try the GRATITUDE EXPERIENCE. This is a wellness exercise that may enlighten your daily life and attitude. The exercise runs for an eight week period. The idea of the exercise is to become more grateful for the goodness in your daily life. Use the following sheet to write down at least 5 good things that you are grateful for in your life each day. The situation can be anything positive, big or little, an event or a thought. Some examples might be; 1. I got a raise today! 2. I had my first summer soft ice cream cone today. 3. The snow flakes where huge and beautiful today. 4. My daughter won the dance contest. 5. I met a new friend today. Discover the gratitude experience! The following page present an opportunity for you to experience the changes that gratitude can generate in your daily life. As you record all the things you are grateful for having, for experiencing, for seeing and hearing, you can become aware of all the precious people and the priceless moments that exist in your world. Dealing with problems and issues from day to day can lead us into a stagnant life-style that we do not even realize is upon us. While these problems and issues still need to be dealt with, we can try not to become too consumed by their impact. By intentionally focusing on the positive realities each day, we can modify our attitude and thinking to recognize just how much we truly have to be thankful for. It can develop our mental health, boost our exercise levels and possibly experience sleep improvements. But - the true influence of gratitude cannot be described nearly as well as it CAN be experienced. A soothing consciousness – an awareness, can be aroused into your being, your daily life-style and your awakened world.

GRATITUDE EXPERIENCE – WELLNESS EXERCISE In a few words record 5 observations of gratitude daily; WEEK – DATE : Day 1
1. ___________________________________________________________________________________________ 2. ___________________________________________________________________________________________ 3. ___________________________________________________________________________________________ 4. ___________________________________________________________________________________________ 5. ___________________________________________________________________________________________
Day 2 1. ___________________________________________________________________________________________ 2. ___________________________________________________________________________________________ 3. ___________________________________________________________________________________________ 4. ___________________________________________________________________________________________ 5. ___________________________________________________________________________________________
Day 3 1. ___________________________________________________________________________________________ 2. ___________________________________________________________________________________________ 3. ___________________________________________________________________________________________ 4. ___________________________________________________________________________________________ 5. ___________________________________________________________________________________________
Day 4 1. ___________________________________________________________________________________________ 2. ___________________________________________________________________________________________ 3. ___________________________________________________________________________________________ 4. ___________________________________________________________________________________________ 5. ___________________________________________________________________________________________
Day 5 1. ___________________________________________________________________________________________ 2. ___________________________________________________________________________________________ 3. ___________________________________________________________________________________________ 4. ___________________________________________________________________________________________ 5. ___________________________________________________________________________________________
Day 6 1. ___________________________________________________________________________________________ 2. ___________________________________________________________________________________________ 3. ___________________________________________________________________________________________ 4. ___________________________________________________________________________________________ 5. ___________________________________________________________________________________________
Day 7 1. ___________________________________________________________________________________________ 2. ___________________________________________________________________________________________ 3. ___________________________________________________________________________________________ 4. ___________________________________________________________________________________________ 5. ___________________________________________________________________________________________

MY GOALS - WELLNESS
MY FITNESS, HEALTH, FINANCIAL, HABITS (etc.) GOALS, REACH GOALS BY (DATE)

THINGS I WANT TO CHANGE IN MY LIFE - WELLNESS
DATE I WANT TO CHANGE…….

DECISION-MAKING PROS & CONS - WELLNESS
DECISION TO MAKE PROS CONS

BALANCED LIFESTYLE - WELLNESS Use the following chart to develop a plan using the four basic elements for living a fulfilled lifestyle.
(i) MIND – list activities that will challenge you intellectually __________________________________________________________________________________ (ii) BODY – list physical activities __________________________________________________________________________________ (iii) SOUL – list your passions or activities that give you great joy to do __________________________________________________________________________________ (iv) HUMAN INTERACTION – list social groups that have your interests in mind

ACHIEVEMENTS / SUCCESSES & TRIUMPHS - WELLNESS
DATE ACHIEVEMENT
SUCCESS TRIUMPH / AWARD
PLACE ATTENDED
PEOPLE ATTENDED /NOTES

SELF HELP AREAS FOR IMPROVEMENT- WELLNESS
AREA START DATE
END DATE ACTION PLAN
Anger Management Anxiety Assertiveness Behavior Modification Codependency Depression Diet / Weight Loss Eating Habits Fitness & Exercise Forgiveness Friendships/Loneliness Goal Setting Gratitude Habits Happiness Investing Listening Skills Love Mind Control / Power Motivation Nutrition Overcoming Fear Positive Thinking Relaxation Self Esteem Stress Management Time Management

WELLNESS CONTACTS - WELLNESS
Name:____________________________________________ Phone: ____________________________________
Reason for Contact:__________________________________________________________________________________
Fax: _____________________________________________ e-Mail: ___________________________________
Mail: _____________________________________________________________________________________________
Mail :______________________________________________________________________________________________
Notes:_____________________________________________________________________________________________
Name:____________________________________________ Phone: ____________________________________
Reason for Contact:__________________________________________________________________________________
Fax: _____________________________________________ e-Mail: ___________________________________
Mail: _____________________________________________________________________________________________
Mail :______________________________________________________________________________________________
Notes:_____________________________________________________________________________________________
Name:____________________________________________ Phone: ____________________________________
Reason for Contact:__________________________________________________________________________________
Fax: _____________________________________________ e-Mail: ___________________________________
Mail: _____________________________________________________________________________________________
Mail :______________________________________________________________________________________________
Notes:_____________________________________________________________________________________________

DAILY/WEEKLY DIARY - WELLNESS
DATE/DAY:________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
DATE/DAY:____________________________________ ____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
DATE/DAY:____________________________________ ____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
DATE/DAY:____________________________________ ____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
DATE/DAY:____________________________________ ____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
DATE/DAY:____________________________________ ____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
DATE/DAY:____________________________________ ____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

PROBLEM SOLVER / SOLUTION - WELLNESS
PROBLEM DETAILS GOALS TO ACHIEVE SOLUTIONS/CORRECTIVE ACTIONS
RESOLVE DATE/TIME
RESOLVED?YES/NO

FINANCIAL SECTION
TABLE OF CONTENTS
PAGE # TOPIC / DESCRIPTION / TITLE

FINANCES – CHECK LIST
√ DESCRIPTION √ DESCRIPTION
HOUSING Mortgage or rent Phone Electricity Gas Water and sewer Cable Waste removal Maintenance or repairs Supplies Other____________________
TRANSPORTATIONVehicle payment Bus/taxi fare Insurance Licensing Fuel Maintenance Other_______________________ Other_______________________ Other_______________________ Other_______________________
INSURANCE Home Health Life Other____________________
FOODGroceries Dining out Other_______________________ Other_______________________
PETS Food Medical Grooming Toys Other____________________ Other____________________ Other____________________
PERSONAL CAREMedical Hair/nails Clothing Dry cleaning Health club Organization dues or fees Other_______________________
ENTERTAINMENT Video/DVD CDs Movies Concerts Sporting events Live theater Other_____________________ Other_____________________ Other_____________________
LOANSPersonal Line of Credit Credit card Credit card Credit card Other_______________________ Other_______________________ Other_______________________ Other_______________________
TAXES Federal State/Provincial Local Other_____________________
SAVINGS OR INVESTMENTS Retirement account Investment account Other_______________________ Other_______________________
GIFTS AND DONATIONS Charity 1 Charity 2 Charity 3 Other_____________________
LEGALAttorney Alimony Payments on lien or judgment Other_______________________
MONTHLY PAYMENTS - FINANCES ITEM AMOUNT DUE DUE DATE NOTES - √
Mortgage Rent Phone Cell Hydro Gas Oil Cable Internet Life Insurance House Insurance Car Insurance Credit Cards Car Payment Property Taxes Personal Taxes Loan Payment RRSP Investment Totals
MONTHLY APPOINTMENTS / REMINDERS Doctor Appointment Dentist Appointment Car Appointment Bank Appointment Hair Appointment Eye Dr. Appointment Birthdays Anniversaries

RECORD OF BILL PAYMENTS - FINANCES
PAYMENT BALANCE JAN FEB MAR APR MAY JUN
PAYMENT JUL AUG SEP OCT NOV DEC DUE
FINANCIAL GOALS
QUARTERLY, SEMI / ANNUAL EXPENSES - FINANCES
Quarterly Expenses AMOUNT $ $ $ $ $ $ Total Expense(s) $
Semi-Annual Expenses AMOUNT $ $ $ $ $ $ Total Expense(s) $
Annual Expenses AMOUNT $ $ $ $ $ $ Total Expense(s) $
Lease Expenses AMOUNT $ $ $ $ $ $ Total Expense(s) $

BASIC MONTHLY EXPENSES- FINANCIAL List all incomes (including spouse) $ AMOUNT $ Total Income(s) List all expenses (including spouse) $ AMOUNT $ Total Expense(s)

QUARTERLY, SEMI/ANNUAL BASIC EXPENSES- FINANCIAL
Quarterly Expenses $ AMOUNT $ Total Expense(s)
Semi-Annual Expenses $ AMOUNT $ Total Expense(s)
Semi-Annual Expenses $ AMOUNT $ Total Expense(s)
Lease Expenses $ AMOUNT $ Total Expense(s)

CONTACTS - FINANCIAL
Name:__________________________________________ Phone: _________________________________
Reason for Contact:_______________________________________________________________________________
Fax: ___________________________________________ e-Mail: _________________________________
Mail: ____________________________________________________________________________________________
Mail :_____________________________________________________________________________________________
Notes:_____________________________________________________________________________________________
Name:__________________________________________ Phone: _________________________________
Reason for Contact:_______________________________________________________________________________
Fax: ___________________________________________ e-Mail: _________________________________
Mail: ____________________________________________________________________________________________
Mail :_____________________________________________________________________________________________
Notes:_____________________________________________________________________________________________
Name:__________________________________________ Phone: _________________________________
Reason for Contact:_______________________________________________________________________________
Fax: ___________________________________________ e-Mail: _________________________________
Mail: ____________________________________________________________________________________________
Mail :_____________________________________________________________________________________________
Notes:_____________________________________________________________________________________________

MONTHLY BANK RECONCILIATION SHEET 1 - FINANCIAL MONTH:
OPENING BALANCE $
DATE DEPOSIT $AMOUNT
CHEQUE NUMBER
$ AMOUNT
AUTOMATIC PAYMENTS
SERVICE CHARGES
OUTSTANDING CHEQUES DEPOSITS
BALANCE
MONTH:
CLOSING BALANCE $

MONTHLY BANK RECONCILIATION SHEET 2 - FINANCIAL MONTH: START DATE: _______________ END DATE:_____________
OPENING BALANCE: $___________________
ADD DEPOSITS:----------------------------------------------------$___________________ ADD INTEREST: -------------------------------------------------$___________________ _____________: ----------------------------------------------------$___________________ SUBTOTAL: $__________________
(ADD SUBTOTAL DEPOSITS) BALANCE: $_+_______________
BALANCE: $_________________ MINUS WITHDRAWALS / CHEQUES / SERVICE CHARGES TOTAL CHEQUES:----------------------------------------------------$__________________ AUTOMATIC PAYMENTS:--------------------------------------------$__________________ SERVICE CHARGES:-------------------------------------------------$__________________ OTHER DEBITS: --------------------------------------------------$___________________ ___________________:-----------------------------------------------$___________________ SUBTOTAL: $__________________
(SUBTRACT WITHDRAWLS ETC.) BALANCE: $_-______________
BALANCE: $________________ ADD OUTSTANDING DEPOSITS:_____________________________________________________$_+_______________
SUBTOTAL: $______________
SUBTRACT OUTSTANDING CHEQUES:________________________________________________$__-______________
CLOSING BALANCE: $___________________________

HOUSE / MORTGAGE INFORMATION SHEET- FINANCIAL Real Estate Agent: _________________________________ Phone #: ________________________ Mortgage Lender / Bank:___________________________ Account / Loan#:_________________ Attorney: _________________________________________ Phone#: _________________________ Insurance Agent: ___________________________________Phone#:__________________________ Insurance Policy#: _________________________________ Renewal Date: ____________________ Engineer/Inspector: _______________________________ Phone#: _________________________ Environmental Inspector:____________________________ Phone#:__________________________ Title Insurance Company:____________________________ Policy #:_________________________ Home Movers: _____________________________________ Phone#: _________________________ Previous Owners:__________________________________ Address:_________________________ UTILITIES Electric Company:______________________________ Phone#: ___________________________ Account#: _____________________________________ Monthly Fee:________________________ Gas Company:__________________________________ Phone#: ___________________________ Account#: _____________________________________ Monthly Fee:________________________ Fuel Oil Company:______________________________ Phone#: ___________________________ Account#: _____________________________________ Monthly Fee:________________________ Telephone Company:___________________________ Phone#: ___________________________ Account#: _____________________________________ Monthly Fee:________________________ Telephone Long Distance:______________________ Phone#: ___________________________ Account#: _____________________________________ Monthly Fee:________________________ Water Company:_______________________________ Phone#: ___________________________ Account#: _____________________________________ Monthly Fee:________________________ Cable TV Company:_____________________________ Phone#: ___________________________ Account#: _____________________________________ Monthly Fee:________________________ Satellite Company:_____________________________ Phone#: ___________________________ Account#: _____________________________________ Monthly Fee:________________________ Internet Company:_____________________________ Phone#: ___________________________ Account#: _____________________________________ Monthly Fee:________________________ _______ Company:______________________________ Phone#: ___________________________ Account#: _____________________________________ Monthly Fee:________________________ _______ Company:______________________________ Phone#: ___________________________ Account#: _____________________________________ Monthly Fee:________________________
ORGANIZATION SECTION
TABLE OF CONTENTS
PAGE # TOPIC / DESCRIPTION / TITLE

TOP SECRET & CONFIDENTIAL INFORMATION CHECKLIST
Check off the list below to ensure you have all pertinent information stored in a fireproof, safe and secure place. WARNING! DO NOT RECORD ANY TOP SECRET OR CONFIDENTIAL INFORMATION HERE. Verbally tell your ‘trusted person(s)’ the whereabouts of the following;
Set up / inform your ‘trusted person(s)’ and advisors
Create a list of ‘Who to call first’
Create an ‘Emergency contacts’ list
Will and estate documents
Funeral arrangements
Insurance policies
Medical information
Deeds, mortgages, other important property papers
Investment statements
Banking records
Business information
Tax returns
Intellectual property, copyrights, trademarks
Codes, passwords
Keys, combinations
Computer passwords
Special words for special people
Other top secret & confidential information
Other ___________________________________________________________
Other ___________________________________________________________
Other ___________________________________________________________
Other ___________________________________________________________

EVENT PLANNER - ORGANIZATION EVENT #______ EVENT # ______
√ DESCRIPTION √ DESCRIPTION
LOCATION Name__________________________________________ Address________________________________________ _______________________________________________ Phone #________________________________________ Cell #__________________________________________ e-mail_________________________________________
LOCATION Name____________________________________________________ Address__________________________________________________ _________________________________________________________ Phone #_________________________________________________ Cell #____________________________________________________ e-mail ___________________________________________________
PARTY BASICS License / Permit________________________________ Liquor_________________________________________ _______________________________________________ _______________________________________________ _______________________________________________ Mix____________________________________________ _______________________________________________ Bartenders_____________________________________ _______________________________________________ Caterer________________________________________ _______________________________________________ Table Settings___________________________________ _______________________________________________
PARTY BASICS License / Permit__________________________________________ Liquor___________________________________________________ _________________________________________________________ _________________________________________________________ _________________________________________________________ Mix______________________________________________________ _________________________________________________________ Bartenders_______________________________________________ _________________________________________________________ Caterer__________________________________________________ _________________________________________________________ Table Settings____________________________________________ ________________________________________________________
MENU PLANNING Meatless Selections______________________________ _______________________________________________ Dietary Restrictions_____________________________ _______________________________________________ Main Menu______________________________________ _______________________________________________ _______________________________________________ _______________________________________________ Desserts_______________________________________ _______________________________________________ Appetizers/Snacks______________________________ _______________________________________________
MENU PLANNING Meatless Selections________________________________________ _________________________________________________________ Dietary Restrictions_______________________________________ _________________________________________________________ Main Menu________________________________________________ _________________________________________________________ _________________________________________________________ _________________________________________________________ Desserts_________________________________________________ _________________________________________________________ Appetizers/Snacks_________________________________________ _________________________________________________________
PARTY ESSENTIALS Invitations______________________________________ _______________________________________________ Entertainment___________________________________ _______________________________________________ Photos/Video___________________________________ _______________________________________________ Decorations_____________________________________ _______________________________________________ Gifts___________________________________________
PARTY ESSENTIALS Invitations_________________________________________________ __________________________________________________________ Entertainment______________________________________________ __________________________________________________________ Photos/Video______________________________________________ __________________________________________________________ Decorations_______________________________________________ __________________________________________________________ Gifts______________________________________________________
GROCERY SHOPPING LIST- ORGANIZATION
FRESH FOOD DRY GOODS HOUSEHOLD PERSONAL

THINGS TO DO - ORGANIZATION
DATE MONTH WEEK DAY TIME THINGS TO DO

DETAILED CONTACT INFORMATION - ORGANIZATION
Name:_______________________ Relation: ___________________
Phone: ______________________ Cell: ______________________
Fax: ________________________ e-Mail: ____________________Mail: ___________________________________________________________
Mail :____________________________________________________________Birthday: ____________________ Website: ___________________
Notes:___________________________________________________________
Name:_______________________ Relation: ___________________
Phone: ______________________ Cell: ______________________Fax: ________________________ e-Mail: ____________________
Mail: ___________________________________________________________
Mail :____________________________________________________________Birthday: ____________________ Website: ___________________
Notes:___________________________________________________________
Name:_______________________ Relation: ___________________
Phone: ______________________ Cell: ______________________
Fax: ________________________ e-Mail: ____________________Mail: ___________________________________________________________
Mail :____________________________________________________________Birthday: ____________________ Website: ___________________
Notes:___________________________________________________________
Name:_______________________ Relation: ___________________
Phone: ______________________ Cell: ______________________Fax: ________________________ e-Mail: ____________________
Mail: ___________________________________________________________Mail :____________________________________________________________
Birthday: ____________________ Website: ___________________
Notes:___________________________________________________________

FAMILY, FRIENDS, CO-WORKER WISH GIFT LIST - ORGANIZATION
BUY GIFT FOR: GIFT ITEM PRICE PURCHASE AT (WHERE?)
OCCASION DATE REQUIRED

DAILY ORGANIZER - ORGANIZATION Date: From______________________ To______________________________
TASK SUN
MON
TUE
WED
THU
FRI
SAT
MEALS
COUNT TOTAL
CALORIES
RECORDTOTAL
CALORIESBURNED
TRACK HEALTH
SYMPTONS
WARDROBE
APPOINTMENTS
MEETINGS
ERRANDS
BILLS
VACATION
SPECIALOCCAS ION
REMINDERS

PERSONAL PROPERTY INVENTORY SHEET 1 - ORGANIZATION
KITCHEN LIVINGROOM ARTICLE REPLACEMENT
COST ARTICLE REPLACEMENT
COST Table $ Couch $ Dinette Set $ Chairs $ Electric Appliances $ Lamps $ Dishes $ Tables $ Cutlery $ Radio/Stereo/Surround Sound $ Utensils $ TV Sets $ Pots & Pans $ Rugs/Carpets $ Bowls, Etc. $ Clocks $ Food Stuffs $ Paintings/Pictures $ Stove $ Curtains/Drapes $ Refrigerator $ Musical Instruments $ Dishwasher $ Phone/Answering Machine/Cell Phone $ Microwave $ Decorations/Ornaments $ $ $ $ $ TOTAL $ TOTAL $
DINING ROOM FAMILY – REC. ROOM ARTICLE REPLACEMENT
COST ARTICLE REPLACEMENT
COST Table $ Chairs $ Chairs $ Curtains, Drapes $ China Cabinet $ Couches $ Buffet $ Tables $ Serving Tables $ Lamps $ Rugs, Carpets $ Rugs, Carpets $ Curtains, Drapes $ Desk $ Electric Appliances $ Stereo/Radio/Surround Sound $ $ TV Set $ $ Gaming Devices $ $ $ $ $ $ $ $ $ $ $ TOTAL $ TOTAL $

PERSONAL PROPERTY INVENTORY SHEET 2 - ORGANIZATION
BEDROOMS REPLACEMENT COST OTHER ROOMS OTHER ROOMS ARTICLE 1 2 3 4 ARTICLE REPLACEMENT
COST ARTICLE REPLACEMENT
COST Chairs Beds Bedding Night Tables Clothes Bench Dressers Mirrors Rugs Lamps Clocks Curtains TOTAL TOTAL
BATHROOM #1 PATIO /DECK/VERANDA BASEMENT/GARAGE MISCELLANEOUS ARTICLE COST TO
REPLACE ARTICLE COST TO
REPLACE ARTICLE COST TO
REPLACE ARTICLE COST TO
REPLACE Curtains Chairs Work Bench Sports Equip. Floor Mats Dining Set Tools Books Sofa Toys Glider Christmas Dec. Tables Hobby Equip. BBQ / Grills Snow Blower Woodworking Equipment Lawn Mower Machinery
BATHROOM #2 Garden Tools House Plants Curtains Furniture Pool Equip. Floor Mats Luggage Air Conditioner Wash Machine Dryer Deep Freeze Freezer Content TOTAL TOTAL TOTAL TOTAL

PERSONAL PROPERTY INVENTORY SHEET 3 - ORGANIZATION
CLOTHING AND LINENS CHINA, CRYSTAL, ETC. ARTICLE REPLACEMENT
COST ARTICLE REPLACEMENT
COST Coats $ $ Raincoats $ $ Jackets $ $ Suits $ $ Dresses $ $ Sports Coats $ $ Shirts $ $ Slacks $ $ Sweaters $ $ Blouses $ $ Skirts $ $ Belts $ $ Scarves $ $ Socks $ $ Hosiery $ $ Ties $ $ Undergarments $ $ Lingerie $ $ Sleepwear $ SILVER, JEWELRY, FURS, STAMP / COIN / COLLECTIONS Shoes $ $ Boots $ $ Rubbers $ $ Slippers $ $ Hats $ $ Handbags $ $ Sportswear $ $ $ $ $ $ Sheets $ $ Pillow Cases $ $ Bedding $ $ Towels, hand & face $ $ $ $ $ $ $ $ $ $ $ $ TOTAL $ TOTAL $

PERSONAL PROPERTY INVENTORY SHEET 4 - ORGANIZATION
SUMMARY AREA TOTAL REPLACEMENT COST Kitchen $ Family – Recreation Room $ Living Room $ Dining Room $ Bedroom 1 $ Bedroom 2 $ Bedroom 3 $ Bedroom 4 $ Bathroom 1 $ Bathroom 2 $ Deck, Patio, Veranda $ Other Rooms $ Other Rooms $ Basement $ Garage $ Miscellaneous $ Clothing and Linen $ China and Crystal $ Silver, Jewelry. Etc. $ $ $ $ $ $ $ $ TOTAL $
Date if Initial Inventory: Revised: Revised:

SHOPPING INTERNET WEBSITES - ORGANIZATION WEBSITE ADDRESS USER I.D. PASSWORD

CONTACT INFORMATION - ORGANIZATION
Name:____________________________________________ Phone: ____________________________________
Reason for Contact:__________________________________________________________________________________
Fax: _____________________________________________ e-Mail: ___________________________________
Mail: _____________________________________________________________________________________________
Mail :______________________________________________________________________________________________
Notes:_____________________________________________________________________________________________
Name:____________________________________________ Phone: ____________________________________
Reason for Contact:__________________________________________________________________________________
Fax: _____________________________________________ e-Mail: ___________________________________
Mail: _____________________________________________________________________________________________
Mail :______________________________________________________________________________________________
Notes:_____________________________________________________________________________________________
Name:____________________________________________ Phone: ____________________________________
Reason for Contact:__________________________________________________________________________________
Fax: _____________________________________________ e-Mail: ___________________________________
Mail: _____________________________________________________________________________________________
Mail :______________________________________________________________________________________________
Notes:_____________________________________________________________________________________________

FAMILY SECTION
TABLE OF CONTENTS
PAGE # TOPIC / DESCRIPTION / TITLE

FIRE HOME ESCAPE PLAN
FIRE DEPARTMENT PHONE NUMBER:_____________________________________________________________
MEETING PLACE:_____________________________________________________________________________
HOW MANY SMOKE ALARMS DO YOU HAVE?______________________________________________________ Draw a floor plan or a map of your home. Show all doors and windows. Mark two ways out of each room. Smoke alarms should be in each sleeping room, outside each sleeping area, and on every level of the home. Pick a family meeting place outside where everyone can meet. Practice your plan at least twice a year!

OUR FAMILY - FAMILY
GRANDPARENTS GRANDPARENTS
PARENTS PARENTS
GENERATION ONE
GENERATION TWO

FAMILY BIRTHDAY LIST - FAMILY
DATE TIME PLACE WEIGHT FULL NAME BIRTHSTONE

FAMILY WEEKLY SCHEDULE - FAMILY DAY TIME
NAME: ________________
NAME: ________________
NAME: ________________
NAME: ________________
MORNING:_______ EVENT
EVENT EVENT EVENT
AFTERNOON:_____ EVENT
EVENT EVENT EVENT
SUN
DATE:_______ EVENING:________
EVENT
EVENT EVENT EVENT
MORNING:_______ EVENT
EVENT EVENT EVENT
AFTERNOON:_____ EVENT
EVENT EVENT EVENT
MON
DATE:_______ EVENING:________
EVENT
EVENT EVENT EVENT
MORNING:_______ EVENT
EVENT EVENT EVENT
AFTERNOON:_____ EVENT
EVENT EVENT EVENT
TUE
DATE:_______ EVENING:________
EVENT
EVENT EVENT EVENT
MORNING:_______ EVENT
EVENT EVENT EVENT
AFTERNOON:_____ EVENT
EVENT EVENT EVENT
WED
DATE:_______ EVENING:________
EVENT
EVENT EVENT EVENT
MORNING:__________
EVENT
EVENT EVENT EVENT
AFTERNOON:_____ EVENT
EVENT EVENT EVENT THU
DATE:_______
EVENING:________ EVENT
EVENT EVENT EVENT
MORNING:_______ EVENT
EVENT EVENT EVENT
AFTERNOON:_____ EVENT
EVENT EVENT EVENT
FRI
DATE:_______ EVENING:________
EVENT
EVENT EVENT EVENT
MORNING:_______ EVENT
EVENT EVENT EVENT
AFTERNOON:_____ EVENT
EVENT EVENT EVENT
SAT
DATE:_______ EVENING:________
EVENT
EVENT EVENT EVENT

COMPANY / GUEST / VISITORS - FAMILY
Family Name:________________________ Arrival:______________ Departure:___________ First Names:__________________________________________________________________________
Contact Phone Numbers: _______________________________________________________________ Transportation Requirements:___________________________________________________________ Accommodations: _____________________________________________________________________ Special Diets / Instructions: ____________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ Family Name:________________________ Arrival:______________ Departure:__________ First Names:__________________________________________________________________________ Contact Phone Numbers: _______________________________________________________________ Transportation Requirements:___________________________________________________________ Accommodations: _____________________________________________________________________ Special Diets / Instructions: ____________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________

PERSONAL CONTACTS - FAMILY
Name:____________________________________________ Relation: ____________________
Phone: ______________________ Cell: ______________________ e-MAIL: _____________________
Mail: ________________________________________________________________________________
Mail :_________________________________________________________________________________
Website: ____________________ ______ Fax: ___________________ Birthday:__________________
Notes:________________________________________________________________________________
_____________________________________________________________________________________
Name:____________________________________________ Relation: ____________________
Phone: ______________________ Cell: ______________________ e-MAIL: _____________________
Mail: ________________________________________________________________________________
Mail :_________________________________________________________________________________
Website: ____________________ ______ Fax: ___________________ Birthday:__________________
Notes:________________________________________________________________________________
_____________________________________________________________________________________
Name:____________________________________________ Relation: ____________________
Phone: ______________________ Cell: ______________________ e-MAIL: _____________________
Mail: ________________________________________________________________________________
Mail :_________________________________________________________________________________
Website: ____________________ ______ Fax: ___________________ Birthday:__________________
Notes:________________________________________________________________________________
_____________________________________________________________________________________

FAMILY TRADITIONS - FAMILY
OCCASION TRADITION

POSITIVE REWARD CHART - FAMILY
NAME:____________________ START DATE:_______________ END DATE:_________________
CHORES/ TASK
BEHAVIOUR / CHANGE
REWARD / INCENTIVE
SUN MON TUE WED THU FRI SAT WEEKLY TOTALS
COMMENTS:________________________________________________________________________________________________________________________________________________________________________________________
NAME:____________________ START DATE:_______________ END DATE:_________________
CHORES/ TASK
BEHAVIOUR / CHANGE
REWARD / INCENTIVE
SUN MON TUE WED THU FRI SAT WEEKLY TOTALS
COMMENTS:________________________________________________________________________________________________________________________________________________________________________________________

“FIND IT” TREASURE NOTES - FAMILY USE “FIND IT” TREASURE NOTES TO CREATE A TRAIL FOR A CHILD TO SEARCH FOR A LITTLE TREASURE THAT IS A TOY, A GIFT OR A TREAT. EACH NOTE LEADS CLOSER TO THE ‘TREASURE’! DRAW OR PRINT A CLUE OR HINT THAT LEADS TO THE NEXT NOTE. THE ‘TREASURE’ (TOY, REWARD, GIFT OR TREAT) CAN BE FOUND AFTER 4 OR 8 CLUES DEPENDING ON THE AGE OF THE CHILD.
CLUE NUMBER _____________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________
CLUE NUMBER _____________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________
CLUE NUMBER _____________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________
CLUE NUMBER _____________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________
FAMILY TREE GENERATION 1 - 3 – FAMILY OUR FAMILY TREE – NAME:________________________________
Husband’s Full Name: Wife’s Full Name: Date of Marriage: Place of Marriage: Our Children:
GENERATION #2 GENERATION #2
GENERATION #3 GENERATION #3
Generation 3 continues next page……
Husband’s Father’s Full Name: Husband’s Mother’s Full Name: Date of Marriage: Place of Marriage: Children:
Wife’s Father’s Full Name: Wife’s Mother’s Full Name: Date of Marriage: Place of Marriage: Children:
Wife’s Paternal Grandfather’s Full Name: Wife’s Paternal Grandmother’s Full Name: Date of Marriage: Place of Marriage: Children:
Husband’s Paternal Grandfather’s Full Name: Husband’s Paternal Grandmother’s Full Name: Date of Marriage: Place of Marriage: Children:

FAMILY TREE GENERATION 3 Con’t & 4 - FAMILY GENERATION #3 GENERATION #3
GENERATION #4 GENERATION #4
HUSBAND’S GREAT GRANDFATHER’S FULL NAME
WIFE’S GREAT GRANDFATHER’S FULL NAME
HUSBAND’S GREAT GRANDMOTHER’S FULL NAME
WIFE’S GREAT GRANDMOTHER’S FULL NAME
HUSBAND’S GREAT GRANDFATHER’S FULL NAME
WIFE’S GREAT GRANDFATHER’S FULL NAME
HUSBAND’S GREAT GRANDMOTHER’S FULL NAME
WIFE’S GREAT GRANDMOTHER’S FULL NAME
HUSBAND’S GREAT GRANDFATHER’S FULL NAME
WIFE’S GREAT GRANDFATHER’S FULL NAME
HUSBAND’S GREAT GRANDMOTHER’S FULL NAME
WIFE’S GREAT GRANDMOTHER’S FULL NAME
HUSBAND’S GREAT GRANDFATHER’S FULL NAME
WIFE’S GREAT GRANDFATHER’S FULL NAME
HUSBAND’S GREAT GRANDMOTHER’S FULL NAME
WIFE’S GREAT GRANDMOTHER’S FULL NAME
Husband’s Maternal Grandfather’s Full Name: Husband’s Maternal Grandmother’s Full Name: Date of Marriage: Place of Marriage: Children:
Wife’s Maternal Grandfather’s Full Name:
Wife’s Maternal Grandmother’s Full Name: Date of Marriage: Place of Marriage: Children:

FAMILY TREE GENERATION 5 - FAMILY GENERATION #5 GENERATION #5
HUSBAND’S GREAT GREAT GRANDFATHER’S FULL NAME
WIFE’S GREAT GREAT GRANDFATHER’S FULL NAME
HUSBAND’S GREAT GREAT GRANDMOTHER’S FULL NAME
WIFE’S GREAT GREAT GRANDMOTHER’S FULL NAME
HUSBAND’S GREAT GREAT GRANDFATHER’S FULL NAME
WIFE’S GREAT GREAT GRANDFATHER’S FULL NAME
HUSBAND’S GREAT GREAT GRANDMOTHER’S FULL NAME
WIFE’S GREAT GREAT GRANDMOTHER’S FULL NAME
HUSBAND’S GREAT GREAT GRANDFATHER’S FULL NAME
WIFE’S GREAT GREAT GRANDFATHER’S FULL NAME
HUSBAND’S GREAT GREAT GRANDMOTHER’S FULL NAME
WIFE’S GREAT GREAT GRANDMOTHER’S FULL NAME
HUSBAND’S GREAT GREAT GRANDFATHER’S FULL NAME
WIFE’S GREAT GREAT GRANDFATHER’S FULL NAME
HUSBAND’S GREAT GREAT GRANDMOTHER’S FULL NAME
WIFE’S GREAT GREAT GRANDMOTHER’S FULL NAME
HUSBAND’S GREAT GREAT GRANDFATHER’S FULL NAME
WIFE’S GREAT GREAT GRANDFATHER’S FULL NAME
HUSBAND’S GREAT GREAT GRANDMOTHER’S FULL NAME
WIFE’S GREAT GREAT GRANDMOTHER’S FULL NAME
HUSBAND’S GREAT GREAT GRANDFATHER’S FULL NAME
WIFE’S GREAT GREAT GRANDFATHER’S FULL NAME
HUSBAND’S GREAT GREAT GRANDMOTHER’S FULL NAME
WIFE’S GREAT GREAT GRANDMOTHER’S FULL NAME
HUSBAND’S GREAT GREAT GRANDFATHER’S FULL NAME
WIFE’S GREAT GREAT GRANDFATHER’S FULL NAME
HUSBAND’S GREAT GREAT GRANDMOTHER’S FULL NAME
WIFE’S GREAT GREAT GRANDMOTHER’S FULL NAME
HUSBAND’S GREAT GREAT GRANDFATHER’S FULL NAME
WIFE’S GREAT GREAT GRANDFATHER’S FULL NAME
HUSBAND’S GREAT GREAT GRANDMOTHER’S FULL NAME
WIFE’S GREAT GREAT GRANDMOTHER’S FULL NAME

FAMILY TREE GENERATION 6 - FAMILY GENERATION #6 GENERATION #6
HUSBAND’S GREAT GREAT GREAT GRANDPARENT’S FULL NAME
WIFE’S GREAT GREAT GREAT GRANDPARENT’S FULL NAME
HUSBAND’S GREAT GREAT GREAT GRANDPARENT’S FULL NAME
WIFE’S GREAT GREAT GREAT GRANDPARENT’S FULL NAME
HUSBAND’S GREAT GREAT GREAT GRANDPARENT’S FULL NAME
WIFE’S GREAT GREAT GREAT GRANDPARENT’S FULL NAME
HUSBAND’S GREAT GREAT GREAT GRANDPARENT’S FULL NAME
WIFE’S GREAT GREAT GREAT GRANDPARENT’S FULL NAME
HUSBAND’S GREAT GREAT GREAT GRANDPARENT’S FULL NAME
WIFE’S GREAT GREAT GREAT GRANDPARENT’S FULL NAME
HUSBAND’S GREAT GREAT GREAT GRANDPARENT’S FULL NAME
WIFE’S GREAT GREAT GREAT GRANDPARENT’S FULL NAME
HUSBAND’S GREAT GREAT GREAT GRANDPARENT’S FULL NAME
WIFE’S GREAT GREAT GREAT GRANDPARENT’S FULL NAME
HUSBAND’S GREAT GREAT GREAT GRANDPARENT’S FULL NAME
WIFE’S GREAT GREAT GREAT GRANDPARENT’S FULL NAME
HUSBAND’S GREAT GREAT GREAT GRANDPARENT’S FULL NAME
WIFE’S GREAT GREAT GREAT GRANDPARENT’S FULL NAME
HUSBAND’S GREAT GREAT GREAT GRANDPARENT’S FULL NAME
WIFE’S GREAT GREAT GREAT GRANDPARENT’S FULL NAME
HUSBAND’S GREAT GREAT GREAT GRANDPARENT’S FULL NAME
WIFE’S GREAT GREAT GREAT GRANDPARENT’S FULL NAME
HUSBAND’S GREAT GREAT GREAT GRANDPARENT’S FULL NAME
WIFE’S GREAT GREAT GREAT GRANDPARENT’S FULL NAME
HUSBAND’S GREAT GREAT GREAT GRANDPARENT’S FULL NAME
WIFE’S GREAT GREAT GREAT GRANDPARENT’S FULL NAME
HUSBAND’S GREAT GREAT GREAT GRANDPARENT’S FULL NAME
WIFE’S GREAT GREAT GREAT GRANDPARENT’S FULL NAME
HUSBAND’S GREAT GREAT GREAT GRANDPARENT’S FULL NAME
WIFE’S GREAT GREAT GREAT GRANDPARENT’S FULL NAME
HUSBAND’S GREAT GREAT GREAT GRANDPARENT’S FULL NAME
WIFE’S GREAT GREAT GREAT GRANDPARENT’S FULL NAME
OUR FAMILY
_________________________________________
Joined
_________________________________________
In marriage
At____________________________________________________________________________ Address______________________________________________________________________ Month_____________________________ Day________________________ Year___________ Married by____________________________________________________________________
HUSBAND’S GENEALOGY WIFE’S GENEALOGY Husband’s full name;____________________ ______________________________________ Birth Date;____________________________ Birth Place;____________________________ Father’s full name;______________________ ______________________________________ Mother’s full name;_____________________ _____________________________________ Brothers and sisters;___________________ ______________________________________ ______________________________________
Wife’s full name;_____________________________ ___________________________________________ Birth Date;__________________________________ Birth Place;_________________________________ Father’s full name;___________________________ ___________________________________________ Mother’s full name;__________________________ ___________________________________________ Brothers and sisters;________________________ ___________________________________________ ___________________________________________

FAMILY TREE INDEX
PAGE# TITLE PAGE# TITLE

FAMILY TREE - OUR (GRAND)/CHILDREN
OUR CHILDREN
FULL NAME PLACE OF BIRTH DATE OF BIRTH
OUR GRANDCHILDREN
FULL NAME PLACE OF BIRTH DATE OF BIRTH

FAMILY TREE – SIBLINGS/NIECES/NEPHEWS HUSBAND, HIS BROTHERS AND SISTERS AND THEIR CHILDREN; BORN DIED SPOUSE ___________________________________________________________________________________________________ CHILDREN_______________________________________________ _____________________________________________________________________________________ CHILDREN_______________________________________________ _____________________________________________________________________________________ CHILDREN_______________________________________________ _____________________________________________________________________________________ CHILDREN_______________________________________________ _____________________________________________________________________________________ CHILDREN_______________________________________________ WIFE, HER BROTHERS AND SISTERS AND THEIR CHILDREN; BORN DIED SPOUSE ___________________________________________________________________________________________________ CHILDREN_______________________________________________ ___________________________________________________________________________________________________ CHILDREN_______________________________________________ ___________________________________________________________________________________________________ CHILDREN_______________________________________________ ___________________________________________________________________________________________________ CHILDREN_______________________________________________ ___________________________________________________________________________________________________ CHILDREN_______________________________________________ ___________________________________________________________________________________________________ CHILDREN_______________________________________________

MY SCHOOL DAYS
START:___________________ COMPLETION:__________________
THIS BOOK BELONGS TO….. ________________________________ ________________________________

MY SCHOOL DAYS - INDEX
PAGE# TITLE PAGE# TITLE

MY SCHOOL DAYS – GRADES____ TO ____
SCHOOL:____________________________ TEACHER:________________ GRADE:_______________ SCHOOL YEAR DATE: START:__________________________ FINISH:______________________ HEIGHT:_______________ WEIGHT:___________ AGE:__________ YEAR:__________
___________________________________________
SIGNATURE
NEW FRIENDS:_________________________________________________________________________ __________________________________________________________________________________________________________________________________________________________________________ EXTRA ACTIVITES:______________________________________________________________________ __________________________________________________________________________________________________________________________________________________________________________ SPECIAL EVENTS ATTENDED:_____________________________________________________________ __________________________________________________________________________________________________________________________________________________________________________ ACHIEVEMENTS / AWARDS:______________________________________________________________ __________________________________________________________________________________________________________________________________________________________________________
PHOTO

MY SCHOOL DAYS – MEMORIES / MILESTONES
WHEN I GROW UP I WANT TO BE;_________________________________________________________ MY CLOSEST FRIENDS;__________________________________________________________________ _______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ CLUBS AND ACTIVITIES I JOINED;_________________________________________________________ _______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ SPECIAL EVENTS I ATTENDED;____________________________________________________________ _______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ CERTIFICATES AND AWARDS I RECEIVED;__________________________________________________ _______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ MY ACADEMIC GOALS;___________________________________________________________________ _______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ MEMORIES AND MILESTONES;_____________________________________________________________ ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

TRAVEL SECTION
TABLE OF CONTENTS
PAGE # TOPIC / DESCRIPTION / TITLE

TRAVEL ITINERARY
VACATION / TRAVEL / TRIP PLANNER******************DEPARTURE******************
DEPARTURE FROM:___________
DESTINATION TO:______________
DURATION OF TRIP_____________
DEPART DATE
DEPART TIME ARRIVAL DATE
ARRIVAL TIME
TRAVEL TIME TRAVEL COST
CAR RENTAL LODGING PHONE NUMBERS FLIGHT # / NOTES
VACATION / TRAVEL / TRIP PLANNER********************RETURN**********************
DEPARTURE FROM:___________
DESTINATION TO:______________
DURATION OF TRIP_____________
DEPART DATE
DEPART TIME ARRIVAL DATE
ARRIVAL TIME
TRAVEL TIME TRAVEL COST
CAR RENTAL LODGING PHONE NUMBERS FLIGHT # / NOTES

ITEMS TO PACK - TRAVEL
√ ITEMS TO PACK √ ITEMS TO PACK
REMINDERS - TRAVEL
√ BEFORE TRIP √ AFTER TRIP

PLACES I HAVE VISITED - TRAVEL
DATE DURATION PLACE

DAILY VACATION ITINERARY - TRAVEL
DAY TIME PLACE/EVENT/NAME: ________________
PLACE/EVENT/NAME: ________________
PLACE/EVENT/NAME: ________________
PLACE/EVENT/NAME: ________________
MORNING:_______ EVENT
EVENT EVENT EVENT
AFTERNOON:_____ EVENT
EVENT EVENT EVENT
SUN
DATE:_______ EVENING:________
EVENT
EVENT EVENT EVENT
MORNING:_______ EVENT
EVENT EVENT EVENT
AFTERNOON:_____ EVENT
EVENT EVENT EVENT
MON
DATE:_______ EVENING:________
EVENT
EVENT EVENT EVENT
MORNING:_______ EVENT
EVENT EVENT EVENT
AFTERNOON:_____ EVENT
EVENT EVENT EVENT
TUE
DATE:_______ EVENING:________
EVENT
EVENT EVENT EVENT
MORNING:_______ EVENT
EVENT EVENT EVENT
AFTERNOON:_____ EVENT
EVENT EVENT EVENT
WED
DATE:_______ EVENING:________
EVENT
EVENT EVENT EVENT
MORNING:__________
EVENT
EVENT EVENT EVENT
AFTERNOON:_____ EVENT
EVENT EVENT EVENT THU
DATE:_______
EVENING:________ EVENT
EVENT EVENT EVENT
MORNING:_______ EVENT
EVENT EVENT EVENT
AFTERNOON:_____ EVENT
EVENT EVENT EVENT
FRI
DATE:_______ EVENING:________
EVENT
EVENT EVENT EVENT
MORNING:_______ EVENT
EVENT EVENT EVENT
AFTERNOON:_____ EVENT
EVENT EVENT EVENT
SAT
DATE:_______ EVENING:________
EVENT
EVENT EVENT EVENT

CONTACTS - TRAVEL
Name:__________________________________________ Phone: _________________________________
Reason for Contact:_______________________________________________________________________________
Fax: ___________________________________________ e-Mail: _________________________________
Mail: ____________________________________________________________________________________________
Mail :_____________________________________________________________________________________________
Notes:_____________________________________________________________________________________________
Name:__________________________________________ Phone: _________________________________
Reason for Contact:_______________________________________________________________________________
Fax: ___________________________________________ e-Mail: _________________________________
Mail: ____________________________________________________________________________________________
Mail :_____________________________________________________________________________________________
Notes:_____________________________________________________________________________________________
Name:__________________________________________ Phone: _________________________________
Reason for Contact:_______________________________________________________________________________
Fax: ___________________________________________ e-Mail: _________________________________
Mail: ____________________________________________________________________________________________
Mail :_____________________________________________________________________________________________
Notes:_____________________________________________________________________________________________

VACATION BUDGET - TRAVEL
GENERAL DETAILS
DESTINATION: ______________________________________ HOW MANY?: _______________________________________ HOW LONG?:________________________________________ DEPART DATE:______________________________________ ARRIVE DATE:_______________________________________ DEPART DATE:______________________________________ RETURN DATE:______________________________________ TOTAL DAYS:________________________________________
TOTAL COSTS TRAVEL EXPENSES:---------------------$___________________
ACCOMMODATIONS:--------------------$___________________
MEALS EXPENSES: ---------------------$___________________
EVENTS EXPENSES : --------------------$___________________
ENTERTAINMENT:----------------------- $___________________
SHOPPING EXPENSE:------------------ $____________________
OTHER EXPENSES:--------------------- $____________________
TOTAL: $_________________
TRANSPORTATION Vehicle $_______________
Fuel $_______________ Maintenance $_______________
Parking $_______________ Highway Fees $_______________ Highway Tolls $_______________
Vehicle Rentals $_______________ Vehicle Lodging $_______________
Vehicle Insurance$_______________ Bus $_______________
Train $_______________ Airplane $_______________
Travel Insurance $_______________ Health Insurance $_______________
Passport Fee $_______________ Other Fees: $_______________ Other Fees: $_______________
TRANSPORTATION INFORMATION
Vehicle Lease #: _______________ Bus Ticket#: _______________ Bus Seat #: _______________
Train Ticket #: _______________ Train Seat #: _______________
Airplane Flight #: _______________ Airplane Seat #: _______________
Hotel Phone#: _______________ Hotel Room #: _______________
Other Information: _______________ Other Information: _______________ Other Information: _______________ Other Information: _______________ NOTES: _________________________ ________________________________ ________________________________
EVENTS & ENTERTAINMENT
Event Tickets: $_______________ Entertainment: $_______________
Other Fees: $_______________ Other Fees: $_______________ Other Fees: $_______________ Other Fees: $_______________
NOTES:_________________________ _______________________________ _______________________________ _______________________________ _______________________________ _______________________________ _______________________________ _______________________________ _______________________________
PERSONAL PURCHASES
Shopping: $_______________ Souvenirs: $_______________
Taxes: $_______________ Duties: $_______________
Other Fees: $_______________ Other Fees: $_______________
NOTES:_________________________ _______________________________ _______________________________ _______________________________ _______________________________ _______________________________ _______________________________ _______________________________ _______________________________
ACCOMMODATIONS Hotel: $_______________
Room & Board: $_______________ Bed & Breakfast: $_______________
Camp Ground : $_______________ Other Fees: $_______________ Other Fees: $_______________
MEALS Restaurants $_______________
Groceries: $_______________ Consumables: $_______________
Other Fees: $_______________ Other Fees: $_______________ Other Fees: $_______________
PETS Boarding/Ship: $_______________
Pet Supplies: $_______________ Other Fees: $_______________ Other Fees: $_______________ Other Fees: $_______________ Other Fees: $_______________
ADDITIIONAL COSTS Other Fees: $_______________ Other Fees: $_______________ Other Fees: $_______________ Other Fees: $_______________ Other Fees: $_______________ Other Fees: $_______________

VACATION SCHEDULER - TRAVEL
PUBLIC HOLIDAYS CIRCLE DATES & RECORD VACATIONS BELOW New Year's Day Jan. 1 ___________________________________ Family Day Feb. 18 Good Friday March 21 ___________________________________ Easter Sunday March 23 Victoria Day May 19 ___________________________________ Canada Day July 1 Labour Day Sept. 1 ___________________________________ Thanksgiving Day Oct. 13 Remembrance Day Nov. 11 ___________________________________ Christmas Dec. 25 Boxing Day Dec. 26 ___________________________________

VEHICLE MAINTENANCE LOG - TRAVEL
VEHICLE:__________________ PLATE No.:_________________ VIN:_________________________
DATE:_________________________
ITEMS TO CHECK
√ - NEEDS
REPAIR
√ - GOOD
CONDITION
MILEAGE:___________________
COMMENTS
Seats, Seat Belts
Brakes
Park Brakes
Horn
Steering & Shifting
Tires
Engine Oil Level
Gauges
Cleanliness
Hood Latch
Safety Labels
Stepping Rails
Fire Extinguisher
Fuel Tank & Radiator
Power Shift Transmission
Battery & Belts & Hoses
Exhaust, / Spark Plugs
Windows & Wipers
Check for leaks, oil, hydraulic & coolant
Air / Fuel Filter (DATE:_________________)
OIL CHANGE DATE:_____________________

JOURNALING SECTION
TABLE OF CONTENTS
PAGE # TOPIC / DESCRIPTION / TITLE

PERSONAL SELF HELP MANUAL – JOURNALING
DATE:______________________________
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
PAGE #_________________________

PERSONAL SELF HELP MANUAL
"The investment you make in yourself today will determine the quality of your life in the days and years to come." Author Unknown © 2008 All forms created for the “Personal Self Help Manual” are copyrighted to Siscan Publications and you are granted permission to print/photocopy as required for your own personal use only.