The emergence of e-patients: Role of internet and social ...
17
The emergence of e-patients: Role of internet and social media in Participatory Medicine BY MEGHANA NITHIN HEGDEKAR GRADE AWARDED: PASS WITH DISTINCTION Research Paper based on lectures at the Medlink or Workshop Conferences at Nottingham University in December 2013 April 2014
Transcript of The emergence of e-patients: Role of internet and social ...

The emergence of e-patients:
Role of internet and social media in Participatory Medicine
BY
MEGHANA NITHIN HEGDEKAR
GRADE AWARDED: PASS WITH DISTINCTION
Research Paper based on lectures at the
Medlink or Workshop Conferences
at Nottingham University
in December 2013
April 2014

2
Abstract:
E-patients are health consumers, who are enabled, empowered, engaged and participate fully in shared decision-making regarding their medical care and take personal responsibility for self-managing their illness. In Participatory Medicine (PM) patients are empowered by available information, and take a more active and responsible role, while clinicians welcome them as knowledgeable partners in clinical practice; thus forming a doctor-patient team. Advances in Information and Communications Technology (ICT) and the enthusiasm of the e-patients, to be involved in their medical care, are playing a major role in transforming and changing the shape of healthcare. This has the potential to become a new level of 21st century healthcare. This paper discusses the benefits and challenges of PM. In particular it focuses on the role of patients, physicians and other policy makers in embracing this sea change; including ethics and the future of internet and social media (SM) in PM.
Introduction:
Participatory movement:
Dr. Tom Ferguson, a physician, coined the term ‘e-patients ‘and was a champion of e-patients. One of the first white papers[1] about e-patients was started by him but was published after his untimely death from multiple myeloma in 2007. He urged patients to educate themselves, share knowledge with one another and to use the Internet as a powerful tool to help take the reins of their own health care. He urged doctors to collaborate with patients rather than command them.
In order to initiate real changes in medicine and healthcare e-patients realised they had to form movements. The authors of the white paper grouped together on E-patients.net[2] and launched a blog. They then founded the Society for Participatory Medicine (SPM) and launched the Journal of Participatory Medicine[3], thus forming the Participatory movement (textbook)
SPM defines PM as a movement in which networked patients shift from being mere passengers to responsible drivers of their health, and in which medical care providers encourage and value them as full partners[4].
Although patients are central to healthcare delivery, often their perspectives and input have not been taken into consideration by providers. But this is changing rapidly and patients are becoming more engaged, with the emergence of patient-centred care to improve quality of care. At the same time, social media in particular and the internet more broadly are widely recognised as having produced huge effects across societies. Thus the three domains—patient-centred healthcare, SM and the internet—are beginning to come together, with powerful and unpredictable consequences in healthcare, with a potential to create a ‘perfect storm’, a phrase that has been used to describe a situation in which a rare combination of circumstances aggravate a situation drastically to result in an event of unusual magnitude[5].
The power of e-patients
E-patient Dave deBronkart, volunteer co-chair of the SPM beat a near fatal cancer, supplementing his great medical care by using internet in every possible way. He is an advocate for patients being empowered and engaged in their health care. In his

3
talk on Ted Maastricht[6], Dave talks about how he found the resources to help fight cancer, the importance of accessing respected medical websites for quality information and also the importance of patient networks. He also talks about how the patient is the most under-used resource in healthcare and ends saying, ‘let patients’ help’ to help healthcare.
Jack Andraka, a 15year old, started researching about pancreatic cancer when he lost
someone close, to the disease. Using internet as one of the sources of information, he
went on to develop a promising early detection test for pancreatic cancer that is super
cheap, effective and non-invasive[7]. This proves that although patients can contribute, they
are an underused source of information in healthcare.
E-patients are more likely than other internet users to engage in SM in general (fig 1). E-patients gather information about medical conditions that impact them and their families, using electronic communication tools (including Web 2.0 tools) in coping with medical conditions (fig 2).
Fig 1
Fig 2

4
E- patients are different to ‘googlers’,(fig 3) who come up with web searches without
strategy and want to be treated as per their search results thus frustrating their doctors and
themselves[8].
Features Googlers E-patients
Use digital technology in their
health management
Yes Yes
use the internet with strategy No Yes
Can deal with the huge amount
of on-line information
No Yes
Relationship with their doctor Frustrating Equal Partners
Use of internet
During the last decade, the Internet has become increasingly popular and now forms an
important part of our daily life. For many citizens of most developed countries, the internet
has become a powerful and familiar healthcare tool(fig 4)
Half of American adults have
searched online for health
information[9]
(fig 5)
Fig 3
Fig 4
5
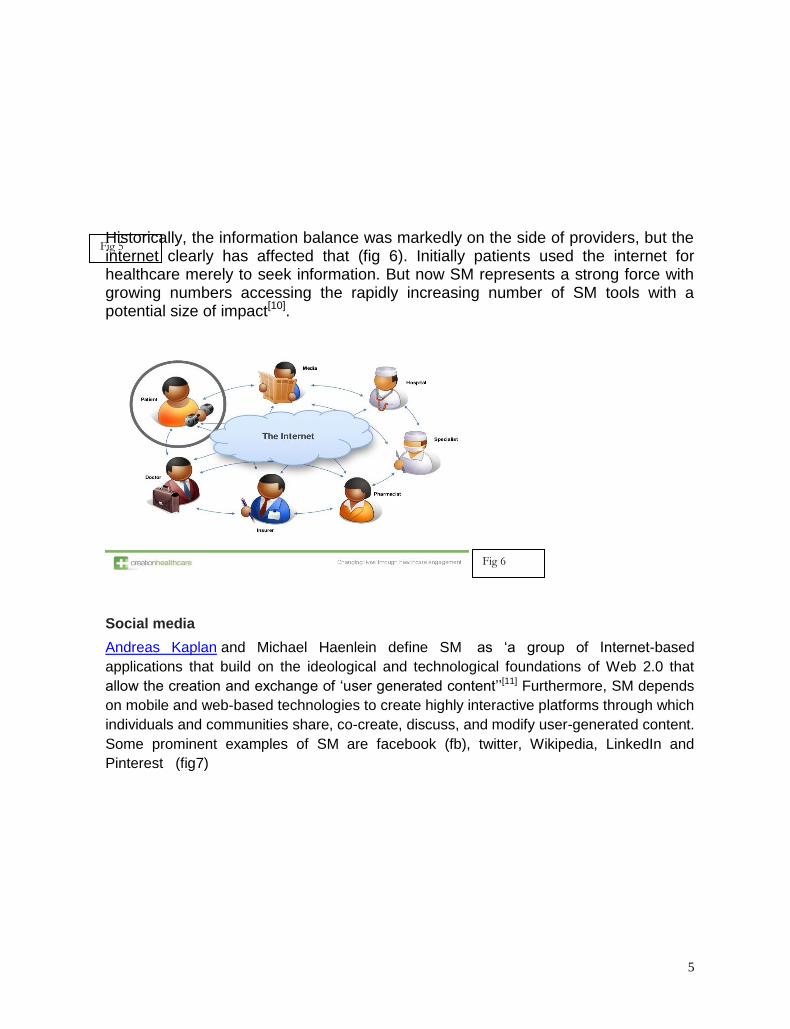
Historically, the information balance was markedly on the side of providers, but the internet clearly has affected that (fig 6). Initially patients used the internet for healthcare merely to seek information. But now SM represents a strong force with growing numbers accessing the rapidly increasing number of SM tools with a potential size of impact[10].
Social media
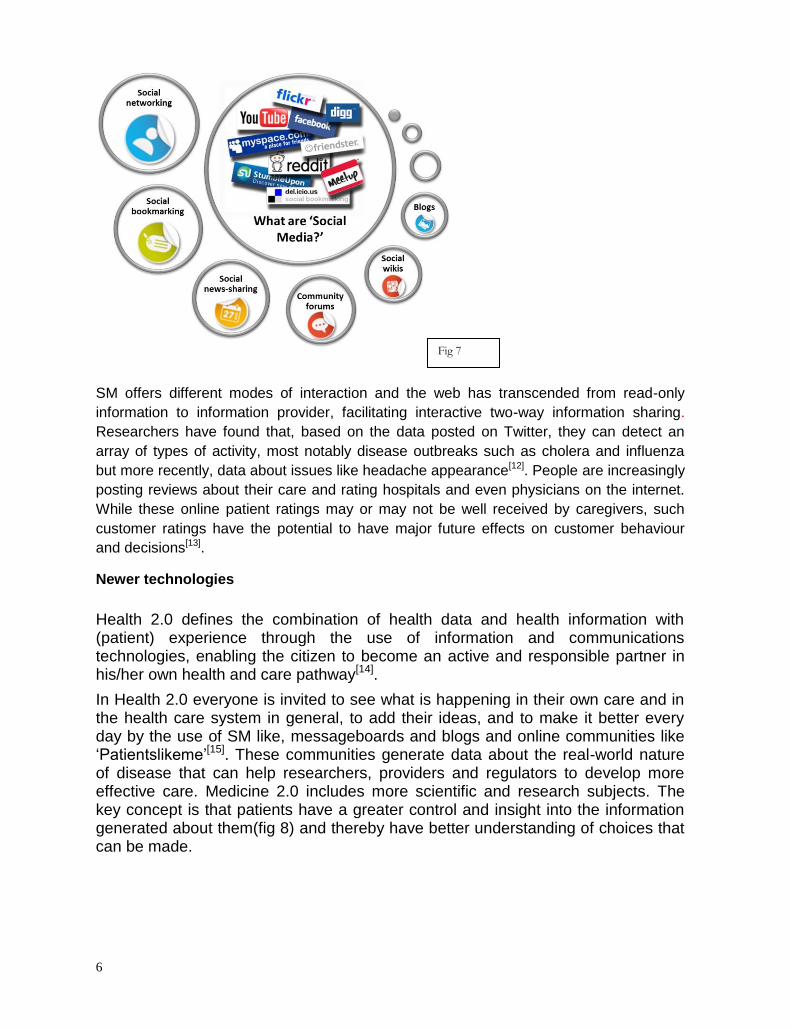
Andreas Kaplan and Michael Haenlein define SM as ‘a group of Internet-based
applications that build on the ideological and technological foundations of Web 2.0 that
allow the creation and exchange of ‘user generated content’’[11] Furthermore, SM depends
on mobile and web-based technologies to create highly interactive platforms through which
individuals and communities share, co-create, discuss, and modify user-generated content.
Some prominent examples of SM are facebook (fb), twitter, Wikipedia, LinkedIn and
Pinterest (fig7)
Fig 5
Fig 6
6
SM offers different modes of interaction and the web has transcended from read-only
information to information provider, facilitating interactive two-way information sharing.
Researchers have found that, based on the data posted on Twitter, they can detect an
array of types of activity, most notably disease outbreaks such as cholera and influenza
but more recently, data about issues like headache appearance[12]. People are increasingly
posting reviews about their care and rating hospitals and even physicians on the internet.
While these online patient ratings may or may not be well received by caregivers, such
customer ratings have the potential to have major future effects on customer behaviour
and decisions[13].
Newer technologies
Health 2.0 defines the combination of health data and health information with (patient) experience through the use of information and communications technologies, enabling the citizen to become an active and responsible partner in his/her own health and care pathway[14].
In Health 2.0 everyone is invited to see what is happening in their own care and in the health care system in general, to add their ideas, and to make it better every day by the use of SM like, messageboards and blogs and online communities like ‘Patientslikeme’[15]. These communities generate data about the real-world nature of disease that can help researchers, providers and regulators to develop more effective care. Medicine 2.0 includes more scientific and research subjects. The key concept is that patients have a greater control and insight into the information generated about them(fig 8) and thereby have better understanding of choices that can be made.
Fig 7

7
The Human Genome Project[16] and e-Health are two fundamental changes that will alter the way we approach human health and life. These two scientific and societal forces will inevitably impact each other. Knowledge regarding genomic variations within the population will enable health promotion messages based on their genomic risk profile, something patients can access or manage as e-patients. Telehealth means the provision of health services at a distance using a range of technologies, such as telephone or video consultation to support diagnosis. Telecare provides physicians an easier way to continue monitoring and engaging with chronic care patients and those with minor health concerns, faster and typically while still at home; thus reducing cost of care. Examples like, monitoring blood pressure and blood sugar at home will reduce visits made to the doctors.
Telemedicine is a rapidly developing application of clinical medicine where medical information is transferred through the phone, Internet or other networks for the purpose of consulting. Telemedicine may be as simple as two health professionals discussing a case over the telephone, or as complex as using satellite technology and video-conferencing equipment to conduct a real-time consultation between medical specialists in two different countries. It is most beneficial for populations living in isolated communities and remote regions. Some examples of telemedicine are transmitting x-rays(fig9) or ECGs for a professional opinion.
Fig 8

8
Mobile Health covers medical and public health practice supported by mobile devices, such as mobile phones, patient monitoring devices, personal digital assistants (PDAs), and other wireless devices[17].
Virtual reality therapy (VRT) or computerised CBT, is a method of psychotherapy that uses simulated experience to treat patients with anxiety disorders and phobias where it has proven very effective[18].
Virtual world[19] is a computer-based simulated environment where users take the form of avatars visible to others. These avatars can meet, share materials and talk and allow for multiple users. One of the most popular virtual realms is Secondlife.com, there are others like Visuland.com. Doctors and students use the platform for giving presentations, presenting cases and the Ann Myers medical centre provides educational simulations. Patients have the health information island with links to support groups and educational materials. Virtual world provides the solution for collaboration when geographical limitations arise.
Discussion
E-patients are driving a healthcare revolution of major proportions; they are the hunters and gatherers of medical information (white paper). With the rise of PM, we are in the midst of one of the most rapid and profound shifts in the history of medicine. As participatory movement gathers speed, patients shift from being mere passengers to responsible drivers of their health, and in which providers encourage and value them as full partners[20].
Although there are tremendous opportunities arising from this exciting movement for the future, equally there are challenges including adapting to the changes and ethical issues of PM.
Benefits
Fig 9
9
E-patients who are well informed of their medical condition are more likely to comply with their provider’s recommended regimen. They are also better able to communicate important health information to their providers, which can assist providers with their diagnosis and care plans. Along with improved health outcomes, active involvement of patients and families can lower underuse or overuse of medical services and reduce health care costs[21]. Educational materials help e-patients to make treatment decisions when faced with multiple treatment options. PM will be proactive with a focus on the individual patient to optimise wellness. We will know the individual patient in depth by creating personalised data clouds and be able to sort out the relative contributions to disease of one’s genome and their environmental exposures. There is a mutual respect that grows between patients and provider with continuity of care and fast access including out of hours.
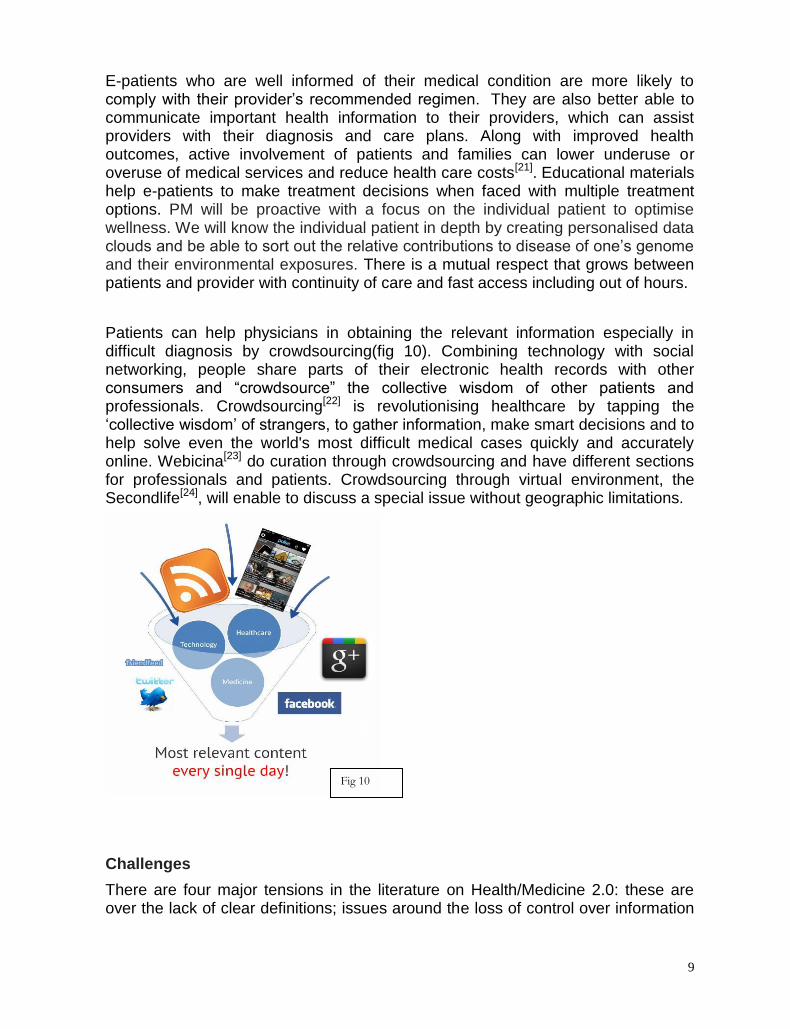
Patients can help physicians in obtaining the relevant information especially in difficult diagnosis by crowdsourcing(fig 10). Combining technology with social networking, people share parts of their electronic health records with other consumers and “crowdsource” the collective wisdom of other patients and professionals. Crowdsourcing[22] is revolutionising healthcare by tapping the ‘collective wisdom’ of strangers, to gather information, make smart decisions and to help solve even the world's most difficult medical cases quickly and accurately online. Webicina[23] do curation through crowdsourcing and have different sections for professionals and patients. Crowdsourcing through virtual environment, the Secondlife[24], will enable to discuss a special issue without geographic limitations.
Challenges
There are four major tensions in the literature on Health/Medicine 2.0: these are over the lack of clear definitions; issues around the loss of control over information
Fig 10
10
that doctors perceive; safety and the dangers of inaccurate information; and issues of ownership and privacy[25]. Changes in healthcare are inevitable but the concept of PM has yet to be fully recognised by many clinicians and the public. They remain unaware or unconvinced that their own behaviour must change if patients are to realise the benefit of care.
This model needs a huge culture shift for the evolution to begin which may take time to occur; health literacy is an enormous barrier. Patients will have to assume a great deal of responsibility in order for this model to work. There will be a significant hurdle depending on the patient’s education level, level of assertiveness and resourcefulness and more importantly on the individual’s medical issues. There are gaps in social class making their true sharing of decision making very uneven. It is not just the physician and patients who need training but also other multidisciplinary staff involved in the care of the patient. Patients must be educated and conscientious to bring the information that is needed when it is needed, without which there will be no partnership in PM. In managing chronic disease, or just maintaining good health, PM would be ideal but when faced with a serious diagnosis or when events cascade, a patient may not be equipped to participate on the principles of this model for a while.
There are obvious fears about digital communication including the fear of learning a new
skill. Government should take the responsibility of regulating; paying for and controlling all
on-line health control as otherwise it may become an unregulated model with no clear
guidelines. The quality of information on the Internet is paramount: accurate relevant
information is beneficial, while inaccurate information is harmful. There is concern over
the quality of user generated content leading to misinformation. There are
limitations for medical doctors to use Google as a diagnostic tool and on the other
hand, patients may delay seeking medical help following internet
searches. Consumers must possess the skills to crowdsource to avoid information
overload.
Changing attitudes of physicians, patients and policy makers
Physicians
Reforming health care must involve engaging and activating patients and providers to
become participatory partners, by encouraging patients to use on-line resources while
physicians help guide and promote discussion. To succeed, there must be open, on-line
patient-provider communication and information exchange. For this to happen, both
physicians and patients will have to adapt to the change and keep up to date with
technology.
In the new model of care, physicians will no longer do things “to” patients; they will do things “with” patients as partners; not ordering the patient but advising them[26]. Since the advent of the Internet, many clinicians have underestimated the benefits and overestimated the risks of online health resources for patients[27]. A minority of physicians feels challenged by patients bringing health information to the visit; reasons for this require further research[28]. A partnership will evolve in which

11
physicians would facilitate a patient's recovery rather than prescribe it which puts doctors in a difficult situation in which they must now incorporate persuasive techniques to convince patients that they offer the best counsel. There must be a multidisciplinary approach to care and may include, pharmacists, nutritionists, and other professional providers. Payment to providers will not be based just on visits to doctors but incentives will be given to communicate in other ways including phone, email, text messages and SM. Physicians in order to practice safely in the changed environment will have to follow strict guidelines.
Patients
For PM to gain a major foothold, patients will receive guidance as well as tools, information, and data that allow them to be active participants in their care and work effectively with their providers to determine the care they receive. In addition to engaging in online research about their health and their medical conditions, patients will network with online communities to discover which treatments, providers, and facilities work best to address their condition. Patients will be able to participate in group visits to gain a greater understanding of their illnesses and to provide stimulating interaction with the provider team and patients with similar conditions.
As providers increasingly adopt electronic communication options (email, web-based secure messaging, videoconferencing, mobile phone conversations, text messaging, and instant messaging), clinical care will shift to a “care anywhere” model. Visit to doctor will become much less important and less frequent, like for procedures or hands-on-examination; where possible, routine cases will be conducted on-line. Patients and providers will increasingly adopt the notion that followup and repeated communication is the norm and that it serves as the best means of achieving optimum outcomes, avoiding diagnostic errors, and obtaining high quality health care at the lowest price.
Policy makers
There must be a responsible body, like the Government, taking responsibility to provide
guidelines and regulate health care on-line. This will require a new business model. It will
only be effective if there are effective financial incentives for patients and providers.
There are concerns of child protection and anti-pornography including quackery and e-pharmacies, which often use SM for direct to consumer advertising. Equally important are questions of identity theft, misrepresentation of identity (e.g., someone falsely claiming to be a medical doctor), and the validity of information that is provided within and through SM. There is the issue of malpractice, whether a health care provider, layman, or digital platform should be held liable for health-related recommendations provided through SM. Public health systems are facing shrinking budgets and increased demand and in times of austerity, ICT can be our most powerful ally to maintain cost efficient and high quality care. The European Union and the United States joined forces on a Transatlantic Cooperation[29] (fig 11), to enhance health-related information and communication technology, called eHealth in Europe and health IT in the US respectively.
12
On-line groups and doctors complement each other. Although there is a considerable amount of research still needed, once developed, this approach should reduce treatment costs and improve patient experience.
Ethics of eHealth
The potential violation of ethical standards, patient privacy, confidentiality, and professional codes of practice, along with the misrepresentation of information and how clinicians may protect themselves during Internet-based interactions are the most common contributors to individual and institutional fear against the use of SM in medicine and health care.
There is an issue of maintaining autonomy over the very sensitive information that is fed onto the websites. There is a lack of understanding of the true risks and liabilities that could result.
If clinicians ignore patient requests sent through SM, one could argue that, by not responding to these requests, clinicians are committing an Act of Omission, as there would be implied consent to respond through the medium given that the patient started the dialogue on SM[30]. Professionals must abide by the ethical codes that govern their professions as practitioners in face-to-face relationships
Numbers of privacy and confidentiality violations committed by physicians who use SM are small[31] Nevertheless, even if violations seldom occur, HCP should always protect patient privacy and confidentiality and do no harm as it is the ethos of the medical profession.
Possibly, those with higher incomes have other means of support, while those with lower
incomes are turning to the Internet for assistance, which may put them at risk if they do not
get needed assessments and treatment[32]; pointing to the ethical issue of justice
Future research will be required to understand the synergies between SM and evidence-based practice, as well as develop institutional policies that benefit patients, clinicians, public health practitioners, and industry alike[33].
Fig 11

13
The landscape of PM is rapidly changing (fig 12) but there are still a huge number of open, web savvy patients than there are physicians who are neither active nor open. In order to close that gap, it is important to educate patients and doctors to get access to the best available SM resources, curate manually with collaboration with patients and professionals around the world. Also to include digital literacy in the medical curriculum to meet the special needs of these patients.
Fig 12
Fig 13

14
The work of the Human Genome Project has allowed researchers to begin to understand the blueprint for building a person. As researchers learn more about the functions of genes and proteins, this knowledge will have a major impact in the fields of medicine, biotechnology, and the life sciences[34]. Combined with the tech savvy patients, it will cause a major change in the way medical healthcare is delivered in the future (fig 13). Patients will be in contact with doctors over web or mobile devices, frequently, prior to their visit and be aware of their records by accessing the EPR, will be preparing questions before-hand, having consulted their communities on-line and using the personalised apps. When they see their doctor face-to-face, it will be more productive and a satisfying experience which they can write a post on their blog to help other e-patients. .
Eric Topol[1] talks about the ‘creative destruction of medicine’, with the super convergence of all the latest technology to give rise to a new form of healthcare(fig14).
Conclusion This paper believes that the exponential and relentless rise in healthcare costs has to be reigned but we have still not taken advantage of innovation involving digital information in medicine. But the inevitable change will happen in the near future with the consumer not just engaging in the change but actually catalysing the change. This change will have profound implications for patient and provider interaction with a fundamental shift in the dynamic between physicians and patients. This new paradigm of care will be much less costly, more patient-centred, more convenient, and will lower barriers to care.
Fig 14

15
To conclude my paper has shown that this is truly a decade when patients will take control of their health given their access to monitoring and communication tools, cutting edge and personalised information, and the power of networking via social media. Spontaneous, unprecedented and massive empowerment of consumers may turn out to be the most important medical transformation of our lifetime. Best practice will be driven by a partnership between physicians and patients to deliver the best health care for the consumer; it will be a new type of care with one goal on mutual respect. Potentially e-patients may have the power to help heal healthcare.
This paper has shown me that there is still a lot of work that is needed to be done to involve digital information in medicine to its full capacity, especially around ethics and safety for both consumers and physicians. I support all aspects of research around this 21st century medicine.
One day in the near future there will be virtual hospitals and patients will be accessing healthcare from home or on the move with mobile devices. They will be able to contact their doctors very easily, perhaps by text or in a virtual world. There will be no geographical barriers patients can consult any expert in the field on virtual world and find the diagnosis or treatment to their undiagnosed ailment. Perhaps there will be a virtual hospital for each health condition, where the physicians and patients meet regularly so they not only help but learn from each other. Virtual world with avatars like in Secondlife may take time to establish as it requires initial investment into complicated technology and education of its users. But Virtual hospital models like texts, monitoring devices, Skype etc can be more easily established to help redesign healthcare to be more cost effective especially triggered by the public spending cuts. This partnership has the potential to revolutionalise the practice of medicine. Path will be tough but it is inevitable.

16
References
1.http://e-patients.net/e-Patients_White_Paper.pdf
2.http://e-patients.net/
3.http://www.jopm.org/
4.http://participatorymedicine.org/
5.http://en.wikipedia.org/wiki/Perfect_storm
6.(http://www.ted.com/talks/dave_debronkart_meet_e_patient_dave#t-371936
7. http://www.ted.com/talks/jack_andraka_a_promising_test_for_pancreatic_cancer_from_a_teenag
er
8. Mesko,B.(2013)Social Media in Clinical Practice.Pgs49-57, Springer
9. http://www.icrossing.com/sites/default/files/how-america-searches-health-and-wellness.pdf
10.http://qualitysafety.bmj.com/content/early/2013/01/31/bmjqs-2012-001744.full 11.https://www.boundless.com/marketing/social-media-marketing/introduction-to-social-media-digital-marketing/what-is-social-media/ 12.http://qualitysafety.bmj.com/content/early/2013/01/31/bmjqs-2012-001744.full) 13 .http://www.bmj.com/content/338/bmj.b1033?ijkey=2c3a3f56c21c9e9e46b0c428ee5f1fff00df16d9&keytype2=tf_ipsecsha) 14.http://citeseerx.ist.psu.edu/viewdoc/download?rep=rep1&type=pdf&doi=10.1.1.183.5834) 15.http://www.patientslikeme.com/). 16.http://www.genome.gov/10001772) 17.http://ec.europa.eu/digital-agenda/en/eu-policy-ehealth 18.http://www.bmj.com/content/319/7220/1305) 19.http://www.techopedia.com/definition/25604/virtual-world 20.http://www.jopm.org/opinion/commentary/2013/05/16/a-model-for-the-future-of-health-care/). 21.http://www.hrsa.gov/healthit/toolbox/HealthITAdoptiontoolbox/MeaningfulUse/intro2meaningfuluseandpatientandfamily.html 22.http://www.merriam-webster.com/dictionary/crowdsourcing 23.http://thecourse.webicina.com/ 24.http://secondlife.com/ 25.http://www.jmir.org/2008/3/e23/ 26.http://www.jopm.org/opinion/commentary/2013/05/16/a-model-for-the-future-of-health-care/ 27.http://www.jmir.org/2006/3/e22/ 28.http://www.jmir.org/2003/3/e17/ 29. http://ec.europa.eu/digital-agenda/en/transatlantic-cooperation 30.http://www.jmir.org/2014/2/e13/?utm_source=rss&utm_medium=rss&utm_campaign=social-media-a-review-and-tutorial-of-applications-in-medicine-and-health-care 32.(http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2762768/ 33.http://www.jmir.org/2014/2/e13/?utm_source=rss&utm_medium=rss&utm_campaign=social-media-a-review-and-tutorial-of-applications-in-medicine-and-health-care 34.http://ghr.nlm.nih.gov/handbook/hgp/description

17
Figures
1. http://perubatan.org/v3/kehidupan/153-kesihatan/1243-medical-student-syndrome-
cyberchondria
2. http://www.slideshare.net/paulgrant/the-epatient-empowered-enabled-and-electronic)
3. Mesko,B.(2013)Social Media in Clinical Practice.Pgs49-57, Springer
4. http://www.slideshare.net/paulgrant/the-epatient-empowered-enabled-and-electronic
5. http://www.icrossing.com/sites/default/files/how-america-searches-health-and-wellness.pdf
6. http://www.slideshare.net/paulgrant/the-epatient-empowered-enabled-and-electronic
7. http://engagementstrategy.com/articles/social-media-lessons-from-around-the-world/
8. http://upload.wikimedia.org/wikipedia/commons/b/b9/Swan_Health_2.0_model.jpg
9. http://www.itu.int/en/ITU-D/ICT-Applications/Documents/JC_30_sept-
Ehealth_Strategy_v2.pdf http://palmitech.com/global-ehealth-adoption-and-ict-management/
10. http://scienceroll.files.wordpress.com/2012/06/filter.jpg
11. http://ec.europa.eu/digital-agenda/en/transatlantic-cooperation
12. http://www.slideshare.net/paulgrant/the-epatient-empowered-enabled-and-electronic
13. http://thecourse.webicina.com/
14. http://e-patients.net/e-Patients_White_Paper.pdf
Title Images
Social network media - http://www.fdcpa.com/Seminar_Presentations/strategic-issues-facing-construction-industry-fall-2011.pdf
Doctor patient team - http://blogs.biomedcentral.com/bmcblog/2014/02/03/the-face-of-medicine-is-changing-are-we-ready-for-the-new-era/