
The Financial Sustainability Plan - WHO
41
The Republic of The Gambia Department of State for Health &Social Welfare The Financial Sustainability Plan Submitted to GAVI November 2003
Transcript of The Financial Sustainability Plan - WHO
The Republic of The Gambia
Department of State for Health &Social Welfare
The Financial Sustainability Plan
Submitted to GAVI
November 2003
The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 2 Printed: 3:33 PM 6/17/2004
Table of Contents
Executive Summary 5 List of Acronyms 6 Acknowledgements 7 SECTION 1
Impact of Country and Health System Context on Immunization Programme Costs, Financing and Financial Management 1.1 Background 8 1.2 Country Vision and main agenda 8 1.3 Macro-economic trends 9 1.4 Administrative context 10 1.5 Health system context 11 1.6 Health Programme Areas 12 1.7 Health Services Delivery 13 1.8 Health Policy and Health Public Expenditure Review 13 1.9 Budget Process and Financial Management 13 1.10 Budgeting, Financial management systems 14 1.11 Accounting and Audit 15 1.12 Health Financing Information 15
SECTION 2
Expanded Programme on Immunization: Characteristics, Objectives and Strategies 2.1 Background 16 2.2 Programme Objectives 17 2.3 Vaccine Procurement and Financing 19 2.4 Programme Management 19 2.5 Transportation and storage facilities 20 2.6 Financing the National Immunisation Programme 20 2.7 Payment of service providers 21 2.8 Plans for the future 21
SECTION 3
Current Expenditure & Financing 3.1 Introduction 22 3.2 Baseline and Current Program Costs 22 3.3 Baseline and Current Program Cost Funding 25 3.4 Supplementary Immunisation Activities 28

The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 3 Printed: 3:33 PM 6/17/2004
SECTION 4 Future Resource Requirements and Programme Financing 4.1 FSP Cost Projections 29 4.2 Strategic Initiatives Planned for and incorporated in the Forecast Period
2003 – 2012 30 4.3 Probable Sources of Finance & Funding Gap 32 4.4 Projected Key Indicators 34 4.5 Scenario B: Projections for inclusion of Pneumococcal Vaccine in 2007 35 4.6 Key Indicators for Scenario B 37
SECTION 5
Sustainable Financing Strategic Plan and Indicators 5.1 Key objectives for the Financial Sustainability Plan 38 5.2 Requirements for Success 38 5.3 Strategic Plan to Achieve Sustainable Financing 39 5.4 Conclusion 41
List of Tables Table 1.1: Health indicators for The Gambia compared with average for Sub-Saharan African countries 9 Table 1.2 Projections for key macroeconomic indicators: 2002- 2005 9 Table 2.1 Percentage immunization coverage over the last eight years 16 Table 2.2 Reported cases of selected vaccine preventable diseases
1995 – 2002 17 Table 3.0 Baseline and Current Year Costing - Summary of
FSP Table 3.1 and 3.2 23 Table 3.1 Baseline Costs 2002 Appendix A Table 3.2 Current Year Costs Appendix A Table 3.3 Wastage Levels Summary 23 Table 3.4 Funding Sources 2002 25 Table 3.5 Summary Indicators 28 Table 4.1 Projections of Future Resource Needs 29 Table 4.2 Projected Vaccine Wastage Savings 30 Table 4.3 Cost Projections 32 Table 4.4 Projected Funding Gap 32 Table 4.5 Projected Financing 32 Table 4.6 Projected Key Indicators 34 Table 4.7 Projections of Future Resource Needs – Scenario B – Including Introduction of Pneumococcal Vaccine 35 Table 4.8 Projected Funding Gap – Scenario B – Including Introduction of Pneumococcal Vaccine 35 Table 4.9 Cost Projections Scenario B – Including Introduction of Pneumococcal Vaccine 36 Table 4.10 Projected Key Indicators – Scenario B – Including Introduction of Pneumococcal Vaccine 37 Table 5.1 Strategic Plan 39

The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 4 Printed: 3:33 PM 6/17/2004
List of Figures Figure 1.1 Organisation of the Health Department 11 Figure 1.2 Organisation of delivery of EPI services 12 Figure 2.1 Proportion of children fully immunised less than 12 months. 18 Figure 3.1 The Gambia National Immunisation Program – 22
Baseline Cost Profile 2002 – Excluding Supplementary Immunisation Activities
Figure 3.2 The Gambia National Immunisation Program – 22 Current Year Cost Profile 2003 – Excluding Supplementary Immunisation Activities
Figure 3.3 The Gambia National Immunisation Programme – 25 Financing of Recurrent EPI Activities – Baseline 2002 Excluding Capital Costs & Supplementary Implementation Activities
Figure 3.4 The Gambia National Immunisation Programme – 26 Financing of Recurrent EPI Activities - Current Year 2003 Excluding Capital Costs & Supplementary Implementation Activities
Figure 3.5 Funding Comparison – 27 Baseline 2002 v Current Year 2003 – Excluding Supp. Immunisation Activities and Capital Costs
Figure 4.1 Projections of Future Resource Needs by Cost Categories 29 Figure 4.2 Projections of Secure and Probable Financing 32
by Source and Funding Gap Figure 4.3 Projections of Future Resource Needs by Cost Categories – 35
Scenario B Figure 4.4 Projections of Secure and Probable Financing 35
by Source and Funding Gap – Scenario B List of Appendices
Appendix A Tables 3.1 and 3.2 Appendix B Section 3 Costing Methodologies. Appendix C Section 3 Supporting Data Tables Appendix D Section 4 Summary Cost & Funding Forecasts Appendix E Section 4 Assumptions made in completing the Future Resource
Requirements Appendix F Section 4 Supporting Data Tables

The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 5 Printed: 3:33 PM 6/17/2004
Executive Summary This Financial Sustainability Plan was completed as a requirement for extended GAVI support for the ongoing programme of immunisation of The Gambia. GAVI requires that before support is given a country must develop a credible plan to achieve the goal of financial sustainability in the delivery of immunisation services. GAVI define sustainability accordingly:
Although self-sufficiency is the ultimate goal, in the nearer term sustainable financing is the ability of a country to mobilize and efficiently use domestic and supplementary external resources on a reliable basis to achieve current and future target levels of immunization performance in terms of access, utilization, quality, safety and equity.
The FSP contains a comprehensive review of the EPI programme in The Gambia. The review covers all aspects from the macro economic environment, the health sector in general, a review and costing of the current programme and a forecast for the ten year period commencing in 2003. This review highlighted three key areas requiring considerable change:
Funding Shortfalls Vaccine Wastage Deterioration of the Cold Chain
Future programme objectives and strategies were modelled using the Financial Sustainability Planning tool developed by GAVI. The modelling process was iterative in nature and evolved after considerable input from key EPI stakeholders. Various scenarios were considered including the impact on the programme of the introduction of new vaccines. The final programme of changes are presented in Section 4 with supporting Appendix data. After careful consideration the forecasts presented represent the strategic framework necessary to strengthen delivery of immunisation services in The Gambia. Strategic objectives, proposed actions, assigned responsibilities and monitoring indicators were developed and presented in Section 5. The final version was presented to meetings convened with the Ministries of Health & Social Welfare, Finance, and Planning together with members of the EPI management and ICC including donor partners. Stakeholder comments have been taken into consideration in the final draft. It is anticipated the FSP act as primary aid to the Government of The Gambia, senior health officials and particularly the senior management of the EPI programme to ensure the successful delivery of immunisation services in The Gambia. It’s success can only be measured by the steps that are taken to start the process of moving The Gambia on its way towards financial sustainability. Most importantly of all the FSP acts as a vital mechanism to help enable the children of The Gambia to continue to receive the best possible protection against vaccine preventable diseases.
The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 6 Printed: 3:33 PM 6/17/2004
Acronyms AD Syringe Auto-Disable Syringe ADB African Development Bank AFP Acute Flaccid Paralysis CFAA Country Financial Accountability Assessment CHN Community Health Nurse CHP Community Health Post CRS Catholic Relief Services DFID Department for International Development (UK Gov) DHT Divisional Health Team DOSH Department Of State for Health EPI Extended Programme on Immunisation EU European Union GAVI Global Alliance for Vaccines & Immunization GDP Gross Domestic Product GoG Government of The Gambia HDI Human Development Index HIPC debt initiative for Heavily Indebted Poor Countries HMIS Health Management Information System ICC Inter-agency Co-ordinating Committee IEC Information Education Communication IDA International Development Association IFMIS Integrated Financial Management Information System IMF International Monetary Fund MCH Maternal & Child Health MRC Medical Research Council NEFCOM National Emergency Finance Committee NGO Non Governmental Organisation NHA National Health Accounts NID National Immunisation Day NNT NeoNatal Tetanus PER Public Expenditure Review PHC Primary Health Centre PHO Public Health Officer PHNP Participatory Health & Nutrition Project PRGF Poverty Reduction and Growth Facility PRSP Poverty Reduction Strategy Programme SDR Special Drawing Rights SEN State Enlisted Nurse SIAs Supplementary Immunisation Activities SRN State Registered Nurse SSA Sub-Saharan Africa SWAp Sector Wide Approach UNICEF United Nations Children’s Fund VHS Village Health Services WHO World Health Organisation BCG Mycobacterium bovis BCG (Bacillus Calmette-Guerin) DPT Diptheria, Pertussis, Tetanus Hep B Hepatitis B Hib Haemophilus influenzae type b OPV Oral Poliomyelitis Vaccine TT Tetanus Toxoid

The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 7 Printed: 3:33 PM 6/17/2004
Acknowledgements The Department of State for Health (DOSH) would like to express gratitude to all the individuals and the various development partners particularly WHO, UNICEF and GAVI for valuable technical support in the development of this financial sustainability plan (FSP) and also members of the task force for the drafting and review of the plan. The review and input by the ICC is also highly appreciated. The participation and efforts of the Central EPI Unit officers has been tremendous. The contribution made by the two consultants (national and international) hired for the assignment and funded by WHO is acknowledged. This plan will support the efforts of the Department of State for Health in implementing its policy to provide quality immunization services for the protection of all children under five years of age and all women of child bearing age from vaccine preventable diseases. Special thanks goes to the task force and our development partners who have contributed in one way or another towards the provision of the health care services in The Gambia. In the same vein a request is being put forward to willing bilateral and multilateral partners and individuals within and outside The Gambia to support this plan with any resources at their disposal. PREPARATION AND REVIEW TEAM TASK FORCE MEMBERS NAME DESIGNATION INSTITUTE Dr. Ayo Palmer Programme Officer UNICEF Dr. O. Sam Director DOSH Dr. Mariatou Jallow Deputy Director DOSH Dr. B.D. Tagodoe MO/EPI WHO Mr. M.K. Cham Ag. Director of Planning DOSH Mrs. Naffie Barry Deputy Permanent Sec. DOSH Dr. P. Mshana Human Resource Development Specialist WHO Dr. Kulmani P. Kulimani Health System Research Specialist WHO Mrs. Yamundow Jallow Ag. EPI Manager DOSH Mr. Robert Ninson EPI Surveillance Officer DOSH CONSULTANTS Mr. William Meaney International Consultant Mr. Robert Hight National Consultant

The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 8 Printed: 3:33 PM 6/17/2004
SECTION 1 1. Impact of Country and Health System Context on Immunization Programme
Costs, Financing and Financial Management 1.1. Background
The Republic of The Gambia, on the West Coast of Africa, is one of the smallest countries on the African continent with a population of 1.4 million1 and an estimated annual growth rate of 4.2% based on the 1993 census. The Gambia became independent in 1965. The democratic process was interrupted by a military takeover in 1994. By early 1997 The Gambia returned to constitutional rule following presidential elections. Since then two elections have been held and the next election is due in 2006. The country is divided into five administrative divisions (Western, Lower River, Central River, Upper River and North Bank) and two municipalities (Banjul and Kanifing). The Gambia is bordered on both sides by Senegal except the small opening to the Atlantic Ocean. It covers an area of 10,680 square kilometres and stretches an approximately 400-kilometre length on either side of The Gambia River, which divides the country in almost two equal halves. Due to civil unrest in neighbouring countries, notably the Cassamance region of Senegal, Sierra Leone and Liberia, The Gambia has increasingly become a haven for refugees which put additional demand on the health service of The Gambia.
1.2. Country Vision and main agenda
The Government’s current national development objectives and priorities are defined in the Mission Statement of Vision 2020, which expresses The Gambia’s aspirations and socio-economic strategy for the period 1996-2020. It accords high priority to the social sectors of Health and Education, gives and calls for focussed attention on child survival, protection and development programmes. The Government recently prepared a Poverty Reduction Strategy Paper (PRSP), which was presented to both the International Monetary Fund (IMF) and World Bank Boards of Directors in July 2002. Child health and survival is one of the priority areas highlighted in the PRSP and in the Millennium Development Goals, 2015. The PRSP presents the country's programme for the coming years, and the Government is preparing a comprehensive technical assistance programme 1 Preliminary data from 2003, Population Census, Central Statistic Department. Detailed information will be provided once the census data is finalised.

The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 9 Printed: 3:33 PM 6/17/2004
to support it. In addition, the IMF approved (also in July 2002) a new three year arrangement under the Poverty Reduction and Growth Facility (PRGF). The Gambia has made some progress towards achieving its health goals, though slow by comparison of its national vital indicators to other countries in the region. The Table below compares key indicators in The Gambia with those in the Sub-Saharan African region. Table 1.1: Health indicators for The Gambia compared with average for Sub-
Saharan African (SSA) countries GNP per
capita (1997 US$)
Life expectancy 1999
Fertility Rate 1999
Infant Mortality rate (per 1,000) 1999
Illiteracy (% of pop. Aged 15+) 2000
Access to safe water (%of pop.) 2000
The Gambia
340 53 5.5 75 63 62
SSA 510 47 5.3 92 40 55 Source: World Development Indicators, 2001 1.3. Macro-economic trends
The economy is predominantly agrarian with a low per capita income of approximately US $330 per annum. Real GDP growth in 2001 was estimated at 5.7 per cent (Economist Intelligence Unit, 2002, p. 31). The total external debt in 2000 was estimated at US $438 million and the debt to export ratio for the same period was 13.8 per cent (Department of State for Finance & Economic Affairs). Human Development Index (HDI) is 0.405 with a ranking of 160 out of 173 countries (HD Report, 2002, p. 152). Poverty is endemic and increasing. The 1998 poverty study indicated that 69 per cent of the population are below the poverty line. The national debt now stands at US $657m. The productive sector has witnessed severe constraints culminating in 2002 in the declaration of a severe food shortage by the Government. Tourism, a major foreign exchange earner is on the decline, thus, resulting in the significant decline of the domestic currency, the Dalasi, against all foreign currencies. High inflation and exchange rate fluctuation have severely reduced household incomes particularly in rural areas. The prices of food and other basic commodities, which are mostly imported, have also escalated with dramatic increases in the prices of staples and fuel. Macro-stability is a key component of poverty reduction, therefore attention has been given to assessing the potential contribution of its various components for the period 2002-2005. Table 1.2 Projections for key macroeconomic indicators: 2002- 2005 Indicator 2002 2003 2004 2005 Real GDP growth (%) 6 6 6 6.2 Fiscal deficit (grants) as GDP 5 2.7 2.3 1.9 Export growth (SDR, assuming an exchange rate of 21.3) 8.4 8.2 5.3 3.5 Current Account deficit (excluding grants) as % GDP 13.2 12.3 11.6 10.3 Current Account deficit (including grants) as % GDP 5.4 5.0 5.8 2.7 Gross official reserves as months of imports (including transit trade) c.i.f
5.0 5.2 5.4 5.5
Broad money growth 13.2 9.9 9.6 9.6 Inflation 5.5 4.0 3 3 Source: Department of State for Finance and Economic Affairs.
Deleted: are compare
Deleted: that of comp

The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 10 Printed: 3:33 PM 6/17/2004
To address fiscal imbalances, the Government has launched a comprehensive work programme to strengthen its capacity to execute and monitor its budget effectively. At the macro level, the Government has been working with several development partners in The Gambia. Apart from the International Development Association (IDA), the largest development partners of The Gambia are: the European Union, the African Development Bank, the United Kingdom (DFID) and agencies of the United Nations family. Bilateral donor support is rare. Specifically with regards to EPI, the main partners are: UN agencies (UNICEF/ WHO); International NGOs (Rotary International, Christian Children’s Fund, Catholic Relief Services), Taiwanese Government, Red Cross and The Medical Research Council of the UK. The Gambia is on track to achieve external debt sustainability within the context of the enhanced HIPC initiative. The Gambia has benefited from interim debt relief from IDA, ADB and IMF. As of August 31st 2002 the IDA had approved 30 credits for The Gambia totalling about US$271m. Twenty four credits have been completed and closed and the current portfolio consists of six projects (Participatory Health, Population and Nutrition, Third Education Sector, Poverty Alleviation and Capacity Building, HIV/AIDS Rapid Response, and Capacity Building for Economic Management, and Gateway) totalling US$99m. Future potential sources of funding for the EPI include the funds emanating from debt relief, the extension of the IDA funded Participatory Health, Population and Nutrition Project and the likelihood of a second new health sector project under the IDA to be implemented in September 2005. 1.4. Administrative context
In order to strengthen the involvement and participation of civil society, the Government has embarked upon the reform of the Local Government system in the form of decentralisation. This will have an important impact on civil society and grassroots involvement in participatory planning and monitoring of programmes. The Local Government Act was enacted by Parliament in 2002. It provides the legal and administrative framework to support Area Councils and Municipalities to respond to the developmental needs of their communities, to articulate and elaborate development plans and to encourage community participation. Some steps have been taken in its implementation. However, the process of implementing these reforms has been fraught with controversy and therefore delayed. Furthermore, a key supportive mechanism, the Local Government Finance & Audit Bill, is still yet to be reviewed and enacted by Parliament. Once this Bill is enacted the Local Councils will begin the process of establishing systems towards greater autonomy in decision making, the management of human resources and the financing and delivery of all public services including immunisation within their administrative area. A divisional SWAp system, the Divisional Development Fund, is proposed. This Fund will serve as the repository of all funds derived from donors, central government and locally generated revenue. Integrated divisional plans will be used as the basis for the allocation of the funds.

The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 11 Printed: 3:33 PM 6/17/2004
1.5. Health system context The health system is organised around a three-tier system with increasing complexity in the type and range of services delivered. The Primary Health Care (PHC) or Village Health Services (VHS) are community based services co-financed by government and the communities. The secondary/district level covers major health centres, minor health centres and dispensaries. Four main hospitals now constitute the tertiary level. The policy is to manage the hospitals as semi or autonomous health care providers, with their management boards, and routine management under chief executive officers. These hospitals receive subventions from the Department and report directly to the Secretary of State for Health, through the Permanent Secretary. The Director of Health Services, Chief Pharmacist and Chief Nurse provide policy and regulatory advice to the Secretary of State. The Permanent Secretary serves as the Chief Administrator and Accounting Officer of the Department. The Secretary of State serves as the Chief Executive of the Department. Health sector management also follows a three-tier system. The management of health resources, both human and material remain heavily centralised. Health reforms were embarked upon in 1993 to overcome this centralised decision making through structural changes at the Ministry of Health. Selected administrative and management responsibilities were devolved to the Divisional Health Teams (DHTs). Despite this the DHTs remain functionally weak and powerless especially with respect to human and financial resource management. This has undermined attempts at increasing efficiency of service delivery at divisional and community level due to lack of decision making at community level. Figure 1.1 Organisation of the Health Department In addition, there are the Directorates of Support Services and Social Welfare.
Office of the Secretary of State (Secretary of State, Permanent Secretary and his deputies)
Directorate of Health Services (Director of Health Services, Chief
Pharmacist, Chief Nurse) Health Programme (Child Health and
Survival) Health Services Delivery
Directorate of Planning & Information Policy analysis and Budgeting Health Human Resource Plan Health Systems Research HMIS

The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 12 Printed: 3:33 PM 6/17/2004
1.6. Health Programme Areas Health Programme Areas develop national programme policies and set national strategic targets. There are several vertical programmes. These require considerable administration which place competing demands on service providers at all levels. One of the main areas of focus is Reproductive and Child Health Programme which includes the following: Reproductive Health Integrated Management of Childhood Illness Expanded Programme on Immunization
Figure 1.2 Organisation of delivery of EPI services There are 196 out reach stations (key villages). Each out reach station serves 6-9 satellite villages.
Village 4
Village 5
Village 6
Village 7
Outreach Station 1
Village 1
Village 2 Village 3
HEALTH FACILITY
MCH team (MCH, FP & EPI)
Base clinic Monday & Thursday
Outreach Station 3
Village
Village Village
Outreach Station 2
Village
Village
Village Village 9
Village 8

The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 13 Printed: 3:33 PM 6/17/2004
1.7. Health Services Delivery Health services are provided by both public and private providers. The private sector is expanding mainly with respect to outpatient care. Divisional Health Services are provided through: Major Health Centres (Divisional Hospitals) Minor Health Centres Outreach Clinics (Maternal and Child Health Outreach posts) Community Health Posts (Village health services) Private providers in the division including the Traditional Healers
1.8. Health Policy and Health Public Expenditure Review
The new health Policy Framework, “Changing for Good” was produced to incorporate new socio-economic and health development challenges to ensure access to quality essential health care to the Gambian population. Amongst the key policy issues identified are availability and access to essential drugs and vaccines, and partnership in the financing of health services provision. Public expenditure reviews (PER) are undertaken annually and are aimed at assessing the performance of the health department with regard to the implementation of the Health Policy to identify achievements, failures and obstacles to implementation, as well as available opportunities. During the period 1992–2000, the health recurrent budget showed an upward trend in both nominal and real terms. The recurrent health expenditure, as a share of the total government expenditure, ranged between 10.8% and 13.4%. This represented real per capita recurrent expenditure of US$ 3.96 to US$ 5.91. In 2000, the recurrent expenditure on health as a proportion of the GDP reached 11.17%, which was slightly below the average in sub-Saharan Africa. The public expenditure per capita in the health sector in 2000 was US$ 6, which was just half of the WHO recommended standard required to provide minimum health care services. 1.9. Budget Process and Financial Management
The national budget development process begins with the release of the call circular for the Department of State for Finance and Economic Affairs (Finance) to all government funded departments and institutions. The call circular explains the revenue forecast for the year being planned for, the budget policies and the allocations to the departments and institutions. Since, 2002, a national budget meeting is also organised, where all the stakeholders including civil society meet to discuss the “sharing of the national cake”. This forum is used to explain the rationale behind the allocations. It also serves as an opportunity for PRSP priority sectors, of which EPI is one, to provide an update on their activities and funding constraints. The departments then proceed to make their budgets in line with what they consider their priority areas. This is followed by budget bilateral meetings (between Finance and the departmental budget team), where Finance, in addition to assessing for allocative efficiency, pays special attention to compliance to the allocation ceiling. Within Health, over the last two years discussion of the Health Agenda have preceded discussions on the annual budget. These discussions are then followed by further inter-departmental

The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 14 Printed: 3:33 PM 6/17/2004
discussions regarding sharing of the allocated health budget. For the 2003 budget preparation, even the allocations for the purchase of health goods like drugs, fuel for ambulances and vaccines were discussed and agreed upon. For the 2004 budget preparation, in addition to discussions of the intra-departmental sharing formula, a major addition was the setting up of per capita allocations targets for drugs, vaccines and food for in-patients. These per capita targets form the basis for bilateral negotiation with Finance. It is hoped that future negotiations between Health and Finance will use this mechanism for allocating funds. This approach has been used for the funding of drugs, vaccines and food at the divisional level based on the size of the population within the division. The HIPC funds allocation to Health for the past two years supports priority areas, like vaccines and essential drugs purchase. From 2004 however, HIPC fund to Health is considered as investment in the form of seed capital for essential drugs and vaccines. The Government Local Fund allocations to divisions would then be used to purchase from the Essential Drugs and Vaccines Supply System based in the Central Medical Stores. 1.10. Budgeting, Financial management systems
1.10.1. Financial Information System (IFMIS) Finance is at an advanced stage in the establishment of an Integrated Financial Management Information System (IFMIS). For a start the system would include the PRSP priority sectors. Within Health, a new computer has been allocated to the Accounts Unit to improve on the tracking of health expenditure. 1.10.2. Disbursement System Disbursement to sectors/departments is influenced by revenue generation capacity. The main source of revenue for The Gambia is from taxation, and unfortunately the base for taxation is very small. Previously, quarterly allocations were disbursed to department including the EPI Unit. The traditional approach for disbursement to departments has been quarterly allocations, however, this could not be maintained for the 2003 budget. The Department of Finance embarked on prudent expenditure control measure, and a monthly cash flow budget system was introduced. With the cash flow budget, departments are provided monthly budget “envelopes”, and they decide on their budget line allocations, and present their expenditure to the National Emergency Finance Committee (NEFCOM) for review, before payments are processed. This means that disbursements may not always match requests and delays can be experienced in accessing allocated funds. For EPI divisional activities funds are normally controlled and released by the Central EPI Unit to the DHTs. This disbursement can lead to delays in the implementation of divisional activities.

The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 15 Printed: 3:33 PM 6/17/2004
1.11. Accounting and Audit The departmental accounts units process payments and maintain the books of accounts (cash book and vote charge books) The Internal Audit department of Finance serves as the clearing house for all the payment requests. The Accountant General Department ensures adherence to the Financial Instructions before payments are finally effected. One of the agreements from discussions of the Country Financial Accountability Assessment report was the production of the Auditor General’s Opinion on the annual financial report provided by the Accountant General. 1.12. Health Financing Information
Funding has been secured from the Participatory Health Population and Nutrition Project to conduct the National Health Accounts (NHA) for 2001 and 2002. It is hoped that this report would guide the Department of Health in designing the Health Financing Policy. The Health Policy “ Changing for Good” advocates for basket funding, The World Bank has taken the lead in this area by supporting the design of a health development strategic Plan using SWAp. In addition, the new health policy identifies the Essential Care Package for The Gambia, as the benefit package for which government will provide financial support.
The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 16 Printed: 3:33 PM 6/17/2004
SECTION 2 2. Expanded Programme on Immunization: Characteristics, Objectives and
Strategies 2.1. Background
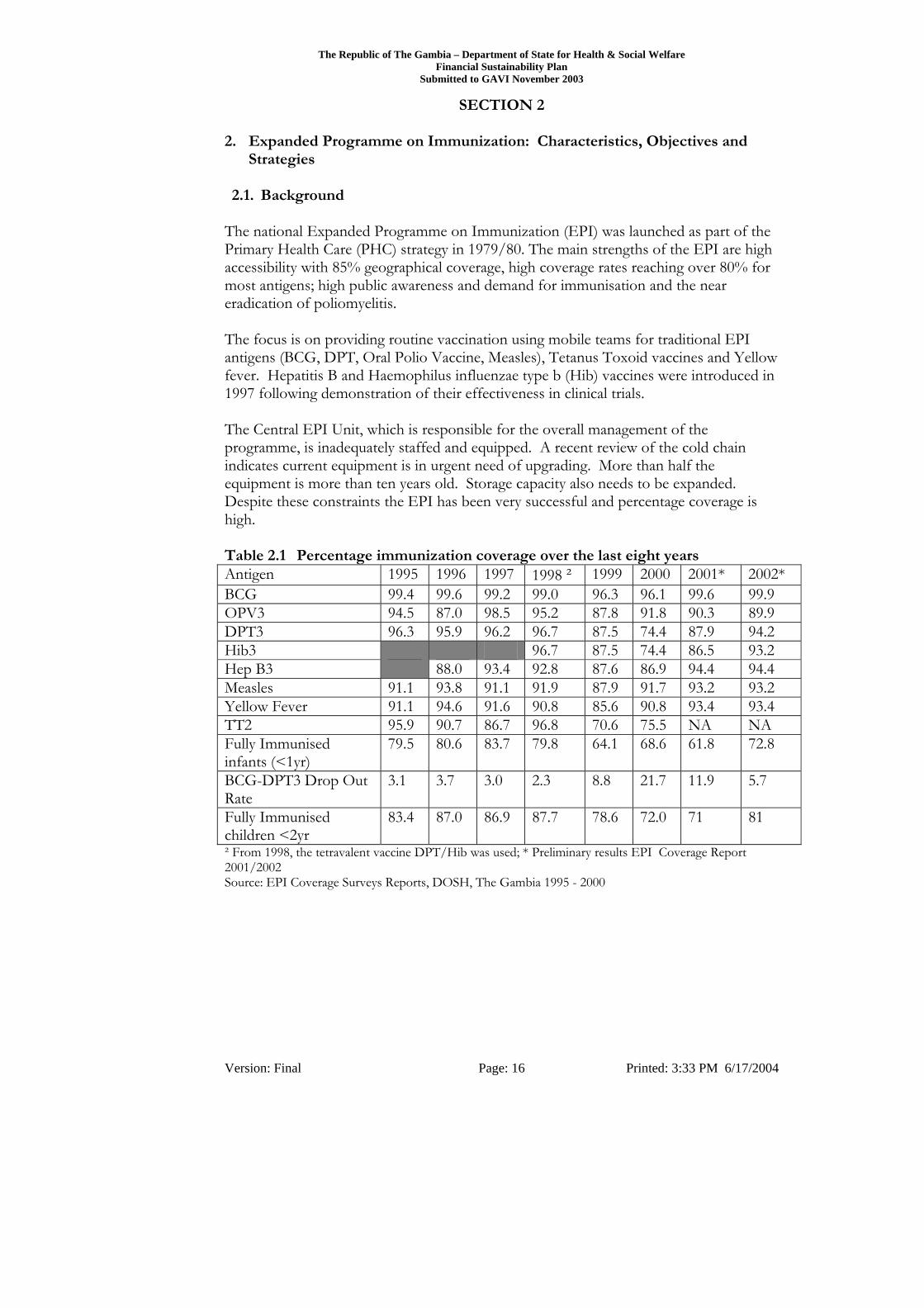
The national Expanded Programme on Immunization (EPI) was launched as part of the Primary Health Care (PHC) strategy in 1979/80. The main strengths of the EPI are high accessibility with 85% geographical coverage, high coverage rates reaching over 80% for most antigens; high public awareness and demand for immunisation and the near eradication of poliomyelitis. The focus is on providing routine vaccination using mobile teams for traditional EPI antigens (BCG, DPT, Oral Polio Vaccine, Measles), Tetanus Toxoid vaccines and Yellow fever. Hepatitis B and Haemophilus influenzae type b (Hib) vaccines were introduced in 1997 following demonstration of their effectiveness in clinical trials. The Central EPI Unit, which is responsible for the overall management of the programme, is inadequately staffed and equipped. A recent review of the cold chain indicates current equipment is in urgent need of upgrading. More than half the equipment is more than ten years old. Storage capacity also needs to be expanded. Despite these constraints the EPI has been very successful and percentage coverage is high. Table 2.1 Percentage immunization coverage over the last eight years Antigen 1995 1996 1997 1998 ² 1999 2000 2001* 2002* BCG 99.4 99.6 99.2 99.0 96.3 96.1 99.6 99.9 OPV3 94.5 87.0 98.5 95.2 87.8 91.8 90.3 89.9 DPT3 96.3 95.9 96.2 96.7 87.5 74.4 87.9 94.2 Hib3 96.7 87.5 74.4 86.5 93.2 Hep B3 88.0 93.4 92.8 87.6 86.9 94.4 94.4 Measles 91.1 93.8 91.1 91.9 87.9 91.7 93.2 93.2 Yellow Fever 91.1 94.6 91.6 90.8 85.6 90.8 93.4 93.4 TT2 95.9 90.7 86.7 96.8 70.6 75.5 NA NA Fully Immunised infants (<1yr)
79.5 80.6 83.7 79.8 64.1 68.6 61.8 72.8
BCG-DPT3 Drop Out Rate
3.1 3.7 3.0 2.3 8.8 21.7 11.9 5.7
Fully Immunised children <2yr
83.4 87.0 86.9 87.7 78.6 72.0 71 81
² From 1998, the tetravalent vaccine DPT/Hib was used; * Preliminary results EPI Coverage Report 2001/2002 Source: EPI Coverage Surveys Reports, DOSH, The Gambia 1995 - 2000
The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 17 Printed: 3:33 PM 6/17/2004
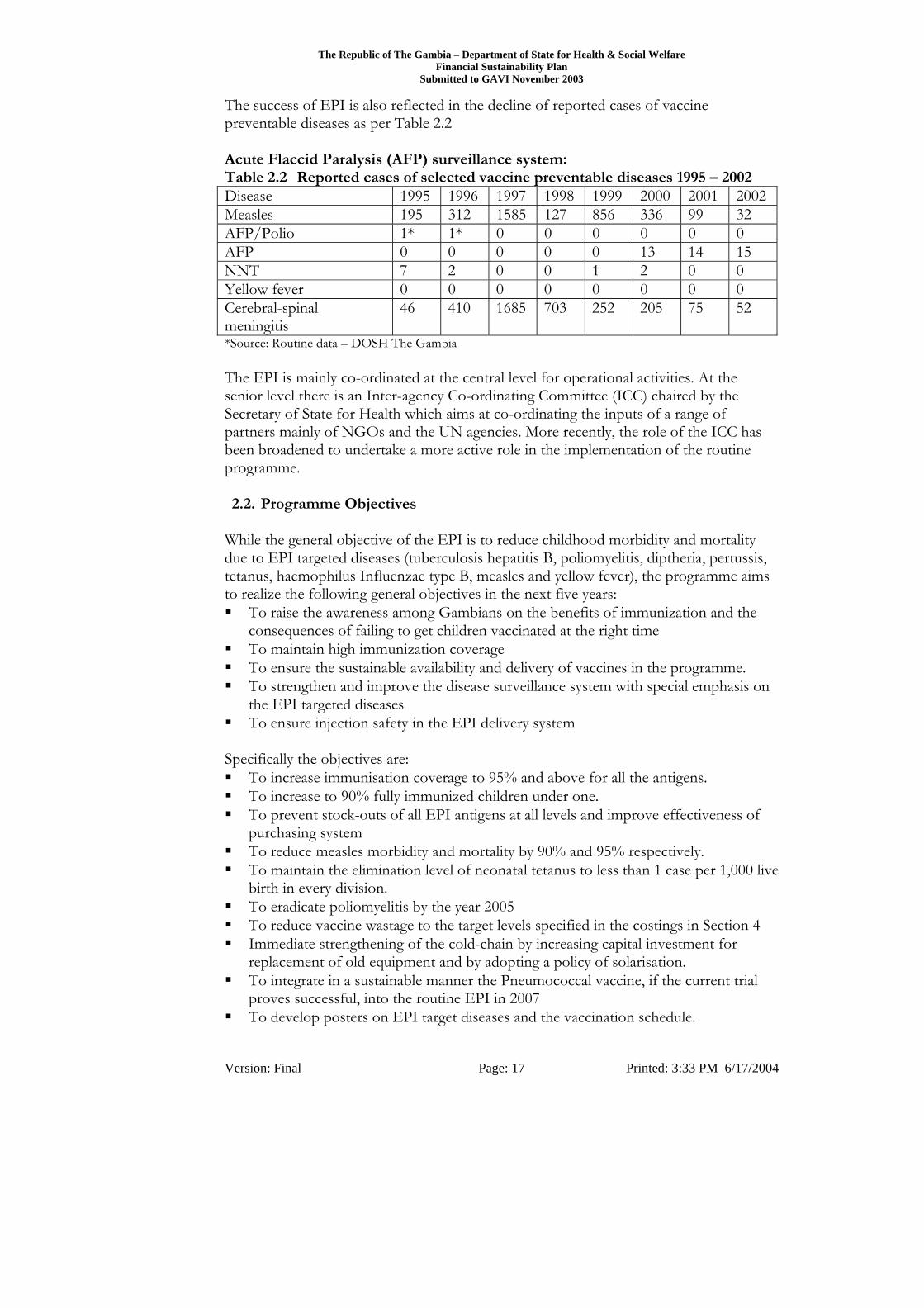
The success of EPI is also reflected in the decline of reported cases of vaccine preventable diseases as per Table 2.2 Acute Flaccid Paralysis (AFP) surveillance system: Table 2.2 Reported cases of selected vaccine preventable diseases 1995 – 2002 Disease 1995 1996 1997 1998 1999 2000 2001 2002Measles 195 312 1585 127 856 336 99 32 AFP/Polio 1* 1* 0 0 0 0 0 0 AFP 0 0 0 0 0 13 14 15 NNT 7 2 0 0 1 2 0 0 Yellow fever 0 0 0 0 0 0 0 0 Cerebral-spinal meningitis
46 410 1685 703 252 205 75 52
*Source: Routine data – DOSH The Gambia The EPI is mainly co-ordinated at the central level for operational activities. At the senior level there is an Inter-agency Co-ordinating Committee (ICC) chaired by the Secretary of State for Health which aims at co-ordinating the inputs of a range of partners mainly of NGOs and the UN agencies. More recently, the role of the ICC has been broadened to undertake a more active role in the implementation of the routine programme. 2.2. Programme Objectives
While the general objective of the EPI is to reduce childhood morbidity and mortality due to EPI targeted diseases (tuberculosis hepatitis B, poliomyelitis, diptheria, pertussis, tetanus, haemophilus Influenzae type B, measles and yellow fever), the programme aims to realize the following general objectives in the next five years: To raise the awareness among Gambians on the benefits of immunization and the
consequences of failing to get children vaccinated at the right time To maintain high immunization coverage To ensure the sustainable availability and delivery of vaccines in the programme. To strengthen and improve the disease surveillance system with special emphasis on
the EPI targeted diseases To ensure injection safety in the EPI delivery system
Specifically the objectives are: To increase immunisation coverage to 95% and above for all the antigens. To increase to 90% fully immunized children under one. To prevent stock-outs of all EPI antigens at all levels and improve effectiveness of
purchasing system To reduce measles morbidity and mortality by 90% and 95% respectively. To maintain the elimination level of neonatal tetanus to less than 1 case per 1,000 live
birth in every division. To eradicate poliomyelitis by the year 2005 To reduce vaccine wastage to the target levels specified in the costings in Section 4 Immediate strengthening of the cold-chain by increasing capital investment for
replacement of old equipment and by adopting a policy of solarisation. To integrate in a sustainable manner the Pneumococcal vaccine, if the current trial
proves successful, into the routine EPI in 2007 To develop posters on EPI target diseases and the vaccination schedule.

The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 18 Printed: 3:33 PM 6/17/2004
To develop key messages on immunization targeting parents and care-givers. To continue to use auto disposable (AD) syringes for all EPI vaccinations. To ensure the use and proper disposal of safety boxes by all facilities conducting
immunization services There has however been increasing concern over the ageing cold chain system; the erratic financing of the EPI, and the number of children below the age of one who are not fully immunised. Figure 2.1:
Proportion of children fully immunised less than 12 months
0
20
40
60
80
100
95 96 97 98 99 2000 2001 2002
year
per
cent
*Source: EPI Coverage Surveys Reports, DOSH, The Gambia 1995- 2000 Also of concern is the high wastage rate of vaccines. From recent data vaccine wastage is estimated to range from 17% to 60%. The study did not identify reasons for high wastage rates. A further concern was the recent increase in drop out rates in 2000 and 2001. Recent coverage surveys indicate that drop out rates have been reduced to acceptable levels. Cold Chain Equipment The total cold chain equipment available in the country is 85. Of these, 59 are located at the various facilities of which 18 are at the DHT stores. There is inadequate capacity for storage (for 0 to 8ºC) including freezing capacity at the national level. About 50% of the total equipment is solar (Electrolux RCW 42 DC). The main energy source used in operating refrigerators at the periphery is solar. Electric compression and absorption equipment are installed at national and divisional level vaccine stores.

The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 19 Printed: 3:33 PM 6/17/2004
2.3. Vaccine Procurement and Financing Prior to 1998, traditional donor agencies, mainly UNICEF, assumed responsibility for the procurement of routine vaccines (the traditional six antigens and yellow fever) and the maintenance of the cold chain system. Financing for the procurement of Hepatitis B and Hib has been precarious and heavily dependent on external donors, namely ADB and more recently the Italian government. In 1998, the financial support provided by UNICEF ceased. Prior to and after this period, UNICEF continued to facilitate the process of seeking alternative sources of finance from external donors. The Gambia became a signatory for the Vaccine Independent Initiative (VII) for Sahelian countries in January 1999 for a period of two years. The EU pledged a total of US$250,000 from regional counterpart funds for the procurement of routine vaccines. In 1999, as part of the agreement the Government created a budget line specifically for vaccines and supplies. In 2000 and 2001 funds allocated for the procurement of vaccines amounted to US$131,275 and US$111,542 respectively. From data derived from the recent EPI Financing study in 2001, the government contribution in 2000 and 2001 as a proportion of total cost was 26% and 22% respectively. The contribution of the Government of The Gambia (GoG) was mainly in the area of operating costs: personnel salaries, maintenance of health facilities and vehicles. A number of other partners also contributed to the financing of the National Immunization Days, notable amongst these are the World Health Organization, the Participatory Health and Nutrition Project (IDA Project), Christian Children Fund and others. The EPI Financing Study also revealed that the annual cost of the EPI taking into consideration capital and recurrent costs was nearly 35% higher than previously estimated. The major contributors to this cost are vaccines and the lack of investment in cold chain equipment. The outreach strategy is over 60% more costly than the fixed strategy, which is reflected in the differences also realised in fully immunising children with the alternative strategies. Overall, at US$37, the cost of fully immunizing a Gambian child is considerably higher than is the case for other countries where comparable data exists in the sub-region. 2.4. Programme Management
There is a need to strengthen the managerial and technical capacity of the management of the national programme. But equally is the need to strengthen the integrated management of Reproductive and Child Health programmes. The Reproductive and Child Health Programme Manager under the technical directive of the Director of Health Services should co-ordinate the activities of the three programmes of Reproductive health, Integrated Management of Childhood Illnesses and Expanded Programme on Immunisation. The procurement of the vaccines has been satisfactory so far. The major constraint is in the safe and proper storage of the vaccines. The construction of a multi-purpose warehouse funded by the African Development Bank has been mentioned several times, however, the definite time frame for the commencement and completion of this work has not been made known. Details on this warehouse construction need to be provided.
The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 20 Printed: 3:33 PM 6/17/2004
Until the time that more information is available on the new warehouse, the requirement for quarterly vaccine delivery to the central store will need to continue. The storage facilities in Banjul are to serve as transit and buffer stock stores. There is a need to have at Central level (Banjul) a cold room for storage of a minimum of 5 months national vaccines stock. 2.5. Transportation and storage of vaccines
The EPI services, which are integrated into the MCH services, are delivered using fixed and outreach delivery sites. Thus reliance on transportation remains a key concern. This will be more so in the future when the existing 196 outreach delivery points are transformed to fixed Community Health Posts with a full staff complement to deliver integrated services. The need for reliable transport for out reach services will be a focus of the Multi-year plan. This will be addressed mainly through the provision of reliable vehicles and support for a replacement and maintenance plan. The use of the two refrigerated vans used as carriers available to the Programme needs to be reviewed. The present indiscriminate use of the vans is a concern for their life span. These carriers could support vaccines distribution to the divisional/regional medical stores. The reform proposed is for the vans to also support vaccines distribution to providers in the Western region- Western division, Kanifing Municipal area and Banjul city area. For distribution in the other divisions (five), there is a need for small distribution vans for each of them. A major threat to vaccines is the storage quality in the divisional stores and at health facilities. There is need to invest in solar refrigeration, due to the erratic nature of electricity supply services, at the divisional medical stores and in all the other vaccines storage facilities countrywide. The Divisional Public Health Officer (Manager of Divisional Disease Control) should take full responsibility of both the vaccines inventory control and cold chain monitoring 2.6. Financing the National Immunisation Programme
There are other proposed reforms in the management of the National Essential Drugs and Vaccines Supply system. The Central Medical Stores would be converted to an autonomous Supplies Institution, with its own management board, procurement system, and accounting department. A good portion of HIPC funds allocated to Health in the next few years would be used to capitalise this new medical supplies organisation. This would ensure availability of routine vaccines in the country. Partnership would be pursued in the following areas: Introduction and purchase of newer vaccines Human resource capacity development National Immunization Days Strengthening the distribution and cold chain systems and immunisation safety Research into newer vaccines Expansion of service delivery points.

The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 21 Printed: 3:33 PM 6/17/2004
2.7. Payment of service providers The important assumption here is that all the health care providers would maintain their own revenue accounts. Providers would have to purchase their vaccines at the divisional supplies depots. The payment mechanism to providers would be defined in the new Health Financing Policy to be developed. A National Health Insurance is an option which would include Community Micro-Health Insurance, however, immunisation as a public health good would remain funded by Government. 2.8. Plans for the future
In the next five years the focus will be on the recruitment of new staff and capacity building of existing central and divisional staff with a focus on programme managers and logistics, surveillance, data management and social mobilisation. The rehabilitation and expansion of the cold chain system nationwide including changing all CFC refrigerators to non-CFC refrigerators; the provision of supporting infrastructure, for example generators and the expansion of storage capacity centrally and within the divisions. SIAs will continue for measles, the integrated EPI/ Vitamin A supplementation programme will be strengthened as will the use of injection safety materials. New vaccines likely to be implemented include Pneumococcal once the results of the trial are known.
The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 22 Printed: 3:33 PM 6/17/2004
SECTION 3 3. Current Expenditure & Financing 3.1. Introduction
The current programme costs and financing are based on a comprehensive review of the EPI program. Due to the relatively small size of the country data was collected on EPI in all divisions and from all health facilities rather than taking sample data. Data collection took place from June to August 2003. The basis for calculation of the data requirements for Section 3 is according to the methodology of the FSP guidelines and assumptions outlined in Appendix B. Areas of particular interest in assessing current cost which required additional data collection and analysis were: Vaccine costs and vaccine wastage Transport costs Personnel costs Cold chain investment
The baseline year has been costed using the standard cost model. The current year was not complete at time of writing and costs were estimated using the forecasting tool. Where possible 2002 costs were calculated in the forecasting tool to ensure consistency of data. It should be noted capital costs were assumed to remain unchanged between the baseline and the current year. 3.2. Baseline and Current Program Costs
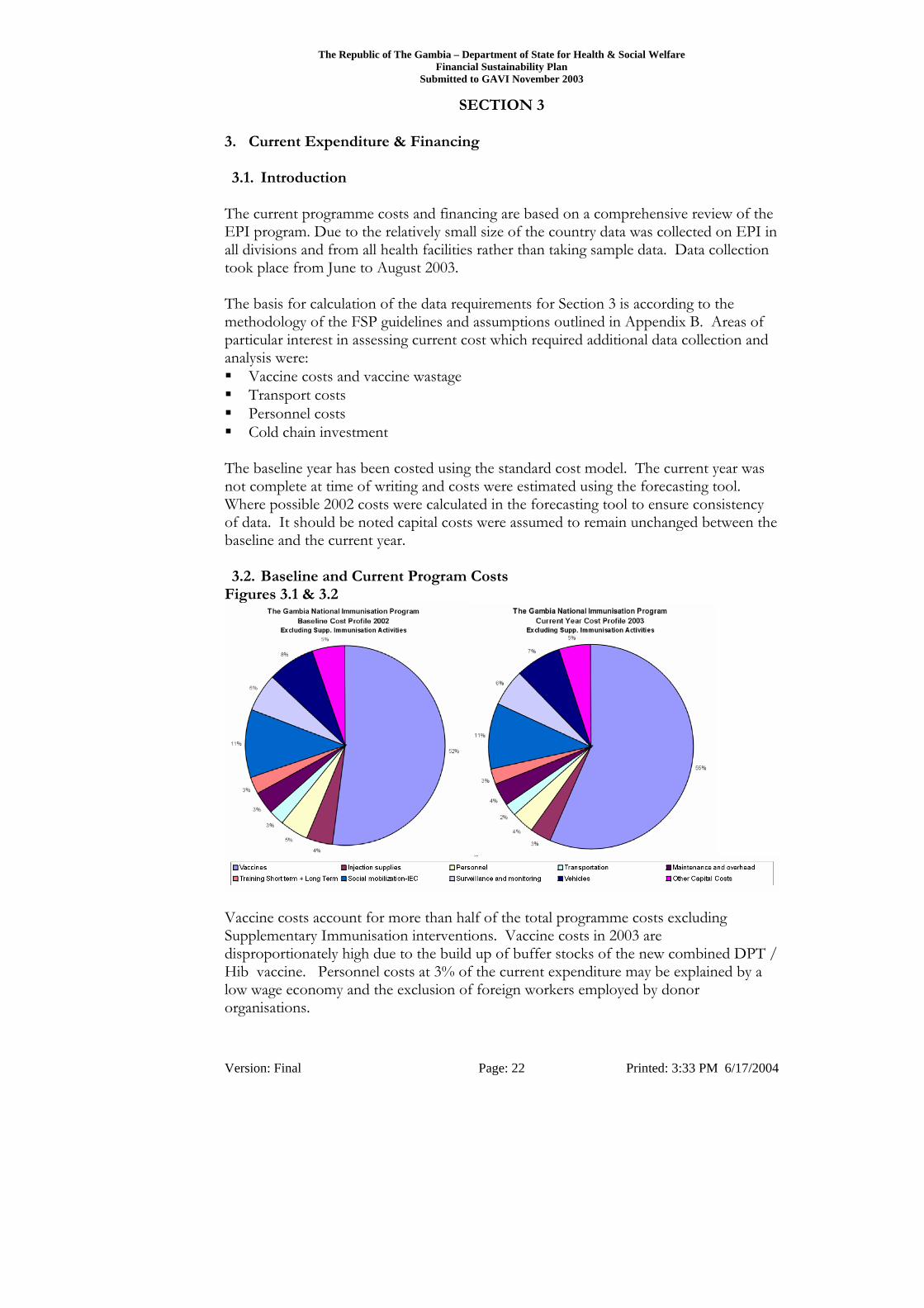
Figures 3.1 & 3.2
Vaccine costs account for more than half of the total programme costs excluding Supplementary Immunisation interventions. Vaccine costs in 2003 are disproportionately high due to the build up of buffer stocks of the new combined DPT / Hib vaccine. Personnel costs at 3% of the current expenditure may be explained by a low wage economy and the exclusion of foreign workers employed by donor organisations.

The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 23 Printed: 3:33 PM 6/17/2004
Total programme costs are summarised below and is compiled from the total of costs exclusive to the EPI programme and the programmes allocation of shared costs. Table 3.0: FSP Table 3.1 and 3.2 Baseline and Current Year Costing 2002 2003 Program Costing Total US$ Share (%) Total US$ Share (%)
Operational Cost
Vaccines 858,669 43.6% 52.0% 997,973 38.5% 56.3% Injection supplies 68,761 3.5% 4.2% 61,939 2.4% 3.5% Personnel 75,266 3.8% 4.6% 63,537 2.5% 3.6% Transportation 44,013 2.2% 2.7% 33,699 1.3% 1.9% Maintenance and overhead 56,437 2.9% 3.4% 62,057 2.4% 3.5% Training Short term + Long Term 45,936 2.3% 2.8% 46,344 1.8% 2.6% Social mobilization-IEC 183,107 9.3% 11.1% 186,769 7.2% 10.5% Surveillance and monitoring 100,723 5.1% 6.1% 102,738 4.0% 5.8%
Subtotal Operational $1,432,913 72.7% 86.8% $1,555,055 60.0% 87.7%
Capital Cost
Vehicles 129,742 6.6% 7.9% 129,742 5.0% 7.3% Other Capital Costs 87,452 4.4% 5.3% 87,452 3.4% 4.9%
Subtotal Capital $217,194 11.0% 13.2% $217,194 8.4% 12.3%
TOTAL Excluding SIAs $1,650,107 84% 100% $1,772,250 68% 100%
Polio Vaccines for NID 67,281 3.4% 435,688 16.8% Measles Vaccines for NID 252,518 12.8% 385,225 14.9% Subtotal Supplementary Immunisation Activities $319,799 16.2% $820,913 31.7%
GRAND TOTAL $1,969,906 100% $2,593,163 100% Vaccines Vaccines account for 64% of routine recurrent cost (52% of total programme costs excluding SIAs in 2002) and are a major component of the EPI program. Vaccine Wastage Vaccine Costs are exacerbated by high wastage levels particularly in the case of reconstituted drugs. Table 3.3 Wastage Levels Summary Vaccines Vial Size Wastage Reconstituted Vaccines BCG 20 55.2% Measles 10 60.2% Yellow Fever 10 56.1% Other Injection Vaccines DPT 10 21.0% Hib 10 33.2% Tetanus (TT) 20 27.2% Hep B 10 20.7% Other Vaccine Polio (OPV) 20 26.2%
Note: Wastage calculated as percentage of total vaccine used.

The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 24 Printed: 3:33 PM 6/17/2004
Detailed analysis of the wastage and how it was calculated is provided by the costing model and supported by supplement information in Appendix B The country policy is to provide immunisations on demand to ensure maximisation of coverage of immunisation. This approach means that vials of vaccine are generally not fully utilised. If only one immunisation is given from a vial of BCG vaccine, 19 potential doses are wasted. It is clear however that there is an opportunity for cost savings for improved vaccine stock management are substantial. EPI Personnel Personnel costs are very low as a percentage of the total delivery costs. Health Sector staff salaries are set by central government and have been consistently declining in US$ terms as the local currency devalues. Low salary rates have resulted in high staff turnover which has the following negative impacts: • Training costs remain high as new staff have to be trained to replace experienced
staff leaving the health system. • Remaining staff have inadequate training and experience leading to:
o High wastage levels of Vaccine. o Cold Chain and other Equipment not properly maintained.
Cold Chain Equipment A recent review of cold chain equipment2 demonstrated that there is insufficient capacity and that equipment is overdue for replacement and often no longer functional. A substantial proportion of the solar fridges are fifteen year old and have become unserviceable as replacement batteries and other key parts are no longer available. The government is working with various funding agencies to obtain replacement equipment. Incinerators Incinerators are old and often inoperable. It is planned to introduce 11 new incinerators at a total cost of US$38,500.
2 “COLD CHAIN ASSESSMENT IN THE GAMBIA Trip Report” Author: Souleymane Kone; ICP/EPI-Log, WHO/Abidjan Dates: 28 April to 2 May 2003

The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 25 Printed: 3:33 PM 6/17/2004
3.3. Baseline and Current Program Cost Funding Figure 3.3:
The Gambia National Immunisation ProgrammeFinancing of Recurrent EPI Activities - Baseline 2002
Excluding Capital Costs & Supplementary Implementation Activities
31%
13%
8%
28%
16%
3%
1%0%
National Government
UNICEF
WHO
Aventis Pasteur
MRC
CISP
Cadre Du Project
GAVI
Baseline Year 2002 Table 3.4: Funding Sources 2002 Funded by Items Funded Value
$,000 % Cost
Aventis Pasteur HIB vaccine – field trial 414 21% UNICEF Supplementary Immunisation
Activities, Vaccines, Per diems, Training
438 22%
MRC Hib / DPT Vaccine – Donation agreed for period of Pneumococcal field trial.
228 12%
WHO Monitoring & Disease Surveillance, Supplementary Immunisation Activities, Vaccines, Per diems, Training
168 9%
Other Donor Capital Purchases, vaccines, training 252 13% Government Traditional Vaccine, Infrastructure,
Personnel, IEC Social Mobilisation. 451 23%
Total 1,969 100%

The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 26 Printed: 3:33 PM 6/17/2004
Figure 3.4:
The Gambia National Immunisation ProgrammeFinancing of Recurrent EPI Acctivities - Current Year 2003
Excluding Capital Costs & Supplementary Implementation Activities
19%
13%
4%
0%
14%
0%0%
50%
NationalGovernmentUNICEF
WHO
Aventis Pasteur
MRC
CISP
Cadre Du Project
GAVI
Historically The Gambia has benefited from participation in field trial of new vaccines given its size and population. In the baseline year reliance was placed upon the donations of Hib vaccine from Aventis Pasteur and the Medical Research Council. Since the market cost of Hib vaccine is high in comparison to traditional vaccines, this equated to funding equivalent to 73% of vaccine costs and 38% of the total routine program budget. The Government contribution is recurrent corresponding mainly to traditional vaccines, personnel, logistics and cold chain maintenance. The Medical Research Council (MRC) vaccine trial commenced in 2000 and provided supplies of Hib and DPT vaccine as part of funded trial of the Pneumococcal vaccine covering the Upper and Central River Divisions. The immunisation phase of the MRC trial ended in April 2003, however, excess stocks from the trial have continued to be made available to these divisions. It is anticipated that these immunisation supplies will be exhausted by the end of 2003 resulting in an increased funding gap. Aventis Pasteur provided donations of Hib as part of a vaccine trial which was completed in 2001. Following the end of the trial, as part of an agreement with the Government, Aventis Pasteur agreed to donate a total of one million dose of the vaccine over a period of 5 years. The remaining stocks from this donation continued to be utilised until finally exhausted in October 2003. The funding gap has been filled by the provision of the combined DPT + Hib vaccine under the GAVI programme.
Comment [A1]: pladonors

The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 27 Printed: 3:33 PM 6/17/2004
UNICEF is the main long term support partner of The Gambia Expanded Program on Immunization. UNICEF was in charge of vaccines and material of vaccinations and cold chain; office equipment and supplies also fuel. From1999 to 2002, the Italian Government, through UNICEF provided temporary funding for provision of HepB Vaccine which was replaced through GAVI support in 2003. WHO contribute for the financing of EPI routine activities and is one of the main funding sources for NIDs. support . CISP and Cadre Du Project – Limited targeted funding has been provided by these donors. There is no ongoing long term agreement. Areas councils provide personnel (labourer for cleansing service) for health services and chairs, tables and benches for outreach stations. Due to lack of information, the estimation of their contributions remains unquantified. Capital equipment has been funded through a broad spectrum of donor agencies on an add hoc basis. GAVI funding of the programme began in November 2002 with initial funding of US$100,000. This was used to supplement government expenditure and donor funding. The change in funding received in the baseline 2002 versus the current year 2003 is contrasted below: Figure 3.5:
Funding Comparison - Baseline 2002 v Current Year 2003 Excluding Supp. Immunisation Activities and Capital Costs
-
200,000
400,000
600,000
800,000
1,000,000
1,200,000
1,400,000
1,600,000
1,800,000
2002 2003
Year
Tota
l Fun
ding
GAVICadre Du ProjectCISPMRCAventis PasteurWHOUNICEFNational Government
The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 28 Printed: 3:33 PM 6/17/2004
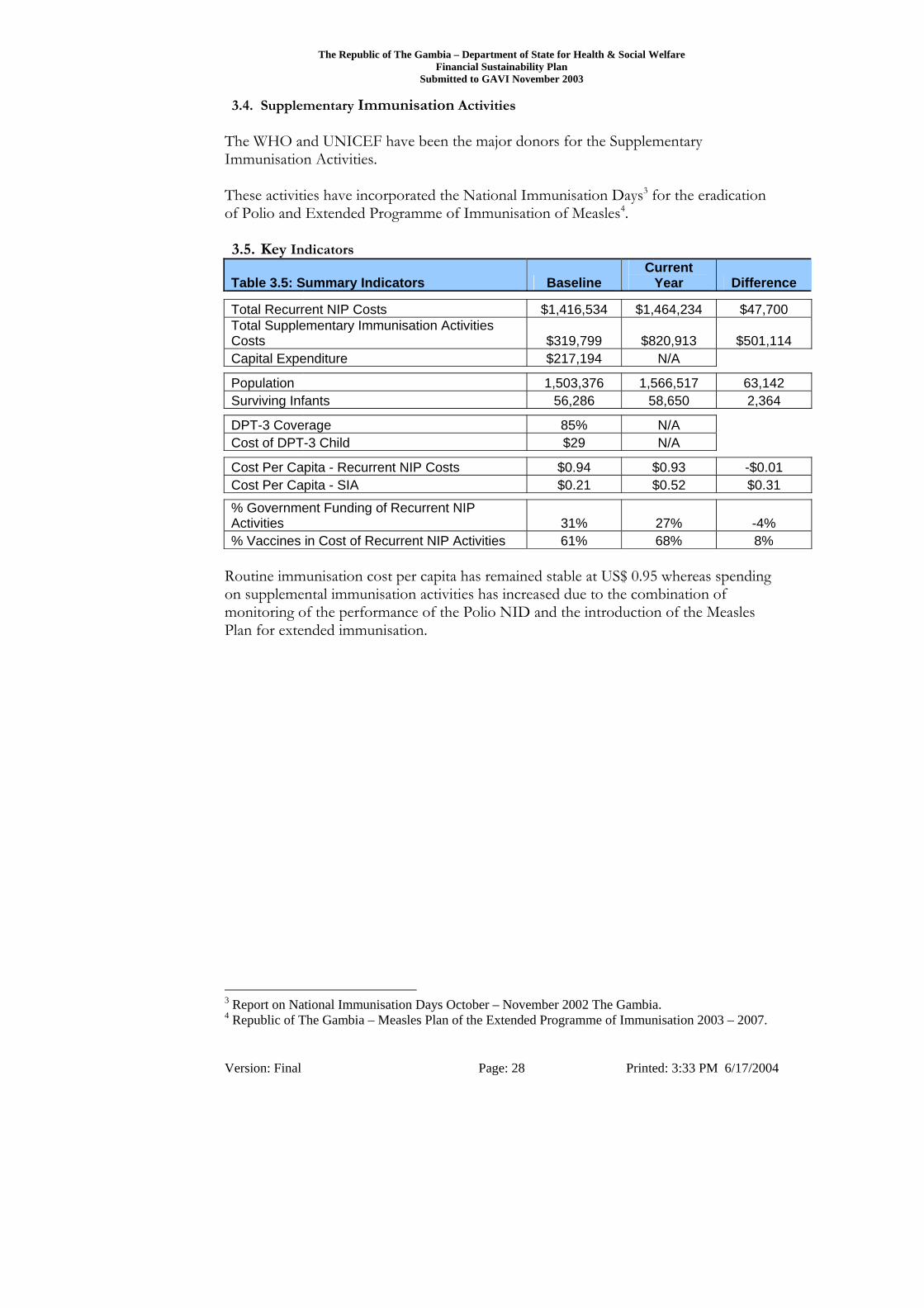
3.4. Supplementary Immunisation Activities The WHO and UNICEF have been the major donors for the Supplementary Immunisation Activities. These activities have incorporated the National Immunisation Days3 for the eradication of Polio and Extended Programme of Immunisation of Measles4. 3.5. Key Indicators
Table 3.5: Summary Indicators Baseline Current
Year Difference
Total Recurrent NIP Costs $1,416,534 $1,464,234 $47,700 Total Supplementary Immunisation Activities Costs $319,799 $820,913 $501,114 Capital Expenditure $217,194 N/A
Population 1,503,376 1,566,517 63,142 Surviving Infants 56,286 58,650 2,364
DPT-3 Coverage 85% N/A Cost of DPT-3 Child $29 N/A
Cost Per Capita - Recurrent NIP Costs $0.94 $0.93 -$0.01 Cost Per Capita - SIA $0.21 $0.52 $0.31
% Government Funding of Recurrent NIP Activities 31% 27% -4% % Vaccines in Cost of Recurrent NIP Activities 61% 68% 8%
Routine immunisation cost per capita has remained stable at US$ 0.95 whereas spending on supplemental immunisation activities has increased due to the combination of monitoring of the performance of the Polio NID and the introduction of the Measles Plan for extended immunisation.
3 Report on National Immunisation Days October – November 2002 The Gambia. 4 Republic of The Gambia – Measles Plan of the Extended Programme of Immunisation 2003 – 2007.

The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 29 Printed: 3:33 PM 6/17/2004
SECTION 4 4. Future Resource Requirements and Programme Financing. 4.1. FSP Cost Projections
In developing the Financial Sustainability Plan, future costings and sources of finance have been forecast for future programme costs for the period 2003 – 2012 utilising the baseline information from 2002 compiled in Section 3. The forecast were projected for the Vaccine Fund Period 2003-2007 and the Post Vaccine Fund period 2008-2012.
-
500,000
1,000,000
1,500,000
2,000,000
2,500,000
3,000,000
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
Other optional information
Shared personnel costs
Measles
Polio
Other capital costs
Cold chain equipment
Vehicles
Other recurrent costs
Transportation
Personnel
Injection supplies
New Vaccines
Traditional vaccines
Figure 4.1 : Projections of Future Resource Needs by Cost Categories
The Total Projected Costs are summarised in the following table. Table 4.1:
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 $,000 $,000 $,000 $,000 $,000 $,000 $,000 $,000 $,000 $,000
2,516 1,846 1,841 1,898 1,717 1,748 1,844 1,943 1,931 1,957 To maintain consistency in the cost forecast for the EPI programme over the projection period a number of assumptions have been made. These assumptions are:
Population growth rate is 4.2% Current coverage rates are expected to be maintained or improved Current structure is maintained subject to phased enhancement set out below Implementation of strategic policies to improve the services provided by the
EPI programme Current exchange rates are assumed and all values are expressed in US$ A scenario for the introduction of Pneumococcal vaccine from 2007 is costed
separately. An explanation of the assumptions made for each cost category and detailed analysis of the individual costings and schedules are provided in Appendices E and F.

The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 30 Printed: 3:33 PM 6/17/2004
4.2. Strategic Initiatives Planned for and incorporated in the Forecast Period 2003 - 2012
The information compiled in the Section 3 highlighted three strategic issues that needed to be addressed:
Reduction in vaccine wastage Strengthening of the cold chain Improvement in service delivery
The projections for future programme costs and financing are therefore based upon addressing these strategic issues are as follows: 4.2.1. Reduction of Vaccine Wastage: Vaccine currently accounts for 64% of recurrent programme costs. Wastage levels are unacceptably high. In the future the primary focus in instituting cost saving must be the reduction of these wastage levels. A targeted reduction of vaccine wastage over a period of five years is set out in the following table:
Table 4.2: Projected Vaccine Wastage Savings Vaccines Vial Size Current Wastage Target
WastageEstimated Savings In
2008 Reconstituted Vaccines Doses Savings BCG 20 55% 30% 55,061 $4,033 Measles 10 60% 30% 74,092 $10,558 Yellow Fever 10 56% 30% 58,275 $43,347Other Injection Vaccines DPT/Hib 10 21%-33% 15% 73,768 $169,285 Tetanus (TT) 20 27% 15% 52,815 $2,161 Hep B 10 21% 15% 17,830 $6,048Other Vaccine Polio (OPV) 20 26% 15% 50,015 $4,775 $240,207
To achieve these savings the forecast has costed the following actions:
Recruitment of two additional staff with exclusive responsibility for vaccine wastage reduction.
Additional training in management information systems, and management. Improvement of computer hardware and information management systems. Changes in service delivery.

The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 31 Printed: 3:33 PM 6/17/2004
4.2.2. Strengthening the Cold chain. As has been highlighted there is insufficient capacity in the cold chain, equipment is overdue for replacement and often no longer functional. A substantial proportion of the solar fridges are fifteen year old and have become unserviceable as replacement batteries and other key parts are no longer available. Provision has therefore been made for:
Adopting a policy of solarisation Provision of central cold store facility Replacing outdated equipment
4.2.3. Improvement in Service Delivery It is proposed that there be a change in policy on service delivery. This new policy will focus on the delivery of enhanced vaccination services utilising the existing community based health service. Provision has therefore been made for:
Recruitment of additional Public Health Officers (PHOs) to work in association with existing Community Health Nurses to provide immunisation services.
Provision of motorcycles for mobilisation of the PHOs and distribution of the vaccine from safe storage located at the fixed health facilities to the community.
Training the CHNs and newly recruited PHOs.
This has the additional benefit of freeing up scarce nursing resource and the use of ambulances for emergency and other uses and ensure that EPI activities are not hindered when the ambulances are unavailable. A detailed analysis of the costing of recurrent and capital cost for the Vaccine Fund Period 2003- 2007 and the Post- Vaccine Fund Period 2008-2012 are provided overleaf. Explanation of the assumptions made for each cost category and detailed analysis of the individual costings and schedules are provided in Appendices E and F

The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 32 Printed: 3:33 PM 6/17/2004
Table 4.3: Cost Projections Vaccine Fund Period Post Vaccine Fund Period [A] Recurrent Costs 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
1 Vaccines 997,973 844,814 859,748 852,481 847,800 845,323 880,827 917,822 956,370 996,538 1.1 Traditional vaccines 71,630 72,251 73,941 73,070 72,537 72,269 75,304 78,467 81,762 85,197 1.2 New Vaccines 926,343 772,563 785,807 779,411 775,263 773,054 805,523 839,355 874,608 911,341 2 Injection supplies 61,939 65,856 70,685 73,476 76,404 79,470 82,808 86,286 89,910 93,686 3 Personnel 9,959 11,619 12,177 12,177 12,177 12,177 12,177 12,177 12,177 12,177 4 Transportation 12,835 16,365 22,356 25,175 25,678 26,192 30,329 34,622 35,314 36,021 5 Other recurrent costs 381,529 376,179 396,547 395,703 403,597 406,339 420,512 433,671 438,924 442,738
Subtotal
1,464,234 1,314,832 1,361,513 1,359,013 1,365,656 1,369,502 1,426,653 1,484,577 1,532,694 1,581,159
[B] Capital Costs 6 Vehicles - 62,424 84,897 32,473 - - 68,921 93,733 35,853 -
7 Cold chain equipment 88,865 166,726 66,277 28,908 37,491 28,472 27,231 30,529 21,758 29,203
8 Other capital costs - 9,838 3,668 3,741 3,816 3,892 3,970 4,050 4,131 4,213
Subtotal
88,865 238,988 154,841 65,122 41,307 32,364 100,123 128,312 61,742 33,416
[C] Supplemental Immunization Activities 9 Polio 435,688 140,076 137,957 140,716 143,531 146,401 149,329 152,316 155,362 158,469 10 Measles 385,225 23,970 24,449 202,529 25,437 25,946 26,465 26,994 27,534 28,085
Subtotal
820,913 164,046 162,406 343,245 168,968 172,347 175,794 179,310 182,896 186,554
[D] Optional Information 12 Shared personnel costs 53,578 56,194 58,769 61,481 64,193 67,173 68,057 68,278 69,162 69,382 13 Shared transport costs 20,864 24,573 26,926 27,299 26,224 26,082 28,625 29,541 30,483 31,450 14 Other optional information 67,651 47,294 76,347 42,457 50,260 80,947 45,056 53,336 54,403 55,491
Subtotal
142,093 128,061 162,042 131,237 140,677 174,203 141,738 151,155 154,047 156,322
Total Requirements
2,516,106 1,845,927 1,840,803 1,898,616 1,716,607 1,748,416 1,844,307 1,943,353 1,931,379 1,957,451

The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 33 Printed: 3:33 PM 6/17/2004
4.3. Probable Sources of Finance & Funding Gap Based on the cost projections from 2003 – 2012 an assessment has been made on the future sources of finance and the degree of certainty associated with prospective funding as below:
$0
$500,000
$1,000,000
$1,500,000
$2,000,000
$2,500,000
$3,000,000
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
Funding Gap
HIPC (EU)
Republic of China (Taiwan)
Catholic Relief Services
WHO
Unicef
GAVI-VF
National Government
Figure 4.2: Projections of Secure and Probable Financing by Source and Funding Gap
Table 4.4 2007 2008 2009 2010 2011 2012 Secure + Probable Funding $1,716,607 $1,206,409 $1,228,105 $1,246,717 $1,254,582 $1,260,459
Funding Gap $0 $542,007 $616,203 $696,636 $676,797 $696,991 An assessment of the future sources of funding are presented in the table below. It is apparent that the EPI programme is heavily dependent on GAVI support up to 2008 and thereafter there is a substantial funding gap. Secure + Probable Funding
2003 $
2004 $
2005 $
2006 $
2007 $
2008 $
2009 $
2010 $
2011 $
2012 $
National Government
226,996
250,876
265,839
272,722
276,235
581,282
593,903
604,577
612,535
620,072
GAVI-VF
1,162,597
1,225,670
1,295,038
1,173,972
1,163,008
-
-
- -
-
Unicef
680,091
172,023
171,203
261,622
174,484
176,174
177,897
179,655
181,448
183,277
WHO
416,456
82,023
81,203
171,622
84,484
86,174
87,897
89,655
91,448
93,277 Catholic Relief Services
29,965
14,974
27,519
18,677
18,396
12,780
18,407
22,830
19,151
13,833
Republic of China (Taiwan)
-
100,362
-
-
-
-
-
-
-
-
HIPC (EU)
-
-
- -
-
350,000
350,000
350,000
350,000
350,000
MRC
207,454
-
- -
-
-
-
-
-
-
Total
2,516,106
1,845,927
1,840,803
1,898,616
1,716,607
1,206,409
1,228,105
1,246,717
1,254,582
1,260,459 Funding Gap
-
-
-
-
- $542,007 $616,203 $696,636 $676,797 $696,991

The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 34 Printed: 3:33 PM 6/17/2004
4.4. Projected Key Indicators A review of the key indicators during and post GAVI support indicate that programme efficiencies resulting from the vaccine wastage reduction, improvement in service delivery resulting in enhanced coverage result in substantially reduced costs per DPT/Hib child over the forecast period 2003 – 2012. Additional benefits of the programme can be seen from the key indicators in the table below:
Table 4.6: Projected Key Indicators 2003 2004 2005 2006 2007 Population 1,566,517 1,632,311 1,700,868 1,772,305 1,846,741 Surviving Infants 58,650 61,114 63,681 66,355 69,142 DTP-Hib (liquid) Coverage 89% 92% 95% 95% 95% Recurrent Cost of DPT- Hib Child $30 $25 $24 $23 $22 Recurrent & Capital Cost of DPT- Hib Child $31 $29 $26 $23 $22 Cost Per Capital - Recurrent NIP Costs $0.93 $0.81 $0.80 $0.77 $0.74 Cost Per Capital - SIA $0.52 $0.10 $0.10 $0.19 $0.09 % Government Funding of Recurrent NIP Activities 15% 18% 18% 19% 19% % Vaccines in Cost of Recurrent NIP Activities 68% 64% 63% 63% 62% 2008 2009 2010 2011 2012 Population 1,924,305 2,005,125 2,089,341 2,177,093 2,268,531
Surviving Infants 72,046 75,072 78,225 81,510 84,934 DTP-Hib (liquid) Coverage 95% 95% 95% 95% 95% Recurrent Cost of DPT- Hib Child $21 $21 $21 $21 $21 Recurrent & Capital Cost of DPT- Hib Child $22 $22 $22 $21 $21 Cost Per Capital - Recurrent NIP Costs $0.71 $0.71 $0.71 $0.70 $0.70 Cost Per Capital - SIA $0.09 $0.09 $0.09 $0.08 $0.08 % Government Funding of Recurrent NIP Activities 40% 39% 38% 38% 37% % Vaccines in Cost of Recurrent NIP Activities 62% 62% 62% 62% 63%
It can be concluded that the benefits that accrue to the EPI programme and the health system in general are substantial.

The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 35 Printed: 3:33 PM 6/17/2004
4.5. Scenario B: Projections for inclusion of Pneumococcal Vaccine in 2007 It is assumed that on completion of the clinical trials of the Pneumococcal vaccine introduction will take place from 2007. It is anticipated that since the Pneumococcal vaccine will be a new vaccine it could qualify for further GAVI support. Due to lack of accurate information it was assumed that the cost per dose was in the region of twice the cost of the DPT/Hib or approximately $50 for a 10 dose vial. With the introduction of the Pneumococcal vaccine projections of future resource needs by cost categories and the impact on the funding gap are illustrated as follows:
-
500,000
1,000,000
1,500,000
2,000,000
2,500,000
3,000,000
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
Other optional information
Shared personnel costs
Measles
Polio
Other capital costs
Cold chain equipment
Vehicles
Other recurrent costs
Transportation
Personnel
Injection supplies
New Vaccines
Traditional vaccines
Figure 4.3 : Scenario BProjections of Future Resource Needs by Cost Categories
Total Projected costs for Scenario B are summarised in the following table: Table 4.7:
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 $,000 $,000 $,000 $,000 $,000 $,000 $,000 $,000 $,000 $,000
2,516 1845 1,841 1,899 2,219 2,167 2,280 2,398 2,405 2,451
$0
$500,000
$1,000,000
$1,500,000
$2,000,000
$2,500,000
$3,000,000
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
Funding Gap
HIPC (EU)
Republic of China (Taiwan)
Catholic Relief Services
WHO
Unicef
GAVI-VF
National Government
Figure 4.4: Scenario BProjections of Secure and Probable Financing by Source and Funding Gap
Table 4.8 2007 2008 2009 2010 2011 2012
Secure + Probable Funding $2,218,904 $1,636,081 $1,675,823 $1,713,240 $1,740,699 $1,766,993
Funding Gap - $531,049 $604,785 $684,738 $664,399 $684,073

The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 36 Printed: 3:33 PM 6/17/2004
Table 4.9: Projected Financing Scenario B - Including Introduction of Pneumonicocal Vaccine
[A] Secure Funding 2007 2008 2009 2010 2011 2012
National Government
193,698
199,013
208,599
216,110
220,773
224,876
Sub-National Government
- -
-
-
-
-
Donor Pool (if applicable)
- -
-
-
-
-
GAVI-VF
1,353,963 -
-
-
-
-
Unicef
- -
-
-
-
-
WHO
- -
-
-
-
-
Catholic Relief Services
18,396
12,780
18,407
22,830
19,151
13,833
Republic of China (Taiwan)
- -
-
-
-
-
HIPC (EU)
- -
-
-
-
-
MRC
- -
-
-
-
-
Total
1,566,057
211,793
227,006
238,941
239,924
238,709
Funding Gap
652,846
1,955,337
2,053,601
2,159,037
2,165,174
2,212,357
[B] Secure + Probable Funding 2007 2008 2009 2010 2011 2012
National Government
276,235
581,282
593,903
604,577
612,535
620,072
GAVI-VF
1,665,305
429,672
447,718
466,522
486,116
506,533
Unicef
174,484
176,174
177,897
179,655
181,448
183,277
WHO
84,484
86,174
87,897
89,655
91,448
93,277
Catholic Relief Services
18,396
12,780
18,407
22,830
19,151
13,833
Republic of China (Taiwan)
- -
-
-
-
-
HIPC (EU)
-
350,000
350,000
350,000
350,000
350,000
MRC
- -
-
-
-
-
Total
2,218,904
1,636,081
1,675,823
1,713,240
1,740,699
1,766,993
Funding Gap -
531,049
604,785
684,738
664,399
684,073
As anticipated programme costs would increase considerably however the forecast remains uncertain given that there is no reliable information on the expected price for this new vaccine.

The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 37 Printed: 3:33 PM 6/17/2004
4.6. Key Indicators for Scenario B A review of the key indicators following the introduction of the Pneumococcal vaccine indicate that programme efficiencies enable the introduction of the new vaccine whilst maintaining the cost per DPT – Hib child at a level considerably lower that the current estimated cost.
Table 4.10: Scenario B Projected Key Indicators 2007 2008 2009 2010 2011 2012 Population 1,846,741 1,924,305 2,005,125 2,089,341 2,177,093 2,268,531 Surviving Infants 69,142 72,046 75,072 78,225 81,510 84,934 DTP/Hib (liquid) Coverage 95% 95% 95% 95% 95% 95% Recurrent Cost of DPT/Hib Child $30 $27 $27 $27 $27 $27 Recurrent & Capital Cost of DPT/Hib Child $30 $28 $28 $29 $27 $27 Cost Per Capital - Recurrent NIP Costs $1.01 $0.93 $0.93 $0.93 $0.92 $0.91 Cost Per Capital - SIA $0.09 $0.09 $0.09 $0.09 $0.08 $0.08 % Government Funding of Recurrent NIP Activities 14% 31% 30% 30% 29% 29%
It should be noted that the detailed financial analysis provided in the Appendix relates to the EPI programme excluding the costs associated with the introduction of the Pneumococcal vaccine discussed above.
The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 38 Printed: 3:33 PM 6/17/2004
SECTION 5 5. Sustainable Financing Strategic Plan and Indicators 5.1. Key objectives for the Financial Sustainability Plan
If the perceived function of the Financial Sustainability Plan is seen to be solely to secure funding from the Global Alliance for Vaccinations and Immunisation, then its true importance is lost. From the government’s perspective, the real value of the FSP is to start the process of moving The Gambia EPI programme on its way towards financial sustainability, which is defined by GAVI as follows:
Although self-sufficiency is the ultimate goal, in the nearer term sustainable financing is the ability of a country to mobilize and efficiently use domestic and supplementary external resources on a reliable basis to achieve current and future target levels of immunization performance in terms of access, utilization, quality, safety and equity.
The FSP will assist The Government of The Gambia and in particular, senior health officials and senior management of the EPI programme to ensure the successful delivery of immunisation services in The Gambia. The Government intends to use the Financial Sustainability Planm as a strategic framework to implement change and deliver continuous programme improvement. 5.2. Requirements for Success
To start the process of moving The Gambia on its way towards financial sustainability of EPI delivery it must achieve the following:
To secure ongoing GAVI and other donor funding To be used as an advocacy tool for the following:
o The Government of The Gambia in their dealing with their development partners.
o The Department of State for Health and Social Welfare in their negotiations with other governmental departments.
o Senior management of the EPI programme for resource mobilisation, programme strengthening and deepening.
To form the basis for strategic planning for the EPI programme of The Gambia. To establish targets and monitor the performance of EPI delivery at all levels. Continual improvement in the effective delivery of immunisation services. Efficiency savings set out in the plan.

The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 39 Printed: 3:33 PM 6/17/2004
5.3. Strategic Plan to Achieve Sustainable Financing In order to achieve these goals the actions outlined below must be achieved: Table 5.1: Strategic Plan Objective Required Actions Responsibility Progress
indicator Means of Verification
To secure ongoing GAVI and other donor funding To secure current round of GAVI Funding
Complete, approve and deliver FSP to GAVI.
MHSW ICC
Submission accepted
Approval of funding
To secure future GAVI funding
Implementation of FSP and reporting as required
DHS EPIM
Timely Reporting. Monitoring of achievement of FSP objectives
Approval of Funding
To secure additional donor funding
To identify and target partners for ongoing funding of EPI services
MHSW DHS EPIM
Clear plan for sustainable funding.
Substantially increased donor support.
To be used as an advocacy tool To secure new sources of funding
Advocacy at senior level with potential strategic partners.
DP MHSW DHS EPIM
Clear plan for sustainable funding.
Substantially increased donor support.
To negotiate with other government departments
Use finance and costings to secure budgetary approval and support for EPI activities
MHSW DHS EPIM
Secured funds to meet all requirements of FSP.
Inclusion in budget.
To strengthen and deepen EPI programme
To ensure all staff in EPI work towards the successful delivery of the FSP Targets.
DHS EPIM
FSP targets achieved.
Targets monitored at senior level.
To form the basis for strategic planning for the EPI programme of The Gambia Develop a strategic plan for health delivery.
Develop clear plan health facility development, infrastructural improvement, equipment and staffing in conjunction with key partners.
MHSW DHS FP
Sector wide approach developed
Development of health provision in accordance with strategic plan.
To establish targets and monitor the performance of EPI delivery at all levels. To establish annual performance targets
Establish clear targets for coverage, reduced drop out and vaccine wastage reduction
MHSW DHS EPIM
Targets set, communicated, and monitored.
Unfavourable performance identified and acted upon.
Monitor targets at central, divisional and health centre level.
Senior management to receive, review and act on monthly reports on all key targets.
MHSW DHS EPIM
Reports issued and unfavourable performance acted upon.
Targets achieved or exceeded.

The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 40 Printed: 3:33 PM 6/17/2004
Objective Required Actions Responsibility Progress
indicator Means of Verification
To achieve continual improvement in the effective delivery of immunisation services. To maintain and enhance coverage
Gradual improvement of service delivery through implementation of policy of community based delivery.
DHS EPIM PHO/CHN
Coverage reports.
Improved coverage.
To reduce drop out Monitor drop out rates and investigate unfavourable levels. Document causes and take corrective action.
EPIM PHO/CHN
Drop Out analysis reports. Causes of drop out documented and addressed
Reduction in drop out rates.
To achieve efficiency savings set out in the plan. Immediate improvement in management reporting
DHS Monthly management reports to senior management.
Action taken to enhance EPI processes.
Recruitment of appropriately qualified personnel responsible only for vaccine wastage reduction.
Require name & dept.
Immediate Recruitment and training.
Staff recruited and retained.
National measurement and monitoring of vaccine usage v actual delivery at Facility level.
VWMRT Standardised timely reporting provided to director and senior management on monthly basis.
Systematic audit to validate accuracy. Immediate management action on unfavourable wastage.
To reduce vaccine wastage
Identify causes of wastage and deliver solutions to reduce wastage.
DHS EPIM VWMRT CHN / PHO
Reduction in reported wastage at targeted facilities.
Comparison of reduction in wastage against annual targets.
To strengthen trained human resources for the effective delivery of EPI services To maintain minimum levels of staffing for the EPI
Establish clear staffing norms for delivery of EPI services at all levels
DHS EPIM
Staffing norms set and monitored
Staffing lists from facilities
Develop incentive package for staff delivering EPI services
DHS EPIM
Incentive packages developed and implemented
Divisional Health Team Annual reports
MHSW – Minister for Health and Social Welfare FP – Funding Partners DP – Diplomatic Personnel PS – Permanent Secretary to Department of State for Health and Social Welfare DHS – Director of Health Services EPIM - EPI Manager VWRMT - Vaccine Wastage Reduction Management Technician CHNs – Community Health Nurse PHOs - Public Health Officers

The Republic of The Gambia – Department of State for Health & Social Welfare Financial Sustainability Plan
Submitted to GAVI November 2003
Version: Final Page: 41 Printed: 3:33 PM 6/17/2004
The successful implementation of the key strategic changes recommended are the requirements for the success of this Financial Sustainability Plan. Since the instigation of the Financial Sustainability Plan advocacy has commenced to secure long term funding for the EPI programme. To date this has secured proposed funding of US$350,000 grant aid from HIPC(EU) which has been allocated to funding the EPI programme. A further US$100,000 is anticipated in loans to the government which has been recorded as a government contribution to the FSP. 5.4. Conclusion
$0
$500,000
$1,000,000
$1,500,000
$2,000,000
$2,500,000
$3,000,000
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
Funding Gap
HIPC (EU)
Republic of China (Taiwan)
Catholic Relief Services
WHO
Unicef
GAVI-VF
National Government
Figure 5.1: Projections of Secure and Probable Financing by Source and Funding Gap
As can be seen from the final graphic representation of future probable funding their achievement will place The Gambia well under way to achieving financial sustainability as government works to bridge the future funding gap.


















