
The Final Stretch
11
04/13/2021 1 The Final Stretch: Inherited Disorders of Connective Tissue Jonathan A. Dyer, MD Philip C. Anderson Chair Professor of Dermatology and Child Health University of Missouri – Columbia E-mail: [email protected] Jonathan A. Dyer, MD DISCLOSURES Investigator: Scioderm; Allergan DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY New Classification of EDS • Beyond Villefranche.. • EDS: – Joint hypermobility – Skin hyperextensibility – Tissue fragility Am J Med Genet Part C Semin Med Genet 175C:8–26 New Classification of EDS • Clinical classification – Molecular confirmation for definite diagnosis • NGS – panel vs. WES/slice • Major/Minor criteria for each subtype • Second pathogenetic classification also created - evolving
Transcript of The Final Stretch

04/13/2021
1
The Final Stretch:Inherited Disorders of Connective
Tissue
Jonathan A. Dyer, MD Philip C. Anderson Chair
Professor of Dermatology and Child Health University of Missouri – Columbia
E-mail: [email protected]
Jonathan A. Dyer, MD
DISCLOSURESInvestigator: Scioderm; Allergan
DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY
New Classification of
EDS
• Beyond Villefranche..
• EDS: – Joint hypermobility
– Skin hyperextensibility
– Tissue fragility
Am J Med Genet Part C Semin Med Genet 175C:8–26
New Classification of EDS
• Clinical classification– Molecular confirmation for definite diagnosis
• NGS – panel vs. WES/slice
• Major/Minor criteria for each subtype
• Second pathogenetic classification also created - evolving

04/13/2021
2
EDS - Classical• AD; COL5A1 or COL5A2 mutations
– >90%
• Incidence ~1:5,000
• PROM; premature birth
Am. J. Med. Genet. Part C (Seminars in Medical Genetics) 175C:27–39 (2017)
EDS- Classical• Major:
– (1) Significant skin hyperextensibility* and atrophic scarring
– (2) Generalized joint hypermobility*
• Minimal criteria suggestive for diagnosis of classical EDS
– Major criteria (1) + either:
– Major criteria (2)
– Or: three of the nine minor criteria
Minor:(1) Easy bruising
(2) Soft, doughy skin
(3) Skin fragility (traumatic splitting)
(4) Molluscoid pseudotumours
(5) Subcutaneous spheroids
(6) Hernia (history of)
(7) Epicanthal folds
(8) Complications of joint hypermobility (e.g., sprains, dislocation/subluxation, pain, pes planus)
(9) Family history- 1st deg; meeting clinical criteriaAm J Med Genet Part C Semin Med Genet 175C:8–26
• Gorlin’s sign– Touch nose with tongue– 10% of population
• Metenier’s sign– Eyelid extensibility
EDS - Classical
Hyperextensibility/ Hypermobility
• No real consensus on how to measure
• What is normal?
• Beighton scale – 5/9 (?7/9 in kids)
• Age cutoffs? – validity- >50 yo invalid– Exercise; ethnicity; gender
• Skin hyperextensibility– >1.5 cm distal
forearms, dorsal hands
– >3 cm neck, elbow, knees
» Remvig et al. 2009
EDS - Classical

04/13/2021
3
Beighton scaleClinical Normal Unilateral Bilateral
Touch floor with open palms and fullyextended knees
0 1
>10 degree knee hyperextension 0 1 2
>10 degree elbow hyperextension 0 1 2
>90 degree passive dorsiflexion of 5th
finger0 1 2
Passive flexion of thumb to forearm 0 1 2
Beighton scale EDS - Classical
• Atrophic scarring• Minor criteria:
– Easy bruising– Molluscoid pseudotumours
• Calcification and fibrosis of old hematomas
– Spheroids• Spherical hard SQ nodules on
forearms and shins that calcify
– Epicanthal folds
• “doughy” or velvety skin
• Other “tricks”:– Swallowing own
tongue
– Absence of labial and lingual frenula is marker of EDS
EDS - Classical
Lancet; 357(9267):1500-2 2001
Reverse Namaskar sign
Indian J Dermatol. 2010 Jan-Mar; 55(1): 86–91.
EDS- ClassicalAdditional features
• Premature aging
• Cerebral spinal fluid leak
• Mitral valve prolapse, tricuspid prolapse: use strict criteria
• Chronic pain with normal X-ray
• Pregnancy: postpartum hemorrhage and uterine prolapse
EDS – ClassicalManagement
• Avoid trauma when possible– Low impact sports - if any– Nonweight bearing exercise– Fall proof the home (or the
child)• Physical therapy• CV: Echo

04/13/2021
4
• Wound care: – Closely spaced, multilayered absorbable
subcutaneous stitches– Closely spaced cuticular stitches
• Leave in at least twice as long • Can use absorbable stitches for cuticular closure
– Aggressive steri-strips at closure and after SR– Pressure bandages to decrease hematoma risk– Aggressive infection control
EDS- ClassicalManagement
Vascular EDS• AD; COL3A
• Major criteria:– Arterial aneurysm; dissection; rupture
• mid-sized
– Intestinal rupture - sigmoid
– Uterine rupture• Pregnancy - 5% mortality
– Family history
– Carotid-cavernous sinus fistula
Am J Med Genet Part C Semin Med Genet 175C:40–47
Vascular EDS• Easy bruising
• Thin, translucent skin
• Limited joint hypermobility– Distal digits
• Acrogeria– Aged appearing extremities
• Hands; C-terminal muts
– Tendon/muscle rupture
Vascular EDS - vEDS• Cong. hip dislocation;
talipes; pneumothorax; early onset varicosity; gingival recession; keratoconus
• “triangular facies”– Lobeless ears
– Thin vermilion
– Micrognathia
– Narrow nose
– Prominent eyes
Vascular EDS
• Diagnostic tests:– DNA blood test for mutation, deletion/duplication
– Biochemical test for abnormal electrophoretic mobility of type III procollagen from cultured skin fibroblasts (Byers lab, Seattle)
vEDS -Management• ID causative variants in COL3A1 (rare COL1A1 Arg-Cys muts)
• Modulate life style - minimize injury, risk of vessel/organ rupture
• ID and create care team
• Plan for emergency care (“vascular EDS passport”) - diagnosis and management plan for use when traveling
• Centralize management at centers of excellence (experience) if feasible
• Maintain BP in normal range / treat hypertension aggressively
• Surveil vascular tree (Doppler US, CTA (low radiation), MRA - annual
04/13/2021
5
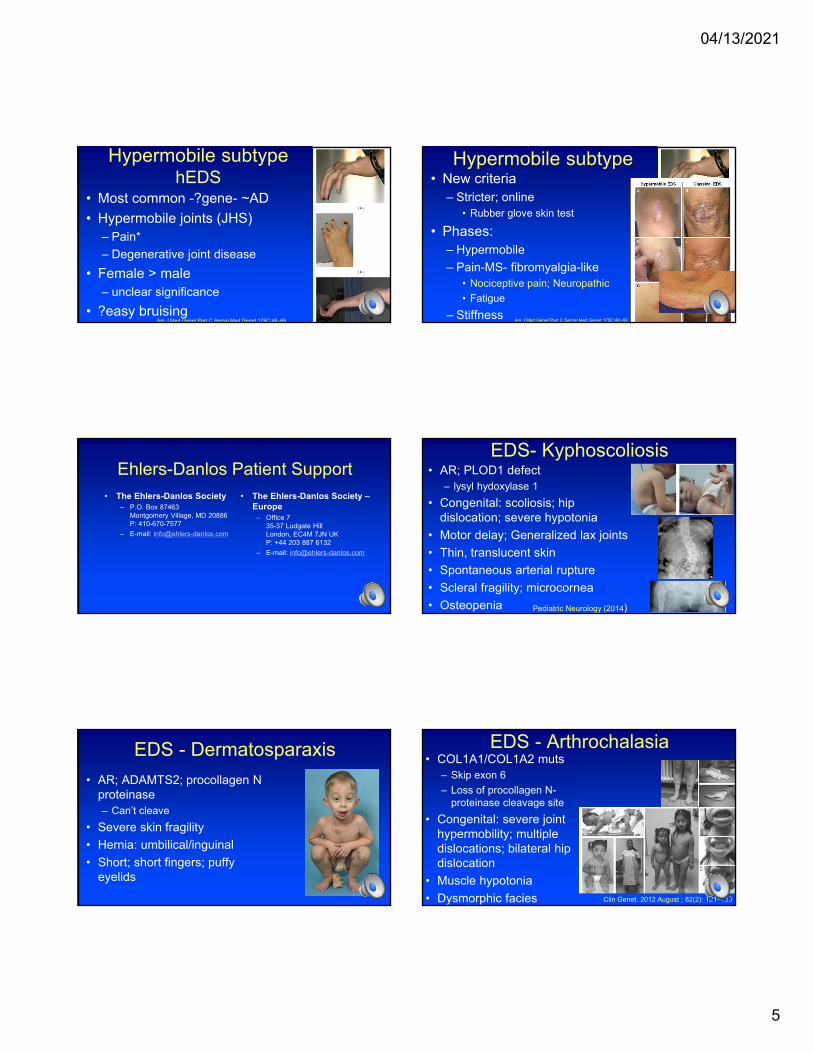
Hypermobile subtypehEDS
• Most common -?gene- ~AD
• Hypermobile joints (JHS)– Pain*
– Degenerative joint disease
• Female > male– unclear significance
• ?easy bruisingAm J Med Genet Part C Semin Med Genet 175C:48–69
Hypermobile subtype• New criteria
– Stricter; online• Rubber glove skin test
• Phases: – Hypermobile
– Pain-MS- fibromyalgia-like• Nociceptive pain; Neuropathic
• Fatigue
– StiffnessAm J Med Genet Part C Semin Med Genet 175C:48–69
Ehlers-Danlos Patient Support• The Ehlers-Danlos Society
– P.O. Box 87463Montgomery Village, MD 20886P: 410-670-7577
– E-mail: [email protected]
• The Ehlers-Danlos Society –Europe
– Office 735-37 Ludgate HillLondon, EC4M 7JN UKP: +44 203 887 6132
– E-mail: [email protected]
EDS- Kyphoscoliosis• AR; PLOD1 defect
– lysyl hydoxylase 1
• Congenital: scoliosis; hip dislocation; severe hypotonia
• Motor delay; Generalized lax joints
• Thin, translucent skin
• Spontaneous arterial rupture
• Scleral fragility; microcornea
• Osteopenia Pediatric Neurology (2014)
EDS - Dermatosparaxis
• AR; ADAMTS2; procollagen N proteinase– Can’t cleave
• Severe skin fragility
• Hernia: umbilical/inguinal
• Short; short fingers; puffy eyelids
EDS - Arthrochalasia• COL1A1/COL1A2 muts
– Skip exon 6
– Loss of procollagen N-proteinase cleavage site
• Congenital: severe joint hypermobility; multiple dislocations; bilateral hip dislocation
• Muscle hypotonia
• Dysmorphic facies Clin Genet. 2012 August ; 82(2): 121–130

04/13/2021
6
Marfan’s syndrome
• AD - Mutations in fibrillin-1– 1:5,000
– ~25% de novo
• Abnormal:• Bone
• Ocular
• Cardiovascular
• Pulmonary; Muscle; Dura
Marfan syndrome
• Long extremities– Dolichostenomelia
– Arachnodactyly
– Arm span > height (>1.05)
– Reduced upper:lower body segment ratio
• Scoliosis: >60%
• Pectus: excavatum/carinatum
Pectus carinatum Pectus excavatum Striae

04/13/2021
7
The Hand in Marfans• Steinberg sign
– Fold thumb into closed fist
– + if thumb tip extends past palmar edge of hand
• Walker-Murdoch sign– + if thumb and fifth finger
overlap when gripping wrist with opposite hand
• Arachnodactyly
Marfans syndromeHand
Marfan syndromeEye
• Subluxation of lens– Ectopia lentis
• Myopia
• Retinal detachment
• Glaucoma
• Early cataract
Marfan syndromeHeart
• Aortic root dilatation– Measured via Z
score - Echo
– Media of arteries affected
• Mitral valve prolapse
Nat. Rev. Cardiol. 2010.31
Marfan syndromeDiagnosing
Score calculator - National MarfanFoundation Web site
• Ghent nosology– Score > or = 7 is
significant
https://www.marfan.org/dx/score

04/13/2021
8
Marfan syndromeFacies*
• Dolichocephaly– Long narrow head
• Downward slanting palpebral fissures
• Enophthalmos– Recession of globe in orbit
• Retrognathia
• Malar hypoplasia *3/5 features = 1 point
Marfan syndrome
• Lumbosacral
• CT/MRI - No preferred method
Nat. Rev. Cardiol..2010.30
Dural ectasia Spontaneous pneumothorax
Marfan syndromeProtrusio Acetabulae
• AP pelvis Xray– Medial protrusion of
acetabulum >3mm beyond ilio-ischial line
Marfan syndromeHindfoot deformity
• Hindfoot valgus - 2– Forefoot abduction
– Lowering of midfoot
• Not just simple “flat feet” -1
Nat. Rev. Cardiol.2010.31

04/13/2021
9
Marfan syndromeTreatment
• Conflicting data in recent studies
• Some show no benefit with losartan
• No effect: dominant negative
• + Effect: haploinsufficiency
• Combining beta-blockers and losartan is considered the best treatment at present
Osteogenesis imperfecta• Type 1 collagen
• Type I most common - AD– Thin, translucent skin, atrophic
scars
– Fragile bones; frequent fractures
– Hearing loss in ~50%
– Blue sclera
• Type II – AD/AR - often lethal
• Type III – AR - severe deformity
Osteogenesis imperfecta• Type 1 collagen
• Type I most common - AD– Thin, translucent skin, atrophic
scars
– Fragile bones; frequent fractures
– Hearing loss in ~50%
– Blue sclera
• Type II – AD/AR - often lethal
• Type III – AR - severe deformity
Osteogenesis imperfecta• Type 1 collagen
• Type I most common - AD– Thin, translucent skin, atrophic
scars
– Fragile bones; frequent fractures
– Hearing loss in ~50%
– Blue sclera
• Type II – AD/AR - often lethal
• Type III – AR - severe deformity
Cutis laxa
• Pendulous, inelasticskin– Not fragile
• Aged appearance
• Abnormal elastic fibers
Cutis laxa• Heterogeneous
– AD-elastin; fibulin5
– AR-fibulin 5 and 4• Most common; severe
– XLR (occipital horn syndrome) –ATP7A
• Lax distal skin; Brittle hair
• Thin face; inverted lower eyelids; hooked/beaked nose

04/13/2021
10
ADCL
ARCL type 1b ARCL type 1a/c
ARCL type 3
Debre- type CL
Cutis laxa
• Emphysema
• Aortic aneurysm
• Pulmonary artery/valve stenosis
• Hernia
• GI diverticula
• Lax joints
• Low ceruloplasminand bilateral exostoses of occiput– Occipital horn
syndrome
Buschke-Ollendorf syndrome
• AD; OMIM#
• LEMD3 gene
• Skin:– Dermatofibrosis
lenticularis disseminata• Elastoma
• Collagenoma
• Bone: osteopoikilosisArch Dermatol. 2010;146(1):63-68

04/13/2021
11
Pseudoxanthoma elasticum (PXE)• AR - Incidence – 1:50,000-75,000
• Fragmentation and mineralization of elastic fibers
• Clinical:– Classic “plucked chicken” skin
• May be seen in children quite early (adolescence)
– Retinal abnormalities• Peau d’orange – early
• Angioid streaks
– Vascular abnormalities• Claudication
• Infarction
PXE is a “metabolic” disease• Caused by defects in ABCC6
– Transmembrane efflux transporter expressed in liver and kidney• Minimal to no expression in skin
• Does transport ATP – major pyrophosphate (PPi) source
– PPi suppresses mineralization
– Progressive
– Serum from patients does not prevent Ca/PO4 precipitation in culture
– Skin grafting studies• wt skin on ABCC6 null mice = PXE
• ABCC6 null skin on wt mice = Normal
PXE - Treatment?
• Abcc6 null mice fed 5 times the standard amount of magnesium did not develop typical mineralization – Replicated in vitro
• J Invest Dermatol. 2009 Jun;129(6):1388-94
• Overexpression of anti-mineralization protein fetuin-A also showed some temporary benefit in mouse model
Why does it matter?
• Not as rare a disease as one would think
• Implications for other conditions where ectopic mineralization/ connective tissue fragmentation occurs in setting of solid organ disease?
Thanks for your attention and attendance!
Thank you for attending!
Jonathan A. Dyer, MD Philip C. Anderson Chair
Professor of Dermatology and Child Health University of Missouri – Columbia
E-mail: [email protected]
Please contact me should you have any questions.


















