
The microbiome in primary sclerosing cholangitis: current ...
Upload
deepak-joshiCategory
view
214download
0
CL IN ICAL STUDIES
The impact of inflammatory bowel disease post-liver transplantation forprimary sclerosing cholangitisDeepak Joshi1, Ingvar Bjarnason2, Ajay Belgaumkar1, John O’Grady1, Abid Suddle1, Michael A. Heneghan1,Varuna Aluvihare1, Mohammed Rela1, Nigel Heaton1 and Kosh Agarwal1
1 Institute of Liver Studies, King’s College Hospital London, UK
2 Department of Gastroenterology, King’s College Hospital London, UK
Keywords
inflammatory bowel disease – liver
transplantation – primary sclerosing
cholangitis – thrombosis
Correspondence
Dr Deepak Joshi, Institute of Liver Studies,
King’s College Hospital, Denmark Hill,
London, UK
Tel: +44 203299 2504
Fax: +44 203299 3899
e-mail: [email protected]
Received 19 April 2011
Accepted 19 October 2011
DOI:10.1111/j.1478-3231.2011.02677.x
AbstractBackground: An association between primary sclerosing cholangitis (PSC)and inflammatory bowel disease (IBD) is well recognized. However, the dis-ease course of IBD following liver transplantation (LT) for PSC remains ill-defined. Aims and methods: We aimed to assess the impact of IBD inpatients that had undergone LT for PSC to help identify risk factors for flareand to assess the impact of IBD on graft survival. Results: 110 patientsunderwent LT for PSC (Oct 1990-Aug 2009) at King’s College Hospital. 74(67%) patients had concurrent IBD and 36 had PSC alone prior to trans-plant. 39 patients developed IBD (flare of IBD and de-novo) post transplant.Cumulative risk for IBD at 1-, 2-, 5- and 10-years was 16%, 24%, 38% and72% respectively. Flare of IBD occurred in 33 patients with a mean time toflare of 30 ± 28 months. De-novo IBD occurred in 6 patients (all UC). Meantime to diagnosis was 29 ± 25 months. Multivariate cox-regression analysisidentified active IBD at time of LT as a significant predictor of graft failurepost LT (HR 10, CI 3-39, P = 0.001) and smoking at time of transplantationand subsequent cessation predictive of recurrent IBD post transplantation(HR 17, 2-180, P = 0.02). Conclusion: In conclusion, smoking at time of LTwas predictive of flare of IBD and active IBD at time of transplantation had asignificant effect on graft survival. Medical therapy needs to be maximised inthe pre-LT period. Patients with poorly controlled IBD refractory to medicaltherapy should be considered for colectomy at time of transplantation.
Primary sclerosing cholangitis (PSC) is a chronic chole-static disorder of possible autoimmune aetiology, char-acterized by inflammation and fibrosis of the intra- andextra-hepatic biliary tree (1). There is a strong associa-tion between PSC and inflammatory bowel disease(IBD), with 70–85% of patients with PSC suffering fromIBD. Of these, 70–80% have ulcerative colitis (UC)(2, 3). However, patients with UC and PSC typicallyhave a different manifestation of bowel symptoms fromthose with UC alone, with a predominantly right sidedcolitis, rectal sparing and backwash ileitis more commonand a less aggressive course of disease reported (4). Thetreatment of UC with and without PSC however doesnot differ, but the incidence of colorectal cancer may besomewhat higher in IBD associated with PSC (5).
Liver transplantation (LT) remains the only definitivetreatment for advanced PSC, with 5-year survival ratesof approximately 85% reported (6). Established IBD inpatients with PSC appears to resume a more aggressivecourse, resistant to treatment post-transplantation(7–10). Risk factors for clinical relapse or flare of IBD
activity post-LT include intestinal symptoms at time ofLT and a short interval of IBD before LT (11). Disparityin none or only one HLA-DR or -DQ loci betweendonor and recipient has also been associated with poorerclinical course compared with patients with disparity atboth (65 vs 0%, P = 0.009) (12). The risk of colorectalcancer continues in the post-LT period with some stud-ies describing an accelerated neoplastic course (4, 13).
De novo presentations of IBD following LT can alsooccur. The risk of this is somewhat controversial. Cyto-megalovirus (CMV) donor–recipient mismatch is a spe-cific risk factor, but a confounding factor is that CMVinfection itself can cause a colitis that resembles UC clo-sely (11, 12, 14). Furthermore, different immunosup-pressive agents may have varying effects on thedevelopment of IBD post-transplant. One study sug-gested that patients treated with azathioprine-contain-ing regimens had a longer IBD-free period post-LTcompared with those patients on other treatments,whilst the use of tacrolimus-based immunosuppressionwas an independent predictor of relapse of IBD (15, 16).
Liver International (2011)© 2011 John Wiley & Sons A/S 1
Liver International ISSN 1478-3223

An increased risk of hepatic artery thrombosis post-LTfor PSC has also been reported. This may be related tounderlying bowel pathology given the known associa-tion between IBD and thromboembolism (17).
The aim of this study was to assess the impact of IBDin a series of patients who underwent successful LT forPSC to identify risk factors for flare of IBD and to assessthe impact of IBD on graft survival.
Patients and methods
We identified all adult (>18 years) patients transplantedfor primary sclerosing cholangitis (PSC) in the Instituteof Liver Studies at King’s College Hospital NHS Foun-dation Trust, London, UK, between October 1990 andAugust 2009 from a computerized database. A total of110 patients, 79 men and 31 women with PSC who hadundergone liver transplantation (LT) during this timewere identified. Mean age at time of transplantationwas 47 ± 11 years, and mean follow-up was 79 ± 58months. Seventy-four (67%) patients had concurrentinflammatory bowel disease (IBD) at the time of LT,and 36 (33%) had PSC alone. Patients with autoim-mune hepatitis (AIH) and with AIH/PSC overlap syn-dromes were excluded from analyses. Valid indicationsfor LT included liver synthetic dysfunction, increasingjaundice, recurrent life threatening cholangitis and anon-dominant stricture. Concurrent cholangiocarcino-ma was deemed an absolute contra-indication to LT.
We reviewed the hospital case notes and electronicrecords of these patients. Data capture included patientdemographics, age at transplantation, age at time ofdiagnosis of PSC and IBD, and pharmacological history.A detailed smoking history was also obtained inparticular in those who stopped in the post-transplantperiod. Twenty-two patients were actively smoking atthe time of transplantation, and four patients hadstopped in the preceding 3 months before transplanta-tion. All 22 patients stopped smoking in the immediatepost-transplant period. Four patients resumed smok-ing at a median time of 6.5 months (6–12 months).Severity of IBD was classified according to the Montrealclassification (18).
PSC/IBD pre-liver transplantation
The diagnosis of PSC was established by conventionalmeans and confirmed on explant histology post-LT inall cases. Intra-ductal cholangiocarcinoma was identifiedin seven patients post-transplantation on explant histol-ogy. The diagnosis of IBD was made using a combina-tion of clinical, endoscopic and histological findings.Data regarding duration and extent of disease, mainte-nance therapy, number and severity of exacerbations,courses of corticosteroid therapy, use of azathioprine,need for colectomy and timing of last colonoscopy werecollated. Irrespective of the previous diagnosis of IBD,all patients had undergone colonoscopy and mucosal
biopsy in the previous 6–12 months before LT evalua-tion.
The mean duration of IBD exceeded the duration ofPSC pre-LT (105 ± 137 months vs 25 ± 40 months,P = 0.0001). Sixty-seven patients (91%) had concurrentulcerative colitis (UC) which was extensive, pan-colonicdisease with rectal sparing in 94% of patients. Six (8%)patients had Crohn’s disease, and one (1%) patient hadan indeterminate colitis. At LT, 58 (78%) of patientshad quiescent IBD, 16 (22%) had active IBD. Accordingto the Montreal classification nine patients had mild UC(<4 stools/day, absence of systemic illness and normalinflammatory markers), four had moderate UC (>4stools/day but with minimal signs of systemic toxicityand three patients had severe UC (at least 6 bloodystools/day, heart rate >90 bpm, haemoglobin <10.5g/100 ml).
Monotherapy with 5-aminosalicylates (5-ASA) wasused in 46 (62%) patients, 6 (8%) were on azathioprineand 5 (7%) were on prednisolone. Seventeen (23%)patients were not requiring any medications for thetreatment of their IBD at time of liver transplant. Sixpatients had previously undergone colectomy andpouch formation, and three had undergone a total pan-proctocolectomy. Twenty-eight patients were deemed‘high risk’ for cytomegalovirus (CMV) viraemia (donorpositive, recipient negative) and received empirical oralvalganciclovir therapy for 3 months. One patient devel-oped CMV colitis (donor negative, recipient positive)and responded successfully to medical therapy.
PSC/IBD post-liver transplantation
All patients underwent Roux-en-Y hepaticojejunostomyat the time of LT. Post-LT treatment was protocol dri-ven and standardized throughout this study period.Dual maintenance immunosuppression consisted ofeither ciclosporin 10 mg/kg/day or tacrolimus 0.1 mg/kg/day in two divided doses in combination with corti-costeroid therapy. Doses were adjusted to maintaintrough blood levels of tacrolimus (8–10 ng/ml) andciclosporin (100–250 ng/ml) within the first month fol-lowing LT. Methylprednisolone was initiated at 16 mgdaily intravenously until patients were able to take oralmedications with prednisolone then commenced at adose of 20 mg daily and then reduced by 5 mg everyweek after 14 days to a maintenance dose of 5–10 mgdaily over a period of 3 months.
The first episode of acute cellular rejection (ACR)(moderate or severe) was treated with a 3-day course ofintravenous methylprednisolone 1 g daily. Mycopheno-late mofetil (MMF) was introduced following the sec-ond episode of ACR. All patients received antifungalprophylaxis with fluconazole 50 mg daily for 3 monthsor until the dose of prednisolone was less than 10 mgdaily. Data were collected on the immunosuppressionregimen at the time of discharge, at 1-year post-LT, timeof presentation of post-LT IBD and at the time of last
Liver International (2011)© 2011 John Wiley & Sons A/S2
Inflammatory bowel disease post-liver transplantation Joshi et al.

acquisition of data (August 2009). Recipients who wereseronegative for CMV and received a graft from a sero-positive donor were deemed ‘high risk’ for CMV vira-emia. CMV viraemia (polymerase chain reaction) wastested for weekly in the first post-transplant month andregularly thereafter for the first 3-month post-trans-plant. Following this, CMV infection was tested for rou-tinely if patients were admitted to hospital or if patientshad any clinical suspicion of CMV infection.
Inflammatory bowel disease medications were fre-quently discontinued post-LT. A clinical flare up of IBDor diagnosis of de novo IBD post-LT was made on clini-cal, endoscopic and histological findings. Biopsies werehistologically and immunohistochemically examined forCMV. Gastrointestinal infections including clostridiumdifficile toxin were excluded in all patients.
Statistical analysis
Quantitative variables were expressed as the mean± standard deviation. For continuous variables, theStudent’s t-test or Mann–Whitney U-test was used.IBD-free and graft survival was determined by con-structing Kaplan–Meier curves. Differences in survivalbetween the subgroups of patients were assessed by Log-rank test. Comparisons were made between patientswith PSC/IBD and PSC alone. Survival analysis was per-formed using Cox regression modelling. To investigatethe influence of possible risk factors, variables were con-sidered in univariate Cox proportional hazards model.Variables with a P-value <0.1 were then entered in amultivariate Cox proportional hazard model were per-formed. A two-tail P-value <0.05 was considered toindicate statistical significance. Analysis was performedusing SPSS for Windows 17 (SPSS, Chicago, IL, USA).
Results
Patient cohort
Patient characteristics between the two groups weresimilar (Table 1). The commonest indications for livertransplantation (LT) included synthetic liver dysfunc-tion (mean MELD 15 ± 6) increasing jaundice, recur-rent cholangitis and a non-dominant biliary stricture.Mean time to recurrence of primary sclerosing cholangi-tis (PSC) (diagnosis based on histology or radiologicalappearances consistent with recurrence and guidedby the Mayo Clinic diagnostic criteria) followingliver transplant was similar between the two groups(59 ± 47 months, PSC vs 73 ± 52 months, PSC/IBD,P = 0.2).
Inflammatory bowel disease post-liver transplantation
Diarrhoea was a common occurrence post-LT andtherefore all patients had infectious aetiologies, includ-ing cytomegalovirus (CMV), actively investigated and
excluded. All patients underwent endoscopic evaluationand biopsy to confirm the diagnosis of inflammatorybowel disease (IBD). Thirty-nine patients (35%) devel-oped IBD (flare and de novo cases) post-LT. Cumulativerisk for IBD for 1-, 2-, 5- and 10-year post-LT was 16,24, 38 and 72% respectively.
Subgroup with IBD pre-liver transplantation
Flare of IBD occurred in 33 patients (10 women). Inall, 3 had a mild flare, 10 moderate and 20 a severeflare according to the Montreal classification. Meantime to flare was 30 ± 28 months. The cumulativerisk for flare of IBD after 1-, 2-, 5- and 10 years was18, 35, 60 and 98% respectively (Fig. 1). Thirteenpatients required an increase in their 5-ASA onlywhich resulted in remission, whereas eight patientsrequired an increase in corticosteroid dose (20–40 mgonce daily). Two patients required the addition ofazathioprine and two patients required infliximab.Two patients of six who had undergone a colectomyand pouch formation [diagnosed with ulcerative coli-tis (UC)] developed histologically proven pouchitiswhich required the combination of topical 5-ASApreparations, probiotics and antibiotics. Six patientswent on to have a colectomy because of failed medi-cal therapy. In total, five cases of colorectal malig-nancy were diagnosed in the post-transplant period.Documented follow-up with annual colonoscopy wasonly available in 54 patients (72%) of patients withevidence of IBD pre-LT as they were followed up atother centres.
Subgroup without IBD pre-liver transplantation
De novo IBD occurred in 6 of 36 (17%) patients. Allsix patients (four women) were evaluated endo-scopically prior to transplantation, but with negativehistological findings for IBD. All six patients werediagnosed with UC and received a tacrolimus-based
Table 1. Patient characteristics pre-liver transplantation
PSC/IBD PSC
N (%) 74 (67) 36 (33)Mean age, years (±SD)* 47 ± 11 48 ± 10Mean duration of PSC pre-LT, months* 47 ± 11 44 ± 50Indications for LT (%)Synthetic liver dysfunction 54 56Increasing jaundice 25 22Recurrent cholangitis 15 15Non-dominant biliary stricture 6 7
MELD* 15 ± 5 15 ± 6Child Pugh score (A/B/C) 10/42/22 6/17/13
*No statistical difference between the two groups.
IBD, inflammatory bowel disease; LT, liver transplantation; MELD, model
for end stage liver disease; PSC, primary sclerosing cholangitis.
Liver International (2011)© 2011 John Wiley & Sons A/S 3
Joshi et al. Inflammatory bowel disease post-liver transplantation

immunosuppressive regimen. Mean time to diagnosisof de novo disease was 29 ± 25 months after trans-plantation. The cumulative risk for de novo IBD after1-, 2-, 5- and 10 years was 7, 16, 22 and 29% respec-tively (Fig. 1). All patients were commenced upon5-ASA in conjunction with an increase in predniso-lone dose (40 mg once daily, reducing by 5 mg every7 days). One patient required the addition of azathio-prine. All patients achieved remission. One patientrequired colectomy for the development of high-gradecolonic dysplasia.
Risk factors for inflammatory bowel disease
From the combined group of de novo and flare of IBD,univariate analysis demonstrated older age, active smok-ing statusand activity of IBD pre-LT as significant riskfactors for exacerbation of IBD post-transplantation. Ina multivariate model, active smoking at the time of liver
transplant was the only significant risk factor for flare ofIBD post-transplantation (Table 2).
Patient and graft survival
Patient survival rates between the PSC/IBD and PSCgroups were similar at 1-, 5- and 10-years (91, 87, 72%vs 96, 88, 75%, Log-Rank score, P = 0.6). Nine (30%)patients died secondary to malignancy (seven from cho-langiocarcinoma) and four patients died (19%) second-ary to sepsis and multiorgan failure. In a multivariablemodel, only age at time of LT was significant predictorof patient survival (HR 1.5, 1.01–1.1, P = 0.02). ActiveIBD at time of LT was not a predictor of patient survival.
Overall, graft survival rates were also similar betweenthe two groups at 1-, 5- and 10-years (91, 87, 72% vs89, 83, 74%, Log-Rank score, P = 0.8) although anincreased incidence (P = 0.04) of hepatic artery throm-bosis (six cases) was noted in the PSC/IBD group all of
Fig. 1. Cumulative risk for flare and de novo inflammatory bowel disease post-liver transplantation for primary sclerosing cholangitis.
Table 2. Risk factors for inflammatory bowel disease after liver transplantation for primary sclerosing cholangitis
Variable Hazard ratio Univariate 95% CI P-value Hazard ratio Multivariate 95% CI P-value
All patients (n = 110)Age 1.05 1.01–1.07 0.01 1 0.9–1.03 NSSmoker at time of LT 6.8 1.3–35.6 0.02 17 2–180 0.02IBD duration pre-LT 1.2 0.9–1.001 0.09 1 0.9–1.00 NSActivity of IBD pre-LT 4 1.3–10.5 0.02 3 0.9–13 0.07Extent of IBD 2.3 0.5–10.2 0.3CMV status 0.8 0.4–1.7 0.5Tacrolimus-based IS 0.5 0.2–1.1 0.08 0.3 0.04–2.4 NS
CMV, cytomegalovirus; IBD, inflammatory bowel disease; IS, immunosuppression; LT, liver transplantation.
Liver International (2011)© 2011 John Wiley & Sons A/S4
Inflammatory bowel disease post-liver transplantation Joshi et al.
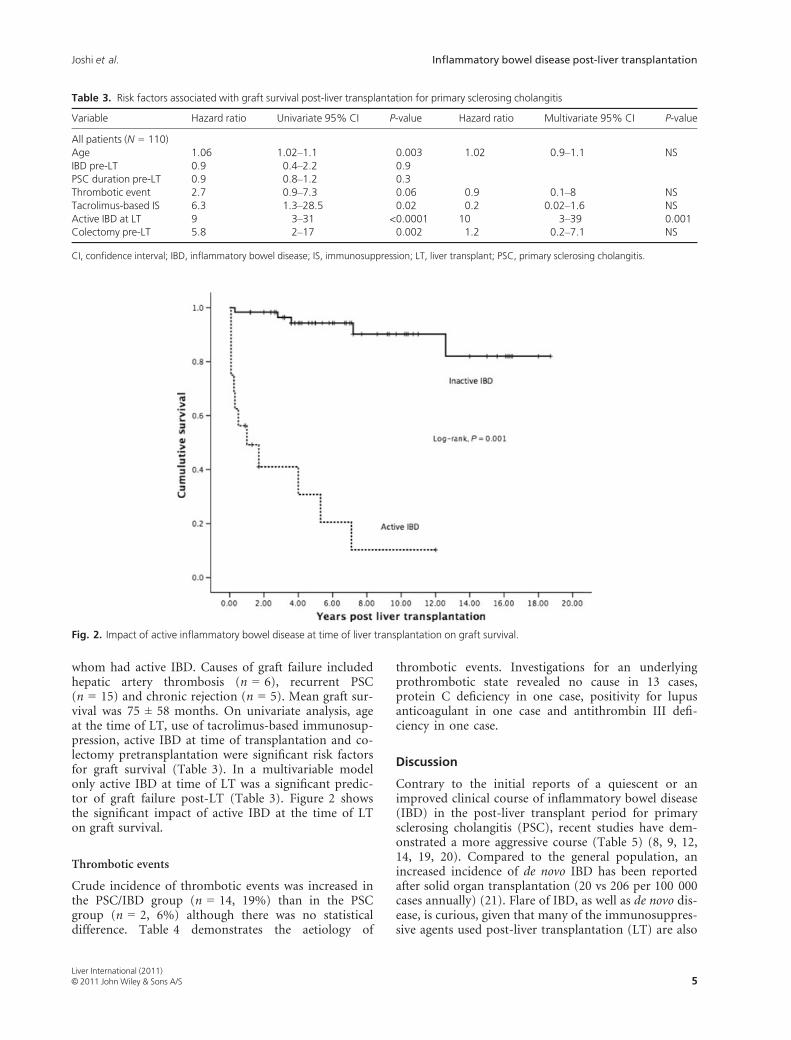
whom had active IBD. Causes of graft failure includedhepatic artery thrombosis (n = 6), recurrent PSC(n = 15) and chronic rejection (n = 5). Mean graft sur-vival was 75 ± 58 months. On univariate analysis, ageat the time of LT, use of tacrolimus-based immunosup-pression, active IBD at time of transplantation and co-lectomy pretransplantation were significant risk factorsfor graft survival (Table 3). In a multivariable modelonly active IBD at time of LT was a significant predic-tor of graft failure post-LT (Table 3). Figure 2 showsthe significant impact of active IBD at the time of LTon graft survival.
Thrombotic events
Crude incidence of thrombotic events was increased inthe PSC/IBD group (n = 14, 19%) than in the PSCgroup (n = 2, 6%) although there was no statisticaldifference. Table 4 demonstrates the aetiology of
thrombotic events. Investigations for an underlyingprothrombotic state revealed no cause in 13 cases,protein C deficiency in one case, positivity for lupusanticoagulant in one case and antithrombin III defi-ciency in one case.
Discussion
Contrary to the initial reports of a quiescent or animproved clinical course of inflammatory bowel disease(IBD) in the post-liver transplant period for primarysclerosing cholangitis (PSC), recent studies have dem-onstrated a more aggressive course (Table 5) (8, 9, 12,14, 19, 20). Compared to the general population, anincreased incidence of de novo IBD has been reportedafter solid organ transplantation (20 vs 206 per 100 000cases annually) (21). Flare of IBD, as well as de novo dis-ease, is curious, given that many of the immunosuppres-sive agents used post-liver transplantation (LT) are also
Fig. 2. Impact of active inflammatory bowel disease at time of liver transplantation on graft survival.
Table 3. Risk factors associated with graft survival post-liver transplantation for primary sclerosing cholangitis
Variable Hazard ratio Univariate 95% CI P-value Hazard ratio Multivariate 95% CI P-value
All patients (N = 110)Age 1.06 1.02–1.1 0.003 1.02 0.9–1.1 NSIBD pre-LT 0.9 0.4–2.2 0.9PSC duration pre-LT 0.9 0.8–1.2 0.3Thrombotic event 2.7 0.9–7.3 0.06 0.9 0.1–8 NSTacrolimus-based IS 6.3 1.3–28.5 0.02 0.2 0.02–1.6 NSActive IBD at LT 9 3–31 <0.0001 10 3–39 0.001Colectomy pre-LT 5.8 2–17 0.002 1.2 0.2–7.1 NS
CI, confidence interval; IBD, inflammatory bowel disease; IS, immunosuppression; LT, liver transplant; PSC, primary sclerosing cholangitis.
Liver International (2011)© 2011 John Wiley & Sons A/S 5
Joshi et al. Inflammatory bowel disease post-liver transplantation

used to help achieve remission in the non-transplantsetting (22, 23).
Effect of liver transplantation on the course ofinflammatory bowel disease
Thirty-nine patients experienced IBD post-LT; of these,six were de novo presentations. The cumulative risk forexperiencing IBD for 1-, 2-, 5- and 10-year post-trans-plantation was 16, 24, 38 and 72% respectively and iscomparable to previously published studies (15, 16).Our data also demonstrated that within 5 years, nearlytwo-thirds our patients (60%) with known IBD suffereda flare of their disease. The majority of patients had their5-ASA based medication stopped post-transplantation,with the expectation that the immunosuppressive regi-mens would continue to maintain IBD remission. How-ever, others have suggested that empirical 5-ASAtreatment decreased the risk of IBD post-LT for patients
with PSC (Hazard ratio 4.8, P = 0.04) (11). All ourpatients continued on a maintenance dose of steroidSmoking status at time of LT was identified as a risk fac-tor for flare of IBD. This might be explained by theknown protective effect of smoking, particularly inulcerative colitis (UC). Patients who discontinue smok-ing in the post-transplant period may therefore repre-sent a higher risk group for IBD.
‘High-risk’ cytomegalovirus (CMV) mismatch(donor positive, recipient negative) has been proposedpreviously as a risk factor for de novo IBD (11). How-ever, it is important to note that in this study, onlyCMV-pp65 antigenemia was utilized and not PCR, aswell as not performing routine CMV screening. Ourstudy failed to demonstrate high-risk CMV mismatch arisk factor for recurrent IBD post-transplantationalthough those at risk of CMV disease were given pro-phylaxis. The only case of CMV viraemia occurred in apatient who was not classified as high risk (both donorand recipient negative) and was successfully treated withintravenous ganciclovir.
We identified six cases of de novo IBD all confirmedendoscopically and histologically as UC. It remainsunclear as to why IBD should occur in the post-trans-plant period. One suggestion is that patients with anautoimmune background would develop IBD evenwithout transplantation, but the validity of this hypoth-esis has been questioned (26). Alternatively the replace-ment of recipient haematopoiesis with donor-derived
Table 4. Thrombosis events in patients with inflammatory boweldisease pre-liver transplantation
Thrombotic events PSC/IBD (n, %) PSC (n, %)
Pulmonary embolus 4 (29) 2 (100)Deep vein thrombosis 2 (14) –Hepatic artery thrombosis 6 (43) –Portal vein thrombosis 1 (7) –Mesenteric thrombosis 1 (7) –
Table 5. Summary of studies investigating course of inflammatory bowel disease post-liver transplantation
References AetiologyNumber ofpatients Immunosuppression IBD activity post-LT
Gavaler et al. (19) PSC 23 CIC + CS long-term CStherapy
Improvement in 82% of cases
Papatheoridis et al. (10) PSC 30 CIC/TAC + AZA CSwithdrawal
Deterioration in 50% of cases
Befeler et al. (20) PSC 23 CS/TAC ± AZA long-termCS therapy
74% had quiescent disease,26% mild flares
Haagsma et al. (15) PSC/AIH 78 CIC/TAC ± AZA ± CS ± MMF,long-term CStherapy
Cumulative risk for IBD, 20, 28,39, 39% at 1, 3, 5, 10 years;cumulative risk of de novo IBD, 0, 4,11, 14% at 1, 3, 5, 10 years
Van de Vrie et al. (13) PSC 18 CIC/TAC ± AZA CSwithdrawal
No change in disease activity in 28%
Ho et al. (9) PSC 20 CIC/TAC ± AZA CSwithdrawal
Increased no. of relapses and higherCS requirement
Verdonk et al. (11) PSC/AIH 91 CIC/TAC ± CS ± MMF ± AZA± Rapamycin
Cumulative risk for IBD, 15, 30,39, 54% at 1, 3, 5, 10 years;cumulative risk of recurrent IBD,29, 51, 63, 72% at 1, 3, 5, 10 years;cumulative risk for de novo IBD, 0, 5,10, 30% at 1, 3, 5, 10 years
Cholangitas et al. (12) PSC 69 CIC/TAC ± AZA ± MMFCS withdrawal
Deterioration in 52% of cases; 49% ofcases showed no change
AIH, autoimmune hepatitis; AZA, azathioprine; CIC, ciclosporin; CS, corticosteroid; IBD, inflammatory bowel disease; LT, liver transplantation; MMF,
mycophenolate mofetil; PSC, primary sclerosing cholangitis; TAC, tacrolimus.
Liver International (2011)© 2011 John Wiley & Sons A/S6
Inflammatory bowel disease post-liver transplantation Joshi et al.

cells could lead to immune cells developing tolerancetowards the liver graft but not to the intestinal luminalantigens post-transplant (27).
Effect of inflammatory bowel disease on patient and graftsurvival
The increased risk of colorectal malignancy is well rec-ognized in IBD in particular those with PSC comparedwith IBD patients without PSC, with duration andextent of disease being the most important risk factors(28–30). We found five cases in the post-transplant per-iod. In the context of LT, a patient’s life span is clearlyincreased and therefore increases the risk of colorectalcancer in a time dependent manner (31). Immunosup-pression plays an important role in carcinogenesis in thepost-transplant period, but LT per se however confersno additional risk for the development of colorectalmalignancy (6). The decreased use of 5-ASAs in patientswith PSC/IBD in the post-LT period may also add tothe increased risk of colorectal malignancy. Our studyprovides an insight into the natural history of PSC fol-lowing LT with regard to the impact of IBD. Active IBDat the time of transplantation was a significant predictorof graft failure and on univariate analysis colectomypre-LT was associated with improved graft survival inthe post-transplant period. In our cohort, this wouldmean undertaking 16 colectomies at the time of LT.This management step would have potentially avoidedsix cases of hepatic artery thrombosis and undoubtedlyimproved graft survival. An intact colon is a recognized
risk factor for recurrent PSC post-transplant and a co-lectomy pre-/peri-LT has been shown to confer a pro-tective effect against recurrent PSC due to theinterruption of lymphocytes via the enterohepatic circu-lation, particularly from the small bowel (32).
Seven cases (6%) of cholangiocarcinoma weredetected post-LT all of which were identified on explanthistology only. All these patients had normal tumourmarkers and normal axial imaging pre-LT. Although therate of cholangiocarcinoma seems high, we feel it mayhave been simply representative of the sensitivity of thepre-LT imaging modalities available across the studyperiod.
Thrombotic events were also increased in patientswith concurrent IBD with no identifiable cause for theprothrombotic state in the majority of cases. The risk ofthromboembolism (TE) is increased in IBD and appearsto be unique in comparison to other chronic inflamma-tory conditions (17). The risk of TE is increased furtherduring the time of a flare with an increased likelihood ofrecurrent TE even after discontinuation of anticoagulanttherapy (13, 17, 33, 34).
In conclusion, we found that active smoking at thetime of LT was predictive of flare of IBD post-LT forPSC. Calcineurin inhibitors did not help maintainremission of IBD, the use of tacrolimus in particularand mycophenolate mofetil associated with an increasedtrend towards recurrent IBD. At present, further studiesare required to assess the role of immunosuppression inthe pathogenesis of recurrent and de novo IBD post-transplantation. Poorly controlled IBD appears to play a
Fig. 3. Influence of immunosuppression (IS) on cumulative risk of inflammatory bowel disease post-liver transplantation for primary scleros-ing cholangitis.
Liver International (2011)© 2011 John Wiley & Sons A/S 7
Joshi et al. Inflammatory bowel disease post-liver transplantation

detrimental role in patients post-LT for PSC withincreased rates of thrombosis and reduced graft survival.Medical therapy should therefore be maximized toinduce remission of IBD prior to LT added to the contin-uation of 5-ASA medications post-LT. Patients withrefractory IBD to medical therapy undergoing assessmentfor LT for PSC should be considered for colectomy attime of transplantation.
References
1. Gow PJ, Chapman RW. Liver transplantation for primarysclerosing cholangitis. Liver 2000; 20: 97–103.
2. Tischendorf JJ, Hecker H, Kruger M, Manns MP, MeierPN. Characterization, outcome, and prognosis in 273patients with primary sclerosing cholangitis: a single cen-ter study. Am J Gastroenterol 2007; 102: 107–14.
3. Broome U, Olsson R, Loof L, et al. Natural history andprognostic factors in 305 Swedish patients with primarysclerosing cholangitis. Gut 1996; 38: 610–5.
4. Loftus EV Jr, Harewood GC, Loftus CG, et al. PSC-IBD: aunique form of inflammatory bowel disease associatedwith primary sclerosing cholangitis. Gut 2005; 54: 91–6.
5. Soetikno RM, Lin OS, Heidenreich PA, Young HS, Black-stone MO. Increased risk of colorectal neoplasia inpatients with primary sclerosing cholangitis and ulcerativecolitis: a meta-analysis. Gastrointest Endosc 2002; 56: 48–54.
6. Graziadei IW, Wiesner RH, Marotta PJ, et al. Long-termresults of patients undergoing liver transplantation for pri-mary sclerosing cholangitis. Hepatology 1999; 30: 1121–7.
7. Dvorchik I, Subotin M, Demetris AJ, et al. Effect of livertransplantation on inflammatory bowel disease in patientswith primary sclerosing cholangitis. Hepatology 2002; 35:380–4.
8. Miki C, Harrison JD, Gunson BK, et al. Inflammatorybowel disease in primary sclerosing cholangitis: an analysisof patients undergoing liver transplantation. Br J Surg1995; 82: 1114–7.
9. Ho GT, Seddon AJ, Therapondos G, Satsangi J, Hayes PC.The clinical course of ulcerative colitis after orthotopicliver transplantation for primary sclerosing cholangitis:further appraisal of immunosuppression post transplanta-tion. Eur J Gastroenterol Hepatol 2005; 17: 1379–85.
10. Papatheodoridis GV, Hamilton M, Mistry PK, et al. Ulcer-ative colitis has an aggressive course after orthotopic livertransplantation for primary sclerosing cholangitis. Gut1998; 43: 639–44.
11. Verdonk RC, Dijkstra G, Haagsma EB, et al. Inflammatorybowel disease after liver transplantation: risk factors forrecurrence and de novo disease. Am J Transplant 2006; 6:1422–9.
12. Cholongitas E, Papatheodoridis GV, Zappoli P, et al.Combined HLA-DR and -DQ disparity is associated witha stable course of ulcerative colitis after liver transplanta-tion for primary sclerosing cholangitis. Liver Transpl 2007;13: 552–7.
13. van de Vrie W, de Man RA, van Buuren HR, et al. Inflam-matory bowel disease and liver transplantation for primarysclerosing cholangitis. Eur J Gastroenterol Hepatol 2003;15: 657–63.
14. Cholongitas E, Shusang V, Papatheodoridis GV, et al.Risk factors for recurrence of primary sclerosing cholan-gitis after liver transplantation. Liver Transpl 2008; 14:138–43.
15. Haagsma EB, van den Berg AP, Kleibeuker JH, Slooff MJ,Dijkstra G. Inflammatory bowel disease after liver trans-plantation: the effect of different immunosuppressive regi-mens. Aliment Pharmacol Ther 2003; 18: 33–44.
16. Verdonk RC, Haagsma EB, Jonker MR, et al. Effects ofdifferent immunosuppressive regimens on regulatoryT-cells in noninflamed colon of liver transplant recipients.Inflamm Bowel Dis 2007; 13: 703–9.
17. Miehsler W, Reinisch W, Valic E, et al. Is inflammatorybowel disease an independent and disease specific risk fac-tor for thromboembolism? Gut 2004; 53: 542–8.
18. Satsangi J, Silverberg MS, Vermeire S, Colombel JF. TheMontreal classification of inflammatory bowel disease:controversies, consensus, and implications. Gut 2006; 55:749–53.
19. Gavaler JS, Delemos B, Belle SH, et al. Ulcerative colitisdisease activity as subjectively assessed by patient-com-pleted questionnaires following orthotopic liver transplan-tation for sclerosing cholangitis. Dig Dis Sci 1991; 36:321–8.
20. Befeler AS, Lissoos TW, Schiano TD, et al. Clinical courseand management of inflammatory bowel disease after livertransplantation. Transplantation 1998; 65: 393–6.
21. Riley TR, Schoen RE, Lee RG, Rakela J. A case series oftransplant recipients who despite immunosuppressiondeveloped inflammatory bowel disease. Am J Gastroenterol1997; 92: 279–82.
22. Carter MJ, Lobo AJ, Travis SP. Guidelines for the manage-ment of inflammatory bowel disease in adults. Gut 2004;53(Suppl. 5): V1–16.
23. Saibeni S, Virgilio T, D’Inca R, et al. The use of thiopu-rines for the treatment of inflammatory bowel diseases inclinical practice. Dig Liver Dis 2008; 40: 814–20.
24. Shaked A, Colonna JO, Goldstein L, Busuttil RW. Theinterrelation between sclerosing cholangitis and ulcerativecolitis in patients undergoing liver transplantation. AnnSurg 1992; 215: 598–603.
25. Lugering A, Lebiedz P, Koch S, Kucharzik T. Apoptosis asa therapeutic tool in IBD? Ann N Y Acad Sci 2006; 1072:62–77.
26. Worns MA, Lohse AW, Neurath MF, et al. Five cases of denovo inflammatory bowel disease after orthotopic livertransplantation. Am J Gastroenterol 2006; 101: 1931–7.
27. Collins RH Jr, Sackler M, Pitcher CJ, et al. Immune recon-stitution with donor-derived memory/effector T cells afterorthotopic liver transplantation. Exp Hematol 1997; 25:147–59.
28. Greenstein AJ, Sachar DB, Smith H, et al. Cancer in uni-versal and left-sided ulcerative colitis: factors determiningrisk. Gastroenterology 1979; 77: 290–4.
29. Katzka I, Brody RS, Morris E, Katz S. Assessment ofcolorectal cancer risk in patients with ulcerative colitis:experience from a private practice. Gastroenterology 1983;85: 22–9.
30. Sokol H, Cosnes J, Chazouilleres O, et al. Disease activityand cancer risk in inflammatory bowel disease associatedwith primary sclerosing cholangitis. World J Gastroenterol2008; 14: 3497–503.
Liver International (2011)© 2011 John Wiley & Sons A/S8
Inflammatory bowel disease post-liver transplantation Joshi et al.

31. Ekbom A, Helmick C, Zack M, Adami HO. Increased riskof large-bowel cancer in Crohn’s disease with colonicinvolvement. Lancet 1990; 336: 357–9.
32. Alabraba E, Nightingale P, Gunson B, et al. A re-evalua-tion of the risk factors for the recurrence of primary scle-rosing cholangitis in liver allografts. Liver Transpl 2009;15: 330–40.
33. Grainge MJ, West J, Card TR. Venous thromboembolismduring active disease and remission in inflammatory boweldisease: a cohort study. Lancet 2010; 375: 657–63.
34. Novacek G, Weltermann A, Sobala A, et al. Inflammatorybowel disease is a risk factor for recurrent venous throm-boembolism. Gastroenterology 2010; 139: 779–87.
Liver International (2011)© 2011 John Wiley & Sons A/S 9
Joshi et al. Inflammatory bowel disease post-liver transplantation


















