THE EFFECT OF NURSE TEACHING INTERVIEWS v ON...
83
The effect of nurse teaching interviews on patients with emphysema Item Type text; Thesis-Reproduction (electronic) Authors Wheeler, Dorothy Fern, 1921- Publisher The University of Arizona. Rights Copyright © is held by the author. Digital access to this material is made possible by the University Libraries, University of Arizona. Further transmission, reproduction or presentation (such as public display or performance) of protected items is prohibited except with permission of the author. Download date 05/07/2018 09:40:12 Link to Item http://hdl.handle.net/10150/318325
Transcript of THE EFFECT OF NURSE TEACHING INTERVIEWS v ON...

The effect of nurse teaching interviewson patients with emphysema
Item Type text; Thesis-Reproduction (electronic)
Authors Wheeler, Dorothy Fern, 1921-
Publisher The University of Arizona.
Rights Copyright © is held by the author. Digital access to this materialis made possible by the University Libraries, University of Arizona.Further transmission, reproduction or presentation (such aspublic display or performance) of protected items is prohibitedexcept with permission of the author.
Download date 05/07/2018 09:40:12
Link to Item http://hdl.handle.net/10150/318325
THE EFFECT OF NURSE TEACHING INTERVIEWS v ON PATIENTS WITH EMPHYSEMA
Dorothy Fern Wheeler
A Thesis Submitted to the Faculty of theCOLLEGE OF NURSING
In Partial Fulfillment of the Requirements For the Degree ofMASTER OF SCIENCE '
In the Graduate CollegeTHE UNIVERSITY OF ARIZONA
1 9 7 0
■ t i + f t , . ' :
M i o ' .
STATEMENT BY.'AUTHOR.:
This thesis has been 'submitted.. in pabtial fulflllmeht df requirements for an advanced degree at The University of Arizona ,and is ■ deposited in the University Library to be made available to borrowers under'rules of the Library.
Brief, quotations from -this thesis are allowable without special permission, provided that accurate acknowledgment of source is made. Requests' for permission for extended quotation from or reproduction.of this manuscript in whole or in part may be granted by the head of the major department or the Dean of the Graduate College when in his judg- ■ ment the proposed use of the material is in the interests.of scholarship., In all other instances, however, permission-must be -obtained, from the author, ..
■ APPROVAL BY THESIS DIRECTOR ■This thesis' has been approved' on the date shown belowj
VIRGIITA J. MILLER 'Associate Professor of Nursing
g /DaGT i d ? ? #
ACraOMLEDGMENT-
Appreciation is expressed to members of my thesis committeej to Dean'.Gladys Sdrensen,- for her advice and valuable suggestions; to . Dr . Janelle. Krueger , f or her. assistance:, in development of the statistical' analysis; to Miss Virginia Miller, who as chairman, gave encouragement and unfailing support throughout the course of the project.
For guidance, early in .the study, appreciation is expressed to Dr. Robert C. Leonard.
.Particular thanks is given to personnel at the Veterans' Administration Hospital, Tucson, Arizona; to Miss Janice Woram, Chief, Nursing Service, and to Mrs., Betty Longstaff, Head Nurse Pulmonary ..Diseases Ward, for providing facilities in which I could work; to Dr * Louis Keitel, Chief of Pulmonary Diseases Section, for development of the questionnaire; and to Mrs» Evangeline Terrazas, Director of • Inhalation Therapy, for administration of the questionnaire.
TABLE OF CONTENTS
■ .. ^ ; : ;P a g e
■ LIST .OF•. TABLES.- © © @ © © « © © © . * ©. © © • © © « © © © © © © © © ©* vzl
v ABSTRACT c © @ © © © © © © © © © © © © © © © © © © © © © © © © © ■ vilxChapter" . .
I TEE. PROBLEM AMD DEFINITIONS OF TERMS USED . . . . , . . TThe. Problem © © © © © © © © © © © © © © © © © © © © 2Purpose of the Study © © © © © © © © © © © © © © © 3
’ . Definitions of Terms Used . . . « « = i t . . . « . 14-Chronic Bronchitis . . . . . . . . , . . . . . IfChronic Obstructive Pulmonary Disease . i . . . IfCopm§ Ability o o » o @ o @ 6 * * @ * « o * o IfEmpiiy s ema o * » © » o © • © o « « « « o • © © © If
• ■ . Expressive Nursing • © . . . . . © © © . © . . ©. If.Interview © * © . . . . © © © © © ©. © © * . © © 5
: "1 Non-participant Observer . « « ... . © . . © © ." 5: Pulmonary Function Test . © © . © . . © . ... . © 5Teaching © . . © © * © © © ©. © © .© © . . © ^Therapy © © * © © . © .© . . © . © ©. ©© . © ^
II . REVIEW OF THE LITERATURE © o o » n o b © o © , © © e
Teaching as. a Function of Nursing . . . . . . . . . . 6The Feelings of the Patient 9
- Identifying the Patient’s Needs and Making Him an Active Participant on the. Health Team , . . . . © . . © © © . © © o © . * . 11
Concept of the Team Approach and the Nurse’sRole on the Health Team . . .'... . . © © © . © 13
III RESEARCH DESIGN . . . . . . . . V © © . . . © , '. © . . l6Hypothesis © © © © © © © © . . © . © © © © © * © . 1^Operational Definitions ©■ . . . . © . . . .' . © . © ' 18
; Selection of the Sample © © © © . © i . . . . . . . 19Limitations of the Study . • © -. . . . ... . . .' . 19
IV

V
■ ' ".TABLE OF COH,EECS---Continued.Chapter Page
IV / DEVELOPMENT OF THE STUDY . . . . . . . . . . . . . . . . 21
Nurse.Teaching Interview . . . . . ... . . . . . . . 21Le s s on. Plari ... . .. © « « © . . » . . © . . © 22.Demonstration and Practice of
Breathing Exercises .' . . .. .■• « . '. . . 231 1 Assessraerit of . Readiness of the Patient ,
..' .iV p : .-Leap n^... ...... .■ -«. . * : . ... « '.»•• "' 2k... -Measurement-and Evaluation . .. .. . ». . . . . 2<5
Development of the Questionnaire . . . . . . . ,. .2.6Development of the Ohjective Measurement . . . ... 27
V DATA COLLECTION. ,.. .. .■ •. . . . . . . . . . . .. . 29 .Overall Collection Time . . ... . . '. . . . . . • 29
Typical Time Schedule . . . . . . . . . . . . . 30Initial Approach to Patient . . . . . . . . . . . . . . 30Admirii strati on of. the Questionnaire . . . . . . . . . 31
Control Group - . . . . . . . . . . . . . . . . . 31■ Experimental Group . . . . . . . . . . . . . . . i 32
; Admiriistration of the Objective Measurement . .... I 3 3... VI - ANALYSIS OF DATA . . . . . . . . . . . . . . ; . . . .- .. . 35
Direction of Change • ... . .: . . . . ’ . ; . . . . . i .' . 37Questionnaire . . . . . . . . ... . . „ . . . . . . 38
■ Objective. Measurement •. .. . . ... . .' . i V . . .. . rioProfile of the Patient . . , . ... . . . . . . . ... . k2 '
VII . SUMMARY, RECOMMENDATIONS AND CONCLUSION ; V . . . . . . . kh-" : - ■ Sumraary ■© © © . * . . . - . « . . . © » ... . * . * .
... Recommendations . . . . . . . . . . .' . . . . . . . 46Conclusion © . . . * . © » . . . . . . . . . . . . * 47
APPENDICES: INSTRUMENTS USED IN THE STUDY . . . ...V . . . . . • "• 4$: . ■ APPENDIX A.: AGREEMENT . .. .. . . . ... V . . . i . . . 50
APPENDIX, B: PROFILE OF PATIENT V . . . . . 51" APPENDIX C : RECORD OF SESSION WITH PATIENT ■ '. . . . 53APPENDIX D: LESSON PLAN .. . . . . . . . . . . . . . 54APPENDIX E: QUESTIONNAIRE . . . . . 65APPENDIX F: OBJECTIVE MEASUREMENT . . . . . . . . . . 68
LIST.OF REFERENCES . . . . . . . . . . . . . 70 .

LIST OF TABLES
Table . PageT ' Raw Scores on Pretests and Posttests . . . . . . . .....' . . 36II Mean Questionnaire Scores of Control and
;: .E^erimental Group" , « « . e . . « < , « « <, « 0- :» <>/ . 38III .Questionnaire Scores by. Percentages of Control
and Experimental Group » « « ■« . <,<,«, * « . . ■ 40
IV Mean Objective Measurement Scores of Controland Experimental Group , . « . . . » « , 0 . .« <> .. « « ' 4.1
V Objective Measurement Scores by Percentages ofControl and Experimental Group <, . * . . . . , . ,■ „ 42

ABSTRACT
A controlled quasi-experimental study was conducted measuring the'effects of nurse teaching interviews on the emphysema patient’s ■ comprehension of.his disease process and his coping ability. A teach"'itig iristmment> 'in the form of a lesson plan and diagrams, was developed and used in two twenty minute interviews with each of ten patients in .:an experimental' group. An equal number of patients in a control group had.noh-directed nurse-patient interviews. Instruments, in the form of a questionnaire and an objective rating.scale, were developed and used as pretests and. posttests to measure the effects of the nurse teaching interviews. 'g -■ /'
The changes in the measurements were statistically.significant with the findings of the questionnaire at the .05 level and the objective measurement at the .01 level, The.study, supported the hypothesis that the nurse teaching interviews improve the emphysema patient’s comprehension of his disease process and of his coping ability. The patient who was individually instructed about his disease and self care by a nurse who encouraged,him to discuss his anxieties and frustrations did have fewer misunderstandings about his disease.and greater confidence in his ability to live within his physical limitations than the patient who did not have such instruction.

CHAPTER I
THE PROBLEM AND DEFINITIONS OF TERMS USED.
Mortality.,, morbidity, and disability from emphysema.:Have risen .v;»*v..ja..':1"sp§.Q-taeu4,ai;<.In the United States and particularly in Arizona. Part of this is attributed to a growing awareness of.the disease through increased medical recognition and part is due to the large, in- migration of people who come to the warm, dry climate for retirement and for health reasons, particularly respiratory problems (Poulsen,. 1967)o
The national mortality rate for emphysema, and chronic bronchitis in 1963 was 9«3 deaths per 100,000 population but in Arizona the rate was 37»3 deaths per 100,000 population (Cppenheimer, 1965, p® l)o In 1966 the Arizona mortality rate from diseases categorized %s "Other Bronchopulmonic Diseases (principally emphysema)" had.risen to k-6 deaths per 100,000 population (Arizona State Department of Health Vital Statistics for 1966, p. 13). In males, 45-61 years of age, emphysema was the fifth ranking cause of death and in males 65-74 years of age emphysema rose to the fourth ranking cause of death in Arizona (Arizona State Department of Health Vital Statistics, for. 1966, p . ,11) <, Dr . ' Poulsen of the Arizona State Health' Department terms Arizona, the "black spot on the map"- because its mortality rate is over twice as high as.any other state in the nation (Poulsen, 1967, pp. 2 , 3).
A survey of patients discharged from Arizona hospitals in March of 1967 showed that patients with chronic respiratory diseases totaled
1,577 discharges with 9/392 days .of hospital stay at-a total cost of hospitalization of $469,600 (Poulsen, 1967, p, 3 ), Multiplying these . figures by twelve would give a reasonable estimate of the annual cost of hospital care alone. Costs not estimated are physicians' servicesy. -.nursing home care, home health services,, drugs, x-rays, laboratory
... services and equipment.On a national level, "the incidence of. emphysema in-men'has
been reported to be as much as ten,times, greater than in.women, and a/b .least twice as great in .white males as in Negro males" ■ (.Chronic - Obstrue . tive Pulmonary Disease: A Manual for Physicians, 1965, p. 13)« TheReport of the Task Force on Chronic Bronchitis and Emphysema, .(1966), estimates that there may be as many as 14,000,000 persons in the nation with some degree of chronic obstructive pulmonary disease. Emphysema is now second only to heart disease as the cause of disabled workers under 65 years of age (Robbins et al., 1969, p. 77). ,Social Security payments represent only a fraction of the cost of emphysema, 'Bradley (1968, p. 4l) says "Annual disability benefits by Social Security in ■ working men over 40 exceed 800 million.dollars . , . and this disability is expected to increase, . '
■' V The Rroblem \ . ‘Many emphysema patients do not:'participate fully in the plan
of treatment prescribed by their physician and therefore the outcome • of their therapy is not as successful as it could be. In order for patients to be active participants in their plan, of treatment they
- must understand the basic physiology of their, respiratory difficulty and the objectives of therapy (Petty and Nett, 1967). Persons with

. ' 3
emphysema, often, experience- a cycMc reacti.w of anxietbyf:rustration/ /confusion^ and'irritability which compounds their problem - of dyspnea 0 Information is given to them by doctors, nurses} therapists and others but they are unable to comprehend it in order, to wholly utilize it. If their:anxiety could be decreased and their conf idence-increased, • many " '.avenues. of self-help" would be , opened- for them'.' The nurse., through, her expressive role in nursing, .or patient-i-centered. therapy, pan intervene to. decrease'the patient’s anxiety and help him to understand his disease process - and. plan of therapy. y. . ' . . .
se of., the . Study It is.the purpose of-this project to study the effects on
emphysema patients of two nurse teaching interviews which, are designed to focus on the patient’s comprehension of his disease and his coping ability. \ . -. . .
• This study was undertaken with the concept of making the patient a more active participant of the health team. It is thought that:l) a patient will be more ready to cooperate if he understands, his disease, process and plan for therapy;.2) nurse teaching interviews, which embody anxiety relieving techniques, with, information, giving, can be used to increase the patient’s, confidence in himself and his coping • ability; 3) patient.centered nursing has positive effects on the patient’s welfare. .
This problem is worthy of investigation because of the growing magnitude of persons affected With emphysema, the cost to society of disabilities resulting from emphysema, and the difficulties of

X working with' these afflicted persons because of their anxiety, depres sion, and hostility. .... ...
. Definitions of Terms Used .Chrpbic.Bronchitis ' . ■
.A long standing infiammation of the bronchi characterized by -excessive mucous secretion in the bronchial tree and-manifested by a-
• persistent .or, recurrent productive cough..
Chronic Obstructive Pulmonary Disease ; . • ■ ' .A term encompassing all conditions which exhibit persistent
obstruction of the bronchial airflow. It includes chronic bronchitis emphysema and asthma.
Coping AbilityThe patient's reaction to his illness, or what he can do to
handle his problems more successfully.
Emphysema .Abnormal enlargement of the air spaces distal to the non- .
respiratory bronchiole, accompanied by destructive changes in the alveolar walls. There is difficulty in exhaling air from the lungs' and poor distribution of inhaled air throughout the lungs.
Expressive NursingTerm used interchangeably with "patient centered nursing,"
focuses on how the patient is defining his situation in order to reduce his.distress, confusion, and misunderstanding.
.InterviewA meeting of people face to face to cozmnunicate. ideas. It is
always purposeful,.meaningful, and goal directed.
Non-participant ObserverOne administering the questionnaires in this study» This per-
* son was■director of the inhalation therapy department and also, a registered nurse« - /y • • ' ; ;
Pulmonary Function Test ■Measurement .of "breathing capacity, usually with a spirometer.
A diagnostic tool to help differentiate the diagnosis" of emphysema from other chronic obstructive pulmonary diseases« Timed" expiratory flow is the most distinguishing test, being abnormally decreased in
.;. emphysema,
TeachingGuidance toward learning or the giving of. information. The
situation may be altered by the patient's ability to understand and ; by his emotional readiness to learn, . Teaching may vary from simple ■ communication between two people to formal classroom situations.
Therapy. An ongoing process of assisting a person in his struggle with
an illness or a problem. '
CHAPTER, II
: ■ ' V V " '/ / REVIEW OF THE LITERATURE
.. Much has been Witten about the nursing care of emphysema •fpatie'nts, and while teaching is an important function of nprsing, ho . studies have been found,-of clinical research that has been done.with the actual, teaching: of,/.emphysema patients. This review of literature will be from the standpoint of. teaching as a function of nursing, feelings of the patient, .identifying the patient's needs and making him an active participant of the health team* and the concept -of the team approach and the nurse's role on the health team.
'' ",v. % - / . . . Teaching as a Function of Hursing ... ' :The teaching of patients has long been a function of pro
fessional nursing (Streeter, 1953J Simms, 1963) Redman,. 1968). , Webster (i960,, p. 1^95) defines the word teach as n. . . the basic inclusive word for the imparting of knowledge or skills and usually connotes some individual attention, to the learner.” One author delineates the function; of the nurse practitioner as consisting;1 .. . of a system rOf actions intended to induce learning,
which provides activities, materials and guidanoe in informal and formal situations; it includes both the activities of communication and the activities of structured teaching;
. it, is directed toward assisting the learner to achieve his ..; potential; the patient for self direction for health, the , co-workers for the improvement of patient care (Pohl, 1965, p » ll)« • .-
Monteiro (1964) says that the teaching of patients ranges from, simple communications with an individual to formal structured classes, with the simplest kind being the most often neglected, An immediate response to expressed need is meaningful to the patient as the response can be oriented to his present condition and to his future needs as well. Another quite simple form of'tedehing is Of the planned incidental kind in which the nurse directs the conversation toward the area in which the patient needs help« This involves plan ning and making a decision about what the patient needs' to be taught Instead of chatting-while giving care, the adept nurse, can plan the general conversation toward patient teaching, -
Petty, Finigan and Nett (1967, pp« 2, 3 ) stress the importance of teaching the emphysema patient:
The enlightened patient is. most able to cope with his dis-- . ease. Patients can be taught by physicians, nurses, or
. physical therapists. Often the-most efficient method is 'through small group sessions conducted by trained nurses,. with individual instruction as a follow-up. This is an ideal way to reinforce information and tailor instructions to personal needs.The trained respiratory care nurse-is probably the most effective teacher because she is apt to be able to devote more time to teaching and because patients are less apt to fear - asking "stupid questions" that display their ignorance .
Studies of teaching patients with other conditions thanemphysema, have been reported, Molen (1968) studied; the effects ofplanned patient teaching on persons with stasis dermatitis and leg .edema. Before and after tests showed that the group which had theteaching made substantial gains in relation to knowledge, skill inself-care, and attitude, toward their condition, as opposed to- thegroup in which there was no change in the before and after tests.

"Bowen, Rich, -and Schlot'feldt (1961) studied the effects of organized :■ instruction bn patients with diabetes mellitus. Two nurses and a dietitian conducted five periods of organized.instruction. Before and after tests were made to evaluate categories of knowledge, attitudes, .and tests- of skill in the use of the clinitest and the administration of ‘insulin. The patients in the experimental group had considerably- -more gain - in their tests after the instruction as .-opposed to the ebntrol group which did not have the instruction, . .
A study of.patient-centered.and task-centered tuberculosis nursing was described by Drummond (1964)« The patient-centered nursing care was of the supportive type in which the patient felt that
.. someone understood his problems and cared what happened to him as- a person; the taskf-centered .nursing care was of an impersonal type which focused on routine tasks at hand. The patient-centered nursing had. a
. more positive effect on the patients as evidenced by increasing their
.-■staying:power In the hospital. This group followed the plans for treatment.and remained in the hospital until discharged by the physi-
• clan, while the group which received the task-centered nursing had more Irregular discharges of patients.
. Dumas, Anderson, and Leonard (196$) report a clinical experiment on the importance of the expressive function of nursing in the .
■ preoperative preparation of patients for surgery; "There was considerably less postoperative vomiting among the experimental patients, and the only systematic difference in their treatment was that they were talked to by the experimental nurse before they had their' operation (p. 27)."

A study by Egbert,. Welch and Bartlett (1964) was done dh.the rev duction of - postoperative pain by encouragement and instruction of pa-, tients = Patients in the. experimental group, were given instruction by the anesthetist preoperatively. The patients were instructed on how to .relax-, breathe deeply,-and how-to turn in bed in order to remain more comfortable. In comparing' the two groups after surgery, it was found that those who had received the instruction and encouragement required one-half the postoperative narcotics and were- discharged 2,7 days earlier than the patients from the control group which did not have the instruction, A key factor was thought to be that the information-given preoperatively was presented in a manner of enthusiasm and confidence and therefore rapport was established between the anesthetist and the patient"(p, 827)°
. The Feelings of the Patient. ' The emotional problems of the patient with emphysema can be
acute. He may be discouraged at not being able to work, afraid of the prospects of complete invalidism, and anxious during periods of •acute dyspnea. All this only increases the dyspnea and the apprehension. The patient needs a careful explanation of what the problem is, why dispnea occurs, how panic compounds, the problem, and what he. can do to. help himself (Hepper and Hyatt, 1964).:
An emphysema patient describes the feelings of persons with the problem of breathlessness:
We actually experience a perpetual mental burden of appre- . hension, physical tension, constant fright, severe depres- . sion, and conscious and unconscious , irritability ,. .. .

vV'::"': - ; ' v' :: y-' - / '- ; ■ ; ■ V . 10always very close to panic, often irrational, usually stubborn, and mysteriously resistant c «; . frequently beset with feelings of personal inadequacy, and we feel neglected to the point.of
■: complete frustration (Jones, 1967, p. 5^)»’• Garrett, (1953) .sees the disabled person as tending to be un
certain of his ability to cope with the, physical world, of his acceptability in the social world, and of his value as a person.'Wright (i960) states that the disabled person has the choice of coping or succumbing to his condition. In coping, the disability is seen as something that can be faced in some way and overcome. Though recognizing the seriousness of the disability, he focuses on the adjustable , or .coping aspects. In succumbing, the difficulties are seen: . " . , . as a quagmire through which there is no path. Perhaps no path is . sought for one is so consumed with the- suffering that one is dragged down to despair. The difficulties are in command and one succumbs to
■ •'them (p. 59)." . ■ • ' i 1,-; ' \ ■ : '1:.:; ' ■'The coping or succumbing of the emphysema patient depends not
Only on the amount of physical, impairment or disability but on psychosocial components as well. If one believes that work and productivity make a person a real man then disability is looked upon, as frustration and defeat; if one believes that the aim in life is to consume everything one can and to produce as little as one can get away with, then disability is fulfillment. The.emphysema patient * s potential for rehabilitation depends not only on the amount of physical impairment but on his motivation as well (Silver, 1968)« The patient may become
. so breathless after exertion that he avoids physical activity, but encouragement from a figure whose authority is accepted and respected can

. . ' /' \ . , ■ " V n'. often.- 'lacnomplish disproportionately good results. . (Christopherson^ a.968, p, 293).”
Doctors, nurses, and therapists can help the emphysema patient best by encouraging and teaching, the patient and his family how to live with breathlessness, according to Jones (1967)° Instruction in proper posture^ diaphragmatic breathing, isometric exercises, and better breathing habits are most helpful, he says. The slogan for instructions should be, "Everyone in the world has a burden. It is not the burden - that counts but how it is carried (p . $4 )»" Encouragement to; .seek and.find, interests which these patients can accomplish within, the limits of their capacities is also important.
The anxiety level of the patient may be so high that it affects M s ability to focus attention On what the nurse or anyone else is saying to him (Peplau, 1963). Until the anxiety level is decreased it serves as a block to communication. Peplau (1962) suggests some steps . to .mitigate:anxiety: . : ' • '
v I. . Encourage the patient to identify, the anxiety as such . ... . .. P.. Encourage the patient to connect the relief giving patterns
'that he uses, to the anxiety which requires such relief . . . .... 3 . Encourage the patient to provide himself and the nurse with
data, descriptive of situations and interactions which go on immediately before an increase in anxiety is noted . . . .
4 . Encourage the patient to formulate from the descriptive.data the probable immediate situational causes for the increase in his anxiety . . . (p. 53).
Identifying the Patient's Needs and Making Him ; an Active Participant on. the Health Team
Eursing skill in identifying and meeting the patient's needsis important to the welfare of the patient. While Newman (1966)

advocates that the nurse be prepared to identify the patient's needs.in a short-span of nurse-patient interaction. Elder and Leonard saythat effective interaction does'take time* Elder (1963) indicates thatpatients do not adequately communicate their needs as a nurse,initiallyapproaches them, but as the first needs or minor requests are taken careof, other more important needs emerge„ She states, "No doubt, effectivenursing care does require more time at specific stages in a-patient'sillness and hospitalization* However, this factor may be balanced by'the time subsequently saved., (p* 35)«" Leonard (1965, p. 3 )reiterates: . . '
One .can often hear the question, can we afford to spend val- : uable nursing time .in talking with patients? The■ answer may be that a few minutes spent at certain points in the patient's course through the,hospital can result in saving many minutes later on— for example extra time spent on admission or in in- troducing some treatment or care procedure1 may prevent;time- consuming misunderstandings later, on and ineffective use of
. . personnel*. As the aphorism goes: 'A stitch in time.saves .;• nineS* :Furthermore, I will argue, a.genuinely professional level of skill may be required for effective performance of the expressive role in the patient care and cure system*;. Dr* Leonard has collaborated with nurses in a number of clin
ical field experiments for evaluating patient care to substantiate the above statements * The studies were conducted using control groups and experimental groups. Those in the experimental groups received as the experimental treatment a patient-centered or expressive nursing approach in which the nurse focused on how the patient was defining his situation or what, he was thinking and feeling about his hospital experience, The patient was helped to express his feelings and was given information to allay anxiety with the resulting feeling of cooperation and satisfaction of both patient; and nurse (.Dumas and Leonard, 19633. Thornton and

■ : . . ' '■ - ' ' ' ' . ■ ' ; ; . ' 13
Leonard, 1964; Anderson, Mertz, and Leonard, 196$; Dumas, Anderson> and Leonard, 1965; . Elms and Leonard, 1966; Tryon and Leonard, 1966) . ,
Tryon (1963, p« 5?) elaborates on the role of the patient as anactive participant in planning his ’cares. ; V
When a patient "participates in, planning for his care, he as*- ,■ '"'Sumes-.some ''responsibility for the outcome or effect of that
,care:«; He is able to use the health, .resources' offered him store-, effectively„ .When .'a L'a l.lcnlar course of action is suggested he knows why it has been suggested and is able to express his' .feelings about ito . If he questions the advisability of,a particular procedure., his reasons are heard and given consideration... .He is not merely, the object of .treatment but is .a partner
.; in .planning’for his recovery. . Such partnership aids in his ■ recovery..
Tryon also indicates that: the nurse's approach is a determinant in. whether the patient perceives his role as active or passive . If the nurse approaches him with orders and structured questions the" patient is forced into a passive role which limits the interaction;
- if the nurse uses a permissive approach in which open-ended questions . are asked to determine the patient's perception of the situation, he is free to express himself and take on a more active role. Although . the interaction may be initiated by the nurse, the patient is able to continue the interaction, and to express his needs more clearly(pp. 48-57). • .
Concept of the Team Approach and the Nurse *s Role on.the Health Team
Because of the growing emphysema problem, several model projects have emerged utilizing teams of specialists to diagnose, treat, and rehabilitate emphysema patients (Petty, Nett, Bigelow and Ashbaugh,
• 1968; Wundohl and Fackler, 1968; Kass and,Sheets, 1969). One model
project uses a ten. member rehabilitation team including a clinicalchesi; physician, a physiatrish (;a physician who specializes in physicalmedicine), a psychologist, a registered nurse,■ a social worker, ahealth educator, a physical therapist, an occupational therapist,, an
. .inhalation therapist, and a,, pulmonary, function technician (#undohl - and'Packler, 1968, p. 4 ). 'In addition to medical treatment, the projectsemphasize psychosocial factors, physical therapy, and■collaborationbetween the members of the health team« . o
While the physician is the titular leader of the health team(Khudsen,- 1966, pe'.S), the professional nurse also takes/a leadership •role (Coulter, 1968) and functions) as a constant.’in the situation,Knudsen describes the operation of the professionalhealth team in ahospital: ■ , ,• ■ ’ ’ : • . . . ’ ' .
*• The physician diagnoses, prescribes and administers some of '■ the cure functions but he comes and goes, .The laboratory technician enters and exits as he gathers.specimens. The nutri- : tionist.appears to counsel on dietary regime but she is on the
. scene.seldom, .The occupational therapist or the physical . therapist arrive for their functions and depart. The medical
. : social worker may enter the scene sporadically. The patient’. 1 : and his family, if he has one, and the professional .nurse« are.
constants in the situation. Who better but the only professional constant--the nurse, to inform each participant in the health team of the planned behaviours of the others? How else do we form a cohesive plan for action? (Knudsen, 1966, p, 2),
. .; In elaborating on the care of the emphysema patient and therole of the nurse. Helming states: -; For the patient to participate in a plan of care that will. assist him to utilize his optimum functional capacities, two
- : conditions must be met. He must understand his disease—>• the . V ;reasons for his dyspnea, cough and fatigue— and how. the var- . ious therapies assist him to minimize them.:: Then he must be.
provided with the. opportunity to express his feelings.about . his health and given direction to assist him to gain insight into the meanings of his behavior. Hopefully.he can then begin to accept his situation' and cope satisfactorily with the limitations it imposes upon him.
15In collaboration with the physician and other members of the health team, the nurse can. contribute in each of these areas.Her teaching and counseling functions.can be.fully utilized here. Making each meeting with a patient .meaningful and having a sustaining relationship to provide continuity will enhance the effectiveness of care (Helming, 1968) pp» ^19=420).
Because of the general tendency for emphysema patients to de-.iteriorate (Burrows, 1968),' it is important that treatment- focus on thetadjushable or coping-aspects of their condition, Betty and Hett (1967)report • that patients seek guidelines on how to live and .breathe des<= ■ •pite- serious disease,. Also stressing the. positive approach is Silver(1968, p, 4 ), "We enable people by an image of action.and. effectivetreatment, We disable people by giving them a discouraging picture oftheir prospects."

CHAPTER • III
research; design .. -
This is a controlled quasi-experimental.study•in which the teaching interview is- the variable being manipulated and the change ,in the patient’s comprehension of his disease and coping ability, or. patient welfare, is the variable being measured.
An experimental study was described by Edwards (1968, pp, 10,ll) as one in which certain variables can be controlled or manipulated directly by the experimenter in a research problem, . The advantages of making observations under controlled conditions are:■ lo Experimenter can make the event happen at a certain time • , and place so is fully prepared'to.make an accurate observa-
' tion,■2 « Controlled conditions being known conditions, the experi-
' menter can set up his experiment a.second time and repeat the observation®
3 o Experimenter can vary the condition and note the concomitant variation in the results.
. This is a quasi-experimental research, design (Campbell, and Stanley, 1967* PP° ^7-50) since it does not meet; the. criteria of a true experimental design because the subjects were not randomly assigned from a common population to the experimental'and the control group. The groups constituted naturally assembled- collections with the subjects being disabled male emphysema patients on one eighteen bed hospital unit.
16
' The teaching interview, by the nurse researcher was given to one group of subjects (experimental) while another group (control) did not receive the teaching interview. The nurse researcher planned to 'spend two twenty minute sessions with subjects in both groups in an at« tempt to eliminate a "Hawthorne" effect (Selltiz, 1959/ P* 497)•
Pretests and posttests} in the forms of a questionnaire .(Appendix E) and an objective measurement scale (Appendix; F) were constructed and used to measure the patient's comprehension of his disease process and coping ability. The interaction of testing and X (the experimental event), as a source of external invalidity is considered (Campbell and Stanley> 1967? PP» 13-24). A pretest may sensitize the subjects and increase the educational effect of X or it might, reduce the efficacy of X« In an attempt tO decrease this sensitization, an 1 interviewer, not the nurse, researcher, administered the pre and post questionnaires to subjects in both groups. The nurse researcher administered. the objective, measurement scale with the patient unaware of the observation. . . :
. 'Hypothesis. • ' The patient, who is instructed about his disease process andself care in a one to one relationship by a nurse who encourages him to discuss his anxieties and- frustrations, will have fewer misunderstandings .about his disease and greater confidence in his ability to cope with the situation than the patient who does not have such instruction, ■.

18
Operational Definitions .The independent variable, is■the nurse teaching interview ad
ministered .by the nurse researcher. It could also be called a nursing.interaction or a treatment, Diers and Leonard (1966) have indicated, that an interaction as a treatment must meet the criteria for any other treatment: (l) it must be specific to the patient’s condition, (2) the.effects must be /measurable., and (3) it must be teachable. The nurse teaching interview is:administered to subjects in the experimental group but not to subjects in the control group. It is theorized that this concentrated patient centered therapy makes a difference in the patient's conception of his disease process and in his coping abilities.
The two dependent variables are the effects of the nurse teaching interviews
1 . The patient's comprehension of his disease process and ; . self care after introduction of the stimulus of the
• teaching.interview. 'Any change is measured by the preand post questionnaire. ■
2 . The patient's, ability to cope with his breathing problem. Selected patient activities and patterns of breathing were used in designing an objective measurement scale and change
; is measured by pre and post observation.Measurement of the dependent variables both before and after introduc- ' tion of the experimental variable increases the precision of an experiment (Selltiz, 1959, pp. 112, 113).

Selection of the Sample Male patients with the diagnosis-of emphysema.were'selected.
from the eighteen bed Respiratory Diseases Ward of a general Veterans, Administration Hospitals All patients were under the care of one physician and had his consent to be included in the study. To be eligible for the study, patients.must, have a knowledge.of the .English language and be physically able to respond to the questionnaires and to the teaching interviews« Criteria for selection also included that .
the severity of the lung disease be documented by a pulmonary function’ test. Each patient, was advised of the nature of the study, and signed
•a consent form (Appendix A)* ■The sample was to have a total of twenty'patients, ten in the
control group and ten in the experimental group.
Limitations of the Study While the importance of random assignment of subjects (Fisher,
19^7) is recognized, it was not feasible with this small, restricted, homogeneous sample. All data concerning subjects in the control group were collected prior to any data collection from the experimental group. Completing the control group first assured no spillover contamination of the teaching interview from the experimental group.■
Another limitation of the study was the lack of standardized measurements of the effects of the nurse teaching interviews. The development of adequate criteria for the. measurement of patient welfare
has long been a problem (Schlotfeldt, 1962). By means of a questionnaire, aspects in the cognitive and affective domains can be determined,

■' ■" ' : - 20 but aspects in the psychombtor domain need to be ascertained by direct observation and this actually may be more subjective than objective„ Since no existing standardized tests were available, a questionnaire. and an objective rating scale were developed and used within the confines of this studyo
b:The u short-;v1span.:1of-Airaetancwored.. by. the teaching interviews was another limitation of the study0 Orlando (1961, p = 191) says, "The improvement is always relative to what the nurse and patient start with, to the length of their contact and to what they are able to . accomplish," The nurse “-patient contact in this study was limited to two twenty minute sessions,, ■ • - '

CHAPTER IV
' DEVELOFMEET;0F THE STUDY .
This chapter is devoted to the preparation'ftir. teaching.
assessing the patient's readiness to learn; evaluation of the patient's learning; and the development of the various instruments..that are used* .... .
The "basic principles of learning and teaching as discussed by. Pohl (1968) were used as a guide with evaluation being an integral part of the learning and teaching processes„ In the final analysis the nurse researcher wanted to know if the subject learned what he needed to know and if it improved his state of being« .
Nurse; Teaching. Interview . An individual type of teaching was planned in order to better
identify the patient's needs; interests; and capacities. This type of . teaching will be called nurse teaching interviews, Bermosk and Mordan (1964) identify six kinds of interviewing in nursing: obtaining .information; giving or sharing information; allowing for the expression of feelings; identifying needs and goals, teaching,and counseling.The plan for the interview can be completely structured as to content, sequence, and kinds of questions, or it can be relatively unstructured. "The interview is essentially communication that is always meaningful> purposeful, and goal directed. The.nurse applies her knowledge of
21

interviewing principles, and throughout the.interview she is aware of what.she. wants to accomplish and what she is accomplishing with the patient (p. 39)•" In this study, all six kinds of interviewing as identif ied were used in -a single interview«
Lesson, Plan • " / ■.. A structured lesson plan (Appendix D).was constructedvto^
the nurse make certain of her own skill and knowledge, of the. material to: be. given to each patient.- Topics to be covered and the principles ;.involved were discussed with tke. Chief of the Pulmonary Diseases Section at the hospital involved. The lesson plan included the. following breathing exercises, brief anatomy and physiology of respiration, conservation of energy, rest and sleep, fluids and nutrition, smoking, 'intermittent, positive pressure breathing machine, prevention of complications, and getting the most out of life.
Pictures from Clba Clinical Symposium, Chronic Obstructive Emphysema (1968) were used, along with several other diagrams.. The ..pictures were trimmed of extraneous material and mounted in plastic covers, by 11 inches, with light blue backgrounds. Each picture •was separate so the patient could hold and study it if he so desired.
In actual presentation of the information during the interview the nurse researcher planned to use only a card with an outline of the topics and the pictures. Topics and pictures would be.presented in the sequence as determined by the.patient's interest during the interview. Dewey (1961, p. 183) points out that the teacher must have her teaching,material so well in mind that she is not concerned, with the • subject matter but can focus instead on its interaction with the
... . ' . ' \ \ ,, ■, ■ •. : - : • ' ' ■ V : ; %;lear'ner’s present needs and capacities. Furthermore,' Eedman .(1968)' ' ' ' - . m•indicates that the skilled teacher is flexible, being able to alter her
. teaching according to the learner’s responses and is capable of using
. 'many techniques and tools in ways best suited to the situation, :A.nurse teaching at the.bedside of a patient, helping him to comprehend the effects of his surgery, will probably give as
'• part of her lesson' an explanation, which could be considered■ ; a; llecture,’- V . . drawing from the patient, infprmatioa, atout
his - symptoms. She ought to be interested in what he .wants ;to know about the entire experience. . . . discuss with him his /feelings'. . . .. This . kind .of easy give and take, ,a combination of -.inf ormatlon-giving and discussion— is of ten .motivating and
.quite useful for assuring that the patient comprehends .(p. 74).. ’. It was planned to cover the lesson plan in approximately two
twenty minute sessions. This time limit was set as an estimate of theusual emphysema patient’s endurance of energy for concentration ac~cording to a pilot study done by the nurse researcher..
Demonstration and Practice, of Breathing Exercises 'It was anticipated that the patients had been instructed in
the breathing exercises by physical therapists at a previous time, soit would be a matter of review of the techniques and the principles involved. The nurse researcher previously consulted physical therapists to check the nurse’s knowledge of the techniques of diaphragmatic breathing and pursed lip breathing and the coordination of the two with the activities of talking and movement.
In presentation of the breathing exercises, it was planned to; use some of the Ciba pictures, as well as demonstrations by the nurse ' researcher, and demonstrations and practice by the patient. Of this teaching, Redman (19.68) states: - . "

2k
Demonstration followed by learner practice is the method most suited to teaching of motor, skills<, Since skills are not
: .learned separately from attitudes and factual knowledge} the -' demonstration and practice sessions are usually combined with . giving of information-and with discussion to clarify concepts and feeling . » . the demdnstration has to be practiced and . submitted to critical examination before it is presented
. . ;. : (ppo '76/ 77). ; ' ' ■ . ■ ■ ■ .
; Assessment of Readiness of the Patient to'hearnTwo forms, Profile of Patient and Agreement - (Appendices B- and
A); were developed as instruments' for the initial assessment -of the readiness of the patient to leafn. As much information as was available was..obtained from the patient’s medical record for the Profile of
;. Patient« It was planned that the nurse researcher would approach'the. patient with an explanation Of the project and obtain his 'signature on . the Agreement«, As she talked with the patient she obtained the neces- '.sary information to complete the Profile of Patient. At this time she also completed the Objective Measurement as one of the pretests. This measurement was an assessment of the patient’s physical capabilities.
As the nurse researcher talked with the patient she was able . ■ to determine something about his emotional status, his feeling'about ..the situation, his interest in learning, and his physical - and mental capacity for learning. This brief contact with the patient afforded
■ the opportunity to establish a relationship between the nurse researcher and the. patient. Redman (1968) says of this relationship:
Teaching involves providing conditions under which.learning will occur. This is accomplished first by a relationship
. .'/which motivates« - The teacher is also skilled in deciding what experiences are likely to be profitable for a particular individual to reach certain objectives, and in helping
- him to carry them out (p. -103).'
Increasing the patient's readiness to learn was not an objective of the questionnaire, however, the questionnaire served this incidental purpose for some patients as was evidenced by their comments.. During the nurse teaching interview patients’ specific questions about the questionnaire indicated that they were seeking information about.certain aspects of their disease,.
'' Immediately after the first nurse teaching interviewy'a. Re'cord of. Session with Patient (Appendix;C)'was completed by the nurse research^ er, This information was helpful in evaluating the session and in planning for the next nurse teaching interview,
' Measurement and EvaluationIn order to operationalize the effects of the nurse teaching
interview on the patient’s comprehension of his disease and his copingability it was necessary to find appropriate measures to determine hiscomprehension and his coping abilities.
Measurement is carried out so that evaluation of the teaching '■ learning process can be done, more accurately than it would be by using general impressions. Evaluation must go beyond measurement in that it involves making a value judgment about- learning' and. teaching. This involves summarizing, the evidence and determining to what degree the objectives are being met (Redman, '1968> p. 123)«
The effects of the teaching interaction, the dependent variables, are measurements of aspects in the cognitive, affective, and psychomotor domains, It was planned to use a questionnaire to measure aspects in the cognitive and affective domains and to use an objective rating scale to measure aspects in the psychomotor domain.

Development of the QuestionnaireIn the " cognitive domain, it was necessary, to measure the pa-.
tient’s'knowledge before and after the nurse teaching interview to ascertain if there was any change in his comprehension of his disease process. Did the teaching interaction make any difference in his .understanding of his emphysema problem? ; Questions.asked of the ..patient before and after the interaction, could discover any change.
' In the affective domain, it was necessary to determine aspects... of the-patient8s attitude. Did the nursing interaction change how he . felt about his disease, his situation, his ability to cope or to handle his problems? How well does he cooperate in the plan of treatment for him? How strong is his desire to help himself, or how motivated is he? Of this aspect Redman (1968).states: . •
Measurement of attitudes by written test differs from measure- ' ment of cognitive skills in that there are no right, answers,.
. only desired attitudes. Usually measurement is taken through a series of statements designed to elicit expression of the degree of acceptance of the attitude. This may be on a scale from ‘strongly agree' to ‘strongly disagree,' or on a scale of how many people are characterized by particular, behavior or
. thoughts (p. 122).As an alternative to a rating scale to determine attitudes
it seemed feasible to ask the same questions before arid" after the interaction. One questionnaire could then be designed to measure aspects in both cognitive and affective domains.
A questionnaire was developed by the nurse researcher to cover material in the lesson plan and aspects of the patientIs attitude. It was used in a pilot study and questions were revised according to patient suggestions. However, in the project, it was reasoned that the

- \ .. . ' ■' : : 27;. questionnaire would "be. more objective if the nurse researcher did not know the exact questions« The information then given to the.patient would be more,general in nature.and the nurse researcher would be less ■ inclined to "teach to the questions«" Consequently, the final questionnaire was developed by the Chief of the Pulmonary Diseases Section using the nurse researcher's previous questionnaire and the outline of . the topics in the lesson plan. In this two-way process the person who designed the questionnaire did not see the lesson plan and the person who did the teaching did not see the final questionnaire.
■ The questionnaire was administered by a non-vparticipant ob- server. The same.person administered all questionnaires after being instructed to read the questions without giving the patient any help
/with, the answers, and to record the. responses as given. The questions were of the true-false,.don't-know variety and the patient was instructed not to guess.at the answers. The nurse researcher did not see the .questionnaire or the patients1 responses until all the data had been collected. • ■. b
■Development of the Objective Measurement"- To measure aspects in the psychomotor domain, it was necessary '
to determine if the patient's skills improved after the teaching interview. Did he actually move more slowly than he did before? Did he use pursed lip and diaphragmatic breathing in a coordinated manner? There is the problem here of objectivity versus subjectivity. How many steps he walked would be an objective measurementj whether he walked more .
: ' ■ '■ \ - : . 28slowly than before' would, be ;a subjective measurement and could be a biased judgment on the part of the observer.
Because it is difficult to determine if the patient is doing „ diaphragmatic breathing correctly without placing one’s hand on the patient, this too could be a biased rather than a true measurement.The, patient would be reminded .of the correct diaphragmatic pattern and would comply when the observer touched him. "The best opportunity for accurate assessment," Redman (19^8) states, "seems to be by direct observation in a.situation in which the individual is unaware that he is being observed for this purpose (p. 106)."
Aware of the bias, and after consultation with several physical therapists, an objective rating scale was constructed as an attempt to measure the patient’s skill in using pursed lip and diaphragmatic . breathing with activities of talking and movement. This Objective measurement was designed to be used as a pretest and as a posttest..It was utilized by the nurse researcher before the first teaching interview and again at the end of the second teaching interview with the
. patient unaware that he was being evaluated.
CHAPTER V
; - . ' DATA. COLLECTION .
The instruments as described, in the previous chapter were, all .used..in collection of the data-. In working with.the-,control..group the nurse researcher experienced some frustrations which she had not anticipated and the collection of. data took longer than expected.
Overall Collection Time ■The data on subjects in the control group were collected first
in order to prevent spillover contamination. Collection time for this ' group took two weeks, from June 2, to June 15. There were five eligi-
■ *,ble subjects on the ward when the study began and it was possible to • collect data on another five subjects by the end of the second week.:The nurse researcher was able to collect data every day including the weekends but the questionnaires were administered only weekdays and during regular working hours. Collection time for subjects in the experimental. group, was-six weeksj from June 15 through August 1 , The longer;, collection time for the experimental group was attributed to the slow turnover of patients making it necessary to wait for new admissions of eligible patients.
.29
30Typical- .Time ScheduleDay I. ' A. Completion of Profile of Patient '
lc Review patient's medical record 2 . Initial approach to patient, explain
project and obtain information which was not in the medical: record ■.
B. Signature on Agreement . ■ C . Ob jective -Measurement^-pretest'
Day II. . A. Questionnaire-r-preteat/ • .B.:: f,Pirst inurae,-patient interview
C. Record of "Session with PatientSecond nurse-patient interview Objective.Measurement--posttest.Record of Session with Patient
.. Day IV. Questionnaire—-posttest .While collection of data from each patient followed the above
sequence, the actual number of days necessary to collect the data from each patient usually varied from.two to four days.
1 ' : i'i- Initial Approach to Patient 'The nurse researcher consulted: with the physician and reviewed
the patient's medical record to determine the subjects? eligibility for ■ the.study and began the Profile of Patient. Additional data to complete the profile were obtained when she approached, the selected patient to explain the project and to elicit his willingness to be included in the. study. All of the patients approached, with the exception of one who said he "just didn't feel like^being bothered," voiced interest in the. study and signed the Agreement' Form. Another patient who firmly denied that he had emphysema., refused to answer the second questionnaire and consequently was dropped from the study.
Day III. A.. • B,
C .
Administration of the Questionnaire \ ; All questionnaires were administered by the same non-participant
observer. The first questionnaire .'was given either the same day on which the consent form was signed or on the ensuing day. The second questionnaire, identical to the first, was given as soon as possible "after the nurse researcher had completed her second nurse teaching.interview. Time varied in the administration of the second questiotihaire from one to three days, depending whether or not a weekend intervened. , In one instance the questionnaire was inadvertently not given until four weeks later and this patient probably should have been dropped from the study as intervening personal problems occurred which possibly affected his responses to the second questionnaire.
In administration Of the questionnaires the patient was given ;a. copy to peruse while the non-participant observer read the questions aloud and recorded the patient’s verbal answers. In some instances it was necessary to reword the questions for the patient to enable him to understand the question content. - ; ; .
Control Group . . . . .In the control group, the nurse researcher performed routine
tasks or sat and visited with the patient; she refrained from doing ■ any teaching or answering questions which might be giving him information, Working with the control group was frustrating for the nurse researcher because the patient recognized her as a nurse but she was unable to fulfil her expectations (and possibly his) of herself as a nurse. While she discovered needs and information gaps in the
patient’s knowledge, she was prohibited from providing the assistance to alleviate those heeds without contaminating the sample of patients„ • One advantage of completing the control group first was that the research nurse did not have to shift her approach.
Experimental Group . • \ .-i 1 h.In the experimental group the research .nu^se^^plored--the
patient’s comprehension of his disease and gave him information according to his capacity and readiness to learn. She offered him the opportunity to express his feelings and encouraged him to define his situation.. Most patients were interested in prolonging the sessions if their physical condition permitted, hut the actual teaching interview was terminated in twenty five minutes even when the patient was verbose .and had digressed from the topics for over five minutes.. "It .was possible to cover the lesson plan in the allotted time if the patient wasn’t too talkative, It was planned to present the pictures during the first session, using them again in the second session only if the patient needed them for clarification or asked questions about them.
: One incident with a patient during the nurse teaching interview bears relating. This, particular patient had no previous instruction in breathing exercises by a physical therapist and he was unable to grasp the technique of diaphragmatic breathing as demonstrated by the nurse researcher, even though he was most interested and tried earnestly. He stated that if this was something that might help him to become more active again, he surely wanted to learn it. After"
conference with the -physician,'.- the patient was referred to the physical therapist for instruction in breathing exercises* The patient was'; motivated but he seemed to lack the coordination of motor skills until taught by a specialist in the field, .The twenty minute teaching in-' terviews-;.limited the-amount of -time which could be spent on any one , .topic and this motor skill in diaphragmatic breathing reguired the, teaching , of a physical-’ therapist .
The first teaching interview occurred on the same , day as;: the ■ first: .questionnaire or on the following day* The - second session .was, done on the day following.the first session with;the exception of one patient when the second session occurred three, days later because of an intervening phase of acute illness*
Late afternoon proved to be the opportune time for the teaching interviews. Usually-the second session was done at-the time selected by the patient. / --
., A record of the session with the patient was completed -immediately after each nurse teaching interview. This information was of help in planning for the. second nurse teaching interview and ' in' evaluating:the patient1s.general response to. the interaction.
., 'i Administration of the Ob jective MeasurementThe first objective measurement was completed by the nurse
.researcher immediately after her initial contact with the patient when she obtained his signature on the Agreement Form* The second objective measurement was completed immediately after the second nurse teaching , interview. This measurement scale proved to be even more biased and '
' ■ . / . ' - , 'V - ■; ■; : ' ■ :: 34
'subjective than 'anticipated. Several patients were bedfast and several ambulated only in wheelchairs, thus limiting the collection of data for the measurement. The patients> who were able to walk, accompanied the nurse researcher down the hall to another room for the interview which afforded the opportunity to observe their coordinated breathing.with the walking and the walking endurance, While the pursed lip breathing was easily observed, the diaphragmatic breathing was not because of the loose clothing which obstructed the view of the patient's chest and waist movements. This measurement was more subjective than objective with the nurse making a judgment about the type of breathing that the patient was actually doing.
CHAPTER VI
;:vv ;m a e y s i s - of data - '.vV -;- .
’ In order to test the effectiveness of the nurse teaching Inter-- view, tests were given before and .after the interaction: in the experimental group.. In the control group, tests were given before and .after ■the nurse "socialized" with the patients.
The highest score that could be attained in the questionnaire ' was twenty "five, or one point, for each question answered correctly.. Actual scores ranged from a low of nine to a high of twenty. -
. . The objective measurement was a rating scale with twenty being the highest number.of points which could be accumulated. Five items were rated: talking, getting out of bed, sitting in a.chair, walking,and walking endurance. Restricted activity of the subject lowered his : cumulative score.. One of the patients was so acutely ill that he did not get out of bed at the time of either test and his score was one on the pretest and one on the posttest. (See Table l). Another patient did not get out of bed at the time of the first test but was able to walk down the hall at the time of the second test and attained a score of -fifteen on the posttest. Several of the patients ambulated only in wheelchairs. The score on the rating scale varied in relation to the; amount of the activity of the patient. Actual scores ranged from one to sixteen. ■ . -
35

% - ''.': ' - # : ' TABLE 1 .' .'■•>: -RAH.-SCORES 0N''PRETESTS AND TOSTTESTS
■ . COIlTROL GROUP'^estioSnaZre^ Objectlye Measurements ;I, II. Difference I. II.. Difference1 6 2 0 A 8 . 1 0 . f 2
1 6 1 3 - 3 • 9 9 0
1 5 1 7 - ■ f 2 1 2 7 ' - 5 '
1 6 1 5 - 1 2 5 > 3
1 1 9 - 2 . 9 7 - 2
10 12 f2' 10 9 . ' -11 4 1 8 . < . 4 , 9 9 0
1 2 9 - 3 1 0 9 - 1
1 5 1 6 f l 6 9 - 3
1 1 1 1 0 - 1 0 1 0 0
Total 1 3 2 1 4 0 8 5 8 4
M e a n 1 3 . 2 1 4 . 0 7 8 . 5 8 . 4
N s 10 . : vL.V'-v'";' : 7 ;:, ; :y,' , ;''' 7
• EXPERIMEHTAL GROUPQuestionnaires';' .7 Objective Measurements
: 1 . I I . D i f f e r e n c e I . •■■■• I I . D i f f e r e n c e ■ .
1 7 : f 7 7 . 8 1 0 • V
7 7 7 . ' 1 0 1 7 + 7 : 7 ' 7 . 1 5 ' ' i-81 5 2 4 . . f 9 . 1 3 1 6 4 3 .
1 2 2 0 A 7 : 5 ; 1 1 4 6
■ 1 2 . 1 6 4 4 6 1 0 4 4
7 1 3 1 7 4 4 - : 1 ' - 1 5 . 4 1 4
" ' '■ ■ : 9 1 2 4 3 6 1 0 . f 4
1 2 1 9 7 4 7 . 1 1 0
7 1 1 9 7 - 2 8 7 : 1 2 • 4 4
■ 2 0 1 6 - 4 5 1 0 4 5
T o t a l I S ! 1 7 4 . 6 0 ■ 1 1 0
M e a n 1 3 . 1 1 7 « 4 6 . 0 1 1 . 0
H - - 1 0

Direction of Change \ The direction'of the change in scores of the two tests was not
consistent (See Table I),• In some subjects the scores on the questionnaire had a positive change while the scores on the objective measurement showed a negative change. and- vice versa. One explanation, is that the patient * s comprehension of the disease as.denoted by the question- -naire results did not correspond with his behavior as denoted by the objective measurement. Another possible explanation could be observer " bias in the objective measurement. In some situations it was necessary for the nurse researcher to make a judgment about the way the.patient Was actually breathing because observations of the chest and abdominal . muscles were not always possible. Also scores were lowered on the . objective measurement when the patient's activities were limited.
■ In the experimental group, eight subjects had positive directional changes with both the questionnaire and the objective measurement, while two subjects had negative changes with the questionnaire and positive changes with the objective measurement. While an explanation can be found for.this dissonance in the last subject, none can be offered for the other subject except that he was a seventy three year old and quite forgetful. With the last subject, the second questionnaire was inadvertently not given until four weeks after the nurse teaching interview. There was a time lapse of approximately a month between the two questionnaires while all other subjects had their second questionnaire within a few days of the first questionnaire and the teaching interviews. This particular subject had gone home - from the hospital to face multiple family problems and the second
' ' :: : i" / : '■' ; . ■ : . 38questionnaire A as -administered.' when he • came into the outpatient clinic. The. time.interval "between the teaching.interviews and the questionnaires, and the. difference in setting (outpatient clinic) help to explain; the negative directional change in his questionnaires. This , subject had attained a score of, twenty on the pretest, which was.higher than that of ..any other sub ject in either the control or experimental group, but on the posttest questionnaire his score was only ■sixteen, - or a loss of four points;
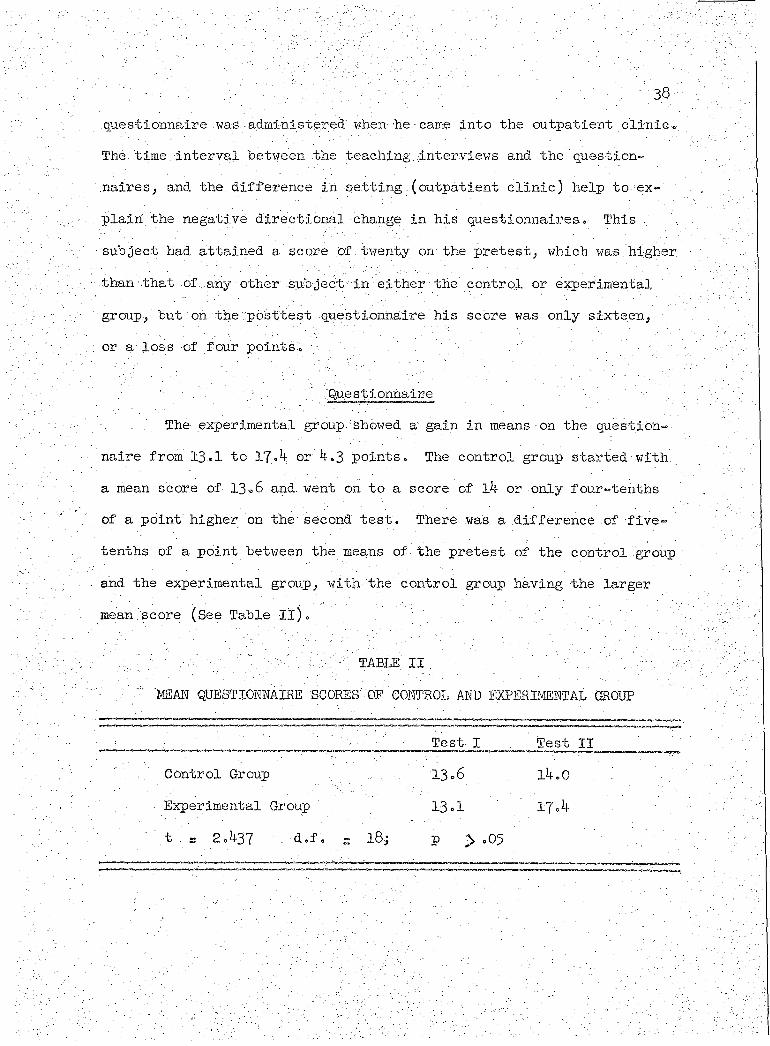
'' '■ . , Questionnaire. The experimental group showed a gain in means on the question- -
naire from 13.1 to 17.4 or 4 .3 points. The control group started with a mean score of 13.6 and. went on to a score of l4 or only four-tenths of a point higher on the second test. There was a difference of -five- tenths of a point between the means of the pretest of the control group and the experimental group, with the control group having the larger mean score (See Table II).
1 Y. " y'y : cY;: YY t 7 " .':rY''v: .Q-'MEAN QUESTIONNAIRE SCORES"OF CONTROL AND EXPERIMENTAL GROUP
Test I Test II. , Control Group 13.6 14.0
• Experimental Group . 13.1 17.4
' " ;t . e 2.437 . d.f. - ’ 18; P > .05

The gain, of four-tenths of a point in the control group might.he attributed to sensitization by the pretest or the effects of taking a test upon the scores of a second testing. Another explanation may be ■maturation of. subjects between the first and second.tests. There was ■an interval of several days between tests and the subject may have gained ,inf o,ri#ilon from, the staff members or from other patients, during.
■ this' ■time = A third possibility is that the change might have occurred by chance alone„ :
The,gain of 4.3 points in the experimental group questionnaire must be attributed to something .more than sensitization to testing and maturation.. This gain is attributed to the nurse teaching interviews. Using, the t test of difference of independent means (McNemar, 1962^ pp o 102} 103)>. the difference between the pretest and posttest scores■ in the.experimental group was significant at the .05 level. The cal-■culated t is 2.^37 or greater than the tabular t of 2.101 at.the .05 ‘. level, so the. null hypothesis can.be rejected and the alternative hypothesis that there was a difference was supported.
In.the.experimental group> 80$ of the subjects, had more right answers on the second questionnaire while 20$ had fewer right answers.In the control group, 50$ had more right answers on the second ques-
■ ' .:■ ■■■ : . ■ ■ - ' ’ ■ ■ tionnaire while 4o$ had fewer right answers and 10$ maintained the samescore (See.Table III). .

'Ho ' '
‘' TABLE IIIQUESTIONNAIRE SCORES' BY PERCENTAGES .. OF CONTROL AND EXPERIMENTAL GROUP
. Control ExperimentalIncreased Score 50^ 80% -
■ Lower Score ■ : hap 20%Same . Score. v — -10% 0 -, , - '- v '
/ • \ Total . loo%; . 100% .;.
An item analysis of the questionnaire.was not. done since thenurse researcher did not construct the. final instrument ,. If the. study, were to he replicated, an item analysis would be done to refine the
, questionnaire and test the validity,
Objective Measurement.The patients were unaware that they were being observed and
rated by the nurse researcher so there was no.sensitization to the test or maturation invalidity. The invalidity was in the observer bias, Because it was necessary for the observer to make some judgments, there may - have been a tendency to rate lower on the first test and higher on the second test, -especially in the - experimental group. This test might, have had more validity if it had been done by a non-participant observer rather than by the nurse researcher.
■ In the experimental group the mean score on the pretest was six, and on the posttest the mean score was eleven, or a gain, of five points (See Table IV). ' ' ,
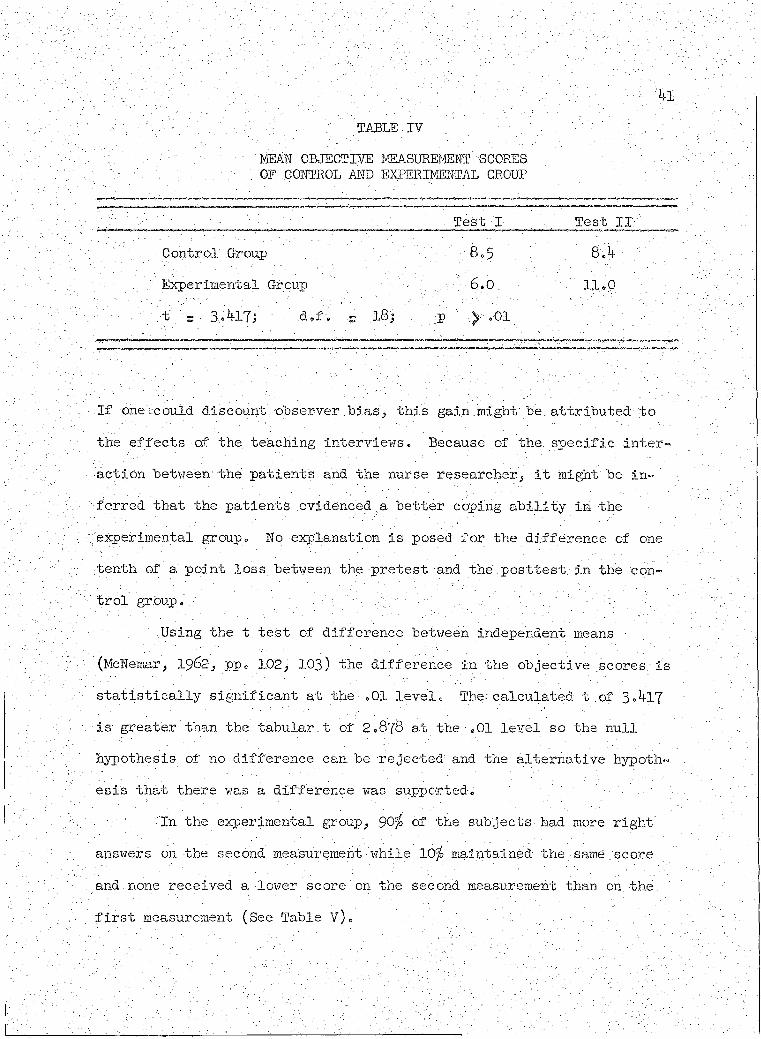
-. w v / y v : : : : ^V. -■ :; ' -TABLE-IV - ; : : ;. ' - ' : ,
MEAH GBIECTIVE MEASUREMENT SCORES.OF . GOMTEOL AMD EXPERIMEBTAL GROUP
Test I Test IT .
Control Group f f f 8.5
.. .. Experimental Group - .' - 6.0. ii«P ;" f t 3.417; - d.f. - 18; p ; >- .oi
If one could discount observer bias, this gain.might be. attributed: -to the effects of the teaching interviews. Because .of the. specific interaction between' the patients and the nurse researcher, it might be inferred that the patients evidenced a better coping ability in the experimental group. No explanation is posed for the difference of one tenth of a point loss between the pretest and the posttest in the control group. ■ % \ . . '' X. - i' f .. ..
. Using the t test of difference between independent means (McNexnar, 19&2, pp. 102y 103) the difference in the objective scores is statistically significant at the .01 level. The-, calculated t .of 3 A l 7
is greater than the tabular.t of 2,878 at the ,01 level so the null hypothesis of no difference can be rejected1 and the alternative hypothesis that there was a difference was supported.
In the experimental group, $0% of the subjects bad more right . answers on the second measurement while 10> maintained the same score and none received a lower score on the second measurement than on. the. first measurement (See Table V).
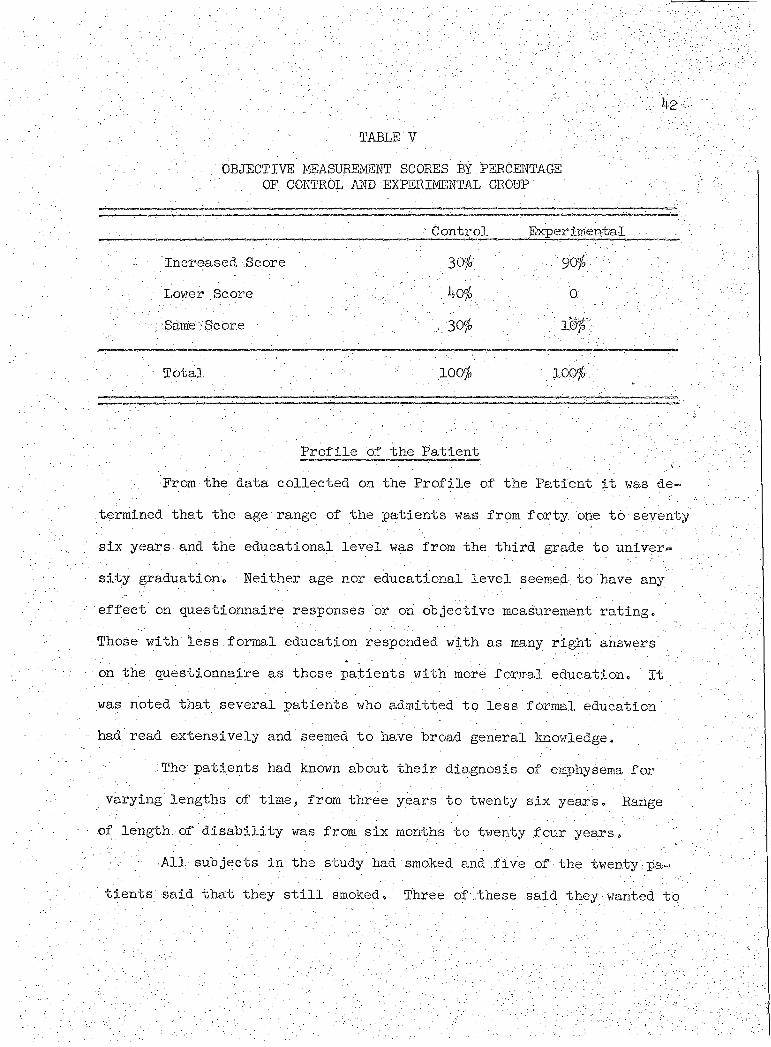
table vOBJECTIVE I-iEASUREMENT SCORES BY PEECEKTAGE
OF CONTROL AMD EXPERB4EETAL GROHP' ‘ :
\ ' Control E%perimemtal .Increased Score
; Lower Score yStiitie : Score
Total • ' ' : 100^ - 100^
• Profile of the Patient From, the data collected on the Profile of the Patient it was de
termined that the age■range of the patients was from forty one to seventy six years and the educational level was from the third grade to university graduation. Neither age nor educational level seemed to have any ;;effect on questionnaire responses or on objective measurement rating. Those with less formal education responded with as many right answers on the questionnaire as those patients with more formal education. It was noted that several patients who admitted to less f ormal education' had read extensively and seemed to have broad general knowledge.
The patients had known about their diagnosis of emphysema for Varying lengths of time, from three years to twenty six year's. Range
of length, of disability was from six months to twenty four years. .All subjects in the study had smoked and five of the twenty pa
tients said that they still smoked. Three of .these said they wanted to
W ,
,30$0
stop smoking and■knew that they should stop hut had been unable to ■break the habit. Two patients said they did not want to stop, and information given to them about the harmful effects of smoking seemed only to annoy them.

CHAPTER VII
■ 'SUMMARY, RECOMIENDATIOItS AND CONCLUSION
In this study a teaching instrument was designed, used-and tested'. ...Measurements ;.of patient welfare in the forms, of-..questionnaires and objective rating scales were constructed and used to test the efficacy of the teaching instrument. While much refinement of all the instruments remains to be done and different methods of applying the instruments might have changed the study, information was gained upon which future studies might be based.
SummaryThe study supported the hypothesis that nurse teaching inter
views -improve the emphysema patient's comprehension of his disease process and his coping ability. The patient, who was instructed about his disease and self-care in a one-to-one relationship by a nurse who encouraged him to discuss his anxieties and frustrations, did have fe.wer misunderstandings about his disease and greater confidence in his ability to live within his physical limitations than the patient who did not have such instruction.
The major purpose of the experiment was to test the effectiveness of nurse teaching interviews with emphysema patients. A teaching instrument in the form of a lesson plan and illustrative pictures and diagrams was designed and used with one group of patients while another group did not have this specific information. Two twenty minute sessions
were spent by the nurse researcher with each.patient, ten subjects in \ the . experimental group and ten subjects in the control group.. The experimental group-had the teaching .interviews while the control group
' had-. non-:directed interviews-;. The teaching interviews provided the opportunity for the patient to express his anxieties and frustrations-and: at the same time gaye him information about his disease process and encouragement' to:histeff orts' to 'liv'e withlh'the limits of his pulmonary
; reserve.'' . ", -.■ •;Instruments':to"measure the .effectiveness of the nurse .teaching
interviews were constructed and used as pretests and posttests. A questionnaire measured the change in the patient’s comprehension of
. his disease process and an objective rating scale measured the change in the patient's coping .ability. The two measurements attempted to measure aspects in the cognitive,affective and psycho-motor domains.. . Success of the nurse teaching interviews was evaluated by com- ..paring the responses to -the questionnaires and the scores of the objective rating scales in the two groups of. patients. The interviews were considered.successful when there was improvement "in scores' of both ' measurements in the experimental group. There was a positive direction-, al change in both instruments in.the experimental group.
From, this study it is theorized that if the patient understands his disease process and plan of therapy, he' is more apt to become an active participant on the health team,. and when he becomes an active participant, he becomes better able to cope with the problems imposed by his disease. For instance,.if a patient understands how the intermittent positive pressure breathing machine helps him, why it is-
important for him to use it at certain times and for-, the full treatment time prescribed, he is apt to participate more-fully with this portion of his prescribed treatment and will benefit both from the physiological ■■and psychological viewpoints =
. l ■ • ' ■ ■ Rec ommendations \' t. ■ : ' . 1 A replication of this study with another.population is recom-.mended. It would be especially of interest•to note, the outcome on emphysema, patients in another setting, either in another hospital or in ah outpatient clinic . .; A study of newly diagnosed emphysema, patients 1
might yield different data than patients who have had the disease for a number of years. V- , ■ V"v-..V
. ;. The effects of teaching patients In groups' father than ■individual teaching, or a combination of .group instruction followed by 'individual instruction, are other facets of. the study which might be explored,. With .the potential of teaching., patients in groups, the give and take of patients helping each other and knowledgeable nurses clarifying health, practices, it is possible that the.number of patients being readmitted to the hospital could be greatly decreased,. . /
.A study over a period of several months or years might measure, long term.behavioral change« It would be of interest to know if patients continued to use the information without repetitious encouragement and support, . . - . . ■
■Other types of questionnaires could be tried with patients.. An ■open-end questionnaire in which the responses were categorized, or a multiple-choice answer type might yield more information than the-
' true-false questionnaire. Axi item analysis of the questionnaire used. / in this study would be of help, in refining the instrument for future use.
The objective rating scale could be made more objective and less biased by having it administered by a non-participant observer who did. not. know which subjects were assigned" to the experimental or control group. Observation of the patient in a setting where he was. stripped to the waist for an unobstructed view of diaphragmatic--breathihg*wbuld: also help to produce more objective data„ . :: t v
: Other types of measures of. coping ability might be. developed.The use of a tape recorder to record cough and a tape measure to measure changes in inspiratory and expiratory chest expansion have been suggested. The tape recorder could be employed to note changes in the effectiveness of coughing efforts before and".after instruction by a physical therapist. A tape measure could be used to note changes in the inspiratory and expiratory chest measurements over a period of months of practicing specific breathing exercises . X
. - -t 1 - Conclusion " - . Vf;/: bf;".-i ■ r ,;v. One justification of this type of teaching interview or ex
pressive nursing intervention is that it helps to.decrease the patient’s anxiety so that he can comprehend the reason for his prescribed plan of therapy and then cooperate in.his treatment. . This gives the patient incentive to take a more-positive approach, to his breathing problem and. thereby enables him to better cope with his situation.: - • Nurses must be prepared to help their patients to define theirsituations and then-to help them understand -how to cope with: -their problems in a positive.fashion. The teaching instrument and nursing .
' approach^ as developed for this - study, could be used by all nurses working with emphysema patients in any setting, whether it be in a hospital, outpatient clinic, or in home follow-up care, y? Patients, by understanding their disease process and by learn^ing:self cafe, might be discharged from the hospital earlier, be read- • mitted less often, and. be able to return to some type of work„ If the teaching were done when the patient were first diaghdsed, it might be possible for him to slow progression of the disease and consequently to maintain his .status'as a productive member of society for .a longer period of time. ' . . 1 iy-'v,; ; '' y '; v..
If all nurses who came in contact with.emphysema patients were cognizant of the many ways in which they could help such patients.,. the mortality,. morbidity, and disability from emphysema could be decreased.
APPENDICES INSTRUMENTS USED IN THE STUDY
APPENDIX. A
' • . AGREEt4ENT
■ A study of people with emphysema is in progress. We want to determine:how much people understand about their breathing . problems and how we can better help them.
Would, you be willing to participate by answering several questionnaires? If so, please sign your name.
Signature
Date
50
i

' : ' \ - ^ APPENDIX B : .
, ' PROFILE OF PATIENT .
- : . . ■ ' ' •; ' ' v':;. - Date .- Hatte..;. ' ' Age Ed« levelDiagnosis - " . ' - ■ ■ . : - ‘
Admitted to hospital . . v ; ■ ■- 'Previous admissions - to hospital for emphysema: :
First diagnosis of emphysema . How long disabled ' ‘ - :Occupation:. Previous Now.'Activities Capabilities: • ■' . bOxygen—"Cont. intermittently . . None.Ambulation: Walks _ -Wheel chair.' NonePersonal Hygiene: Self care \ ■ Needs helpTime spent out of bed: Most Part . None.Spends free time Previous Instruction:Breathing exercises ■' By whomBronchial Hygiene. ' v • By whom.Conservation of energy " ' . By whomDisease process . - - By whom ,
51

52:Smoking History:Has" never smoked. Began smoking■ Amount, .of smoking nowTapered off smoking Stopped smokingReason ' - ' \ ' ' - ..i

APPENDIX G
RECORD OF SESSION WITH PATIENT
Name Session Date'Time/began,.,.. . . .Time ended ... Total
Conversation topics
Questions asked by patient
What I did with patient.
53
APPENDIX D
Learner's readiness: - Determined by nmrse-researcher from the pa.tierit,;s
.Main objectives To have patient understand his. disease; process so that he can better cope -with the present situation and move forward.in pro- gre'sslve. ihdependence«.: ' - 'Subobjectives s .Each of the topics has a specific objective. In general, objectives are to build upon the knowledge he already has, arid to give him confidence in his ability to live more adequately within his' limited physical capacity. ' - -
CONTENT ■ I " v , t- TEACHING ACTION' 1; : ’ ... - . v;v u ' General approach: Sit at pa-.. , -; 1 . . :' i tient's bedside, encourage ques-
. ; . tions, and discussion. . Watch for./ : clues abput confidence that he can
‘ . fulfill his role as a patientV - with a desire to learn. Follow
/ . . ; - ' : . riP i&ith discussion of his anxi- -eties if he seems to lack confi-
... derice. Show pictures, watch for. ; . . 1 ; reaction, and discuss topics in

'.I.o Abdominal .breathing:
detail as patient'■s' need is determined»
Breathing retraining to■learn how to empty the lungs more .efficiently in a coordinated, relaxed manner, so that new air can be . inhaled o Inhaling--puff out abdominal- muscles (around waist)»Emphasize exhalation phase. Contract abdominal muscles very . gently, expel air slowly. Neck muscles are of.no use and should be relaxed during coordinated breathing. Practice, use abdominal breathing in normal life experiences (talking, etc.) to avoid becoming dyspneic.Benefits: Breathing retrainingworks by improving coordination ; and efficiency and by strengthening the muscles of respiration. It does not strengthen the lungs themselves, but people feel marked relief of- symptoms with
Find out if he knows how his breathing pattern, differs now from when he became sick.
Show picture of man doing abdominal breathing.
Show diagram of diaphragm. Explain the diaphragm as the most important- respiratory muscle.
Ascertain that he is performing correctly by placing hands on diaphragmatic area (just below ribs).

the hew breathing pattern. They '."(yoti) are gradually able to in- ... crease physical activity without becoming dysptieie. Concentration, on relaxed > coortiinated breathing :is one method to allay anxiety.
II. Pursed lip breathing;With ordinary breathing in emphysema the bronchioles tend ;to collapse because of " positive intrathoracic pressure and loss of elasticity (flabby wet straw principle)»In pursed lip breathing, re- ; sistance to outflow at lips maintains intra-bronchial pressure and keeps, airways open longer.More air is exhaled, then more air can get in with the next inhalation. . Breathe in through nose, out through pursed lips, .GENTLY. Exhalation phase is at least twice as long as inhalation.
III. . Spirogram; Pulmonary function test to determine the
Stress that YOU also can be helped.
Show picture of man doing ordinary breathing and pursed lip breathing.Ascertain that patient comprehends the words "bronchioles" and "airway."
Demonstrate.Have patient practice.Get shoulders back- and relaxed.
Show picture of patient making a spirogram. ■
decrease in: functional capacity.. Air intake is limited because of non-ventilating cysts. Large: distended alveoli prevent other alveoli from expanding. Respirations in emphysema are more shallow and exhalation is slower.,
IV. Brief anatomy of the respiratory system. Identify the structures with emphasis on bronchioles and alveoli. Each bronchiole terminates in a cluster of air sacs. Each air sac is surrounded by blood capillaries for oxygen and carbon dioxide exchange. The lungs themselves are spongy.elastic tissue. On inhalation, the lungs expand and the negative intrapleural pres-; sure increases (-15). On exhalation the lungs contract and - the intrapleural pressure decreases (-5). The lungs change in size because of their elas-' ticity and because of the work '
Point out the difference in the normal and emphysematous spirogram, ■
Show diagram of Respiratory ■ System, . ' • .p.Picture.of terminal pulmonary air spaces.Ascertain that he comprehends the words "alveoli" and "air sacs."
Picture of intrapulmonary blood circulation.(if this information seems, too detailed for patient to grasp,. . it should be omitted,.)
Point , out difference in, size of chest., ... /:
.done by the-muscles of. respiration, the diaphragm and the intercostals.•,In emphysema the air sacs become distended because' of the loss of elasticity of their walls-*-air- is . not expelled. .The walls break and large cysts are formed. ■ Bronchioles are blocked by mucus., thickened mucosa, and bronchialspasrns.
V. Conservation of energy;•Anxiety and physical activity take varying amounts of energy. Relate use of energy, oxygen need, and dyspnea.A. Reduce, anxiety by developing and USING a coordinated pattern of breathing in the activities of daily living.B. Move slowly="quick, jerky movements take more energy. Think about what you want to do; then do • it with.slow, even motions and you
Point out diaphragm and intercostals.. ... ■
Point out distended air sacs.
Point out blocked air ways. Ascertain that he comprehends "brbrichialspasms.
Talk with patient, encourage him to talk. He may have thought of more ways to conserve energy.
Ascertain that he. comprehends “dyspnea"- =• shortness of breath.
; ■ ■ : / ; : won't get out of breath so soon ". .(dressing yourself), -
Co Eat small meals. Large meals take touch energy to digest„ It is less tiring to eat several (4 ;or 5) small meals instead; of .t.he. ■ usual three. Eat in a relaxed, slow•manner« A. light evening meal ■ makes sleep-more comfortable. It .is important to avoid getting overweight or underweight, so a nutri- . tious balanced meal. is. needed« One high in proteins:(meats) and low in starches (breads) is usually recommended e • ,
VIe Best and sleep. Seven toeight hours of uninterruptedsleep are usually required,A o Preparation•f or sleep e.
1, A short evening walk. . f ollowed by a little snack '
may. help to put you in amood for sleep,
. ' - S', Bronchial hygiene to clear the airways prior to sleep.
Discuss with patient his sleeping patterns.
How does he prepare for sleep?
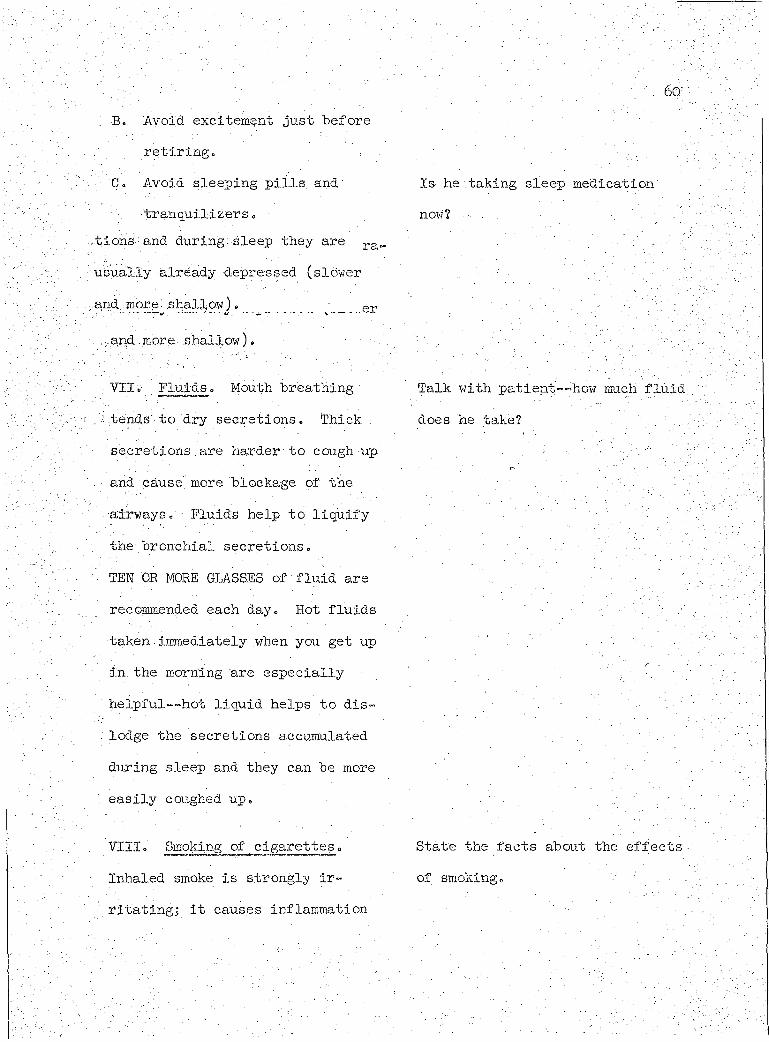
•BV Avoid expitement just beforeretiring
C, Avoid sleeping pills and' Is he taking sleep medication
Medications often depress respira-tions and during sleep they are usually already depressed (slower :a,nd: mor e - shallow) ,
VII. Fluids. Mouth breathing Talk with patient— how much fluid;/'tends to dry secretions. Thick does he take?
secretions .are harder to cough up vand cause more blockage of theairways. Fluids help to liquify . ' ■the bronchial secretions.TEN OR MORE GLASSES of fluid arerecommended each day. Hot fluidstaken immediately when you get up 'in the morning are especially ' :: %helpful--hot liquid helps to dis™ lodge the secretions accumulatedduring sleep and they can be more ' v-easily coughed up.
VIII. Smoking of cigarettes. State the facts about the effects -Inhaled smoke is strongly ir~ of smoking,ritatingj it causes inflammation

61of the airways, causing the raucous glands to secrete an excessive .amount of raucus which is hard to cough upc The cilia (fine, hair like projections) in-, side the airways ordinarily keep moving the secretions toward the throat in: wave-like motions.■But the smoking of one. cigarette can paralyze the ciliary activity for 15 minutes to one hour.This allows secretions to collect and block the airways. .Smoking Contributes to the progression of the disease process.Smoking is a personal air pollution problem which can be avoided.
IX. IPPB Machine.' It supplies' either air or an oxygen mixture, at an adjustable pressure and rate of flow. Your doctor decides whether you should have air or oxygen and the pressure which he thinks is best, for you. The machine' provides extra pressure on
Point out cilia in diagram .of. the Respiratory System.
(if he is a smoker)Stress that one of the best ways he can help himself is to stop smoking.

inhalation so that'you can get morefresh air into the air sacs* ■ . :Sold the mouthpiece firmly in the .. ' ■ ' ;mouth between the lips--don't bite ' ,it. You may use hose clips or holdyour nose with your fingers at first . ' ■until, you learn to breathe completely ’ ■through, your mouth«. let the pressure ■ ■ . . .help you inflate your lungs as youinhale; when, the pressure reaches - ; / '' ■the pre-set point, a valve turns off ' ;.and an exhaust opens. Then you exhale o Pause brief ly af ter each. ex- .1. V- / . ■haling 1 Sit . straight and relax. ; .Breathe, yith- the.machine. The treat- '• , . ... ‘ment should not:tire you. It is im- ; . ' 'y -portant to use the machine the prescribed length of time (.15 to 20 minutes).. Always have a fluid inthe nebiilizer--whatever your doctor • .*7 ■ ' ' ' - -has ordered. . . . .:Purposes of the IPPB Machine;A. .To get more fresh air into Point out blockage of bronchioles
more air sacs. in picture of emphysema breathing.B. To get moisture or medica
tion deep into the bronchioles /

Ascertain his comprehension of ''bronchod.ialator 0"
Xo Prevention of complications: You can learn of ways to prevent complications. .’Each infection causes more damage to your lungs, and because your lungs are al- . ready in a weakened condition, you are more, susceptible to infections. Avoid infections.A. Avoid crowds and people with
colds. If a cold does occur, cough Increases, or secretions lecbme thickened or colored; consult your doctor at once.
B. Avoid getting overtired.. How-. ever you need to keep up physi- . cal activity within the limits of your breathing capacity...
C. Keep up good body nutrition and take abundant fluids.
and air sacs to help dislodge secretions.C. To stimulate , the. c.ough reflex
and make coughing more pro-;’• ductive. ’ .- -
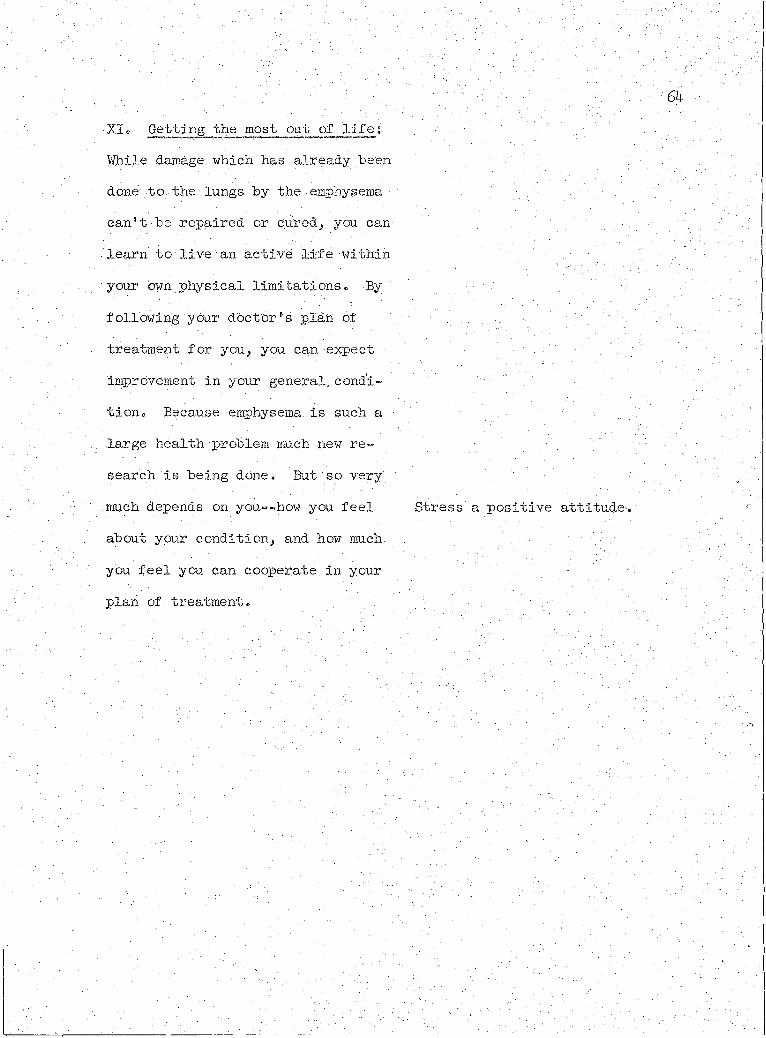
■'XIo Getting the most out of life;Wile lamage which has already, "been done to the lungs by the emphysema can't be repaired or cured, you can learn to live an active life within ■ your own physical limitations. By .following;ybur doctor's plan of treatment for you, you can expect Improvement in your general, condition, Because emphysema, is such a large health problem much new research is being done. . But so very .much depends on you--how you feel Stress a positive attitude-, about your condition, and how much you feel, you can cooperate, in your plan of treatment.
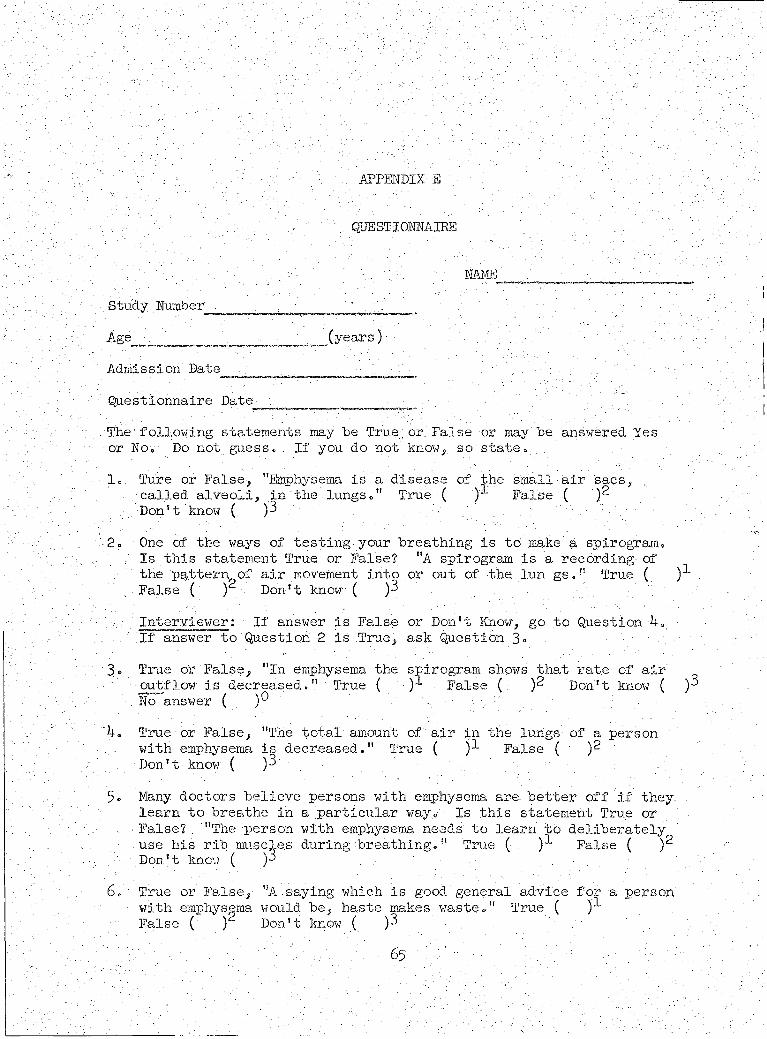
APPENDIX E
QUESTIONNAIRE
NAMEStudy Number . ; . "' 'Age (years) . .'t': V,; ': ;Admission'Date . . . r. ' ;
‘ 'Questionnaire Date ..; . The.following statements may he True:or False or may he.answered Yes
or.No. Do not guess.. If you do not know,.so state,1.: Ture or False-, "Emphysema is a disease of the. small ■ air sacs, :
. called alveoli, in the. lungs." True ( ) Palse. ( ')? ". Don’t know ( )3 -' y' \
2. One of the ways of testing.your, breathing is to make a spirogram.Is this statement True or False? "A spirogram is a recording of
.- the pattern of air movement into or out of the lun gs." True ( .False ( ) Don't know ( )3Interviewer; If answer, is False or Don't Know, go to Question 4.
• If answer to Question 2 is .True, ' ask Question 3 =3» True or False, "In emphysema the spirogram shows that rate of air
outflow is decreasedTrue ( ■).-*- False ( )2 Don't know ( )3No answer (
\ T r u e or False, "The total amount of :air in. the lungs of a person... with emphysema is decreased." True ( )-*- False ( )2
Don't know ( )35. Many doctors believe persons with emphysema are. better off if they. .
learn to breathe in a particular way. Is this statement True or■ False?. "The person with emphysema needs to learn to deliberately use his rib muscles during breathing." True ( False ( )2Don't know ( )3
6. True or False, "A.saying which is good general advice for a personwith emphysema would be, haste makes waste." True ( )•*•False ( ) Don't know ( )3
I / . . : % ''yV'.

7V . True or .False-, "A :per.son with -emphysema should'eat two large meals . daily rather than .many small meals.. '' True ( False ( )?•.
. Don't know. ( )3 . \ ;..8. True. or: False-,' "Breathing out- through pursed lips often relieves .
shortness, of 'breath in a person with emphysema." True ( )!... False. ( )- Don' t know ( )3 .Interviewer: ;If, answer vis .False or Don't Know go to Question 9«
■ If a,nswer No. 8 is True, state. Is this statement True or False? "Pursed lip.breathing helps because it enables the person with emphysema to concentrate on inhaling." True ( )“ False ( )Don't.know ( )< No answer ( )
9» True or False, "A stimulating period just before bed is desirable : for persons with emphysema." True ( . False ( • )2Don ' t know ( )3 .; ;
10. True or False, Exhausting exercises are desirable for persons. with emphysemab" True. ( )-*- False ( )2 Don't know ( )3
11. True or False, "Sleepiing'pills tend to make breathing slow and shallow." True ( )T False ( . )2 Don't know ( )3
12. True or False, "To breathe better, a person with emphysema should sit. in a chair, lean forward and apply as much muscle effort to
. breathing as possible." True ( )-*- False ( )2 Don't know ( )313. True or.False, "Smoking, cigarettes soothes air passages."
True ( )-*- False ( )2 Don't know ( )314. True dr . False, "To.avoid further .complications of his breathing
problem a person with emphysema should restrict activities to the' essential things." True ( )-*- False ( ) Don't know ( )3
15. True or False, "An Intermittent Positive Pressure Breathing (IPPB) ■ ' machine sucks air out of the lungs." True ( )1 False (Don't know ( ) .
16. True or False, "Treatment of persons with emphysema attempts to return the lungs to normal." True ( )-*- False ( )2Don't, know ( )
17. ' A person with emphysema needs to take fluids every day. Would. you say the right amount is 2 to 5 glasses every day? Yes (true) .
( )"*- No (false) ( )2 Don't know \ )318. True or False "It is better for a person with emphysema to be a
- few pounds overweight than underweight." True ( )(False ( )2 ' Don't know ( )3

n
19o ; True or False, "Sleeping pills give a sound, night's sleep and -v • are"therefore good for persons with emphysema." True ( )-kFalse ( Don't know ( . )3
20. True or False, "Smoking of. cigarettes causes the secretions . from air passages to increase.” True ( . False ( )2Don't know ( )3
21. True or False, "Inactivity is bad for persons with emphysema." • True ( False ( Don't know ( )
22. True or False, "It is possible to become emotionally dependent" upon IPPB devices." True' ( False ( . )2 Don't know ( )3
23° True or False, "Breathing exercises.have been Shown to improvefunction of the lungs.” True ( )•*• False (Don't know ( )3
24. True or False, "Loss of weight is a good sign in persons withemphysema." True ( False ( Don't know ( )3
25. True or False, "Persons with emphysema should try to suppress their cough." True ( ) False ( . Don't know ( )3 ,
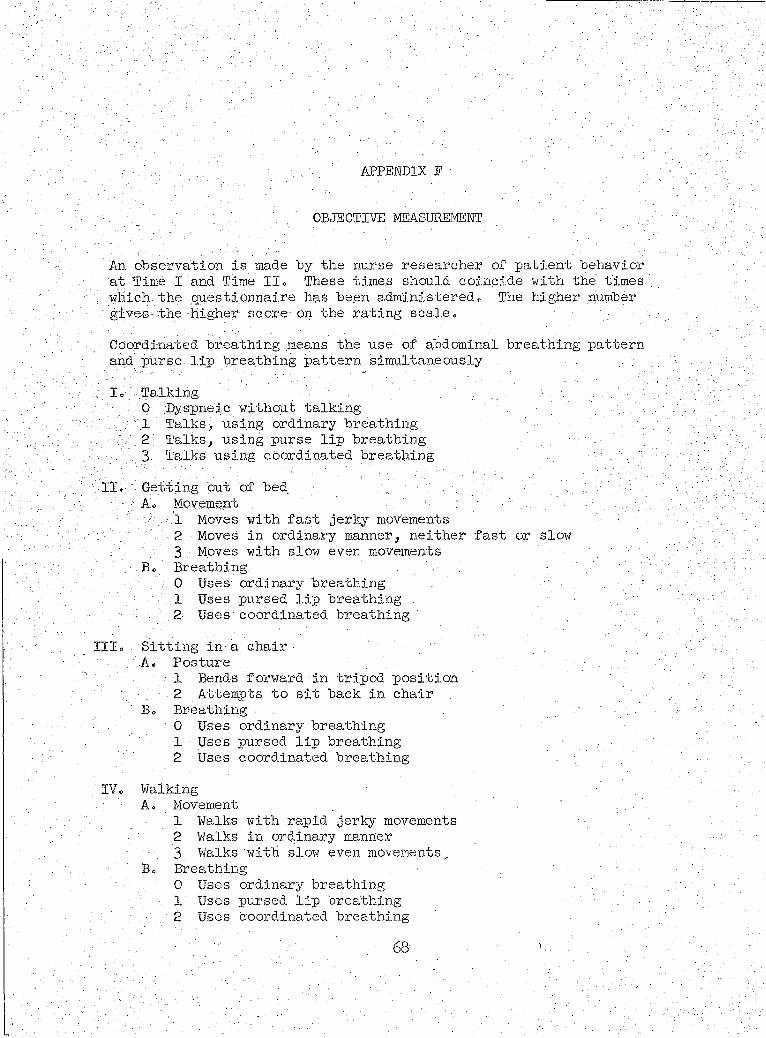
APPENDIX P
OBJECTIVE MEASUREMENT
An observation is made by the nurse researcher of patient behavior at Time I and Time II. These times should coincide with the times which the questionnaire has been'administered. The higher number ogives the higher- score on the rating scale.Coordinated breathing means the use of abdominal breathing pattern and purse lip breathing pattern simultaneouslyI. Talking; : 0 :Dyspnelc without talking . . .
. . 1 Talks, using ordinary breathing. ' ■2 Talks, using purse lip breathing
. 3 Talks using coordinated breathing . :':. II. " Getting cut of bed , „ :' "" ' :'b:.i'c 1 A;.: Mpvement : ' ; ■ ■ ' .
1 Moves with fast jerky movements -'2 Moves in ordinary manner, neither fast or slow ' 3 Moves with slow even movements
B. Breathing0 Uses; ordinary breathing . •1 Uses pursed lip breathing .
C - ; ■. 2 Uses coordinated breathingIII. Sitting in a chair . "
A. Posture1 Bends forward in tripod position
. 2 Attempts to sit back in chairB. . Breathing ■
0 Uses ordinary breathing1 Uses pursed lip breathing2 Uses coordinated breathing . - ;
IV. WalkingA. Movement- . 1 Walks with rapid jerky movements
■ 2 Walks in ordinary manner_ 3 Walks with slow even movements^
B. Breathing - . ' ' '. . 0 Uses ordinary breathing
\ 1 Uses pursed lip breathing 2 Uses coordinated breathing
68

69;Walking, endurance.-:-How far did he .walk without dyspnea? 0 Dyspneic. to start :■ 1 ■ Walked up to 10 steps • / .2. Walked up to 20 steps 3 Walked over 20 steps .

LIST OF REFERENCES
' Anderson,; Barbara, Hilda Meriz* and Robert C. Leonard, . "Two Experi=» ' mental Tests 6f: "a Patient Centered Admission Process,"
• ■ : Nmrsing'Research, l4:l51"157',' Spring 1965 ,• „ Arizona State Department of Health, Health Data. AnalysisAnnual; ■ Report of Vital: Statistics• Berrnosk, Loretta, and Mary J, Mordan, Interviewing in Nursing,
' New York': The McMillan Company, 1955T™*Bowen, Rhoda, Rosemary Rich, and Rozella Schlotfeldt.. "Eff ects, of
Organized Instruction for Patients with the Diagnosis of Diabetes Mellitus," .Nursing Research, 10:15-15.9; Summer 1961,
Bradley, Joan, ."Emphysema: Are Nurses Prepared," Registered Nurse,31 Al; ^2, 43, 75; January 1968,
Burrows, Benjamin. "The Course of Patients with Chronic ObstructiveLung Disease," Current Research in Chronic Respiratory Disease pp. 253“258« Proceedings of Eleventh Aspen Emphysema Confer-.
, • ence June 1968. Washington, D.C,: Pu.blic Health Service,Campbell, Donald, and Julian. C. Stanley. Experimental and Quasi-
Experimental Designs for Research. Chicago: Rand McNally andCompany,
Christopherson, Victor A. "Role Modifications of the Disabled Male,". American Journal of Nursing, 68:290-293, February.1968.
Chronic Obstructive Pulmonary Disease: A Ifenual For Physicians. ■■ • National Tuberculosis and Respiratory Disease Association.
Portland, Oregon: Oregon Thoracic Society, 1965.Ciba Clinical Symposium, Chronic Obstructive Emphysema. New Jersey:
Ciba Pharmaceutical Company, April, May, and June, 1968.Coulter, Pearl Parvin, "The Real Nurse— A Search For Identity,"
Focus on'Nursing, pp. 5-15. Papers presented at the Dedica- . tion Ceremony of the College of Nursing Building, October, 1968. ■ Tucson,' Arizona: College of Nursing, The Universityof Arizona, 1968.
Dewey, John.■ Democracy and Education. New York: The MacmillanCompany, 196I. '
■' • ■ " •’ ■ . 70 ■ ■ : ■: -
71Diers, Donna, and. Robert C. Leonard. "Interaction Analysis, " Nursing , :
Research, 15:225^228, Summer 19660Drummond, Eleanoro- "Patient Centered and Task Centered Tuberculosis
Nursing," Nursing Research, 13:56-62, Winter 1964cDumas, R» Go, Barbara Anderson, and Robert Co Leonardo "The Importance
of the Expressive Function in Pre-operative Preparation," . Social. Interaction and Patient Dare 0 Ed» Skipper, J« K., and Robert:C« Leonard, pp. 26^277" Philadelphia: J. B. Lippincott -Company, 1965.., arid Robert Co Leonard. "The Effect of Nursing on the Incidence of Post operative Vomiting: A Clinical Experiment,"Nursing Research, 12:12-15, 1963o
.Edwards, Allen L. Experimental Design in Psychological Research, ■New York: Holt, Rinehart, and Winston> I968T"™
Egbert, Li D., George B. Welch, and Claude M. Bartlett. ■"Reduction of Post. Operative Pain, by Encouragement and Instruction of Patients: . A Study of Doctor-Patient Rapport," New England Journal of Medicine, 270:825-827, April l6, 1907.
Elder, Ruth G. "What Is the Patient Saying," Nursing Forum, 2:25-37,1963 . . :
ElmSy Roslyn, and Robert C. Leonard. "Effects of Nursing Approaches During Admission," Nursing Research, 15:39=^8, Winter 1966.
Fisher, Ronald A. Design of Experiment. Edinburgh: ■ Oliver and. Boyd $ 1947. ~ ~~
Garrett, James. Psychological Aspects of Physical Disability. Department of Health, Education, and Welfare, Rehabilitation Service Series Number 210, 1953°
Helming, Mary G. "Nursing Care of Patients With Chronic Obstructive Lung Disease," Nursing Clinics of North America, 3:413-422, September 1968.
Hepper, Norman, and Robert Hyatt. "Office Management of Chronic Bronchitis and Emphysema," The Medical Clinics of North America, 48:857-865, July 1954.
Jones, William R. "Living With Emphysema," Nursing Outlook, 15:53-57, September 1967° :
Kass, Irving, and Phyllis Sheets. "Emphysema— A New Approach to an.Old Disease," National Tuberculosis and Respiratory Diseases Bulletin, 55: l¥-T67 May 1959. . "

Knuds on, Eleanor Gray. "The Case for Coordination," address .delivered- . •... at the Council of Member Agencies Meeting, Seattle., “Washington,■ ■ Kovember 1966» (Unpublished)
Leonard, Robert C. "The Impact of Some Major Social Trends on the ■/ Professionalization of Patient Care." Revision of keynote
address to Annual Educational Institute, California^ Board of, • . Nursing Education and Nurse Registration, Asllomar, .October -
1965» '
McNemar, Quinn. Psycholbgical .Statistics. New York: John"Wiley, and.Sons, 19627*
Molen, Marilyn. "Effects of Planned Patient Teaching on Persons with . Stasis Dermatitis and Leg. Edema,".American Journal'of'Nursing, 68:1276, June 1968.
. Monteiro, Lois. '•Notes on Patient Teaching~-A Neglected Area,"Nursing Forum, 3:26-33, 1964.
Newman, Margaret. "identifying and Meeting Patients.1 Needs in ShortSpan Nurse“Patient Relationships," Nursing. Forum, 5:76-86, -I966
Oppenheimer, E. A. "Respiratory Dis.ea,ses in Arizona," A paper pre- .• sented at the Arizona Chest Disease Symposium, Tucson, Arizona, October 1965 = (Unpublished)
■Orlando, Ida Jean. The Dynamic Nurse-Patient Relationship. New York:■ G. ,P. Putnam's Sons, 196T.•
Peplati, Hildegard E. "Interpersonal Techniques: Crux of PsychiatricNursing," American Journal of Nursing, 62:90-94, June 1962.
. .• "A Working Definition of Anxiety," Some Clinical Approaches'to Psychiatric Nursing,. Ed. Burd, Shirley and Margaret Marshall New York: Macmillan Company, 1963= -
Petty, Thomas L., Michael Finigan, and Louise M. Nett. "Can We Help Them Breathe? Yes.I" National Tuberculosis and Respiratory Diseases Bulletin, February 19^7, pp73^71 ■
__ , and Louise M. Nett. For Those Who Live and Breathe WithEmphysema and. Chronic Bronchitis. Springfield: Charles C.Thomas Publishers, 1967.'' x • :-Louise M. Nett, Boyd Bigelow, and David Ashbaugh. "The
Management of Acute and Chronic Respiratory Insufficiency," Archives of Environmental Health," 17:398-402, September 1968.
Pohl, Margaret L. "Teaching Activities of the Nursing Practitioner Nursing Research, 1.4:4-11, Winter 1969.
fl
Pohl-., Margaret L. Teaching Function of the Nursing Practitioner: Piibuque: William CP.BroWn Conpany^ 1958. . :' ' -'
Poulsen, Niels H. "Black Spot on the. Map," Arizona's Health, 2-:2-4,- v22, 23r June-July 1967.
Redman, Barbara King. The Process of Patient Teaching in Hursing.' St. Louis: The C. V. :M.osby Company.,~1958. .
Report of the Task Force on Chronic■Bronchitis . and•Emphysemao A reportprepared by the Rational Tuberculosis Association. Mount Morris, Illinois:. National Tuberculosis Association, May, 1967•
Robbins, Arthur, Harry Epstein,-Paul Diamond, M. J. Plishner, and. HaryeyPinkelstein. ’ "A Project'for the Prevention of Disability
• from Chronic Respiratory. Disease in Working Males," American', r 99:77-8$, January 1969..
Schlotfeldt, Rozella M. Problems on the;Development of Adequate •Criteria," Hursing Research, 2:211-213, Fall 1962.
Selltiz, Claire, Marie .Jahoda, MOrton Deutsch, and Stuart W. Cook.: Research Methods in; Social Relations. Hew York: HOlt,
Rinehart, and Winston, 1959«Silver, Harold M. "Disabled by Chronic R D--Is This the Final
. Answer?" Rational Tuberculosis and Respiratory Diseases Association Bulletjn7"5472 47~MaY' -9557~''
Simms, Laura L. The Hospital Staff Rurse Position as Viewed by Baccalaureat Graduates in Nursing. Hew York: Columbia
. University,'T953T™’Streeter, Virginia* "The Rurse‘s Responsibility for Teaching
Patients," American Journal of Hursing, 53:818-820, July' 1953. ’
Thornton, Thelma, and Robert C. Leonard. "Experimental Comparison. of Effectiveness of Three Hursing Approaches," Hursing Research, 13:122-125, Spring 1964.
Tryon, Phyllis A. "Patient Participation vs. Patient Passivity,".Hursing Forum, 2(2):48-57, 1963., and Robert C. Leonard. "A .Clinical Test of Patient CenteredHursing," Journal of Health and Human Behavior, 7:183-192, Fall 3.966.
Webster's Hew World Dictionary of the American Language., College Edition. Cleveland: "World Publishing "CompanyJ i960.

74Wright, Beatrice A. Physical Disability— A Psychological Approach*
New York:- ' Harper, and Row, igGo, . '■ Wundohl, Frank P., and William A. Fackler« "The Lif e Cycle -of Olin'
VAnsink," National Tuberculosis and Respiratory Disease Assp~. ; elation Bulletin%^4T3^5, November IgBBT^ ™"
I