
The Impact of Dental Devices on Neurostimulators
4
The Impact of Dental Devices on Neurostimulators Steven Roberts, DDS,* John R. Vender, MD, † Mark S. Causey, BS, ‡ Jefferson R. Roberts, MD, § Robert J. Loushine, DDS,* Walter J. Morris, DMD, k and Stephen W. Looney, PhD { Abstract Spinal cord stimulation has been a therapeutic option for chronic pain for over 40 years. The neurostimulator (NS) is a device consisting of three primary components: an elec- trode array configured either as a paddle or wire; an implantable pulse generator (IPG) consisting of a minicom- puter, a transceiver/antenna, an electrical generator, and a battery; and insulated wiring connecting the electrode to the IPG. The electrode array can be implanted into the epidural space overlying the dorsal spinal cord or along a peripheral nerve. The device generates pulsed electrical signals that stimulate the underlying dorsal columns of the spinal cord resulting in the perception of paresthesia by the patient. When overlapped with painful areas, the paresthesia can help decrease the patient’s level of pain. The increased applications and indications for this technology enhance the likelihood that the NS patient will be seen in the dental practice. Therefore, the purpose of this study was to investigate whether electromagnetic interference of the NS occurred during the operation of the apex locator, the electric pulp tester (EPT), or the electro- cautery unit. An NS was implanted into the epidural space of a human cadaver. The dental devices were used intra- orally, and the implant’s circuitry was tested after each trial. Two apex locators, two EPTs, and one electrocautery unit were tested. Seventy trials were used by each dental device on each tissue. Using the exact binomial method of determining confidence intervals, the probability of damage to the NS by any of the devices was negligible. (J Endod 2009;35:422–425) Key Words Apex locator, electric pulp tester, electrocautery, neuro- stimulator T he development and advancement of biotechnological devices have improved the quality of life for many medically compromised patients. The function of these devices, however, may be adversely affected by extraneous electromagnetic energy fields. With the introduction of cardiac pacemakers in 1958, patients were advised to avoid certain environments considered potentially hazardous to the implant’s func- tion (1, 2). Dental devices emitting electromagnetic energy similarly represented potential hazards to the pacemaker patients (3–6). A 1991 in vivo evaluation of the impact of the air scaler, ultrasonic curette, electric pulp tester, and electrotome on the function of artificial pacemakers concluded that, although none of the devices caused an irreg- ularity in pacemaker function, a risk remained for patients with older pacemakers (5). Results of in vitro monitoring of atrial and ventricular pacemaker output and electro- cardiographic activity also indicated that the electric pulp tester, dental handpieces, radiography, and sonic scalers did not interfere with pacemaker function, although certain electrosurgical and ultrasonic instruments may produce deleterious effects (6). Several years after cardiac pacemakers were introduced, cochlear stimulators were successfully implanted in deaf patients. In 2002, Roberts et al (7) showed on cadavers that although the electric pulp tester (EPT), apex locator, electrocautery unit, and panoramic radiograph machine appeared safe, the electrosurgery unit at higher settings could potentially damage the cochlear implant. In 1967, Dr C. Norman Shealy, a neurosurgeon, implanted the first neuroaugmen- tive device for the relief of intractable pain in a terminally ill cancer patient (8). By 1970, six patients had undergone this treatment by Shealy et al. Since that time, neurostimu- lator (NS) technology has accelerated with respect to equipment design, flexibility, and reliability (Fig. 1). Although initially believed to reduce pain via a gate mechanism, newer data suggest that the analgesic effect produced by NSs is mediated by a release of endogenous opioids within the spinal cord parenchyma. This can explain the prolonged effect after the device has been turned off. NSs are now widely used for spinal axial pain as well as ischemic limb pain, certain anginal pain syndromes, chronic diabetic neuropathic pain, sympathetically mediated pain, and failed back surgery syndrome (9–11). Recent literature reveals both a clinical and a cost-benefit advantage of spinal stimulation over reoperative spinal fusion (12). With improved technology and greater experience, the use of NSs has become safer and more effective. Therefore, the dental practitioner can expect to see an increasing number of patients with these devices. No study exists on the effect of dental equipment on the integrity of the NS. As with pacemaker or cochlear implant patients, the electromagnetic field created by dental instruments may present a potential hazard to NS patients. Damage to the NS could potentially not only irreparably damage the implant but would also necessitate a surgical procedure to replace it. The purpose of this study was to investigate the effects of electromagnetic interference on an NS during the operation of the EPT, apex locator, and electrocautery unit. Materials and Methods A human cadaver was obtained from the Department of Anatomy and Cell Biology of the Medical College of Georgia. A vertical midline linear incision was created over the posterior spinous processes at T12 and L1. Subcutaneous tissues were dissected to the level of the lumbodorsal fascia. By using a loss-of-resistance technique, the epidural space was accessed with a #14-G Tuohy needle. An epidural dissecting wire was then passed into the epidural space (Fig. 2A). This was subsequently removed, and an From the *Department of Endodontics, School of Dentistry, Medical College of Georgia, Augusta, GA; † Department of Neurosurgery, School of Medicine, Medical College of Georgia, Augusta, GA; ‡ School of Dentistry, Medical College of Georgia, Augusta, GA; § Department of Internal Medicine, Walter Reed Army Hospital, Washington, DC; k Department of Prosthodon- tics, School of Dentistry, Medical College of Georgia, Augusta, GA; and { Department Biostatistics, Medical College of Georgia, Augusta, GA. Address requests for reprints to Dr Steven Roberts, Depart- ment of Endodontics, School of Dentistry, Medical College of Georgia, Augusta, GA 30912-1129. E-mail address: [email protected]. 0099-2399/$0 - see front matter Published by Elsevier, Inc. on behalf of American Associa- tion of Endodontists. doi:10.1016/j.joen.2008.12.005 Case Report/Clinical Techniques 422 Roberts et al. JOE — Volume 35, Number 3, March 2009
-
Upload
steven-roberts -
Category
Documents
-
view
216 -
download
3
Transcript of The Impact of Dental Devices on Neurostimulators

The Impact of Dental Devices on NeurostimulatorsSteven Roberts, DDS,* John R. Vender, MD,† Mark S. Causey, BS,‡ Jefferson R. Roberts, MD,§
Robert J. Loushine, DDS,* Walter J. Morris, DMD,k
and Stephen W. Looney, PhD{
Case Report/Clinical Techniques
AbstractSpinal cord stimulation has been a therapeutic option forchronic pain for over 40 years. The neurostimulator (NS) isa device consisting of three primary components: an elec-trode array configured either as a paddle or wire; animplantablepulse generator (IPG) consistingofa minicom-puter, a transceiver/antenna, an electrical generator, anda battery; and insulated wiring connecting the electrode tothe IPG. The electrode array can be implanted into theepidural space overlying the dorsal spinal cord or alonga peripheral nerve. The device generates pulsed electricalsignals that stimulate the underlying dorsal columns of thespinal cord resulting in the perception of paresthesia bythe patient. When overlapped with painful areas, theparesthesia can help decrease the patient’s level ofpain. The increased applications and indications for thistechnology enhance the likelihood that the NS patientwill be seen in the dental practice. Therefore, the purposeof this study was to investigate whether electromagneticinterference of the NS occurred during the operation of theapex locator, the electric pulp tester (EPT), or the electro-cautery unit. An NS was implanted into the epidural spaceof a human cadaver. The dental devices were used intra-orally, and the implant’s circuitry was tested after eachtrial. Two apex locators, two EPTs, and one electrocauteryunit were tested. Seventy trials were used by each dentaldevice on each tissue. Using the exact binomial method ofdetermining confidence intervals, the probability ofdamage to the NS by any of the devices was negligible.(J Endod 2009;35:422–425)
Key WordsApex locator, electric pulp tester, electrocautery, neuro-stimulator
From the *Department of Endodontics, School of Dentistry,Medical College of Georgia, Augusta, GA; †Department ofNeurosurgery, School of Medicine, Medical College of Georgia,Augusta, GA; ‡School of Dentistry, Medical College of Georgia,Augusta, GA; §Department of Internal Medicine, Walter ReedArmy Hospital, Washington, DC; kDepartment of Prosthodon-tics, School of Dentistry, Medical College of Georgia, Augusta,GA; and {Department Biostatistics, Medical College of Georgia,Augusta, GA.
Address requests for reprints to Dr Steven Roberts, Depart-ment of Endodontics, School of Dentistry, Medical College ofGeorgia, Augusta, GA 30912-1129. E-mail address:[email protected]/$0 - see front matter
Published by Elsevier, Inc. on behalf of American Associa-tion of Endodontists.doi:10.1016/j.joen.2008.12.005
422 Roberts et al.
The development and advancement of biotechnological devices have improved thequality of life for many medically compromised patients. The function of these
devices, however, may be adversely affected by extraneous electromagnetic energyfields. With the introduction of cardiac pacemakers in 1958, patients were advisedto avoid certain environments considered potentially hazardous to the implant’s func-tion (1, 2).
Dental devices emitting electromagnetic energy similarly represented potentialhazards to the pacemaker patients (3–6). A 1991 in vivo evaluation of the impact ofthe air scaler, ultrasonic curette, electric pulp tester, and electrotome on the functionof artificial pacemakers concluded that, although none of the devices caused an irreg-ularity in pacemaker function, a risk remained for patients with older pacemakers (5).Results of in vitro monitoring of atrial and ventricular pacemaker output and electro-cardiographic activity also indicated that the electric pulp tester, dental handpieces,radiography, and sonic scalers did not interfere with pacemaker function, althoughcertain electrosurgical and ultrasonic instruments may produce deleterious effects (6).
Several years after cardiac pacemakers were introduced, cochlear stimulatorswere successfully implanted in deaf patients. In 2002, Roberts et al (7) showed oncadavers that although the electric pulp tester (EPT), apex locator, electrocauteryunit, and panoramic radiograph machine appeared safe, the electrosurgery unit athigher settings could potentially damage the cochlear implant.
In 1967, Dr C. Norman Shealy, a neurosurgeon, implanted the first neuroaugmen-tive device for the relief of intractable pain in a terminally ill cancer patient (8). By 1970,six patients had undergone this treatment by Shealy et al. Since that time, neurostimu-lator (NS) technology has accelerated with respect to equipment design, flexibility, andreliability (Fig. 1).
Although initially believed to reduce pain via a gate mechanism, newer data suggestthat the analgesic effect produced by NSs is mediated by a release of endogenous opioidswithin the spinal cord parenchyma. This can explain the prolonged effect after thedevice has been turned off. NSs are now widely used for spinal axial pain as well asischemic limb pain, certain anginal pain syndromes, chronic diabetic neuropathicpain, sympathetically mediated pain, and failed back surgery syndrome (9–11). Recentliterature reveals both a clinical and a cost-benefit advantage of spinal stimulation overreoperative spinal fusion (12).
With improved technology and greater experience, the use of NSs has becomesafer and more effective. Therefore, the dental practitioner can expect to see anincreasing number of patients with these devices. No study exists on the effect of dentalequipment on the integrity of the NS. As with pacemaker or cochlear implant patients,the electromagnetic field created by dental instruments may present a potential hazardto NS patients. Damage to the NS could potentially not only irreparably damage theimplant but would also necessitate a surgical procedure to replace it. The purposeof this study was to investigate the effects of electromagnetic interference on an NSduring the operation of the EPT, apex locator, and electrocautery unit.
Materials and MethodsA human cadaver was obtained from the Department of Anatomy and Cell Biology
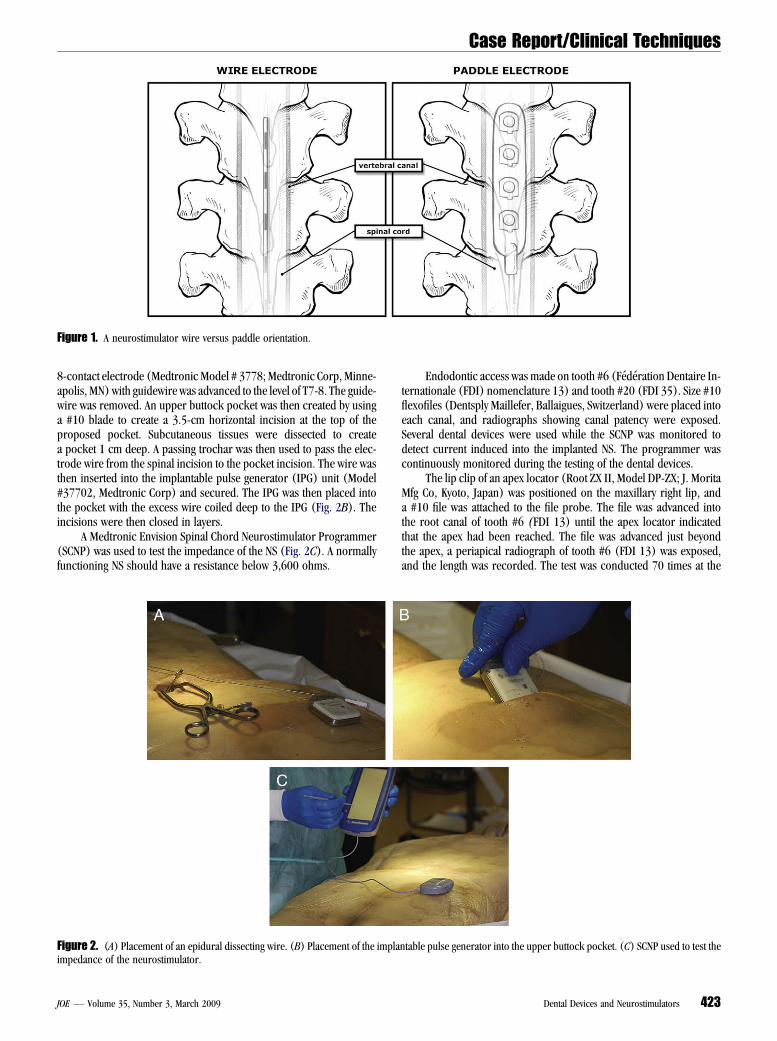
of the Medical College of Georgia. A vertical midline linear incision was created over theposterior spinous processes at T12 and L1. Subcutaneous tissues were dissected to thelevel of the lumbodorsal fascia. By using a loss-of-resistance technique, the epiduralspace was accessed with a #14-G Tuohy needle. An epidural dissecting wire was thenpassed into the epidural space (Fig. 2A). This was subsequently removed, and an
JOE — Volume 35, Number 3, March 2009
Case Report/Clinical Techniques
Figure 1. A neurostimulator wire versus paddle orientation.
8-contact electrode (Medtronic Model # 3778; Medtronic Corp, Minne-apolis, MN) with guidewire was advanced to the level of T7-8. The guide-wire was removed. An upper buttock pocket was then created by usinga #10 blade to create a 3.5-cm horizontal incision at the top of theproposed pocket. Subcutaneous tissues were dissected to createa pocket 1 cm deep. A passing trochar was then used to pass the elec-trode wire from the spinal incision to the pocket incision. The wire wasthen inserted into the implantable pulse generator (IPG) unit (Model#37702, Medtronic Corp) and secured. The IPG was then placed intothe pocket with the excess wire coiled deep to the IPG (Fig. 2B). Theincisions were then closed in layers.
A Medtronic Envision Spinal Chord Neurostimulator Programmer(SCNP) was used to test the impedance of the NS (Fig. 2C). A normallyfunctioning NS should have a resistance below 3,600 ohms.
JOE — Volume 35, Number 3, March 2009
Endodontic access was made on tooth #6 (Federation Dentaire In-ternationale (FDI) nomenclature 13) and tooth #20 (FDI 35). Size #10flexofiles (Dentsply Maillefer, Ballaigues, Switzerland) were placed intoeach canal, and radiographs showing canal patency were exposed.Several dental devices were used while the SCNP was monitored todetect current induced into the implanted NS. The programmer wascontinuously monitored during the testing of the dental devices.
The lip clip of an apex locator (Root ZX II, Model DP-ZX; J. MoritaMfg Co, Kyoto, Japan) was positioned on the maxillary right lip, anda #10 file was attached to the file probe. The file was advanced intothe root canal of tooth #6 (FDI 13) until the apex locator indicatedthat the apex had been reached. The file was advanced just beyondthe apex, a periapical radiograph of tooth #6 (FDI 13) was exposed,and the length was recorded. The test was conducted 70 times at the
Figure 2. (A) Placement of an epidural dissecting wire. (B) Placement of the implantable pulse generator into the upper buttock pocket. (C) SCNP used to test theimpedance of the neurostimulator.
Dental Devices and Neurostimulators 423

Case Report/Clinical Techniques
TABLE 1. One-sided 95% Confidence Interval for True Chance of Damaging the NeurostimulatorDevice Tissue n 95% One-Sided Confidence Interval
Apex locator #1 Tooth #6 70 (0-5.1)Tooth #20 70 (0-5.1)Combined (#6 and #20) 140 (0%, 2.6%)
Apex locator #2 Tooth #6 70 (0-5.1)Tooth #20 70 (0-5.1)Combined (#6 and #20) 140 (0-2.6)
Apex locators #1 & #2 All tissues 280 (0-1.3)Electrocautery unit Right palatine tonsil 70 (0-5.1)Electric pulp tester #1 Enamel of tooth #7 70 (0-5.1)
Enamel of tooth #26 70 (0-5.1)Dentin of tooth #6 70 (0-5.1)Gingiva 70 (0-5.1)All tissues 280 (0-1.3)
Electric pulp tester #2 Enamel of tooth #7 70 (0-5.1)Enamel of tooth #26 70 (0-5.1)Dentin of tooth #6 70 (0-5.1)All tissues 210 (0-1.7)
Electric pulp testers #1 and #2 All tissues 490 (0-0.7)
measured length. The test was conducted 70 times in the same fashionon tooth #20 (FDI 35).
The test was conducted 70 times each on tooth #6 (FDI 13) andtooth #20 (FDI 35) using the same model of a second apex locator(Root ZX II, Model DP-ZX). An electrocautery unit (ElectrocauteryChange-A-Tip; Aaron Medical Industries, Petersburg, FL) was activatedfor 3 seconds at the superior pole of the right palatine tonsil. The testwas conducted 70 times.
The probe tip of an EPT (Model 2001; Analytic Technology Corpo-ration, Redmond, WA) was placed on the enamel of tooth #7 (FDI 12).To complete the circuit, the handle of the EPT was placed on the arm ofthe cadaver. The output current was allowed to achieve its maximumsetting of 80. The procedure was repeated 70 times. The EPT was simi-larly used for 70 repetitions on the enamel of tooth #26 (FDI 42), thedentin of tooth #6 (FDI 13), and the attached gingiva in the vestibulebetween tooth #5 (FDI 14) and tooth #6 (FDI 13).
The probe tip of a second EPT (Model 2006, Analytic TechnologyCorporation) was placed on the enamel of tooth #7 (FDI 12). Tocomplete the circuit, the handle of the EPT was placed on the arm ofthe cadaver. The output current was allowed to achieve its maximumsetting of 80. The procedure was repeated 70 times. The EPT was simi-larly used for 70 repetitions on the enamel of tooth #26 (FDI 42) andthe dentin of tooth #6 (FDI 13). The NS was removed from the cadaverand was tested independently by a second SCNP.
Statistical analysis using the exact method of determining the confi-dence interval for the probability of destroying the NS was performed(13). The exact method uses the binomial distribution to calculatethe upper limit of a 95% confidence interval for the true proportionof detrimental responses. The chance of damaging the NS at the 95%level of confidence is between 0% and 1% with 365 trials, between0% and 5% with 70 trials, between 0% and 7% with 50 trials, andbetween 0% and 31% at 10 trials. Therefore, a sample size of n = 70was chosen for each tissue examined with each device.
ResultsThe devices were used on the cadaver at several different indi-
vidual intraoral locations. Two hundred eighty trials of the two apexlocators on two different teeth, 70 trials of the electrocautery unit,and 490 trials of two electric pulp testers on four different tissues failedto compromise the NS. Seventy trials of each device on each tissue failedto damage the NS; therefore, with 95% confidence, the chance of
424 Roberts et al.
damaging the NS is between 0% and 5% for each tissue examined byeach device. By combining the results for all tissues for each deviceor all results for each type of device, the results are even stronger (Table1).
One SCNP was used to test the NS that was implanted in the cadaver.A second SCNP was used to test the NS after it was removed from thecadaver. Both SCNPs showed that the NS was functional.
DiscussionDevices that transmit electromagnetic signals to the NS present
a potential hazard. Not only could the implant be permanentlydamaged, requiring replacement, but sufficient electrical energy couldalso necrose vital cells resulting in spinal cord or peripheral nerveinjury. Even if these cells were not damaged, reimplantation wouldinvolve significant expense to the patient plus the hazards of anothersurgery.
The NS was monitored by an SCNP throughout the numerous trialsof dental devices on the cadaver. In addition, after the NS was removedfrom the cadaver, it was tested again by a second SCNP, which showedthat the NS was still functional.
Three different devices were used in the oral cavity of thecadaver. However, the current was conducted at different distances;therefore, the path of the current had three different relationshipsto the implanted electrical device, the NS. The electrocautery unitdelivered bipolar high-frequency alternating current between twoelectrodes that were separated by less than 3 mm, a very shortdistance. The apex locator delivered a monopolar current betweenthe mucosa inside of the cheek and the apex of a tooth that was withina few centimeters, a distance that remained completely within the oralcavity. The EPT also delivered monopolar energy between the arm ofthe cadaver and various tissues within the oral cavity, a much largerdistance that extended beyond the oral cavity. None of these devicesaffected the NS.
Neurostimulators can be placed in a variety of locations. By far, themost common location is within the epidural space at T7-T10 becauseimplants are most commonly performed for low-back and lower-extremity pain. T7 was selected because it was the highest level likelyto be encountered in the majority of patients. Stimulators can also belocated in the cervical region for neck and upper-extremity pain oralong peripheral nerves. The location of the implant is determined bythe location of the patient’s pain.
JOE — Volume 35, Number 3, March 2009

Case Report/Clinical Techniques
Several options exist for electrodes. In general, the electrode arraycan be incorporated into a wire or paddle orientation (Fig. 1). Thechoice of wire or paddle depends on several factors including priorepidural scar, prior electrode migration, skill set, and preference ofthe implanting surgeon.
Numerous other types of electrical devices are in various stages ofresearch and development. At this time, the endodontic literature hasreported on the impact of dental devices on only three biotechnicaladvancements: the cardiac pacemaker, the cochlear implant, and theNS (1–7). Other types of electrical implants that are being developedinclude remote glucose sensor systems, stress incontinence stimulators,deep brain stimulators, and second sight retinal stimulators. With theadvent of new electrical implants and their entry into clinical use, thedental community must be aware of the impact of their electrical deviceson these electrically based implants.
AcknowledgmentsWe thank Dr Mohamed Sharawy, Department of Oral Biology
and Maxillofacial Pathology, Medical College of Georgia School ofDentistry, and David Adams, Department of Cellular Biology andAnatomy, Medical College of Georgia, for their invaluable supportin the Gross Anatomy Laboratory as well as Dr Franklin Tay, Depart-ment of Endodontics, Medical College of Georgia School ofDentistry, for his advice and support. The authors are grateful toMarie Churchville for her secretarial support.
JOE — Volume 35, Number 3, March 2009
References1. Whalen RE, Starmer F, McIntosh HD. Electric hazards associated with cardiac
pacing. Ann N Y Acad Sci 1964;11:922.2. Smyth NPD, Parsonnet V, Escher DJW, et al. The pacemaker patient and the electro-
magnetic environment. JAMA 1974;227:1412.3. Woolley LH, Woodworth J, Dobbs JL. A preliminary evaluation of the effects of electrical
pulp testers on dogs with artificial pacemakers. J Am Dent Assoc 1974;89:1099–101.4. Walter C. Dental treatment of patients with cardiac pacemaker implants. Quant Into
1975;8:57.5. Zappa U, Studier M, Merle A, et al. Effect of electrically powered dental devices on
cardiac parameter function in humans (German). Parodontologie 1991;2:299–308.6. Miller CS, Leonelli FM, Latham E. Selective interference with pacemaker activity by elec-
trical dental devices. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998;85:3–6.7. Roberts S, West LA, Liewehr FR, et al. Impact of dental devices on cochlear implants.
J Endod 2002;28:40–3.8. Shealy CN, Mortimer JT, Reswick JB. Electrical inhibition of pain by stimulation of
the dorsal columns. Anesth Analg 1967;46:489–91.9. de Vos CC, Rajan V, Steenbergen W, et al. Effect and safety of spinal cord stimulation
for treatment of chronic pain caused by diabetic neuropathy. J Diabetes Complica-tions 2008. Apr 16 (Epub ahead of print).
10. Anderson DJ, Ormond M. Perioperative care of patients undergoing an epiduralspinal cord stimulator for angina. J Peranesth Nurs 1999;14:330–5.
11. Atallah J, Armah FA, Wong D, et al. Use of spinal cord stimulator for treatment oflumbar radiculopathy in a patient with severe kyphoscoliosis. Pain Physician2008;11:555–9.
12. North RB, Kidd D, Shipley J, et al. Spinal cord stimulation versus reoperation forfailed back surgery syndrome: a cost effectiveness and cost utility analysis basedon a randomized, controlled trial. Neurosurgery 2007;61:361–8.
13. Agresti A. An introduction to categorical data analysis. 2nd ed. Hoboken, NJ: JohnWiley and Sons; 2007.
Dental Devices and Neurostimulators 425


















