The Everting Suture: A New Technical Aid for Ureteral Nipple Construction
2
Vol. 155,1372-1373. Apnl 1996 Prrnfcd fn U.S.A. Urologists At Work THE EVERTING SUTURE: A NEW TECHNICAL AID FOR URETERAL NIPPLE CONSTRUCTION MOWED ADEL ATTA From the Department of Urology, Alexandria School of Medicine, Alexandria, Egypt ABSTRACT Purpose: A new technique using an everting suture to construct a ureteral nipple is described. Materials and Methods: The method was used to create 28 ureteral nipples. A 2-zero silk suture is passed through the ureteral wall, transfming the lumen, and is tied 5 cm. away from the ureteral wall. The ends are cut 10 cm. long. The suture is grasped within the ureteral lumen and with traction the ureter is everted in 1 step without trauma. Results: The suture resulted in smooth 1-step atraumatic eversion of the ureter in all cases. Conclusions: With this technique a well formed nipple of the desired length can be constructed. KEY WORDS: ureter, urinary diversion, suture techniques, sutures A nipple is an efficient valve mechanism that prevents retrograde flow of fluid. Nipples constructed with jejunum have been used to prevent reflw of intestinal contents into a feeding cutaneous jejunostomy.' The efficacy and applicabil- ity of the nipple mechanism as a leakproof valve in biliary, pancreatic, gastrointestinal and urinary tracts have been shown in experimental as well as clinical studies.'--5 Re- cently, the ileal nipple technique has been revived and used in continent urinary diversions to provide a continent uri- nary cutaneous stoma as well as to prevent ureteral reflux.6.7 The ureteral nipple, on the other hand, is not widely used as an antireflux mechanism, although it was introduced in early clinical and experimental studies.8-12 A technique is de- scribed using an everting suture to facilitate ureteral nipple construction, which is sometimes difficult and requires re- peated manipulations of a delicate structure. PATIENTS AND METHODS The technique was performed during 28 ureteral reimplan- tations, including 24 ureterointestinal and 4 ureterovesical anastomoses. A 2-zero silk suture is passed through the ureter 2 cm. proximal to the stoma (the desired length of the nipple), transfixing the ureteral lumen (fig. 1, A). The suture is tied 5 cm. away from the ureteral wall and the ends are cut 10 cm. long. A fine, nontoothed forceps is passed through the ureteral lumen to grasp and pull up the suture (fig. 1, B). The ureteral orifice is spatulated and, with continuous traction on the suture, the ureteral wall is easily everted using 2 fine nontoothed forceps to hold the edges. Four basal fixation sutures are then passed between the ureteral and bladder or intestinal edges, and through the adventitia of the ureter at the entrance into the bladder (fig. 2, A). The suture is cut and easily removed by pulling the long threads (fig. 2, B). RESULTS The everting suture resulted in simple, smooth, atraumatic eversion of the ureter in all cases. Eversion was accomplished in 1 step and in no case did the suture cut through the ureter. Urine was seen efluxing from the new orifice and ureteral stents were not needed. Followup studies, including ascend- Accepted for publication September 22, 1995. A 3 FIG. 1. A, 2-zero silk suture is passed through ureter 2 cm. prox- imal to stoma (desired length of nipple), transfixing ureteral lumen. B, suture is tied 5 cm. away from ureteral wall and ends are cut 10 cm. long. Fine, nontoothed forceps is passed through ureteral lumen to grasp and pull up suture. Ureteral orifice is spatulated and, with continuous traction on everting suture, ureteral wall is easily everted. ing images, revealed no reflw 3 to 5 months postoperatively in 5 cases and endoscopy of the intestinal pouch showed an intact nipple in 3. DISCUSSION The use of a nipple mechanism in the ureter to prevent reflux has some advantages. The resulting new ureteral ori- fice after construction has intact epithelium and, accordingly, little chance of early postoperative edema or late stricture formation. Also, for dilated thick-walled ureters, as occurs with bilharziasis, the choice of antireflux techniques is lim- ited, with tailoring and tunneling frequently resulting in 1372
-
Upload
mohamed-adel -
Category
Documents
-
view
213 -
download
1
Transcript of The Everting Suture: A New Technical Aid for Ureteral Nipple Construction

Vol. 155, 1372-1373. Apnl 1996 Prrnfcd f n U.S.A.
Urologists At Work
THE EVERTING SUTURE: A NEW TECHNICAL AID FOR URETERAL NIPPLE CONSTRUCTION
M O W E D ADEL ATTA From the Department of Urology, Alexandria School of Medicine, Alexandria, Egypt
ABSTRACT
Purpose: A new technique using an everting suture to construct a ureteral nipple is described. Materials and Methods: The method was used to create 28 ureteral nipples. A 2-zero silk
suture is passed through the ureteral wall, transfming the lumen, and is tied 5 cm. away from the ureteral wall. The ends are cut 10 cm. long. The suture is grasped within the ureteral lumen and with traction the ureter is everted in 1 step without trauma.
Results: The suture resulted in smooth 1-step atraumatic eversion of the ureter in all cases. Conclusions: With this technique a well formed nipple of the desired length can be constructed.
KEY WORDS: ureter, urinary diversion, suture techniques, sutures
A nipple is an efficient valve mechanism that prevents retrograde flow of fluid. Nipples constructed with jejunum have been used to prevent reflw of intestinal contents into a feeding cutaneous jejunostomy.' The efficacy and applicabil- ity of the nipple mechanism as a leakproof valve in biliary, pancreatic, gastrointestinal and urinary tracts have been shown in experimental as well as clinical studies.'--5 Re- cently, the ileal nipple technique has been revived and used in continent urinary diversions to provide a continent uri- nary cutaneous stoma as well as to prevent ureteral reflux.6.7 The ureteral nipple, on the other hand, is not widely used as an antireflux mechanism, although it was introduced in early clinical and experimental studies.8-12 A technique is de- scribed using an everting suture to facilitate ureteral nipple construction, which is sometimes difficult and requires re- peated manipulations of a delicate structure.
PATIENTS AND METHODS
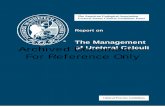
The technique was performed during 28 ureteral reimplan- tations, including 24 ureterointestinal and 4 ureterovesical anastomoses. A 2-zero silk suture is passed through the ureter 2 cm. proximal to the stoma (the desired length of the nipple), transfixing the ureteral lumen (fig. 1, A) . The suture is tied 5 cm. away from the ureteral wall and the ends are cut 10 cm. long. A fine, nontoothed forceps is passed through the ureteral lumen to grasp and pull up the suture (fig. 1, B ) . The ureteral orifice is spatulated and, with continuous traction on the suture, the ureteral wall is easily everted using 2 fine nontoothed forceps to hold the edges. Four basal fixation sutures are then passed between the ureteral and bladder or intestinal edges, and through the adventitia of the ureter at the entrance into the bladder (fig. 2, A) . The suture is cut and easily removed by pulling the long threads (fig. 2, B ) .
RESULTS
The everting suture resulted in simple, smooth, atraumatic eversion of the ureter in all cases. Eversion was accomplished in 1 step and in no case did the suture cut through the ureter. Urine was seen efluxing from the new orifice and ureteral stents were not needed. Followup studies, including ascend-
Accepted for publication September 22, 1995.
A 3
FIG. 1. A, 2-zero silk suture is passed through ureter 2 cm. prox- imal to stoma (desired length of nipple), transfixing ureteral lumen. B, suture is tied 5 cm. away from ureteral wall and ends are cut 10 cm. long. Fine, nontoothed forceps is passed through ureteral lumen to grasp and pull up suture. Ureteral orifice is spatulated and, with continuous traction on everting suture, ureteral wall is easily everted.
ing images, revealed no reflw 3 to 5 months postoperatively in 5 cases and endoscopy of the intestinal pouch showed an intact nipple in 3.
DISCUSSION
The use of a nipple mechanism in the ureter to prevent reflux has some advantages. The resulting new ureteral ori- fice after construction has intact epithelium and, accordingly, little chance of early postoperative edema or late stricture formation. Also, for dilated thick-walled ureters, as occurs with bilharziasis, the choice of antireflux techniques is lim- ited, with tailoring and tunneling frequently resulting in
1372

A EVERTING SUTURE FOR URETERAL NIPPLE CONSTRUCTION 1373
REFERENCES
1. Perl, J . I.: Intussuscepted conical valve formation in jejunosto- mies. Surgery, 2 5 297, 1949.
2. Basso, D. E.: Efficacy and applicability of an intussuscepted conical valve in preventing regurgitation and leakage of intes- tinal contents. Ann. Surg., 133 477, 1951.
3. Smith, G. I. and Hinman, F., Jr.: The intussuscepted ileal cys- tostomy. J. Urol., 7 3 261, 1955.
4. Turner, R. D. and Goodwin, W. E.: Experience with intussus- cepted ileal valve in ureteral substitution. J. Urol., 81: 526, 1959.
5. Bergman, B. and Nilson, A. E. V.: Intussusception of the ileal loop: an operative method for preventing urinary backflow in ileal conduits. J. Urol., 112: 735, 1974.
6. Reiner, W. G. and Jeffs, R. D.: Ileal intussusception as an anti- reflux mechanism in urinary diversion for myelomeningocele. J. Urol., 121: 212, 1979.
7. &&, N. G., Nilson, A. E., Nilsson, L. 0.. Norlen, L. J. and Philipson, B. M.: Urinary diversion via a continent ileal reservoir: clinical results in 12 patients. J . Urol., 128: 469,
8. ill, J. E., Dodson, A. I., Jr. and Hooper, J. W., Jr.: Experimental ureteroneocystostorny using nipple anastomosis technique. J. Urol., 7 4 596, 1955.
9. Councill, W. A. H., Jr.: Surgical treatment of vesicoureteral
B
u - . ./-
FIG. 2. A, 4 basal fixation sutures are passed between ureteral and bladder or intestinal edges through adventitia of ureter a t en- trance into bladder. B, suture is then cut and removed easily by pulling long threads.
1982. sten0sis.1~ Since the ileal nipple works effectively to Prevent reflux, the dilated ureter should work similarly.
CONCLUSIONS reflux. South Med. J., 4 9 1104, 1956.
10. Grey, D. N.9 F l P n , p. and hodwin , w. E.: Experimenta1 meth- ods of ureteroneocystostomy: experiences with the intestinal intussusception to produce a nipple or valve. J . Urol., 77: 154,
Eversion of the ureter to form a nipple is frequently cum-
structure, which may be injured. The everting suture de- scribed was used successfullv in normal as well as dilated
bersome and requires repeated manipulations of a delicate
rnrr) LJJ I .
ureters, and resulted in simple, atraumatic ureteral ever- sion. The suture does not cut through the ureteral wall even under strong traction because the force of traction is evenly distributed along half of the circumference of the ureteral wall. Another advantage of the technique is easy control of the length of the ureteral nipple formed.
11. Taylor, J. N. and Jasper, W. s.: Experimental ureteroneocystos- torny by Mathisen technique. J . Urol., 77: 709, 1957.
12. Labardini, M. M. and Kallet, H. A,: Experimental ureteroneo- cystostomy: preliminary report. J . Urol., 101: 171, 1969.
13. Arafa, A,: Management of Bilharzial Stricture of the Ureter. M. D. Thesis, Alexandria University, Alexandria, Egypt, 1972.