The Emerging Role of Physicians in Disease Management Programs
43
The Emerging Role of Physicians in Disease Management Programs David Sobel, MD, JD Rushika Fernandopulle, MD, MPP Emmi Solutions, LLC Renaissance Health Chicago, IL Cambridge, MA
description
The Emerging Role of Physicians in Disease Management Programs David Sobel, MD, JDRushika Fernandopulle, MD, MPP Emmi Solutions, LLCRenaissance Health Chicago, ILCambridge, MA. Who am I?. Recovering Attorney: University of Michigan Law School (1992) - PowerPoint PPT Presentation
Transcript of The Emerging Role of Physicians in Disease Management Programs

The Emerging Role of Physicians in Disease Management Programs
David Sobel, MD, JD Rushika Fernandopulle, MD, MPPEmmi Solutions, LLC Renaissance HealthChicago, IL Cambridge, MA

Who am I?
Recovering Attorney:- University of Michigan Law School (1992)- Paul, Weiss, Rifkind, Wharton & Garrison (1992-96)
Urological Surgeon:- University of Illinois Medical School (2000)- Rush University Medical Center (2000-2005)
Chief Medical Officer & founder of Emmi Solutions, LLC

Historical Context
“Life is short, the Art long, Opportunity fleeting, Experiment treacherous, Judgment difficult. The physician must be ready, not only to do his duty himself, but also to secure the co-operation of the patient, of the attendants and of externals.” [emphasis added]
-Hippocrates

Historical Context
Only section of the Hippocratic Corpus that addresses doctor-patient communication:
-“[p]erform [your duties] calmly and adroitly, concealing most things from the patient while you are attending to him. Give necessary orders with cheerfulness and serenity, turning his attention away from what is being done to him; sometimes reprove sharply and emphatically, and sometimes comfort with solicitude and attention, revealing nothing of the patient’s future or present condition.” [emphasis added]

“In our country, patients are the most under-utilized resource, and they have the most at stake. They want to be involved and they can be involved. Their participation will lead to better medical outcomes at lower costs with dramatically higher patient /customer satisfaction.”
Charles Safran, M.D.President, American Medical Informatics Association
From his Testimony Before the Subcommittee on Healthof the House Committee on Ways and Means
New Paradigm

Evolution
Disease Management
Care Management
Population Management

New Paradigm
Medical Home Model:- Ongoing relationship between a provider and patient
- Around the clock access
- Respect for the patient/family’s cultural and religious beliefs
- Comprehensive approach to care
- Coordination of care through providers and community services
- AAMC

American College of Physicians’ Definition
Best quality care is provided through:- Patient-centered, physician guided
- Cost-efficient and longitudinal
- Encompasses and values the art and science of medicine
Attributes of Medical Home include:- Promotion of a continuous healing relationship
- Through delivery of care in a variety of care settings
- According to the needs of the patient and skills of the medical provider

Consistent Themes
Patient Centric “Wellness”
Physician Driven Enhanced Access

Even Better
Engaged Patients Leveraged Physicians

Redefining the Physician’s Role
Doctor walks into a bar . . .-Pain-Misery-Suffering YOU
TOO

Wednesday May 14, 2008
18 Patients in the AM:- 8:30 -10:00- 8:30 -10:10- 8:40 -10:20- 8:50 -10:20- 9:00 -10:30- 9:10 -10:40- 9:20 -11:00- 9:30 -11:15- 9:40- 9:50
21 Patients in PM- 1:00 -2:30 -4:00- 1:10 -2:40- 1:20 -2:50- 1:30 -3:00- 1:40 -3:10- 1:50 -3:20- 1:50 -3:20- 2:00 -3:30- 2:10 -3:40- 2:20 -3:50

How to spot a physician?

Can you spot the caregiver? Which one manages disease?

Redefining the Physician’s Role
CV:- AOA graduate from Emory University
Medical School- Internal Medicine Resident – voted best
resident by peers- Invited for Chief Residency position
How he described his patients:- “20 semi-strangers who do nothing but
complain.”
How he described his day:- “It’s like suffering through Thanksgiving
everyday of the week.”

Redefining the Physician’s Role
Medical Home Model demands that the physician be:
- All knowing This requires technology to assemble virtual teams of people and resources as needed based on patient needs
- Always present This requires technology such as IVR, web coaching, and web visits to automate routine communications
- Service with a smile This requires training and technology to help physicians communicate with empathy and clarity

Conversation is the Key
Communication isn’t a message sent; it’s a message received- We need to be better listeners
People don’t always say what they mean- We need to actively listen
- Position: demand or assertion often expressed with strong feeling
- Interest: the underlying concern that generated the position
Communication isn’t always verbal

The Power of Conversation
12 Angry Patients:- No one is a doctor
- Everyone is a patient
- “I know how to talk to patients”

Can you catch cancer? Can you catch cancer?


EXTEND The Conversation

Low Tech
“We are sorry! We always try to meet your scheduled appointment time. Sometimes we run late and we apologize. A patient’s visit sometimes takes longer than we anticipate. Sometimes that patient is you.”
James W. Saxton, Esq., The Satisfied Patient, 2003

Leverage Technology
Literature review of computer-based patient education (1970-2001):
- Majority of studies showed significant gains in knowledge acquisition- Also:
• Increased prevalence of self-care behaviors• Improved health outlook• Increased adherence to health management regimens• Increased patient satisfaction• Positively impacted several different clinical outcome measures.
• Lewis, D. Computers in Patient Education. Comput, Informat, Nurs 2003

“The Disease of Familiarity”
Interactive computer programs were as effective or even more effective than instruction provided by staff educators
Krishna, Santosh, Balas, E. Andrew, Francisco, Benjamin D., Konig, Peter, Graff, Gavin R., Madsen, Richard W., Internet-Enabled Interactive Multimedia Asthma Education Program: A Randomized Trial. Pediatrics, 00314005, Mar2003
Green, MJ, et al, Effect of Computer-based Decision Aid on Knowledge, Perceptions, and Intentions about Genetic Testing for Breast Cancer Susceptibility. J Am Med, 2004
Jenny, NYY, et al, Evaluating the Effectiveness of an Interactive Multimedia Computer-based Patient Education Program in Cardiac Rehabilitation. Occup Ther J Res, 2001
Jones, RB, et al. Randomized Trial of Personalized Computer-based Education for Patients with Schizophrenia. Br Med J, 2001
Martin, JT, et al. NPs vs. IT for Effective Colposcopy Patient Education. Nurse Pract Am J Prim Health Care, 2005
Miller, DP, et al. Using a Computer to Teach Patients about Fecal Occult Blood Screening – A Randomized Trial. J Gen Intern Med, 2005
Evans, AE, et al, Computer-assisted Instruction: An Effective Instructional Method for HIV Prevention Education?, J Adolesc Health, 2000

Best Practices
VisualsCreating programs that rely on simple graphics and animation to illustrate key concepts makes the program
easier to follow for most people, but is critical for those patients with diminished reading skills. (1)
EmpathyStudies have found that consumers “seemed more willing to confide in computers than in human interviewers, possibly because the computers were perceived as nonjudgmental or evoked less embarrassment on sensitive
subjects.” (2)
Plain LanguageNearly half of all American adults have difficulty understanding and using health information Higher rate of hospitalization and emergency services when patient’s have limited health literacy. (3)
1) Sechrest, R.C. & D.J. Henry. Computer-based patient education: observations on effective communication in the clinical setting
2) Mantone, Joseph. (August 8, 2005). Reading, writing and relating. Modern Healthcare.
3) Health Literacy: A Prescription to End Confusion, IOM April 2004

Best Practices
Visuals - show it, don’t say it.
Empathy - say it, don’t write it.
Plain Language - write it. But, write it well.

Unlike people with type 1 diabetes, people with type 2 diabetes produce insulin; however, the insulin their pancreas secretes is either not enough or the body is unable to recognize the insulin and use it properly. This is called insulin-resistance. When there isn't enough insulin or the insulin is not used as it should be, glucose (sugar) can't get into the body's cells. When glucose builds up in the blood instead of going into cells, the body's cells are not able to function properly. Other problems associated with the buildup of glucose in the blood include: Dehydration. The buildup of sugar in the blood can cause an increase in urination (to try to clear the sugar from the body). When the kidneys lose the glucose through the urine, a large amount of water is also lost, causing dehydration. Diabetic Coma (Hyperosmolar nonketotic diabetic coma). When a person with type 2 diabetes becomes severely dehydrated and is not able to drink enough fluids to make up for the fluid losses, they may develop this life-threatening complication. Damage to the body. Over time, the high glucose levels in the blood may damage the nerves and small blood vessels of the eyes, kidneys, and heart and predispose a person to atherosclerosis (hardening) of the large arteries that can cause heart attack and stroke. Anyone can get type 2 diabetes. However, those at highest risk for the disease are those who are obese or overweight, women who have had gestational diabetes, people with family members who have type 2 diabetes and people who have metabolic syndrome (a cluster of problems that include high cholesterol, high triglycerides, low good 'HDL' cholesterol and a high bad 'LDL' cholesterol and high blood pressure). In addition, older people are more susceptible to developing the disease since aging makes the body less tolerant of sugars. Although it is more common than type 1 diabetes, the causes of type 2 diabetes are less well understood. It is likely caused by multiple



When “Prescribed” by a Physician
• 89% watched program from start to finish• 87% of patients experienced increased confidence
in their doctor• 96% of patients reported improved understanding
– No $ incentives– No free iPods– No rewards or threats

Rushika Fernandopulle, M.D., M.P.P.
Renaissance Health
Cambridge, MA, USA
May, 2008
Putting the Physician Back into Disease
Management

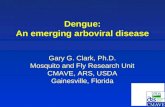
Start with the Sickest Patients
Source: Large West-coast self-insured employer PPO data, 2005. n=147K
Healthy- 50-100%ile- 5% costs
Acute illnesses- 20-50%ile- 15% costs
Complex- 0-10%ile- 65% costs
Simple Chronic- 10-20%ile- 15% costs
The most leveraged target for redesign are what we call Complex patients- those with multiple chronic conditions who end up costing up to 2/3 of all health care dollars, and are poorest served by the current system.
Average spending for percentile groups
$-
$20,000
$40,000
$60,000
$80,000
$100,000
$120,000
0% 20% 40% 60% 80% 100% 120%

A new model from the ground-up
New Principles
•Meet the needs of our patients and focus on experience
•We cannot manage our patients’ health; they must, and we can provide tools and resources
•Continually innovate and improve
New Processes
•Jointly created strategic health plans
•In depth education and coaching from RN/CHWs
•Unfettered access to help
•Proactive management
•Remote monitoring
•Integrated mental health
•Specialists as consultants
New Structures
•Different staffing and true team care
•Robust Information Technology Platform
•Physical Design
•Business model
•Culture
The RenHealth Complex Care ModelRe-imagining the entire care system for complex patients

Early Pilots of the Model (and Variants)
Part of a larger movement
•AAFP- Transfor-med (36 sites)
•ACP- Patient Centered Medical Home
•IMP- Ideal Micro Practices
•CMS- Case Management for high cost Beneficiaries Demonstration
Legacy Sites- Active before 2006
Sites in Implementation Phase
Sites in Planning Phase

Variant 1: Working with existing Medical Groups
• Boeing is a leading aerospace company headquartered in Chicago, but with >150K employees in 70 countries
• Annual revenue 2006 US$61.5 billion• Self insured, large, stable, geographically concentrated
workforce; >US$2b in medical costs• High and rising health costs put them at a competitive
disadvantage with their major competitor (Airbus)

• Focus on Puget Sound, WA market • Two major plants to assemble commercial
airliners, may other sites; total of >150K lives• Partnering with three well respected,
progressive providers to build A-ICU model for 700 predicted high cost employees and dependents

Linking payment change with clinical redesign
• Patients selected through predictive modeling, invited by their doctors to participate
• Provide RN Health coaches to work within medical groups to help manage patients
• Practice are staffed by high performing MD, RN “health coach”, other help• Shared care plan, access, proactive care all implemented• No benefit changes, so sites continue to bill Fee-for-service for MD visits• Sites get paid a case rate pmpm (roughly 2.5% of total spending) to cover
non-traditional services• In subsequent years will consider sharing savings with sites

Variant 2: “Workplace” Clinic for Complex Patients
Atlantic City, NJ
• HEREIU Fund- Large multi-employee trust fund for service workers- hotel, restaurant and casino
• Focus on Atlantic City, NJ with approx 25K lives• Partner with a large not-for-profit integrated
delivery system (IDS)- Atlanticare to build a new clinic for predicted high cost employees and dependents
• Patients are given incentives (through waived copayments for visits and pharmaceuticals) to seek care at the Special Care Center
• Globally budgeted, costs shared by Fund and Health System

A redesigned care space, team, and system

Anecdotally Making a difference
• “I look forward to seeing IOCP patients on my schedule. I can see what’s happening with patients whom I have generally struggled with for years. The light bulbs are turning on, they are engaged and motivated.”
• “Patients respond positively to their relationship with their care manager. It’s like the whole tenor of the visit is changing from one of resignation that nothing is likely to change, to one of improved results, optimism, and hope.”
• “I have been helped more in the last six months than years of seeing multiple doctors.”
• “Being a patient in the IOCP has been a life-changing event for me. I have learned to change the way I live and think. I finally stopped smoking. Somebody actually listens to me and is giving me the help I need.”
• “My BP is now normal after being high for many years. I am getting good advice about my prescriptions. I am able to take walks and hope to be swimming again soon. I am feeling positive now, I once felt doomed. I feel like a new person.”
Physician Feedback Patient Feedback

Goals tracked across multiple vectors
Health Costs
Reduce net total health care spending trend for
target population vs. control group in 1-2
yearsFunctional status
Improve self reported functional scores (SF-12)
and improve productivity in the
workplace
Patient Experience
Improve patient’s experience of care
across all dimensions in a standard survey (ACES/CG-CAHPS)
Quality
Improve performance on chronic disease
measures, both claims based and ones based
on clinical data
Staff SatisfactionCreate an excellent work
environment for physicians and staff

Advantages Over Traditional DM
• Much higher engagement rates• Able to manage with clinical as well as claims data• In person relationship and transference from MD
helps with behavior change• Effector arm to change care if needed• Spillover effects of collaboration between payer and
provider

Renaissance HealthOne Broadway, 14th floorCambridge, MA 02142P: 617.682.3669F: 617.475.6027W :www.renhealth.netE: [email protected]
“Insanity is doing the same thing over and over and expecting different results”
-Albert Einstein