THE EFFECT OF REMITTANCES ON POPULATION HEALTH: AN ...
32
THE EFFECT OF REMITTANCES ON POPULATION HEALTH: AN ANALYSIS OF REMITTANCES, HEALTH OUTCOMES, AND HEALTH EXPENDITURES A Thesis submitted to the Faculty of the Graduate School of Arts and Sciences of Georgetown University in partial fulfillment of the requirements for the degree of Master of Public Policy By Andrea Thoumi, M.Sc. Washington, DC April 10, 2016
Transcript of THE EFFECT OF REMITTANCES ON POPULATION HEALTH: AN ...

THE EFFECT OF REMITTANCES ON POPULATION HEALTH: AN ANALYSIS OF
REMITTANCES, HEALTH OUTCOMES, AND HEALTH EXPENDITURES
A Thesis submitted to the Faculty of the
Graduate School of Arts and Sciences
of Georgetown University
in partial fulfillment of the requirements for the
degree of Master of Public Policy
By
Andrea Thoumi, M.Sc.
Washington, DC
April 10, 2016

ii
Copyright 2016 by Andrea Thoumi
All Rights Reserved

iii
THE EFFECT OF REMITTANCES ON POPULATION HEALTH: AN ANALYSIS OF
REMITTANCES, HEALTH OUTCOMES, AND HEALTH EXPENDITURES
Andrea Thoumi, M.Sc.
Thesis Advisor: Andreas Kern, Ph.D.
ABSTRACT
While the search for alternative health financing mechanisms to fund national
health systems is not a new international development challenge, fiscal pressures to
identify alternative sources of revenue for health are growing. Today, low- and middle-
income countries are facing a dual burden of infectious and chronic diseases.
Remittances, or the money that migrants send back to their households, have been found
to positively impact certain health outcomes, including infant mortality and under-5
mortality; however, it is less clear if health spending is the channel leading to this
outcome. This study uses data from the World Development Indicators database between
1995-2011 to explore the two-part question of whether remittances are associated with
health spending and if health spending is associated with the positive health outcomes
that result from higher levels of remittances. The study uses a multivariate analysis and a
dynamic GMM approach. The key findings suggest that remittances are not significantly
associated with a reduction in government health spending, but are positively associated
with certain health outcomes, such as infant mortality rate and under-5 mortality rate.
Policy implications include increasing public health spending to raise total health
spending, implementing policy reforms to facilitate the transfer of remittances, and
creating alternative routes to increase household consumption.

iv
To Ines and Charlie

v
Table of Contents
Introduction ......................................................................................................................... 1
Chapter 1: Literature Review and Conceptual Framework ................................................ 4
Effect of Remittances on Health Outcomes .................................................................... 4
Effect of Remittances on Health Spending ..................................................................... 5
Effect of Remittances on Public Goods Provision .......................................................... 6
Theoretical Considerations and Hypothesis .................................................................... 7
Chapter 2: Empirical Analysis ............................................................................................ 9
Chapter 3: Results ............................................................................................................. 11
Chapter 4: Policy Implications.......................................................................................... 14
Chapter 5: Conclusions and Limitations ........................................................................... 16
References ......................................................................................................................... 24

vi
List of Tables
Table 1: Description of World Development Indicators ....................................................... 19
Table 2: Descriptive Statistics (1995-2011) ............................................................................. 20
Table 3: Effects of Remittances (USD) on Health Outcomes ............................................... 21
Table 4: Effect of Public Health Spending (% of Government Expenditure) on Health
Outcomes ....................................................................................................................................... 22
Table 5: Effect of Remittances on Health Spending Measures ........................................... 23

1
Introduction
While the search for alternative health financing mechanisms to fund national
health systems is not a new international development challenge, fiscal pressures to
identify alternative sources of revenue for health are growing.1-3 As low- and middle-
income countries (LMICs) continue to battle infectious diseases and preventable
maternal, child and newborn mortality rates, these countries are undergoing
epidemiological transitions. Driven by aging populations, improved technologies, and
globalization, LMICs are facing a greater burden of non-communicable diseases, such as
cardiovascular disease and diabetes, which are increasingly common causes of mortality
and morbidity.4 Along with the changing needs of populations, efforts to expand
universal health coverage schemes continue to exert pressure on national health accounts,
which are comprised of public and private health expenditures.3 Furthermore, many
factors beyond health expenditure determine health outcomes, higher health spending
reduces adverse health outcomes, including infant mortality rate and under-5 mortality
rate.5,6 Thus, identifying innovative sources to cover rising health spending needs and to
improve population health is relevant and timely.
Theoretically, one funding source that has been identified as a potentially
innovative health financing tool for domestic mobilization of health care expenditures is
the transfer of remittances.3 Remittances are the private transfers of money from a
migrant to family members remaining in the country of origin. In 2015, remittance
financial flows accounted for over $600 billion globally.7 As these cash transfers occur
formally through banks or informally through other channels, this estimate is an
underestimated amount. Compared to other capital inflows, such as foreign direct

2
investment (FDI) and official development assistance (ODA) that are tied to specific
projects, remittances offer relative flexibility and stability to remittance-receiving
households by smoothing income and consumption and increasing the household’s ability
to allocate funding to their specific needs.8-10 For example, for top remittance-receiving
countries, remittances can represent 20 to 40 percent of national gross domestic product
(GDP);7 for remittance-receiving households, remittances can account for up to 50
percent of the household’s income and act as a tool to reduce poverty and income
inequality.11,12 Nevertheless, remittances may also create inflation, increase corruption,
lower governance and increase dependency on an external labor market.13-17 Despite
these potentially challenging macroeconomic effects, many countries and the
international community have argued in favor of using remittances for fostering
economic development.16,18,19
Studies have shown the positive impact of remittances on health outcomes,
including lowering infant mortality rates, increasing infant birth weight, household health
spending, and health knowledge, and equalizing access to care.10,20-23 Despite the positive
effects on health indicators at the micro level, the global evidence on the effect of
remittances on health spending at the macro level is mixed. Some evidence indicates that
remittances can increase corruption and lower political demand for change, resulting in a
government decreasing its social spending.14,24,25 Other studies suggest that the
government will increase accountability instead.15 To date, few studies have analyzed the
effect of remittances on public health expenditures or the exact channel between
remittances and improvements in health outcomes.24,26,27 Therefore, do remittances have
3
an effect on public health spending and through which channel do remittances affect
health outcomes?
The purpose of this paper is to expand the literature around remittances, public
health spending and health outcomes. The two-part study includes an analysis of whether
public health spending is the channel through which remittances are positively affecting
infant mortality rate, under-5 mortality rate, and maternal mortality ratio and if
remittances impact public health spending. The study analysis is based on static and
dynamic (GMM) estimation techniques that are used to model the impact of remittances
on health outcomes and health spending. The use of dynamic estimation techniques
minimizes endogeneity bias – especially reverse causality between remittances and health
spending measures – that might threaten the statistical validity of the analytical results.
This study contributes to the literature by providing preliminary evidence that remittances
will not significantly reduce public health spending suggesting that the results could
mitigate concerns that remittances negatively affect social spending.
While the literature suggests that remittances will likely decrease public health
spending, the data show that there is no effect. Furthermore, the data confirm that
remittances have a positive impact on health, though remittances do not affect maternal
mortality ratio. This is likely because maternal mortality ratio reflects the functional
status of the health care system whereas other health outcome measures, such as infant
mortality rate and under-5 mortality rate, depend on many social determinants of health
beyond health services. Lastly, the data show that raising overall health expenditure, not
other health spending measures, will affect infant mortality rate and under-5 mortality
rate.
4
Chapter 1: Literature Review and Conceptual Framework
Global evidence shows the impact of remittances spans from reducing national
poverty levels to improving economic and social development outcomes, including health
and education.11,18,19,28 Studies have shown that remittances generally have a positive
effect on health outcomes, including reducing infant mortality rate and infant birth
weight, improving child health and increasing overall health spending.20,21,29 Moreover,
remittances have been found to counter the initially negative effect on health of having a
parent leave a household.30 Other studies have suggested that there may be a negative
effect on public health spending because the government may begin to engage in a public
moral hazard knowing that households are now receiving more income from abroad,
which could be invested in health through the private sector.24
Effect of Remittances on Health Outcomes
Overall, studies show the effect of remittances on infant mortality rate is positive.
Kanaiaupuni and Donato (1999) found that migration in Mexico initially had a disruptive
effect on community and family life, increasing infant mortality rate; however, overtime
this effect positively impacted infant mortality rate as communities experienced long-
term migration patterns. Other studies further support the positive association between
remittances and health outcomes. Zhunio, Vishwasrao and Chiang (2012) found that a
1% increase in remittances per capita increased life expectancy by 0.03% and reduced
infant mortality rate by 0.15% in Mexico. Duryea, Lopez Cordova, Olmedo (2005)
posited that this positive association is partly due to improved housing conditions. Others
have found a differential effect between migrant households compared to non-migrant
households that are due in part to the influx of money to spend on more nutritional food,

5
medical care, and improved housing. For example, infants born in migrant households are
3% less likely to die than in non-migrant households and are approximately 5% less
likely to be born underweight.20 As more households receive remittances, infant mortality
rate declines further.27
Effect of Remittances on Health Spending
Studies have shown a mixed effect of remittances on health care spending at the
household- and government-level. On the one hand, Amuedo-Dorantes and Pozo (2009)
estimated that a 100 Mexican peso increase in remittances in Mexico augments
household health expenditure by 5 or 6 Mexican pesos, though the effect of remittances
will differ depending on the amount of remittances received. Similarly, in Ecuador, an
increase of $10 resulted in a private health spending increase of 5%.22 Cen Camal (2012)
found an additional household level effect. Specifically, Mexican households use
remittances to pay off health related debt, suggesting that remittances can be used at the
household level to prevent catastrophic health payments that can push a household further
into poverty.
In addition to the positive correlation between remittances and private health
spending, the literature indicates differences depending on the level of remittances
received. Amuedo-Dorantes, Sainz and Pozo (2007) found that higher income remittance-
receiving households spend 7% of remittances on health compared to 4% in lower
income remittance-receiving households. Others estimates suggest that households that
do not have access to formal health insurance will spend 11% of remittances on health
compared to 8% for households with formal health insurance.31

6
Effect of Remittances on Public Goods Provision
Despite the positive effects of remittances on household health spending, the
evidence on the effect of remittances at the macro-level is mixed. While there is general
consensus that remittances will change the local political economies in home countries,
including altering the way that tax revenues are allocated, studies have found that
remittances have a mixed effect on corruption and governance, key determinants of the
provision of public goods. Ahmed (2012) noted that a 3 percentage point increase in
remittances increases corruption by 1 point on a corruption index. Abdih et al (2008)
found a similar negative association between remittances and corruption, indicating the
potential for governments to free ride based on the availability of remittances to
substitute their provision of public goods.32 In contrast, Tyburski (2012) found that
remittances have the potential to counter corruption by increasing government
accountability. The relationship between remittances and governance is relevant to health
outcomes given that the positive effect of higher health spending on health outcomes is
dampened in low governance environments.33
These results on overall government indicators suggest that the effect of
remittances on health spending may be mixed. Indeed, while Naanwaab and Yeboah
(2013) found that a 10% increase in remittances is associated with a 0.30% increase in
health spending as percent of GDP, Ebeke (2012) argued that remittances reduce health
spending in countries with poor governance structures. A recent study exploring the
effect of remittances on social spending found that the stabilizing effect of remittances at
the household level lowered the public’s demand on the government to provide social

7
services.25 These findings suggest the potentially downward effect of remittances on
health spending.
Theoretical Considerations and Hypothesis
Remittance-receiving households use remittances for a variety of reasons
spanning immediate consumption to long-term investments for human development, such
as education and health. Often times, migrants cite increasing health care spending as a
primary reason for sending remittances; however, households may use remittances to buy
common household items, such as clothing, food or electronics, or to invest in physical
infrastructure or social development, such as education.8,29,34 The lag in spending on
social development is likely due to effects that materialize in the long-term. In other
words, a remittance-receiving household can receive immediate benefits, or higher utility,
by purchasing durable goods, whereas the impact of a better education or better health
access may occur in the long-term.
Remittances are sent to households through two main mechanisms: formal and
informal. The formal exchange of remittances is through banks, credit unions and the use
of money transfer organizations (MTO), such as Western Union or MoneyGram.
Formally remitting money can be expensive due to high transaction costs and asymmetric
information between the bank and the sender. Other challenges include fear of interacting
with the formal financing system or that the financial system in the home country is
inadequate.35,36
Assuming the migrant household can access a bank to receive the remittances, the
decision on how to use the remittance will be the responsibility of the head of household
in the home country. Often times, the primary reason a migrant cites for remitting may

8
not coincide with the primary use of the remittances. For example, nearly half of Mexican
remitters have cited health care spending as a primary reason for sending money to
families, which aligns with altruistic, insurance and investment theories that explain why
immigrants transfer remittances home.11 However, households are more likely to use
remittances to buy common household items, such as clothing, food or electronics, or
invest in physical infrastructure or social development, such as education.10 Households
will likely spend remittances on immediate basic consumption needs, followed by
investments, which can include home construction or human capital. Therefore, while the
implications on direct health spending are limited, household investments (e.g., improved
housing conditions or social standing) due to the higher budgetary constraint could have a
greater impact on health outcomes.
The health implications of the informal exchange channel depend on whether the
remittances are intended to support the community or the individual household. Migrants
may form hometown associations (HTA) to send money back home to a community.
Money pooled through HTAs could be used to build a health clinic for a local community
with matching funds from the municipal government.37 While the HTA is creating a
public good that can positively impact the population’s health, an individual household
may benefit more if the informal mechanism is at the individual household level. As the
money is directly tied to the migrant’s household, instead of the community, the
household could receive more direct benefits than if the informal channel is community-
based. An additional benefit to the individual household level mechanism is that
knowledge may be transferred more easily, especially if the migrant is travelling back
home and relaying health knowledge that may have been acquired abroad.

9
The determinants for health outcomes include social standing, income, education,
living conditions, and access to health systems.38 Regardless of whether the intended use
of remittances aligns with the actual household expenditure, remittances can increase a
household’s standard of living by increasing their consumption budget line. It is through
this expansion of the budget line that households may be able to invest more money in
factors that affect health. This can include improvements in housing and living
conditions, higher direct out-of-pocket spending on health services, or improved access to
food and nutrition. It is possible that households may seek services through the private
sector as they now have higher purchasing power to spend on health care.
Based on the theory posited in the literature, the main hypotheses of this paper are
that remittances will result in the government lowering public health spending and that
the channel through which remittances is impacting health outcomes is indirect. The
government may lower public spending on health care if they perceive this higher out-of-
pocket spending as a substitute to government spending. Furthermore, as higher
remittance levels implies that the country has a higher migrant stock, there may also be
less public pressure to reform behaviors, such as corruption or lower social spending.15,25
Moreover, as households receive remittances, they will likely increase their household
consumption, which will have a greater impact on health outcomes, such as infant
mortality rate and under-5 mortality rate, that are a function of social determinants of
health.
Chapter 2: Empirical Analysis
The analysis follows a two-step approach. First, the effect of remittances on
health outcomes and health spending are analyzed. Second, an empirical model studying
10
the effects of health spending on actual health outcomes is developed as a complementary
tool. This second stage of analysis allows a more detailed exploration of the two key
questions: whether and through which channels remittances impact selected health
outcomes. The basic multivariate specification is the following:
The central dependent variable in the model, HealthExpi,t, is health spending (all
measures included in Table 1) for a country, i, at a time, t. The main independent
variable, remittances (measures included in Table 1), is lagged, t-1, to minimize the threat
of reverse causality and to capture the lagged adjustment of public health expenditures.
Furthermore, remittances and health spending measures are logged. Controls are denoted
through Xi,t and country and time fixed effects are captured using ut and Θt . All data are
from the World Bank’s World Development Indicators (WDI) dataset, a multisectoral,
multi-country panel dataset that spans over 200 countries over 50 years. To ensure
overlap between the independent variable, remittances, and the dependent variable,
public health expenditure, the time period for this study is 1995-2011. Table 1 describes
the variables, short form and source of the selected variables used in the model. Table 2
describes the number of observations and other summary statistics for the variables
included in the model.
Other controls included in the model were GDP per capita, GDP growth rate,
urban population rate and life expectancy. As the selected model specification was
relatively small, country and time fixed effects (fe) were used to eliminate the potential
for omitted variable bias in a multivariate analysis. To control for the potential of reverse
causation, a dynamic panel approach was used. Other studies have used instrumental
11
variables to achieve this same goal.24 The same approach was used for the analyses using
health outcome data, including infant mortality rate, under-5 mortality rate and maternal
mortality ratio. Sensitivity analyzes were also conducted by geographic region (i.e.,
Africa, Asia, Americas, Europe) and income group (i.e., Low, Middle).
Chapter 3: Results
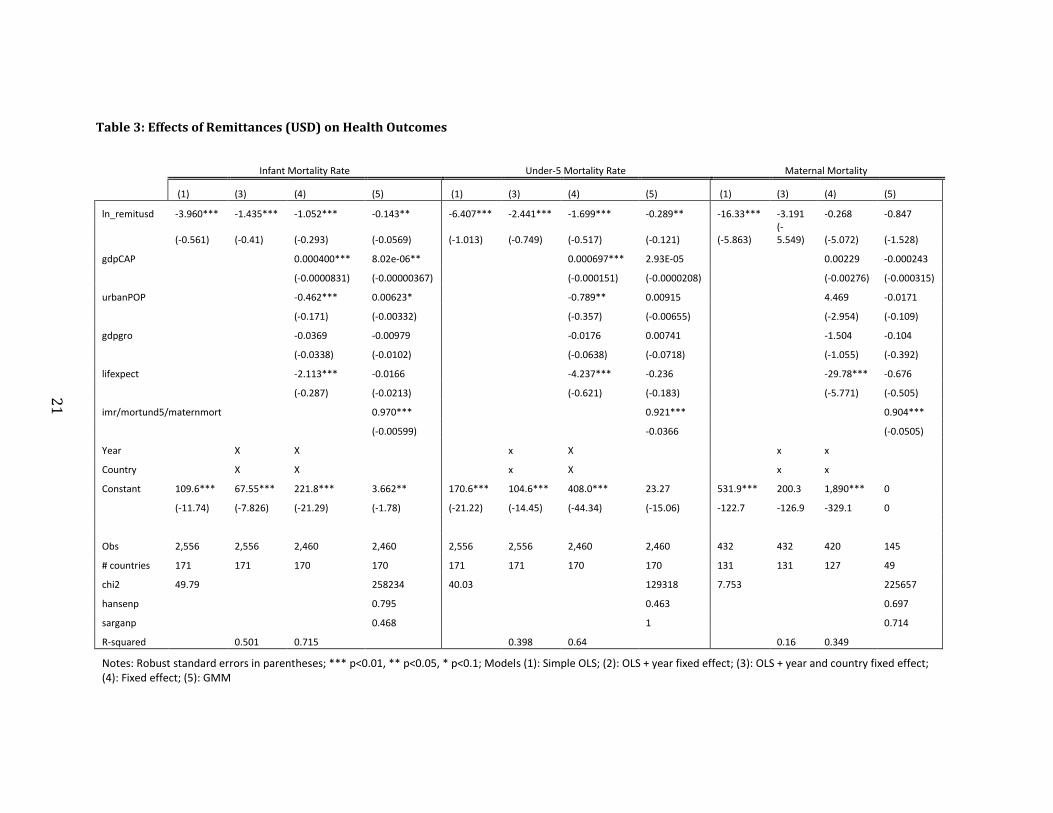
Remittances and Health Outcomes: In a year and time fixed effect model
including GDP per capita, the percentage of urban population, and GDP growth as
controls, remittances (in USD) have a statistically significant effect on infant mortality
rate and under-5 mortality rate (Table 3). On average, a one percent increase in
remittances is associated with a reduction of 1.015 infant deaths per 1,000 live births.
Similarly, including time-varying and country-varying controls, a one percent increase in
remittances is associated with a 1.699 under-5 deaths per 1,000. In contrast, there is no
statistically significant association between remittances and maternal mortality ratio.
These relationships hold when robustness checks were conducted using a different
measure of remittances (as percent of GDP) (Appendix A7) or regional and economic
variation (Appendix A8). The GMM model shows the same statistical association;
however, the relationship is somewhat smaller. The GMM model eliminates the problems
due to reverse causality (e.g., improved health could create a larger migrant pool, which
could, in turn, increase remittances) and serial correlation between health outcomes and
remittances (e.g., health outcomes may remain relatively constant over time). Overall, the
results indicate that remittances improve health the results indicate that remittances
improve health outcomes. Separate analyses on the relationship between health spending
and health outcomes are used to isolate the channels through which remittances operate.
12
Health Spending and Health Outcomes: In a year and time fixed effect model
including GDP per capita, the percentage of urban population, and GDP growth as
controls, public health expenditure (as % of government expenditure) has a statistically
significant effect on maternal mortality ratio but does not have a statistically significant
effect on IMR and under-5 mortality rate (Table 4). On average, a one-unit increase in the
log of the percent of public health expenditure (% of government expenditure) is
associated with a reduction of 81 maternal deaths per 100,000 live births. The GMM
model shows a different statistical association where only under-5 mortality rate has a
statistically significant effect. These relationships vary when robustness checks were
conducted using different measures of public health expenditure (Appendix A3, A4, A5)
or regional and economic variation (Appendix A9). For example, main findings from
robustness checks using differing measures of health expenditure show the following:
First, on average, a one percent increase in expenditure per capita is associated
with a reduction of 2.335 infant deaths per 1,000 live births. There is no statistical
association with under-5 mortality rate or maternal mortality ratio or in the GMM model
(Appendix A3). Second, on average, a one unit increase in the log of the percent of public
health expenditure (% of GDP) is associated with a reduction of 3.785 under-5 deaths per
1,000 and a reduction of 7.325 maternal deaths per 100,000 live births. There is no
statistical association with infant mortality rate or in the GMM model (Appendix A4).
Third, on average, a one unit increase in the log of the percent of public health
expenditure (% of total health expenditure) is associated with a reduction of 4.628 under-
5 deaths per 1,000 and 122.2 maternal deaths per 100,000 live births. There is no
statistical association with IMR or in the GMM model (Appendix A5).

13
Other robustness checks focused on the effect of household consumption,
government consumption and development assistance show the following (Appendix
A10). First, on average, a one-unit increase in the log of the percent of household
consumption, as percent of GDP, is associated with a reduction of 5.603 maternal deaths
per 100,000 live births and a reduction of 2.906 infant deaths per 1,000 live births. There
is no statistically significant association between household consumption and under-5
mortality rate. Second, on average, a one-unit increase in the log of the percent of
government consumption as percent of GDP is associated with a reduction of 5.425
under-5 deaths per 1,000 and reduction of 3.99 infant deaths per 1,000 live births. There
is no statistically significant association between government consumption and maternal
mortality ratio. Lastly, there is no statistically significant association between
development assistance and the three selected health outcomes.
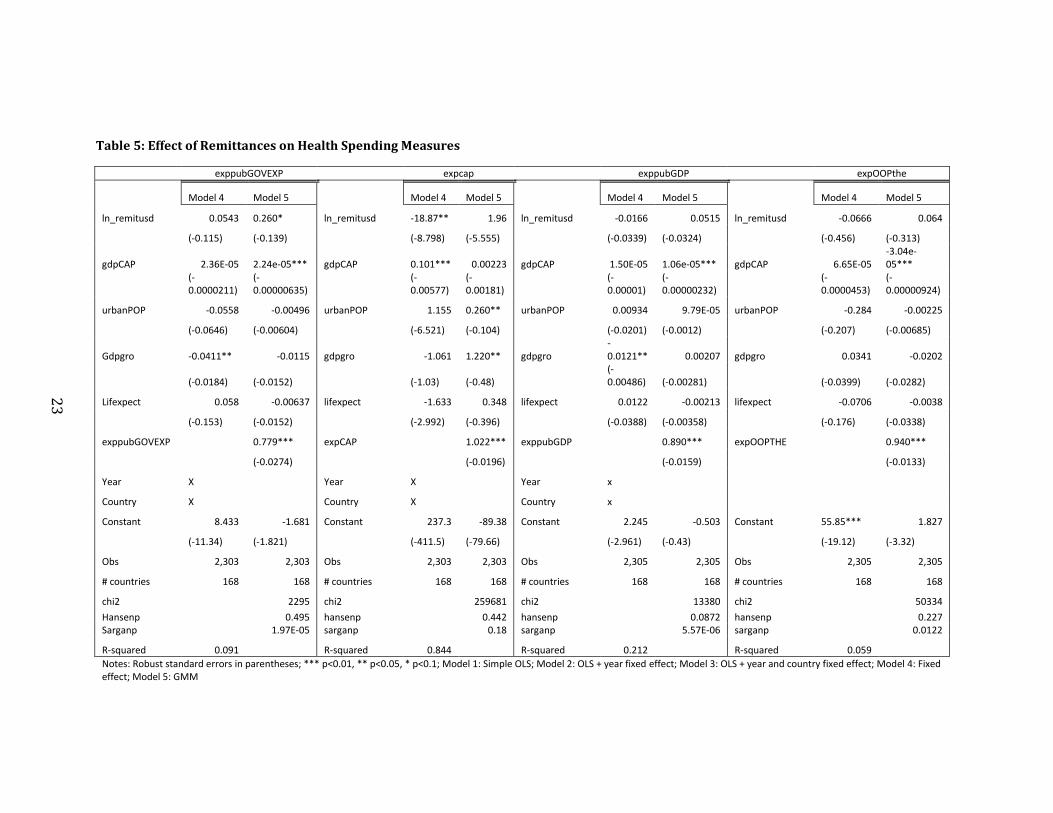
Remittances and Health Spending: In a year and time fixed effect model including
GDP per capita, the percentage of urban population, and GDP growth as controls,
remittances (in USD) have a statistically significant effect on expenditure per capita
(Table 5). On average, a one percent increase in remittances is associated with a
reduction of $18 in health expenditure per capita. There is no other statistically
significant effect on other health expenditure measures. The GMM model shows a
statistically significant effect on public health expenditure as percent of government
expenditure. On average, a one percent increase in remittances is associated with a 0.2
unit reduction in the log of public health expenditure as percent of government
expenditure. There is no other statistically significant effect on other health expenditure
measures.
14
Chapter 4: Policy Implications
The key findings from this analysis suggest that remittances are not significantly
associated with a reduction in government health spending, but are positively associated
with certain health outcomes, such as infant mortality rate and under-5 mortality rate.
Instead of inducing moral hazard, as the literature suggests, it appears that the
government does not change their spending patterns based on remittance levels. While
the results on remittances and health outcomes are consistent with the literature (e.g.,
remittances have an effect on health outcomes), remittances do not appear to have a
significant association with health spending measures, including out-of-pocket payments
or expenditure per capita. This indicates that the channel through which remittances
impact health outcomes is not likely through direct health spending.
Robustness checks analyzing household and government consumption strengthen
the case that remittances primarily impact health outcomes through more stable and
enhanced household consumption. Remittances increase the amount of disposable income
at the household level, which may be invested in improving housing conditions or
increase availability of food. These channels appear to have a stronger impact than direct
health spending.
Unlike infant mortality rate and under-5 mortality rate, which are associated with
many social determinants of health, such as housing, food access, nutrition and family
security, maternal mortality reflects direct access to health services. The results for
maternal mortality support the hypothesis that maternal mortality ratio will not be driven
by remittances, and instead, depend on the health system overall.
15
Based on the results from this study, governments should consider the following
interrelated policy solutions, which weigh the positive effects of remittances against the
potentially adverse macroeconomic effects:
First, the data on health spending and health outcomes suggest that total
health spending should increase. If migrants are spending more money on non-health
services and durable goods, such as food or improvements to living conditions, then
policy makers should respond by investing in public health expenditure to increase total
health spending. This policy recommendation is also aligned with the World Health
Organization’s (WHO) efforts to increase universal coverage for health and reduce
reliance on out-of-pocket spending, or the money that people spend on health care
services directly. The data show that out-of-pocket payments do not have a statistically
significant effect on health outcomes, which indicates that they should not be promoted
as a measure to improve health outcomes.
Second, governments should implement policy reforms to make it easier for
migrants to send remittances back home. Remittances appear to have a sustained and
consistent relationship on key health outcomes, such as infant mortality rate and under-5
mortality. This positive effect suggests that governments should open the channels
through which remittances flow to increase the disposable income available to
households, especially those who heavily rely on remittances as part of their household
income. To account for potential negative effects, or the flow of illicit money without
oversight, the international community should increase efforts toward improving
government and regulatory frameworks. While making it easier for migrants to send
money home can help at the household level, remittances are comprised of many sources
16
of funding, suggesting that more comprehensive financial channels should be in place to
maximize the benefits of remittances and reduce the potentially negative consequences.
Third, although governments should promote remittances for household
consumption, national governments should consider alternative routes to increase
household consumption. For example, governments can create or continue to invest in
social protection programs that increase the availability of cash to program eligible
households. In doing so, these types of programs can increase household consumption,
which appears to be a driving force behind the reductions in mortality rates. This policy
measure could be implemented in conjunction with the first recommendation regarding
increasing total health spending.
Chapter 5: Conclusions and Limitations
As governments consider the policy recommendations described above, policy
makers should consider the inherent trade-off regarding remittances. While increasing
remittances and maintaining a stable flow of household consumption can increase health
outcomes, remittances can also produce negative macroeconomic consequences, such as
inflation or higher exchange rates. Facilitating the flow of remittances to benefit
households could also inadvertently lead to the higher flow of illicit funds. Furthermore,
the effect of remittances on chronic diseases, such as diabetes, remains unknown. A
future study on the effect of remittances on chronic diseases, such as diabetes, which tend
increase over time with lifestyle changes, would likely result in another negative outcome
associated with remittances.
In light of this policy trade-off, policy makers should reform remittance policy
within a more comprehensive framework to mitigate the concerns. More work should be
17
directed toward improving financial regulation and governance to facilitate the growth of
remittances in low- and middle-income countries, but maximizing the beneficial effects.
Furthermore, governments should increase health spending to complement the higher
household consumption to increase health outcomes, such as infant mortality rate and
under-5 mortality rate, and improve health outcomes, such as maternal mortality ratio,
that primarily depend on the existing health system instead of social determinants of
health.
The main limitations of this study were the following. First, the time period used
was determined based on the availability of health spending data, which only began to be
collected on an international level in 1995. Therefore, the effect of remittances and health
outcomes used in this study was restricted to a 20-year time period. Second, remittances
are underreported given that these data only capture formally recorded remittances.
Others have also noted inconsistency in data reporting across countries.21 Third, there is
missing data across the three areas of interest: remittances, health outcomes and health
spending. Therefore, it is possible that the results may change over time or when a more
complete dataset is available.
The international community and many national governments have been using
remittances as a tool for development for some time. While this study supports that
remittances should continue to be used to increase household consumption, it is important
that governments do not rely on remittances as the sole mechanism for health
improvements. It is evident that remittances can be a driving force to improve health
outcomes, especially those that rely on social determinant of health, but remittances fall
short of being a panacea for all health problems. Long-standing health issues such as

18
maternal mortality ratio and the growing burden of chronic diseases will require other
solutions that go beyond increasing household consumption. Therefore, governments in
developing countries, along with partners in international health funding institutions,
should continue to identify innovative ways to use remittances and other funding sources
more effectively.

19
Table 1: Description of World Development Indicators
Variable Short form Type Source (as described in WDI)
Personal remittances, received (current
US$)
Remitusd Independent
World Bank estimates based on IMF balance of payments data,
and World Bank and OECD GDP estimates
Personal remittances, received (% of GDP) Remitgdp Independent World Bank estimates based on IMF balance of payments data,
and World Bank and OECD GDP estimates
Health expenditure, public (% of GDP) exppubGDP Dependent
WHO Global Health Expenditure database
Health expenditure, public (% of
government expenditure)
exppubGOVEXP Dependent WHO Global Health Expenditure database
Health expenditure, public (% of total
health expenditure)
expPUBTHE Dependent WHO Global Health Expenditure database
Health expenditure, total (% of GDP) expGDP Dependent WHO Global Health Expenditure database
Health expenditure per capital (current $) expCAP Dependent WHO Global Health Expenditure database
GDP per capita (current US$) gdpCAP Control
World Bank, International Comparison Program database
Urban population (% of total) urbanPOP Control
World Bank
GDP growth (% annual) gdpgro Control
World Bank
Life expectancy at birth, total (years) Lifexpect Control/Dependent
UNPD and others
Mortality rate, under-5 (per 1,000) mortund5 Dependent UN Inter-agency for Child Mortality Estimation
Maternal mortality ratio (modeled
estimate, per 100,000 live births)
Maternmort Dependent UN Inter-agency
Mortality rate, infant (per 1,000 live births) Imr Dependent
UN Inter-agency for Child Mortality Estimation

20
Table 2: Descriptive Statistics (1995-2011)
Variable N Mean SD Min Max
Remitusd 2786 1.66 e+09 4.17e +09 0.00 6.88e+10
Remitgdp 2725 4.06 6.85 0.00 61.99
exppubGDP 3184 3.70 2.35 0.00 21.11
exppubGOVEXP 3180 11.09 4.63 0.00 42.38
expPUBTHE 3181 57.22 20.34 0.39 99.98
expGDP 3184 6.28 2.69 0.00 22.19
expCAP 3182 674.344 1276.119 0 9120.81
gdpCAP 3479 10727.47 18016.55 64.81 1.94e+05
urbanPOP 3726 55.32 24.47 7.21 100.00
gdpgro 3434 4.076798 5.748358 -47.553 106.2798
Lifexpect 3318 67.83558 10.10695 31.239 85.16341
Maternmort 517 163.9222 275.7378 0 2100
mortund5 3438 50.78365 53.0938 2.2 278.9
imr 3438 35.42693 32.18131 1.7 153.1
21
Table 3: Effects of Remittances (USD) on Health Outcomes
Infant Mortality Rate Under-5 Mortality Rate Maternal Mortality
(1) (3) (4) (5) (1) (3) (4) (5) (1) (3) (4) (5)
ln_remitusd -3.960*** -1.435*** -1.052*** -0.143** -6.407*** -2.441*** -1.699*** -0.289** -16.33*** -3.191 -0.268 -0.847
(-0.561) (-0.41) (-0.293) (-0.0569) (-1.013) (-0.749) (-0.517) (-0.121) (-5.863) (-5.549) (-5.072) (-1.528)
gdpCAP
0.000400*** 8.02e-06**
0.000697*** 2.93E-05
0.00229 -0.000243
(-0.0000831) (-0.00000367)
(-0.000151) (-0.0000208)
(-0.00276) (-0.000315)
urbanPOP
-0.462*** 0.00623*
-0.789** 0.00915
4.469 -0.0171
(-0.171) (-0.00332)
(-0.357) (-0.00655)
(-2.954) (-0.109)
gdpgro
-0.0369 -0.00979
-0.0176 0.00741
-1.504 -0.104
(-0.0338) (-0.0102)
(-0.0638) (-0.0718)
(-1.055) (-0.392)
lifexpect
-2.113*** -0.0166
-4.237*** -0.236
-29.78*** -0.676
(-0.287) (-0.0213)
(-0.621) (-0.183)
(-5.771) (-0.505)
imr/mortund5/maternmort
0.970***
0.921***
0.904***
(-0.00599)
-0.0366
(-0.0505)
Year
X X
x X
x x
Country
X X
x X
x x
Constant 109.6*** 67.55*** 221.8*** 3.662** 170.6*** 104.6*** 408.0*** 23.27 531.9*** 200.3 1,890*** 0
(-11.74) (-7.826) (-21.29) (-1.78) (-21.22) (-14.45) (-44.34) (-15.06) -122.7 -126.9 -329.1 0
Obs 2,556 2,556 2,460 2,460 2,556 2,556 2,460 2,460 432 432 420 145
# countries 171 171 170 170 171 171 170 170 131 131 127 49
chi2 49.79
258234 40.03
129318 7.753
225657
hansenp
0.795
0.463
0.697
sarganp
0.468
1
0.714
R-squared 0.501 0.715 0.398 0.64 0.16 0.349
Notes: Robust standard errors in parentheses; *** p<0.01, ** p<0.05, * p<0.1; Models (1): Simple OLS; (2): OLS + year fixed effect; (3): OLS + year and country fixed effect; (4): Fixed effect; (5): GMM

22
Table 4: Effect of Public Health Spending (% of Government Expenditure) on Health Outcomes
Infant Mortality Rate Under-5 Mortality Rate Maternal Mortality
(1) (3) (4) (5) (1) (3) (4) (5) (1) (3) (4) (5)
ln_exppubGOVEXP -4.164** 0.289 -0.364 -0.147 -8.116** -1.051 -2.516 -0.692* -83.54*** -80.14** -81.88** 5.591
(-1.932) (-1.298) (-1.132) (-0.174) (-3.602) (-2.503) (-1.962) (-0.418) (-29.63) (-35.11) (-35.67) (-5.875)
gdpCAP
0.000395*** 1.05e-05***
0.000693*** 3.24e-05**
0.00483* -0.000315
(-0.0000683) (-0.00000308)
(-0.000125)
(-0.0000159)
(-0.00261)
(-0.000325)
urbanPOP
-0.332** 0.00443
-0.620* 0.00601
4.442 0.0503
(-0.158) (-0.00307)
(-0.326) (-0.00592)
(-2.909) (-0.0809)
Gdpgro
-0.02 -0.0106*
-0.0144 -0.00616
-1.127 0.0845
(-0.0483) (-0.00594)
(-0.0825) (-0.0375)
(-1.16) (-0.339)
Lifexpect
-2.189*** -0.0370**
-4.343*** -0.24
-27.00*** -0.615
(-0.269) (-0.0171)
(-0.558) (-0.164)
(-5.539) (-0.544)
imr/mortund5/maternmort
0.969***
0.927***
0.913***
(-0.00566)
(-0.0324)
(-0.0473)
Constant 44.13*** 41.89*** 202.2*** 2.843** 68.01*** 64.16*** 380.9*** 19.66 412.3*** 315.7*** 1,871*** 0
(-5.078) (-3.046) (-18.24) (-1.377) (-9.463) (-5.944) (-36.66) (-12.75) (-73.93) (-102.2) (-332.3) 0
Obs 3,178 3,178 2,961 2,961 3,178 3,178 2,961 2,961 488 488 471 155
# countries 190 190 185 185 190 190 185 185 150 150 142 51
chi2 4.644
435108 5.078
186883 7.95
163396
Hansenp
0.0683
0.275
0.619
Sarganp
0
0.974
0.145
R-squared 0.486 0.699 0.395 0.642 0.182 0.337
Notes: Robust standard errors in parentheses; *** p<0.01, ** p<0.05, * p<0.1; Model 1: Simple OLS; Model 2: OLS + year fixed effect; Model 3: OLS + year and country fixed effect; Model 4: Fixed effect; Model 5: GMM
23
Table 5: Effect of Remittances on Health Spending Measures
exppubGOVEXP expcap exppubGDP expOOPthe
Model 4 Model 5 Model 4 Model 5 Model 4 Model 5 Model 4 Model 5
ln_remitusd 0.0543 0.260* ln_remitusd -18.87** 1.96 ln_remitusd -0.0166 0.0515 ln_remitusd -0.0666 0.064
(-0.115) (-0.139) (-8.798) (-5.555) (-0.0339) (-0.0324) (-0.456) (-0.313)
gdpCAP 2.36E-05 2.24e-05*** gdpCAP 0.101*** 0.00223 gdpCAP 1.50E-05 1.06e-05*** gdpCAP 6.65E-05 -3.04e-05***
(-0.0000211)
(-0.00000635)
(-0.00577)
(-0.00181)
(-0.00001)
(-0.00000232)
(-0.0000453)
(-0.00000924)
urbanPOP -0.0558 -0.00496 urbanPOP 1.155 0.260** urbanPOP 0.00934 9.79E-05 urbanPOP -0.284 -0.00225
(-0.0646) (-0.00604) (-6.521) (-0.104) (-0.0201) (-0.0012) (-0.207) (-0.00685)
Gdpgro -0.0411** -0.0115 gdpgro -1.061 1.220** gdpgro -0.0121** 0.00207 gdpgro 0.0341 -0.0202
(-0.0184) (-0.0152) (-1.03) (-0.48) (-0.00486) (-0.00281) (-0.0399) (-0.0282)
Lifexpect 0.058 -0.00637 lifexpect -1.633 0.348 lifexpect 0.0122 -0.00213 lifexpect -0.0706 -0.0038
(-0.153) (-0.0152) (-2.992) (-0.396) (-0.0388) (-0.00358) (-0.176) (-0.0338)
exppubGOVEXP
0.779*** expCAP
1.022*** exppubGDP
0.890*** expOOPTHE
0.940***
(-0.0274)
(-0.0196)
(-0.0159)
(-0.0133)
Year X Year X Year x
Country X Country X Country x
Constant 8.433 -1.681 Constant 237.3 -89.38 Constant 2.245 -0.503 Constant 55.85*** 1.827
(-11.34) (-1.821) (-411.5) (-79.66) (-2.961) (-0.43) (-19.12) (-3.32)
Obs 2,303 2,303 Obs 2,303 2,303 Obs 2,305 2,305 Obs 2,305 2,305
# countries 168 168 # countries 168 168 # countries 168 168 # countries 168 168
chi2
2295 chi2
259681 chi2
13380 chi2
50334
Hansenp
0.495 hansenp
0.442 hansenp
0.0872 hansenp
0.227 Sarganp
1.97E-05 sarganp
0.18 sarganp
5.57E-06 sarganp
0.0122
R-squared 0.091 R-squared 0.844 R-squared 0.212 R-squared 0.059
Notes: Robust standard errors in parentheses; *** p<0.01, ** p<0.05, * p<0.1; Model 1: Simple OLS; Model 2: OLS + year fixed effect; Model 3: OLS + year and country fixed effect; Model 4: Fixed effect; Model 5: GMM

24
References
1. Jamison DT, Summers LH, Alleyne G, et al. Global health 2035: a world
converging within a generation. The Lancet. 2013;382(9908):1898-1955.
2. World Bank. World Development Report 1993: Investing in Health. Washington,
D.C.: The World Bank;1993.
3. World Health Organization. The World Health Report: Health System Financing:
The Path to Universal Coverage. Geneva, Switzerland: World Health
Organization;2010.
4. Daniels ME, Donilon TE, Bollyky TJ. The Emerging Global Health Crisis:
Noncommunicable Diseases in Low- and Middle-Income Countries. New York,
NY: Council on Foreign Relations;2014.
5. Farag M, Nandakumar A, Wallack S, Hodgkin D, Gaumer G, Erbil C. Health
expenditures, health outcomes and the role of good governance. Int J Health Care
Finance Econ. 2013;13:33-52.
6. Nixon J, Ulmann P. The relationship between health care expenditure and health
outcomes. Evidence and caveats for a causal link. Eur J Health Econom.
2006;7:7-18.
7. World Bank. Migration and Remittances Factbook 2016. Washington, D.C.: The
World Bank;2016.
8. Brown S. Can Remittances Spur Development? A Critical Survey. International
Studies Review. 2006;8:55-75.
9. Vassall A, Martinez-Alvarez M. The health system and external financing. In:
Smith RD, Hanson K, eds. Health Systems in Low- and Middle-Income Countries:
An Economic and Policy Perspective. Oxford, England: Oxford University Press;
2012.
10. Amuedo-Dorantes C, Sainz T, Pozo S. Remittances and Healthcare Expenditure
Patterns of Populations in Origin Communities: Evidence from Mexico. Vol
112007.
11. Amuedo-Dorantes C, Pozo S. Remittances and Income Smoothing (Discussion
paper no. 5568). Bonn, Germany: Institute for the Study of Labor;2011.
12. Acevedo C, Cabrera M. Social policies or private solidarity? The equalizing role
of migration and remittances in El Salvador. In: Cornia G, ed. Falling inequality
in Latin America: Policy Changes and Lessons. Oxford, United Kingdom: Oxford
University Press; 2012:164-187.
13. Mughal M. Remittances as development strategy: Stepping stones or slippery
slope? . Journal of International Development. 2013;25:583-595.
14. Ahmed FZ. Remittances deteriorate governance. The Review of Economics and
Statistics. 2013;95(4):1116-1182.
15. Tyburski MD. The resource curse reversed? Remittances and corruption in
Mexico. International Studies Quarterly. 2012;56:339-350.
16. Mundaca G. Remittances, Financial Market Development, and Economic Growth:
The Case of Latin America and the Caribbean. Review of Development
Economics. 2009;13(2):288-303.

25
17. Nyamongo EM, Misati RN, Kipyegon L, Ndirangu L. Remittances, financial
development and economic growth in Africa. Journal of Economics and Business.
2012;64:240-260.
18. Ratha D. The Impact of Remittances on Economic Growth and Poverty.
Washington, D.C.: Migration Policy Institute;2013.
19. Chami R, Barajas A, Cosimano T, Fullenkamp C, Gapen M, Montiel P.
Macroeconomic Consequences of Remittances.
Washington, D.C.: International Monetary Fund;2008.
20. McKenzie D. Beyond remittances: the effects of migration on Mexican
households. International migration. 2005.
21. Zhunio MC, Vishwasrao S, Chiang EP. The influence of remittances on education
and health outcomes: a cross country study. Applied Economics.
2012;44(35):4605-4616.
22. Ponce J, Olivie I, Onofa M. The role of international remittances in health
outcomes in Ecuador: prevention and response to shocks. International Migration
Review. 2011;45(3):727-745.
23. López-Cevallos DF, Chill C. Migration, remittances, and health care utilization in
Ecuador. Rev Panam Salud Publica. 2012;31(1):9-16.
24. Ebeke CH. Do Remittances Lead to a Public Moral Hazard in Developing
Countries? An Empirical Investigation. Journal of Development Studies.
2012;48(8):1009-1025.
25. Doyle D. Remittances and Social Spending. American Political Science Review.
2015;109(4):785-802.
26. Naanwaab C, Yeboah OA. Migrant remittances and human capital investments.
Review of Applied Socio- Economic Research 2013;6(2):191-203.
27. Duryea S, Lopez Cordova JE, Olmedo A. Migrant remittances and infant
mortality: evidence from Mexico. Washington, D.C.: Inter-American
Development Bank;2005.
28. Adams RH. Evaluation the Economic Impact of International Remittances on
Developing Countries Using Household Surveys: A Literature Review. . Journal
of Development Studies. 2011;47(6):809-828.
29. Amuedo-Dorantes C, Pozo S. New evidence on the role of remittances on
healthcare expenditures by Mexican households. Rev Econ Household. 2009;9:69-
98.
30. Kanaiaupuni S, Donato K. Migradollars and mortality: The effects of migration
on infant survival in Mexico. Demography. 1999;36(3):339-353.
31. Valero JN. Remittances and the household’s expenditures on health. Munich
Personal RePEc Archive;2008.
32. Abdih Y, Chami R, Dagher J, Montiel P. Remittances and institutions: Are
remittances a curse? Washington, D.C.: International Monetary Fund;2008.
33. Makuta I, O'Hare B. Quality of governance, public spending on health and health
status in Sub Saharan Africa: a panel data regression analysis. BMC Public Health
2015;15:932-943.
34. Cen Caamal M. Remesas y estructura del gasto en los hogares receptores: Caso de
estudio de una comunidad maya contemporanea. (Remittances and Expenditure

26
Structure of Recipient Households: A Study Case of a Contemporary Mayan
Community. With English summary.). Analisis Economico. 2012;27(64):5-21.
35. Hernandez-Coss R. The U.S.-Mexico Remittance Corridor: Lessons on Shifting
from Informal to Formal Transfer Systems. . Washington, DC: World Bank;2005.
36. The World Bank. Mexico’s Financial Inclusion Strategy. 2010;
http://siteresources.worldbank.org/FINANCIALSECTOR/Resources/282044-
1260476242691/Mexico_Financial_Inclusion.pdf Accessed December 1, 2015.
37. Orozco M. Mexican Hometown Associations and Development Opportunities.
Journal of International Affairs. 2004;57(2):1-21.
38. Loewenson R, Gilson L. The health system and wider social determinants of
health. In: Smith RD, Hanson K, eds. Health systems in low- and middle-income
countries. New York, NY: Oxford University Press; 2012.