The Evaluation Of Ischemia. Case A 58 year old woman with diabetes and hypertension presents with...
52
The Evaluation Of Ischemia
-
Upload
kristin-lane -
Category
Documents
-
view
215 -
download
0
Transcript of The Evaluation Of Ischemia. Case A 58 year old woman with diabetes and hypertension presents with...
The Evaluation Of Ischemia

Case
• A 58 year old woman with diabetes and hypertension presents with symptoms of chronic chest pain. She reports that she can walk about 4 blocks at a moderate pace before developing squeezing chest pain, shortness of breath and diaphoresis that resolves with rest. An EKG in the office is normal.
Case
• What is the best next step?– Give her nitroglycerin sublingual and order a
treadmill stress test– Refer for emergent angiography– Order nuclear perfusion imaging– Start ASA, BB, nitrates and monitor symptoms
Case
• During a treadmill stress test she exercises for 6 minutes and stops for chest discomfort. There are infer-lateral ST depressions and nuclear imaging shows a moderate sized reversible inferior defect and no fixed defects. Which of the following is true?– An angiogram followed by a stent will improve her
symptoms– An angiogram follow by a stent with improve her
symptoms and prolong her life– The patient should be sent for a CABG – The patients medical therapy is not optimized
CAD And Angina: Significant Morbidity and Mortality
• Incidence 213/100,000 over 30• Lifetime risk: nearly 50% men, 32% women• 13,200,000 with CAD, 6,500,000 with angina• 7,200,000 post MI• 53% of cardiovascular deaths• About 1 in 5 deaths in Americans• 142.5 billion in 2006• 11.1 million deaths worldwide by 2020
Libby. Braunwald’s Heart Disease. 8th Ed.

Cumulative Risk Of CAD Remains High In Advanced Age
Lloyd-Jones. Lancet, 1999.
Angina• Chest or surrounding area caused by ischemia• Brought on by exertion• No associated with myocardial necrosis• Variety of discomfort
– Heavy, squeezing, pressure numb burning• Location
– Substernal, arms, epigastric• Anginal equivalents
– Dyspnea, faintness, fatigue• Duration
– Better with rest or nitroglycerin
Not Angina
• Pleuritic pain• Highly localized pain• Reproduced by movement• Duration very long or very short• Pain radiating to the lower extremities• Resolution more than 5-10 minutes after
nitrates or rest
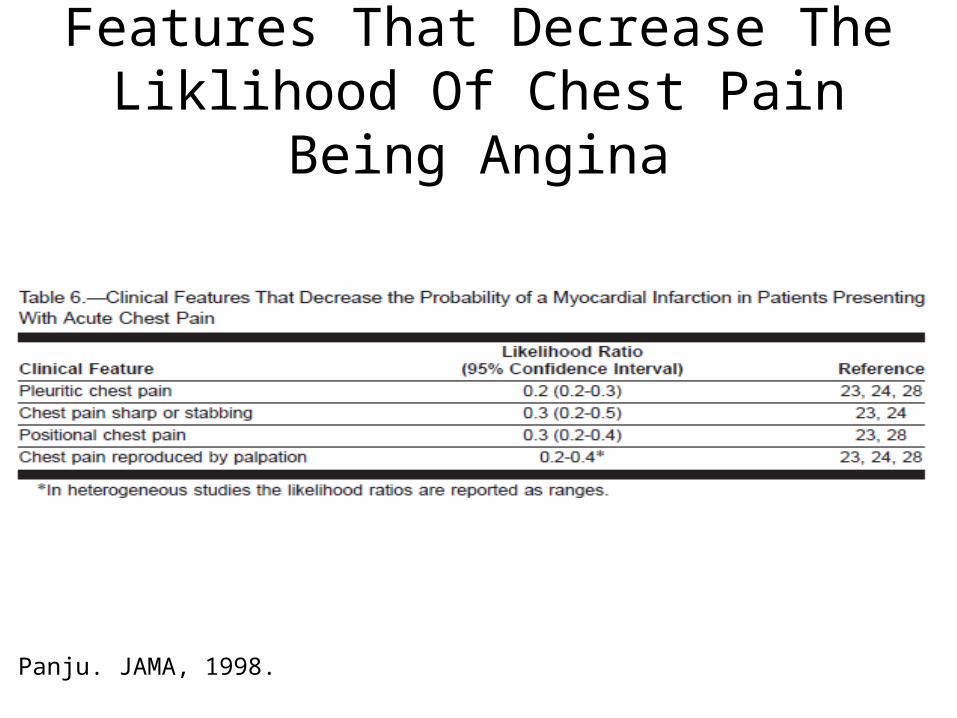
Features That Decrease The Liklihood Of Chest Pain Being Angina
Panju. JAMA, 1998.

Grading Angina
• Class I: angina with strenuous activity• Class II: Slight limitation of ordinary activity• Class III: Marked limitation of ordinary activity• Class IV: Inability to do any physical activity or
angina at rest
Goldman. Circulation, 1981.

If It Is Not From The Heart….
Panju. JAMA, 1998.
Pathophysiology
• Regional myocardial ischemia– Inadequate coronary blood flow– Increased myocardial oxygen demand

Pathology of Atherosclerosis
Abrams. NEJM, 2005.
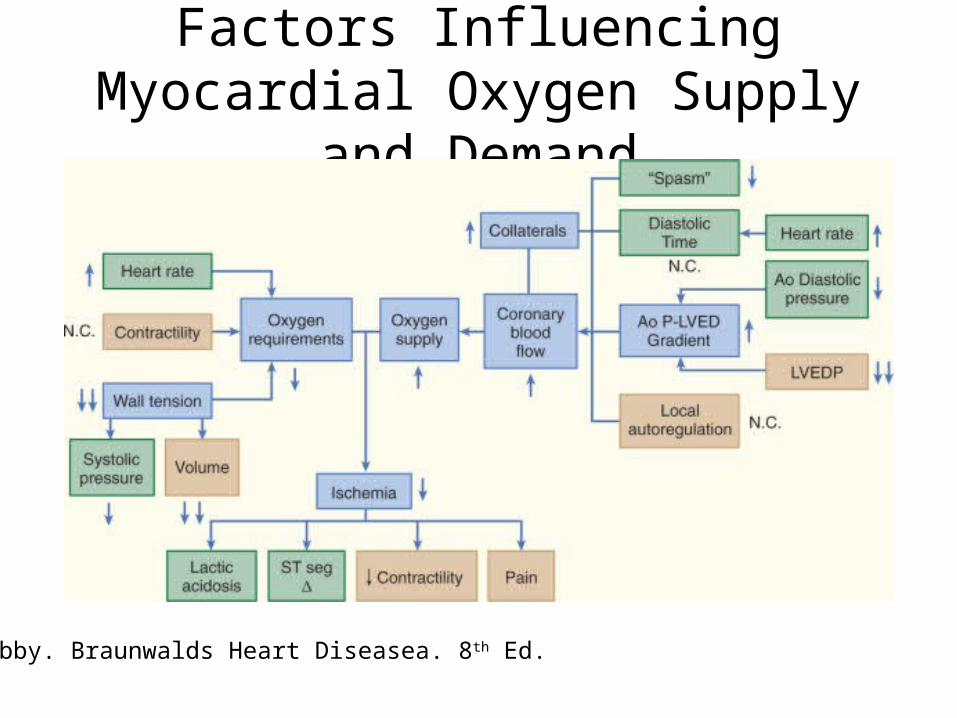
Factors Influencing Myocardial Oxygen Supply and Demand
Libby. Braunwalds Heart Diseasea. 8th Ed.

Cardiovascular Risk Assessment
• Very high risk: no further estimation– Established vascular disease
• Prior MI = 5-7x risk of recurrent MI• Prior stroke= 2-3x risk of MI• PVD = 4x risk of MI
– Diabetes– Chronic kidney disease– Hereditary dislipidemia
Canto. JAMA, 2003.
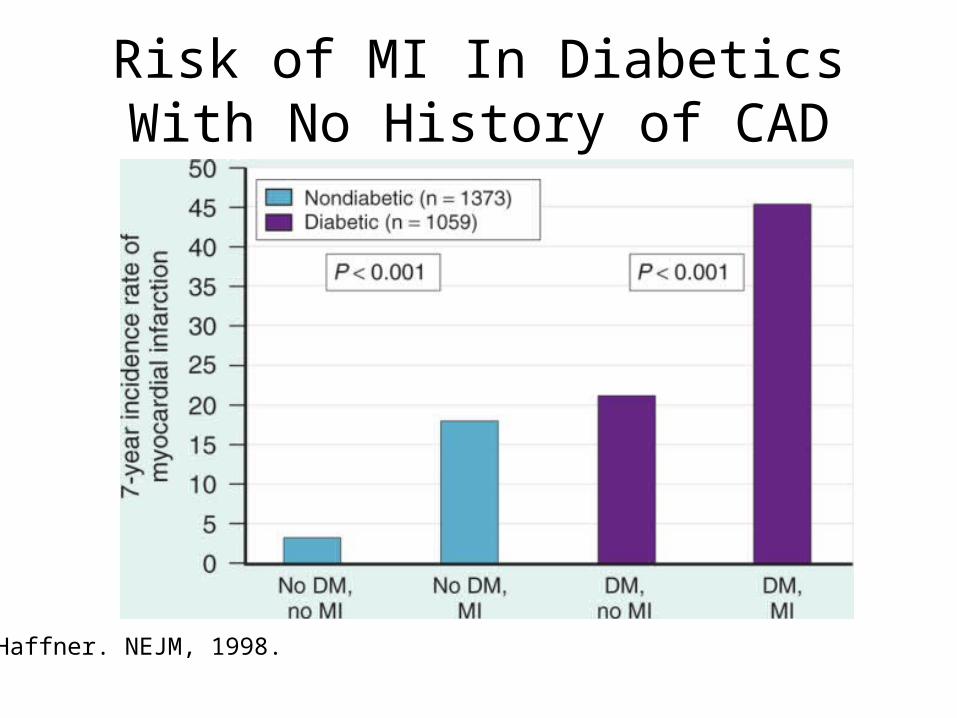
Risk of MI In Diabetics With No History of CAD
Haffner. NEJM, 1998.
Why Assess Risk?
• Required for determination of medical management
• More than 90% of CHD events in patients with at least one risk factor

Risk Factors Associated With CAD
Yusuf. Lancet, 2004.

Framingham Risk Calculator
• Predicts risk of MI, CAD death and angina– Low risk <10% risk in 10 years– Intermediate 10-20% risk in 10 years– High risk >20% in 10 years

Risk Assessment Tools: Framingham Risk Calculator
Other Risk Calculators
• SCORE• QRISK/QRISK 2• Reynolds

Limitations Of Risk Calculation
• Falsely reassure patients with borderline risk factors
• Does not consider lifetime risk• Inability to account for effects of current
therapy• Variation in severity of first event• Variation by type of vascular disease

High Sensitivity CRP: Additive Value?
• Most patients with CAD have traditional risk factors
• Unclear that CRP adds value in clinical practice to traditional risk factors
Evaluation of Anginal Chest Pain
• Risk factor assessment• Physical Examination• Resting electrocardiogram
Asymptomatic Patients
• No need for stress testing

Non Invasive Stress Testing In Symptomatic Patients
• Not useful for diagnosis of CAD in low risk or high risk patients
• Useful if it will alter the planned management strategy
Treadmill Stress Testing
• Useful in patients who can:– Exercise on the treadmill adequately– Have a interpretable EKG

Echo Stress Testing
• Can be performed with exercise or with dobutamine
• Requires adequate echo visualization of the heart
Nuclear Stress Testing
• Can be performed with exercise vasodilator drugs– Adenosine– Dipyridamole
• Nuclear tracer is distributed in areas with normal blood flow
• Requires contrast between areas of the heart– False negatives with global ischemia
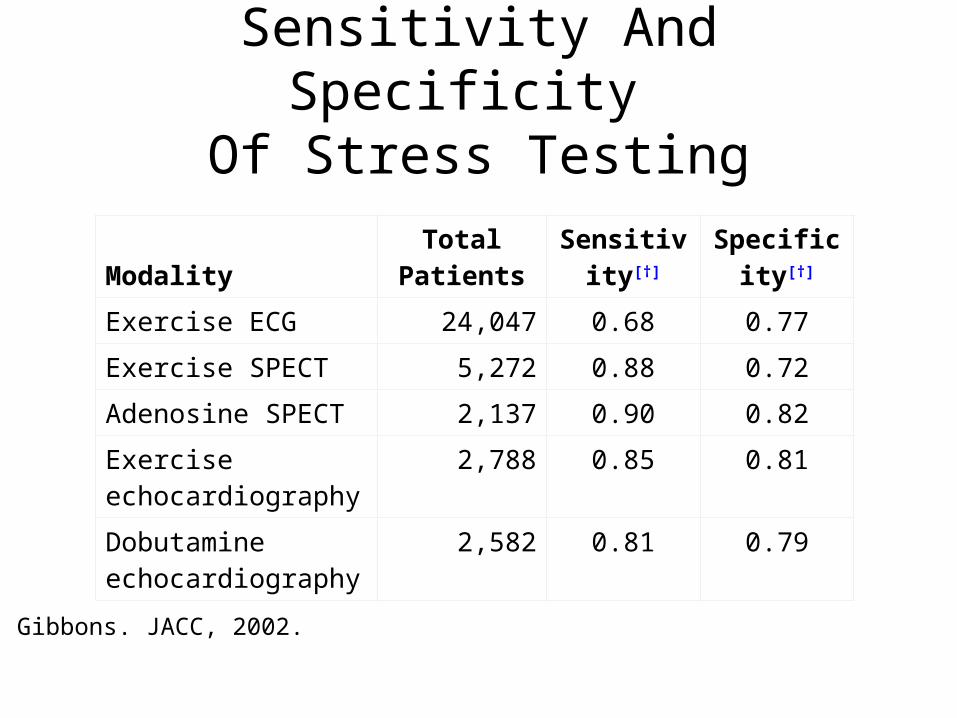
Sensitivity And Specificity Of Stress Testing
ModalityTotal
PatientsSensitivity
[†]
Specificity[†]
Exercise ECG 24,047 0.68 0.77
Exercise SPECT 5,272 0.88 0.72
Adenosine SPECT 2,137 0.90 0.82
Exercise echocardiography
2,788 0.85 0.81
Dobutamine echocardiography
2,582 0.81 0.79
Gibbons. JACC, 2002.

High Risk Stress Test Features: Proceed to Angiography
Gibbons. JACC, 2002.
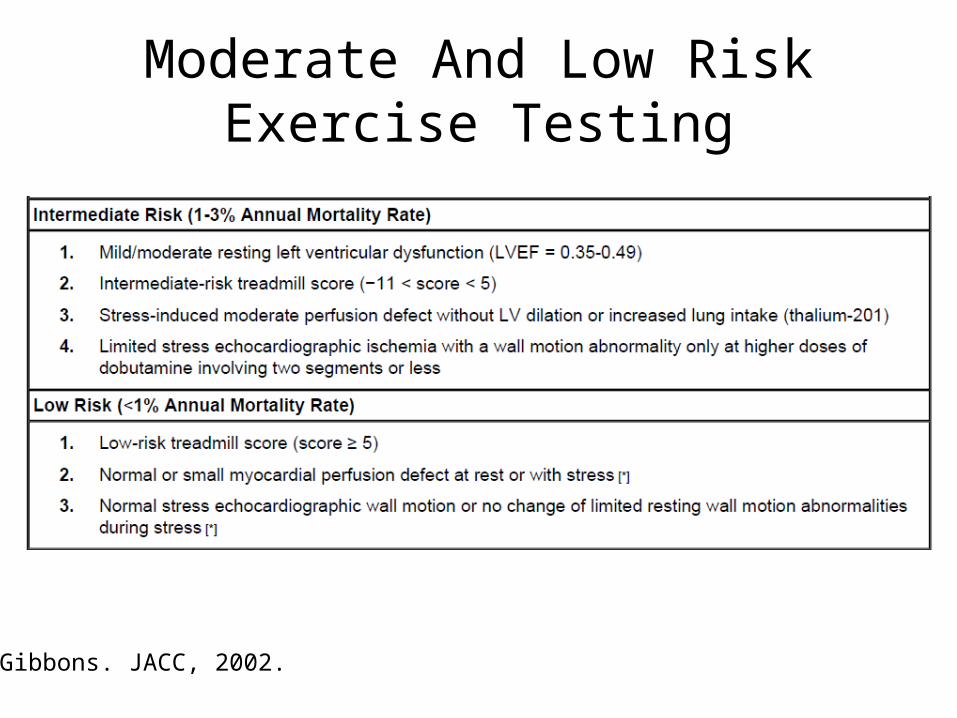
Moderate And Low Risk Exercise Testing
Gibbons. JACC, 2002.
CT Coronary Angiography
• Sensitity 90%• Specificity 50%• Not recommended for clinical use

Coronary Angiography
• Gold standard for identification of significant CAD• Potential for revascularization• Cannot predict future site of plaque rupture and MI• Indications
– Concern for left main or triple vessel disease– Poorly controlled symptoms– Ischemia at a low workload (5-6 mets)– Large or multiple defects or WMA
Assessment of Left Ventricular Function
• Echocardiography or nuclear study• Necessary for strategizing the approach to
management
Treat Medical Conditions That Can Worsen Ischemia
• Anemia• Weight gain• Thyroid disease• Fever • Infections• Tachycardia• Cocaine

Necessary Lifestyle Modification
• Diet • Exercise• Work activities• Leisure activities
– Avoidance of sudden exertion or isometric exercise
• Sexual activity– If equivalent level of activity is well tolerated– Sildenafil cannot be taken with nitrates

Hypertension Management
• For adults, the risk of CAD double for every increase of 20 mmHg over SBP 115
• Predisposes to vascular injury, accelerates CAD, increases myocardial O2 demand and worsens ischemia
• Goals of treatment– Less than 140/90 or– Less than 130/80 in DM or CKD
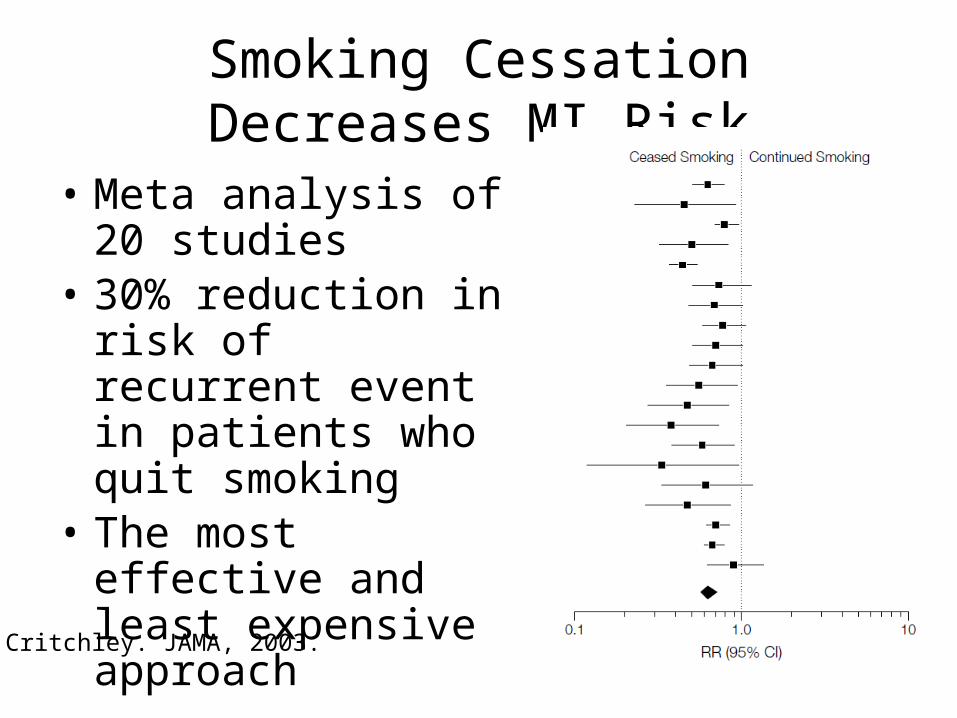
Smoking Cessation Decreases MI Risk
• Meta analysis of 20 studies
• 30% reduction in risk of recurrent event in patients who quit smoking
• The most effective and least expensive approach
Critchley. JAMA, 2003.

Goals Of Medical Management In Stable CAD
• Improve mortality and morbidity • Manage symptoms
– Improve treadmill performance and time to ST changes
• Prevent progression of atherosclerotic disease• Requires adequate dosing and combination
approach

Aspirin
• Myocardial infarction reduction of 34-87%• No difference in 81 vs 325 mg dose • Clopidogrel may substitute for aspirin in
intolerant patients
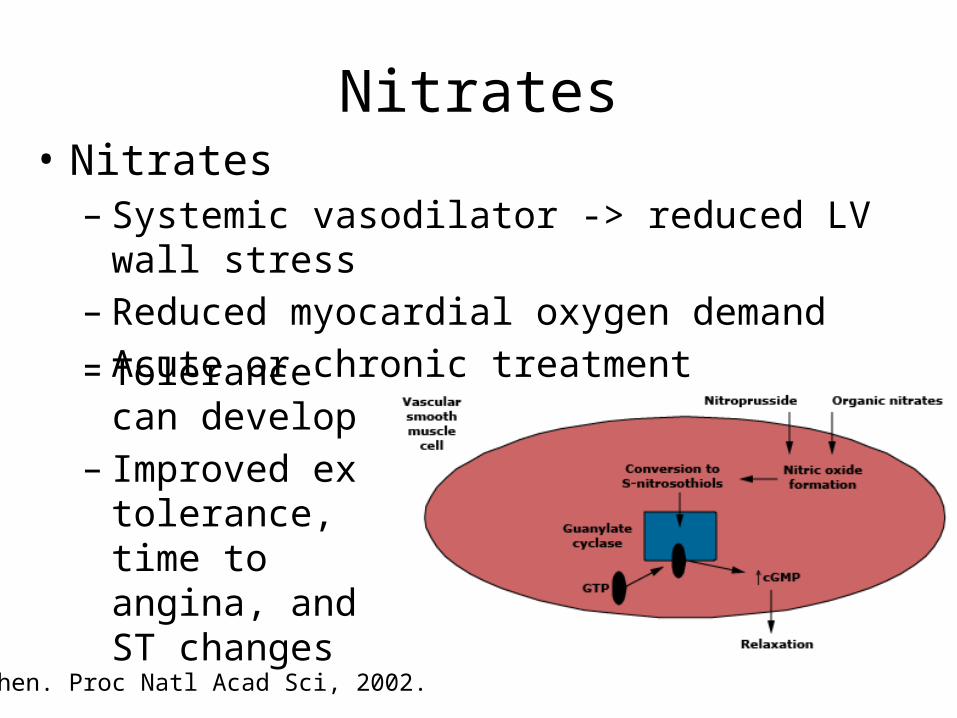
Nitrates
Chen. Proc Natl Acad Sci, 2002.
• Nitrates– Systemic vasodilator -> reduced LV wall stress– Reduced myocardial oxygen demand – Acute or chronic treatment– Tolerance can
develop– Improved ex
tolerance, time to angina, and ST changes
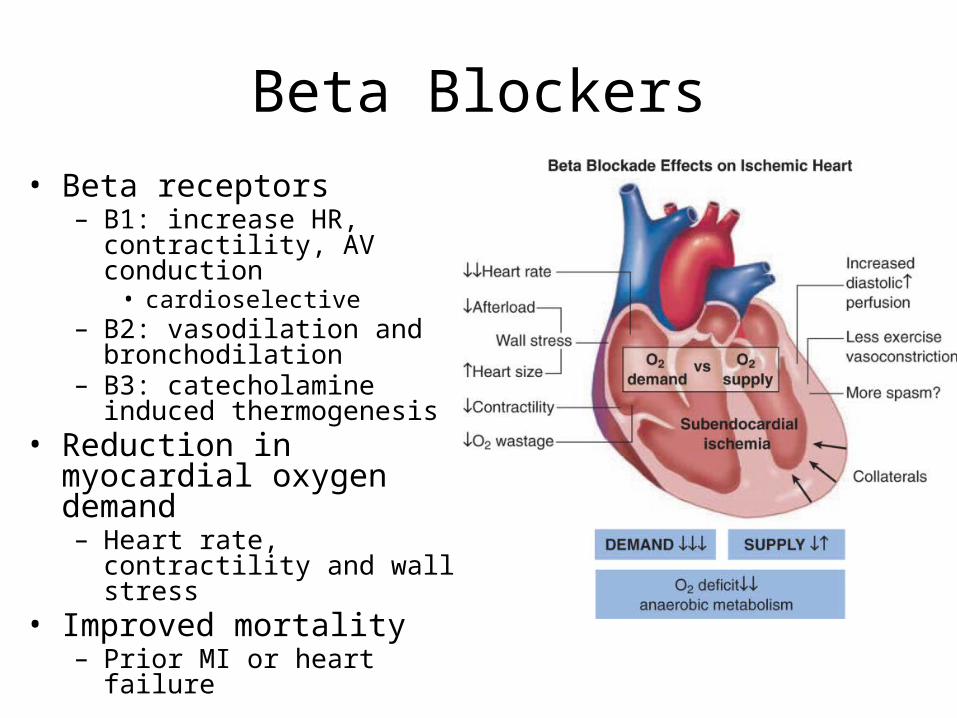
Beta Blockers• Beta receptors
– B1: increase HR, contractility, AV conduction
• cardioselective– B2: vasodilation and
bronchodilation– B3: catecholamine induced
thermogenesis• Reduction in myocardial
oxygen demand– Heart rate, contractility and wall
stress• Improved mortality
– Prior MI or heart failure

ACE Inhibitors
• No benefit in the reduction of ischemia
• Benefits shown in patients with CAD and normal LV function
• Improve endothelial functioning
• HOPE Trial and EUROPA– 20-22% RR ischemic event
HOPE Investigators. NEJM, 2000.
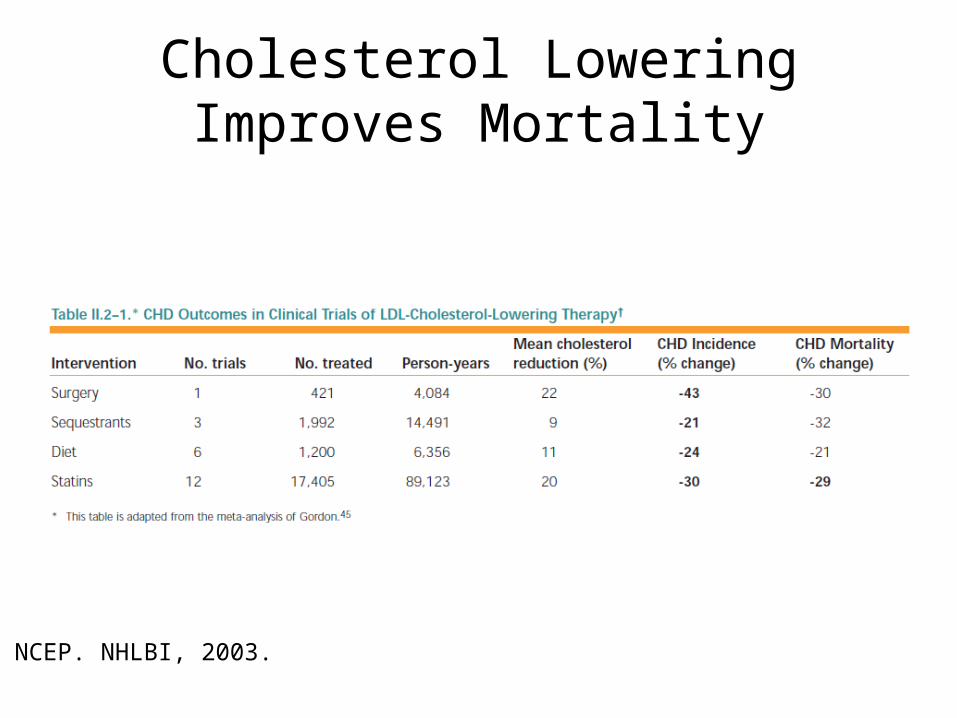
Cholesterol Lowering Improves Mortality
NCEP. NHLBI, 2003.

Number Needed To Treat Is Low
NCEP. NHLBI, 2003.

LDL Target Based On Presence of Risk Factors

After Reaching LDL Goals, Target Non-HDL Cholesterol, Then HDL
• Total cholesterol – HDL= LDL + VLDL• 30 mg/dl higher than LDL goal• Treatment
– Statin followed by niacin or fibrates• Low HDL: <40• Treatment
– Lifestyle modification– Niacin or fibrates

Ranolazine: Novel Antianginal
• No significant changes in heart rate or blood pressure• Reduction in calcium overload via inhibition of the
late Na current• Improved exercise performance and time to ischemia• Slight prolongation of the the QT interval, but no
association with TDP• Contraindicated in pre-existing QT prolongation
Revascularization
• CABG or PCI• No evidence for mortality reduction in
patients with stable angina and normal LV function

Courage Trial: Initial Medical Management vs PCI
• Unclear benefit of PCI in stable CAD• Inclusion criteria
– At least one70% proximal stenosis, and objective ischemia– At least one 80% stenosis and classic angina
• Exclusion criteria– Persistent CCS class IV angina– Markedly positive stress test– Refractory heart failure or cardiogenic shock– EF < 30%– Revascularization within 6 months– Anatomy unfavorable to PCI
• Randomized 1149-> PCI, 1138-> medical management• Endpoints
– Death and nonfatal MI– Death, MI, stroke or unstable angina

Courage Trial: No Difference Between Initial PCI And Medical Management
Boden. NEJM, 2007.