The Evolution and Future of ACC/AHA Clinical Practice ... report of the American College of...
12
TASK FORCE STATEMENT The Evolution and Future of ACC/AHA Clinical Practice Guidelines: A 30-Year Journey A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines Alice K. Jacobs, MD, FACC, FAHA, Immediate Past Chair Jeffrey L. Anderson, MD, FACC, FAHA, Chair Jonathan L. Halperin, MD, FACC, FAHA, Chair-Elect ACC/AHA Task Force Members Jeffrey L. Anderson, MD, FACC, FAHA, Chair Jonathan L. Halperin, MD, FACC, FAHA, Chair-Elect Nancy M. Albert, PhD, CCNS, CCRN, FAHA Biykem Bozkurt, MD, PhD, FACC, FAHA Ralph G. Brindis, MD, MPH, MACC Lesley H. Curtis, PhD, FAHA David DeMets, PhD* Lee A. Fleisher, MD, FACC, FAHA Samuel Gidding, MD, FAHA Judith S. Hochman, MD, FACC, FAHA* Richard J. Kovacs, MD, FACC, FAHA E. Magnus Ohman, MD, FACC Susan J. Pressler, PhD, RN, FAHA Frank W. Sellke, MD, FACC, FAHA Win-Kuang Shen, MD, FACC, FAHA Duminda N. Wijeysundera, MD, PhD *Former Task Force member during the writing effort. In 2014, we mark the 30th anniversary of the first publication of an American College of Cardiology (ACC) and American Heart Association (AHA) clinical practice guideline (CPG). This joint effort was undertaken in response to the U.S. government’s request to review the evidence concerning cardiac pacemakers and develop CPGs to mitigate potential overuse. Since then, fueled by a shared sense of responsibility to translate available evidence into clinical practice to guide cardiovascular clini- cians, the ACC and AHA have developed 23 CPGs across the spectrum of cardiovascular diseases and procedures. The “why” and “how” of CPGs continue to evolve. Although the “why” is based on the directive to develop evidence-based recommendations for selection of diagnostic tests, proce- dures, and treatments to improve quality of care and out- comes for patients with cardiovascular disease, it is precisely where evidence is lacking or is controversial that clinicians need the most guidance. A 2012 survey of ACC and AHA members provides important insight into the way clinicians and other healthcare professionals apply CPGs; further details are provided below. The results highlight a natural tension This document was approved by the American College of Cardiology Board of Trustees and the American Heart Association Science Advisory and Coordinating Committee in May 2014. The American College of Cardiology requests that this document be cited as follows: Jacobs AK, Anderson JL, Halperin JL. The evolution and future of ACC/AHA clinical practice guidelines: a 30-year journey: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014;64:1373–84. This article is copublished in Circulation. Copies: This document is available on the World Wide Web sites of the American College of Cardiology (www.cardiosource.org) and the American Heart Association (my.americanheart.org). For copies of this document, please contact the Elsevier Inc. Reprint Department, fax (212) 633-3820, e-mail [email protected]. Permissions: Multiple copies, modification, alteration, enhancement, and/or distribution of this document are not permitted without the express permission of the American College of Cardiology. Requests may be completed online via the Elsevier site (http://www.elsevier.com/ authors/obtaining- permission-to-re-use-elsevier-material). JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY VOL. 64, NO. 13, 2014 ª 2014 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION AND THE AMERICAN HEART ASSOCIATION, INC. ISSN 0735-1097/$36.00 http://dx.doi.org/10.1016/j.jacc.2014.06.001 PUBLISHED BY ELSEVIER INC.
Transcript of The Evolution and Future of ACC/AHA Clinical Practice ... report of the American College of...
J O U R N A L O F T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y V O L . 6 4 , N O . 1 3 , 2 0 1 4
ª 2 0 1 4 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O UN DA T I O N
A N D T H E A M E R I C A N H E A R T A S S O C I A T I O N , I N C .
I S S N 0 7 3 5 - 1 0 9 7 / $ 3 6 . 0 0
h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j a c c . 2 0 1 4 . 0 6 . 0 0 1
P U B L I S H E D B Y E L S E V I E R I N C .
TASK FORCE STATEMENT
The Evolution and Future ofACC/AHA Clinical Practice Guidelines:A 30-Year JourneyA Report of the American College of Cardiology/American Heart Association Task Force onPractice Guidelines
Alice K. Jacobs, MD, FACC, FAHA, Immediate P
ast ChairJeffrey L. Anderson, MD, FACC, FAHA, ChairThis document was approved by the American College of Cardiology Boa
Coordinating Committee in May 2014.
The American College of Cardiology requests that this document be cited a
ACC/AHA clinical practice guidelines: a 30-year journey: a report of the Am
Practice Guidelines. J Am Coll Cardiol 2014;64:1373–84.
This article is copublished in Circulation.
Copies: This document is available on the World Wide Web sites of the A
Heart Association (my.americanheart.org). For copies of this document, plea
Permissions: Multiple copies, modification, alteration, enhancement, and
permission of the American College of Cardiology. Requests may be complete
permission-to-re-use-elsevier-material).
Jonathan L. Halperin, MD, FACC, FAHA, Chair-Elect
ACC/AHA TaskForce Members
Jeffrey L. Anderson, MD, FACC, FAHA, ChairJonathan L. Halperin, MD, FACC, FAHA, Chair-
ElectNancy M. Albert, PhD, CCNS, CCRN, FAHABiykem Bozkurt, MD, PhD, FACC, FAHARalph G. Brindis, MD, MPH, MACCLesley H. Curtis, PhD, FAHADavid DeMets, PhD*Lee A. Fleisher, MD, FACC, FAHASamuel Gidding, MD, FAHA
Judith S. Hochman, MD, FACC, FAHA*Richard J. Kovacs, MD, FACC, FAHAE. Magnus Ohman, MD, FACCSusan J. Pressler, PhD, RN, FAHAFrank W. Sellke, MD, FACC, FAHAWin-Kuang Shen, MD, FACC, FAHADuminda N. Wijeysundera, MD, PhD
*Former Task Force member during the writing effort.
In 2014, we mark the 30th anniversary of the first publication ofan American College of Cardiology (ACC) and American HeartAssociation (AHA) clinical practice guideline (CPG). This jointeffort was undertaken in response to the U.S. government’srequest to review the evidence concerning cardiac pacemakersand develop CPGs to mitigate potential overuse. Since then,fueled by a shared sense of responsibility to translate availableevidence into clinical practice to guide cardiovascular clini-cians, the ACC and AHA have developed 23 CPGs across thespectrum of cardiovascular diseases and procedures.
The “why” and “how” of CPGs continue to evolve. Althoughthe “why” is based on the directive to develop evidence-basedrecommendations for selection of diagnostic tests, proce-dures, and treatments to improve quality of care and out-comes for patients with cardiovascular disease, it is preciselywhere evidence is lacking or is controversial that cliniciansneed the most guidance. A 2012 survey of ACC and AHAmembers provides important insight into the way cliniciansand other healthcare professionals apply CPGs; further detailsare provided below. The results highlight a natural tension
rd of Trustees and the American Heart Association Science Advisory and
s follows: Jacobs AK, Anderson JL, Halperin JL. The evolution and future of
erican College of Cardiology/American Heart Association Task Force on
merican College of Cardiology (www.cardiosource.org) and the American
se contact the Elsevier Inc. Reprint Department, fax (212) 633-3820, e-mail
/or distribution of this document are not permitted without the express
d online via the Elsevier site (http://www.elsevier.com/ authors/obtaining-

Jacobs et al. J A C C V O L . 6 4 , N O . 1 3 , 2 0 1 4
Evolution and Future of ACC/AHA CPGs S E P T E M B E R 3 0 , 2 0 1 4 : 1 3 7 3 – 8 4
1374
between the needs of clinicians for comprehensive clin-ical advice from seasoned experts and for a clear delin-eation of diagnostic and therapeutic measures for whichstrong scientific evidence exists.
Notably, there has been an increased focus on the“how” of CPGs and changes in the methodology used tocollect and evaluate the evidence. In 2011, the Instituteof Medicine (IOM) published 2 reports, Clinical PracticeGuidelines We Can Trust (1) and Finding What Works inHealth Care: Standards for Systematic Reviews (2). Inresponse to these reports and our own mandate to con-tinually improve processes and methods while evaluat-ing the continuous stream of new knowledge andmaintaining relevance at the point of care, the ACC/AHATask Force on Practice Guidelines (Task Force) held aMethodology Summit in December 2011. The Method-ology Summit focused on the standards for systematicreviews and process improvements. The response to the21 standards and 82 supporting elements proposed by theIOM was published in the “ACCF/AHA Clinical PracticeGuideline Methodology Summit Report” (3). However,many of the IOM recommendations and standards arethemselves based more on consensus than data, andthere is little evidence on the extent to which theirimplementation may have a favorable impact on clinicaloutcomes. Hence, the effectiveness of the IOM reportrecommendations must be assessed over time as organ-izations similar to the ACC and AHA begin the complexprocess of applying the proposed standards in CPGdevelopment.
During the past few years, several process improve-ment initiatives have been implemented to limit thenarrative text in CPGs by substituting increased use ofsummary and evidence tables (with references linked toabstracts in PubMed). Consensus conferences at whichmembers of guideline writing committees (GWCs) reachagreement and concordance on overlapping recom-mendations are now held routinely. Methodologicalenhancements include development and future vali-dation of a scoring tool to consistently assess the qualityof randomized trials that inform recommendations in thedomains of bias, relevance, and fidelity. In addition, ananalysis of Bayesian approaches to evidence synthesiswas undertaken (4). Other enhancements include sepa-ration of the Class III recommendations to delineatewhether the recommendation is determined to be of “nobenefit” or associated with “harm” to the patient, aswell as inclusion of comparative-effectiveness recom-mendations based on comparative-effectiveness studiesto indicate when one treatment/strategy is preferred toanother. Lastly, to harmonize with other CPG classi-fication schema, we now more precisely indicate thestrength of the recommendation associated with the Classof Recommendation (COR).
RATIONALE FOR CPGS
In the IOM report (1), CPGs were redefined as follows:
Clinical practice guidelines are statements thatinclude recommendations intended to optimizepatient care that are informed by a systematic reviewof the evidence and an assessment of the benefits andharms of alternative care options.
CPGs that are rigorously developed have the potentialto improve the quality of cardiovascular care, lead tobetter patient outcomes, improve cost-effectiveness bytargeting resources to the most effective therapies,enhance the appropriateness of clinical practice, andidentify critical gaps in evidence and areas needingadditional research. In fact, when patients are treatedaccording to ACC/AHAClass I recommendations, outcomesare improved. Specifically, data from the quality of careCRUSADE (Can Rapid Risk Stratification of Unstable AnginaPatients Suppress Adverse Outcomes With Early Imple-mentation of the ACC/AHA Guidelines) Registry demon-strate that in patients with acute coronary syndromes,there is a 10% reduction in in-hospital mortality for every10% increase in adherence to ACC/AHA Class I guideline-directed medical therapies (5). Similarly, data fromADHERE (Acute Decompensated Heart Failure NationalRegistry) demonstrate that patients treated according toheart failure performance indicators have a significantreduction in in-hospital mortality and length of stay (6).
DEVELOPMENT PROCESS
The Task Force, which is composed of a broad con-stituency with varying content expertise, oversees anddirects the CPG development process and methodologythat are the foundation of the documents and theunderpinning of their broad recognition. The processbegins with selection of a topic for a new, revised, orupdated CPG by the Task Force with the input of GWCsand ACC and AHA council and committee members. Inview of the overarching goal of inclusivity and collabo-ration, selected organizations and professional societieswith similar interests and expertise are invited to partic-ipate as partners or collaborators. Next, a GWC chair isselected by the Task Force, and, with input from theleadership of participating organizations, potentialmembers of the GWC are identified, based on a detailedand specific policy on relationships with industry andother entities (RWI) and a desire to balance intellectualand practice perspectives in addition to sex, race, geo-graphic location, and ethnicity. In view of the AHA’s focuson the patient and the public it serves and its lay mem-bership, the ACC’s initiative on patient-centered care, andthe recommendations of the Methodology Summit, the

J A C C V O L . 6 4 , N O . 1 3 , 2 0 1 4 Jacobs et al.S E P T E M B E R 3 0 , 2 0 1 4 : 1 3 7 3 – 8 4 Evolution and Future of ACC/AHA CPGs
1375
Task Force now invites lay representatives (i.e., patients,patient advocates, or consumer organization representa-tives) to participate as members of GWCs and may includethem on the Task Force. Methods to identify, select, train,and manage RWI and the intellectual perspectives of layrepresentatives are in development. Lay representativesmay participate in topic selection; delineation of diag-nostic and therapeutic options, values, preferences, andpatient-oriented outcomes; and shared decision making.
The GWC outlines the document content, performsa detailed and specific evidence acquisition and review,and drafts recommendations based on the strength andquality of evidence with limited preliminary text. On thebasis of the Methodology Summit recommendations, theprocess has started to involve an Evidence Review Com-mittee (ERC) that is separate from the GWC. The ERCincludes methodologists, epidemiologists, clinicians, andbiostatisticians tasked with formal systematic review ofavailable evidence and responsibility for identification,abstraction, and quality assessment of the evidence.Given practical considerations, including limited resour-ces and time constraints, the role of ERCs will be limitedto addressing critical questions where the evidence lendsitself to a systematic review and that are most clinicallyrelevant to the CPG topic. The role of the ERC in selectedCPGs may be fulfilled by a partnership with other highlyregarded organizations that perform systematic reviews,such as the National Institutes of Health, the CochraneCollaborative, and Kaiser Permanente. When appropriate,other stakeholders may be invited. In 2013, the Task Force
PC
201AHA/ACC SPrevention G
2013 ACC/AHASTEMI Guideline
2012ACC/AHAUA/NSTEMIGuideline
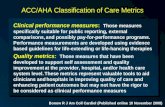
FIGURE 1 Concordance Among Existing Guideline Recommendations and Th
ACC indicates American College of Cardiology; AHA, American Heart Association
vention; SCAI, Society for Cardiovascular Angiography and Interventions; SIHD, s
UA/NSTEMI, unstable angina/non–ST-elevation myocardial infarction.
successfully piloted a focused ERC approach to a confinedtopic using a PICOTS (Population, Intervention, Com-parator, Outcomes, Timing, and Setting) format todevelop critical questions for the systematic review. ThePICOTS format specifically identifies the target pop-ulation (P) for whom the intervention is intended; definesthe intervention (I) and whether the comparator (C) isplacebo, no intervention, or some alternative strategy;designates the outcome (O) as a clinical event (e.g.,mortality, nonfatal myocardial infarction) or a patient-oriented endpoint (e.g., symptoms, functional capacity,quality of life, diagnosis, or prognosis); and specifiesthe timing (T) of measurement for the intended outcomeand the setting (S) in which the outcome is measured.Developing appropriate questions is a collaborativeprocess, with input from the GWC chair and members,the Task Force, partner organizations involved with theCPG, and the ERC. The questions may also be reviewedmore broadly by organizational leadership and thepublic. It is then the responsibility of the GWC to developrecommendations using the evidence reviewed by theERC.
Once recommendations and limited text are drafted,the vetting process begins. In the absence of new evi-dence, prior recommendations in ACC/AHA CPGs do notchange. Because recommendations often overlap acrossmultiple documents (Figure 1), reconciliation can becomplex and time consuming. The first consensus con-ference was held in 2009 and attended by members ofthe GWCs of the percutaneous coronary intervention,
I
2011ACC/AHACABGGuideline
2012ACC/AHA SIHDGuideline
1econdaryuideline
ose From the 2011 ACC/AHA/SCAI PCI Guideline
; CABG, coronary artery bypass graft; PCI, percutaneous coronary inter-
table ischemic heart disease; STEMI, ST-elevation myocardial infarction; and
Jacobs et al. J A C C V O L . 6 4 , N O . 1 3 , 2 0 1 4
Evolution and Future of ACC/AHA CPGs S E P T E M B E R 3 0 , 2 0 1 4 : 1 3 7 3 – 8 4
1376
coronary artery bypass surgery, and ST-elevation myo-cardial infarction CPGs all of which were under revision.With input from the stable ischemic heart disease GWC,the attendees crafted a combined section on coronaryrevascularization for inclusion in all 3 CPGs. The con-sensus conference approach broadens input on relatedrecommendations, facilitates consensus, enhancesimplementation at the point of care, expedites the CPGdevelopment process, and promises to be useful in similarfuture applications.
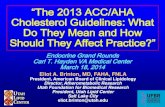
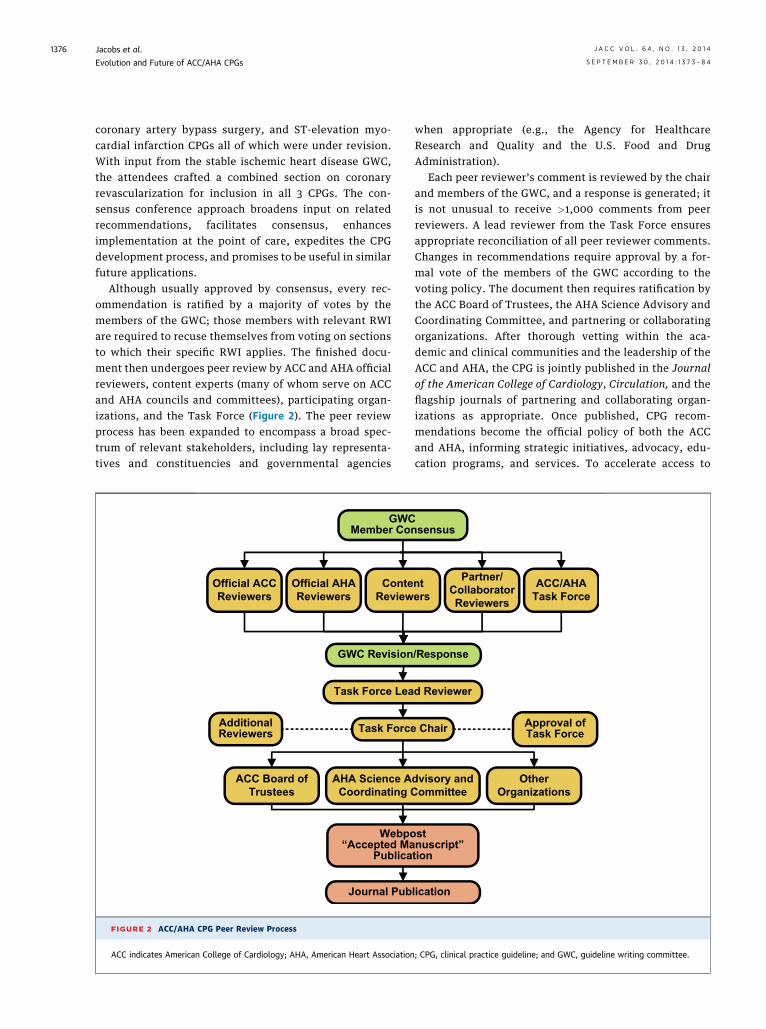
Although usually approved by consensus, every rec-ommendation is ratified by a majority of votes by themembers of the GWC; those members with relevant RWIare required to recuse themselves from voting on sectionsto which their specific RWI applies. The finished docu-ment then undergoes peer review by ACC and AHA officialreviewers, content experts (many of whom serve on ACCand AHA councils and committees), participating organ-izations, and the Task Force (Figure 2). The peer reviewprocess has been expanded to encompass a broad spec-trum of relevant stakeholders, including lay representa-tives and constituencies and governmental agencies
Official ACCReviewers
GWCMember Con
Official AHAReviewers
ConteReview
GWC Revision
Task Force Lea
Task ForceAdditionalReviewers
ACC Board ofTrustees
AHA Science ACoordinating C
Journal Pub
Webpo“Accepted Ma
Publica
FIGURE 2 ACC/AHA CPG Peer Review Process
ACC indicates American College of Cardiology; AHA, American Heart Association
when appropriate (e.g., the Agency for HealthcareResearch and Quality and the U.S. Food and DrugAdministration).
Each peer reviewer’s comment is reviewed by the chairand members of the GWC, and a response is generated; itis not unusual to receive >1,000 comments from peerreviewers. A lead reviewer from the Task Force ensuresappropriate reconciliation of all peer reviewer comments.Changes in recommendations require approval by a for-mal vote of the members of the GWC according to thevoting policy. The document then requires ratification bythe ACC Board of Trustees, the AHA Science Advisory andCoordinating Committee, and partnering or collaboratingorganizations. After thorough vetting within the aca-demic and clinical communities and the leadership of theACC and AHA, the CPG is jointly published in the Journalof the American College of Cardiology, Circulation, and theflagship journals of partnering and collaborating organ-izations as appropriate. Once published, CPG recom-mendations become the official policy of both the ACCand AHA, informing strategic initiatives, advocacy, edu-cation programs, and services. To accelerate access to
sensus
nters
Partner/CollaboratorReviewers
ACC/AHATask Force
/Response
d Reviewer
Chair Approval ofTask Force
dvisory andommittee
OtherOrganizations
lication
stnuscript”tion
; CPG, clinical practice guideline; and GWC, guideline writing committee.

J A C C V O L . 6 4 , N O . 1 3 , 2 0 1 4 Jacobs et al.S E P T E M B E R 3 0 , 2 0 1 4 : 1 3 7 3 – 8 4 Evolution and Future of ACC/AHA CPGs
1377
CPGs that have received final approval, the ACC and AHArelease the manuscripts before typesetting, allowing thedocuments to be available nearly 2 months ahead of for-mal publication in the journals.
RELATIONSHIPS WITH INDUSTRY
AND OTHER ENTITIES
The validity and reliability of CPGs have been questioned,based on concerns that the CPGs are composed by indi-viduals with perceived conflicts of interest (COI), primarilydue to RWI engaged in the development or marketing ofmedical technology or pharmaceutical agents. The per-ception that all RWI imply COI is not inherently accurate(7,8). There is no evidence to confirm or deny that RWIlead to a bias in writing recommendations, and the quan-titative impact of RWI is unknown. Bias may also existwithout RWI, and individuals with RWI often have thegreatest expertise in the subject.
Even so, strict policies are in place to prevent undueinfluence of commercial or other special interests on theCPG development process (9). In late 2009, well inadvance of the IOM report, policies were updated torequire more rigorous management of RWI. The ACC andAHA believe that, when transparent and properly man-aged, including experts with RWI on GWCs strengthensthe writing effort and results in improved documents byensuring the availability of necessary expertise. The 2011Methodology Summit participants supported this view,noting that the “absence of experts (perhaps with rele-vant RWI) on the GWC would undermine the credibility ofthe review and CPG as much or more than the presence ofcommittee members with RWI” (3). Moreover, the term“RWI” is preferred over “COI” because the former doesnot imply ethically conflicting interests or objectives.
In addition to managing RWI, the ACC and AHA mon-itor and manage other potential biases that may be rele-vant to the writing effort, including academic settings,race, sex, geography, intellectual stance, or scope ofclinical practice. On the basis of the Methodology Summitrecommendations, the intellectual (referring to priorpublished opinion or research) and practice (applyingwhen an individual’s income is enhanced by or derivedfrom reimbursement for performing specific tests or pro-cedures) perspectives relevant to the guideline topic arerecognized, defined, disclosed, and managed. As with thechoice of the term “RWI” rather than “COI,” the ACC andAHA have chosen the terms “intellectual perspective” and“clinical practice perspective” (rather than bias) to denoteintellectual and practice-related opinions and expertisebased on knowledge or experience.
To address these issues, the ACC and AHA rely on theprinciples of define, disclose, and manage. The relevance,scope, and level of RWI are clearly defined. For the
purpose of identifying a chair and/or member of a GWC,the following criteria are used to determine if a relevantrelationship with a company or other entity exists:
� The relationship or interest relates to the same or sim-ilar subject matter, intellectual property or asset, topic,or issue addressed in the document; or
� The company/entity (with whom the relationshipexists) makes a drug, drug class, or device addressed inthe document or makes a competing drug or deviceaddressed in the document; or
� The person or a member of the person’s family orhousehold has a reasonable potential for financial,professional, or other personal gain or loss as a result ofthe issues/content addressed in the document.
In terms of scope, the ACC and AHA require disclosureof all RWI (comprehensive for the previous 12 months)involved in the production, marketing, distribution, orreselling of healthcare goods, services, advice, or infor-mation consumed by patients, investors, or physicians.This may include relationships with government entitiesas well as not-for-profit institutions and organizations,which differs from and is more comprehensive than theIOM standards. In addition, authors are strongly dis-couraged from engaging in new RWI until the documenthas been approved by the organizations and published.
The amount or level of RWI is defined as:
� None—If the individual has no conflicts or relationshipsto disclose, he or she must indicate none.
� Modest (<$10,000)—A relationship is considered mod-est if it is less than significant. (In the fall of 2014, thiswill change to <$5,000 to align with U.S. Public HealthService regulations.)
� Significant ($$10,000)—A person is deemed to have asignificant interest in a business if it represents own-ership of $5% of the voting stock or share of theentity, ownership of $$10,000 of the fair market valueof the entity, or if funds received from the entityexceeded 5% of the individual’s gross income duringthe prior year. (In the fall of 2014, this will changeto $$5,000 to align with U.S. Public Health Serviceregulations.)
Disclosure of relationships of members of the GWC isperformed as follows:
� In advance—RWI are reviewed and vetted during ini-tiation of the GWC to ensure fair balance on the GWC.
� On an ongoing basis—verbally and in writing at the startof every meeting and conference call.
� Published—in print and online using a tabular format tohighlight type and level of relationship; publicationof all relevant relationships for authors and peer re-viewers with each guideline, including documentation

Jacobs et al. J A C C V O L . 6 4 , N O . 1 3 , 2 0 1 4
Evolution and Future of ACC/AHA CPGs S E P T E M B E R 3 0 , 2 0 1 4 : 1 3 7 3 – 8 4
1378
of sections from which authors recused themselvesfrom writing or voting; and online posting of compre-hensive RWI for each author and oversight Task Forcemember.
Reporting categories include consultancies, speakersbureaus, ownership, partnerships, principal roles, researchsupport, salary, institutional and organizational relation-ships, and expert witness activities.
Management of RWI involves selection of a balancedGWC and requires that both the chair and a majority ofmembers have no relevant RWI. Authors are restrictedwith respect to writing or voting on sections to whichRWI apply. Although they are permitted to participate indiscussion and comment on the draft, the chair isresponsible for ensuring that this does not result inundue or unfair influence. All CPG recommendationsrequire approval by a majority of the members of theGWC without relevant RWI through confidential ballot-ing. Members recused from voting are listed in the RWItable. Members of the final approving bodies of theACC Board of Trustees and AHA Science Advisory andCoordinating Committee also recuse themselves fromvoting if they have relevant RWI. The RWI of GWCmembers and peer reviewers pertinent to the CPG arelocated in the Appendix. In addition, to ensure completetransparency, comprehensive disclosure information—including RWI not pertinent to the document—is avail-able online for all members of the GWC, as is disclosureinformation for the entire Task Force. The creation ofCPGs and the work of the GWC are supported exclusivelyby the ACC, AHA, and partnering organizations withoutcommercial support. Members of the GWC and TaskForce volunteer for this activity without compensation.The ACC and AHA are fully committed to transparency inthe development of CPGs, have aligned RWI policieswith respect to CPG documents, and continuously eval-uate these policies.
RECOMMENDATION CLASSIFICATION SYSTEM
In analyzing evidence and developing recommendations,GWCs use benchmarks developed by the Task Force (9).The COR is a statement of the strength of the recom-mendation and continues to serve as the primary guidefor clinicians. The choice of the COR may involve con-sideration of an estimate of the size and strength of theeffect of the intervention (diagnostic test or therapeuticstrategy, medication, device, procedure, or other inter-vention) and the magnitude of benefit in relation to risk.The Level of Evidence (LOE) describes the certainty orprecision of the information supporting the recom-mendation based on the type and quality of the evidence.Class I and III recommendations are considered strongrecommendations and are based on size, strength, and
positive or negative benefit–risk estimate of the effect andgeneralizability of benefit over risk. Class IIa recom-mendations carry intermediate strength and correspondto less benefit in proportion to risk. Class IIb recom-mendations, the weakest, address measures associatedwith marginal benefit–risk ratios or uncertain outcomeadvantages and suggest that additional evidence is nee-ded to clarify the relative benefit–risk of the intervention.
Class III recommendations are unique in that they have2 qualifiers. Class III: Harm is a strong recommendationusually derived from 1 or more trials in which outcomeswere worse with the intervention than with the control.Class III: No Benefit is a moderate recommendation that isapplied infrequently when evidence suggests that astrategy is no better than the control. Class III: No Benefitrecommendations should not be associated with weakevidence or expert opinion—LOE C or E—because it isvirtually impossible to ascertain lack of benefit withoutrandomized trials or carefully conducted observationalstudies when safety is not the primary concern. Class III:No Benefit recommendations should be supported bymoderate or high-quality evidence. The adequacy of thesupporting data, including sample size and event rates,needs careful consideration based upon objective criteria(i.e., validated grading tools).
The LOE rates the precision and quality of the scientificevidence supporting the effect of an intervention basedon the type, quantity, consistency, and quality of clinicaltrials and other relevant evidence. The ERC or GWCgrades the evidence supporting each recommendation,depending on whether this includes randomized, obser-vational, prospective, or retrospective studies, and theirquality, including objectively defined criteria for assess-ment of potential bias in addition to their relevanceand fidelity. When published scientific evidence is lack-ing, a consensus of expert opinion is sought to gaugestandards of care based on clinical experience and rankedas Level E.
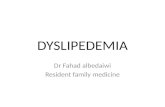
To accommodate the more quantitative, gradedapproach to evidence assessment, the Task Force hascautiously modified the COR/LOE schema (Table 1) toprovide additional categories that offer greater gran-ularity with separate categories for randomized andnonrandomized/observational evidence to define thelevel and quality of evidence. The COR/LOE schemacontinues to evolve as we refine tools to assess the qualityof evidence and collaborate with other organizations suchas the European Society of Cardiology to enhance theclarity, accuracy and utility of guideline recom-mendations. Suggested phrases for writing recom-mendations are provided in the interest of consistency.The revised grading schema consists of the followingcategories, with studies assessed by the GWC or (selec-tively) the ERC, increasingly using standardized evidence
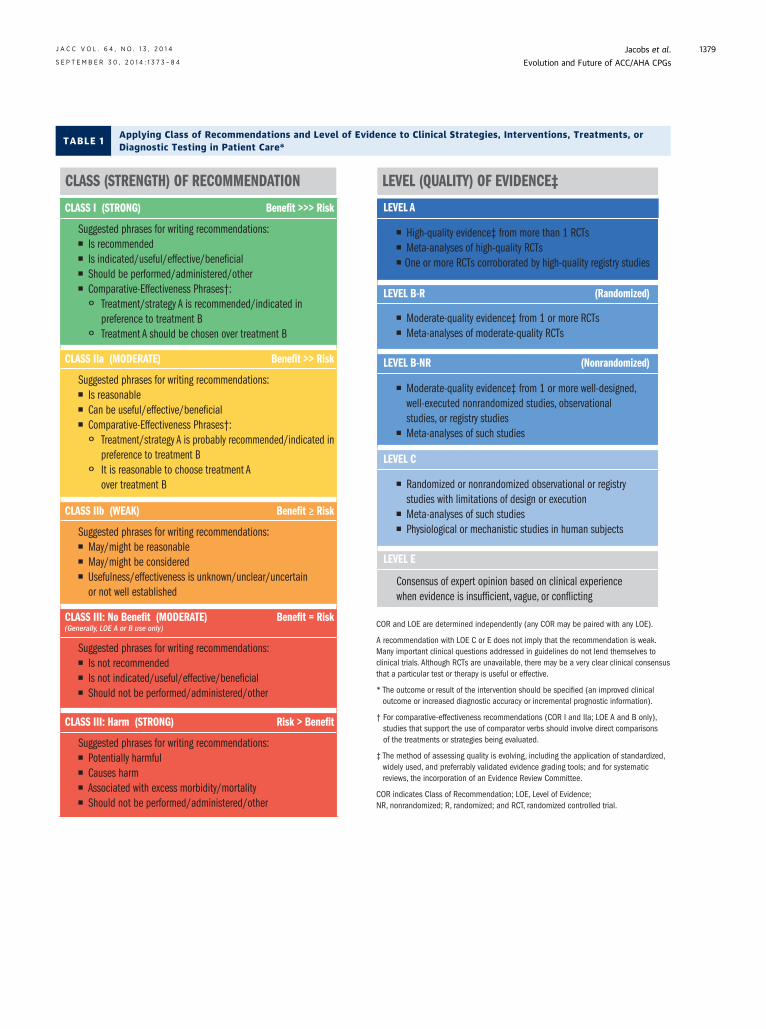
TABLE 1Applying Class of Recommendations and Level of Evidence to Clinical Strategies, Interventions, Treatments, orDiagnostic Testing in Patient Care*
J A C C V O L . 6 4 , N O . 1 3 , 2 0 1 4 Jacobs et al.S E P T E M B E R 3 0 , 2 0 1 4 : 1 3 7 3 – 8 4 Evolution and Future of ACC/AHA CPGs
1379
Jacobs et al. J A C C V O L . 6 4 , N O . 1 3 , 2 0 1 4
Evolution and Future of ACC/AHA CPGs S E P T E M B E R 3 0 , 2 0 1 4 : 1 3 7 3 – 8 4
1380
grading tools where useful to facilitate consistent evalu-ation of the quality of evidence:
� Level AB High-quality evidence* from more than 1 randomizedcontrolled trial (RCT)
B Meta-analyses of high-quality RCTsB One or more RCTs corroborated by high-quality reg-istry studies
� Level B-R (Randomized)B Moderate-quality evidence* from 1 or more RCTsB Meta-analyses of moderate-quality RCTs
� Level B-NR (Nonrandomized)B Moderate-quality evidence* from 1 or more well-designed, well-executed nonrandomized studies,observational studies, or registry studies
B Meta-analyses of such studies� Level C
B Randomized or nonrandomized observational or reg-istry studies with limitations of design or execution
B Meta-analyses of such studiesB Physiological ormechanistic studies in human subjects
� Level EB Consensus of expert opinion based on clinical experi-ence when evidence is insufficient, vague, orconflicting
In view of the increasing number of studies involving activecontrols rather than placebos, recommendations addressingthe relative effectiveness of one clinical strategy comparedwith another continue to be included with specific phrase-ology. These apply to COR I and IIa recommendations onlyand to LOE A or B-R/B-NR.
To address the concern about coupling the strong CORcategories I and III with lower LOEs or expert opinion,specific new guidance from the Task Force is being givento GWCs as follows: Class I recommendations based onlyon LOE C/E should be minimized, and Class III: No Benefitrecommendations should be avoided whenever possible ifsupported only by LOE C/E.
An analysis of the 3,271 recommendations across 19CPGs published by 2013 showed that nearly 50%were ClassI recommendations. In addition, 50% of recommendationswere informed by LOE C and <10% were based on LOE A.Of the Class I recommendations, only 11% were based onLOE A, and 46% were informed by LOE C; even fewer wereassigned LOE A within COR IIa, IIb, and III. Taken together,these results indicate an important gap in evidence sug-gesting a need for clinical trial evidence in the future.Across CPGs, the proportion of LOE C recommendations
* The method of assessing quality is evolving, including the application of
standardized, widely used, and preferably validated evidence grading tools;
and for systematic reviews, the incorporation of an ERC.
has prompted criticism and questions about whether CPGsshould define the standard of care (8,10). Yet, when evi-dence is weak, conflicting, or absent, clinicians seek andneed the most guidance. Moreover, it is recognized thatcertain LOE C recommendations that represent commonsense and conventional wisdom are unlikely to be studied.However, a review of past LOE C recommendations sug-gested that many were, in fact, supported by lower levelsof evidence as well as expert opinion. Overall, theseobservations and concerns highlight the need for evi-dence-based and practice-directed CPG recommendationsand have prompted the revisions in evidence analysis andCOR/LOE grading schema shown in Table 1.
2012 GUIDELINE SURVEY:
SUMMARY OF RESULTS AND IMPLICATIONS
To better understand the views and requirements ofthe ACC/AHA CPG user, a survey was taken from Sep-tember to October 2012. The survey was conducted via 2online sources: 1) the ACC CardioSurve Panel, which iscomposed of U.S. cardiologists who are currently activeFellows of the ACC, and 2) an open, online survey emailedto representative members of the ACC Board of Trustees,AHA, Heart Rhythm Society, and Society for Car-diovascular Angiography and Interventions. The Car-dioSurve survey received a total of 166 responses from 450CardioSurve panelists for a response rate of 37%. A total of40 of 301 members of the organizations above completedthe survey for an overall response rate of 13%. Thus, thefinal number of responses for this survey was 206.
The findings of the survey are summarized as follows:
� When members were asked to rate the relevance ofweaker COR and LOE (Class IIa and IIb and LOE C) totheir practice, more than two thirds of cardiologistsindicated that the weaker class/levels were helpful orvery helpful when making informed diagnostic andtherapeutic decisions. This is an important observa-tion, because it indicates that clinicians seek guidanceon important topics even in situations where the evi-dence base is weak. It also suggests that focusing CPGsonly on strong evidence is not adequate for cliniciansto deliver comprehensive best practices. These obser-vations highlight the natural tension between the valueto clinicians of a comprehensive CPG and a morerestricted CPG limited to a few recommendationsinformed by a strong scientific evidence base.
� More than 90% of cardiologists found the ACC/AHACPGs routinely useful in clinical practice. In fact, >80%of cardiologists apply CPGs in managing patients inmost circumstances. The CPG features found mostuseful are clinical applicability and authority, brevityand clarity, comprehensiveness, ease of access and use,and currency.

J A C C V O L . 6 4 , N O . 1 3 , 2 0 1 4 Jacobs et al.S E P T E M B E R 3 0 , 2 0 1 4 : 1 3 7 3 – 8 4 Evolution and Future of ACC/AHA CPGs
1381
� For cardiovascular or multispecialty practice clinicians,the most frequent use of CPGs is to address a specificclinical question at the point of care, such as in theoffice, in the hospital, or on rounds. For cardiologists inmedical schools and universities, CPGs are most com-monly used as a teaching tool.
� Cardiologists are almost uniformly more interested inan electronic means to access CPGs compared withprint access alone. However, they do not have a singlepreference for electronic means of accessing CPGs.They are nearly evenly split between ACC/AHA web-sites through topic listings, smartphone applications,search engines, or electronic tablet applications. Themajority of cardiologists prefer a comprehensive CPGseparated into different sections or chapters, with allsections published together as a single document.
� More than two thirds of cardiologists prefer a“dynamic” update of CPGs, either continuously as a“living” electronic document or as an update thatoccurs whenever new information requires changes tothe content/recommendations.
� The majority of cardiologists are very or extremelysatisfied with the current use of a color-coded recom-mendation table format. In addition, more than twothirds of cardiologists prefer limited text informing therecommendations, with links to an evidence table thatprovides pertinent details of each study that can beaccessed as desired.
� Nearly three fourths of cardiologists believe that clini-cians have a responsibility to help society provideoptimal care for all patients and that CPGs shouldincorporate available information about cost/resourceutilization to educate providers, payers, and patientsabout the value of various strategies.
The IOM recommendation to have CPGs informed by thehighest-quality (i.e., RCT) evidence and meta-analyses,assessed by an independent ERC, may seem to be discordantwith the views and needs of these CPG users, that is, toinclude not only strong evidence-based recommendations,but also those based on lesser evidence and expert opinionand to do so in a timely, concise, and accessible way. Thisdilemma presents an ongoing and major challenge to theTask Force in charting the future course for CPGs.
EVOLUTION IN CPG METHODS AND PROCESSES
To provide a balanced response to the IOM, clinicians, andCPG users and the concern that recommendations are notbased only on the highest LOE, the following initiativeswere undertaken in 2013 and 2014:
� An ERC was established to provide an independentsystematic review of evidence related to key PICOTSquestions generated by the GWC in collaboration with
the ERC. To ensure transparency and consistency, theERC uses a standardized quantitative tool for assessingRCT data and a separate standardized, quantitative toolfor grading registry/observational data.
� The challenge to generate CPGs based on a more delib-erative, independent, and transparent approach to evi-dence review while responding to the desire for moretimely, responsive, “living” guidelineswill be addressedby compiling CPGs from individual recommendations,each a concise knowledge “byte,” accompanied by con-cise supporting text and linked to supporting referencesand evidence tables (as piloted in the 2014 AHA/ACCvalvular heart disease guideline [11]) and stored in anelectronic repository. The individual recommendationsfor each CPG will then be assembled together for theweb-published and print versions. Not only will thesebe accessible through a variety of electronic searchstrategies, enabled by a standard taxonomy, but theywill be capable of being shared among overlappingdocuments and individually updated or expanded in a“living” document fashion as new evidence becomesavailable. Accessing and updating individual modulesfrom the electronic guideline content managementsystem will be much less onerous and more efficientonce the initial guideline has been developed. Thesedocuments may include revision history and can beaccessed from mobile devices at the point of care andcan eventually be integrated into electronic medicalrecord systems and other patient management tools.
CPG UPDATES: CURRENT PROCESS
The process for initiating, revising, and updating CPGscontinues to evolve under the direction of the Task Force.Keeping pace with new data is an ongoing challenge in thedevelopment of CPGs. In the early 1980s, the Task Forceestablished policies and procedures for maintaining therelevancy of published recommendations. The processinvolved full revisions and shorter updates. Full revisionoccurred after 2 updates or when new evidence requiredrevision of a significant portion of the recommendations.Each topic was reviewed a year after publication of a CPGdocument and annually thereafter. There was on averagea 4- to 5-year span between revisions of each topic.
Recognizing the necessity to review new and rapidlychanging evidence in an ongoing fashion and the timerequired to initiate, develop, review, and publish a CPG,the Task Force developed a new initiative in 2005 tointegrate an accelerated focused update process. TheGWC (whose membership often spans >1 document) andTask Force members review late-breaking clinical trialspresented at major meetings and scan the literaturepertaining to each guideline topic twice annually.The decision to initiate a focused update of a CPG is based
Jacobs et al. J A C C V O L . 6 4 , N O . 1 3 , 2 0 1 4
Evolution and Future of ACC/AHA CPGs S E P T E M B E R 3 0 , 2 0 1 4 : 1 3 7 3 – 8 4
1382
on specific criteria, including the publication of ade-quately powered RCTs or nonrandomized studies withsafety or efficacy implications (see criteria below). Theydo not require comprehensive accounting for all literaturepublished since the date of the previous CPG evidencereview; the evidence review period is noted in the intro-duction of each CPG.
The criteria and considerations for new data includethe following:
� Publication of the full report (rather than the abstract)in a peer-reviewed journal
� Adequately powered RCT(s)� Important nonrandomized data that affect safety and
efficacy assumptions� Strengths/weaknesses of research methodology and
findings� The likelihood that additional studies will influence the
findings or conclusions� The impact on current performance measure(s) or the
need to develop new measures� Requests for review and update from the practice
community, key stakeholders, and other sources free ofbias or commercial relationships
� The number of previous studies with consistent results� Consistency with other CPGs or CPG revisions� Approval of new drugs, devices, or applications by the
U.S. Food and Drug Administration that have an impacton cardiovascular care
Initiation of a focused update does not imply that arecommendation must change but rather that new evi-dence is critically reviewed by the GWC to reach a deci-sion. With the exception of the recommendationsmodified in focused updates, the full CPG remains current.Recommendations in focused updates are current untilsuperseded by another update or a full revision of theCPG. Since the publication of the first 2 focused updates in2007 (12,13), they have been created as stand-alonedocuments with section numbers corresponding to theCPG and new and revised recommendations denoted inadjacent tabular columns. The focused updates are alsoincorporated into the full CPG, which is republished onlinein order to provide a complete, comprehensive CPG.
CPG DERIVATIVES
The recommendations in CPGs remain the primary sourceof guidance for clinicians. Access to CPGs will increasinglybe through sources other than the full, written versions ofthe CPGs, including Web sites (such as those of the AHAand ACC), pocket guides, and electronic access such assmartphone applications. Performance measures oper-ationalize CPG recommendations and are developed asderivatives of CPGs by a separate task force, the ACC/AHA
Task Force on Performance Measures. Performancemeasures focus on critical recommendations carryinglarge benefit based on high-quality evidence to providequantitative metrics for assessing the quality of patientcare for specific cardiovascular conditions. Failure todeliver this care to an eligible patient suggests a qualitylapse. Increasingly, performance measures are used as thebasis for public reporting and pay-for-performance pro-grams. Recommendations selected for performancemeasures must be measureable, valid, reliable, andactionable; address demonstrable gaps in care; and lead toimproved patient outcomes (14,15). Currently, the num-ber of measures, feasibility of data collection, exceptions,and correct attribution are under active consideration bythe ACC/AHA Task Force on Performance Measures.
The ACC appropriate use criteria documents, anotherderivative of CPGs, supplement the recommendations byproviding representative clinical scenarios that allowclinicians to document practice patterns for comparisonagainst established benchmarks. In addition, they addressscenarios for which evidence is lacking. The appropriateuse criteria methodology is based on the RAND (ResearchAnd Development) Delphi model, which provides con-sensus judgments about the utility of interventions inspecific clinical situations. Clinical scenarios are con-structed by a committee using CPG recommendations andare then evaluated by a separate technical panel to trans-late and implement CPG recommendations in clinicalpractice. When CPGs and appropriate use criteria docu-ments were directly mapped against each other for coro-nary revascularization indications in validation testing,all Class I recommendations were appropriate and allClass III recommendations mapped to inappropriate (16).
Whereas CPG recommendations are “should” or“should not” directives, performance measures represent“must do” and appropriate use criteria “reasonable to do”clinical steps. Taken together, these documents definebest practices based on evidence, measure how con-sistently these practices are implemented in patient care,and facilitate benchmarking of practice patterns relativeto peers to promote quality improvement in the interestof safe and effective patient care.
The AHA scientific statements and the ACC clinicalexpert consensus documents represent another importanteducational product ancillary to CPGs. These documentsprovide expert opinion and evidence summaries onimportant focused cardiovascular topics too narrow orimmature to warrant a full CPG but for which there issignificant scientific and clinical interest.
ONGOING CHALLENGES
Responding to the continually expanding evidence basein a timely manner while maintaining rigorous processes

J A C C V O L . 6 4 , N O . 1 3 , 2 0 1 4 Jacobs et al.S E P T E M B E R 3 0 , 2 0 1 4 : 1 3 7 3 – 8 4 Evolution and Future of ACC/AHA CPGs
1383
and methodology, that is, to lead rather than lag behindclinical practice, remains an ongoing challenge. Theaddition of formal systematic reviews, expansion of thepeer review process to include patients and other stake-holders, and selection of the GWC in accordance with astrict RWI policy are time-consuming endeavors. Futurechallenges in delineation of RWI policy include recog-nition that manufacturers of recently approved devicesare typically required to provide operator training topromote safe deployment of new technology. The ACCand AHA encourage training of clinicians to ensure suffi-cient expertise while requiring disclosure of industry-sponsored training by members of GWCs. Although thedelivery of timely CPGs is essential, it is also important tobalance speed with deliberation and accuracy and toallow new treatments to adequately dwell in the clinicalarena to assess generalizability and long-term outcomesin clinical practice.
Most apparent, particularly to members of the GWC,are the gaps in evidence. A lack of quality studies in manyareas contributes to the relatively high proportion of LOEC/E recommendations, particularly in the many specificconditions and circumstances where clinicians needguidance. Like the research on which most recom-mendations are based, clinical science is an iterativeprocess in continual evolution. Initiatives such as theAHA’s Get With the Guidelines and Mission: Lifeline andthe ACC’s Door to Balloon Alliance and Hospital2Homehave led to improvements in quality of care. However, therelative paucity of funding for implementation scienceand other barriers challenge the uptake of CPG recom-mendations in the clinical community.
Furthermore, despite the privilege and reward ofserving on ERCs or GWCs, the requisite time commitmentmay preclude participation in future endeavors as thedemands of clinical practice and academic responsibilitiescontinue to increase.
FUTURE DIRECTIONS
Looking to the future, it is clear that the ACC/AHACPG methodology will evolve in response to a changinghealthcare environment and the availability of newformats with which to deliver recommendations. Creationof ongoing “living” documents is under development on
various digital platforms. Embedding CPG recom-mendations and prompts within electronic medical recordsystems and mobile devices accessible at the point of carewill require new ways of crafting and parsing informationinto “bytes” of data that support individual recom-mendations and will require resource utilization efforts.
Although past GWCs have excluded cost con-siderations from recommendations, it is clear that withlimited healthcare resources and rising costs, it is impor-tant and appropriate to consider cost, cost-effectiveness,and value. Going forward, it is recommended that theCOR and LOE criteria summarizing the strength/level andquality of evidence supporting clinical benefit, based onvalidated evidence assessment tools, be supplemented byan assessment of value (17). Furthermore, although CPGsare more broadly disease based (rather than procedurebased), the documents are sometimes crafted in silos;recognition and incorporation of multiple comorbiditieswill become increasingly important as the patient pop-ulation ages and people live longer with more advancedcardiovascular disease. The future also may see innova-tions in clinical trial designs and an important interactionbetween CPGs and data registries, which may expandpatient/subject subgroups of interest poorly representedin clinical trials and create a “learning health system”
where a continuous cycle of evidence-based practiceleads to feedback of practice-based evidence to validateand further refine clinical evidence (18).
To maintain consistency and facilitate implementationof CPG recommendations, it is important to harmonizeour CPGs with those issued by other organizationswithin the United States and abroad. Notwithstandingdifferences in resources, economy, RWI policies, andavailability of guideline-directed medical therapies, har-monization across CPGs has the potential to minimizeconfusion in the caregiver community and enhanceadherence to recommendations.
Perhaps most important is to preserve the steadfastcommitment to the development and dissemination ofCPGs based on a thorough, unbiased evaluation of avail-able evidence combined with a focus on patient-centriccare and shared decision making. What will remainunchanged is the overall goal of providing guidance toclinicians to improve quality of care and outcomes forpatients with cardiovascular disease.
RE F E RENCE S
1. Committee on Standards for Developing Trust-worthy Clinical Practice Guidelines, Institute of Medi-cine. Clinical Practice Guidelines We Can Trust.Washington, DC: The National Academies Press, 2011.
2. Committee on Standards for Systematic Reviews ofComparative Effectiveness Research, Institute ofMedicine. Finding What Works in Health Care:
Standards for Systematic Reviews. Washington, DC:The National Academies Press, 2011.
3. Jacobs AK, Kushner FG, Ettinger SM, et al. ACCF/AHA clinical practice guideline methodology summitreport: a report of the American College of CardiologyFoundation/American Heart Association Task Force onPractice Guidelines. J Am Coll Cardiol. 2013;61:213–65.
4. Bittl JA, He Y, Jacobs AK, et al. Bayesian methodsaffirm the use of percutaneous coronary interventionto improve survival in patients with unprotected leftmain coronary artery disease. Circulation. 2013;127:2177–85.
5. Peterson ED, Roe MT, Mulgund J, et al. Associationbetween hospital process performance and outcomes
Jacobs et al. J A C C V O L . 6 4 , N O . 1 3 , 2 0 1 4
Evolution and Future of ACC/AHA CPGs S E P T E M B E R 3 0 , 2 0 1 4 : 1 3 7 3 – 8 4
1384
among patients with acute coronary syndromes. JAMA.2006;295:1912–20.
6. Fonarow GC. The Acute Decompensated HeartFailure National Registry (ADHERE): opportunities toimprove care of patients hospitalized with acutedecompensated heart failure. Rev Cardiovasc Med.2003;4 Suppl 7:S21–30.
7. Kung J, Miller RR, Mackowiak PA. Failure of clinicalpractice guidelines to meet Institute of Medicinestandards: two more decades of little, if any, progress.Arch Intern Med. 2012;172:1628–33.
8. Shaneyfelt T. In guidelines we cannot trust. ArchIntern Med. 2012;172:1633–4.
9. ACCF/AHA Task Force on Practice Guidelines.Methodology Manual and Policies From the ACCF/AHATask Force on Practice Guidelines. Available at: http://assets.cardiosource.com/Methodology_Manual_for_ACC_AHA_Writing_Committees.pdf and http://my.americanheart.org/idc/groups/ahamah-public/@wcm/@sop/documents/downloadable/ucm_319826.pdf. American College of Cardiology and AmericanHeart Association. Accessed May 12, 2014.
10. Shaneyfelt TM, Centor RM. Reassessment of clin-ical practice guidelines: go gently into that good night.JAMA. 2009;301:868–9.
11. Nishimura RA, Otto CM, Bonow RO, et al. 2014AHA/ACC guideline for the management of patientswith valvular heart disease: a report of the American
CommitteeMember Employment
Jeffrey L. Anderson Intermountain Heart Institute,Intermountain Healthcare—AChief of Cardiology
Jonathan L. Halperin The Cardiovascular Institute, MMedical Center, Division of CProfessor of Medicine
Alice K. Jacobs Boston University School of MeProfessor of Medicine; BostCenter, Department of MedChair for Clinical Affairs
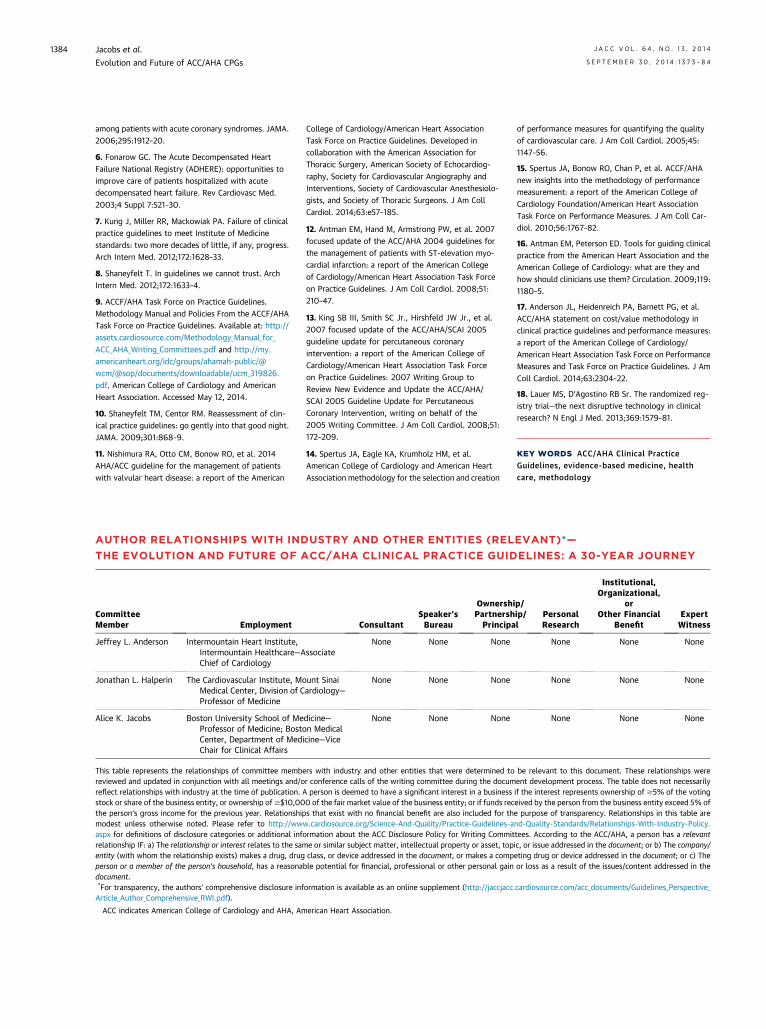
This table represents the relationships of committee membreviewed and updated in conjunction with all meetings and/oreflect relationships with industry at the time of publication.stock or share of the business entity, or ownership of$$10,00the person’s gross income for the previous year. Relationshipmodest unless otherwise noted. Please refer to http://wwaspx for definitions of disclosure categories or additional infrelationship IF: a) The relationship or interest relates to the samentity (with whom the relationship exists) makes a drug, drugperson or a member of the person’s household, has a reasonadocument.*For transparency, the authors’ comprehensive disclosure inf
College of Cardiology/American Heart AssociationTask Force on Practice Guidelines. Developed incollaboration with the American Association forThoracic Surgery, American Society of Echocardiog-raphy, Society for Cardiovascular Angiography andInterventions, Society of Cardiovascular Anesthesiolo-gists, and Society of Thoracic Surgeons. J Am CollCardiol. 2014;63:e57–185.
12. Antman EM, Hand M, Armstrong PW, et al. 2007focused update of the ACC/AHA 2004 guidelines forthe management of patients with ST-elevation myo-cardial infarction: a report of the American Collegeof Cardiology/American Heart Association Task Forceon Practice Guidelines. J Am Coll Cardiol. 2008;51:210–47.
13. King SB III, Smith SC Jr., Hirshfeld JW Jr., et al.2007 focused update of the ACC/AHA/SCAI 2005guideline update for percutaneous coronaryintervention: a report of the American College ofCardiology/American Heart Association Task Forceon Practice Guidelines: 2007 Writing Group toReview New Evidence and Update the ACC/AHA/SCAI 2005 Guideline Update for PercutaneousCoronary Intervention, writing on behalf of the2005 Writing Committee. J Am Coll Cardiol. 2008;51:172–209.
14. Spertus JA, Eagle KA, Krumholz HM, et al.American College of Cardiology and American HeartAssociation methodology for the selection and creation
ConsultantSpeaker’sBureau
OwnershiPartnershPrincipa
ssociateNone None None
ount Sinaiardiology—
None None None
dicine—on Medicalicine—Vice
None None None
ers with industry and other entities that were determined tor conference calls of the writing committee during the documA person is deemed to have a significant interest in a business0 of the fair market value of the business entity; or if funds recs that exist with no financial benefit are also included for thw.cardiosource.org/Science-And-Quality/Practice-Guidelines-aormation about the ACC Disclosure Policy for Writing Commite or similar subject matter, intellectual property or asset, topclass, or device addressed in the document, or makes a comp
ble potential for financial, professional or other personal gain
ormation is available as an online supplement (http://jaccjacc.
of performance measures for quantifying the qualityof cardiovascular care. J Am Coll Cardiol. 2005;45:1147–56.
15. Spertus JA, Bonow RO, Chan P, et al. ACCF/AHAnew insights into the methodology of performancemeasurement: a report of the American College ofCardiology Foundation/American Heart AssociationTask Force on Performance Measures. J Am Coll Car-diol. 2010;56:1767–82.
16. Antman EM, Peterson ED. Tools for guiding clinicalpractice from the American Heart Association and theAmerican College of Cardiology: what are they andhow should clinicians use them? Circulation. 2009;119:1180–5.
17. Anderson JL, Heidenreich PA, Barnett PG, et al.ACC/AHA statement on cost/value methodology inclinical practice guidelines and performance measures:a report of the American College of Cardiology/American Heart Association Task Force on PerformanceMeasures and Task Force on Practice Guidelines. J AmColl Cardiol. 2014;63:2304–22.
18. Lauer MS, D’Agostino RB Sr. The randomized reg-istry trial—the next disruptive technology in clinicalresearch? N Engl J Med. 2013;369:1579–81.
KEY WORDS ACC/AHA Clinical PracticeGuidelines, evidence-based medicine, healthcare, methodology
AUTHOR RELATIONSHIPS WITH INDUSTRY AND OTHER ENTITIES (RELEVANT)*—
THE EVOLUTION AND FUTURE OF ACC/AHA CLINICAL PRACTICE GUIDELINES: A 30-YEAR JOURNEY
p/ip/l
PersonalResearch
Institutional,Organizational,
orOther Financial
BenefitExpertWitness
None None None
None None None
None None None
be relevant to this document. These relationships wereent development process. The table does not necessarilyif the interest represents ownership of $5% of the votingeived by the person from the business entity exceed 5% ofe purpose of transparency. Relationships in this table arend-Quality-Standards/Relationships-With-Industry-Policy.tees. According to the ACC/AHA, a person has a relevantic, or issue addressed in the document; or b) The company/eting drug or device addressed in the document; or c) Theor loss as a result of the issues/content addressed in the
cardiosource.com/acc_documents/Guidelines_Perspective_
Article_Author_Comprehensive_RWI.pdf).ACC indicates American College of Cardiology and AHA, American Heart Association.
http://my.americanheart.org/idc/groups/ahamah-public/@wcm/@sop/documents/downloadable/ucm_319826.pdf
http://my.americanheart.org/idc/groups/ahamah-public/@wcm/@sop/documents/downloadable/ucm_319826.pdf
http://my.americanheart.org/idc/groups/ahamah-public/@wcm/@sop/documents/downloadable/ucm_319826.pdf