The - indri.lecture.ub.ac.id · 1/3 caudal ventral abdomen. Above linea arcuata / 2/3 cranial...
52
•The Wall • The Cavity • The Mesentery The The The The Abdomen Abdomen Abdomen Abdomen EMBRYOLOGY EMBRYOLOGY EMBRYOLOGY EMBRYOLOGY
Transcript of The - indri.lecture.ub.ac.id · 1/3 caudal ventral abdomen. Above linea arcuata / 2/3 cranial...

•The Wall• The Cavity• The Mesentery
The The The The
AbdomenAbdomenAbdomenAbdomen
EMBRYOLOGYEMBRYOLOGYEMBRYOLOGYEMBRYOLOGY

ABDOMINAL REGION
subcostal
transtubercular

The Abdominal Wall • Cutan• Subcutan � Fascia abdominis
superficialis• Muscles and its fasciae
a. M. obliquus abdominis externus
b. M. obliquus abdominis internus
c. M. Transversus abdominis
d. M. Rectus abdominis � anterior abdominal wall
• Fascia Transversalis • Peritoneum Parietalis

Struktur Khusus pada Dinding Abdomen (anterior)
� Linea albaLinea albaLinea albaLinea alba � garis o.k. pertemuan aponeurosis otot-2 dinding abdomen
� SSSSarungarungarungarung Rectus Rectus Rectus Rectus ( Vagina ( Vagina ( Vagina ( Vagina m.rectim.rectim.rectim.recti abdominisabdominisabdominisabdominis ) ) ) ) ���� Kumpulan aponeurosis yang membungkus M. rectus abdominis :◦ 2/3 2/3 2/3 2/3 atasatasatasatas dindingdindingdindingdinding abdomen abdomen abdomen abdomen ( ( ( ( diatasdiatasdiatasdiatas linealinealinealinea arcuataarcuataarcuataarcuata ) ) ) )� diatas m. rectus : lamina anterior : Fascia m.o.a.e &
Fascia m.o.a.i� dibawah m. rectus : lamina posterior : Fascia m.o.a.I &
Fascia m.transversus abdominis◦ 1/3 1/3 1/3 1/3 bawahbawahbawahbawah dindingdindingdindingdinding abdomen abdomen abdomen abdomen ( ( ( ( dibawahdibawahdibawahdibawah linealinealinealinea arcuataarcuataarcuataarcuata ) ) ) )� diatas m. rectus : lamina anterior & posterior � dibawah m. rectus : Fascia transversalis
� CanalisCanalisCanalisCanalis inguinalisinguinalisinguinalisinguinalis

Subkutan(Fascia Superficialis )• Fascia Camperi � fatty layer• Fascia Scarpae � membranous layer
M.Latissimus dorsi
M.Serratus anterior
M.Obliquus abdominis externus
SUPERFICIAL SUPERFICIAL SUPERFICIAL SUPERFICIAL VENTRAL WALLVENTRAL WALLVENTRAL WALLVENTRAL WALL

Linea albaM. Rectus abdominis
Inscriptiones tendinea
M.Pyramidalis
M.o.a.externusM. Intercostalis externus
M. Obliquus abdominis internus INTERMEDIATEINTERMEDIATEINTERMEDIATEINTERMEDIATE
VENTRAL WALLVENTRAL WALLVENTRAL WALLVENTRAL WALL

M.Transversus abdominis
A/V epigastrica inferior
Peritoneum parietalis
Rectus sheath
ventral
dorsal Linea arcuata
DEEP VENTRAL WALLDEEP VENTRAL WALLDEEP VENTRAL WALLDEEP VENTRAL WALL
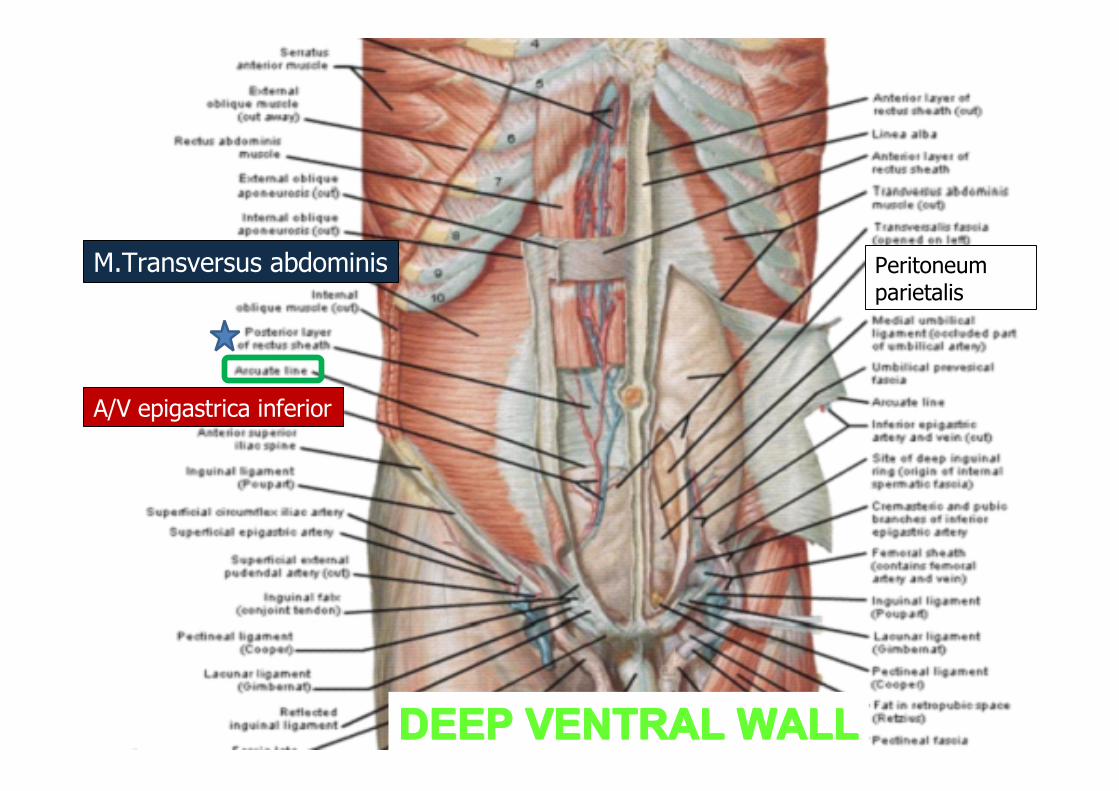
M.Transversus abdominis
A/V epigastrica inferior
Peritoneum parietalis
DEEP VENTRAL WALLDEEP VENTRAL WALLDEEP VENTRAL WALLDEEP VENTRAL WALL

Above linea arcuata / 2/3 cranial ventral abdomen)
Below linea arcuata /1/3 caudal ventral
abdomen

Above linea arcuata / 2/3 cranial ventral abdomen)
Below linea arcuata /1/3 caudal ventral
abdomen

Peritoneum & Its Derivates• Peritoneum parietalis
• Cavum Peritonei , divided into :
• Saccus major ( Cavum peritoneum s.s. )� ventral gaster
• Saccus minor ( Bursa Omentalis )� dorsal gaster
• The two is connected through Foramen Winslowi
• Peritoneum visceralis :
• Omentum
• Mesenterium

Omentum minus
Saccus major
Omentum majus
Bursa omentalis
Bare Area ( pars affixa hepatis )



Omentum
• OmentumOmentumOmentumOmentum minus minus minus minus
2 folds of peritoneum 2 folds of peritoneum 2 folds of peritoneum 2 folds of peritoneum
visceralisvisceralisvisceralisvisceralis between between between between
curvaturacurvaturacurvaturacurvatura minor minor minor minor gastergastergastergaster & & & &
heparheparheparhepar
• OmentumOmentumOmentumOmentum majusmajusmajusmajus
4 folds of peritoneum 4 folds of peritoneum 4 folds of peritoneum 4 folds of peritoneum
visceralisvisceralisvisceralisvisceralis arise from arise from arise from arise from
curvaturacurvaturacurvaturacurvatura major distally major distally major distally major distally
G
I
H
Om
OM
SM
Sm(BO)


2. Mesenterium• Mesogastrium VentralisMesogastrium VentralisMesogastrium VentralisMesogastrium Ventralis
Mesenterium Ventralis :Mesenterium Ventralis :Mesenterium Ventralis :Mesenterium Ventralis :– 1. Lig. Falciformehepatis 1. Lig. Falciformehepatis 1. Lig. Falciformehepatis 1. Lig. Falciformehepatis– 2. Omentum minus 2. Omentum minus 2. Omentum minus 2. Omentum minus ( lig. gastro- hepatica ) ( lig. gastro- hepatica ) ( lig. gastro- hepatica ) ( lig. gastro- hepatica )– 3. Lig. Triangulare hepatis 3. Lig. Triangulare hepatis 3. Lig. Triangulare hepatis 3. Lig. Triangulare hepatis– 4. Lig. Coronaria hepatis 4. Lig. Coronaria hepatis 4. Lig. Coronaria hepatis 4. Lig. Coronaria hepatis
• Mesogastrium DorsalisMesogastrium DorsalisMesogastrium DorsalisMesogastrium Dorsalis
Mesenterium Dorsalis :Mesenterium Dorsalis :Mesenterium Dorsalis :Mesenterium Dorsalis :– 5. Lig. Gastrolienalis 5. Lig. Gastrolienalis 5. Lig. Gastrolienalis 5. Lig. Gastrolienalis– 6. Lig. Gastrophrenica 6. Lig. Gastrophrenica 6. Lig. Gastrophrenica 6. Lig. Gastrophrenica
G
L
H
G
Ventral
123456
MV
MD
Dorsal
CP
CPCP

18
CANALIS INGUINALIS
• oblique passage taken through the lower abdominal wall by
the testis and cord (the round ligament in the female).
• The canal is 1.5 in (4 cm) long.
• It passes downwards and medially from the internal to the
external inguinal rings
• parallel to the inguinal ligament.



EMBRIOLOGYof DIGESTIVE SYSTEM

Divisions of Gut Tube
Result of cephalocaudal & lateral folding � Primitive Gut : Primitive Gut : Primitive Gut : Primitive Gut :
–Pharyngeal gut : Pharyngeal gut : Pharyngeal gut : Pharyngeal gut : bucopharyngeal mbr – tracheobr diverticulum
–FFFForegut : oregut : oregut : oregut : caudal pharyngeal tube- liver bud
–MMMMidgutidgutidgutidgut : : : :liver bud – 2/3 prox colon transversum
–HHHHindgut : indgut : indgut : indgut : 1/3 distal colon transv – cloacal mbr


ForegutESOPHAGUSESOPHAGUSESOPHAGUSESOPHAGUS• 4 weeks old : lung bud appears from ventral
wall of the foregut � tracheoesophageal septum :– Respiratory primordium : ventral– Esophagus : dorsal

formation of the gastrointestinal tract and the various derivatives originating from the endodermal germ layer

Clinical Correlates
• Esophageal atresia• Tracheo-
esophageal fistula• Congenital hiatal
hernia
Foregut

STOMACH• 4th week :fusiform dilatation• Rotate :longitudinal and anteroposterior axis
Foregut

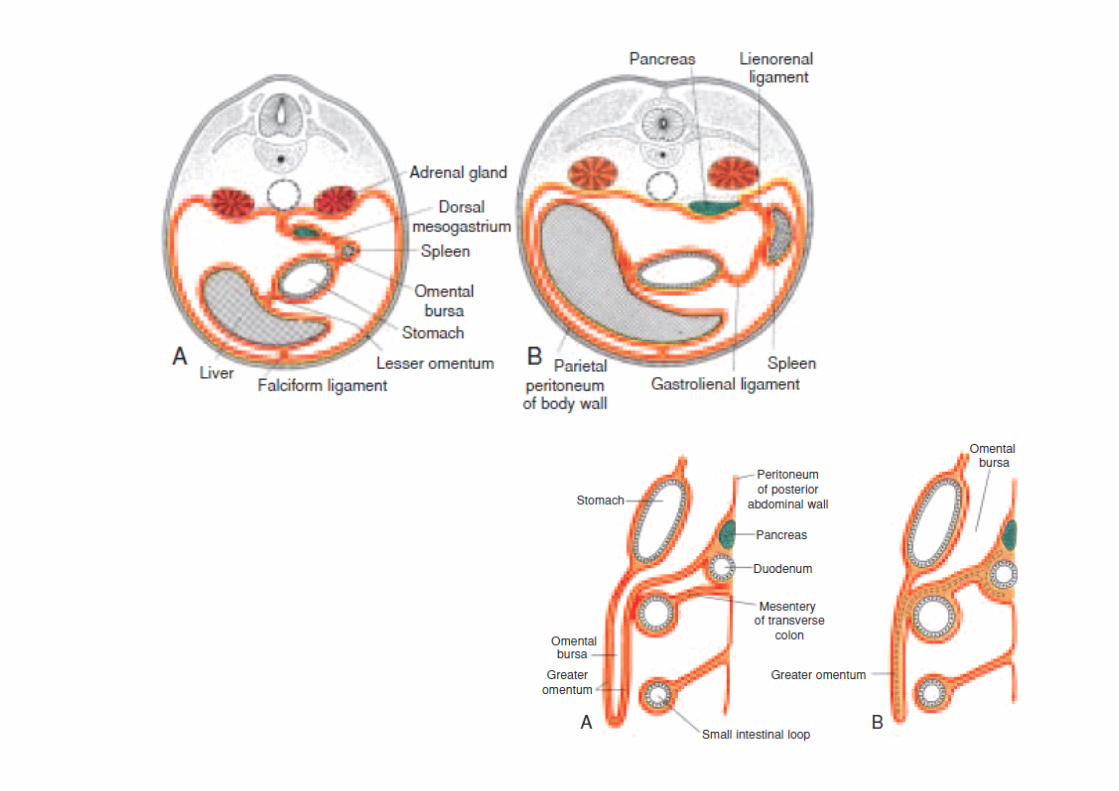
Mesentery• Stomach attached to :
– Dorsal dorsal mesogastrium– Ventral : ventral mesogastrium
• Rotation longitudinal axis : space behind stomach � bursa omentalis, lengthen of dorsalmesogastrium : spleen and pancreas become retroperitoneal
• Rotation ant-post axis : omentum majus• Growth of the liver into the mesenchyme of the septum
transversum divides the ventral mesentery into– (a)The lesser omentum, extending from the lower portion of
the esophagus, the stomach, and the upper portion of the duodenum to the liver, and
– (b)the falciformligament,


Duodenum• As the stomach rotates � C-shaped , swings
to the left side of abdominal cavity• Duodenum and pancreas� dorsal body wall � retroperitoneal, except duodenal cap
• 2nd month, lumen of duodenum obliterated � recanalisation
Foregut


Liver and Gall Bladder
• 3rd week : outgrowth endodermal epithelium at distal part of foregut � liver bud � penetrate septum transversum
• Connection between liver bud and duodenum narrowing � bile duct , gall bladder, cystic duct
• 10th week ; the liver approximately 10% of total body weight � 5% at 7th month


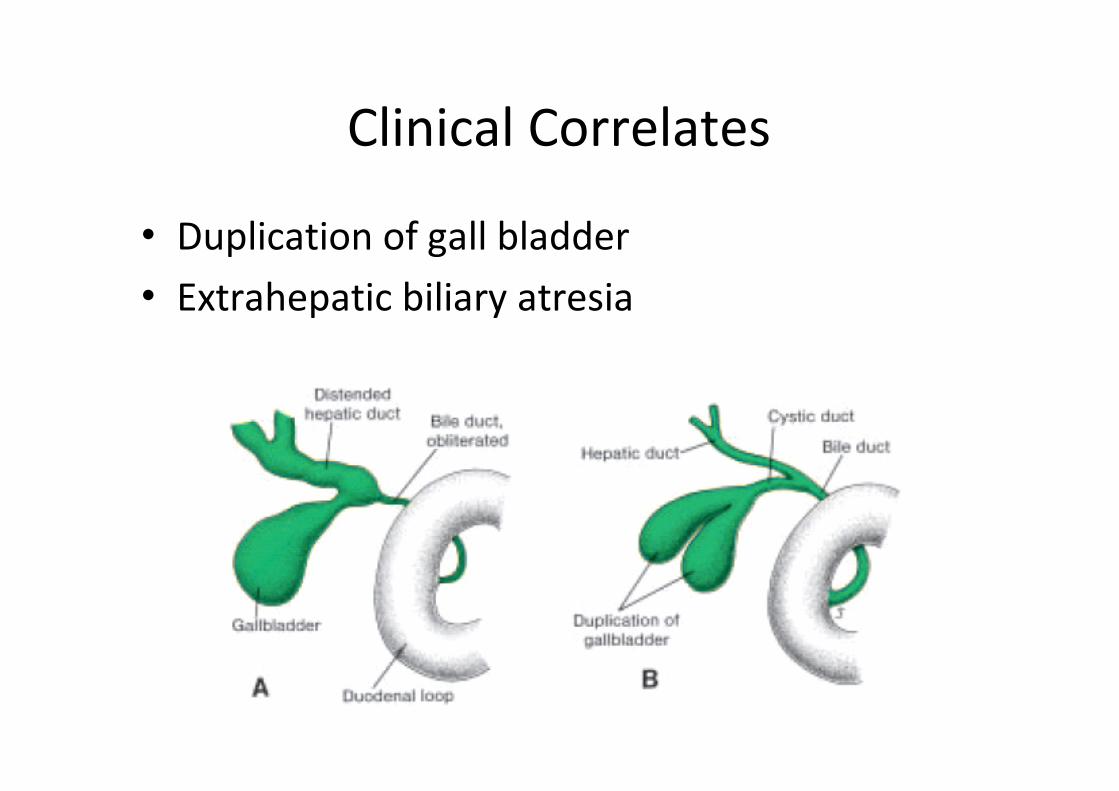
Clinical Correlates
• Duplication of gall bladder• Extrahepatic biliary atresia

Pancreas• Formed by two buds originating from
endodermal lining of duodenum– Dorsal pancreatic bud– Ventral pancreatic bud

Pancreas• Duodenum rotates� ventral pancreatic bud comes to below
and behind the dorsal bud• Ductus pancreaticus major (Wirsungi) : formed by distal part
of dorsal pancreatic duct and entire ventral pancr duct• Ductus pancreaticus minor (Santorini) : proximal part of
dorsal pancr duct

Pancreatic abnormalities
• Annular pancreas• Accessory pancreatic tissue
Midgut
• 5th week : midgut suspended :– Dorsal : dorsal mesentery– Ventral : communicates with the yolksac by
vitteline duct• Rapid elongation of gut and its mesentery �
primary intestinal loop– Cephalic limb : distal part duodenum, jejunum,
part of ileum– Caudal limb: lower part of ileum, caecum,
appendix, ascending colon, 2/3 prox colon
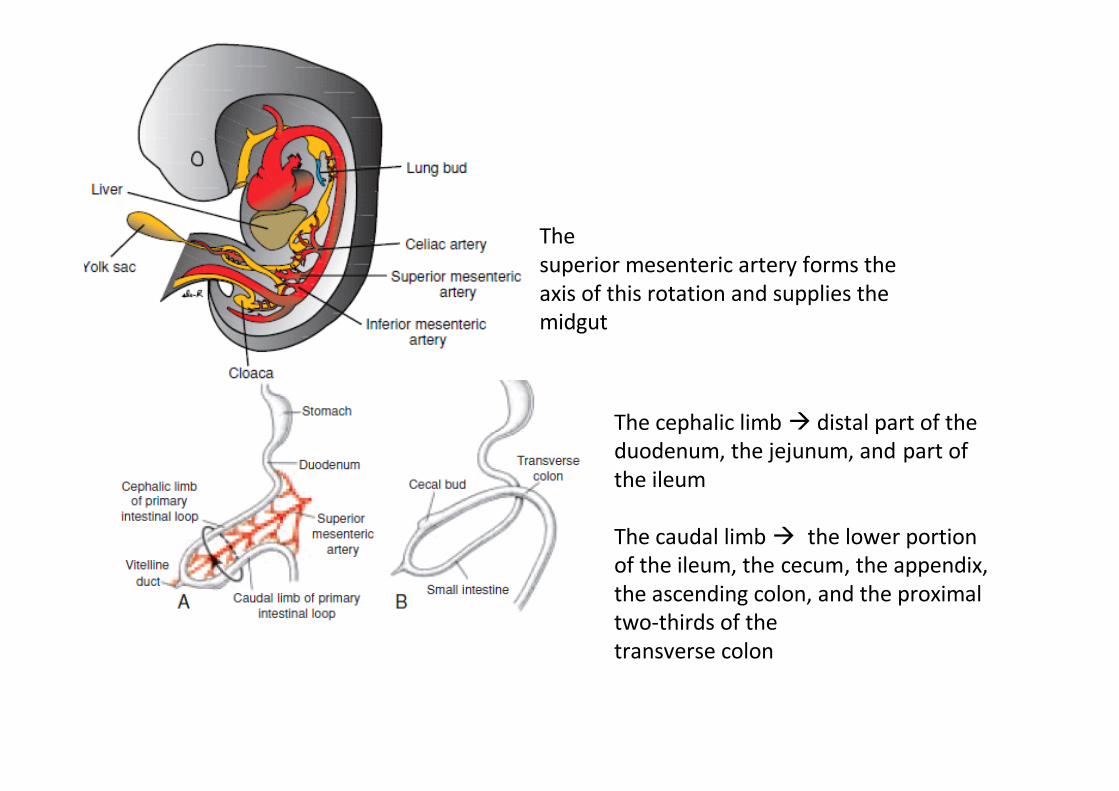
Thesuperior mesenteric artery forms the axis of this rotation and supplies the midgut
The cephalic limb � distal part of the duodenum, the jejunum, and part of the ileum
The caudal limb � the lower portion of the ileum, the cecum, the appendix, the ascending colon, and the proximal two-thirds of thetransverse colon

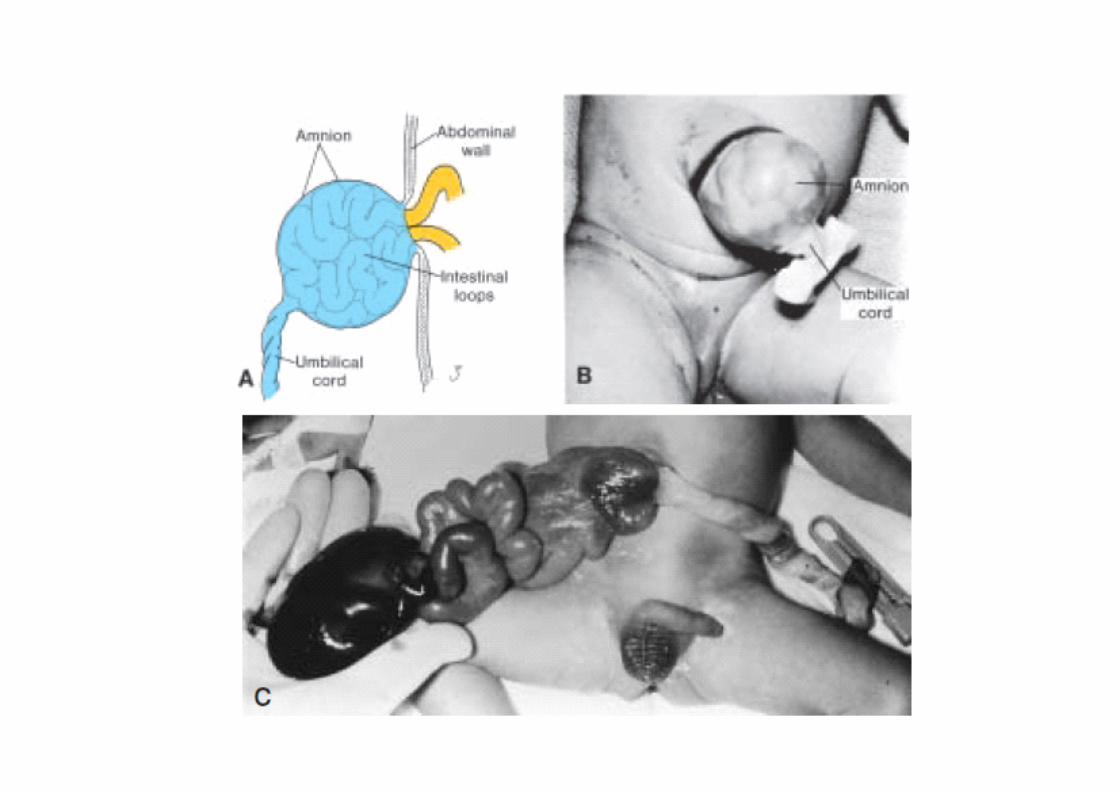
• Physiological Physiological Physiological Physiological herniationherniationherniationherniation ; as a result of rapid elongation and expansion of the liver, during 6th week. The abdominal cavity temporarily becomes too small to contain all the intestinal loops, and they enter the extraembryonic cavity in the umbilical cord
• Rotation of the Rotation of the Rotation of the Rotation of the midgutmidgutmidgutmidgut : primary intestinal loop rotates around an axis formed by superior mesenteric artery, counterclockwise, counterclockwise, counterclockwise, counterclockwise, 270°. (total)
• TTTThe first 90he first 90he first 90he first 90◦◦◦◦ of rotation occurs during of rotation occurs during of rotation occurs during of rotation occurs during herniationherniationherniationherniation

• Coiling Coiling Coiling Coiling phenomenonephenomenonephenomenonephenomenone : cephalic limb• The large intestine likewise lengthens
considerably but does not participate in the coiling phenomenon
• Retraction of herniated loop Retraction of herniated loop Retraction of herniated loop Retraction of herniated loop : during 10th week, jejunum is the first part which reenter the abdominal cavity, lie on the left side, cecal bud is the last

Midgut Abnormalities
• Omphalocele : herniation of abdominal viscera through enlarge umbilical ring
• Gastroschisis : herniation of abdominal content through abd wall directly into amniotic cavity.
• Vitteline duct abN : persistens, cyst, fistula• Gut rotation deffect• Gut atresias/stenosis


The most commonly occurring bowel atresias and stenoses.

Hindgut
• gives rise to the distal third of the transverse colon, the descending colon, the sigmoid, the rectum, and the upper upper upper upper part of the anal canalpart of the anal canalpart of the anal canalpart of the anal canal.
• The terminal portion � the primitive anorectal canal (posterior region of the cloaca)
• Cloaca covered by surface ectoderm,the boundary :cloacal membrane
• Urorectal septum: mesoderm, separates allantois-hindgut, � come closer to cloaca membrane

• The tip of urorectal septum form the perineal body• 7th week :Cloaca mbr ruptures :�Ventral opening : urogenital sinus�Dorsal opening : hindgut
• Proliferation of ectoderm closes the caudal most region of the anal canal
• Recanalization during 9th week

Hindgut AbnormalitiesEx:• Rectoanal atresia and fistula. Cx : posterior cloacal membrane
is short, the opening of the hindgut shifts anteriorly.• Imperforate anus

Selamat belajar ya...…