
The extraordinary spectrum of diseases caused by Aspergillus David W. Denning Wythenshawe Hospital...
68
The extraordinary spectrum of diseases caused by Aspergillus David W. Denning Wythenshawe Hospital University of Manchester
-
Upload
magnus-mitchell -
Category
Documents
-
view
214 -
download
0
Transcript of The extraordinary spectrum of diseases caused by Aspergillus David W. Denning Wythenshawe Hospital...

The extraordinary spectrum of diseases caused by Aspergillus
David W. DenningWythenshawe Hospital
University of Manchester

The genus The genus AspergillusAspergillus - importance to - importance to humanityhumanity
www.aspergillus.org.uk
cause invasive and allergic diseasein humans and other animals:
A. fumigatus
cause plant and food spoilage and produce mycotoxins:
A. flavus and A. parasiticus
on the negative side:on the negative side:

The genus The genus AspergillusAspergillus - importance to - importance to humanityhumanity
www.aspergillus.org.uk
on the positive side:on the positive side:
composting
well-established model organism in cell biology and genetics:A. nidulans
food production:enzymes and organic acids: A. niger East Asian foods: A. oryzae and A. sojae
pharmaceuticals:echinocandins: A. nidulans and A. sydowilovastatin: A. terreusfumagillin: A. fumigatus
Spores inhaled Germination
Mass of hyphae (plateau phase)
Hyphal elongation and branching
Aspergillus Life-cycle
www.aspergillus.org.uk

A. nidulans – may be amphotericin B resistant
The genus The genus AspergillusAspergillus – – ~800 species, ~800 species,
~50 have caused disease (able to grow at 37C)~50 have caused disease (able to grow at 37C)
Common in the environmentCommon in the environment
A. nigerA. terreus – resistant to AmBA. flavus -sometimes amphotericin B resistant
www.aspergillus.org.uk
A. fumigatus low frequency of azole resistance
Aspergillus fumigatus
conidial head

CLASSIFICATION OF ASPERGILLOSIS
Persistence without disease - colonisation of the airways or nose/sinuses
Airways/nasal exposure to airborne Aspergillus
Invasive aspergillosis• Acute (<1 month course)• Subacute/chronic necrotising (1-3 months)
Chronic aspergillosis (>3 months)• Chronic cavitary pulmonary• Aspergilloma of lung• Chronic fibrosing pulmonary• Chronic invasive sinusitis • Maxillary (sinus) aspergilloma
Allergic• Allergic bronchopulmonary (ABPA)• Extrinsic allergic (broncho)alveolitis (EAA)• Asthma with fungal sensitisation• Allergic Aspergillus sinusitis (eosinophilic fungal rhinosinusitis)

Immunosuppression and infection
• Inhalation of aspergillus spores is a common daily occurrence. A healthy immune system would normally remove the spores and no symptoms or infection would occur.
• In individuals whose immune system may be suppressed either because of illness eg AIDS, cancer patients or drugs, spores may germinate and resulting tissue or systemic aspergillus invasion can result.
• Individuals with allergies such as asthma, can also be vulnerable to allergic aspergillosis

Global opportunistic infections
DiseaseMost common species
LocationEstimated Life-ThreateningInfections / Year
Mortality Rates(% in infected populations)
Opportunistic Systemic Mycoses
Invasive aspergillosisAspergillus spp.
worldwide >200,000 30 - 95%
Invasive candidiasisCandida spp.
worldwide >400,000 46 - 75%
CryptococcosisCryptococcus neoformans
worldwide >1,000,000 20 - 70%
MucormycosisRhizopus oryzae
worldwide >10,000 30 – 90%
PneumocystisPneumocystis jirovecii
worldwide >400,000 20 - 80%
Brown et al, Sci Transl Med 2012;4:165rv13
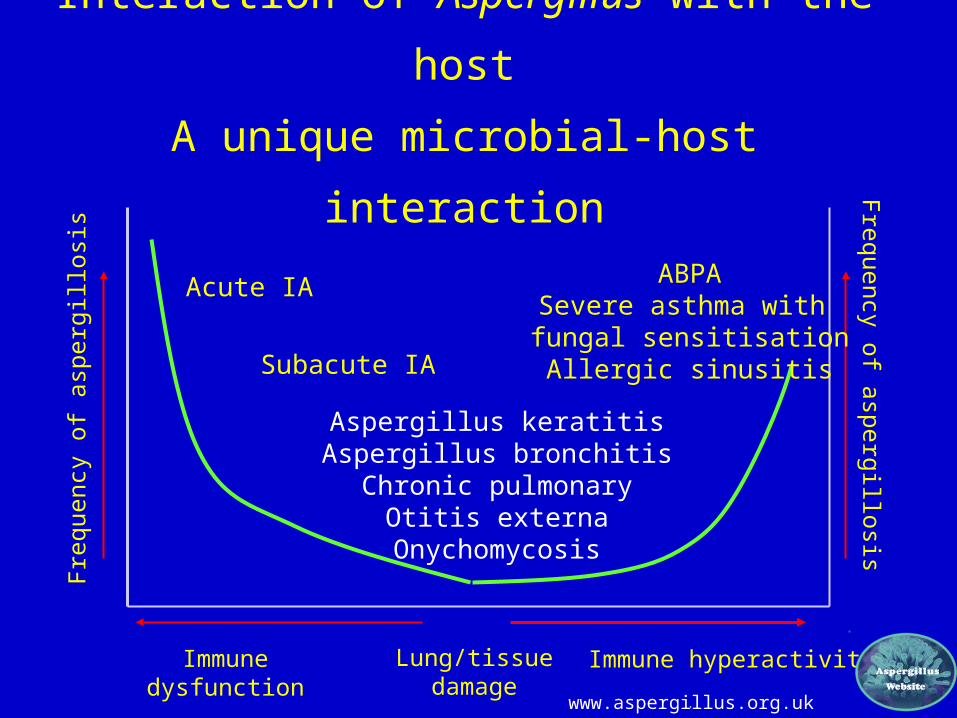
Interaction of Aspergillus with the host
A unique microbial-host interaction
Immune dysfunction
Frequency
of a
sperg
illosis
Immune hyperactivity
Frequency
of
asp
erg
illosi
s
Acute IA
Subacute IA
Aspergillus keratitisAspergillus bronchitisChronic pulmonary
Otitis externaOnychomycosis
ABPASevere asthma with fungal sensitisation
Allergic sinusitis
. Lung/tissue
damagewww.aspergillus.org.uk

Aspergillosis burden in Europe
ECDC report published February 2013
Type of aspergillosis
Predominant risk groups
Risk population size (000’s)
Aspergillosis rate
Annual aspergillosis
burden (000’s)
ABPAAsthma 35,474 2.5%
887 (248 – 1,242)
Cystic fibrosis 29 15% 4.3SAFS
Severe asthmaa 3,547 33%1,170 (886 –
1,774) Chronic
pulmonary aspergillosis
COPD, TB, sarcoidosis, ABPA,
Pneumothorax>13,600 1-10% 240
Invasive aspergillosis
Myeloid leukaemia,
Other haematological
HSCT
4411.4
7%
3.13.1
0.8
COPD hospital admissions
3,600 1.2% 34
Solid organ transplantation
30 0.75% 0.25
Medical ICU 1,100 ( all ICU) 2% 22Total
aspergillosis annual burden
All - - 2,364.55
63,250
2,061,300

Invasive pulmonary aspergillosis
www.aspergillus.org.uk
Normal lungIPA
IPA occurs in ~7% of acute
leukaemia patients, 10-15% allogeneic BMT
patients

Unequivocal ‘Halo sign’ surrounding a noduleUnequivocal ‘Halo sign’ surrounding a nodule
Herbrecht, Denning et al, NEJM 2002;347:408-15.
Halo sign

Recent examples of the frequency of invasive aspergillosis
Underlying condition Incidence Reference/yearAcute myeloid leukaemia
8% Cornet, 2002
Acute lymphatic leukaemia
6.3% Cornet, 2002
Allogeneic HSCT 11-15% Grow, 2002; Marr, 2002
Lung transplantation 6.2-12.8% Minari, 2002; Singh,2003
Heart-lung transplantation
11% Duchini, 2002
Small bowel tranplantation
11% Duchini, 2002
AIDS 2.9% Libanore, 2002

Gillies & Campbell, www.aspergillus.org.uk
Bleeding as an aspect of disseminated invasive aspergillosis
Fumagillin is anti-angiogenic
A haemolysin described from Aspergillus fumigatus
Other factors that contribute to thrombosis or a coagulopathy?

How does Aspergillus fumigatus cause thrombosis (clotting of vessels) and also bleeding?
Filler et al, Blood 2004;103:2134; Paris et al, Infect Immun 1997;65:1510.
Interaction of conidia and
endothelial cell projections
Internalisation of conidia (and hyphae) by
endothelial cells with injury
apparent at 4 hours
www.aspergillus.org.uk
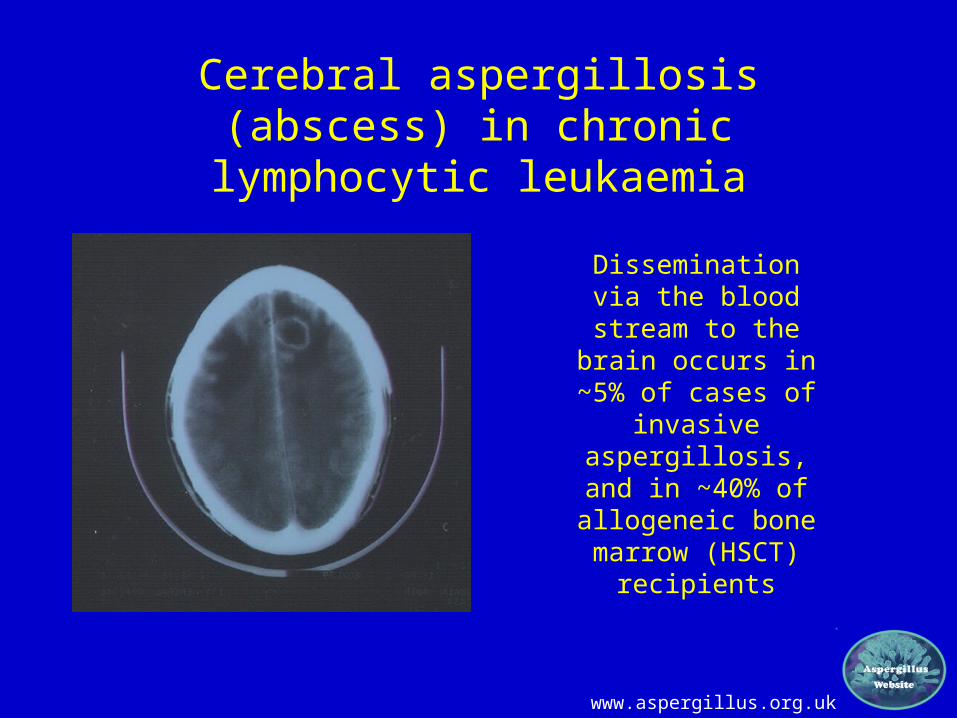
Cerebral aspergillosis (abscess) in chronic lymphocytic leukaemia
Dissemination via the blood stream
to the brain occurs in ~5% of cases of
invasive aspergillosis, and
in ~40% of allogeneic bone marrow (HSCT)
recipients

Early diagnosis of invasive aspergillosis is important
Treatment started <10d >11dMortality 40% 90%
Von Eiff et al, Respiration 1995;62:241-7.

Sputum Cultures for Fungus
Bacteriological media inferior to fungal media – 32% higher yield on fungal
media
A four day A. fumigatus culture on malt extract agar (above). Light microscopy
pictures are taken at 1000x, stained with lacto-phenol cotton blue.

Aspergillus Antigen Test
• Diagnosis or surveillance? • Only blood, or BAL, CSF etc• Best OD cut-off - 0.7• False positives in kids / antibiotics• False negative with antifungal
prophylaxis• Not as useful for non-hematology• Not useful if pre-existing antibody
Herbrecht et al, J Clin Microbiol 2002;20:1898-906; and others

Use of serology, PCR, and GM to establish patient groups
• 130 patients not on azoles• Total IgE, specific IgE aspergillus, specific
IgG aspergillus, sputum galactomannan, sputum PCR
• Cluster analysis – software Mplus version 6.1
Baxter, J Allerg Clin Immunol 2013;132:560
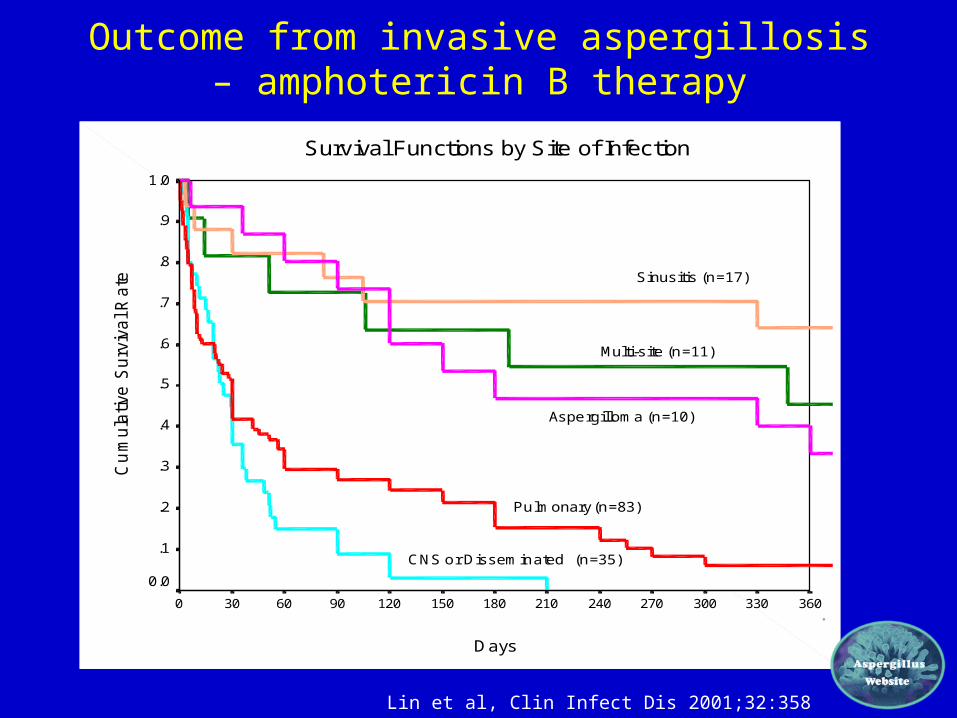
Outcome from invasive aspergillosis – amphotericin B therapy
Survival Functions by Site of Infection
Days
3603303002702402101801501209060300
Cu
mu
lative
Su
rviv
al R
ate
1.0
.9
.8
.7
.6
.5
.4
.3
.2
.1
0.0
CNS or Disseminated
Pulmonary (n=83)
Aspergilloma (n=10)
Multi-site (n=11)
Sinusitis (n=17)
(n=35)
Lin et al, Clin Infect Dis 2001;32:358

Risk groups and frequencies of invasive aspergillosis – different test performances
Herbrecht, Ann NY Acad Sci 2012;1271:23

Sub-acute invasive aspergillosis in AIDSSub-acute invasive aspergillosis in AIDS
www.aspergillus.org.uk

Sub-acute invasive aspergillosisSub-acute invasive aspergillosis
• Less immunocompromised patients• Slower progression of disease (> 1 month)• Cavitary or nodular pulmonary disease typical • Vascular invasion less common• Dissemination less common• Antigen testing less useful• Antibody testing may be helpful in diagnosis
www.aspergillus.org.uk

Aspergillus otitis externa
• Almost always A. niger• Acute otitis affects 1 in 250
persons annually • Chronic otitis affects 3-5%
of the population (200-350 million)
• ~10% are fungal in origin

Aspergillus onychomycosis
• Almost always toenails• 0.5-3% of all cases of
onychomycosis• 10’s to 100’s millions with
onychomycosis worldwide• ? 1 million cases

Aspergillus keratitis• Usually A. flavus or A.
fumigatus• ~50% of keratitis fungal,
and ~50% of these are due to Aspergillus.
• 1-12 million affected worldwide, especially in India, Nepal, Sri Lanka, Myanmar.
• Usually farmers and labourers, occasionally contact lens wearers

Aspergillus bronchitis• Complicates cystic fibrosis
and bronchiectasis• Recurrent infection and/or
mucus plugging• Superficial invasion of the
bronchial wall.• 8600 UK CF patients, 5000
adults.• Aspergilus bronchitis
affects ~1,500• Non-CF patients unclear

Chronic necrotizing aspergillosis(CNPA)
Chronic necrotizing pulmonary aspergillosis (CNPA) is a subacute process usually found in patients with some degree of immunosuppression.
Usually it is associated with underlying lung disease, alcoholism, or chronic corticosteroid therapy. Because it is uncommon, CNPA often remains unrecognized for weeks or months and causes a progressive cavitary pulmonary infiltrate.

Chronic necrotising pulmonary aspergillosis
Denning, Clin Microbiol Infect 2001;7(Suppl 2):25-31.
Right upper lobe. Patient has diabetes and pulmonary
mycobacterium avium- shows small cavitary lesion PT MS 1995.
Right upper lobe showing circular shadow partly filled by a mass. PT
MS 1997
Same lobe shows expansion of the shadow, still partially
filled with a mass. Pt MS 1998
Right lobe shows huge cavity containing some
debris, with +ve aspergillus precipitins.Pt
MS 2000

CLASSIFICATION OF ASPERGILLOSIS
Persistence without disease - colonisation of the airways or nose/sinuses
Airways/nasal exposure to airborne Aspergillus
Invasive aspergillosis• Acute (<1 month course)• Subacute/chronic necrotising (1-3 months)
Chronic aspergillosis (>3 months)• Chronic cavitary pulmonary• Aspergilloma of lung• Chronic fibrosing pulmonary• Chronic invasive sinusitis • Maxillary (sinus) aspergilloma
Allergic• Allergic bronchopulmonary (ABPA)• Extrinsic allergic (broncho)alveolitis (EAA)• Asthma with fungal sensitisation• Allergic Aspergillus sinusitis (eosinophilic fungal rhinosinusitis)

Aspergillus and airways
Langley, ATS 2004
Types of aspergillosis of the airways• Colonisation (no disease – could be at risk)• Obstructing Aspergillus tracheobronchitis /Mucus
impaction (non-invasive)• Aspergillus bronchitis/tracheobronchitis (superficially invasive only)• Ulcerative Aspergillus tracheobroncitis (locally
invasive) (lung transplants – at anastomosis)• Pseudomembranous Aspergillus tracheobronchitis
(Extensive disease, locally invasive, associated with IPA and may disseminate)

Aspergillus tracheobronchitis
Autopsy drawing of a ‘normal’ 3 year old who died over 10 days
Wheaton, Path Trans 1890; 41:34-37

Aspergillus bronchitis
Young et al. Medicine (Balt) 1970;49:147

Aspergillus tracheobronchitis
Review of 58 patients in literature for normal and immuno compromised patients - risk factors
%None (ie normal) 25Heart / Lung transplant 18Solid tumour 15BMT 13Leukaemia 13HIV/AIDS 8Other 8
Kemper et al, Clin Infect Dis 1993; 17: 344

Spectrum of pulmonary aspergillosis
Hope. Med Mycol 2005:43 (Suppl 1) S207

Different patterns of CPA
Radiological response varies by subtype of CPA

AspergillomaAspergilloma
Patient RTDecember 2002
Fungus ball

Chronic pulmonary aspergillosis – pre-Chronic pulmonary aspergillosis – pre-existing diseaseexisting disease
All 18 patients had prior pulmonary disease
9 TB, 5 with atypical mycobacteria
13 smokers or ex-smokers
All 18 non-immunocompromised
3 excess alcohol
Denning DW et al, Clin Infect Dis 2003; 37:S265

Chronic pulmonary aspergillosis - Chronic pulmonary aspergillosis - presentationpresentation
Weight loss 16 / 18 (89%)Cough 15 / 18 (83%)Shortness of breath 9 / 18 (50%)Haemoptysis 9 / 18 (50%)Fatigue / malaise 5 / 18 (28%)Chest pain 3 / 18 (17%)Sputum production ++ 3 / 18 (17%)Fever 2 / 18 (11%)
Denning DW et al, Clin Infect Dis 2003; 37:S265

Chronic pulmonary aspergillosis - serology
All 18 patients had positive Aspergillus precipitins (1+ - 4+)
All 18 patients had elevated inflammatory markers, CRP, PV and / or ESR
14 of 18 (78%) had elevated total IgE (>20), 13 >200 and 7 >400
9 of 14 (67%) had Aspergillus specific IgE (RAST)
Denning DW et al, Clin Infect Dis 2003; 37:S265

Chronic cavitary pulmonary aspergillosis Chronic cavitary pulmonary aspergillosis (CCPA)(CCPA)
Patient RWSeptember 1992 Relapse in normal lung
www.aspergillus.org.uk
Patient RWDecember 1991 Pre surgical resection

Chronic cavitary pulmonary Chronic cavitary pulmonary aspergillosisaspergillosis
Patient RWJuly 1993
www.aspergillus.org.uk

Chronic Cavitary Pulmonary Chronic Cavitary Pulmonary AspergillosisAspergillosis
Patient JAJan 2001

Chronic Cavitary Pulmonary Chronic Cavitary Pulmonary AspergillosisAspergillosis
Patient JAFeb 2002

Chronic Cavitary Pulmonary Chronic Cavitary Pulmonary AspergillosisAspergillosis
Patient JAApril 2003

Chronic Cavitary Pulmonary Chronic Cavitary Pulmonary AspergillosisAspergillosis
Patient JAJuly 2003

Chronic cavitary pulmonary Chronic cavitary pulmonary aspergillosisaspergillosis
Patient JP June 1999
Denning DW et al, Clin Infect Dis 2003; 37:S265

Chronic Cavitary Pulmonary Aspergillosis, Chronic Cavitary Pulmonary Aspergillosis, with aspergillomawith aspergilloma
Patient JP July 2001
Denning DW et al, Clin Infect Dis 2003; 37:S265

Chronic Fibrosing Pulmonary Chronic Fibrosing Pulmonary AspergillosisAspergillosis
Patient JPApril 2002
Denning DW et al, Clin Infect Dis 2003; 37:S265

Prognosis
CPA + subacute IAKorea (1995-2007)
CPA Japan (2001-9)
75% mortality
80% mortality
Nam Int J Infect Dis 2010;14:e479; Ohba et al, Resp Med 2012; 106:724

CLASSIFICATION OF ASPERGILLOSIS
Persistence without disease - colonisation of the airways or nose/sinuses
Airways/nasal exposure to airborne Aspergillus
Invasive aspergillosis• Acute (<1 month course)• Subacute/chronic necrotising (1-3 months)
Chronic aspergillosis (>3 months)• Chronic cavitary pulmonary• Aspergilloma of lung• Chronic fibrosing pulmonary• Chronic invasive sinusitis • Maxillary (sinus) aspergilloma
Allergic• Allergic bronchopulmonary (ABPA)• Extrinsic allergic (broncho)alveolitis (EAA)• Asthma with fungal sensitisation• Allergic Aspergillus sinusitis (eosinophilic fungal rhinosinusitis)

ALLERGIC BRONCHOPULMONARY ASPERGILLOSIS – Key diagnostic criteria
• Asthma• Blood eosinophilia (>1,000 / cu
mm)• History of pulmonary infiltrates• Central bronchiectasis
Rickett et al. Arch Intern Med 1983; 143: 1553; Patterson, Chest 2000;118:7
ABPA possibleABPA possibleABPA probable
ABPA almost certain
• Precipitins against A. fumigatus positive• Aspergillus IgE antibody >2x asthma control• Aspergillus IgG antibody >2x asthma control• Total serum IgE concentration, >1000 iu/mL
If 3 tests +ve, then ABPA very likely, If all 4 +ve the diagnosis established

ABPA versus SAFS
Denning et al, Med Mycol 2013:51:361

How common is ABPA in asthma?
13/500 (2.6%)
10/1390 (0.72%)
9/255 (3.5%)
6/264 (2.3%)+ 5/200 (2.5%) China
Donnelly, Irish J Med Sci 1991;160:288; Eaton, Chest 2000;118:66; Al-Mobeireek, Resp Med 2001;98:341

ABPA
www.aspergillus.org.uk
Before bronchoscopy
After bronchoscopy

ABPA mucous plugging
www.aspergillus.org.uk

ABPA - CT showing central bronchiectasis
www.aspergillus.org.uk

ABPA and surfactant
5 surfactant proteins in man, SPA1, SPA2, SPB, SPC and SPD – all ‘collectin’ family
Mason et al, Am J Physiol 1998;275:L1-13.

ABPA – surfactant defects
2 exonic polymorphisms, and 2 intronic polymorphisms in SP-A2 associated with ABPA
A1660G = OR of 4.78; or if combined with G1649C = OR 10.4
Also associated with higher peripheral eosinophilia
Saxena et al, J Allergy Clin Immunol 2003;111:1001-7.

Eosinophilic fungal rhinosinusitis or allergic fungal sinusitis
Patient with chronic symptoms of nasal obstruction, loss of smell and nasal polyps
Ponikau et al, Mayo Clinic Proc 1999;74:877 & www.aspergillus.org.uk

Eosinophilic fungal rhinosinusitis(link with airborne fungi - ?which most important
= Myelin basic protein, highly toxic to local epithelium
Ponikau et al, Mayo Clinic Proc 1999;74:877

A link between Aspergillus and asthma?

Fungal-associated asthma – evidence
Fungal-associated asthma
ABPA
Treatment of ABPAand pilot data
Severe asthma linked with fungal
sensitisation
Frequency of fungal sensitisation
High spore counts and asthmatic attacks

Spore counts and asthma attacks and admission to hospital
All circumstantial evidence
• Thunderstorm asthma – linked to Alternaria
• Asthma deaths (Chicago) linked to high ambient spores counts and season (summer autumn) when spore counts highest
• Asthma hospital admission linked to high ambient spore counts (Derby, New Orleans, Ottawa
• Asthma hospital attendance linked to high spore counts , but not pollen counts (Canada)
• Asthma symptoms increased on days of high spore counts (California, Pennsylvania)
O'Hollaren, N Engl J Med 1991; 324: 359; Newson, Occup Environ Med 2000; 57: 786-92.

Fungus at homeEnvironmental data
• Mouldy housing associated with worse asthma, with a correlation between asthma severity and degree of dampness in the home and separately with visible mould growth
• In Germany bronchial reactivity in children was associated with damp housing
• Mouldy and damp school associated with asthma symptoms and emergency room visits
• Highest concentration of Aspergillus fumigatus is at home
Williamson, Thorax 1997;52:229. Taskinen, Acta Paediatr 1999; 88:1373.

Severe asthma and moulds
Mild asthma – 564 (50%)
Moderate asthma – 333 (29%)
Severe asthma – 235 (21%) – linked with fungus skin test positivity
Zureik et al, Br Med J 2002;325:411

Asthma severity, house dust mites, cats and moulds
Langley, ATS 2004
Allergen No asthman= 111
Mild asthma FEV1 >75%
<90%n= 67
Moderate asthma FEV1
>60% <75%n= 42
Severe asthma FEV1
>60% n= 42
House dust mite
61% 71% 45% 77%
Cats* 49% 51% 38% 35%
Moulds# 17% 19% 36% 31%
* P = 0.05# p = 0.01


















