Engelberg Center for Health Care Reform Brookings Institution
The Engelberg Center for Health Care Reform at Brookings | The Dartmouth Institute
June 6–8, 2012
Third Annual National ACO Summit
Follow us on Twitter at @ACO_LN
and use #ACOsummit.
Physician Leadership As An Essential Capability for Transformation and
Accountable Care
Mark Werner, MD, CPE, FACPEChief Clinical Integration Officer
Fairview Health ServicesMinneapolis, MN
Fairview Overview• Not-for-profit established in 1906• Academic Health System since 1997
partnership with University of MN• Named a top 10 U.S. health system by
Thomson Reuters (2009)• 22,000+ employees• 2,500 aligned physicians
−
Employed−
Faculty −
Independent
• 8 hospitals/medical centers (1,515 staffed beds)
• 42 primary care clinics• 55-plus specialty clinics• 278-providers included in model• 55 - New Hires since fall 2009• 25 -Attrition since fall 2009
Vital Statistics•
4.8 million outpatient encounters •
80,314 inpatient admissions•
$333.6 million community contributions
•
Total assets of $2.4 billion•
$2.7 billion total revenue
2
One View of Today’s Leadership Challenge
• Creating a sustainable approach to improving health• -health disparities• -aging population• -increasing incidence of chronic diseases• -unsustainable cost increases• Responding to complexity with true system change• -clinical leadership• -sophisticated change management• -community engagement
4
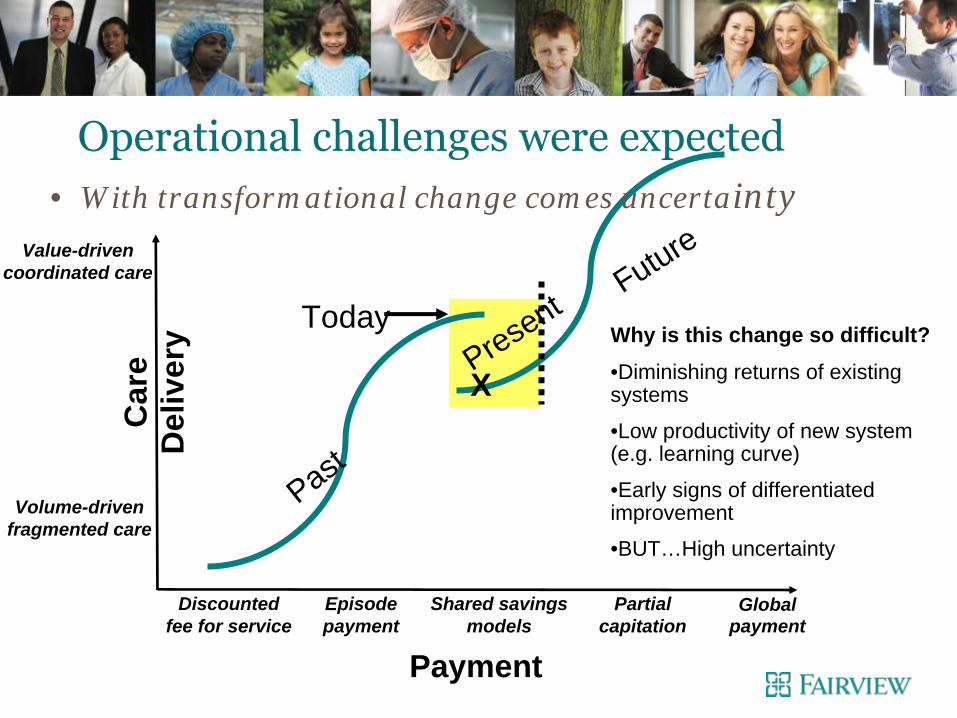
Why is this change so difficult?
•Diminishing returns of existing systems
•Low productivity of new system (e.g. learning curve)
•Early signs of differentiated improvement
•BUT…High uncertainty
Car
e D
eliv
ery
Value-drivencoordinated care
Volume-drivenfragmented care
Discountedfee for service
X
TodayPresent
Episodepayment
Shared savingsmodels
Partialcapitation
Global payment
Past
Future
Payment
• With transformational change comes uncertainty
Operational challenges were expected
5
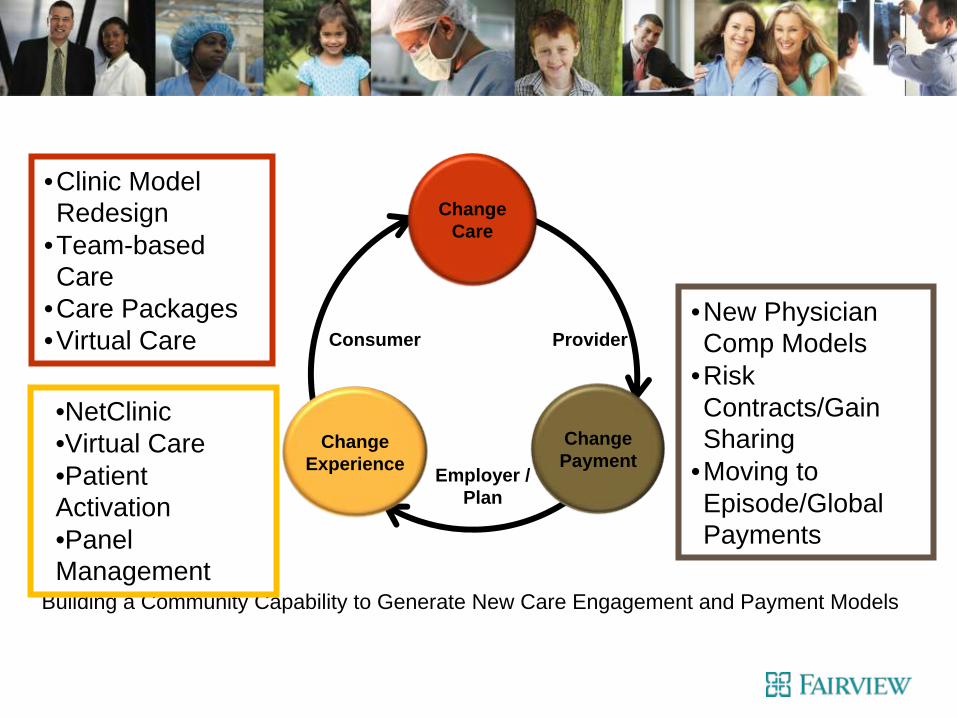
Change Experience
Change Care
Change Payment
Consumer
Employer / Plan
Provider
Building a Community Capability to Generate New Care Engagement and Payment Models
• Clinic Model Redesign
• Team-based Care
• Care Packages• Virtual Care
• New Physician Comp Models
• Risk Contracts/Gain Sharing
• Moving to Episode/Global Payments
•NetClinic•Virtual Care•Patient Activation•Panel Management
6

What Patients Expect From Physicians Negotiating a New Covenant
Then• Creativity• Intuition• Intellect• Mindfulness• Expert• Advocacy
Now• Compliance with evidence• Consistency/Uniformity• Honesty/Transparency• Understanding• Collaborator• Advocacy
Key Aspects of Culture
• Honest, Forthright, Transparent• Teamwork – about group not individuals• Shared Success – accountable to each other• Physician Leadership – Must be real and
committed • Change, uncertainty, vagueness, learning• Clinical and financial integration- physician
“owner/managers”

Being a Catalyst for Innovation
• Typically 90% of effort is on improving current operations• Need 80% of effort designing the future state- criterion,
outcomes, and performance based• Create internal structures and process that support
flexibility and rapid adaptability• Move from expert leadership to process leadership• Create the “future conversation”
Physician Leadership Effectiveness
Physician Leadership Effectiveness

Physician Leadership Skills
• Listening to diagnose vs. understand• Proactive in the setting of uncertainty and evolving
environment• Ethical centering
Collaborative Leadership Style
• Redefine success from narrow agendas to bigger goals• Involve others: move from autocratic to inclusive decision
making• Be accountable: move from blaming to taking
responsibility• Can be hard for us all, physicians and non-physicians
alike
“Collaboration” by Morten Hansen
Developing Physician Leaders
• Commitment, create authorized roles, support OJT• Create forums for conversation, shared learning, decision
making• Endless, tireless, repetitive conversations• Formal development programs- leadership, management,
finance/budgets, strategy, capital/program decisions• Dyadic model is effective• Continuous re-organizing to align work and operating
model
Not As Simple As …….
• Moving physicians to senior team• Seeking more input• Placing on governing boards• Employing and creating a physician group• Contracting networks• New vision in same old operating company
15
Must Be About …..
• Physicians having decisional authority and its accountability
• Physicians as “owner/operators” of the enterprise• Re-organizing the company to achieve this• Steadfastly focusing on the patients’ best interests as the
core of all decisions and expecting clinical leaders to make this happen
16
Physician Leadership Messages
• Believe in what you do• Be willing to fail• Enable others• Find great mentors
Track 4: Clinical Transformation
Panel 1: Clinical Leadership Characteristics Required for ACO Success
Mark Werner, MD Chief Clinical Integration Officer, Fairview HealthJustine M. Carr, MD Chief Medical Officer and Senior Vice President of Quality and Safety, Steward Health Care System, LLCKenneth C. Wilson, MD System Vice President, Clinical Effectiveness and Quality, Norton HealthcareRandall E. Williams, MD, FACC Chief Executive Officer, PHAROS InnovationsDon Caruso, MD, MPH Chief Medical Officer, Cheshire Medical Center/Dartmouth-Hitchcock Keene (Moderator)
Building Coordinated, PatientBuilding Coordinated, Patient‐‐CenteredCentered Care Management TeamsCare Management Teams
Jim Barr, MDCMO/VP Physician Network DevelopmentOptimus Healthcare Partners ACO
&VP of Medical ServicesAveta Health Solutions MSO
PatientPatient‐‐Centered Care Management TeamsCentered Care Management Teams Keynote AgendaKeynote Agenda
Optimus Healthcare Partners ACO Overview
Clinical Transformation • Structures• Processes
Care Management Teams• Engagement• Models• Tools & Resources
Summary & Questions
Optimus Healthcare Partners ACO OverviewOptimus Healthcare Partners ACO Overview
• Summit, New Jersey
• 550 Physicians
• Independent Physician Offices
• 180 PCP’s (120 FM/IM)
• Physician Governed‐Directed ACO
• Hospital Alignment/Support
• CMS MSSP ACO (30,000 members)
• Commercial ACO Arrangements
www.OptimusHealthcarePartners.com

Clinical Transformation Clinical Transformation
•
Why Change & WIIFM•
Team‐Based Office Workflows▫
Patient‐Centered Medical Home Model
▫
Resource: Population Care ManagersPopulation Care Managers
•
Population‐Based Care▫
Proactively Identify & Manage Patient Care Opportunities
▫
Tools: Aveta Patient Registry Aveta Patient Registry and and Patient Care PlansPatient Care Plans
•
Care Coordination & Communication▫
ACP PCMH‐Neighbor Model
▫
Tool: OptimusOptimus
PCPPCP‐‐Specialist Care Coordination GuideSpecialist Care Coordination Guide
▫
Tool: Aveta Health Information Exchange Aveta Health Information Exchange (HIE)(HIE)▫
Program: Optimus PatientOptimus Patient‐‐Centered Care Transitions ProgramCentered Care Transitions Program
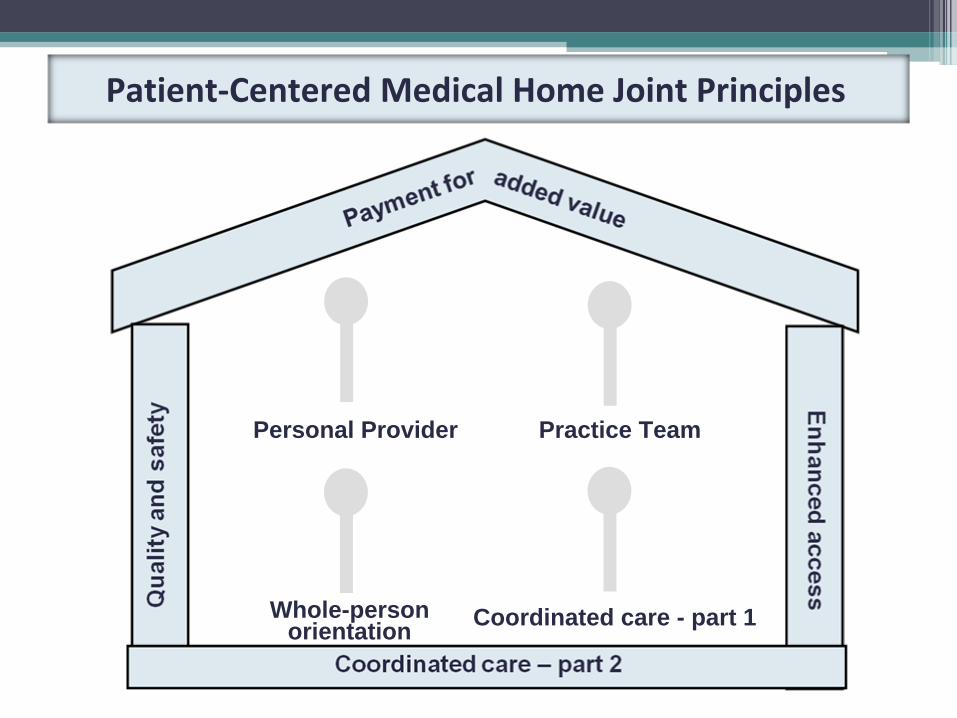
Patient‐Centered Medical Home Joint Principles
Personal Provider
Coordinated care - part 1
Practice Team
Whole-person orientation
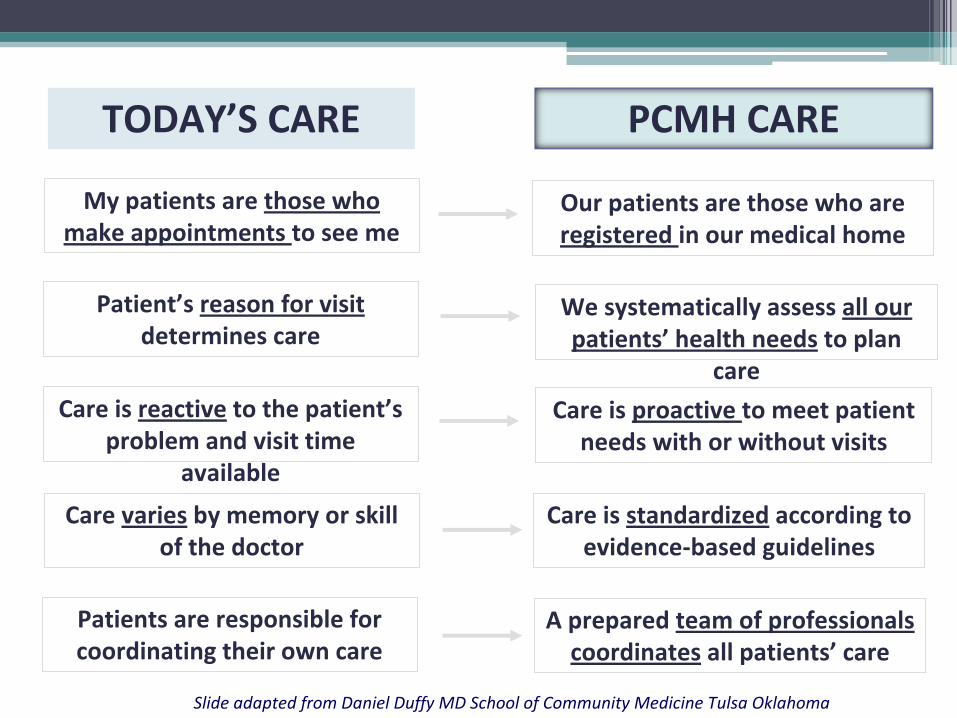
TODAY’S CARE PCMH CARE
My patients are those who
make appointments to see meOur patients are those who are
registered in our medical home
Patient’s reason for visit
determines careWe systematically assess all our
patients’
health needs
to plan
care
Care is reactive
to the patient’s
problem and visit time
available
Care is proactive to meet patient
needs with or without visits
Care varies
by memory or skill
of the doctorCare is standardized
according to
evidence‐based guidelines
Patients are responsible for
coordinating their own careA prepared team of professionals
coordinates
all patients’
care
Slide adapted from Daniel Duffy MD School of Community Medicine Tulsa Oklahoma
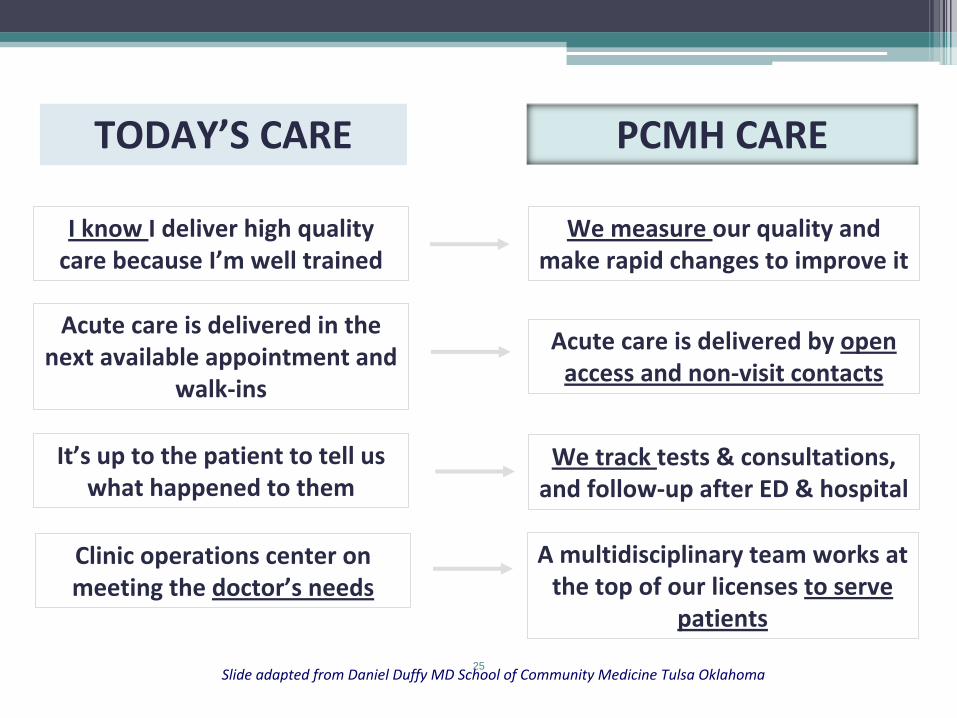
25
I know I deliver high quality
care because I’m well trainedWe measure our quality and
make rapid changes to improve it
It’s up to the patient to tell us
what happened to themWe track tests & consultations,
and follow‐up after ED & hospital
Clinic operations center on
meeting the doctor’s needsA multidisciplinary team works at
the top of our licenses to serve
patients
Acute care is delivered in the
next available appointment and
walk‐ins
Acute care is delivered by open
access and non‐visit contacts
TODAY’S CARE PCMH CARE
Slide adapted from Daniel Duffy MD School of Community Medicine Tulsa Oklahoma
““Preparing Your Team for Preparing Your Team for PerformancePerformance‐‐Based ContractsBased Contracts””
Practice RequirementsPractice Requirements
••
Provider ChampionProvider Champion••
Clinical CoordinatorClinical Coordinator
••
Potential Team MembersPotential Team Members••
OnOn‐‐sitesite
••
OffOff‐‐sitesite••
CommunicationsCommunications▫
Secure E‐Mail, Web‐Based Registry, HIE
▫
Webinars & Meetings
••
Office Project Management PlanOffice Project Management Plan
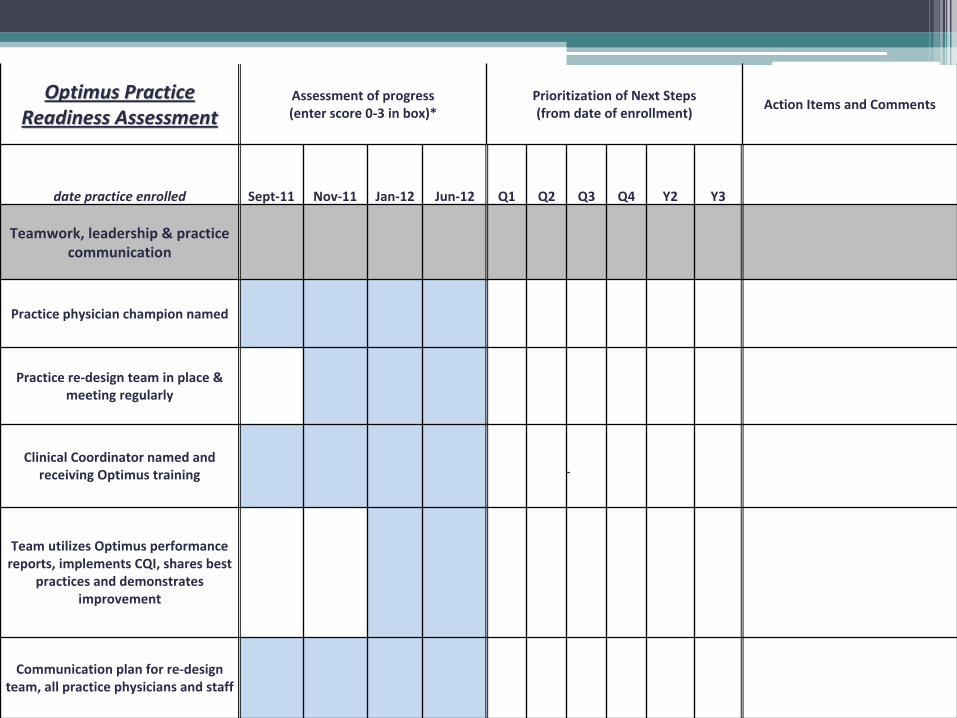
Optimus Practice Optimus Practice
Readiness AssessmentReadiness Assessment
Assessment of progress
(enter score 0‐3 in box)*Prioritization of Next Steps
(from date of enrollment)Action Items and Comments
date practice enrolled Sept‐11 Nov‐11 Jan‐12 Jun‐12 Q1 Q2 Q3 Q4 Y2 Y3
Teamwork, leadership & practice
communication
Practice physician champion named
Practice re‐design team in place &
meeting regularly
Clinical Coordinator named and
receiving Optimus training
Team utilizes Optimus performance
reports, implements CQI, shares best
practices and demonstrates
improvement
Communication plan for re‐design
team, all practice physicians and staff
Practice Readiness Assessment

Clinical CoordinatorsClinical Coordinators
•
Utilize the Patient Registry Patient Registry and HIEHIE
•
Develop goal‐directed patient care planscare plans
••
OutreachOutreach
to patients with gaps in care
•
Coordinate ER, hospital ER, hospital and
home care home care patients
••
CommunicateCommunicate
with office providers & staff
••
Communicate Communicate with other clinical coordinators
••
Coordinate Coordinate office participation in ACO clinical programs
TeamTeam‐‐Based Office WorkflowsBased Office Workflows••
Morning HuddleMorning Huddle▫
Schedule Review and Visit Preparation
▫
Care Plan Review
••
PrePre‐‐visit Activitiesvisit Activities▫
Automated orders
▫
Screenings and testing
••
VisitVisit
••
PostPost‐‐visit Activitiesvisit Activities▫
Barrier Analysis & Motivational Interviewing
▫
Patient Self‐Management (copy of Care Plans)
CareCare
Management TeamsManagement Teams••
Prioritize Based On:Prioritize Based On:
•
Potential Medical Cost Savings
•
Validated “Hard Savers”
•
Feasibility of Implementation & Timelines
•
Ability to Measure & Validate
••
Engagement Engagement
•
Business Case
•
Commitment & Participation•
Performance Management Framework
•
Transparency
Patient Access Patient Access
•
Office Visit Enhanced Access for ACO members •
Reserved Appointments
•
Open Access Scheduling•
Extension of Hours
•
Extended Hours•
Evenings
•
Weekends
•
After hours coverage with other offices•
Urgent care options
•
Communications

Care Coordination & CommunicationCare Coordination & Communication
••
PCPPCP‐‐Specialist Care Coordination GuideSpecialist Care Coordination Guide▫
Consultation Requests
▫
Hospitalizations▫
Co‐Management
••
Referral Guidelines and ManagementReferral Guidelines and Management
••
ACO PatientACO Patient‐‐Centered Care Transitions ProgramCentered Care Transitions Program▫
Emergency Room, Hospital, Sub‐Acute, Skilled
Nursing Facility (SNF), Long Term Care,Home Care
▫
Case Managers, Navigators, Vendors
Emergency Room ProcessesEmergency Room Processes•
Appropriate Utilization Education
•
ER Notification Process•
Sharing of Patient Information
•
Involving ACO Specialists•
ER Patient Follow‐Up•
Office processing of ER reports
•
Clinical coordinator role•
Patient medical record documentation
•
Patient care plan modification•
Coordinating and communicating next steps
Hospital CareHospital Care•
Notification of Admission Protocol•
Appropriate utilization
•
Alternative settings (observation beds/subacute)•
Case Managers & Utilization Managers•
Optimus ACO & Aveta
•
Health Plan•
Hospital
•
Prevention of Readmission•
Medication reconciliation
•
Post‐hospital visit coordination•
Home care, support

Imagine??Imagine??•
Patient Access & Communication
•
Office Workflows•
Planned visits
•
More time with patients•
Access to Information
•
Appropriate and Efficient Care Transitions•
Trusted Patient Relationships
•
Activated and Engaged Patients•
High‐Quality Affordable Healthcare
•
Physician and Staff Satisfaction
Summary & QuestionsSummary & QuestionsProvide Clarity & Build Culture
Provide Models, Tools & Resources
Performance Management Framework
Team Focus
Thank You,Jim Barr, MD
Optimus Healthcare Partners ACOAveta Health Solutions
Track 4: Clinical TransformationPanel 2: Building Coordinated, Patient‐Centered Care Management
Teams
James E. Barr, MD CMO and VP Physician Network Development, Optimus Healthcare Partners, VP of Medical Affairs, Aveta Health SolutionsNancy Boerner, MD, MBA CMO, Monarch HealthcareJames Dold, RN, BSN Director of Clinical Performance, New England Quality Care Alliance Susan Kendig, JD, MSN Principal, Health Policy Advantage, LLC; Outside Counsel, Missouri Center for Patient SafetyNeil Calman, MD President and CEO, The Institute for Family Health, Inc., Clinical Professor of Family and Social Medicine, Albert Einstein College of

The Engelberg Center for Health Care Reform at Brookings | The Dartmouth Institute
June 6–8, 2012
Third Annual National ACO Summit
Follow us on Twitter at @ACO_LN
and use #ACOsummit.