The Evolution of Surgery--DMU cannula & semi-rigid instruments Access from many angles & no...
15
9/26/14 1 Joel E. Rand, MPAS, PA-C DMU Luncheon May 1, 2014 No financial relationship or commercial interest in any of the technologies discussed Not supporting any non-FDA “off label” uses of any product or service Some of the slides were obtained from the vendor’s website with their permission Eat lunch and have fun—no quiz to follow Recognize common surgical conditions Learn the current treatment options available Review the risks and benefits of different surgical modalities Discuss the dramatic progress that has taken place in the last 20 years Prognosticate what the next 10-30 years may look like
Transcript of The Evolution of Surgery--DMU cannula & semi-rigid instruments Access from many angles & no...

9/26/14
1
Joel E. Rand, MPAS, PA-C DMU Luncheon
May 1, 2014
¨ No financial relationship or commercial interest in any of the technologies discussed
¨ Not supporting any non-FDA “off label” uses of any product or service
¨ Some of the slides were obtained from the vendor’s website with their permission
¨ Eat lunch and have fun—no quiz to follow ¨ Recognize common surgical conditions ¨ Learn the current treatment options available ¨ Review the risks and benefits of different
surgical modalities ¨ Discuss the dramatic progress that has taken
place in the last 20 years ¨ Prognosticate what the next 10-30 years may
look like

9/26/14
2
Foregut Surgeries
Bariatric Surgery Weight Loss Nissen Fundoplication GERD
Esophageal Hernia Repair Hiatal Hernia
Heller Myotomy Achalasia
Cholecystectomy Gallbladder Disease
Colorectal Surgery Benign and Malignant colon and rectal disease Gynecologic Surgery Benign and Malignant Uterine and Ovarian disease
Ventral Hernia Repair Abdominal Hernia
Inguinal Hernia Repair Groin Hernia
Pros: • Efficacious and historically the “gold standard” • Readily available instruments • Easily collaborative
Cons: • Highly invasive • Ergonomically challenging for the surgeon and assistant • Long and painful recovery • High postoperative complication rates

9/26/14
3

9/26/14
4
Pros: • Minimally invasive
• Faster recovery time
• Less scaring and risk of infection
• Less blood loss and subsequent transfusion
• Less pain and complications from narcotics
• Better visualization
Cons: • Counterintuitive motion • Two-dimensional vision with poor depth perception
• Ergonomically challenging
• Longer operative time
• Decreased venous return due to CO2 insufflation of peritoneal cavity • Expensive instruments

9/26/14
5
¨ Reduced postoperative pain ¨ Lower morbidity ¨ Faster recovery time (i.e. earlier return to normal ADLs & work) ¨ Fewer wound complications ¨ Possible lower cost due to shorter hospital stay ¨ Cosmesis ¨ Reduced trocars equals less site herniation and infection, less puncture risk ¨ Ability to rapidly and readily convert SILS to conventional laparoscopic
procedure

9/26/14
6
¨ Potential risks
¡ Increased wound complications ¡ Increased incisional hernia ¡ Prolonged operative time ¡ Plus all risks inherent in laparoscopic surgery
¨ SILS versus standard laparoscopy
¡ Single portal of entry ¡ Altered ergonomics ¡ Fencing/Crossing of Instruments ¡ Difficulty maintaining pneumoperitoneum ¡ Need of new Instrumentation (multi-lumen ports, articulating/flexible
instrumentation) ¡ Learning curve issues ¡ Insurance reimbursement concerns
da Vinci Surgery overcomes the limitations of open and traditional laparoscopic surgery
High Definition 3D Vision § Surgeon-controlled § Stable and immersive view § Up to 10x zoom
Precision & Dexterity § Mimics surgeon’s hands § Scales down movements § With tremor filtration
Intuitive® Motion § Advanced software
enables intuitive control (instead of cross-handed)
3cm 1cm

9/26/14
7
Stable 3DHD visualization of tissue plane and hernia site
Ability to suture from a variety of angles to repair defects

9/26/14
8

9/26/14
9
Adoption of MIS for Hysterectomy
0%
5%
10%
15%
20%
25%
1988
1990
1992
1994
1996
1998
2000
2002
2004
2006
2008
2010
Year
Adop
tion
Laparoscopyda Vinci
¨ Inguinal hernia ¨ Ventral hernia ¨ Cholecystectomy ¨ Low anterior resection ¨ Right colon ¨ Sigmoid colon ¨ Nissen fundoplication and Heller myotomy ¨ Sleeve gastrectomy ¨ Hysterectomy ¨ Appendectomy ¨ Roux en Y gastric bypass
¡ Reduced complications
¡ Short Hospital Stay
¡ Low rate of conversion to open surgery
¡ Low rate of recurrence
Ventral Hernia Repair, incl. da Vinci Ventral Hernia Repair, Potential Patient Risks ¡ Pain ¡ Infection ¡ Hernia recurrence ¡ Adhesion ¡ Obstruction of small/large intestine
MIS incl. da Vinci Surgery Potential Patient Risks ¡ Longer operative time than anticipated ¡ Conversion to open surgery ¡ Need for additional or larger incision(s) ¡ Temporary pain or discomfort from
pneumoperitoneum
vs. Traditional Lap Surgery
da Vinci Ventral Hernia Repair Potential Patient Benefits
9/26/14
10
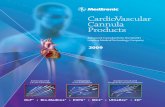
Ia Systemic reviews of randomized controlled trials Ib Randomized controlled trials Ic Randomized controlled trials for robotic technique studies
IIa Systematic reviews of only comparison studies and
independent database population studies IIb Prospective non-randomized studies and RCTs with N<20
IIIa Systematic reviews of mixed studies (comparison and single
arm) IIIb Retrospective non-randomized studies and prospective
comparison studies with N<20
IVa Literature reviews IVb Single arm studies and retrospective comparison studies with
N<20 V Case reports, Animal and Cadaver studies, Expert Opinion and
Editorials
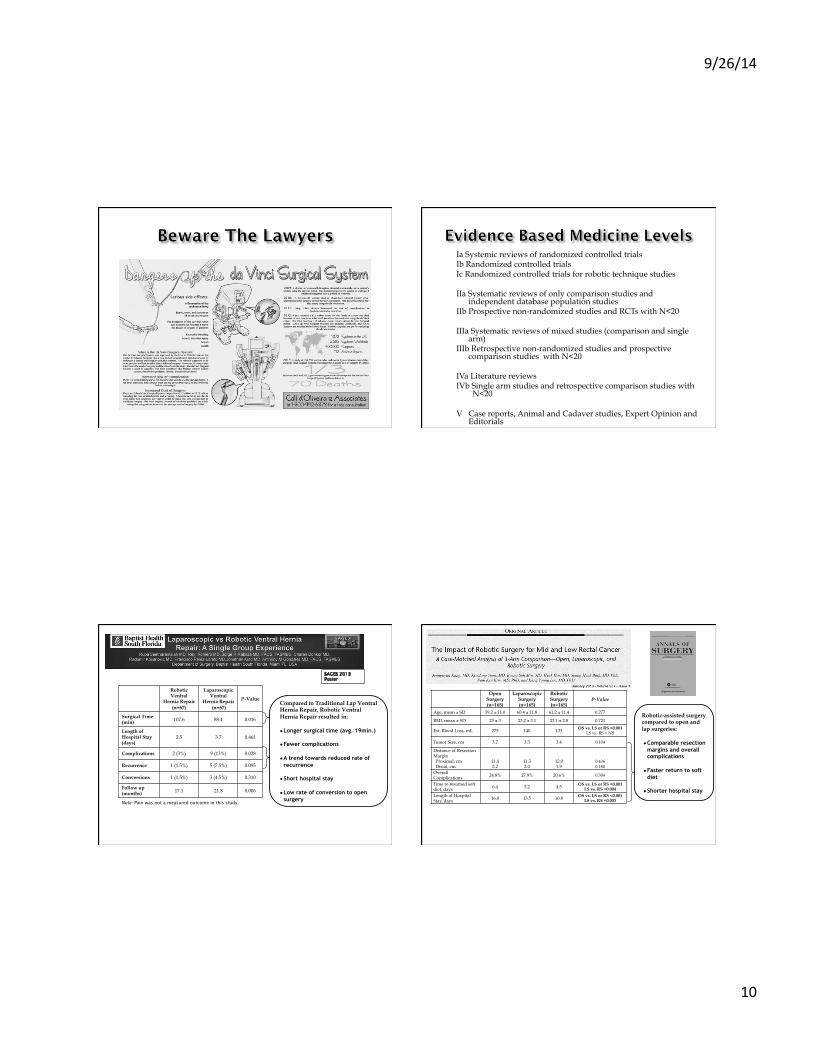
Note: Pain was not a measured outcome in this study.
Robotic Ventral
Hernia Repair (n=67)
Laparoscopic Ventral
Hernia Repair (n=67)
P-Value
Surgical Time (min) 107.6 88.4 0.016
Length of Hospital Stay (days)
2.5 3.7 0.461
Complications 2 (3%) 9 (13%) 0.028
Recurrence 1 (1.5%) 5 (7.5%) 0.095
Conversions 1 (1.5%) 3 (4.5%) 0.310
Follow up (months) 17.1 21.8 0.006
Compared to Traditional Lap Ventral Hernia Repair, Robotic Ventral Hernia Repair resulted in: ● Longer surgical time (avg. 19min.)
● Fewer complications
● A trend towards reduced rate of recurrence
● Short hospital stay
● Low rate of conversion to open surgery
Open Surgery (n=165)
Laparoscopic Surgery (n=165)
Robotic Surgery (n=165)
P-Value
Age, mean ± SD 59.2 ± 11.0 60.4 ± 11.8 61.2 ± 11.4 0.277
BMI, mean ± SD 23 ± 3 23.2 ± 3.1 23.1 ± 2.8 0.721
Est. Blood Loss, mL 275 140 133 OS vs. LS or RS <0.001 LS vs. RS = NS
Tumor Size, cm 3.7 3.3 3.4 0.104
Distance of Resection Margin Proximal, cm Distal, cm
11.4 2.2
11.3 2.0
12.0 1.9
0.436 0.180
Overall Complications 24.8% 27.9% 20.6% 0.304
Time to resumed soft diet, days 6.4 5.2 4.5 OS vs. LS or RS <0.001
LS vs. RS =0.004
Length of Hospital Stay, days 16.0 13.5 10.8 OS vs. LS or RS <0.001
LS vs. RS =0.003
Robotic-assisted surgery compared to open and lap surgeries: ● Comparable resection
margins and overall complications
● Faster return to soft diet
● Shorter hospital stay

9/26/14
11
No. Post-Op IV analgesics Opioids, mean ± SD
Open Surgery (n=165)
Laparoscopic Surgery (n=165)
Robotic Surgery (n=165)
P-Value
Post-Op, Day 1 0.7 ± 1.0 0.4 ± 0.7 0.2 ± 0.6 <0.001
Post-Op, Day 2 0.8 ± 1.0 0.6 ± 1.0 0.2 ± 0.6 <0.001
Post-Op, Day 3 0.5 ± 0.9 0.4 ± 0.7 0.2 ± 0.6 0.004
Post-Op, Day 4 0.3 ± 0.7 0.2 ± 0.7 0.1 ± 0.5 0.229
Post-Op, Day 5 0.2 ± 0.6 0.2 ± 0.5 0.1 ± 0.3 0.015
Post-Op Pain Status (mean ± SD) All P <0.001
SD = standard deviation VAS = visual analog scale POD = postoperative day
Robotic-assisted surgery compared to open and lap surgeries: ● Significant decrease
in post-op pain
● Significant decrease in analgesia usage
Laparoscopic Nissen Fundoplication
¨ Surgical Supplies - $95.02
¨ Surgical Instruments - $1480.52
¨ Total Cost = $1575.04
Robotic Nissen Fundoplication
Early Surgeries ¨ Surgical Supplies – $91.82 ¨ Surgical Instruments - $ 2656.77 ¨ Total Cost = $2738.59
Cost Controlled Cases ¨ Removal of extra instruments not
needed and supplies ¨ Total Cost = $1639.59
Laparoscopic Inguinal Hernia
¨ Tacker - $600 ¨ Trocars x3 - $90 ¨ Lap scissors - $85 ¨ Graspers, bipolar– $45-$225 ¨ Mesh $350
¨ Total = $820- $1000 ¨ Total w/ 2 tackers = $1,500
Robotic Inguinal Hernia
¨ Fenestrated Bipolar - $270 ¨ Mega Suture cut - $240 ¨ Suture x3 - $5 ¨ Drapes $200 ¨ Mesh $350
¨ Total = $775
¨ Bilateral – no tacker, Suture is cheap
¨ No use of extra instruments.

9/26/14
12
§ Curved cannula & semi-rigid instruments
Access from many angles & no instrument crowding
§ Designed to limit cannula shift Minimize potential port-site trauma & post-op pain
§ A single incision in the belly button Virtually scarless
¡ Low rate of major complications
¡ Low conversion rate to open surgery
¡ Virtually scarless
¡ High patient satisfaction
¡ Minimal pain
Cholecystectomy, incl. da Vinci Cholecystectomy Potential Patient Risks ¡ Bile duct injury
¡ Bile leakage
¡ Pancreatitis
¡ Incision-site hernia
MIS, incl. da Vinci Surgery Potential Patient Risks ¡ Longer operative time than anticipated ¡ Conversion to open surgery ¡ Need for additional or larger incision(s) ¡ Temporary pain or discomfort from
pneumoperitoneum
da Vinci Single-Site Cholecystectomy Potential Patient Benefits
https://www.youtube.com/watch?v=O4pO_RXELvE

9/26/14
13
• Decreased postoperative pain • Improved cosmesis • Reduced physiologic, psychological and immune response to surgery • Decreased wound complications • Decreased anesthesia requirements • Accelerated patient recovery • Improved access to organs that are otherwise difficult to visualize with conventional tools
• Developing training programs • Managing intraoperative complications • Determining optimal orifice to use • Reliably closing the viscotomy • Minimizing infection with instruments passing through a nonsterile orifice • Create an endoscopic suturing device • Address difficulty with spatial orientation • Maintain stable pneumoperitoneum • Transvaginal access only in women obviously

9/26/14
14

9/26/14
15
¨ Questionnaire-based study asked people to share their preferences in a hypothetical acute appendicitis scenario
¨ 80.6% chose SILS over NOTES at this point ¨ More education of the public as surgeons
perfect techniques ¨ NOTES over the next 10-15 years will see
incremental gains, not the overnight success of da Vinci
¨ Perhaps NOTES and da Vinci will combine