The Growing Burden of Chronic Disease in America
12
g Burden of ease in America he Johns Hopkins University, Baltimore, MD derson, PhD, Bloomberg School of Public Health, The Johns Hopkins University, 624 N. Broadway 5-7310; fax 410-955-2301; e-mail <[email protected]>. Health In 2000, approximately 125 million Americans (45% of the population) had chronic conditions and 61 million (21% of the population) had multiple chronic conditions. The number of people with chronic conditions is projected to increase steadily for the next 30 years. While current health care financing and delivery systems are designed primarily to treat acute conditions, 78% of health spending is devoted to people with chronic conditions. Quality medical care for people with chronic conditions requires a new orientation toward prevention of chronic disease and provision of ongoing care and care manage- ment to maintain their health status and functioning. Specific focus should be applied to people with multiple chronic conditions. METHODS We define chronic conditions as those conditions that last a year or more and require ongoing medical attention and/or limit activities of daily living. 1 To determine which specific conditions met our definition, we convened two physician panels to review all medical conditions represented by the Interna- tional Classification of Diseases, 9th Revision (ICD-9) codes. 1 We applied the resulting classifications to data from the Medical Expenditure Panel Survey (MEPS), a survey sponsored by the Agency for Healthcare Research and Qual- ity (AHQR). The Household Component of the 1998 MEPS is a nationally representative sample of the non-institutional U.S. population. Two groups of respondents (24,072 people total) were interviewed three times each during the 1998 survey period. The MEPS Household Component provides information on health status, health services utilization, and health care spending. Health care spend- ing is calculated by AHRQ using respondents’ medical claims or other records. 2 This is a survey of people living in the community, and therefore does not provide information on people residing in institutions such as nursing homes. This is an important point. As a result, our data analysis understates the num- ber of people with chronic conditions as well as health care spending on their
-
Upload
simon-cartoon -
Category
Documents
-
view
2 -
download
0
description
disturbing
Transcript of The Growing Burden of Chronic Disease in America
Practice Articles
Public Health Reports / May–June 2004 / Volume 119 � 263
Gerard Anderson, PhDa
Jane Horvath, MHSAa
The Growing Burden ofChronic Disease in America
aBloomberg School of Public Health, The Johns Hopkins University, Baltimore, MD
Address correspondence to: Gerard Anderson, PhD, Bloomberg School of Public Health, The Johns Hopkins University, 624 N. Broadway#302, Baltimore, MD 21205; tel. 410-955-7310; fax 410-955-2301; e-mail <[email protected]>.
©2004 Association of Schools of Public Health
In 2000, approximately 125 million Americans (45% of the population) hadchronic conditions and 61 million (21% of the population) had multiplechronic conditions. The number of people with chronic conditions is projectedto increase steadily for the next 30 years. While current health care financingand delivery systems are designed primarily to treat acute conditions, 78% ofhealth spending is devoted to people with chronic conditions. Quality medicalcare for people with chronic conditions requires a new orientation towardprevention of chronic disease and provision of ongoing care and care manage-ment to maintain their health status and functioning. Specific focus should beapplied to people with multiple chronic conditions.
METHODS
We define chronic conditions as those conditions that last a year or more andrequire ongoing medical attention and/or limit activities of daily living.1 Todetermine which specific conditions met our definition, we convened twophysician panels to review all medical conditions represented by the Interna-tional Classification of Diseases, 9th Revision (ICD-9) codes.1 We applied theresulting classifications to data from the Medical Expenditure Panel Survey(MEPS), a survey sponsored by the Agency for Healthcare Research and Qual-ity (AHQR).
The Household Component of the 1998 MEPS is a nationally representativesample of the non-institutional U.S. population. Two groups of respondents(24,072 people total) were interviewed three times each during the 1998 surveyperiod. The MEPS Household Component provides information on healthstatus, health services utilization, and health care spending. Health care spend-ing is calculated by AHRQ using respondents’ medical claims or other records.2
This is a survey of people living in the community, and therefore does notprovide information on people residing in institutions such as nursing homes.This is an important point. As a result, our data analysis understates the num-ber of people with chronic conditions as well as health care spending on their

264 � Practice Articles
Public Health Reports / May–June 2004 / Volume 119
behalf because those living in institutions and thehealth spending on their behalf are excluded fromMEPS.
RESULTS
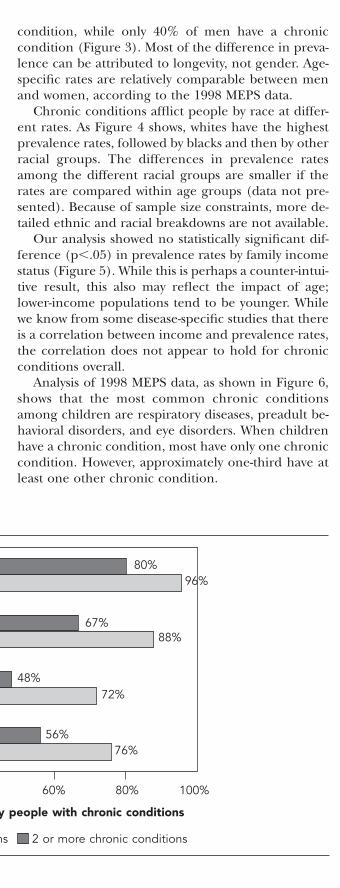
Analysis of the 1998 MEPS data shows that almost fourin five health care dollars (78%) are spent on behalfof people with chronic conditions. People with chronicconditions are the heaviest utilizers of medical care:96% of home health, 88% of prescriptions, 72% ofphysician visits, and 76% of inpatient hospital stays areattributed to people with chronic conditions (Figure1). Most of the utilization is by people with two ormore chronic conditions: 80% of home health, 67%of prescriptions, 48% of physician visits, and 56% ofinpatient stays.
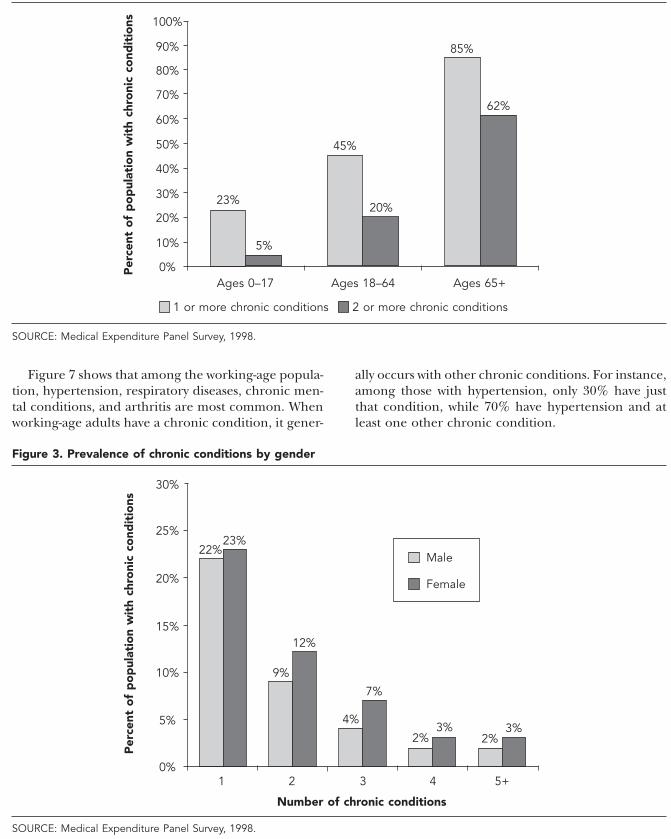
Analysis of 1998 MEPS data (Figure 2) shows thatchronic conditions are more prevalent in older popu-lations. Eighty-five percent of people aged 65 yearsand older have one or more chronic conditions,whereas 23% of children have one or more chronicconditions. Among the working-age population, 45%have a chronic condition. Prevalence of multiple con-ditions also increases with age, as shown in Figure 2:only 5% of children have multiple chronic conditions,but 62% of people aged 65 years and older have mul-tiple chronic conditions.
Almost 50% of women have at least one chronic
condition, while only 40% of men have a chroniccondition (Figure 3). Most of the difference in preva-lence can be attributed to longevity, not gender. Age-specific rates are relatively comparable between menand women, according to the 1998 MEPS data.
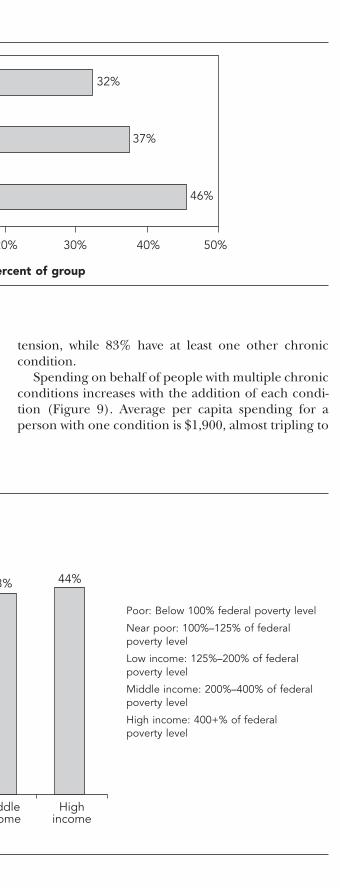
Chronic conditions afflict people by race at differ-ent rates. As Figure 4 shows, whites have the highestprevalence rates, followed by blacks and then by otherracial groups. The differences in prevalence ratesamong the different racial groups are smaller if therates are compared within age groups (data not pre-sented). Because of sample size constraints, more de-tailed ethnic and racial breakdowns are not available.
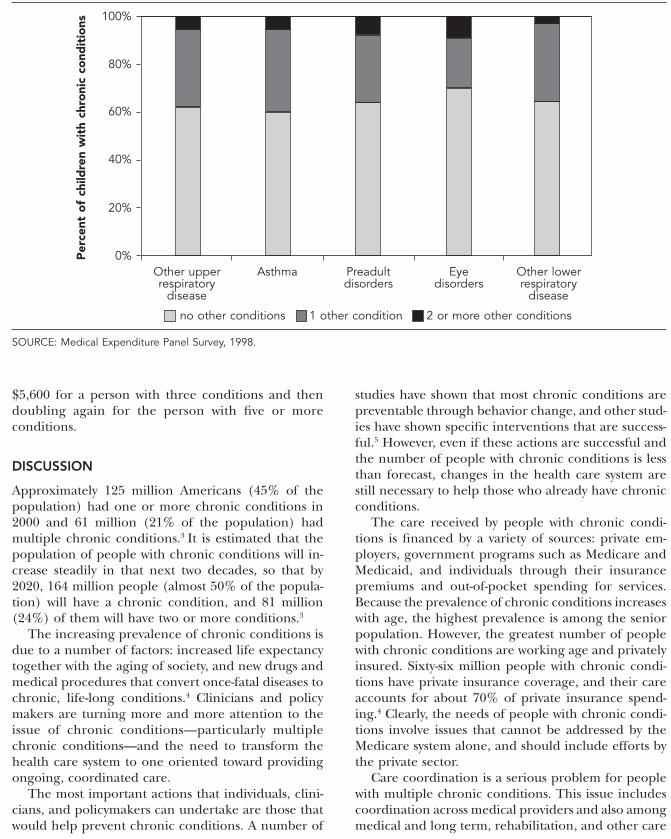
Our analysis showed no statistically significant dif-ference (p�.05) in prevalence rates by family incomestatus (Figure 5). While this is perhaps a counter-intui-tive result, this also may reflect the impact of age;lower-income populations tend to be younger. Whilewe know from some disease-specific studies that thereis a correlation between income and prevalence rates,the correlation does not appear to hold for chronicconditions overall.
Analysis of 1998 MEPS data, as shown in Figure 6,shows that the most common chronic conditionsamong children are respiratory diseases, preadult be-havioral disorders, and eye disorders. When childrenhave a chronic condition, most have only one chroniccondition. However, approximately one-third have atleast one other chronic condition.
Figure 1. Services use by people with chronic conditions
SOURCE: Medical Expenditure Panel Survey, 1998.
Home healthvisits
Prescriptions
Physician visits
Inpatient stays
Percent of services used by people with chronic conditions
100%80%60%40%20%0%
80%96%
67%88%
48%72%
56%76%
1 or more chronic conditions 2 or more chronic conditions
264 � Practice Articles
Public Health Reports / May–June 2004 / Volume 119
behalf because those living in institutions and thehealth spending on their behalf are excluded fromMEPS.
RESULTS
Analysis of the 1998 MEPS data shows that almost fourin five health care dollars (78%) are spent on behalfof people with chronic conditions. People with chronicconditions are the heaviest utilizers of medical care:96% of home health, 88% of prescriptions, 72% ofphysician visits, and 76% of inpatient hospital stays areattributed to people with chronic conditions (Figure1). Most of the utilization is by people with two ormore chronic conditions: 80% of home health, 67%of prescriptions, 48% of physician visits, and 56% ofinpatient stays.
Analysis of 1998 MEPS data (Figure 2) shows thatchronic conditions are more prevalent in older popu-lations. Eighty-five percent of people aged 65 yearsand older have one or more chronic conditions,whereas 23% of children have one or more chronicconditions. Among the working-age population, 45%have a chronic condition. Prevalence of multiple con-ditions also increases with age, as shown in Figure 2:only 5% of children have multiple chronic conditions,but 62% of people aged 65 years and older have mul-tiple chronic conditions.
Almost 50% of women have at least one chronic
condition, while only 40% of men have a chroniccondition (Figure 3). Most of the difference in preva-lence can be attributed to longevity, not gender. Age-specific rates are relatively comparable between menand women, according to the 1998 MEPS data.
Chronic conditions afflict people by race at differ-ent rates. As Figure 4 shows, whites have the highestprevalence rates, followed by blacks and then by otherracial groups. The differences in prevalence ratesamong the different racial groups are smaller if therates are compared within age groups (data not pre-sented). Because of sample size constraints, more de-tailed ethnic and racial breakdowns are not available.
Our analysis showed no statistically significant dif-ference (p�.05) in prevalence rates by family incomestatus (Figure 5). While this is perhaps a counter-intui-tive result, this also may reflect the impact of age;lower-income populations tend to be younger. Whilewe know from some disease-specific studies that thereis a correlation between income and prevalence rates,the correlation does not appear to hold for chronicconditions overall.
Analysis of 1998 MEPS data, as shown in Figure 6,shows that the most common chronic conditionsamong children are respiratory diseases, preadult be-havioral disorders, and eye disorders. When childrenhave a chronic condition, most have only one chroniccondition. However, approximately one-third have atleast one other chronic condition.
Figure 1. Services use by people with chronic conditions
SOURCE: Medical Expenditure Panel Survey, 1998.
Home healthvisits
Prescriptions
Physician visits
Inpatient stays
Percent of services used by people with chronic conditions
100%80%60%40%20%0%
80%96%
67%88%
48%72%
56%76%
1 or more chronic conditions 2 or more chronic conditions
Growing Burden of Chronic Disease � 265
Public Health Reports / May–June 2004 / Volume 119
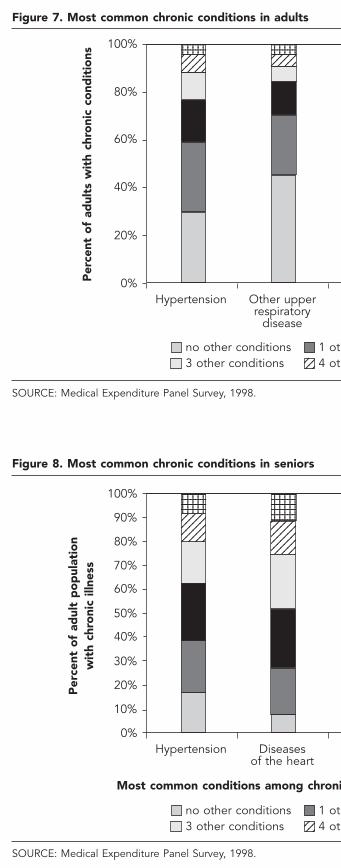
Figure 7 shows that among the working-age popula-tion, hypertension, respiratory diseases, chronic men-tal conditions, and arthritis are most common. Whenworking-age adults have a chronic condition, it gener-
ally occurs with other chronic conditions. For instance,among those with hypertension, only 30% have justthat condition, while 70% have hypertension and atleast one other chronic condition.
Figure 3. Prevalence of chronic conditions by gender
SOURCE: Medical Expenditure Panel Survey, 1998.
Male
Female
10%
5%
0%
15%
20%
25%
30%
5+
23%22%
9%
12%
4%
7%
2%3%
2%3%
4321
Number of chronic conditions
Per
cent
of
po
pul
atio
n w
ith
chro
nic
cond
itio
ns
Figure 2. Prevalence of chronic conditions by age
SOURCE: Medical Expenditure Panel Survey, 1998.
1 or more chronic conditions 2 or more chronic conditions
20%
10%
0%
30%
40%
50%
60%
70%
80%
90%
100%
Ages 0–17 Ages 18–64 Ages 65+
23%
5%
45%
20%
62%
85%
Per
cent
of
po
pul
atio
n w
ith
chro
nic
cond
itio
ns

266 � Practice Articles
Public Health Reports / May–June 2004 / Volume 119
The prevalence of comorbidities increases with age.Among seniors, hypertension, heart disease, arthritis,eye disorders, and diabetes are the most commonchronic condition. As Figure 8 shows, comorbiditiesare a major concern in seniors. Among seniors withhypertension, for example, only 17% have only hyper-
Figure 5. Chronic condition prevalence by income status
SOURCE: Medical Expenditure Panel Survey, 1998.
20%
10%
0%
30%
40%
50%
60%
Per
cent
wit
h ch
roni
c co
ndit
ions
41%
Lowincome
Nearpoor
Poor
Income group
Middleincome
Highincome
46%44% 43% 44%
Poor: Below 100% federal poverty level
Near poor: 100%–125% of federalpoverty level
Low income: 125%–200% of federalpoverty level
Middle income: 200%–400% of federalpoverty level
High income: 400+% of federalpoverty level
tension, while 83% have at least one other chroniccondition.
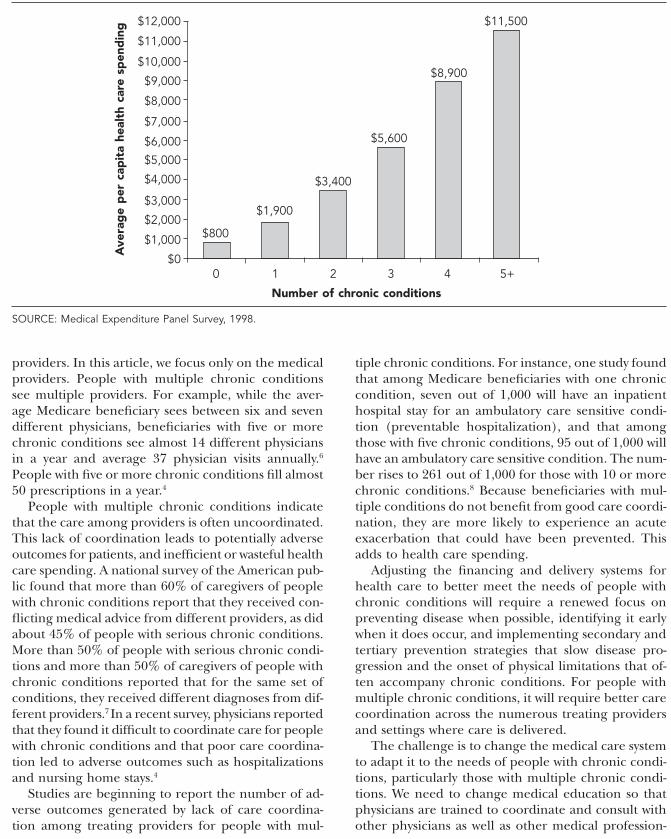
Spending on behalf of people with multiple chronicconditions increases with the addition of each condi-tion (Figure 9). Average per capita spending for aperson with one condition is $1,900, almost tripling to
Figure 4. Prevalence of chronic conditions by race
SOURCE: Medical Expenditure Panel Survey, 1998.
Other
Black
White
Percent of group
50%40%30%20%10%0%
32%
37%
46%
Rac
ial
gro
up
266 � Practice Articles
Public Health Reports / May–June 2004 / Volume 119
The prevalence of comorbidities increases with age.Among seniors, hypertension, heart disease, arthritis,eye disorders, and diabetes are the most commonchronic condition. As Figure 8 shows, comorbiditiesare a major concern in seniors. Among seniors withhypertension, for example, only 17% have only hyper-
Figure 5. Chronic condition prevalence by income status
SOURCE: Medical Expenditure Panel Survey, 1998.
20%
10%
0%
30%
40%
50%
60%
Per
cent
wit
h ch
roni
c co
ndit
ions
41%
Lowincome
Nearpoor
Poor
Income group
Middleincome
Highincome
46%44% 43% 44%
Poor: Below 100% federal poverty level
Near poor: 100%–125% of federalpoverty level
Low income: 125%–200% of federalpoverty level
Middle income: 200%–400% of federalpoverty level
High income: 400+% of federalpoverty level
tension, while 83% have at least one other chroniccondition.
Spending on behalf of people with multiple chronicconditions increases with the addition of each condi-tion (Figure 9). Average per capita spending for aperson with one condition is $1,900, almost tripling to
Figure 4. Prevalence of chronic conditions by race
SOURCE: Medical Expenditure Panel Survey, 1998.
Other
Black
White
Percent of group
50%40%30%20%10%0%
32%
37%
46%
Rac
ial
gro
up
Growing Burden of Chronic Disease � 267
Public Health Reports / May–June 2004 / Volume 119
$5,600 for a person with three conditions and thendoubling again for the person with five or moreconditions.
DISCUSSION
Approximately 125 million Americans (45% of thepopulation) had one or more chronic conditions in2000 and 61 million (21% of the population) hadmultiple chronic conditions.3 It is estimated that thepopulation of people with chronic conditions will in-crease steadily in that next two decades, so that by2020, 164 million people (almost 50% of the popula-tion) will have a chronic condition, and 81 million(24%) of them will have two or more conditions.3
The increasing prevalence of chronic conditions isdue to a number of factors: increased life expectancytogether with the aging of society, and new drugs andmedical procedures that convert once-fatal diseases tochronic, life-long conditions.4 Clinicians and policymakers are turning more and more attention to theissue of chronic conditions—particularly multiplechronic conditions—and the need to transform thehealth care system to one oriented toward providingongoing, coordinated care.
The most important actions that individuals, clini-cians, and policymakers can undertake are those thatwould help prevent chronic conditions. A number of
studies have shown that most chronic conditions arepreventable through behavior change, and other stud-ies have shown specific interventions that are success-ful.5 However, even if these actions are successful andthe number of people with chronic conditions is lessthan forecast, changes in the health care system arestill necessary to help those who already have chronicconditions.
The care received by people with chronic condi-tions is financed by a variety of sources: private em-ployers, government programs such as Medicare andMedicaid, and individuals through their insurancepremiums and out-of-pocket spending for services.Because the prevalence of chronic conditions increaseswith age, the highest prevalence is among the seniorpopulation. However, the greatest number of peoplewith chronic conditions are working age and privatelyinsured. Sixty-six million people with chronic condi-tions have private insurance coverage, and their careaccounts for about 70% of private insurance spend-ing.4 Clearly, the needs of people with chronic condi-tions involve issues that cannot be addressed by theMedicare system alone, and should include efforts bythe private sector.
Care coordination is a serious problem for peoplewith multiple chronic conditions. This issue includescoordination across medical providers and also amongmedical and long term, rehabilitation, and other care
Figure 6. Most common chronic conditions in children
SOURCE: Medical Expenditure Panel Survey, 1998.
40%
20%
0%
60%
80%
100%
Per
cent
of
child
ren
wit
h ch
roni
c co
ndit
ions
no other conditions 1 other condition 2 or more other conditions
Other upperrespiratory
disease
Preadultdisorders
Eyedisorders
Other lowerrespiratory
disease
Asthma
268 � Practice Articles
Public Health Reports / May–June 2004 / Volume 119
Figure 7. Most common chronic conditions in adults
SOURCE: Medical Expenditure Panel Survey, 1998.
Per
cent
of
adul
ts w
ith
chro
nic
cond
itio
ns
Hypertension
no other conditions 1 other condition 2 other conditions3 other conditions 4 other conditions 5 or more other conditions
Other upperrespiratory
disease
Mentalconditions
Chronicrespiratoryinfections
Arthritis
1234123412341234
123456123456123456123456123456
123123123
123123123
40%
20%
0%
60%
80%
100% 1234123412341234
123412341234
123451234512345
1234512345
123456123456
123456123456123456123456
123456123456123456
123456123456123456
Figure 8. Most common chronic conditions in seniors
SOURCE: Medical Expenditure Panel Survey, 1998.
Per
cent
of
adul
t p
op
ulat
ion
wit
h ch
roni
c ill
ness
Most common conditions among chronically ill seniors, 65+ years and comorbidity rates
Hypertension
no other conditions 1 other condition 2 other conditions3 other conditions 4 other conditions 5 or more other conditions
Diseasesof the heart
Arthritis Eyedisorders
Diabetes
123412341234123412341234
123456123456123456123456123456123456
123123123
123123123
40%
20%
0%
60%
80%
100%12341234123412341234
12341234123412341234
123451234512345123451234512345
1234512345123451234512345
123456123456123456123456123456123456
123456123456123456123456123456
123456123456123456123456123456123456
123456123456123456123456123456
90%
70%
50%
30%
10%

268 � Practice Articles
Public Health Reports / May–June 2004 / Volume 119
Figure 7. Most common chronic conditions in adults
SOURCE: Medical Expenditure Panel Survey, 1998.
Per
cent
of
adul
ts w
ith
chro
nic
cond
itio
ns
Hypertension
no other conditions 1 other condition 2 other conditions3 other conditions 4 other conditions 5 or more other conditions
Other upperrespiratory
disease
Mentalconditions
Chronicrespiratoryinfections
Arthritis
1234123412341234
123456123456123456123456123456
123123123
123123123
40%
20%
0%
60%
80%
100% 1234123412341234
123412341234
123451234512345
1234512345
123456123456
123456123456123456123456
123456123456123456
123456123456123456
Figure 8. Most common chronic conditions in seniors
SOURCE: Medical Expenditure Panel Survey, 1998.
Per
cent
of
adul
t p
op
ulat
ion
wit
h ch
roni
c ill
ness
Most common conditions among chronically ill seniors, 65+ years and comorbidity rates
Hypertension
no other conditions 1 other condition 2 other conditions3 other conditions 4 other conditions 5 or more other conditions
Diseasesof the heart
Arthritis Eyedisorders
Diabetes
123412341234123412341234
123456123456123456123456123456123456
123123123
123123123
40%
20%
0%
60%
80%
100%12341234123412341234
12341234123412341234
123451234512345123451234512345
1234512345123451234512345
123456123456123456123456123456123456
123456123456123456123456123456
123456123456123456123456123456123456
123456123456123456123456123456
90%
70%
50%
30%
10%
Growing Burden of Chronic Disease � 269
Public Health Reports / May–June 2004 / Volume 119
Figure 9. Per capita spending by number of chronic conditions
SOURCE: Medical Expenditure Panel Survey, 1998.
$12,000
$800
Ave
rag
e p
er c
apit
a he
alth
car
e sp
end
ing
$1,900
$3,400
$5,600
$8,900
$11,500
5+4320
Number of chronic conditions
1
$11,000
$10,000
$9,000
$8,000
$7,000
$6,000
$5,000
$4,000
$3,000
$2,000
$1,000
$0
providers. In this article, we focus only on the medicalproviders. People with multiple chronic conditionssee multiple providers. For example, while the aver-age Medicare beneficiary sees between six and sevendifferent physicians, beneficiaries with five or morechronic conditions see almost 14 different physiciansin a year and average 37 physician visits annually.6
People with five or more chronic conditions fill almost50 prescriptions in a year.4
People with multiple chronic conditions indicatethat the care among providers is often uncoordinated.This lack of coordination leads to potentially adverseoutcomes for patients, and inefficient or wasteful healthcare spending. A national survey of the American pub-lic found that more than 60% of caregivers of peoplewith chronic conditions report that they received con-flicting medical advice from different providers, as didabout 45% of people with serious chronic conditions.More than 50% of people with serious chronic condi-tions and more than 50% of caregivers of people withchronic conditions reported that for the same set ofconditions, they received different diagnoses from dif-ferent providers.7 In a recent survey, physicians reportedthat they found it difficult to coordinate care for peoplewith chronic conditions and that poor care coordina-tion led to adverse outcomes such as hospitalizationsand nursing home stays.4
Studies are beginning to report the number of ad-verse outcomes generated by lack of care coordina-tion among treating providers for people with mul-
tiple chronic conditions. For instance, one study foundthat among Medicare beneficiaries with one chroniccondition, seven out of 1,000 will have an inpatienthospital stay for an ambulatory care sensitive condi-tion (preventable hospitalization), and that amongthose with five chronic conditions, 95 out of 1,000 willhave an ambulatory care sensitive condition. The num-ber rises to 261 out of 1,000 for those with 10 or morechronic conditions.8 Because beneficiaries with mul-tiple conditions do not benefit from good care coordi-nation, they are more likely to experience an acuteexacerbation that could have been prevented. Thisadds to health care spending.
Adjusting the financing and delivery systems forhealth care to better meet the needs of people withchronic conditions will require a renewed focus onpreventing disease when possible, identifying it earlywhen it does occur, and implementing secondary andtertiary prevention strategies that slow disease pro-gression and the onset of physical limitations that of-ten accompany chronic conditions. For people withmultiple chronic conditions, it will require better carecoordination across the numerous treating providersand settings where care is delivered.
The challenge is to change the medical care systemto adapt it to the needs of people with chronic condi-tions, particularly those with multiple chronic condi-tions. We need to change medical education so thatphysicians are trained to coordinate and consult withother physicians as well as other medical profession-
270 � Practice Articles
Public Health Reports / May–June 2004 / Volume 119
als. We need to improve health care to provide moresupport for ongoing care of chronic conditions, in-cluding when people have access to otherwise coveredbenefits. Often today, covered services are terminatedwhen a patient no longer improves but are authorizedagain only after deterioration has occurred. Medicalnecessity criterion should be interpreted to allowpeople to maintain their health and functional status.We need information systems that allow clinicians tocommunicate with each other on a timely basis. Fi-nally, and perhaps most importantly, we need to alignfinancial incentives within health care systems to pro-mote coordination within the medical care system andamong medical and supportive care systems. Ultimately,care coordination for people with multiple chronicconditions must become a standard of quality care,against which health plans and providers are measured.
The health care system has successfully adapted tomeet new challenges in the past. Examples includethe creation of a public health system in the early 20thcentury to combat communicable diseases, and thedevelopment of services and financing systems to ef-fectively treat acute conditions such as heart attacks inthe latter half of the 20th century. The system musttransform itself again by reorienting to the major chal-lenge of the 21st century—effective prevention andtreatment of chronic conditions.
This paper was supported by the Robert Wood JohnsonFoundation. Dr. Anderson and Jane Horvath are director anddeputy director, respectively, of Partnership for Solutions: BetterLives for People with Chronic Conditions. Partnership forSolutions is a National Program Office of the Robert WoodJohnson Foundation, lead by the Johns Hopkins University.
REFERENCES
1. Hwang W, Weller W, Ireys H, Anderson G. Out of pocketmedical spending for care of chronic conditions. HealthAff 2001;20:268-9.
2. Agency for Healthcare Research and Quality. MedicalExpenditure Panel Survey (MEPS) [cited 2003 Dec 22].Available from: URL: http://www.ahrq.gov/data/mepsix.htm
3. Wu S, Green A. Projection of chronic illness prevalenceand cost inflation. Prepared for Partnership for Solutionsby RAND Corporation. Baltimore: The Johns HopkinsUniversity; 2000.
4. Partnership for Solutions. Chronic conditions: makingthe case for ongoing care. Baltimore: The Johns HopkinsUniversity; 2002. Also available from: URL: http://www.partnershipforsolutions.org/DMS/files/chronicbook2002.pdf
5. McGinnis JM, Foege WH. Actual causes of death in theUnited States. JAMA 1993;270:2207-12.
6. Berenson R, Horvath J. Confronting the barriers tochronic care management in Medicare. Health AffairsOnline (Web Exclusive) [cited 2003 Jan 22]: Availablefrom: URL: http://content.healthaffairs.org/cgi/content/full/hlthaff.w3.37v1/DC1
7. Partnership for Solutions. Chronic conditions: publicperceptions about health care access and services. Balti-more: The Johns Hopkins University; 2002. Also avail-able from: URL: http://www.partnershipforsolutions.org/DMS/files/polling_final.pdf
8. Wolff J, Starfield B, Anderson G. Prevalence, expendi-tures, and complications of multiple chronic conditionsin the elderly. Arch Intern Med 2002;162:2269-76.
270 � Practice Articles
Public Health Reports / May–June 2004 / Volume 119
als. We need to improve health care to provide moresupport for ongoing care of chronic conditions, in-cluding when people have access to otherwise coveredbenefits. Often today, covered services are terminatedwhen a patient no longer improves but are authorizedagain only after deterioration has occurred. Medicalnecessity criterion should be interpreted to allowpeople to maintain their health and functional status.We need information systems that allow clinicians tocommunicate with each other on a timely basis. Fi-nally, and perhaps most importantly, we need to alignfinancial incentives within health care systems to pro-mote coordination within the medical care system andamong medical and supportive care systems. Ultimately,care coordination for people with multiple chronicconditions must become a standard of quality care,against which health plans and providers are measured.
The health care system has successfully adapted tomeet new challenges in the past. Examples includethe creation of a public health system in the early 20thcentury to combat communicable diseases, and thedevelopment of services and financing systems to ef-fectively treat acute conditions such as heart attacks inthe latter half of the 20th century. The system musttransform itself again by reorienting to the major chal-lenge of the 21st century—effective prevention andtreatment of chronic conditions.
This paper was supported by the Robert Wood JohnsonFoundation. Dr. Anderson and Jane Horvath are director anddeputy director, respectively, of Partnership for Solutions: BetterLives for People with Chronic Conditions. Partnership forSolutions is a National Program Office of the Robert WoodJohnson Foundation, lead by the Johns Hopkins University.
REFERENCES
1. Hwang W, Weller W, Ireys H, Anderson G. Out of pocketmedical spending for care of chronic conditions. HealthAff 2001;20:268-9.
2. Agency for Healthcare Research and Quality. MedicalExpenditure Panel Survey (MEPS) [cited 2003 Dec 22].Available from: URL: http://www.ahrq.gov/data/mepsix.htm
3. Wu S, Green A. Projection of chronic illness prevalenceand cost inflation. Prepared for Partnership for Solutionsby RAND Corporation. Baltimore: The Johns HopkinsUniversity; 2000.
4. Partnership for Solutions. Chronic conditions: makingthe case for ongoing care. Baltimore: The Johns HopkinsUniversity; 2002. Also available from: URL: http://www.partnershipforsolutions.org/DMS/files/chronicbook2002.pdf
5. McGinnis JM, Foege WH. Actual causes of death in theUnited States. JAMA 1993;270:2207-12.
6. Berenson R, Horvath J. Confronting the barriers tochronic care management in Medicare. Health AffairsOnline (Web Exclusive) [cited 2003 Jan 22]: Availablefrom: URL: http://content.healthaffairs.org/cgi/content/full/hlthaff.w3.37v1/DC1
7. Partnership for Solutions. Chronic conditions: publicperceptions about health care access and services. Balti-more: The Johns Hopkins University; 2002. Also avail-able from: URL: http://www.partnershipforsolutions.org/DMS/files/polling_final.pdf
8. Wolff J, Starfield B, Anderson G. Prevalence, expendi-tures, and complications of multiple chronic conditionsin the elderly. Arch Intern Med 2002;162:2269-76.