The Effectiveness of an Educational Program about...
101
1 NATIONAL RIBAT UNIVERSITY Faculty of Graduate Studies and Scientific Research The Effectiveness of an Educational Program about Occupational Hazards Safety Measures on Critical Care Nurses at Khartoum State Public hospitals Sudan 2013-2016 Research Presented to a Ph. D in community Health Nursing Prepared By: Yasmin Elsiddig Abdalla Supervisor: Dr. Adil Abu Almaali Elsiddig August 2016
Transcript of The Effectiveness of an Educational Program about...

1
NATIONAL RIBAT UNIVERSITY
Faculty of Graduate Studies and Scientific Research
The Effectiveness of an Educational Program about
Occupational Hazards Safety Measures on Critical
Care Nurses at Khartoum State Public hospitals
Sudan 2013-2016
Research Presented to a Ph. D in community Health Nursing
Prepared By: Yasmin Elsiddig Abdalla
Supervisor: Dr. Adil Abu Almaali Elsiddig
August 2016
2
Dedication
I dedicate this work
To my
Mother, husband, sisters and brothers for their support and encouragements
To my
Children: Mohammad, Mafaz, Yomna and Mariam
God bless you all, wish you always live in love and peace
I

3
Acknowledgement
I would like to acknowledge Dr Adil Abu Elmaali for his guidance and help,
my thanks extended to Khartoum state ministry of health personnel who
facilitated this work, and critical care nurses who worked in my study hot
areas.
II
4
Contents
III
Title Page No.
Chapter (1)
Introduction
2
Justification 4
Thesis questions 4
Objectives 5
Chapter (2)
Literature review
6
Previous study 26
Chapter (3)
Research methodology
33
Study design 34
Study population 34
Sampling technique 34
Sample size 34
Participants number 35
Interventions 35
Study tools 35
Study variables 36
Ethical consideration
37
Chapter (4)
Results
38
5
Title Page
No.
Chapter (5)
Discussion
75
Conclusion
77
Recommendations
78
References
79
Bibliography
82
Annex 1 (questionnaire)
84
Annex 2 (check-list)
87
Annex 3 (formal letters)
88
Annex 4 ( manual of the educational program)
92

6
IV
List of abbreviations and figures
Abbreviation
AACCN: American Association of critical care nursing
A/N: afternoon/night
BSI: body substance isolation
CDC: center for diseases control and prevention
CCU: cardiac or coronary care unit
CC: critical care
CCN: critical care nursing
CCNs: critical care nurses
CMV: cytomegalovirus
DB: the decibel
E.G: example gratia, (gratia is Latin word means for the sake of)
HBV: hepatitis B virus
HCV: hepatitis C virus
HAI: hospital acquired infection
ICU: intensive care unit
ILO: international labor organization
MPD: maximum permissible dose
MRSA: methicillin resistant staphylococcus aureus
NCRPM: the national council on radiation protection and managements
OH: occupational hazards
OSHA: the occupational safety and health administration
OHN: occupational health nurse
PPE: personal protective equipment
RN: registered nurse
RR: recovery room
TB: tuberculosis

7
WHO: world health organization
V
Figures & tables
Figure 1: CCNs distributions in study areas
Figure 2: CCNs distributions in CC areas types
Figure 3: CCNs age groups
Figure 4: participants’ gender
Figure 5: CCNs educational level
Figure 6: main working shift
Figure 7: length of experience
Figure 8: meaning of occupational hazard
Figure 9: tapes OHs
Table 1: CCNs knowledge about meaning of occupational hazards
Table 2 : types of OHs
Table 3: causes of OHs
Table 4: preventive measures of OHs
Table 5: component of universal precautions
Table 6: availability of PPE
Table 7: coping characteristics of CCNs
Table 8: CC units per hospitals
Table 9: types of CC units
Tables 10: assess attitude of CCNs for preventive measures
8
VI
الخالصة
األهداف
بالمستشفيات الحكومية بوالية الخرطوم وهي: مستشفى بأقسام الرعاية الحرجةأجريت هذه الدراسة
ومستشفى أ حمد قاسم للقلب أم درمان التعليمي، بحري التعليمي، الخرطوم التعليمي، الشعب التعليمي
عنوسط تقنيي التمريض لتقويم التأثير الناتج عن البرنامج التعليميهذه الدراسة تهدفو .والكلى
.(والسالمةالمخاطر المهنية )المعرفة
- المنهجية:
الى 2014 الفترة )من، أجريت في (وبعد التدخلقبل ) الدراسة التداخلية بطريقةدراسة تم إنفاذ هذه ال
وبعد قبل استخدام استبيان وقائمة تم ،)تغطية كاملة( تمريضتقني 200عينة الدراسة كانت ،)2016
أقسام تقنيي تمريض والسالمة لدىالبرنامج التعليمي في المعرفة عنالتأثير الناتج لمعرفة التدخل
أيضا وقد تم عملهم،في مكان الموجودةالمهنية طر افيما يتعلق بالمخ الرعاية الحرجة أو العناية المكثفة
.مستشفى لإجراء مقابلة مع رئيسة التمريض لك
-النتائج:
%67 وحملة البكالوريوس يمثلون %17% بينما الذكور 83تمثل نسبة اإلناث في الدراسة
مقارنة وذلك بعدلبرنامج التعليمي على المشاركين أثر إيجابي معتبر إحصائيا لاوضحت الدراسة
% 14.5هي التدخل الفيزيائية قبلفكانت نسبة معرفة المشاركين للمخاطر .وبعد البرنامجالنتائج قبل
% قبل 17، كذلك خطر اإلشعاع كانت نسبة معرفته أي الغالبية العظمى %99.5أما بعده فقد أصبحت
بعده. كل المشاركين %100والتدخل
وبعد % قبل 100الدراسة المعرفة الممتازة للمشاركين للمخاطر الحيوية حيث كانت بنسبة بينت
كالتالي: المخاطرخاطر المهنية كانت نسبة نتيجتها ممعرفة طرق السالمة أو الوقاية من ال .التدخل
% 100% قبل و81.5بعده، طرق السالمة من اإلشعاع هي % 99.5 –% قبل التدخل 93الكيميائية
%.99% قبل التدخل وبعده أصبحت 14.5نسبته نفسيالبرنامج التعليمي، وتخفيف الضغط ال بعد
9
بالطريقة التي تحتمها طبيعة عمل الوسائل الواقية من العدوى المعروفة عالمياً لم يتم توفيرها
.من العدوى المتوفرة بطريقة جيدة المشاركون في العينة يستخدمون الوسائل الواقية المشاركين،
V11
-الخاتمة:
لعدد من المخاطر المهنية، حيث يمكن الوقاية االمهن التي يتعرض العاملين فيه التمريض منيعتبر
في مكان العمل كتقديم الرعاية الواجبات اليومية ويصبح أحدمن بعضها بينما البعض اآلخر ال مفر منه
.وبال تأجيلللمرضي في وضع قيام
-التوصيات:
المعرفة بالمخاطر المهنية عبر برامج تدريب دوريةتطوير -
توفير وسائل الوقاية بصورة دائمة -
تحسين بيئة العمل -
تشجيع التصنيع الداخلي لوسائل الوقاية المعروفة عالميا -
القيام ببحوث في الموضوع مستقبال -
تعيين ممرض صحة مهنية لكل مستشفى -
ى السودان بالقيام نوصي المختصين في الصحة المهنية على مستو هذه الدراسةاستنادا على -
ببرامج تدريب لهذه الفئة في كل مستشفيات الواليات األخرى.

10
VIII
Abstract
Objective:
The aim of the study was to assess the effectiveness of an educational program on critical
care nurses about occupational hazards, knowledge and safety.
Methodology:
It was a pre/post interventional, hospital-based study carried during 2014-2016, The study
subjects were 200 critical care nurses working in intensive care settings, Khartoum state
public hospitals. Questionnaire and checklist were used, pre and post the educational
program to assess the effectiveness of the program on critical care nurses’ knowledge,
safety practice regarding occupational hazards; interview was carried with hospital’s
matron.
Results:
Knowledge about Physical hazards as type in pre intervention results was 14.5%, and
99.5% in posttest, Knowledge about radiation hazard was 17% in pretest, 100% in post
intervention.
Knowledge about biological hazard type was 100% in both pre and post results. Knowledge
about chemical hazard as one of hazards in pretest was 11.5% and 98.5% in posttest.
Knowledge about psychosocial hazards was 34% in pretest and 99.5% in posttest.
Regarding preventive measures of occupational hazards, participants showed 93% of pre
intervention knowledge about chemical hazards prevention and 99.5% in posttest result,
prevention of radiation by distance 81.5% in pretest and 100% post intervention test.
Stress mitigation by relaxation exercise results was 14.5% in pretest and 99% posttest.
Personal protective equipment were poorly provided. Shoes cover, face shield
unavailable.

11
IX
Conclusion
The educational program for critical care nurses had efficiency results, evidenced by the
improved results of critical care nurses’ knowledge about occupational hazards types,
causes and preventive measures for each hazards in critical care settings in post educational
program results.
Recommendations:
• Based on this study, regular trainings and educational meetings to enhance
occupational safety, develop/introduce policies and guidelines or strategies in all
aspects related to occupational hazards safety measures need to be offered in all
Sudan states hospitals.
• Develop effective continuous commitment program for provision of protective
measures.
• Improvement of the physical and social environment of critical care settings.
• Occupational health Department at the level of the State should have a role in
protecting the workforce in health care settings.
• Encouragement of manufacturing the protective measures locally.
• Future research recommended for this specialty population.

12

13

14
Chapter (1)
Introduction
Objectives
15
Introduction
Daily patient care presents the nurses with a real risk for infectious diseases, toxic
substances, back injuries, and radiation. Nurses also are subject to hazards such as stress,
shift work, and violence in the workplace. These typically fall under the broad categories
of chemical, biological, physical, and psychosocial occupational hazards.
Nurses continue to report high levels of job-related injury and illness. Working
environment, responsibilities, and duties of nurses put them in the frontline of numerous
occupational hazards. (1, 2, 3, 4)
The Bureau of Labor Statistics reports that there are 1,859,000 registered nurses (1993)
and 659,000 licensed practitioners nurses (1992) employed in the United States. Of the
2,518,000 nurses, 882,647 35% are employed in hospitals, and the rest in other health
care settings including but not limited to nursing homes, health maintenance
organizations, physicians' offices, community health agencies, schools, and corporations.
In 1992, the rate of occupational injury and illness for nurses in health care settings was
18.6% per 100 full-time workers (18.2% accounted for injuries). This is higher than for
hazardous occupations such as heavy construction where the rate of occupational injury
and illness is 13.8% per 100 full-time workers or mining where the total is 7.5% per 100
full-time workers. (3)
Some common occupational hazards that nurses might face are:
* Communicable and contagious diseases and exposure to blood-borne pathogens (e.g.,
HIV, HCV, and HBV) due to needle-stick injuries threaten health of nurses. It is
estimated that 600000 to 800000 needle-stick injuries occur each year in all healthcare
settings. Injections (21%), suturing (17%), and drawing blood (16%) are the main causes
of exposures. Severe acute respiratory syndrome (SARS), tuberculosis, and methicillin
resistant staphylococcus infection are other infectious diseases that can afflict nurses.
(2, 5)
16
* The vast majority of nurses experience persistent job-related pain, mainly
musculoskeletal pain in at least one region, it seems that work-related musculoskeletal
pain and injuries are common among nurses all over the world. Most of these pain and
injuries are due to lifting and moving patients manually. (6, 7)
* Work overload and stress are other factors that threaten the health of nurses and can
cause burnout and fatigue. Working in three shifts, in difficult settings such as oncology,
intensive care units or emergency wards, and caring of incurable patients puts a
considerable psychologic, spiritual, and physical pressures on nurses. As a result، fatigue
is a common feeling among nurses.
* Chemical materials are other hazardous sources to nurses. Disinfectants and sterility
products such as glutaraldehyde and ethylene oxide, hazardous drugs such as drugs that
are used during chemotherapy and latex exposure are among other occupational hazards
for nurses.(2)
* Nurses, continue to experience high rates of on-the-job violence, experiencing verbal
abuse and physical violence. (8)
Critical care nursing specialty, concerns with delivery of care for physiologically
unstable patients, with life- threatening condition and it is a highly interdisciplinary
specialty, this give big chance for those nurses to face more occupational hazards. RNs
who work with critically ill patients also may suffer emotional strain from observing
patient suffering and from close personal contact with patients’ families.
Nurses must observe rigid, standardized guidelines to guard against diseases and other
dangers posed by work hazards. Indeed, the cost to prevent, control, and treat
occupationally acquired illness is considerable, in terms of both money spent and lives
affected. Rather, incurring the risk for occupationally acquired illness is necessary for
daily health care delivery. The willingness of health care workers to accept this risk is, in
many ways, as important to health care as their professional skills. Every healthcare
setting should address this important issue and give priority to the safety of health care
workers. (2, 9, 10)

17
Justification
As the critical care areas are the units of hospitals offering potentially life-saving
intervention during physiological crises and life threatening conditions, the nurse who
works in these units must has essential part in health workers safety programs.
Critical care nurses expose to variety of biological, physical, chemical, ergonomic,
psychosocial hazards in the work and chemical dependency. They must be aware of the
potential hazards they face, and preventive strategies that are effective for developing
appropriate occupational safety programs. (2)
The researcher master thesis was a descriptive, cross-sectional study carried in April,
May and June 2011 in Ahmed Gasim Hospital Cardiac Surgery and Renal Transplant
Center, about occupational hazards and illnesses among CCNs, the Study subjects are 66
nurses working in CC area for more than one year. Questionnaire and checklist were used
to assess occupational illness among critical care nurses and preventive measures that
actually used.
The results revealed that low backache, eye fatigue, muscles pain, irritability and upset
stomach occurred to more than 50% of the participants, 6% HBV, 1.5% HCV and 4.5%
TB. According to these values, the researcher found it was important to provide
occupational hazards safety educational program on similar areas to nurses in Khartoum
State public hospitals.
Thesis questions:
1- Would an educational program about occupational hazards safety for CCNs be
effective?
2- Would CCNs know OH they face in work, the causes and prevention of each
hazard?
3- Are personal protective equipment available in CC areas?
4- Would CCNs practice suitable safety measures in their areas?
5- Would CCNs know the coping methods that make them successful nurses,
tolerating their job hazards?

18
Objectives
a) General objectives
To assess the effectiveness of an educational program for critical care nurses about
occupational hazards knowledge and safety.
b) Specific objectives
1. To assess the effectiveness of an educational program for critical care nurses about:
- Physical hazard knowledge and safety
- Radiation hazard knowledge and safety
- Biological hazard knowledge and safety
- Chemical hazard knowledge and safety
- Psychosocial hazard knowledge and safety
2. To determine changes in CCNs practice post the educational program
3. To evaluate changes in CCNs awareness about universal precaution of infection
control.
4. To test availability of personal protective equipment in critical care settings.

19
Chapter (2)
Literature Review
Previous studies
20
Literature Review
Occupational health
It is defined as the prevention among workers, of departures from health caused by their
working conditions, The protection of the workers in their employment from risks resulting
from factors adverse to health, the placing and maintenance of the worker in an
occupational environment adapted to his physiological and psychological equipment, and
to summarize the adaptation of work to man and each man to his job.
Occupational health aims at the promotion and maintenance of the highest degree of
physical, mental, and social well- being of all workers in all occupations.
The joint ILO/ WHO committee on occupational health, in the course of its first session,
held in 1950, gave the fallowing definition: (Occupational health should aim at the
promotion and maintenance of the highest degree of physical, mental and social wellbeing
of workers in all occupations). (11, 12)
Occupational hazards:
OHs are an external conditions and influences, which have their effects on work
population, in their work environment.
Workers may be exposed to five types of hazards depending upon their occupation.
Occupational Hazards are:
(1) Physical
(2) Chemical
(3) Biological
(4) Mechanical
(5) Psychosocial hazards. (12)
Critical Care Settings:
Are the units offering potentially life-saving intervention during physiological
crises, with emphasis of medical needs and availability of technology, called tertiary care
areas or intensive care units (ICUs, CCU),are brightly lit, windowless units, often noticed
by infrequent visitors in fact are noisy (Hilton1985). (13, 14)

21
Critical care nurse or intensive-care nurse:
A professional registered nurse who works in an intensive-care unit. Receives the patient
into the ward; gives him/her the necessary personal treatment; connects him, according to
need, to the appropriate medical system (e.g. respiratory instruments, artificial-feeding
set-up, blood and plasma transfusion system, measuring and monitoring systems, etc.);
Conducts a follow-up of his health condition and has to be aware of any change in the
health situation of the patient.
Assists the medical doctor in the treatment in extreme events of required resuscitation
and in connecting into the necessary instrument systems, highly proficient in the medical
model, had broad knowledge base in physiological and pathophysiological of the organ
systems and response quickly and intelligently to subtle alteration in critically ill patient.
Examples of occupational hazards in critical care units:
• Biological hazards [infectious hazards]
• Physical and ergonomics [noise, musculoskeletal injuries]
• Chemical hazards [cytotoxic drugs]
• Radiological hazards [portable radiography and fluoroscopy]
• Psychosocial hazards [stress, conflicts, job dissatisfaction] (2)
Infectious (biological) hazards:
There is a potentially high risk of acquiring infectious diseases in the critical care
units. Potential infection may be transmitted by blood or body fluids, by droplets in the air,
or by direct contact. Blood–borne pathogens of major concern include human
immunodeficiency virus (HIV), hepatitis B virus (HBV), and hepatitis C virus. Infections
transmitted by air–borne particles include cytomegalovirus (CMV), tuberculosis (TB), and
meningococcal disease. Direct contact with secretions infected with herpes simplex virus
produces herpetic whitlow. Adherence to strict procedures involving body substance
isolation (BSI) minimizes the risk of occupational exposure to infectious agents.
The risk of acquiring infection from exposure to blood and body fluids varies, it is
estimated that 10% to 20% of health care workers are seropositive (anti-HBs) for hepatitis

22
B (Patterson et al., 1995). The risk of seroconversion following exposure to blood from
HIV – infected patients is less than 1% (Gurevich, 1989; CDC, 1988, 1989).
Methods of minimizing exposure to blood and body fluids are known as universal
precautions or BSI. Since the infection status of patients is usually unknown, all patients
should be considered potential carriers of HIV, HBV, and other blood-borne pathogens.
Recommendations from the Centers for Disease Control, (CDC, 1989) for health care
professionals who are likely to have percutaneous or mucous membrane exposure to blood
or body fluids include:
1. Proper handling and disposal of needles or other instruments.
2. Use of gloves, masks, gowns, or eyewear when direct contacts, aerosolization, or
splashing of blood and body fluids are likely.
3. Immediate washing of hands and other skin surface after contamination with blood
or body fluids.
4. Use of effective germicides for cleaning spills of blood or body fluids (1: 10
dilution of household bleach).
Special attention should be given to proper handling and disposal of needles because
the incidence of needle–stick injury remains high among nurses (Jackson et al., 1986).
Needles should never be recapped, bent, or separated from the syringe. Impervious
receptacles for needle – disposal should be conveniently placed as close to the bedside as
possible.
The hepatitis B virus is a potentially unrecognizable source of infection for critical care
nurses because asymptomatic carries remain infectious. The risk of acquiring HBV
infection following a puncture from a contaminated needle ranges from 6% to 30%. Two
types of vaccines are effective in preventing hepatitis B. One is plasma – derived, and the
other is a recombinant vaccine. Use of the plasma- derived vaccine is restricted to dialysis
patients, other immunocompromised persons, and those with a known allergy to yeast. Pre-
exposure vaccination is recommended for all health care and public safety workers due to
their risk of exposure to blood or body fluids (Centers for Disease Control, 1990). (2, 12,
16, 17, 18)

23
Universal infection control precautions:
. Devised in US in the 1980’s in response to growing threat from HIV and hepatitis B
. Not confined to HIV and hepatitis B
. Treat ALL patients as a potential biohazard
. Adopt universal routine safe infection control practices to protect patients, self and
colleagues from infection
- Composed of:
1. Hand washing
- Single, most effective action to prevent HAI - resident/transient bacteria
- Correct method - ensuring all surfaces are cleaned - more important than agent
used or length of time taken
- No recommended frequency - should be determined by intended/completed actions
- Research indicates:
* poor techniques - not all surfaces cleaned
*frequency diminishes with workload/distance
*poor compliance with guidelines/training
2. Personal protective equipment [PPE]
PPE when contamination or splashing with blood or body fluids is anticipated:
Are:
*Disposable gloves
*Plastic aprons
*Face masks
*Safety glasses, goggles, visors
*Head protection
*Foot protection
*Fluid repellent gowns
3. Preventing/managing sharps injuries
Prevention by:
24
Correct disposal in appropriate container
Avoid re-sheathing needle
Avoid removing needle
Discard syringes as single unit
Avoid over-filling sharps container
Management by:
Follow local policy for sharps injury
4. Aseptic technique
Sepsis – is harmful infection by bacteria
Asepsis – is prevention of sepsis
Minimize risk of introducing pathogenic micro-organisms into
susceptible sites
Prevent transfer of potential pathogens from contaminated site to other
sites, patients or staff
Follow local policy
5. Isolation
Single room or group
Source or protective
Source - isolation of infected patient
Mainly to prevent airborne transmission via respiratory droplets
respiratory MRSA, pulmonary tuberculosis
Protective - isolation of immuno-suppressed patient (May, 2000)
Significant psychological effects (Davies et al, 1999)
6. Staff health
(Risk of acquiring and transmitting infection)
- Acquiring infection
Immunization
Cover lesions with waterproof dressings
Restrict non-immune/pregnant staff
25
- Transmitting infection
Advice when suffering infection
Report accidents/untoward incidents
Follow local policy
7. Linen handling and disposal
Bed making and linen changing techniques
Gloves and apron - handling contaminated linen
Appropriate laundry bags
Avoid contamination of clean linen
Hazards of on-site ward-based laundering
Follow local policy
8. Waste disposal
Clinical waste
- high-risk red color, Potentially/actually contaminated waste including body fluids
and human tissue
Sharp objects
- Yellow plastic sack, tied prior to incineration
Household waste - low risk
- green color
Paper towels, packaging, dead flowers, other waste which is not dangerously
Contaminated
- black plastic sack, tied prior to incineration
Follow local policy
9. Spillages of body fluids
PPE - disposable gloves, apron
Soak up with paper towels, kitchen roll
Cover area with hypochlorite solution e.g., Milton, for several minutes
Clean area with warm water and detergent, and then dry
Treat waste as clinical waste - yellow plastic sack
26
Follow local policy
10. Environmental cleaning
Recent concern regarding poor hygiene in hospital environments
Some pathogens survive for long periods in dust, debris and dirt
Poor hygiene standards - hazardous to patients and staff
Report poor hygiene to Domestic Services
“Hospitals should do the sick no harm” (Nightingale, 1854)
11. Risk management/assessment
No risk of contact/splashing with blood/body fluids - PPE not required
Low or moderate risk of contact/splashing - wear gloves and plastic apron
High risk of contact/splashing - wear gloves, plastic apron, gown, eye/face
protection.
(Body fluids are Cerebrospinal fluid, peritoneal fluid, pleural fluid,
synovial fluid, amniotic fluid, semen, vaginal secretions, and
Any other fluid containing visible blood e.g., urine, faeces. (3, 17)
Musculoskeletal injuries
Fatigue and lower back pain due to the handling of heavy patients and long periods of
work in a standing posture. Back pain occurs frequently among nurses despite their
training and experience. The frustration and discomfort of back pain decreases patient
care efficiency. Determining the cause in individual cases is complex because nurses
perform many activities that lead to musculoskeletal strain. Since the continuum of
symptoms ranges from minor to severe pain, it is difficult to characterize back injury.
Most injuries involve the lumber muscle group.
In a study in Iran, on average, the nurses reported musculoskeletal pain, 89% had
musculoskeletal pain, mainly in lower back (74%), and knees (48.5%). (6)
In a study in the Netherlands, 57% of nurses had musculoskeletal pain in at least one
region. In another study in Brazil, 80.7% of nurses complained of musculoskeletal pain.
Upper extremity, shoulder, and neck injuries are also common among nurses. It seems

27
that work-related musculoskeletal pain and injuries are common among nurses all over
the world. Most of these pain and injuries are due to lifting and moving patients
manually. (6, 7)
Results from a number of back pain studies conducted during the past 15 years show
an annual prevalence rate of 400 to 500 injuries per 1000 nurses at risk ( Buckle, 1999).
Strains and sprains of the lower back account for 50% of all musculoskeletal disorders
among American workers (Williamson et al., 1988). Back injuries result in more lost time
and wages among nurses who provide bedside care than any other single injury.
Nursing is unique because the occupation involves lifting and transferring human
beings rather than inanimate objects. As Harber and associates (1985) point out, the
human body is not a compact mass, and patients are unpredictable. Sudden resisting
movements are common in critical care. The proper technique for lifting or transferring a
patient may depend on patient size, available staffing, or accessible equipment.
Nurses must assess each individual patient separately to minimize the risk of back
injury, especially during patient transfers.
Conditions that predispose nurses to musculoskeletal injury can be classified into
two major categories: nurse characteristics and hospital environment (Feldman, 1986).
Nurse characteristics are divided into three subgroups: physical, emotional, and
preferential. Preferential characteristics include activities that nurses perform on their own
volition. The categories and subgroups are not mutually exclusive. Fox example, stress
caused by inadequate staffing may cause fatigue, which in turn may produce carelessness.
Physical characteristics such as length or heredity cannot be changed. However, emotional
and preferential characteristics of nurses can be modified or alleviated to reduce the risk of
back injury.
In a study, 43.4% of nurses reported excessive fatigue. Raftopoulos et al. also reported that
91.9% of Cypriot nurses had fatigue.
28
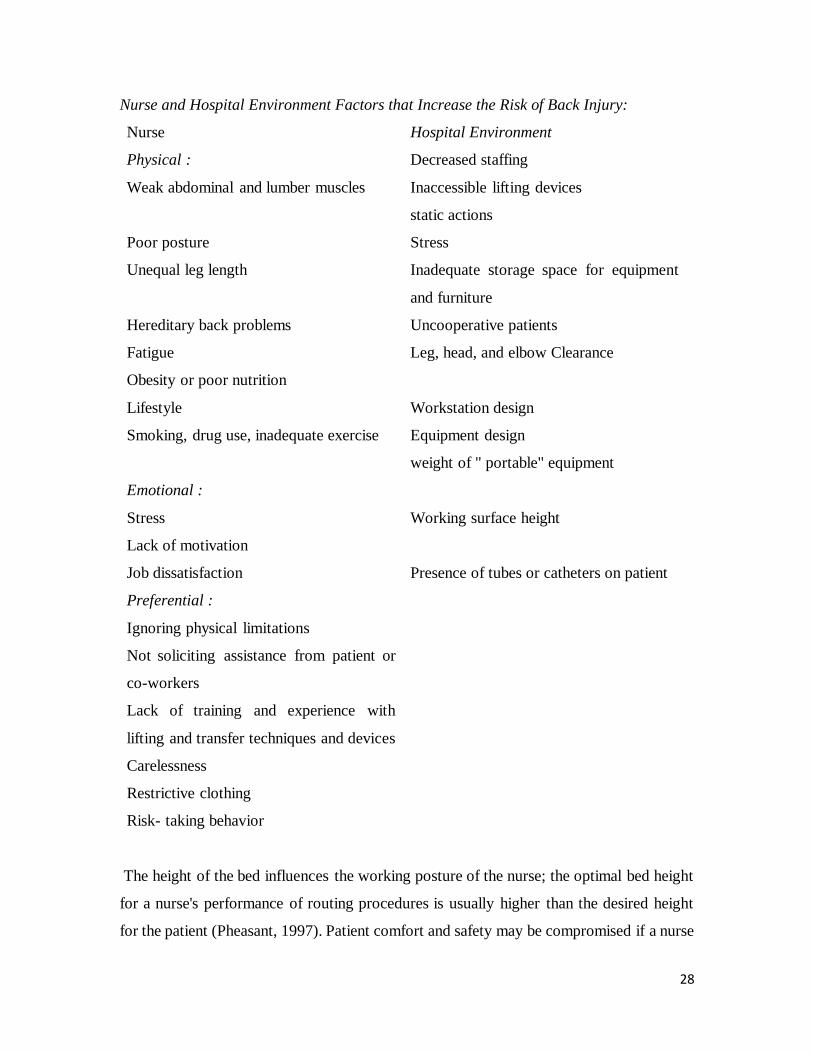
Nurse and Hospital Environment Factors that Increase the Risk of Back Injury:
Nurse Hospital Environment
Physical : Decreased staffing
Weak abdominal and lumber muscles Inaccessible lifting devices
static actions
Poor posture Stress
Unequal leg length Inadequate storage space for equipment
and furniture
Hereditary back problems Uncooperative patients
Fatigue Leg, head, and elbow Clearance
Obesity or poor nutrition
Lifestyle Workstation design
Smoking, drug use, inadequate exercise Equipment design
weight of " portable" equipment
Emotional :
Stress
Lack of motivation
Working surface height
Job dissatisfaction Presence of tubes or catheters on patient
Preferential :
Ignoring physical limitations
Not soliciting assistance from patient or
co-workers
Lack of training and experience with
lifting and transfer techniques and devices
Carelessness
Restrictive clothing
Risk- taking behavior
The height of the bed influences the working posture of the nurse; the optimal bed height
for a nurse's performance of routing procedures is usually higher than the desired height
for the patient (Pheasant, 1997). Patient comfort and safety may be compromised if a nurse

29
adjusts the bed height to provide protection from back strain. Bed height will be different
for each nurse depending on the procedure to be performed and the height of the nurse.
Maintaining ergonomically correct equipment for each nurse at any given time is
problematic, especially when more than one nurse is assigned to a patient.
Patient contact activities in critical care frequently require nurses to maintain an
awkward, stressful posture for an extended period of time. In an observational study,
Harber and colleagues (1998) found that 78% of static actions were performed in a
squatting or semi-squatting position. These actions may be particularly stressful on the
lower back because the same muscle groups are involved throughout the activity.
It is important to recognize and develop ways to minimize stressful postures a
combination of personal and environmental modifications should be implemented to be
effective. No single method will completely prevent or control low back pain.
Nurses are not selected by physical ability, and job strength requirements are rarely
addressed in critical care. Conducting pre-employment strength tests to determine whether
the nurse can perform strenuous nursing tasks is feasible (Keyserling et al, 1987). Patient
assignments could then be matched according to the physical strength of the nurse.
Methods for Minimizing Low Back Injury:
Personal:
Strengthen abdominal lumbar muscles through regular exercise
Maintain good posture
Maintain proper nutrition
Solicit assistance from co-workers and patients
Use mechanical devices for lifting
Review knowledge of proper lifting techniques
Alleviate risk–taking behaviors
Wear nonrestrictive clothing
Lift no more than 35% of your body weight or less
Raise or lower beds to facilitate good posture
Minimize stress
Environmental:
Design workplace layout using ergonomic principles
30
Provide adequate staffing
Conduct pre- employment strength testing and evaluation
Make lifting devices accessible
Conduct regular in – service training addressing static actions
Consult a nursing ergonomic specialist
Redesign storage areas
Maintain clear paths for walking and moving furniture or equipment
Install nonslippery floor surfaces
Because the number of low back injuries among nurses has not shown any
appreciable decline, researchers question the effectiveness of training programs that focus
on safe lifting procedures (Haber et al., 1995, 1997a and; Stubbs et al., 1993; Snook et al.,
1988). As Cato and colleagues (1989) point out, perhaps training programs are more
effective when used in conjunction with ergonomic job analysis and job – specific training.
Training programs should provide information on correct postures to minimize muscle
strain, exercises to strengthen the back, and proper lifting techniques. A well – trained
“nursing ergonomic consultant" who is sensitive to each nurse's physical ability could
provide services and assistance to individuals who are at risk of low back injury (Harbor
et al., 1985).
Although patient comfort and safety are the highest priorities in hospital care, nurses
should be encouraged to develop an understanding of basic ergonomic concepts and to
analyze their own safety at the bedside and work station. Personal habits are not easily
modified, but awareness and effort to maintain a safe environment in the workplace is
important. Efforts should be made to minimize back injury away from the workplace as
well. Application of these principles will reduce musculoskeletal injury, increase
productivity, improve health and safety, and provide a higher quality of patient care.( 2, 4,
19, 20)
Chemical hazards
There are varieties of chemicals, including many therapeutic agents, in the critical care
setting that may pose a hazard to nurses.

31
Danger of exposure to anesthetic gases (ethyl bromide, ethyl chloride, ethyl ether,
halothane, nitrous oxide.).
Skin defatting, irritation, and dermatoses because of frequent use of soaps, detergents,
And disinfectants.
Irritation of the eyes, nose, and throat because of exposure to airborne aerosols or contact
with droplets of washing and cleaning liquids.
Chronic poisoning because of long-term exposure to medications, sterilizing fluids (e.g.
glutaraldehyde), and anesthetic gases.
Latex allergy caused by exposure to natural latex gloves and other medical devices.
Nearly 400.000 cancer patients received therapy with cytotoxic drugs in 1986
(Williamson et al., 1988). Some of these patients required care for septic complications.
Aerosolized drugs used to treat infections in neonates and persons with HIV infection may
cause birth defects. Pregnant women should avoid ribavirin because so many unknown
factors are associated with these agents, nurses should minimize contact with all potential
chemical hazards. Antineoplastic agents may enter humans inadvertently through
inhalation, ingestion, or absorption through unprotected skin. These agents have
carcinogenic potential. All nurses should wear gloves when handling potentially hazardous
drugs. Strict adherence to body substance isolation precautions will help prevent exposure
to drugs and their metabolites in body fluids, including urine. (2, 10, 20, 21, 22)
Radiation Hazards
Portable radiography and fluoroscopy are routine bedside procedures in critical care
areas. Radiation exposure carries the potential for both short-term and long-term biologic
effects. Familiarity with the types and sources of radiation, the maximum permissible doses
for occupational exposure and ways in which the risk of exposure to ionizing radiation can
be minimized will protect nurses from harmful biologic effects.
When atoms and molecules undergo change, energy is released in the form of heat
or light. This energy is referred to as radiation. The three common forms of radiation used
in hospitals are alpha particles, beta particles, and gamma rays (x-rays). Alpha particles
travel only inches in the air and are stopped by health skin tissue. Beta particles may travel

32
several feet before they are absorbed by a thin piece of metal or wood. Gamma rays travel
hundreds of feet and have great penetrating power.
The penetrating ability of each type of radiation varies. Harmful effects to human
tissue result largely from the energy absorbed by the cells. The amount of energy absorbed
or deposited in human tissue determines the total biologic effect. The rem (roentgen
equivalent man or mammal) is the unit that represents the biologic dose used to estimate
potential damage caused by radiation.
There are three potential sources of scattered radiation in critical care environment:
portable x-ray equipment, fluoroscopic equipment, and diagnostic or therapeutic
radionuclide. Scattered or secondary radiation occurs after the primary radiation beam or
application passes through matter. All x-ray and fluoroscopic examinations generate some
scattered radiation. Alpha, beta, and gamma rays exist in the isotopes used for external and
internal radiation treatments. The amount of secondary radiation emitted by patients
receiving radionuclide therapy depends on the organ in which it is localized, the dosage,
the elapsed time after injection, patient size and the distance from the patient (Jankowski,
1984).
Critical care nurses should pay particular attention to the levels of secondary radiation
received from patients who receive radionuclide because the number of hours they spend
in individual patient contact is greater than the time needed in other unit in the hospital.
The body fluids of patients who have received injections of radioactive substances contain
significant amounts of radioactivity. Compliance with BSI procedures is crucial.
The National Council on Radiation Protection and Measurements (NCRPM)
establishes maximum permissible dose (MPD) levels of radiation for occupational
exposure. The current recommendation is 5000 mrem per year for employees who are
likely to be exposed to ionizing radiation during the course of their work (National Council
on Radiation Protection and Measurements, 1980). According to the Code of Federal
Regulations (CFR), radiation dosimetry badges are required when nurses receive doses in
excess of 1250 mrem every 3months.
Actively proliferating cells, such as the gonads, are highly sensitive to radiation.
Teratogenic or carcinogenic effects may occur when an embryo, fetus, or male germ cell

33
is irradiated. Studies show that ionizing radiation damages the gonads, alters genetic
material, reduces fertility, and induces spontaneous abortion (Hunt, 1988).
Exposure to scattered radiation can be minimized in three ways: by time, by
distance, and by shielding.
Protection from secondary radiation can be enhanced by completing procedures in the
shortest possible time without compromising good clinical practice. Penetrable radiation
rapidly decreases as the distance from the source increases. For example, a single film
taken by a portable x-ray machine at 1 meter will produce approximately 0.06 merm of
scattered radiation. At 2 meters the amount is indistinguishable from background radiation
existing in the natural environment.
The third method of minimizing exposure to secondary radiation is the use of
protective shielding lead screens or aprons 5 mm in lead – equivalent thickness should be
used during x-ray and fluoroscopy to protect the gonads. Protective shielding is particularly
important when working with patients who have received radiopharmaceuticals. Leaded
glasses and a thyroid shield are recommended during procedures involving elevated levels
of radiation such as angioplasty (Patterson et al., 1985).
Further epidemiologic studies on the effects of long-term occupational exposure to
ionizing radiation are needed. Until more data are available, pocket dosimeters and film
badges for monitoring exposure to radiation should be used by nurses who are likely to
receive more than 1250 mrem in a 3-month period. Radiation safety committees should
periodically monitor nurses for proper radiation safety techniques. Radiation safety should
be included in hospital orientation programs for new staff and should be reviewed annually
for all employees. Finally, hospital policies regarding the use of radioactive substances and
equipment should be reviewed and revised to include methods for minimizing radiological
hazards to staff. (2, 21, 23)
Noise
Prolonged exposure to noise can be distracting and can prohibit mental
concentration. Psychological responses to noise include increased annoyance and
irritability, impaired judgment, and altered perception (Hilton, 1997). Controlling noise in
the critical care environment will help to minimize fatigue and reduce errors. Factors that

34
influence the impact of noise on nurses include the intensity or loudness of the sound, type
of sound, distance from the source, frequency and duration of exposure, individual
perception of sound, stress level, and age.
The decibel (dB) is used to express the sound level associated with noise
measurement. The Occupational Safety and Health Administration (OSHA) standard for
permissible exposure to noise is 90 dB during an 8- hour shift (Code of Federal
Regulations, 1990). The International Noise Council recommends that sound levels in
patient care areas not exceed 45 dB during the day and 20 dB at night (Hansell, 1994).
Background noise occurs in most work environments. Critical care areas, however,
are remarkably loud. One study reported that sound levels in four critical care units were
as high as 77 dB, which is comparable to hospital cafeteria at noon (Redding et al., 1987).
Other studies have reported sound levels greater that 50 dB over a 24-hour period, with a
number of noises exceeding 70 dB (Hilton,1997; Hansell, 1994). Noise levels of this
magnitude increase the tendency for nurses to become desensitized to noise levels in the
critical care environment.
Elimination or reduction of unnecessary sources of noise is essential. Increasing
nurses' sensitivity to the level of noise on the unit will help to develop appropriate
interventions to decrease or control unwanted sound. Everyone should be encouraged to
speak softly. Patients report that staff conversations and activity are the most disturbing
noise (Hansell, 1984). Discussions among nurses and other hospital staff can generate
sound levels as high as 90 dB (Hilton, 1997). Normal conversational tones measure
between 56 and 60 dB. As Hilton (1997) points out, whispering may be appropriate at
night. Conversations between staff should be limited to patient care concerns, especially at
the bedside. A system of concentrated noise may be helpful (Lindenmuth et al., 1990).
Noise can also be reduced by introducing sound absorbing materials into the architectural
design of the unit. Carpeted walls and floors in the nursing station and patient care areas
will have a dramatic effect on reducing noise. Each unit should have a soundproof section
in which nurses and physicians can confer or spend break periods without disturbing
patients (Dracup, 1998). Utility rooms with sinks, refrigerators, and ice machines should
be partitioned separately from patient care areas. Alarm parameters should be set
appropriately to avoid false alarms. Nurses must take an active role in developing effective

35
strategies to reduce noise. Strict compliance with the standards of occupational exposure
to noise will enhance awareness of noise reduction among the staff. Nurses should be
responsible for evaluating and purchasing equipment such as ventilators, monitors, and
balloon pumps. Equipment that produces excess noise can be modified by the manufacture
to meet noise reduction standards. Nursing consultants should assist in the development of
plans for construction or remodeling of critical care units (Dracup, 1998).
Suppression of noise is an important element of occupational safety and health in
the critical care environment. Nurses and other hospital staff must develop an appreciation
for a quiet working environment. Keeping the noise level as low as reasonably possible is
advantageous to nurses and beneficial to patients. (2, 12)
Stress among critical care nurses
Stress is an imbalance between demand and the ability to cope with it. Stress response
results when the individual fails to cope with a stimulus. Shouk Smith defined it as the
body state of tension, which result from external or internal stressors. External or internal
stressors trigger a stress response. External stressor is an environmental event such as
disasters or being taken seriously ill very suddenly. Internal stressors are our own responses
to wide range of events and situations.
Nurses in critical care units face great amount of stress, which is recognized by all health
professionals. Nursing has been identified as a stressful occupation. Health authorities 1988
report in the public sector included nursing as one of the four high stress occupations
together with police, social works and teaching (Roger D. Poppy N.1999).
Critical care nursing involves excessive physical and emotional stress due to the
nature of the environment which is a closed one, isolated from the rest of the hospital. In a
critical care unit there is constant use of sophisticated machines and equipment amidst
which a nurse is expected to work calmly and efficiently at all times. Nurses encounter
stress while facing death of patients in the critical care units when they have nursed
carefully which perceived as a failure of their work. A sense of inadequacy prevails among
nurse as they lack confidence in handling the patients and equipment's.
Death and dying are the major stressors in critical care, the unpredictability of critical
care environment is another leading stressor other factors of stress also every step must be

36
charted. frequent situation of acute crisis, physical dangers ( inadequate protection from x-
rays, needles, isolation patients, and those who are delirious), lifting heavy unresponsive
patients, constant sounds of moaning, crying, screaming, buzzing, and beeping monitors,
gurgling suction pumps, and whooshing respirators.
Poor communication causes stress leading to a spiral of conflict that leaves everyone
dissatisfied. Furthermore, communications is the medium through which stress is
expressed.
The accumulation of stressors from this intense environment can result in individual’s
developing physical or psychological symptoms. Each person’s response to stress is unique
and individualized. (20, 24, 25)
Effects of stress
Behavioral
Short term irritability, forgetfulness, disorganization thinking, overindulge in drugs,
alcohol, smoking, accidents, impulsive behavior, poor relationship with others, poor work
performance.
Long term: difficulty concentrating on tasks, decreased interest in relationship, Marginal
family breakdown, social isolation.
Physical
Short term: Headaches, backache, insomnia, indigestion and gastrointestinal upset,
tightness in chest, nausea, dizziness, excessive sweating and unexplained shortness of
breath.
Long term: Heart diseases, hypertension, ulcer, poor general health.
Emotional
Short term: Tiredness, anxiety, boredom, irritability, and depression, lack of concentration
low self-esteem, apathy.
Long terms: Depression, neurosis break down, suicide.
CCNs need to listen to their bodies and thoughtfully consider their sense of well-being.
Frequent personal assessment for signs of stress is important to longevity and satisfaction
in critical care nursing. Awareness of the early warning signs of stress can facilitate rapid
identification and swift intervention to enhance individual coping.
37
CCNs are vulnerable to burnout, which is the response to chronic emotional strain
extensively with other human beings, particularly when they are troubled, ill, or having
personal problems.
The condition of burnout renders the individual feeling resigned, ineffective, and hopeless
about working in such an environment. The behavior common in burnout include
absenteeism, anger, frustration, anxiety, and loss of commitment. The result of burnout is
that the employee either leaves the job or remains in the position functioning ineffectively.
(2, 13, 14, 25, 26)
Chemical dependency
Chemical dependency occurs among workers in every occupation. Nurses are
exposed to constant stress and human suffering. They also have easy access to narcotics
and other drugs. Although there are no reliable estimates of the number of nurses who
suffer from chemical dependency, the problem of chemical dependency is surfacing more
frequently. The costs to society of chemical dependency include increased use of health
insurance benefits, decreased productivity, increased absenteeism, poor patient relations,
reduced staff morale, poor judgment and increased mistakes or accidents. Mistakes or
accidents often lead to litigation and damage to the reputations of both the organization
and the nurse. Drugs that may be abused include cocaine, marijuana, alcohol, narcotics,
amphetamines, and tranquilizers. Nurses should be observant of colleagues who may
display signs of chemical dependency or impairment and should refer them to the peer
counseling program run by the nurses' association or employee assistance program at the
hospital.(2, 25)
Personality and coping characteristics of successful CCNs:
- Adventurous
- Detached ( based on defense mechanisms), which reduces anxiety level
- Strong capacity for coping and adaptation
- Hardiness: control, commitment, challenge, companionship
- Resiliency (bounces back): insight, independence, social support, and initiative.
(13, 27)

38
CONCLUSION
It has been established that those in the nursing profession are susceptible to a number of
Occupational hazards, many of which are avoidable and preventable while others are
inevitable, being parts of the everyday nursing duties. Nurses must pay attention for the
potential hazards they face and preventive strategies that are effective.
CCNs must examine the hazards in the critical care work environment. An awareness of
hazards and nurses perceptions of their causes and solutions set the stage for developing
appropriate occupational safety programs. Nurse with research skills and a familiarity with
the tasks, procedures, and physical environment of the critical care unit have an opportunity
to study and contribute to the understanding of occupational hazards and ways to prevent
them.
39
Previous studies
1. Chen-Yin Tung, Department of Health Promotion and Health Education, College of
Education, National Taiwan University, carried study on Occupational Hazards
Education for Nursing Staff through Web-Based Learning, Published: in 2014.
The study was a pre/post-test control group design. The subjects were nursing staff from
two hospitals in Taipei City, Taiwan. One hospital was the experimental group and the
other one was the control group. The study aimed to explore the efficiency of using
online education as an intervention measure to prevent occupational hazards in a clinical
nursing setting as well as to understand nursing staff’s experiences of occupational
injuries. The subjects were 320 female nursing staff from two hospitals in Taiwan.
The questionnaire results indicated that the subjects primarily experienced human factor
occupational hazards, as well as psychological and social hazards. Specifically, 73.1%
and 69.8% of the subjects suffered from poor sleep quality and low back pain. the
experimental group had higher post-test scores than the control group in knowledge.
The subjects of the experimental group and the control group did not show significant
differences in their attitudes and practices toward the prevention of occupational hazards.
A possible explanation for this result may be that the education website lacked an online
discussion forum, which could offer solutions to the problems encountered by the nursing
staff in the prevention of occupational hazards. (28)
2. Amosu.M. Department of Nursing, Igbinedion University, Okada, Nigeria 2011
Studied the Level of Knowledge Regarding Occupational Hazards among Nurses in
Abeokuta, Ogun State, Nigeria.
Descriptive survey was carried out to investigate the level of knowledge on the
predisposing factors to occupational hazards, among nurses in health facilities in Abeokuta,
Ogun state, Nigeria. The study population consisted of nurses of varying categories
working in ten public and two privately owned health facilities in five local government
areas of the state. The simple random sampling technique employed in selecting 1,200
respondents across the health facilities. A validated structured questionnaire developed.
The results revealed that 5.7% of the respondents were males, 94.3% were females,
40
four hundred and sixty-nine (39.1%) respondents have 1-10 years working experience
while 60.9% have spent 11 years and above in the nursing profession.
96.2% of the respondents knew that, the profession is prone to occupational hazards, and
as expressed by 88.6% of the respondents, back injury is the commonest hazard, followed
by neck and back pain as attested to by 84.8% of the nurses. The most prominent
predisposing factor was prolonged standing as viewed by 84.5% of the sample. (29)
3. Occupational Health and Safety issue Among Nurses in the Philippines:
Castro - A. B.2009. Studied the health and safety issues among nurses in Philippine. The
study was designed to gain preliminary insights into some of the occupational health and
safety problems faced by nurses in the Philippines.
He found that 38% of nurses reported being inadequately informed by employers about
workplace hazards. When asked to rank their top concerns, respondents reported acute
and chronic effects of stress and being overworked; a disabling back injury; and being
infected with a blood borne pathogen from a needle stick. These injuries and illnesses
appeared to be consequential not only for the nurse, but also for the workplace. About
23% reported missing 2 or more days in the past year due to a work-related injury or
illness, and 76% reported that unsafe working conditions interfered with the delivery of
quality nursing care.
Nurses in developed countries such as the United States may have safer working conditions
lesser than nurses in developing countries. This advantage may result from greater
economic resources and regulatory oversight that support quality occupational health and
safety protections. For example, in 1991, the U.S. Occupational Safety and Health
Administration (OSHA) promulgated the Blood borne Pathogen Standard to protect all
workers at risk for exposure to blood borne pathogens through sharps injuries or contact
with skin or mucous membranes (OSHA, 1991). In contrast, the Philippines has no
equivalent policy, even though the nursing profession is regulated by the Department of
Labor and Employment and the Department of Health. (30)

41
4. Study published in 2010 by Ticiani D. et al, Department of Nursing, University
of Brasilia
Studied occupational health hazards in ICU nursing staff Hospital de Base of the
Federal District, Was a descriptive cross-sectional study which was carried out with
nurses and nursing technicians at the ICU at the Hospital de Base, a public
institution located in Brasilia, Brazil. The study analyzed occupational health
hazards for Intensive Care Unit (ICU) nurses and nursing technicians, comparing
differences in the number and types of hazards which occur at the beginning and
end of their careers. The study population were 26 nurses and 96 nursing
technicians.
Results: The study found that the psychological and social hazard levels were
tolerable. Leg pains and sleep disturbance symptoms were at critical levels among
nurses; among nursing technicians, critical levels were detected for leg and back
pains. Concerning psychological hazards it may be verified that for both categories,
levels were satisfactory with regard to negative feelings (loss of self-confidence,
loss of self-control, feeling of emptiness, bitterness, feeling of defeat, crying for no
apparent reason, willingness to give everything up, long-lasting feeling of despair,
and negative image of oneself). A moderate level of sadness was identified among
nurses, being considered satisfactory for nursing technicians. The study concluded
that most of these professionals held more than one job to maintain family income
levels, as a consequence of working two shifts possibly provoking certain psycho-
emotional illnesses. (31)
5. Prevalence and risk factors of low back pain among nurses in a typical Nigerian
hospital
Sikuru Land Hanifa S, 2010 studied LBP among nurses, the objective of this study was to
determine the prevalence and risk factors of LBP among nurses in a typical Nigerian
Specialist Hospital. A cross-sectional study was designed to determine the prevalence and
risk factors for LBP among nurses in a typical Nigerian Hospital. A department-to-
department enquiry was conducted using a self-structured valid and reliable questionnaire.

42
The main results of that study: Four hundred and eight respondents (148 [36.27%] males
and 260 [63.73%] females) participated in the study. The 12-month prevalence of LBP
was 300 (73.53%). LBP was more prevalent among female nurses (68%) than the male
nurses (32%). It was also associated with occupational hazard and poor knowledge of
back care ergonomics. in the study LBP did not feature as a major cause of sickness
absence in the work place. The study concluded that poor back care ergonomics is the
major predisposing factor of LBP. (32)
6. Stress in nurses working in intensive care unit, Antonio Carlos, RN, Hospital
Israelita Albert Einstein, Doctoral student at São Paulo Federal University,
Brazil.
study aimed to identify the presence of stress in nurses working in intensive care units,
the stressing agents and symptoms associated to the nurses' perceptions of stress, and to
assess the correlation between the occurrence of stress, sources of stress, and symptoms
shown by the nurses. Seventy-five nurses took part in the study. The data were collected
from questionnaires. The study showed the presence of stress related to work
dissatisfaction, activities regarded as critical situations in intensive care units, symptoms
related to cardiovascular, digestive and musculoskeletal disorders. The study indicated
that there was a relation between the stress sources identified by the questionnaire of
critical situations with the levels of stress and general dissatisfaction with work.
The conclusion was that stress presents in nurses' activities in intensive care units,
related to characteristics of the health area itself, causing dissatisfaction and stress-related
symptoms. (33)
7. Occupational Health Hazards among Healthcare Workers in Kampala, Uganda
Rawlance Ndejjo et al. Department of Disease Control and Environmental Health, School
of Public Health, Makerere University, Kampala, Uganda.
Study published in 2015, assessed the occupational health hazards faced by healthcare
workers and the mitigation measures. A cross-sectional study conducted utilizing
43
quantitative data collection methods among 200 respondents who worked in eight major
health facilities in Kampala.
Results. Overall, 50.0% of respondents reported experiencing an occupational health
hazard. Among these, 39.5% experienced biological hazards while 31.5% experienced
nonbiological hazards. Predictors for experiencing hazards included not wearing the
necessary personal protective equipment (PPE), working overtime, job related pressures,
and working in multiple health facilities.
Among those that experienced nonbiological hazards, the majority experienced stress
(21.5%), physical, psychological, sexual, and/or verbal abuse (10.5%), and
musculoskeletal injuries (10.5%). The proportions of nonbiological hazards were higher
among females (male (26.3%) versus female (33.6%)), those older than 30 years (≤30 years
(23.3%) versus >30 years (38.2%)).
Thhe study concluded that interventions should be instituted to mitigate the hazards,
specifically PPE supply gaps, job related pressures, and complacence in adhering to
mitigation measures should be addressed. (34)
8. Knowledge and practices among registered nurses on occupational hazards in
Onandjokwe health district: Oshikoto region, Namibia 2015
By Julia Tuvadimbwa, MSC, public health, University of Namibia
The aim of the study was to determine the existing knowledge and practices of the
registered nurses and strategies that were in place to guide practice on occupational hazard
and safety in the Onandjokwe health district.
A quantitative research design utilizing a survey by means of questionnaires is used. The
population of the study were registered nurses in direct contact with patients (50 nurses).
The results indicated that a significant number of registered nurses have knowledge on
occupational hazards, although there were a few numbers which have insufficient
knowledge on occupational hazards. Population also were trying to practice occupational
safety but the restrictions such as non-availability of facilities prevented them from the
safety practices.
44
It seems that the majority of the respondents, that is 39 (76%) of the sample understood
occupational hazards as it was indicated in their responses. Six (6) 12% respondents have
only mentioned the types of occupational hazards instead of explaining the meaning.
Thirty seven (37) 74% respondents have indicated that they are exposed either through
handling of sharp instruments or equipment, lifting of patients, exposure to aggressive patients,
exposure to airborne diseases.
Nineteen 19 (38%) respondents indicated that they are aware of the content of the guidelines
on body mechanics. Twenty-eight 28 (56%) respondents were not aware of the content of the
body mechanics guideline.
All the respondents that were 50 (100%) indicated that they wash their hands on duty to prevent
or reduce cross infections.
Non-availability of facilities may also contribute to protective measures not to be used.
Sixteen (16) 32% responded that they do not use spectacles/goggles on duty
The researcher strongly recommended that the knowledge on occupational hazard and
safety among nurses should be improved through the following means:
- Registered nurses on a regular basis should attend training on occupational
hazards and safety.
- A well-trained occupational nurse should be appointed to educate health workers
on the prevention and management of occupational hazards. (35)
9. Anwar Abbas Ahmed studied occupational hazards affecting dental manpower in
Khartoum state, 2004.
The data of his study collected through two methods, interviews and observation, analysis
of the results revealed the high knowledge of the respondents about biological hazards
(95.9%), ( 94.1%) about physical hazards, (77.7% ) about chemical hazards and( 66.7%)
psychological hazards. The acceptance of protective tools and sterilization is poor (61.9%
& 55.6% respectively).
The results may indicate that, the knowledge of the dental manpower included in the study
about professional hazards is not reflected as behavior. The following recommendation is
suggested:
1- Dental manpower including dentists, assistants and nurses should be informed and
reminded about occupational hazards and mean of avoiding them.
45
2- Continuous surveillance and the inception of proper protective measures against
occupational hazards need to be arranged, through frequent check visits by
organizing licensing periodic.
3- Education of professional and generate public awareness. (36 )
10. Study done by (the researcher), for a complementary program of MSc in nursing
It was a descriptive, cross-sectional study carried during April, May and June 2011,
aimed to investigate occupational hazards that facing nurses in critical care areas, the Study
subjects were 66 nurses working in Ahmed Gasim Hospital Cardiac Surgery and Renal
Transplant Center areas for more than one year. Questionnaire and checklist were used to
assess occupational hazards among critical care nurses and preventive measures that
actually used. Respondents mentioned high level of knowledge (90%) about infectious,
stress and musculoskeletal disorders.
The results revealed that low backache, eye fatigue, muscles pain, irritability and upset
stomach occurred to more than 50% of the participants, 6% HBV, 1.5% HCV and 4.5%
TB. International measures are poorly applied. Shoes, covering, face shield and plastic
gown are not available. Participants appropriately use available protective measures.
46
Chapter (3)
Research Methodology
Research Methodology
Study design:
This study was pre - post-intervention, one group, hospital-based study carried out during
2013-2016.
Study area:

47
This study was carried out at critical care settings (Intensive care units), in Khartoum
state governmental hospitals.
In the following five hospitals:
• Khartoum teaching hospital ( one postoperative ICU)
• Omdurman teaching hospital (CCU, medical ICU, surgical ICU)
• Khartoum North teaching hospital (Bahari) (ICU A, ICU B)
• Elshaab teaching hospital (ICCU, ICU, Asthma ICU)
• Ahmed Gasim hospital - cardiac and renal center (CCU, ICU, RR)
The study population:
All nurses working in CCU, ICU and RR, in Khartoum state (governmental hospitals).
Sample size and sampling technique:
Sampling technique:
Total coverage of all population
The sample size:
Two hundred and fifty (250) nurses.
The participants’ number (who agreed to participate):
Two hundred (200) nurses
The rest of the population 50 CCNs dropped because of an individual and institutional
causes.
Number of staff in all study areas is greater than this study sample, because about hundred
jobs were covered with same CCNs, in mean of double shift work.
Hospitals CCNs total
number
Participants
number
CCNs Jobs/
hospital
Khartoum hospital 40 30 40
Omdurman hospital 50 45 55
Khartoum north hospital 45 30 52
Elshaab hospital 55 40 108
Ahmed Gasim hospital 60 55 102

48
Total 250 200 357
Interventions:
After the first questionnaire administered with participants, an educational program was
conducted by:
1. Lectures in hospital conference hall contain:
- Purposes of occupational health – occupational hazards types, causes, and preventive
methods. – Infection control universal precautions. – Stress and its effects – training on
relaxation exercises technique – health education session about personality, and coping
methods to gain success in life despite this stressful job.
(same contents of lecture taught in other educational types)
2. Discussions in the prescribed units as sitting group’s discussion
3. Direct individual educational session.
(Manual of the educational program hard copy and International datasheets on OHs for
ICU nurse of ILO, distributed to all nurses in critical care areas)
The study tools:
1. An interviewing structured closed ended questionnaire was used, developed by
the researcher to identify nurses’ knowledge about possible occupational hazard,
causes, and prevention measures in intensive care units. The questionnaire composed of
seven sessions:
a. background data about participants
b. knowledge of meaning and types of OHs. c. knowledge of OHs causes
d. knowledge of OHs preventive methods. e. knowledge of universal precaution
f. provision of PPE g. coping characteristics of CCNs to gain success.
2. Observational Checklist (Adapted from CDC & AACCN procedure book)
Prepared to evaluate nurses' practice regarding the suitable uses of universal preventive
measures of occupational hazards.
3. Interview with key persons (I.K.P), structured and guided by researcher with
Hospital matron for discussion of:

49
- Causes behind unavailability of personal protective equipment and causes of gaps
in supply of that equipment.
- Availability of hand washing sinks, soaps and germicides
- Pre-employment education about safety measures.
- Assigned OHN in hospital.
Study variables:
Dependent variable
Occupational hazards in critical care areas.
Independent variables
- Efficiency of educational program on CCNs knowledge about OHs
- Knowledge about occupational hazards types, and causes.
- Knowledge about prevention and mitigation of OHs.
- Availability of PPE in CC areas
The data analysis Data were assessed, coded, managed, and analyzed by Statistical Package of Social
studies (SPSS), were presented in forms of frequency figures and table for cross
tabulation. Significance differences of results were tested by Pearson’s chi squire, the p
value was accepted below 0.05.
Ethical Considerations
Many formalities were done before starting data collection, ethical approvals to carry out
the study was obtained from Ribaat National University, to curative medicine
administration, Khartoum state ministry of health, formal letter was sent to each hospital
general director, which was directed to hospital’s research director and hospital’s

50
matron, followed by letter to critical area nursing director then each CCN informed
verbally by researcher with mentioning of information confidentiality.
Study Limitations
The limitations of this study were:
- One hospital was not included because there were obstacles from hospital
managers’ side to carry the study in their area (Ibrahim Malik Hospital).
- In (CCU, Elshaab hospital), the head of nursing staff refused to do this study in
her unit; she told this time consuming program.

51
The Results
Chapter (4)
Results

52
n =200
Figure 1. Reflects respondents distribution in study areas
Figure 2. Reflects respondents distribution in critical care settings types
27.5%
22.5%
20%
15%15%
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
0
10
20
30
40
50
60HOSPITALS
ICU CCU RR
84.0%
12.5% 3.0%
CC AREAS
53
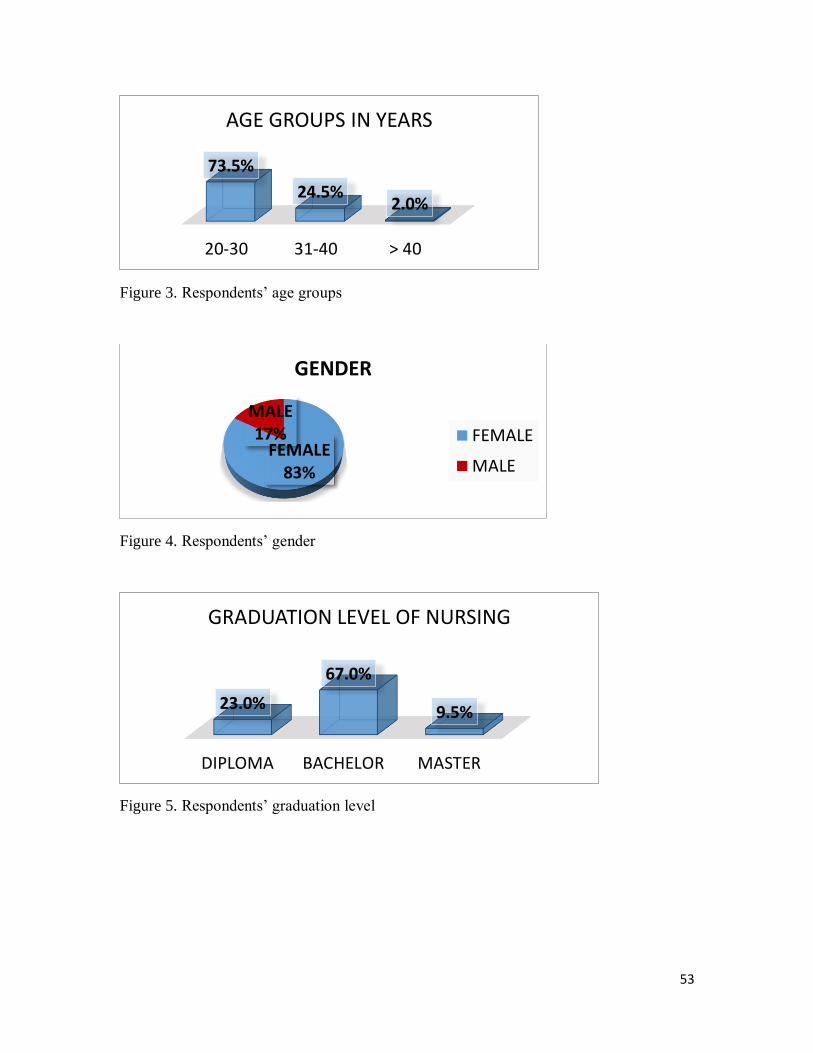
Figure 3. Respondents’ age groups
Figure 4. Respondents’ gender
Figure 5. Respondents’ graduation level
20-30 31-40 > 40
73.5%
24.5%2.0%
AGE GROUPS IN YEARS
FEMALE83%
MALE17%
GENDER
FEMALE
MALE
DIPLOMA BACHELOR MASTER
23.0%
67.0%
9.5%
GRADUATION LEVEL OF NURSING

54
Figure 6. CCNs in morning shift were more than afternoon/night shift
Figure 7. Shows participants’ experience length in years
MORNING
54%
A/N46%
MAIN WORKING SHIFT
MORNING A/N
< 1 YR 1-5 YRS > 5 YRS
24.0%
43.5%
32.0%
THE LENGTH OF EXPERIENCE IN YEARS
55
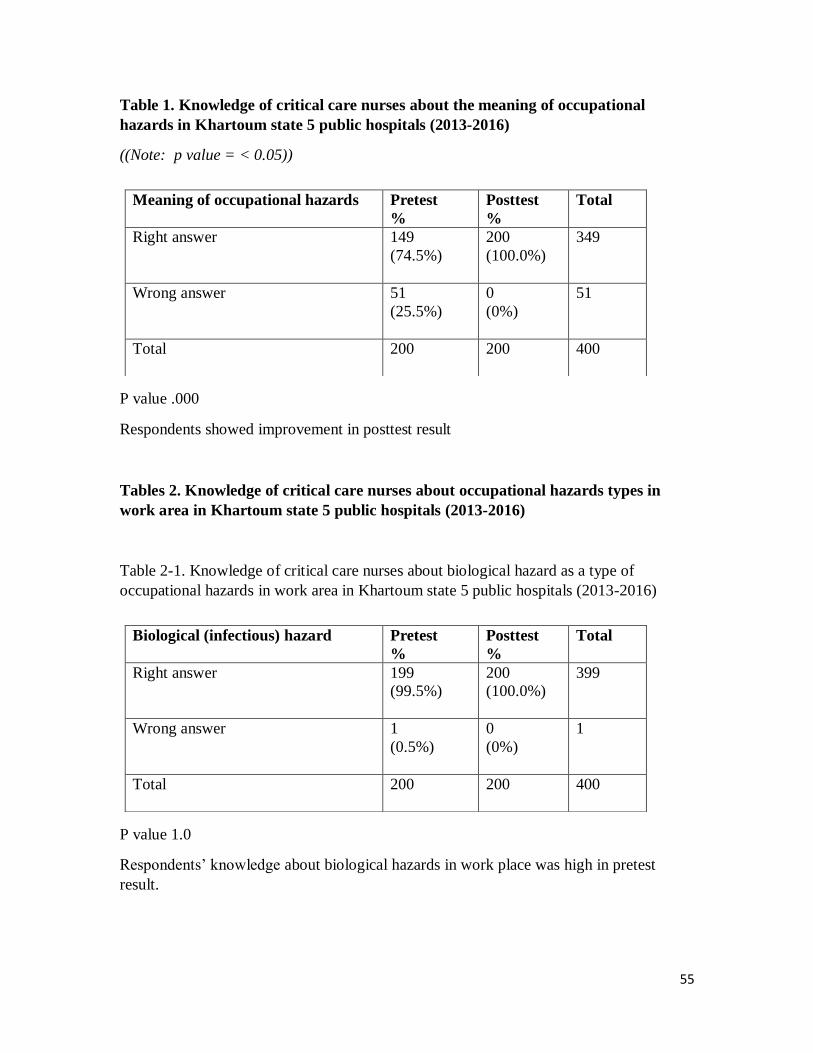
Table 1. Knowledge of critical care nurses about the meaning of occupational
hazards in Khartoum state 5 public hospitals (2013-2016)
((Note: p value = < 0.05))
P value .000
Respondents showed improvement in posttest result
Tables 2. Knowledge of critical care nurses about occupational hazards types in
work area in Khartoum state 5 public hospitals (2013-2016)
Table 2-1. Knowledge of critical care nurses about biological hazard as a type of
occupational hazards in work area in Khartoum state 5 public hospitals (2013-2016)
P value 1.0
Respondents’ knowledge about biological hazards in work place was high in pretest
result.
Meaning of occupational hazards Pretest
%
Posttest
%
Total
Right answer 149
(74.5%)
200
(100.0%)
349
Wrong answer 51
(25.5%)
0
(0%)
51
Total 200
200 400
Biological (infectious) hazard Pretest
%
Posttest
%
Total
Right answer 199
(99.5%)
200
(100.0%)
399
Wrong answer 1
(0.5%)
0
(0%)
1
Total 200
200 400
56
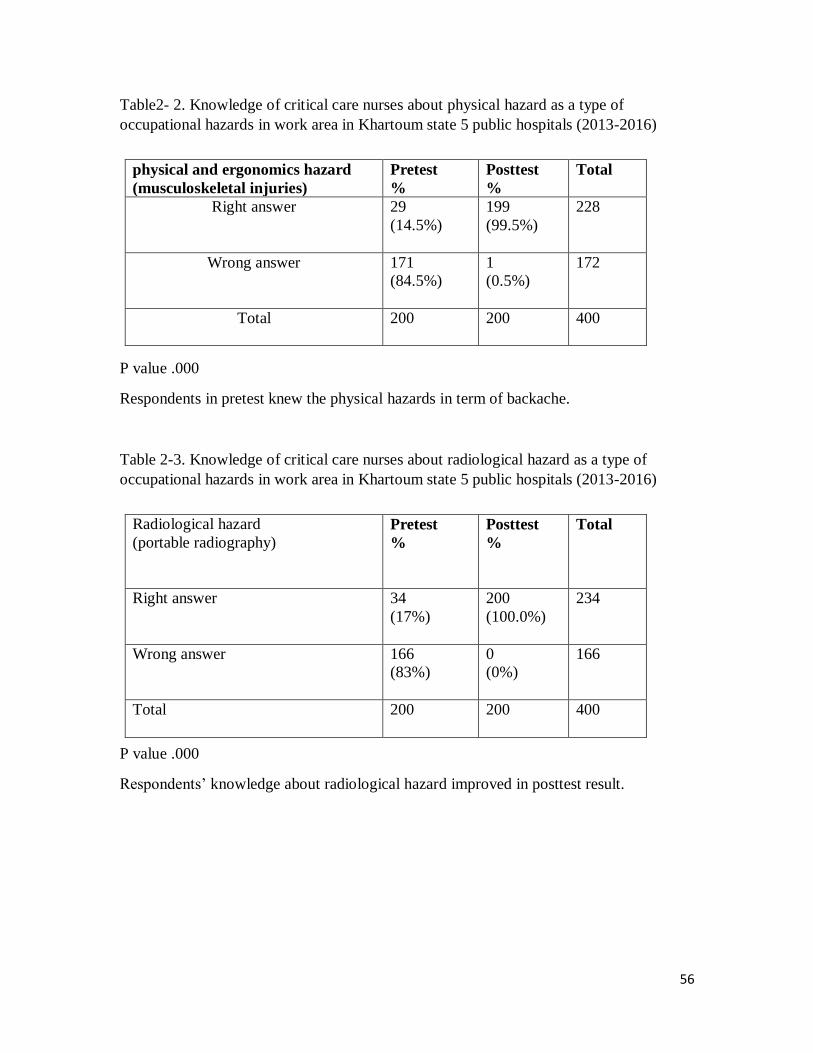
Table2- 2. Knowledge of critical care nurses about physical hazard as a type of
occupational hazards in work area in Khartoum state 5 public hospitals (2013-2016)
P value .000
Respondents in pretest knew the physical hazards in term of backache.
Table 2-3. Knowledge of critical care nurses about radiological hazard as a type of
occupational hazards in work area in Khartoum state 5 public hospitals (2013-2016)
P value .000
Respondents’ knowledge about radiological hazard improved in posttest result.
physical and ergonomics hazard
(musculoskeletal injuries)
Pretest
%
Posttest
%
Total
Right answer 29
(14.5%)
199
(99.5%)
228
Wrong answer 171
(84.5%)
1
(0.5%)
172
Total 200
200 400
Radiological hazard
(portable radiography)
Pretest
%
Posttest
%
Total
Right answer 34
(17%)
200
(100.0%)
234
Wrong answer 166
(83%)
0
(0%)
166
Total 200
200 400
57
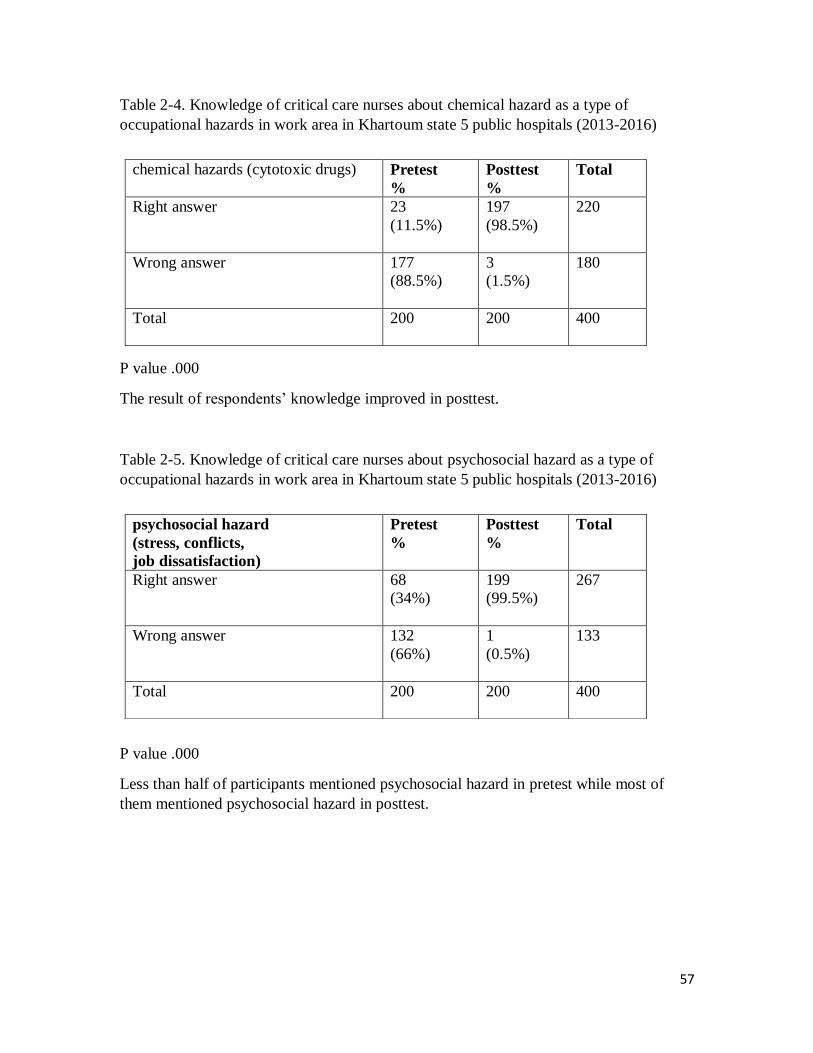
Table 2-4. Knowledge of critical care nurses about chemical hazard as a type of
occupational hazards in work area in Khartoum state 5 public hospitals (2013-2016)
P value .000
The result of respondents’ knowledge improved in posttest.
Table 2-5. Knowledge of critical care nurses about psychosocial hazard as a type of
occupational hazards in work area in Khartoum state 5 public hospitals (2013-2016)
P value .000
Less than half of participants mentioned psychosocial hazard in pretest while most of
them mentioned psychosocial hazard in posttest.
chemical hazards (cytotoxic drugs)
Pretest
%
Posttest
%
Total
Right answer 23
(11.5%)
197
(98.5%)
220
Wrong answer 177
(88.5%)
3
(1.5%)
180
Total 200
200 400
psychosocial hazard
(stress, conflicts,
job dissatisfaction)
Pretest
%
Posttest
%
Total
Right answer 68
(34%)
199
(99.5%)
267
Wrong answer 132
(66%)
1
(0.5%)
133
Total 200
200 400
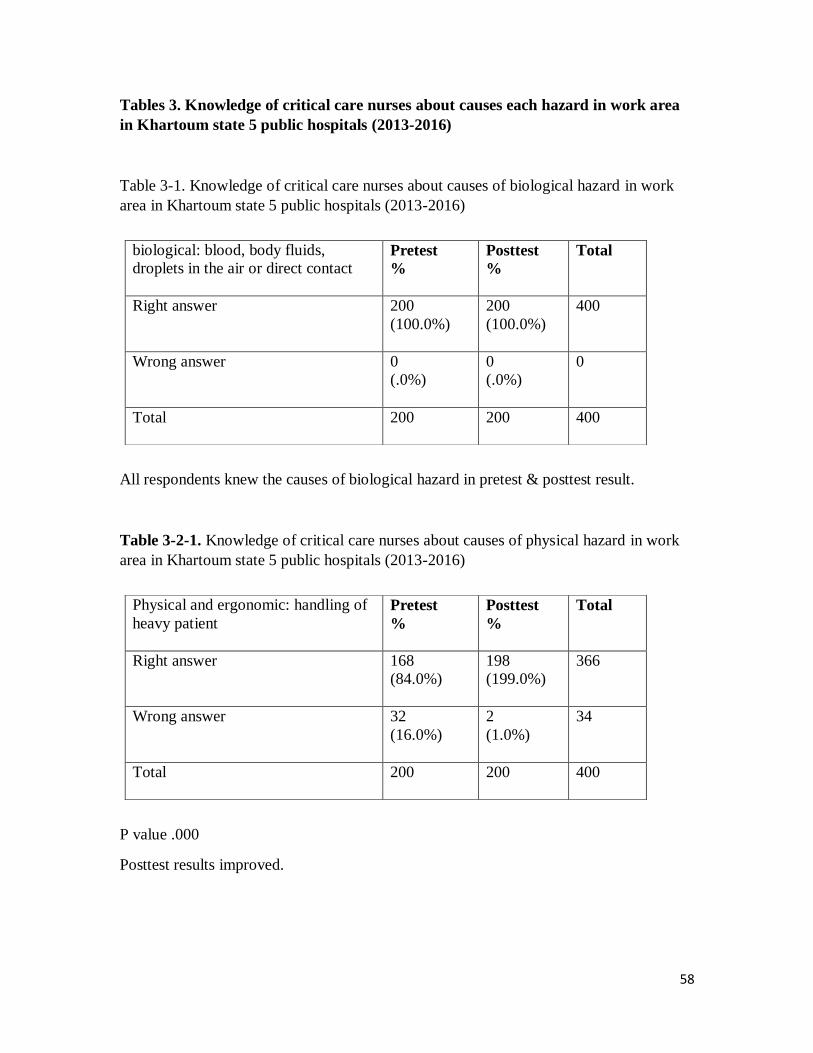
58
Tables 3. Knowledge of critical care nurses about causes each hazard in work area
in Khartoum state 5 public hospitals (2013-2016)
Table 3-1. Knowledge of critical care nurses about causes of biological hazard in work
area in Khartoum state 5 public hospitals (2013-2016)
All respondents knew the causes of biological hazard in pretest & posttest result.
Table 3-2-1. Knowledge of critical care nurses about causes of physical hazard in work
area in Khartoum state 5 public hospitals (2013-2016)
P value .000
Posttest results improved.
biological: blood, body fluids,
droplets in the air or direct contact
Pretest
%
Posttest
%
Total
Right answer 200
(100.0%)
200
(100.0%)
400
Wrong answer 0
(.0%)
0
(.0%)
0
Total 200
200 400
Physical and ergonomic: handling of
heavy patient
Pretest
%
Posttest
%
Total
Right answer 168
(84.0%)
198
(199.0%)
366
Wrong answer 32
(16.0%)
2
(1.0%)
34
Total 200
200 400
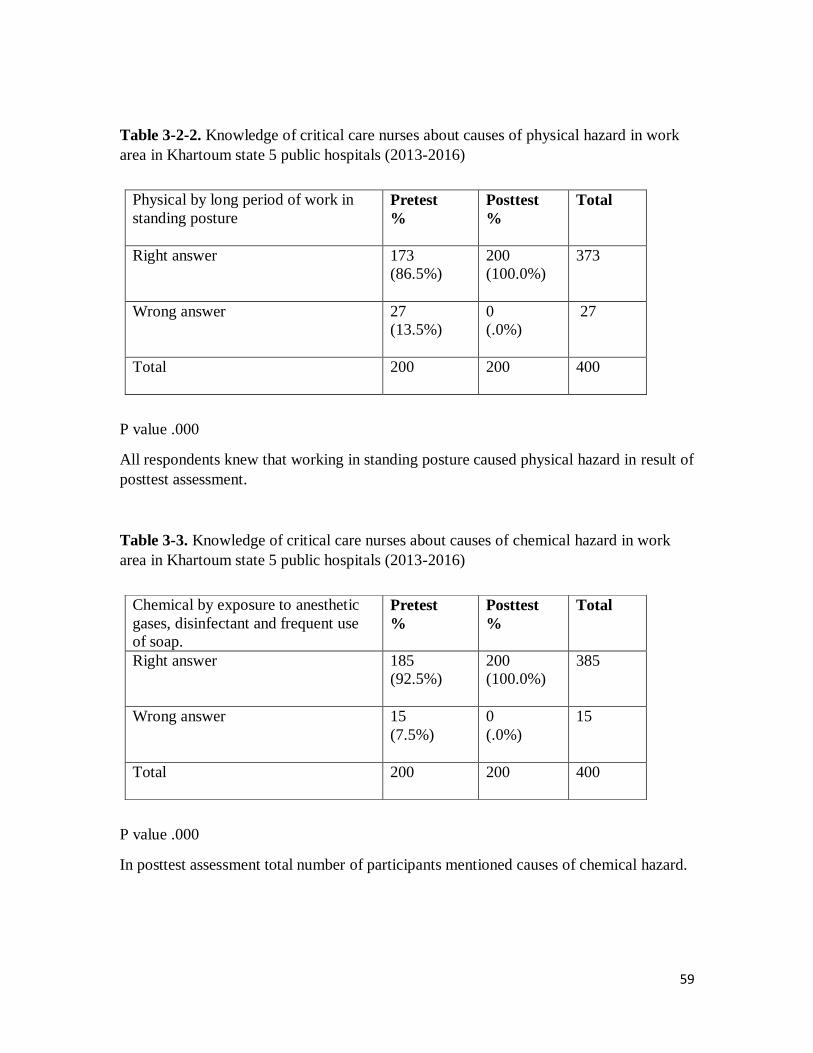
59
Table 3-2-2. Knowledge of critical care nurses about causes of physical hazard in work
area in Khartoum state 5 public hospitals (2013-2016)
P value .000
All respondents knew that working in standing posture caused physical hazard in result of
posttest assessment.
Table 3-3. Knowledge of critical care nurses about causes of chemical hazard in work
area in Khartoum state 5 public hospitals (2013-2016)
P value .000
In posttest assessment total number of participants mentioned causes of chemical hazard.
Physical by long period of work in
standing posture
Pretest
%
Posttest
%
Total
Right answer 173
(86.5%)
200
(100.0%)
373
Wrong answer 27
(13.5%)
0
(.0%)
27
Total 200
200 400
Chemical by exposure to anesthetic
gases, disinfectant and frequent use
of soap.
Pretest
%
Posttest
%
Total
Right answer 185
(92.5%)
200
(100.0%)
385
Wrong answer 15
(7.5%)
0
(.0%)
15
Total 200
200 400

60
Table 3-4. Knowledge of critical care nurses about causes of radiological hazard in work
area in Khartoum state 5 public hospitals (2013-2016)
P value .000
Vast majority of respondents answered rightly in posttest assessment.
Table 3-5. Knowledge of critical care nurses about causes of psychosocial hazard in
work area in Khartoum state 5 public hospitals (2013-2016)
P value .030
Causes of this hazard known by most participants in first assessment.
Radiological by portable radiography
Pretest
%
Posttest
%
Total
Right answer 179
(89.5%)
199
(99.5%)
378
Wrong answer 21
(10.5%)
1
(0.5%)
22
Total 200
200 400
Psychosocial by stress, conflict and
job dissatisfaction
Pretest
%
Posttest
%
Total
Right answer 194
(97.0%)
200
(100.0%)
394
Wrong answer 6
(3.0%)
0
(.0%)
6
Total 200
200 400

61
Table 4. Knowledge of critical care nurses about preventive measures that mitigate
occupational hazards in Khartoum state, 5 public hospitals (2013-2016)
Table 4-1-1. Knowledge of critical care nurses about preventive measures that mitigate
biological hazard in Khartoum state, 5 public hospitals (2013-2016)
P value 0.499
High knowledge of participants about prevention by using of personal protective
equipment in the two parts of assessment.
Table 4-1-2. Knowledge of critical care nurses about preventive measures that mitigate
biological hazard in Khartoum state, 5 public hospitals (2013-2016)
P value .000
In pretest, about half of participants mentioned prevention by hand washing while vast
majority mentioned it in posttest.
Prevention of biological hazards by
uses of PPE Pretest
%
Posttest
%
Total
Right answer 198
(99%)
200
(100.0%)
398
Wrong answer 2
(1%)
0
(.0%)
2
Total 200
200 400
Prevention of biological hazards by
hand washing
Pretest
%
Posttest
%
Total
Right answer 99
(49.5%)
199
(99.5%)
298
Wrong answer 101
(50.5%)
1
(0.5%)
102
Total 200
200 400

62
Table 4-1-3. Knowledge of critical care nurses about preventive measures that mitigate
biological hazard in Khartoum state, 5 public hospitals (2013-2016)
P value .000
Improvement in posttest results about prevention of biological hazard by uses of
germicide.
Table 4-1-4. Knowledge of critical care nurses about preventive measures that mitigate
biological hazard in Khartoum state, 5 public hospitals (2013-2016)
P value .000
Less than quarter of respondents mentioned the right answer in pretest while most of
them mentioned the right answer in posttest.
Prevention of biological hazards by
uses of effective germicide
Pretest
%
Posttest
%
Total
Right answer 13
(6.5%)
183
(91.5%)
196
Wrong answer 187
(93.5%)
17
(8.5%)
204
Total 200
200 400
Prevention of biological hazards by
proper handling and disposal of sharp
objects
Pretest
%
Posttest
%
Total
Right answer 32
(16%)
196
(98%)
228
Wrong answer 168
(84%)
4
(2%)
172
Total 200
200 400

63
Table 4-2-1. Knowledge of critical care nurses about preventive measures that mitigate
physical hazards in Khartoum state, 5 public hospitals (2013-2016)
P value .000
Posttest result improvement was noticed.
Table 4-2-2. Knowledge of critical care nurses about preventive measures that mitigate
physical hazards in Khartoum state, 5 public hospitals (2013-2016)
P value .000
Respondents’ knowledge was improved in posttest results.
Prevention of physical hazards by
maintain good posture
Pretest
%
Posttest
%
Total
Right answer 162
(81%)
199
(99.5%)
361
Wrong answer 38
(19%)
1
(.5%)
39
Total 200
200 400
Prevention of physical hazards by use
of mechanical device for lifting
Pretest
%
Posttest
%
Total
Right answer 15
(7.5%)
179
(98%)
194
Wrong answer 185
(92.5%)
21
(10.5%)
206
Total 200
200 400
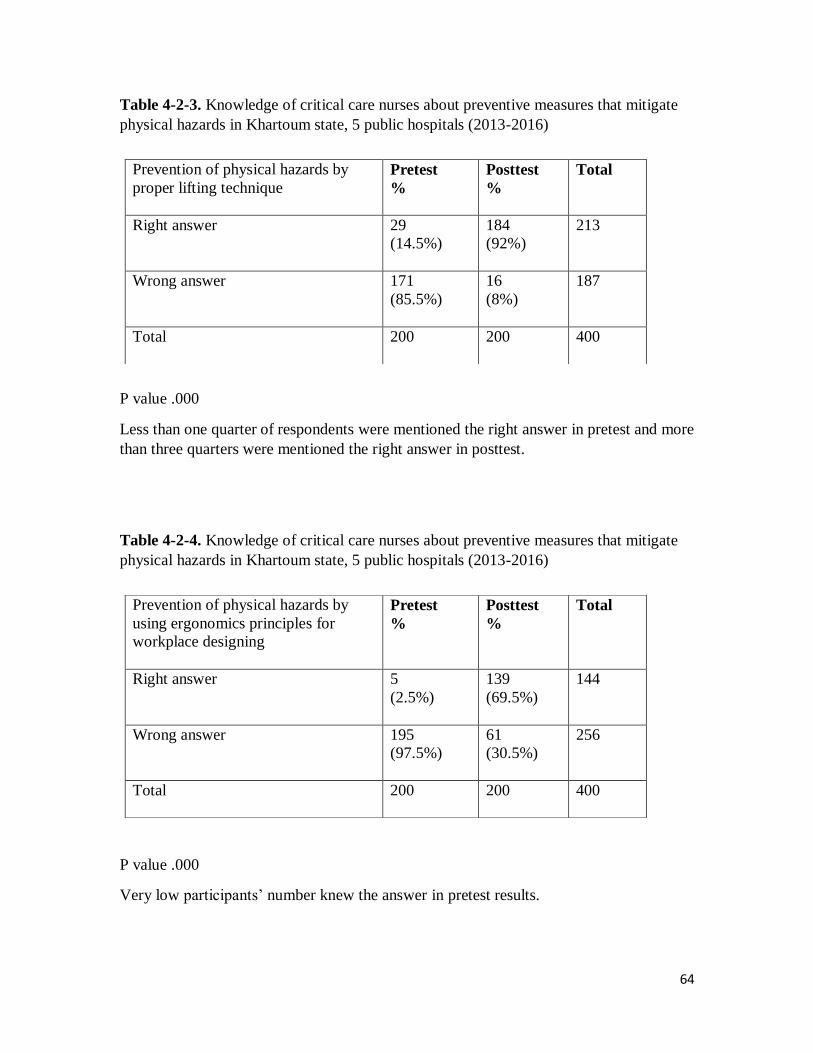
64
Table 4-2-3. Knowledge of critical care nurses about preventive measures that mitigate
physical hazards in Khartoum state, 5 public hospitals (2013-2016)
P value .000
Less than one quarter of respondents were mentioned the right answer in pretest and more
than three quarters were mentioned the right answer in posttest.
Table 4-2-4. Knowledge of critical care nurses about preventive measures that mitigate
physical hazards in Khartoum state, 5 public hospitals (2013-2016)
P value .000
Very low participants’ number knew the answer in pretest results.
Prevention of physical hazards by
proper lifting technique
Pretest
%
Posttest
%
Total
Right answer 29
(14.5%)
184
(92%)
213
Wrong answer 171
(85.5%)
16
(8%)
187
Total 200
200 400
Prevention of physical hazards by
using ergonomics principles for
workplace designing
Pretest
%
Posttest
%
Total
Right answer 5
(2.5%)
139
(69.5%)
144
Wrong answer 195
(97.5%)
61
(30.5%)
256
Total 200
200 400

65
Table 4-2-5. Knowledge of critical care nurses about preventive measures that mitigate
physical hazards in Khartoum state, 5 public hospitals (2013-2016)
P value .000
The respondents’ posttest results were improved.
Table 5-2-6. Knowledge of critical care nurses about preventive measures that mitigate
physical hazards in Khartoum state, 5 public hospitals (2013-2016)
P value .000
Posttest results were showed noticeable improvement.
Prevention of physical hazards by
adequate staffing
Pretest
%
Posttest
%
Total
Right answer 55
(27.5%)
181
(90.5%)
236
Wrong answer 145
(72.5%)
19
(9.5%)
164
Total 200
200 400
Prevention of physical hazards by
exercise
Pretest
%
Posttest
%
Total
Right answer 6
(3%)
186
(93%)
192
Wrong answer 194
(97%)
14
(7%)
208
Total 200
200 400

66
Table 4-3. Knowledge of critical care nurses about preventive measures that mitigate
chemical hazards in Khartoum state, 5 public hospitals (2013-2016)
P value .000
Most of participants knew how they could prevent chemical hazards in first assessment
results. `
Table 4-4-1. Knowledge of critical care nurses about preventive measures that mitigate
radiological hazards in Khartoum state, 5 public hospitals (2013-2016)
P value .000
Noticeable elevation in posttest values.
Prevention of chemical hazards by
adherence to body substance isolation
Pretest
%
Posttest
%
Total
Right answer 186
(93%)
199
(99.5%)
385
Wrong answer 14
(7%)
1
(.5%)
15
Total 200
200 400
Prevention of radiological hazards by
time
Pretest
%
Posttest
%
Total
Right answer 6
(3%)
192
(96%)
198
Wrong answer 194
(97%)
8
(4%)
202
Total 200
200 400

67
Table 4-4-2. Knowledge of critical care nurses about preventive measures that mitigate
radiological hazards in Khartoum state, 5 public hospitals (2013-2016)
P value .000
All respondents mentioned the right answer in posttest
Table 4-4-3. Knowledge of critical care nurses about preventive measures that mitigate
radiological hazards in Khartoum state, 5 public hospitals (2013-2016)
P value .000
Vast majority of respondents gained the knowledge of radiation prevention by shielding
in posttest results.
Prevention of radiological hazards by
distance
Pretest
%
Posttest
%
Total
Right answer 163
(81.5%)
200
(100.0%)
363
Wrong answer 37
(18.5%)
0
(.0%)
37
Total 200
200 400
Prevention of radiation hazards by
shielding
Pretest
%
Posttest
%
Total
Right answer 68
(34%)
199
(99.5%)
267
Wrong answer 132
(66%)
1
(.5%)
133
Total 200
200 400
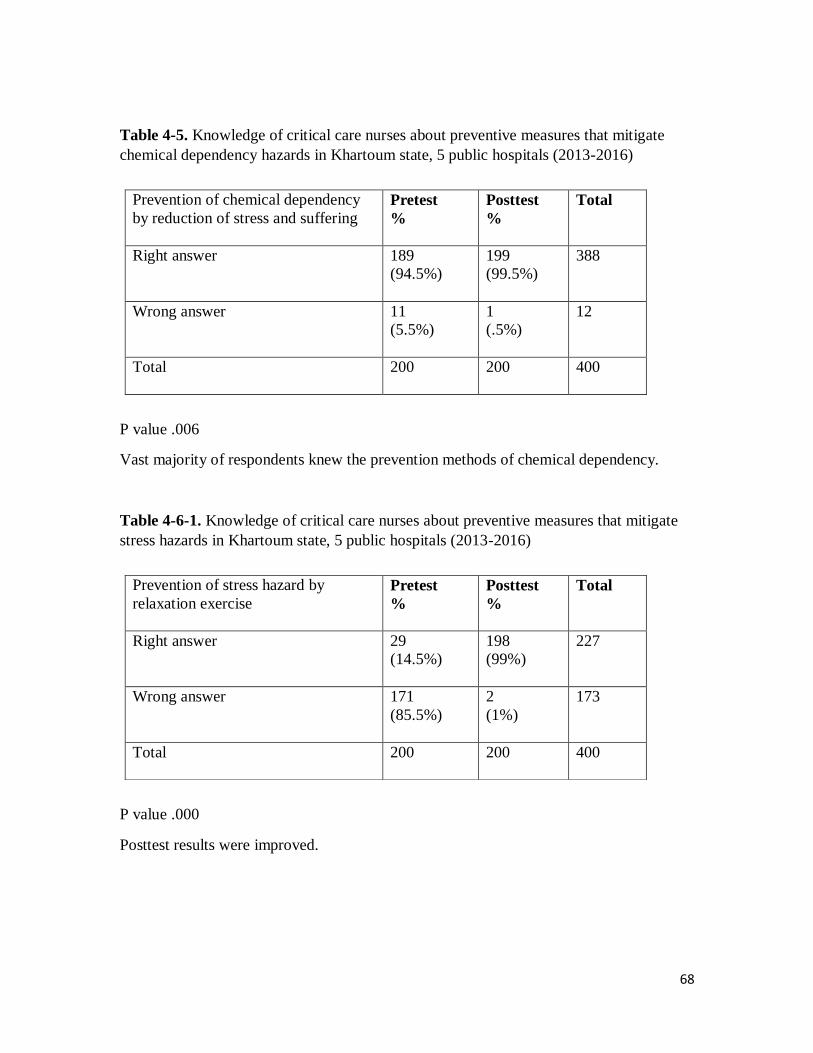
68
Table 4-5. Knowledge of critical care nurses about preventive measures that mitigate
chemical dependency hazards in Khartoum state, 5 public hospitals (2013-2016)
P value .006
Vast majority of respondents knew the prevention methods of chemical dependency.
Table 4-6-1. Knowledge of critical care nurses about preventive measures that mitigate
stress hazards in Khartoum state, 5 public hospitals (2013-2016)
P value .000
Posttest results were improved.
Prevention of chemical dependency
by reduction of stress and suffering
Pretest
%
Posttest
%
Total
Right answer 189
(94.5%)
199
(99.5%)
388
Wrong answer 11
(5.5%)
1
(.5%)
12
Total 200
200 400
Prevention of stress hazard by
relaxation exercise
Pretest
%
Posttest
%
Total
Right answer 29
(14.5%)
198
(99%)
227
Wrong answer 171
(85.5%)
2
(1%)
173
Total 200
200 400

69
Table 4-6-2. Knowledge of critical care nurses about preventive measures that mitigate
stress hazards in Khartoum state, 5 public hospitals (2013-2016)
P value .000
Respondents gained a noticeable knowledge evidenced by elevation in posttest results.
Table 4-6-3. Knowledge of critical care nurses about preventive measures that mitigate
stress hazards in Khartoum state, 5 public hospitals (2013-2016)
P value .000
Social support as prevention method of stress in pretest was known by less than one
quarter of respondents.
Prevention of stress hazards by
coping and adaptation
Pretest
%
Posttest
%
Total
Right answer 89
(44.5 %)
199
(99.5%)
288
Wrong answer 111
(55.5%)
1
(.5%)
112
Total 200
200 400
Prevention of stress hazards by social
support
Pretest
%
Posttest
%
Total
Right answer 34
(17%)
195
(97.5%)
229
Wrong answer 166
(83%)
5
(2.5%)
171
Total 200
200 400

70
Tables 5. Knowledge of critical care nurses about the component of universal
precautions that prevent infectious hazards in Khartoum state, 5 public hospitals
(2013-2016)
Tables 5-1. Knowledge of critical care nurses about hand washing as one of the
component of universal precautions that prevent infectious hazards in Khartoum state, 5
public hospitals (2013-2016)
P value .000
In Posttest evaluation, all respondents mentioned the right answer.
Table 5-2. Knowledge of critical care nurses about PPE as a component of universal
precautions that prevent infectious hazards in Khartoum state, 5 public hospitals (2013-
2016)
P value .000
Noticeable improvement was seen in posttest result.
Hand washing as one of universal
precautions
Pretest
%
Posttest
%
Total
Right answer 69
(34.5%)
200
(100.0%)
269
Wrong answer 131
(65.5%)
0
(.0%)
131
Total 200
200 400
Personal protective equipment as one
of universal precautions Pretest
%
Posttest
%
Total
Right answer 86
(43%)
200
(100.0%)
286
Wrong answer 114
(57%)
0
(.0%)
114
Total 200
200 400

71
Table 5-3. Knowledge of critical care nurses about preventing sharp injuries as a
component of universal precautions that prevent infectious hazards in Khartoum state, 5
public hospitals (2013-2016)
P value .000
Less than one quarter from the participants in the first assessment knew the right answer
while vast majority of them in posttest answered correctly.
Table 5-4. Knowledge of critical care nurses about aseptic technique as a component of
universal precautions that prevent infectious hazards in Khartoum state, 5 public hospitals
(2013-2016)
P value .000
The different between two assessments values was clear.
Preventing and managing sharp
injuries as one of universal
precautions
Pretest
%
Posttest
%
Total
Right answer 16
(8%)
198
(99%)
214
Wrong answer 184
(92%)
2
(1.0%)
186
Total 200
200 400
Aseptic technique as one of
universal precautions
Pretest
%
Posttest
%
Total
Right answer 6
(3%)
196
(98.0%)
202
Wrong answer 194
(97%)
4
(4%)
198
Total 200
200 400

72
Table 5-5. Knowledge of critical care nurses about isolation as a component of universal
precautions that prevent infectious hazards in Khartoum state, 5 public hospitals (2013-
2016)
P value .000
Knowledge status of participants elevated in posttest evaluation.
Table 5- 6. Knowledge of critical care nurses about staff health as a component of
universal precautions that prevent infectious hazards in Khartoum state, 5 public hospitals
(2013-2016)
P value .000
Pretest value was very low and posttest value increased.
Isolation as one of universal
precautions
Pretest
%
Posttest
%
Total
Right answer 11
(5.5%)
195
(97.5%)
206
Wrong answer 189
(94.5%)
5
(2.5%)
194
Total 200
200 400
Staff health as one of universal
precautions
Pretest
%
Posttest
%
Total
Right answer 3
(1.5%)
190
(95.5%)
193
Wrong answer 197
(98.5%)
10
(5.0%)
207
Total 200
200 400

73
Table 5-7. Knowledge of critical care nurses about linen handling as a component of
universal precautions that prevent infectious hazards in Khartoum state, 5 public hospitals
(2013-2016)
P value .000
Pretest value was very low and posttest value was improved.
Table 5-8. Knowledge of critical care nurses about waste disposal as a component of
universal precautions that prevent infectious hazards in Khartoum state, 5 public hospitals
(2013-2016)
P value .000
Small number of participants had the knowledge in pretest while in posttest participants’
number became bigger.
Linen handling and disposal as one
of universal precautions
Pretest
%
Posttest
%
Total
Right answer 2
(1%)
191
(95.5%)
193
Wrong answer 198
(99%)
9
(4.5%)
207
Total 200
200 400
Waste disposal as one of universal
precautions
Pretest
%
Posttest
%
Total
Right answer 6
(3%)
188
(94%)
194
Wrong answer 194
(97%)
12
(6%)
206
Total 200
200 400

74
Table 5-9. Knowledge of critical care nurses about spillage of body fluid care as a
component of universal precautions that prevent infectious hazards in Khartoum state, 5
public hospitals (2013-2016)
P value .000
Improvement in posttest evaluation was clearly seen.
Table 5-10. Knowledge of critical care nurses about environmental cleaning as a
component of universal precautions that prevent infectious hazards in Khartoum state, 5
public hospitals (2013-2016)
P value .000
More than three quarters of participants knew the right answer in second test.
Spillage of body fluid care as one of
universal precautions
Pretest
%
Posttest
%
Total
Right answer 2
(1%)
182
(91%)
184
Wrong answer 198
(99%)
18
(9%)
216
Total 200
200 400
Environmental cleaning as one of
universal precautions
Pretest
%
Posttest
%
Total
Right answer 15
(7.5%)
186
(93%)
201
Wrong answer 185
(92.5%)
14
(7.0%)
199
Total 200
200 400

75
Table 5-11. Knowledge of critical care nurses about risk management as a component of
universal precautions that prevent infectious hazards in Khartoum state, 5 public hospitals
(2013-2016)
P value .000
Improvement in participants’ posttest evaluation was clearly seen.
Table 6. Personal protective equipment availability in critical care areas in
Khartoum state, 5 public hospitals (2013-2016)
Table 6-1. Face mask availability in critical care areas in Khartoum state, 5 public
hospitals (2013-2016)
P value .889
Participants’ answers about availability of facemasks showed small changes in the second
assessment results.
Risk management and assessment
as one of universal precautions
Pretest
%
Posttest
%
Total
Right answer 2
(1%)
174
(87%)
176
Wrong answer 198
(99%)
26
(13%)
224
Total 200
200 400
Face mask availability Pretest
%
Posttest
%
Total
available 169
(84.5%)
171
(85.5%)
340
Not available 31
(15.5%)
29
(14.5%)
60
Total 200
200 400

76
Table 6-2. Disposable gloves availability in critical care areas in Khartoum state, 5
public hospitals (2013-2016)
Table 6-3. Plastic gown availability in critical care areas in Khartoum state, 5 public
hospitals (2013-2016)
P value 1.000
Plastic gowns available in one unit from the study areas.
Table6-4. Safety glasses availability in critical care areas in Khartoum state, 5 public
hospitals (2013-2016)
Disposable gloves availability Pretest
%
Posttest
%
Total
available 200
(100.0%)
200
(100.0%)
400
Not available 0
(.0%)
0
(.0%)
0
Total 200
200 400
Plastic gown availability Pretest
%
Posttest
%
Total
available 14
(7%)
13
(6.5%)
27
Not available 186
(93.0%)
187
(93.5%)
373
Total 200
200 400
Safety glasses availability Pretest
%
Posttest
%
Total
available 0
(.0%)
0
(.0%)
0
Not available 200
(100.0%)
200
(100.0%)
400
Total 200
200 400

77
Table 6-5. Shoes covering availability in critical care areas in Khartoum state, 5 public
hospitals (2013-2016)
P value 1.000
Shoes covers was available in one unit from study areas.
Table 6-6. Face shield availability in critical care areas in Khartoum state, 5 public
hospitals (2013-2016)
No study area had face shield available before.
Shoes covering availability Pretest
%
Posttest
%
Total
available 8
(4%)
7
(3.5%)
15
Not available 192
(96%)
193
(96.5%)
385
Total 200
200 400
Face shield availability Pretest
%
Posttest
%
Total
Available 0
(.0%)
0
(.0%)
0
Not available 200
(100.0%)
200
(100.0%)
400
Total 200
200 400
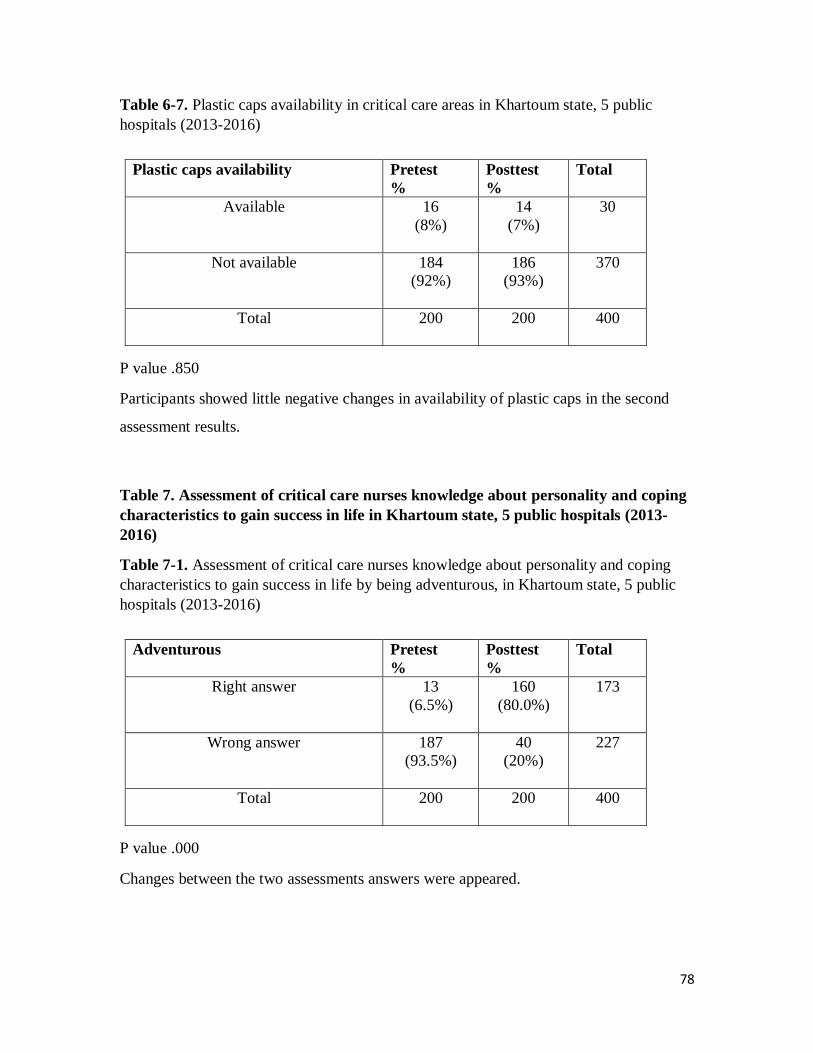
78
Table 6-7. Plastic caps availability in critical care areas in Khartoum state, 5 public
hospitals (2013-2016)
P value .850
Participants showed little negative changes in availability of plastic caps in the second
assessment results.
Table 7. Assessment of critical care nurses knowledge about personality and coping
characteristics to gain success in life in Khartoum state, 5 public hospitals (2013-
2016)
Table 7-1. Assessment of critical care nurses knowledge about personality and coping
characteristics to gain success in life by being adventurous, in Khartoum state, 5 public
hospitals (2013-2016)
P value .000
Changes between the two assessments answers were appeared.
Plastic caps availability Pretest
%
Posttest
%
Total
Available 16
(8%)
14
(7%)
30
Not available 184
(92%)
186
(93%)
370
Total 200
200 400
Adventurous Pretest
%
Posttest
%
Total
Right answer 13
(6.5%)
160
(80.0%)
173
Wrong answer 187
(93.5%)
40
(20%)
227
Total 200
200 400
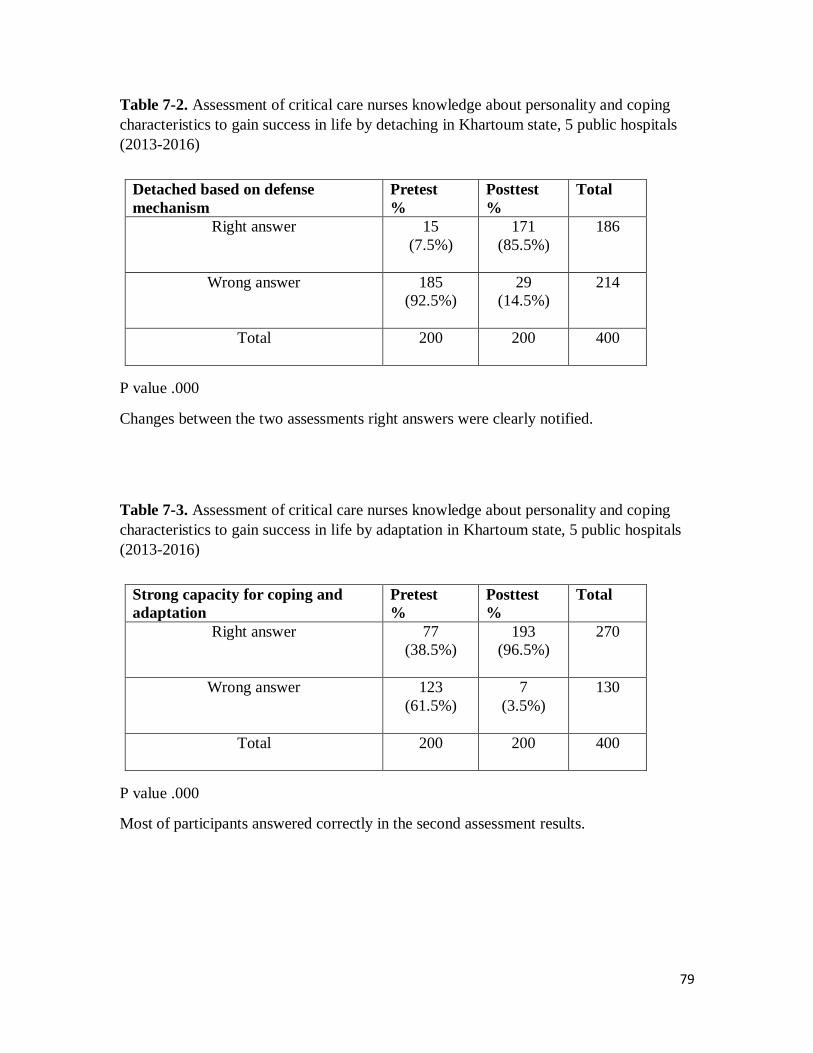
79
Table 7-2. Assessment of critical care nurses knowledge about personality and coping
characteristics to gain success in life by detaching in Khartoum state, 5 public hospitals
(2013-2016)
P value .000
Changes between the two assessments right answers were clearly notified.
Table 7-3. Assessment of critical care nurses knowledge about personality and coping
characteristics to gain success in life by adaptation in Khartoum state, 5 public hospitals
(2013-2016)
P value .000
Most of participants answered correctly in the second assessment results.
Detached based on defense
mechanism
Pretest
%
Posttest
%
Total
Right answer 15
(7.5%)
171
(85.5%)
186
Wrong answer 185
(92.5%)
29
(14.5%)
214
Total 200
200 400
Strong capacity for coping and
adaptation
Pretest
%
Posttest
%
Total
Right answer 77
(38.5%)
193
(96.5%)
270
Wrong answer 123
(61.5%)
7
(3.5%)
130
Total 200
200 400

80
Table 7-4. Assessment of critical care nurses knowledge about personality and coping
characteristics to gain success in life by hardiness in Khartoum state, 5 public hospitals
(2013-2016)
P value .000
About one quarter of respondents replied in correct manor during the first assessment.
Table 7-5. Assessment of critical care nurses knowledge about personality and coping
characteristics to gain success in life by resiliency in Khartoum state, 5 public hospitals
(2013-2016)
P value .000
Changes between the two assessments right answers were clearly notified regarding
resiliency.
Hardiness: control, commitment,
challenge and companionship
Pretest
%
Posttest
%
Total
Right answer 41
(20.5%)
169
(84.5%)
210
Wrong answer 159
(79.5%)
31
(15.5%)
190
Total 200
200 400
Resiliency (bounces back): insight,
independence, social support and
initiative
Pretest
%
Posttest
%
Total
Right answer 13
(6.5%)
174
(87.0%)
187
Wrong answer 187
(93.5%)
26
(13%)
213
Total 200
200 400

81
Checklist
(Adapted from CDC & AACCN)
Table 8. The number of critical care areas in each hospital
Frequencies represented numbers of critical areas in each hospital.
Table 9. The critical care units
Critical areas Frequency Percent
ICU 8 61.5
CCU 4 30.8
R R 1 7.7
Total 13 100.0
Frequencies represented types of critical care units.
Hospitals Frequency Percent
Khartoum
north 2 15.4
Omdurman 3 23.1
Alshaab 4 30.8
Khartoum 1 7.7
Ahmed
Gasim 3 23.1
Total 13 100.0

82
Table 10. Assesses critical care nurses practice regarding right using of preventive
measures of occupational hazards in CC areas, Khartoum state 5 governmental
hospitals (2013-2016)
Prevention measures
pre
post
frequency percent frequency percent
1. hand washing
in suitable
time
done perfectly
8
61.5
8
61.5
not done
5
38.5
5
38.5
total
13 100.0 13 100.0
2. wearing gloves
when needed
done perfectly
13
100.0
13
100.0
Hand washing not done in needed time, when there was no hand-washing sink available
or so far form the unit, no change noticed in pre/post observation.
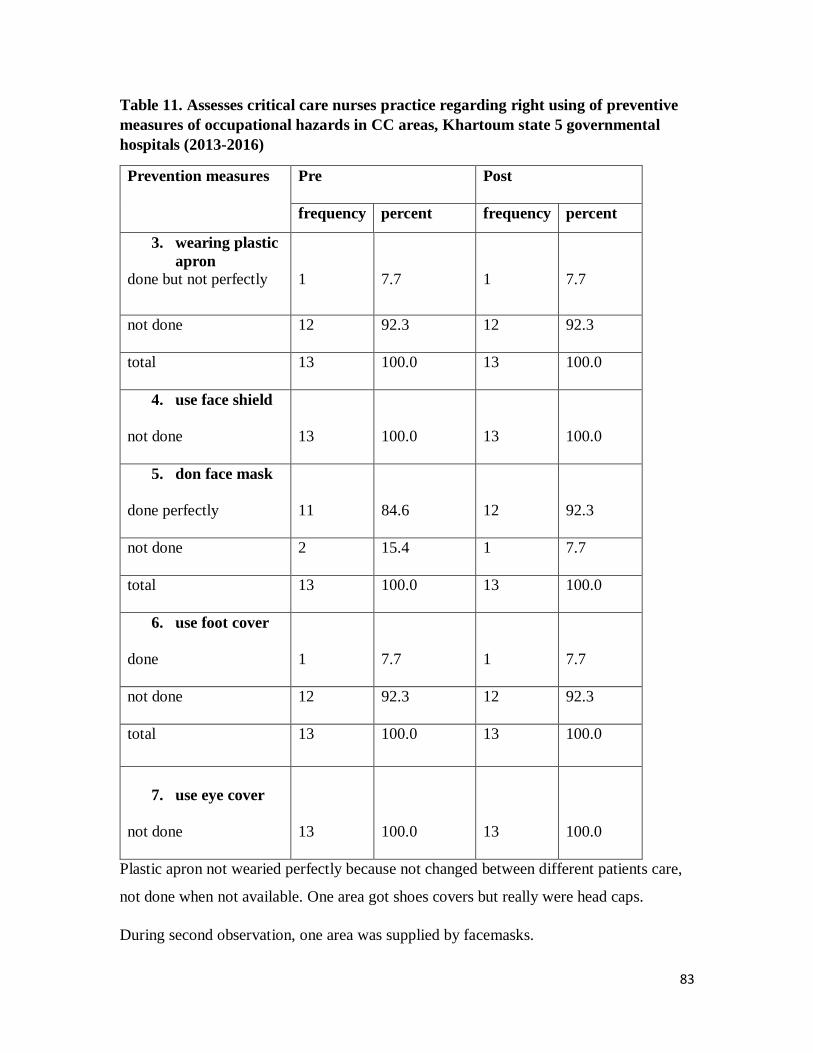
83
Table 11. Assesses critical care nurses practice regarding right using of preventive
measures of occupational hazards in CC areas, Khartoum state 5 governmental
hospitals (2013-2016)
Prevention measures Pre
Post
frequency percent frequency percent
3. wearing plastic
apron
done but not perfectly
1
7.7
1
7.7
not done
12
92.3
12
92.3
total 13
100.0 13
100.0
4. use face shield
not done
13
100.0
13
100.0
5. don face mask
done perfectly
11
84.6
12
92.3
not done
2
15.4
1
7.7
total
13 100.0 13 100.0
6. use foot cover
done
1
7.7
1
7.7
not done
12
92.3
12
92.3
total 13
100.0 13
100.0
7. use eye cover
not done
13
100.0
13
100.0
Plastic apron not wearied perfectly because not changed between different patients care,
not done when not available. One area got shoes covers but really were head caps.
During second observation, one area was supplied by facemasks.

84
Table 12. Assesses critical care nurses practice regarding right using of preventive
measures of occupational hazards in CC areas, Khartoum state 5 governmental
hospitals (2013-2016)
Preventive measures Pre Post
frequency percent Frequency Percent
8. use head cover
done perfectly
1
7.7
1
7.7
not done
12
92.3
12
92.3
total
13
100.0 13
100.0
9. disposal of sharp
objects
done perfectly
13
100.0
13
100.0
10. linen handling &
disposal
done perfectly
1
7.7
1
7.7
done but not perfectly 8 61.5
8 61.5
not done
4
30.8
4
30.8
total
13
100.0 13
100.0
11. protect self from
radiation
done perfectly
13
100.0
13
100.0
Sharp objects well treated, dirty linens not collected properly, and poor transference to
laundries in eight areas, four areas not did linens care where offered by patient’s family.
85
Interview with hospital’s matron results
During august 2015 five hospitals matrons interviewed, the points discussed were:
1. availability of PPE and causes of gaps in supply
2. Availability of sinks, soaps and germicides.
3. Pre-employment education about safety measures
4. Assigned OHN in hospital
There was similarity in all matrons’ talks, especially in PPE provision and recruited
OHN, they sent their thanks to ministry of health because disposable gloves available in
all hospital wards. Face masks, plastic apron and head covers not regularly provided, the
rest of PPE not provided. They shortage of PPE due to low hospital income and credit in
ministry of health, the set of PPE is very expensive.
Area without hand washing sink, matron said because the building not designed for ICU
from the beginning. Soap available but germicides not regularly found.
No hospital offered new nurses planned pre-employment educational program concerning
OHs, Matrons told that, they made orientation talk about hospital and sometimes,
occupational health mentioned in term of safety practice.
No hospital recruited occupational health nurse.
86
Chapter (5)
Discussion
Conclusion
Recommendations

87
Discussion
The study highlights the clear effectiveness of study interventions evidenced by the
improved results of CCNs knowledge about occupational hazards types and preventive
measures for each hazards in CC settings. In post education results, as examples,
knowledge about Physical and ergonomics hazards in pre intervention results was
mentioned by 14.5% of respondents while 99.5% of respondents in post questionnaire
knew that hazards, for radiation hazard 17% in pretest while 100% in post intervention
result. For preventive measures, participants showed 93% of pre intervention knowledge
about chemical hazards prevention and 99.5% in posttest result, stress mitigation by
relaxation exercise results were 14.5% in pretest and 99% after the intervention and
training in relaxation techniques.
These findings supported study conducted by Chen-Yin Tung, in Occupational Hazards
Education for Nursing Staff through Web-Based Learning, Taiwan, (28)
After web-based learning, post-test scores of the experimental group were higher than the
control group in terms of knowledge, attitudes, and in their knowledge about the
prevention of occupational hazards.
Participants showed good knowledge about their work biological hazards and ways to
prevent them (100%). This may be similar to the results found in other studies, (the
results from Philippine revealed that the high knowledge of the respondents about
biological hazards 95.9%), Nigeria, Uganda and Sudan also showed high nurses
knowledge of nurses about biological hazards. (29, 30, 37)
the using of the necessary personal protective equipment was associated with reduced
exposure to both biological and chemical hazards, following recommendations from the
Centers for Disease Control, (CDC, 1989) for health care professionals’ to use PPE for
infection control. ( 2 )
Indeed, use and compliance with utilization of PPE has been recognized as important
infection control measure in the healthcare industry, which should be emphasized to
minimize exposure to occupational hazards. Despite these recommendations, PPE
provision contracting with that mention above is not proper in our study areas, gaps appear

88
in plastic aprons and face masks supplies, face shield, and shoes covers never been
provided to that areas. Prevention of biological hazards by adherence to PPE, took place in
many previous studies, no study mentioned gaps in PPE provision except this study and
other two studies carried out in Uganda and Namibia, which represented similar situations
in African developing countries.
A considerable portion of the respondents reported increased level in knowledge about
causes of occupational hazards faces them in work place even though the hazards name not
mentioned by them. The possible answers for these results might reveal the actual presence
of the hazards in their areas, also might reflect that when hazard mentioned for respondents
become easier for them to find out its causes, they were not familiar with such terms. E.g.
physical and ergonomic hazards known by 14.5% in pretest while 84% enumerated causes
of physical and ergonomic hazards in pretest.
Based on the descriptions of American Board for Occupational Health Nurses (ABOHN),
(38) The Roles and Responsibilities of Occupational Health Nurses are clinical activities,
manager or administrator, educator/advisory roles, advocator, nurse practitioner,
occupational health service coordinator, and health promotion specialist. These great
roles of OHNs are absent in our study areas because there is no recruited or assigned
nurse for this job, so many CCNs don’t have enough knowledge about many aspects of
OH, e.g. knowledge about coping methods with this stressful work to gain success in life.
The importance for the advisory and OH services coordinator roles of OHN in health care
team arise to mitigate the negative effects and motivate CCNs.
Occupational health nurses advocate for occupational health and safety policies, they can
be particularly effective at this level by directly monitoring workplace exposures and
advocating to management for actions that protect workers, the study found that no any
study area assigned occupation health nurse to performe these roles, which was
supporting Amosu, A. M study about occupational hazards in Nigeria. (29)

89
Conclusion
The above study can be concluded as:
Those in the nursing profession are susceptible to a number of occupational hazards, to
work in a hazardous job nurses need to follow universal safety practice measures e.g.
recommendation from CDC.
Unavailability of personal protective measures, working overtime, experiencing work
related pressures, overload of work, low income and the inefficient role of the occupation
health department, are the main points reported by participants.
90
Recommendations
According to the results the study found that the following points are recommended:
• Teaching about international datasheets on occupational hazards for ICU nurse
before employment needs to be practiced in critical care areas.
• Improvement of the physical and social environment of critical care settings.
• Occupational health Department at the level of the State should have a role in
protecting the workforce in hospitals.
• Reporting of occupational injuries and illnesses suggest a surveillance program.
It would be useful in identifying problems.
• Based on this study regular trainings and educational meetings to enhance
occupational safety, develop/introduce policies and guidelines or strategies on all
aspects related to occupational hazards/safety need to be offered in all Sudan
states hospitals.
• A well-trained occupational health nurse should be assigned to educate health
workers on the prevention and management of occupational hazards.
• Additionally an occupational psychologist should be introduced to teach health
workers on how to cope with stress and emotional disturbances within the
working environment.
• The knowledge on occupational hazard and safety among CCNS can be
improved through Workshops, in-service training, mass meetings and refresh
courses providing information on occupational hazards safety attended by
registered nurses on a regular basis.
• Develop effective continuous commitment program for provision of protective
measures.
91
References
1. . Clement I. Occupational health. Basic Concept of Community Health Nursing, second
edition, Jaypee Brother medical publisher, New Delhi, India, 2009, Pp 291- 309.
2. John M, Suzan L, Critical care nursing, third edition, W. B. Saunders Company,
Philadelphia. 2009, p 98- 111.
3. NIOSH, CDC, Occupational hazards in hospitals, 2008 July, No – 136, available in
www.cdc.gov/niosh.
4. Smith M.R, Roy T.A. Authentic leader creating healthy work environments for
nursing practice. American J. Critical Care, , 2007, 15: 256-267.
5. Gershon M. et al, The prevalence and risk factors for percutaneous injuries in registered
nurses in the home health care sector, The American Journal of Infection Control, 2009,
37 (7): 525–533.
6. Madani M, Masoudi N. Taghizadeh M. Non-Specific Musculoskeletal Pain and
Vitamin D Deficiency in Female Nurses in Kashan, Iran. Journal of Musculoskeletal
Pain. 2014 , 22: p 1–7.
7. Souza AC, Alexandre NM. Musculoskeletal symptoms, work ability, and disability
among nursing personnel. Workplace Health & Safety journal. 2012, 60(8): 53–60.
8. Hunt R. Introduction to Community- Based nursing, fifth edition, Walter Kluwer
health/ Lippincott Williams & Williams, Philadelphia 2013, p 243.
9. American Association of Critical Care Nurses (AACN). Standards for establishing and
sustaining healthy work environments: a journey to excellence. American Journal of
Critical Care, 2008, 14: p 187-197.
10. Baumann, A. Positive practice environments: quality workplaces = quality patient
care: information and action tool kit. International Council of Nurses, 2008, available
in http://www.icn.ch/indkit.
11. . Bassavanthappa, BT, community health nursing, second edition, Jaypee Brother
medical publisher, India. 2008, p 290- 301.
12. Park K. Text Book of Preventive and Social Medicine, 19th edition, Banarisidas Bhanot
Publishers, New Delhi, India, 2007, p 658-670.

92
13. Burns S. Essentials of critical care nursing, second edition, Mc Graw Hill, New
York, 2014, p 30, 33.
14. Gallo M, Andrei S. Critical Care Nursing, seventh edition, Lippincott-Raven
publishers, USA. 2007, p 121- 134.
15. Ruth F. Patricia J, Maureen P. Regina N , Marjorie K, Franklin H. et al, Fundamentals
of Nursing, Lippincott Williams & Wilkins, Philadelphia. (2009),p 807- 833.
16. Elshiekh M, Khoja T, Pittet D, Al Salman J, Al Zahrani M, Francis C, et al. Infection
control and prevention, 2ed edition, Gulf Cooperation Council Riyadh. E-book
22490, Kingdom of Saudi Arabia, 2013, p 13- 30.
17. Siegel, E. Rinehart, M. Jackson P, guideline for isolation precautions: preventing
transmission of infectious agents in health care settings, American Journal of Infection
Control, 2007, 35(2): p 65- 164.
18. Kent, A. occupationally acquired infections in health workers, 2006, available in
www. Heart-intl.net.
19. Crayon, P. Handbook of human factors and ergonomics in health care and patient care,
New York: Routledge. 2006.
20. . Sedlak, C. Nurse Safety: Have We Addressed the Risks?" Online Journal of Issues
in Nursing. 2010, 9: 3- 5.
21. Gorman T. Jonathan D. controlling health hazards to hospital workers: New Solution,
The journal of occupational health policy, 2013, 23: p 25- 28.
22. Encyclopedia of Occupational Health and Safety, 5th edition, ILO, Geneva, 2000, 1: p.
6- 12, 2: p 34- 97.
23. Beaton R., Promoting occupational health nursing training, Journal of Workplace
health and safety, March 2012, 59(9): p 401- 405.
24. . Alli B.O. Fundamental principles of occupational health and safety, 2nd edition,
Geneva: ILO, 2008. E-book.
25. Van Den M, De Jonge J. Managing job stress in nursing: what kind of resources do
we need? Journal of Advanced Nursing, 2008, 63: p 75–84.
26. Harry D. Occupational health of health care workers, Tarot, Estonia, 2010, p 33, 34.
27. James D. A new look at nursing safety, second edition, BMJ publishing group,
London, 2010. E-book.

93
28. Chen-Yin Tung, Occupational Hazards Education for Nursing Staff through Web-
Based Learning, International Journal of Environmental Research and Public Health,
2014, 13035-13046: 10.3390.
29. Amosu A.M. The level of knowledge regarding occupational hazards among nurses
in Nigeria, Journal of Biological sciences, 2011, 3(6): P 586- 590.
30. Castro, AB. Occupational Health and Safety Issues among Nurses in the
Philippines, 2009, available from
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2797477.
31. . Ticiani D, Shimizu H, Branco A. Occupational Health Hazards in ICU Nursing
Staff, Brazil, Journal of Nursing Research and Practice, 2010: ID 849169.
32. Sikiru, L. And Hanifa, S. 2010, Prevalence and risk factors of low back pain among
nurses in a typical Nigerian hospital, available from
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2895788
33. Carlos A, stress in nursing work in ICU, Israelita hospital, Brazil, Latino Americana
de Enfermagem, 2008, 16:2008.
34. Ndejjo R. et al. (2015), Occupational Health Hazards among Healthcare Workers in
Kampala, Uganda, Journal of Environmental and Public Health, 2015: Article
ID 913741.
35. Tuvadimbwa J, knowelege and practice among nurses on occupational hazards in
Namibia, 2015, available from www. unam.na.
36. Abass A. Occupational hazards affecting dental manpower in Khartoum state, Sudan,
2004, available from http:/ khartoumspace.uofk.edu.
37. Bwogi A, Namale C. (2010) Sero-prevalence and risk factors for hepatitis B virus
infection among health care workers in a tertiary hospital in Uganda, Infectious
Diseases, 10:, ID. 191.
38. American Board of Occupational Health Nursing - ABOHN. Job analysis survey of
occupational health nursing practice. Hinsdale, Illinois; 1999.

94
Bibliography
• AAOHN, Optimal nurse staffing to improve quality of care and patient outcome,
Journal of Workplace health and safety, Nov 2015, 3(4): p 8-10.
• Sandra M., Lippincott manual of nursing practice, 10th edition, Lippincott
Williams & Williams A Wolters Kluwer Company, 2014, pp 26- 28.
• Judith A. &Walton B., community health nursing, Lippincott Williams &
Williams A Wolters Kluwer Company, 2014, p 706- 708.
• Janice L. BRUNNER&SUNNDARTHS’ Textbook of Medical surgical nursing,
13th edition, Walter Kluwer health/ Lippincott Williams & Williams,
Philadelphia. 2013, p 7, 28, 78-88.
• Kulkarni J. Hand hygiene practices among health care workers (HCWs) in a
tertiary care facility in Pune,” Medical Journal Armed Forces India, 2013, 69
(1)9 : p 54–56.
• John C. Occupational health and safety for health care workers. American
Journal of Critical Care, 2009, 12: 122-128.
• Buerhaus, P. The Recent Surge in Nurse Employment: Causes and Implications,
Health Affairs, 2009. 28(4): 657-668.
• Thomson R. (2015), Journal of Workplace Health & Safety: Promoting
Environments Conducive to Well-Being and Productivity, volume 64, issue five.
• Bureau of Labor Statistics, Personal Communication. Centers for Disease
Control and Prevention, HIV/AIDS Surveillance Report, 6:1, p 11.
• Harry A. Evan T, ABC of Resuscitation, Infection risk and resuscitation, 5th
edition, BMJ publishing group, London, 2008, p 87- 89, E-book.
• Amakali K. Perception of health workers regarding occupational health in
Namibia, Hospital Administration Journal, 2015, 4 (5): p: 34- 4o.
• Leigh J, Miller T. Costs of Occupational Injury and Illness within the Health
Services Sector, Intl. J. of Health Services, 2007, 35(2): p 342-359.
95
Annexes
Annex 1. Questionnaire
Annex 2. Checklist
Annex 3. Formal letters
Annex 4. Manual of the program

96
Annex 1.
RIBAAT NATIONAL UNIVERSITY - FACULTY OF POST GRADUATE
QUESTINARE ABOUT OCCUPATIONAL HAZARD IN CRITICAL CARE SETTINGS
Session one
1. Age:
20—30 ( ) 31---40 ( ) More than 40 ( )
2. Sex :
Female ( ) Male ( )
3. Graduation level of nursing:
Diploma ( ) Bachelor ( ) Master ( ) Doctorate ( )
4. What is the length of your experience in years?
Less than one year ( ) Less than five years ( ) More than five years (
)
5. What is your main working shift?
Session two
6. What is the meaning of occupational hazards?
External conditions and influences affect work population in their work area ( )
7. Enumerate types of occupational hazards in your work with an example of each
hazard?
• Biological hazards [infectious hazards] ( )
• Physical and ergonomics [noise, musculoskeletal injuries] ( )
• Chemical hazards [cytotoxic drugs] ( )
• Radiological hazards [portable radiography and fluoroscopy] ( )
• Psychosocial hazards [stress, conflicts, job dissatisfaction] ( )
Session three:
8. What are the causes of each hazard in your work?
*Biological hazards [infectious hazards]:
Blood or body fluids, by droplets in the air, or by direct contact. ( )
*Physical and ergonomics
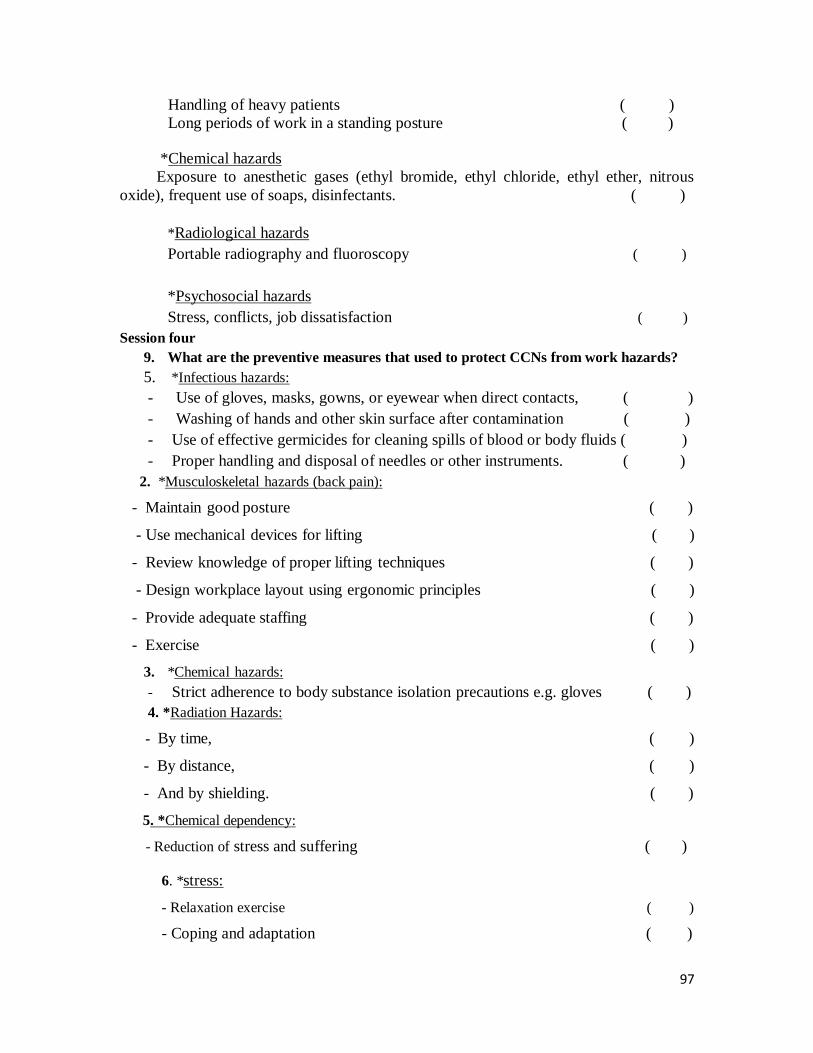
97
Handling of heavy patients ( )
Long periods of work in a standing posture ( )
*Chemical hazards
Exposure to anesthetic gases (ethyl bromide, ethyl chloride, ethyl ether, nitrous
oxide), frequent use of soaps, disinfectants. ( )
*Radiological hazards
Portable radiography and fluoroscopy ( )
*Psychosocial hazards
Stress, conflicts, job dissatisfaction ( )
Session four
9. What are the preventive measures that used to protect CCNs from work hazards?
5. *Infectious hazards:
- Use of gloves, masks, gowns, or eyewear when direct contacts, ( )
- Washing of hands and other skin surface after contamination ( )
- Use of effective germicides for cleaning spills of blood or body fluids ( )
- Proper handling and disposal of needles or other instruments. ( )
2. *Musculoskeletal hazards (back pain):
- Maintain good posture ( )
- Use mechanical devices for lifting ( )
- Review knowledge of proper lifting techniques ( )
- Design workplace layout using ergonomic principles ( )
- Provide adequate staffing ( )
- Exercise ( )
3. *Chemical hazards:
- Strict adherence to body substance isolation precautions e.g. gloves ( )
4. *Radiation Hazards:
- By time, ( )
- By distance, ( )
- And by shielding. ( )
5. *Chemical dependency:
- Reduction of stress and suffering ( )
6. *stress:
- Relaxation exercise ( )
- Coping and adaptation ( )

98
- Social support ( )
Session five
10. What are the components of universal precautions?
12. Hand washing ( )
13. Personal protective equipment [PPE] ( )
14. Preventing/managing sharps injuries ( )
15. Aseptic technique ( )
16. Isolation ( )
17. Staff health ( )
18. Linen handling and disposal ( )
19. Waste disposal ( )
20. Spillages of body fluids ( )
21. Environmental cleaning ( ) 11. Risk management/assessment ( )
Session six
22. Do you have this personal protective equipment in your units?
Available Not available Other
1. Face mask
2. Disposable gloves
3. Plastic gowns
4. Safety glasses
5. Shoes covering
6. Face shield
7. Plastic caps
Session seven
23. What are the personality and coping characteristics of successful CCNs?
- Adventurous ( )
- Detached ( based on defense mechanisms) reduces anxiety level ( )
- Strong capacity for coping and adaptation ( )
- Hardiness: control, commitment, challenge, companionship ( )
- Resiliency (bounces back): insight, independence, social support, ( )
and initiative.
24. What are your suggestions to improve your work environment?
------------------------------------------------------------------------------------------------------------
------------------------------------------------------------------------------------------------------------
------------------------------------------------------------------------------------------------------------
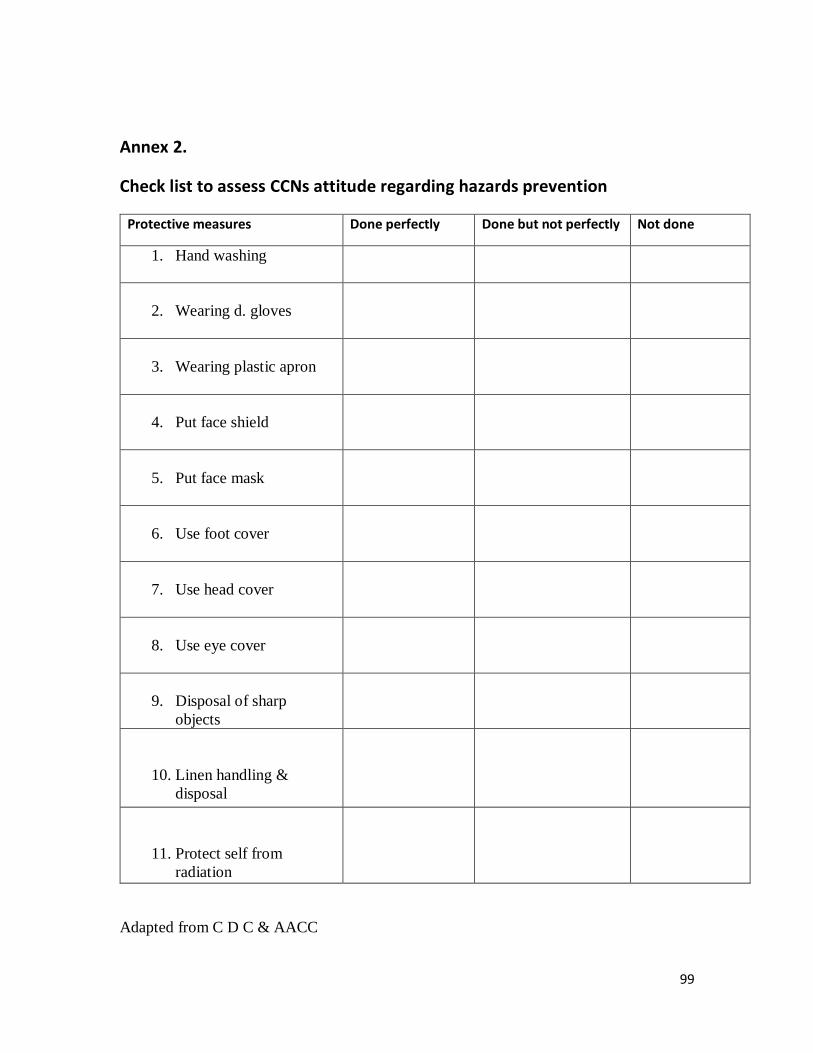
99
Annex 2.
Check list to assess CCNs attitude regarding hazards prevention
Protective measures Done perfectly Done but not perfectly Not done
1. Hand washing
2. Wearing d. gloves
3. Wearing plastic apron
4. Put face shield
5. Put face mask
6. Use foot cover
7. Use head cover
8. Use eye cover
9. Disposal of sharp
objects
10. Linen handling &
disposal
11. Protect self from
radiation
Adapted from C D C & AACC

100
Annex three. Formal Letters

101
Annex four.
The manual of educational program