The effect of body configuration on the strain magnitude ...
14
The effect of body configuration on the strain magnitude and distribution within the acetabulum during sideways falls: A finite element approach Shahab Khakpour a,⇑ , Petri Tanska b , Simo Saarakkala a,c,d , Rami K. Korhonen b , Timo Jämsä a,c,d a Research Unit of Medical Imaging, Physics, and Technology, University of Oulu, Oulu, Finland b Department of Applied Physics, University of Eastern Finland, Kuopio, Finland c Medical Research Center, University of Oulu and Oulu University Hospital, Oulu, Finland d Diagnostic Radiology, Oulu University Hospital, Oulu, Finland article info Article history: Accepted 24 November 2020 Keywords: Sideways fall Body configuration Acetabular fracture Hip fracture Effective strain abstract While the incidence of hip fractures has declined during the last decades, the incidence of acetabular frac- tures resulting from low-energy sideways falls has increased, and the mechanisms responsible for this trend remain unknown. Previous studies have suggested that body configuration during the impact plays an important role in a hip fracture. Thus, the aim of this study was to investigate the effect of body con- figuration angles (trunk tilt angle, trunk flexion angle, femur horizontal rotation angle, and femur diaph- ysis angle) on low-energy acetabular fractures via a parametric analysis. A computed tomography–based (CT) finite element model of the ground–proximal femur–pelvis complex was created, and strain magni- tude, time-history response, and distribution within the acetabulum were evaluated. Results showed that while the trunk tilt angle and femur diaphysis angle have the greatest effect on strain magnitude, the direction of the fall (lateral vs. posterolateral) contributes to strain distribution within the acetabulum. The results also suggest that strain level and distribution within the proximal femur and acetabulum resulting from a sideways fall are not similar and, in some cases, even opposite. Taken together, our sim- ulations suggest that a more horizontal trunk and femoral shaft at the impact phase can increase the risk of low-energy acetabular fractures. Ó 2020 The Author(s). Published by Elsevier Ltd. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/). 1. Introduction The incidence of low-energy acetabular and pelvic fractures has increased significantly in Finland (Kannus et al., 2015) and the Uni- ted Kingdom (Laird and Keating, 2005). At the same time, the inci- dence of hip fractures has declined (Korhonen et al., 2013). The mechanisms behind the change in the controversial incidence of acetabular and hip fractures remain unknown (Kannus et al., 2015). Finite element (FE) analysis is a noninvasive tool to study side- ways falls (Li et al., 2006; Majumder et al., 2004; Shim et al., 2010; Watson et al., 2017) and can provide reasonable accuracy (Parashar and Sharma, 2016). Without limitations to the loading type or number of simulations, it offers valuable information regarding internal and external forces and related tissue reactions, which can be used to predict fracture load and type of fracture (Shim et al., 2010). Nasari Sarvi and Luo (Nasiri Sarvi and Luo, 2017) reviewed stud- ies that used the aforementioned methods to measure or predict ground reaction force, hip fracture load, and fracture capacity. In vivo measurement of impact load or strain within acetabulum dur- ing sideways falls seems challenging, and was done only for pros- thetic hips during daily activities (Bergmann et al., 2001; Hodge et al., 1986). Ex vivo and computational studies on acetabular and pelvic fracture resulting from sideways impact were mostly con- ducted for high-energy trauma (motor vehicle accidents) (Dawson et al., 1999; Li et al., 2007; Majumder et al., 2004) in which the impact was applied directly to the acetabulum (Dawson et al., 1999; Majumder et al., 2004). Clarke et al. (2013), through a sensitivity analysis, used daily activities loading condi- tions to study acetabular stress–strain. To the best of our knowl- edge, the FE study by Shim et al. (2010) is the only one focusing on acetabular fracture resulting from a low-energy fall. They devel- https://doi.org/10.1016/j.jbiomech.2020.110156 0021-9290/Ó 2020 The Author(s). Published by Elsevier Ltd. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/). ⇑ Corresponding author at: University of Oulu/Faculty of Medicine/Research Unit of Medical Imaging, Physics and Technology, P.O. Box 5000, FI-90014 University of Oulu, Finland. E-mail address: Shahab.khakpour@oulu.fi (S. Khakpour). Journal of Biomechanics 114 (2021) 110156 Contents lists available at ScienceDirect Journal of Biomechanics journal homepage: www.elsevier.com/locate/jbiomech www.JBiomech.com
Transcript of The effect of body configuration on the strain magnitude ...

Journal of Biomechanics 114 (2021) 110156
Contents lists available at ScienceDirect
Journal of Biomechanicsjournal homepage: www.elsevier .com/locate / jb iomech
www.JBiomech.com
The effect of body configuration on the strain magnitude anddistribution within the acetabulum during sideways falls: A finiteelement approach
https://doi.org/10.1016/j.jbiomech.2020.1101560021-9290/� 2020 The Author(s). Published by Elsevier Ltd.This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
⇑ Corresponding author at: University of Oulu/Faculty of Medicine/Research Unitof Medical Imaging, Physics and Technology, P.O. Box 5000, FI-90014 University ofOulu, Finland.
E-mail address: [email protected] (S. Khakpour).
Shahab Khakpour a,⇑, Petri Tanska b, Simo Saarakkala a,c,d, Rami K. Korhonen b, Timo Jämsä a,c,d
aResearch Unit of Medical Imaging, Physics, and Technology, University of Oulu, Oulu, FinlandbDepartment of Applied Physics, University of Eastern Finland, Kuopio, FinlandcMedical Research Center, University of Oulu and Oulu University Hospital, Oulu, FinlanddDiagnostic Radiology, Oulu University Hospital, Oulu, Finland
a r t i c l e i n f o a b s t r a c t
Article history:Accepted 24 November 2020
Keywords:Sideways fallBody configurationAcetabular fractureHip fractureEffective strain
While the incidence of hip fractures has declined during the last decades, the incidence of acetabular frac-tures resulting from low-energy sideways falls has increased, and the mechanisms responsible for thistrend remain unknown. Previous studies have suggested that body configuration during the impact playsan important role in a hip fracture. Thus, the aim of this study was to investigate the effect of body con-figuration angles (trunk tilt angle, trunk flexion angle, femur horizontal rotation angle, and femur diaph-ysis angle) on low-energy acetabular fractures via a parametric analysis. A computed tomography–based(CT) finite element model of the ground–proximal femur–pelvis complex was created, and strain magni-tude, time-history response, and distribution within the acetabulum were evaluated. Results showed thatwhile the trunk tilt angle and femur diaphysis angle have the greatest effect on strain magnitude, thedirection of the fall (lateral vs. posterolateral) contributes to strain distribution within the acetabulum.The results also suggest that strain level and distribution within the proximal femur and acetabulumresulting from a sideways fall are not similar and, in some cases, even opposite. Taken together, our sim-ulations suggest that a more horizontal trunk and femoral shaft at the impact phase can increase the riskof low-energy acetabular fractures.� 2020 The Author(s). Published by Elsevier Ltd. This is an open access article under the CC BY-NC-ND
license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
1. Introduction
The incidence of low-energy acetabular and pelvic fractures hasincreased significantly in Finland (Kannus et al., 2015) and the Uni-ted Kingdom (Laird and Keating, 2005). At the same time, the inci-dence of hip fractures has declined (Korhonen et al., 2013). Themechanisms behind the change in the controversial incidence ofacetabular and hip fractures remain unknown (Kannus et al.,2015).
Finite element (FE) analysis is a noninvasive tool to study side-ways falls (Li et al., 2006; Majumder et al., 2004; Shim et al., 2010;Watson et al., 2017) and can provide reasonable accuracy (Parasharand Sharma, 2016). Without limitations to the loading type ornumber of simulations, it offers valuable information regarding
internal and external forces and related tissue reactions, whichcan be used to predict fracture load and type of fracture (Shimet al., 2010).
Nasari Sarvi and Luo (Nasiri Sarvi and Luo, 2017) reviewed stud-ies that used the aforementioned methods to measure or predictground reaction force, hip fracture load, and fracture capacity. Invivo measurement of impact load or strain within acetabulum dur-ing sideways falls seems challenging, and was done only for pros-thetic hips during daily activities (Bergmann et al., 2001; Hodgeet al., 1986). Ex vivo and computational studies on acetabular andpelvic fracture resulting from sideways impact were mostly con-ducted for high-energy trauma (motor vehicle accidents)(Dawson et al., 1999; Li et al., 2007; Majumder et al., 2004) inwhich the impact was applied directly to the acetabulum(Dawson et al., 1999; Majumder et al., 2004). Clarke et al. (2013),through a sensitivity analysis, used daily activities loading condi-tions to study acetabular stress–strain. To the best of our knowl-edge, the FE study by Shim et al. (2010) is the only one focusingon acetabular fracture resulting from a low-energy fall. They devel-

S. Khakpour, P. Tanska, S. Saarakkala et al. Journal of Biomechanics 114 (2021) 110156
oped a hemipelvis FE model for two quasi-static loading scenarios:falling from standing height (low energy) and impact applied by acar dashboard (high energy).
Among all biomechanical factors, body configuration at theimpact can remarkably affect the severity and type of hip andacetabular fractures resulting from low-energy sideways falls(Butterwick et al., 2015; Nankaku et al., 2005; Nasiri and Luo,2017). The impact force is transmitted via the greater trochanterto the femoral neck and head and finally to the acetabulum(Butterwick et al., 2015). We hypothesized that body configurationat the moment of impact will affect the risk of a low-energyacetabular fracture. We simulated the effect of different body con-figurations on strain magnitude, time-history response, and distri-bution within the acetabulum during sideways falls as a sign ofacetabular fracture probability. A computed tomography (CT) -based FE model of the ground–proximal femur–pelvis complexwas used.
2. Materials and methods
A research permit was granted by the institutional ethical com-mittee. Cortical and trabecular bones of the proximal femur andpelvic girdle of a 50th percentile male patient with no fracture his-tory were thresholded and segmented in Mimics� (version 21.0,Materialise Software, Belgium) by using abdominal CT data col-lected in Oulu University Hospital (Philips, 110 kVp, 105 mAs,453 slices with 0.5 mm thickness, resolution 0.75 � 0.75 mm2).The cortical thickness in four different regions of the acetabulumis presented and compared with measurements of Giudice et al.(Sebastian Giudice et al., 2018) in Appendix A. Also, the assignedmaterials at the hip joint were depicted in Fig. 1a. The obtainedthree-dimensional (3D) model included right proximal femur,sacrum and left and right coxal bones. Ramos and Simões (Ramosand Simões, 2006) showed that linear and quadratic tetrahedraland hexahedral elements (converged meshes) in the simulationof the proximal femur do not yield a significant difference. There-fore, by considering the model size and to reduce the computationcosts, the Solid285 elements (3D 4-node mixed u-P tetrahedralfirst-order elements) in ANSYS Autodyn� (version R19.2, ANSYS,USA) were used. To avoid volumetric and shear locking (Bonetet al., 2001), especially in the thin cortical bone regions, nodal-based strain formulation was considered for the bony parts. Thefinal mesh (element size 1.16–6.06 mm, comparable to previousstudies (Fleps et al., 2018; Majumder et al., 2007)), was selectedbased on a prior mesh convergence study. The total degree of free-dom in the model was equal to 406182.
2.1. Material properties
The material parameters are presented in Table 1 and relateddetails are given in Appendix B.
The origin and insertion regions for the hip and pelvic ligamentswere estimated based on the Human Biodigital� online platform.The ligaments were modeled using tension-only linear springs(in ANSYS Autodyn�). More details in Appendix C. Muscle forceswere not included as a relaxed freefall scenario.
2.2. Body configuration
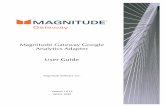
Since posture during CT imaging differs from that during a side-ways fall, the obtained model parts were saved in STEP format andexported to ANSYS SpaceClaim� (version R19, ANSYS SCDM, USA)for appropriate positioning. Four angles defining body posturewere defined (Fig. 1c): (1) trunk tilt angle (Trunk-Tilt or TTA):the angle between the midline of the S1 vertebrae and the vertical
2
line in the coronal plane, (2) trunk flexion angle (Trunk-Flex orTFA): the relative angle between the midlines of the S1 vertebraeduring supine and flexed postures in the sagittal plane (pelvic tiltangle in the sagittal plane), (3) femur horizontal plane rotationangle (Femur-Rotate or FHA): the angle between the centerline ofthe femur head and acetabulum in the sagittal plane, and (4) femurdiaphysis angle (Femur-Diaphysis or FDA): the angle between cen-terline of femur diaphysis and the horizontal line in the coronalplane. These angles were previously used (Boulay et al., 2006;Ford, et al., 1996; Luo and Sarvi, 2015; Luo et al., 2014; Sarviet al., 2014).
A parametric analysis was conducted where each of angle wasvaried in four stages in the FE model based on previous motion-capture studies (Luo et al., 2014; Sarvi et al., 2014; van derZijden et al., 2012), experimental investigation (Boulay et al.,2006; Ford et al., 1996; Grassi et al., 2012; Holzer et al., 2009;Keyak et al., 2001; van den Kroonenberg et al., 1996), and ananatomical feasibility study (Keyak et al., 2001). In each model,the other three angles were kept constant during parametric inves-tigation (Table 2). The used initial and boundary conditions arereported in Appendix B.
2.3. Solution
Thirteen models (Table 2) were simulated using explicitdynamic analysis. Impact phase durations have been reported torange from 40 ms (Fleps et al., 2018) to 100 ms (Luo et al., 2014).Majumder et al. (2007) stated a time to peak force ranging from13 to 23 ms for different trochanteric soft tissue thicknesses. In thisstudy, the models were solved by ANSYS Autodyn� for a durationof 100 ms with a stable time step of 3.30 � 10�4 ms. The averageCPU time per parallel run (16 cores (2.5 GHz) and 48 GBs ofRAM)) was 86 h.
The maximum effective strain (ESmax), as used by Westerling(2002) for modeling failure, was used as indicators of acetabularfracture risk, and ES (Appendix D) distribution (determining typeof fracture) was considered to find the regions more susceptibleto acetabular fracture (Xiao and Hu, 2019). Since this study aimedto focus on the effect of body posture on strain magnitude and dis-tribution, the lateral (the lunate surface of the acetabulum and theacetabular fossa) and medial (the inner wall of the acetabulum)surfaces of the acetabular cortical bone (Fig. 1d) were selected asregions of interest.
3. Results
3.1. Ground reaction force
The effect of body posture on the GRFmax (see Appendix E forGRFmax components) was substantial. Trunk-Tilt and Femur-Rotate exhibited a similar effect (17.8% and 17.5%, respectively)on GRFmax variation. When increasing Trunk-Tilt from 35� to 50�,GRFmax was reduced from 2271 N to 1905 N (Fig. 2a). The Trunk-Flex variation had the greatest effect (30.8%) on GRFmax. Whenincreasing Trunk-Flex from 0� to 10�, GRFmax rose from 1905 N to2470 N and remained at a high level at 20� and 30� (Fig. 2a).Femur-Rotate 15�, 30�, and 45� resulted in higher GRFmax thanFemur-Rotate 0�. Femur-Diaphysis variation also significantlyinfluenced GRFmax (24.8% variation in GRFmax). When increasingFemur-Diaphysis from 0� to 10�, GRFmax first increased (1905 Nto 2440 N) while at Femur-Diaphysis 10� and Femur-Diaphysis15�, GRFmax was nearly unchanged (Fig. 2a). The up-to-end of sim-ulations impulse (I100ms) and up-to-GRFmax (IGRFmax) impulse (areaunder the GRF curves) for each of the configurations are presentedand discussed in Appendix E.

Fig. 1. (a) Assigned materials (Table 1) at the hip joint. (b) Typical body posture at the impact and the applied boundary conditions. (c) Body configuration defining angles(TTA (Trunk Tilt Angle), TFA (Trunk Flexion Angle), FHA (Femur Horizontal rotation Angle), and FDA (Femur Diaphysis Angle)). (d) Lateral (the lunate surface of theacetabulum and the acetabular fossa) and medial (the inner wall of the acetabulum) surfaces of the acetabulum (the region of interest).
Table 1Material properties of the ground- proximal femur- pelvis complex.*
Tissue/part Model Density(q)
Elasticmodulus (E)
Poisson ratio (m) Yield strength (ryÞ Post-yield tangentmodulus (ET)
Cortical bone Isotropic homogenousbilinear
1900 Kgm�3 a
17.00 GPa b 0.30b 118.00 MPa c 850.0 MPa d
Trabecular bone Isotropic homogenousbilinear
1061 Kgm�3 e
70.00 MPa b 0.20b 3.09 MPa f 3.5 MPa d
Density(q)
C10 C01 C11 IncompressibilityParameter (d1Þ
Sacroiliac cartilage &interpubic disc
Compressible hyperelasticmooney-rivlin
1100 Kgm�3 g
0.10 MPa h 0.45 MPa h 0.60 MPa h 0.0036 MPa�1h
Density(q)
Poisson ratio(m)
Instantaneous shearmodulus (G0Þ
Characteristicrelaxation time (s)
Dimensionless shearmoduli (a)
Polyurethane foam Viscoelastic maxwell 72 Kg m�3
i0.45 i 34.50 MPa i 10.00 s i 0.05 i
Density(q)
Initial shear modulus (l) Incompressibility parameter (d2)
Articular cartilage Compressible hyperelasticneo-hookean
1100 Kgm�3 g
5.32 MPa j 0.0036 MPa�1h
aCameron et al. (Cameron and Grant., 1999), b Watson et al. (2017), c Leng et al. (Leng, Dong, and Wang, 2009), d Majumder et al. (Bayraktar et al., 2004), e Vivanco et al.(Vivanco et al., 2014), f Zhang et al. (Zhang, Magland, Rajapakse, Lam, and Wehrli, 2013), g Bortel et al. (Bortel et al., 2017), h Li et al. (Li et al., 2006), i Mills et al. (Mills, 2006), j
Henak et al. (Henak et al., 2014).* Elastic modulus (E) and postyield tangent modulus (ET) explained in Appendix A, Eq. (1). The corresponding yield strain (ey) for the cortical bone was 0.007 (Bayraktar
et al., 2004). The applied loading during an impact was impulse type (instantaneous). Cartilage tissues were modeled as hyperelastic materials (Papanicolaou and Zaoutsos,2019). Both the sacroiliac cartilage (Vleeming et al., 2012) and the interpubic disc (Becker et al., 2010) were modeled as fibrocartilage using the compressible Mooney-Rivlin(three-parameter) model (i.e., hyperelastic, Appendix A, Eq. (2)) using material parameters C10, C01, C11, and d1. A thick mattress made from open-cell (with shock absorberapplication) polyurethane foamwas modeled as a viscoelastic material using a Prony series–based material description of a single Maxwell element (Appendix A, Eq. (3)) withviscoelastic material parameters G0, a, and s. The acetabular and femoral cartilages were hyaline type and were modeled as a compressible neo-Hookean model (Appendix A,Eq. (4)) using material parameters l and d2.
S. Khakpour, P. Tanska, S. Saarakkala et al. Journal of Biomechanics 114 (2021) 110156
3

Table 2Body posture defining angles (TTA, TFA, FHA, and FDA) for different sideways fallconfigurations.
Studied angles Constant angles
TTA 35�, 40�, 45�*, 50�** TFA0�, FHA0�, FDA0�TFA 0�**, 10�, 20�, 30� TTA50�, FHA0�, FDA 0�FHA 0�*, 15�, 30�, 45� TTA45�, TFA0�, FDA 0�FDA 0�**, 5�, 10�, 15� TTA50�, TFA0�, FHA0�
TTA: Trunk Tilt Angle, TFA: Trunk Flexion Angle, FHA: Femur Horizontal planerotation Angle, FDA: Femur Diaphysis Angle.Models marked by * or ** represent the same body posture.
S. Khakpour, P. Tanska, S. Saarakkala et al. Journal of Biomechanics 114 (2021) 110156
3.2. Proximal femur effective strain magnitude
ESmax within the proximal femur (Fig. 2b) was more sensitive tobody configuration than ESmax within the acetabulum (Fig. 2c), andplastic deformation (e > 0.007) was observed in all the studiedbody postures only in the proximal femur. Trunk posture alsoshowed a considerable effect on ESmax changes within the proximalfemur (from 0.019 to 0.043 for Trunk-Tilt and 0.035 to 0.048 forTrunk-Flex). By increasing Trunk-Tilt, ESmax was generally elevated(in contrast to GRFmax) whereas the increase in Trunk-Flex firstresulted in a decrease and then an increase of ESmax within theproximal femur (Fig. 2b). Changes in the Femur-Rotate andFemur-Diaphysis led to variation in ESmax within the proximalfemur ranging from 0.015 to 0.061 and from 0.013 to 0.043, respec-tively. Higher Femur-Rotate (30� and 45�) caused remarkablyhigher ESmax in comparison with lower Femur-Rotate (0� and15�) (0.061 and 0.043 vs. 0.026 and 0.015, respectively). In contrastto GRFmax, when increasing Femur-Diaphysis from 0� to 10�, theESmax in the proximal femur decreased considerably (from 0.043to 0.013). Interestingly, further increasing the Femur-Diaphysisfrom 10� to 15� increased the ESmax in the proximal femur(Fig. 2b). Femoral orientation (Femur-Rotate and Femur-Diaphysis) had a greater impact on ESmax variation within theproximal femur in compression with trunk orientation (Trunk-Tilt and Trunk-Flex) (120% and 108% vs. 77% and 30%, respectively).
3.3. Acetabular effective strain magnitude
ESmax within the acetabulum remained under the yield point.The influence of Trunk-Tilt and Femur-Diaphysis variations onESmax (ranging from 0.0033 to 0.0040) within the acetabulum weresimilar and considerable (20% of variation). In contrast to GRFmax,when increasing Trunk-Tilt, ESmax mostly elevated whereas the risein Femur-Diaphysis led to a decline in ESmax (Fig. 2c). Trunk-Flexalteration showed a minor effect (13.8%) on ESmax variation withinthe acetabulum. By increasing Trunk-Flex from 0� to 10�, the ESmax
declined from 0.0040 to 0.0035 and then grew gradually fromTrunk-Flex 10� to Trunk-Flex 30� (0.0038) (Fig. 2c). Femur-Rotateinfluence on the ESmax variation was the least among the studiedangles, ranging from 0.0034 to 0.0037. Lower Femur-Rotate (0�and 15�) resulted in higher ESmax than higher Femur-Rotate (30�and 45�) (Fig. 2c). By increasing Femur-Diaphysis from 0� to 10�,ESmax fell from 0.0040 to 0.0033 and remained constant afterward.
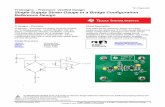
3.4. Acetabular effective strain distribution
Changes in body posture led to moderate differences in the ESdistribution within the acetabulum. ES concentration wasobserved mostly at the anterosuperior region of the lateral andmedial surfaces (Fig. 3). By changing Trunk-Tilt, ES distributionremained almost constant, and only the region with high ES valuesmoved slightly from the superior toward the inferior regions of themedial and lateral surfaces. In contrast to Trunk-Tilt, Trunk-Flexchange resulted in an obvious alteration in ES distribution at the
4
medial surface (Fig. 3). By increasing Trunk-Flex, ES concentrationlocation changed from the acetabular fossa to the rim at the lateralsurface. Furthermore, for the extreme values of Trunk-Flex (0� and30�), the highest ES was observed at the posterior region whereasthe region with high ES values for Trunk-Flex 10� and Trunk-Flex20� were divided into two areas at the anterior and posteriorregion of the medial surface (Fig. 3). Femur-Rotate variation hada remarkable effect on ES distribution. ES concentration forFemur-Rotate 0� and Femur-Rotate 15� was located at the anteriorrim of the lateral surface and the anterior region of the medial sur-face whereas the high ES region was almost faded at the anteriorrim of the lateral surface and was split in two regions at the ante-rior and posterior regions of the medial surface for Femur-Rotate30� and Femur-Rotate 45� (Fig. 3). Femur-Diaphysis had the lowestinfluence among the studied angles on ES distribution within theacetabulum. For almost all Femur-Diaphysis, the highest ES valuesappeared at the anterior and inferior regions (especially at theanterior rim) of the lateral surface and the anterior area of themedial surface. By increasing Femur-Diaphysis, the region withthe high ES at the medial surface expanded gradually toward thesuperior and inferior regions (Fig. 3).
The Pearson correlation coefficients between angle variation,GRFmax, Time-to-GRFmax, IGRFmax, and ESmax within the proximalfemur and acetabulum can be found in Appendix E. Also, theresults and discussion related to the effect of body configurationon the acetabular effective strain time history is presented in theAppendix F.
4. Discussion
We investigated the effect of body posture on the fall severityand magnitude, time response, and distribution of effective strainwithin the acetabulum and proximal femur. This was conductedthrough explicit FE analysis of a CT-based model in different bodyconfigurations, simulated by changing four angles defining bodyposture at impact. To the best of our knowledge, this is the firststudy comprehensively evaluating the effects of body configura-tion on fall severity. This study suggests that body configurationduring sideways falls affects more substantially the proximalfemur than the acetabulum, and fall direction has a remarkableeffect on the magnitude of GRFmax. Remarkably, varying Trunk-Tilt and Femur-Diaphysis affect GRFmax and ESmax differently.Moreover, our results suggest that a more horizontal trunk (higherTrunk-Tilt) and femur shaft (lower Femur-Diaphysis) cause higherlevels of strain within the acetabulum.
4.1. Model validation
The models were validated against previous experimental stud-ies on low-energy sideways falls since no direct empirical validationwas available. The time history of GRF was compared with experi-mental measurements (Sarvi et al., 2014; van der Zijden et al.,2017) (see Appendix G, Fig. F). Generally, the GRF increases sharplyup to theGRFmax (0–40ms) and remains at the same level for awhile(40–60ms) and thengradually decreases (60–100ms). Although theGRFmax magnitude and time-to-GRFmax were not the same betweenthe current study and the experiments, considering the difference intesting conditions between these studies, the time response of theGRF of ourmodelswas in good agreementwith theirmeasurements.
4.2. Body configuration effect on GRFmax
We observed fairly moderate GRFmax values (1905.4–2598.3 N).While some studies (Fleps et al., 2018; Majumder et al., 2007; vander Zijden et al., 2012) have reported significantly higher

Fig. 2. Body posture effect (TTA (Trunk-Tilt), TFA (Trunk-Flex), FHA (Femur-Rotate), and FDA (Femur-Diaphysis)) on the magnitude of (a) Maximum ground reaction force. (b)Maximum effective strain within the proximal femur. (c) Maximum effective strain within the acetabulum. (Dashed line = mean value).
S. Khakpour, P. Tanska, S. Saarakkala et al. Journal of Biomechanics 114 (2021) 110156
GRFmax values (4000–8600 N) resulted from falling from standing,other studies (Luo et al., 2014; Sarvi et al., 2014; van der Zijdenet al., 2017; Varga et al., 2016) have presented GRFmax of 1750–2800 N. Shim et al. (2010) experimentally obtained an acetabularfracture load of 3400 N, which was not exceeded in any of our sim-ulations, explaining no plastic deformation in our study.
Luo et al. (2014) reported GRFmax equal to 1902.7, 1751.0 and2967.1 N for Trunk-Tilt 37.8�, 40.2� and 48.1�, respectively. Therewas no obvious relationship between Trunk-Tilt variation andGRFmax, but it should be noted that the other angles defining body
5
configuration at impact were not kept constant between theirstudy subjects. Although Trunk-Tilt has the least effect on GRFmax
among the studied angles, our results suggest that a more horizon-tal trunk at the impact (Trunk-Tilt 45� and 50�) could decrease fallseverity by lowering GRFmax, confirming the hypothesis of Groenet al. (2007). An explanation could be that a more horizontal trunkincreases the distance between the upper-extremity and pelvicweights (labeled as C and B in Fig. 1b respectively) with the hiprotation center in the coronal plane. Consequently, the pelvic girdlerotates more extensively (an increase in rotational momentum)

Fig. 3. Effect of the TTA (Trunk-Tilt), TFA (Trunk-Flex), FHA (Femur-Rotate), and FDA (Femur-Diaphysis) at the impact on the effective strain distribution. Upper rows: Lateral(the lunate surface of the acetabulum and the acetabular fossa). Lower rows: the medial (the inner wall of the acetabulum) surfaces of the acetabulum.
S. Khakpour, P. Tanska, S. Saarakkala et al. Journal of Biomechanics 114 (2021) 110156
and results in the generation of an upward force through the hipjoint ligaments and finally reduces the GRFmax. Our findings onthe effect of fall direction on GRFmax is consistent with the studyof Nasiri and Luo (2017). Here, a more flexed trunk at impact(Trunk-Flex 10�, 20�, and 30�) increased GRFmax extensively. Inthe opposite way to Trunk-Tilt, by increasing the Trunk-Flex, thedistance between the upper-extremity and pelvic weights withthe hip rotation center in the sagittal plane decreases. It leads toa decrease in the upward force generated by hip ligaments andconsequently an increase in GRFmax. Through an experimentalstudy, Nankaku et al. (2005) found a non-significant trend forhigher GRFmax resulting from a posterolateral compared to lateralfall. In our study, the average of GRFmax (2309.8 N) force for a lat-eral fall (Femur-Rotate 0� and 15�) was 2.7% higher than the aver-age GRFmax (2247.1 N) for a posterolateral fall (Femur-Rotate 30�and 45�). In addition, a nonhorizontal femur shaft at impact leadto higher values of GRFmax. Van der Zijden et al. (2012) comparedGRFmax for two falling techniques from kneeling height: blockand martial arts. The block techniques led to higher Femur-Diaphysis and GRFmax in comparison with the martial arts tech-nique, also confirming our results. Whereas during the martialart techniques both femur and pelvis rotate together, during theblock techniques, the pelvis girdle is rotating and the femur isattached to the ground horizontally (low Femur-Diaphysis) whichcauses the hip ligaments to experience higher extension and pro-duce more upward force, leading to decrease in GRFmax.
4.3. Fracture risk assessment: GRFmax vs. ESmax
Many researchers tried to use GRFmax to assess the risk of frac-ture (Nasiri Sarvi and Luo, 2017). But, it should be noted that a
6
higher magnitude of GRFmax does not necessarily imply a higherrisk of fracture. For instance, by increasing Trunk-Tilt, GRFmax
declined, while ESmax increased for both the proximal femur andacetabulum, or by increasing Femur-Diaphysis, even thoughGRFmax increased, ESmax decreased within the proximal femurand the acetabulum. These can be addressed in the context ofthe generated force by the hip ligaments and the moment arms.While the tensile force generated in the hip ligaments tends to pro-duce an upward force and reduce GRF, it also causes the femoralhead to compress the acetabulum (frictionless contact) andincreases the strain energy within the hip region (increase inESmax). Also, in the case of Femur-Diaphysis, by increasing theangle, the moment arm of GRFmax decreases, and consequentlythe exerted moment of force declines.
4.4. Body configuration effect on ESmax within the proximal femur
Majumder et al. (2008) assumed that the body is with supineposture (Trunk-Tilt 90�) at impact, which may lead to underesti-mation of the impact velocity and fall severity (Majumder et al.,2007). Our study suggests while an increase in Trunk-Tilt causesa decrease in GRFmax, this generally leads to increased ESmax withinthe proximal femur and acetabulum. Trunk-Flex had a minor effecton ESmax variation within the proximal femur. Majumder et al.(2009) studied the effect of Femur-Diaphysis on strain magnitudeand distribution during a backward fall. In another study(Majumder et al., 2007), by including the soft tissue and assuminga completely horizontal trunk at the lateral fall, the maximumcompressive strain within the trochanter was about 0.035, compa-rable to our study (0.043 for Trunk-Tilt 50�, the most (not com-pletely) horizontal trunk).

S. Khakpour, P. Tanska, S. Saarakkala et al. Journal of Biomechanics 114 (2021) 110156
4.5. Body configuration effect on ESmax within the acetabulum
Our study showed that a more horizontal trunk (larger Trunk-Tilt) and femoral shaft (smaller Femur-Diaphysis) at impact leadsto higher ESmax within the acetabulum and could be associatedwith a higher risk of acetabular fracture. In addition to the changein the force generated by the hip ligaments, the change in theacetabular coverage angle (by an increase in Trunk-Tilt or adecrease in Femur-Diaphysis) may lead to the establishment of astronger contact between femoral head and acetabulum and finallyincrease of ESmax and the risk of fracture. Furthermore, trunk flex-ion had a negligible effect on ESmax within the acetabulum, and thelateral falls (Femur-Rotate 0� and 15�) resulted in a slightly higherESmax than during posterolateral fall. Finally, our results suggestthat a proximal femur fracture could occur more likely during aposterolateral fall while an acetabular fracture could be more likelyto occur during a lateral fall. It could owe to that during a lateralfall, the GRF is almost acting in the vertical direction (higher Z-Component, see Appendix E) and produce a shear force in the com-bination of the upper-extremity weight. Since the cortical bone isthicker and trabecular bone is denser within the proximal femurthan the acetabulum, the proximal femur transfers the force tothe acetabulum and experiences lower ESmax than the acetabulum.In the posterolateral fall, the GRF vector is far from the upper-extremity weight and not mostly vertical (higher X and Y-Components). This leads to applying a bending moment and con-centration of the impact energy in the femoral neck, instead ofthe acetabulum. These results are in good agreement with Nan-kaku et al. (Nankaku et al., 2005) finding a posterior lateral fallas the highest risk of proximal femur fracture.
4.6. Body configuration effect on ES distribution within the acetabulum
Effective strain distribution within the acetabulum depends onthe way of contact establishment between femoral head cartilageand the lunate surface of the acetabulum which itself is dependentof contact force magnitude and direction (the body configurationat the impact) (Wang et al., 2017). The anterior column combinedwith posterior hemitransverse is a typical geriatric acetabular frac-ture type (Culemann et al., 2010), which is consistent with the pre-dicted ES distribution (i.e., strain concentration locations) in ourstudy for almost all models. The present study suggests that whileTrunk-Flex does not have a substantial effect on ESmax, it may influ-ence ES distribution within the acetabulum and thus might con-tribute to the type of acetabular fracture. Again, our studyrevealed that fall direction (lateral vs. posterolateral) has a consid-erable role in the type of acetabular fracture. The high-ES-concentration locations predicted here for a posterolateral fall(Femur-Rotate 30� and 45�) are similar to the posterior columnfracture (Letournel, 2019; Shim et al., 2010).
4.7. Body configuration effect on ES: Proximal femur vs. acetabulum
Our results showed that the effect of different body configura-tions on ESmax and GRFmax variation within the proximal femurand acetabulum is not the same. Since the proximal femur is hitinitially by the ground and subsequently by the pelvis, it mightbe more sensitive to body configuration whereas the acetabulumexperiences the impact exerted by the femoral head at the impact.This could explain why, while GRFmax and the acetabular ESmax ofposterolateral and lateral falls were relatively similar, ESmax inthe proximal femur during posterolateral falls (Femur-Rotate 30�and Femur-Rotate 45�) was substantially higher than during lateralfalls (Femur-Rotate 0� and Femur-Rotate 15�). This finding is con-sistent with previous studies. Keyak et al. (2001) found a 46.3%
7
lower fracture load resulted from posterolateral in comparisonwith lateral falls. Similarly, Ford et al. (1996) reported that thestructural capacity (the minimum force required to onset struc-tural collapse) of the femur decreased by 26% with increasedFemur-Rotate. Since femur geometry and material properties werekept constant in our study, the observed difference in ESmax
between lateral and posterolateral falls is most likely related tothe change in loading direction. The study limitations and thefuture work are presented in Appendix H.
5. Conclusion
This study showed that body configuration during sidewaysfalls can remarkably affect the risk of acetabular fracture and fallseverity. Furthermore, for different body configurations, strainmagnitude and distribution within the proximal femur and acetab-ulum during a sideways fall are not similar, and in some cases, suchas lateral and posterolateral falls, seem to be even opposite. Therisk of acetabular fracture resulting from a more horizontal trunkand proximal femur shaft during a sideways fall seems higher thanfor other body configurations. The information obtained in these FEsimulations can be valuable in the fracture risk assessment, fallprevention, and design of protective measures such as hip pads.
Declaration of Competing Interest
The authors declare that they have no known competing finan-cial interests or personal relationships that could have appearedto influence the work reported in this paper.
Acknowledgements
This project was supported by the I4Future doctoral programunder the Marie Skłodowska-Curie grant agreement No 713606.CSC – IT Center for Science LTD, Finland, is acknowledged for pro-viding FE software and computational resources.
Appendix A. Trabecular bone and cartilage modeling, andacetabular cortical thickness
It was assumed that trabecular bone has filled the cortical bonecavity. Since the CT images were not acquired with a contrastagent, the femoral, acetabular (Mechlenburg et al., 2007) andsacroiliac cartilages (Zheng et al., 1997), and interpubic disc (Liet al., 2006) were added by using 3-matic� (version 13.0, Materi-alise Software, Belgium).
The location-dependent cortical thickness was obtained viaslice-by-slice local thresholding (662–1988 HU). The obtainedthicknesses were in the typical range (Du et al., 2018; SebastianGiudice et al., 2018). The acetabular cortical bone thicknessmeasurement is presented in four cross-sections. The measuredthicknesses are consistent with Giudice et al. (Sebastian Giudiceet al., 2018) who reported the ranges of 0–2.4 mm and1.8–3.6 mm for the cortical thicknesses of the acetabular fossaand rim of the acetabulum, respectively.
Meshes were refined especially around the region of interestand contact areas (acetabulum, femoral head, and the greatertrochanter). The element edge length at the thinnest region ofthe acetabulum was about 1.16–1.35 mm (aspect ratio was keptless than10), corresponding to five to nine tetrahedral elementsthrough the thickness.

S. Khakpour, P. Tanska, S. Saarakkala et al. Journal of Biomechanics 114 (2021) 110156
Appendix B. Material models, initial and boundary conditions
-Material Models:
- Incompressible homogenous isotropic bilinear model (corticaland trabecular bones)
r ¼ Ee;r < ry
ETe;r � ry
�ð1Þ
8
where r, e, and ry are stress, strain, and yield strength, respectively.ET was set as 0.05 � E and 0.001 � E [7] for the cortical and trabec-ular bones, respectively.
A wide range of yield (ey = 0.0036–0.0115) and ultimate strains(eu = 0.013–0.036) have been reported for different testing direc-tions and loading modes (Wolfram and Schwiedrzik, 2016). For thisstudy, we considered ey = 0.007 (the yield strength divided by theelastic modulus). The ultimate strain for the onset of microcracksdepends on bone microstructure, degree of mineralization, osteo-porosis level, and microdamage present in the bone (O’Brien

S. Khakpour, P. Tanska, S. Saarakkala et al. Journal of Biomechanics 114 (2021) 110156
et al., 2005) and varies from individual to individual. Based on thereported yield and ultimate strain by Wolfram & Schwiedrzik(Wolfram and Schwiedrzik, 2016), a rough estimate of the criticalstrain change could be 0.0094–0.0245.
- Compressible Mooney-Rivlin (three-parameter) model (sacroil-iac cartilage and interpubic disc)
W ¼ C10 I�1 � 3
� �þ C01 I
�2 � 3
� �þ C11 I
�1 � 3
� �I�2 � 3
� �
þ 1d1
ðJ � 1Þ2 ð2Þ
where W is the strain energy density function. I�1, I
�2 and I
�3 are
invariants of the volume change eliminated left Cauchy–Greendeformation tensor (i.e. B). d1 is the incompressibility parameter(for the Mooney-Rivlin model), and J is the determinant of thedeformation gradient tensor.
- Time-dependent Maxwell viscoelastic material model (opencell polyurethane foam)
GðtÞ ¼ G0 1� aþ ae�t=s� � ! t ¼ 0 ! G 0ð Þ ¼ G0
t ! 1 ! G 1ð Þ ¼ G0ð1� aÞ�
ð3Þ
where G is the shear modulus. a and G0 are dimensionless andinstantaneous shear modulus, respectively, and s is the characteris-tic relaxation time (Table 1).
The trochanteric soft tissue consists of several tissues such asmuscle, fat, bursae, and skin with very different viscoelastic prop-erties and to best of our knowledge, for the trochanteric soft tissueas a whole, the viscoelastic parameters are not available in the lit-erature. One study (Bandak et al., 2001) presented these parame-ters for the constitutive tissues of the trochanteric soft tissue(bulk modulus = 3.666 and 48,330 psi; instantaneous shear modu-lus = 5.537 and 729.9 psi; equilibrium shear modulus = 7.383 and973.2 psi for muscle and fat layers respectively). Other studies pre-ferred to neglect the viscous behaviors of the trochanteric soft tis-sue and modeled it as a hyperelastic material (Fleps et al., 2018;Majumder et al., 2007). On the other hand, mattresses made fromviscoelastic polyurethane foam are used in the fall experiments(Nasiri Sarvi and Luo, 2017). Therefore, in this study to facilitatemodeling of body configurations and reduce the model size, thesoft tissue covering the greater trochanter was not included anda 13-cm thick mattress (Nankaku et al., 2005) made from polyur-ethane foam was added as the ground.
- Compressible neo-Hookean hyperelastic model (acetabular andfemoral cartilages)
12l I
�1 � 3
� �þ 1d2
J � 1ð Þ2 ð4Þ
where l is the shear modulus under infinitesimal strain, and d2 isthe incompressibility parameter for the neo-Hookean model.
-Initial and boundary conditions
It was assumed that during sideways falls, early contacts of theknees and outstretched arms with the ground happened, and thetrunk and lower-extremity inertias were negligible (van derZijden et al., 2012), and only the inertia of the proximal femur–pel-vis complex was included. Since the upper extremity was not con-sidered in the simulation, it was assumed that the degrees offreedom (DOF) of the pelvic girdle and trunk were tied to eachother (pelvic rotation = trunk rotation).
9
To reduce CPU time, the bottommost node of the femur–pelviscomplex was brought 0.1 mm to the ground. Sixty-five percent ofthe bodyweight of a 50th-percentile male (485 N) was appliedon the S1 vertebrae articular surface as the upper bodyweight(Majumder et al., 2004). The impact (initial) velocity(2.321 m s�1) (van den Kroonenberg et al., 1996) and the gravita-tional acceleration (Fig. 1b) were applied to the femur–pelvis com-plex. Because the trochanteric soft tissue was excluded, the impactvelocity was chosen from the lower reported range for low-energyfalls (Nasiri and Luo, 2017). The mattress nodes at the bottom andside walls were fixed in all DOFs to prevent ground movement(Fig. 1b). The distal region of the proximal femur was preventedfrom rotating about the diaphysis axis to simulate knee joint resis-tance (Ford et al., 1996). It was assumed that the outermost layer ofthe trabecular bone and the innermost layer of the cortical boneare matched, and the corresponding nodes are tied in all DOFs.The concave and convex sides of the femoral and acetabular carti-lages were tied to bone. The interpubic disc and sacroiliac carti-lages were rigidly attached to the in-contact bony regions. Forthe initial contact between the femoral and acetabular cartilages,the model was relocated so that the maximum penetration underthe contact areas remained under 0.1 mm. The contact betweenthe acetabular and femoral cartilages was assumed frictionless(Clarke et al., 2013; Fleps et al., 2018), and between the greater tro-chanter and ground frictional, with a friction coefficient of 0.5(Lemmon et al., 1997).
Appendix C. Ligament stiffness
The stiffnesses of the anterior/posterior sacroiliac, the long pos-terior sacroiliac, and the sacrospinous, sacrotuberous, and anterior/posterior/superior/inferior pubic ligaments were obtained from(Clarke et al., 2013) while the values for the ischiofemoral and ilio-femoral ligaments were obtained from (Hewitt et al., 2002) and thepubofemoral ligament from (Silvestri, 2008). Finally, the stiffnessvalues for the hip ligamentum teres were based on (O’Donnellet al., 2018).
Ligament
Stiffness (N/mm)Anterior sacroiliac
2400.0 Posterior sacroiliac 2400.0 Long posterior sacroiliac 530.0 Sacrospinous 800.0 Sacrotuberous 1200.0 Anterior pubic 800.0 Posterior pubic 800.0 Superior pubic 800.0 Inferior pubic 800.0 Pubofemoral 560.0 Iliofemoral 99.3 Ischiofemoral 36.9 Ligamentum teres 16.0Appendix D. Effective strain
Effective strain (incremental geometrical) is defined as follows(Westerling, 2002):
e� ¼
Z t
0
ffiffiffiffiffiffiffiffiffiffiffiffiffi23_eij _eij
rdt
wheree�and _eij are the effective and strain rate tensors, respectively.

Appendix E. Maximum ground reaction force components, up-to-end of simulation GRF impulse (I100ms), up-to-GRFmax GRF impulse(IGRFmax), time-to-GRFmax, and Pearson correlation coefficients
Maximum ground reaction force components (based on the coordinate system showed in Fig. 1.a)
Model X-Component (N) Y-Component (N) Z-Component (N) Sum (N)
Trunk-Tilt 35� 931.0 168.1 2065.2 2271.6Trunk-Tilt 40� 300.6 105.6 2159.7 2183.1Trunk-Tilt 45� 277.4 105.1 2083.7 2104.7Trunk-Tilt 50� 165.5 142.8 1892.8 1905.4Trunk-Flex 0� 165.5 142.8 1892.8 1905.4Trunk-Flex 10� 1033.6 214.9 2233.5 2470.4Trunk-Flex 20� 1083.3 207.6 2352.6 2598.3Trunk-Flex 30� 1107.1 244.0 2292.8 2557.8Femur-Rotate 0� 277.4 105.1 2083.7 2104.7Femur-Rotate 15� 1023.3 436.0 2255.6 2514.9Femur-Rotate 30� 1022.8 573.1 1869.5 2206.7Femur-Rotate 45� 1183.6 866.4 1755.3 2287.4Femur-Diaphysis 0� 165.5 142.8 1892.8 1905.4Femur-Diaphysis 5� 992.7 150.1 2025.9 2261.0Femur-Diaphysis 10� 1243.3 162.4 2097.7 2443.9Femur-Diaphysis 15� 1308.3 147.1 2010.6 2403.3
Up-to-end of simulation GRF impulse (I100ms), up-to-GRFmax GRF impulse (IGRFmax), and time-to-GRFmax
Model I100ms (Ns) IGRFmax (Ns) Time-to-GRFmax (ms)
Trunk-Tilt35� 131.8 53.4 38.5Trunk-Tilt40� 138.4 55.2 38.6Trunk-Tilt45� 147.7 56.1 39.7Trunk-Tilt50� 155.3 57.5 33.4Trunk-Flex 0� 155.3 57.5 33.4Trunk-Flex10� 163.0 57.6 40.1Trunk-Flex20� 169.0 60.2 41.6Trunk-Flex30� 167.1 56.3 40.0Femur-Rotate0� 147.7 56.1 39.7Femur-Rotate15� 155.0 55.3 33.8Femur-Rotate30� 142.5 47.4 39.4Femur-Rotate45� 142.3 51.4 38.6Femur-Diaphysis0� 155.3 57.5 33.4Femur-Diaphysis5� 153.6 54.8 40.1Femur-Diaphysis10� 149.6 54.8 37.2Femur-Diaphysis15� 143.8 54.1 37.2
Pearson correlation coefficients
Time-to-GRFmax IGRFmax ESmax: proximal femur ESmax: acetabulum
Angle variation: Trunk-Tilt �0.66 0.99 0.87 0.51Angle variation: Trunk-Flex 0.76 �0.08 0.37 �0.18Angle variation: Femur-Rotate 0.11 �0.71 0.63 �0.81Angle variation: Femur-Diaphysis 0.40 �0.88 �0.81 �0.93GRFmax: Trunk-Tilt 0.81 �0.96 �0.93 �0.62GRFmax: Trunk-Flex 0.99 0.24 0.10 �0.65GRFmax: Femur-Rotate �0.96 0.19 �0.46 0.41GRFmax: Femur-Diaphysis 0.67 �0.95 �0.99 �0.99Time-to-GRFmax: Trunk-Tilt 1.00 �0.65 �0.88 �0.70Time-to-GRFmax: Trunk-Flex 1.00 0.34 0.08 �0.70Time-to-GRFmax: Femur-Rotate 1.00 �0.41 0.65 �0.65Time-to-GRFmax: Femur-Diaphysis 1.00 �0.79 �0.67 �0.56IGRFmax: Trunk-Tilt �0.65 1.00 0.90 0.42IGRFmax: Trunk-Flex 0.34 1.00 0.46 �0.15IGRFmax: Femur-Rotate �0.41 1.00 �0.96 0.87IGRFmax: Femur-Diaphysis �0.79 1.00 0.90 0.92
S. Khakpour, P. Tanska, S. Saarakkala et al. Journal of Biomechanics 114 (2021) 110156
10

Fig. E. Effect of the angles defining the body posture at the impact on the effective strain time history: (a) TTA (Trunk Tilt Angle). (b) TRUNK-FLEX (Trunk Flexion Angle).(c) FEMUR-ROTATE (Femur Horizontal rotation Angle). (d) FEMUR-DIAPHYSIS (Femur Diaphysis Angle).
S. Khakpour, P. Tanska, S. Saarakkala et al. Journal of Biomechanics 114 (2021) 110156
Results showed that except Femur-Diaphysis, GRFmax isstrongly correlated to time-to-GRFmax (Trunk-Tilt and Trunk-Flexpositively and Femur-Rotate negatively). It means a delay in reach-ing GRFmax leads to a higher GRFmax for Trunk-Tilt or Flex, and alower GRFmax for Femur-Rotate.
11
Since the boundary conditions, geometry, materials, and thedistance of the bottommost node to the ground were kept fixedamong all models, the total GRF impulse is expected to remain con-stant, but by referring to the table containing I100ms - IGRFmax values,it is not exactly the case. This could be explained by the fact that

S. Khakpour, P. Tanska, S. Saarakkala et al. Journal of Biomechanics 114 (2021) 110156
the models (and therefore GRF curves) were solved only up to100 ms and the simulations did not continue until the stationaryphase (when the GRF must be equal to the bodyweight for all mod-els). Therefore, up-to-GRFmax impulse (IGRFmax) was considered forfurther discussion.
Strong correlations between IGRFmax and ESmax variation for allangles (except Trunk-Flex) indicate that GRF impulse directlyaffects the ESmax and consequently the risk of proximal femur frac-ture. A similar trend also exists within the acetabulum (IGRFmax isstrongly correlated with ESmax variation for Femur- Rotate andFemur-Diaphysis and moderately with Trunk-Tilt). These resultsshow that the proximal femur is affected by both trunk and femurconfigurations (proximal femur is pressed between trunk andground), but the acetabulum is more likely to be affected by femurconfiguration than trunk posture.
Result showed that only Trunk-Tilt and Femur-Diaphysis anglevariation within the proximal femur, and Femur-Rotate andFemur-Diaphysis with the acetabulum are strongly correlated withESmax variation directly. Again, only for the Trunk-Tilt and Femurdiaphysis cases, GRFmax is strongly (negative) correlated withIGRFmax and GRFmax in the case of Trunk-Tilt and Femur-Diaphysiswithin the proximal femur and Femur-Diaphysis within theacetabulum is strongly correlated with ESmax. Results showed thatthe angle variation affects the ESmax through IGRFmax. The body con-figuration angles (except Trunk-Flex) variation are strongly corre-lated with IGRFmax, which itself is strongly correlated with ESmax
within the proximal femur (except Trunk-Flex) and the acetabu-lum (except Trunk-Flex and moderately with Trunk-Tilt). Theseresults suggest the IGRFmax as a better predictor of the risk of frac-ture than GRFmax. It could have a root in the fact that GRF impulseis affected not only by GRF magnitude, but also by the time-to-GRFmax and the manner which is applied. Also, whereas the biggestGRFmax (2598.3 N) and biggest IGRFmax (60.2 Ns) belong to Trunk-Flex 20�, the highest ESmax within the proximal femur and acetab-ulum were observed in Femur-Rotate 30� and Trunk-Tilt 50� (equalto Trunk-Flex 0� and Femur-Diaphysis 0�) respectively. These
Fig. F. Model validation against experimental studies
12
results show that ESmax may provide wider and more critical infor-mation than GRFmax and IGRFmax about the risk of fracture since itsimultaneously depends on the magnitude, location, duration,and manner of all existing forces (Luo et al., 2014).
Appendix F. Acetabular effective strain time history
The changes in the studied angles affected the time-to-ESmax
(tp) and the oscillatory pattern of the ESmax experienced by theacetabulum during the impact phase. The initial effect(0–10 ms) of impact on the ES for all models were similar. Forsmaller Trunk-Tilt (35� and 40�), tp was shorter (20–30 ms) thangreater Trunk-Tilt (45� and 50�) (75–85 ms) (Fig. Ea). Interest-ingly, ESmax occurred during the early phase of the impact(25–30 ms) for Trunk-Flex 10� and 30� while for Trunk-Flex 0�and 20�, ESmax occurred during the late phase of the impact(75–85 ms) (Fig. Eb). For Femur-Rotate 0� and Femur-Rotate15�, the tp was greater (65–80 ms) than half of the studied per-iod, whereas ESmax happened much sooner (around 30 ms) forFemur-Rotate 30� and Femur-Rotate 45� and the ES declinedafterward (Fig. Ec). For all Femur-Diaphysis, ES behavior withinthe acetabulum during the impact was similar, and tp occurredbetween 70 and 85 ms. It seems that by increasing Femur-Diaphysis, the difference between the ESs within the acetabulumdeclines gradually (Fig. Ed).
Considering the inertias of bone during falling and the priorcontact of the knee with the ground, our findings support thehypothesis (in contrast with the assumption made by Majumderet al. (2007) that acetabular and femoral cartilages are not firmlytied together during the descent phase of sideways falls, and animpact happens between the femur and pelvis after the impactof the femur and the ground (Butterwick et al., 2015). This couldexplain the observed delay between ESmax and GRFmax peak times.For instance, for the case of Trunk-Tilt of 45� and 50�, GRFmax
occurred during 30–40 ms whereas ESmax occurred during75–85 ms. Also, several peaks of ES could be attributed to the
of M.N. Sarvi et al and A.M. van der Zijden et al.

S. Khakpour, P. Tanska, S. Saarakkala et al. Journal of Biomechanics 114 (2021) 110156
establishment of contact between the femoral and acetabularcartilages in conjunction with the contribution of hip ligamentsduring the impact phase.
Appendix G. Model validation
See Fig. F.
Appendix H. Study limitations and future work
This study has limitations. First, the material properties of thetissues were simplified, and heterogeneity, anisotropy, and vis-coelasticity of bone were not considered. Also, the trochanteric softtissue was not considered and instead surrogated by a thick foammattress, which differs from real soft tissue (Nasiri Sarvi and Luo,2017). Furthermore, since the abdominal CT images were usedfor creating the geometries, data regarding the trunk and shankinertias were not available and, therefore, only upper-extremitybody weight was considered. We did not includemuscle forces intothe model. Previously, Clarke et al. (Clarke et al., 2013) concludedthat muscle forces do not affect acetabular stress and strain duringa normal gait, but data during falls is lacking. Finally, only one CT-based model was used, and gender effect was not investigated. Infuture, parametric studies on the effect on impact velocity, mate-rial properties of trochanteric soft tissue, bone tissue, and groundon the acetabular fracture are of interest.
References
Bandak, F.A., Tannous, R.E., Toridis, T., 2001. On the development of an osseo-ligamentous finite element model of the human ankle joint. Int. J. Solids Struct.38 (10-13), 1681–1697.
Bayraktar, H.H., Morgan, E.F., Niebur, G.L., Morris, G.E., Wong, E.K., Keaveny, T.M.,2004. Comparison of the elastic and yield properties of human femoraltrabecular and cortical bone tissue. J. Biomech. 37 (1), 27–35.
Becker, I., Woodley, S.J., Stringer, M.D., 2010. The adult human pubic symphysis: Asystematic review. J. Anatomy, 217(5), 475–487. https://doi.org/10.1111/j.1469-7580.2010.01300.x
Bergmann, G., Deuretzbacher, G., Heller, M., Graichen, F., Rohlmann, A., 2001. Hipcontact and gait patterns from routine activities.PDF, 34, 859–871
Bonet, J., Marriott, H., Hassan, O., 2001. An averaged nodal deformation gradientlinear tetrahedral element for large strain explicit dynamic applications.Commun. Numer. Meth. Engng. 17 (8), 551–561.
Bortel, E.L., Langer, M., Rack, A., Forien, J.B., Duda, G.N., Fratzl, P., Zaslansky, P., 2017.Combining coherent hard x-ray tomographies with phase retrieval to generatethree-dimensional models of forming bone. Front. Mater. 4. https://doi.org/10.3389/fmats.2017.00039.
Boulay, C., Tardieu, C., Hecquet, J., Benaim, C., Mouilleseaux, B., Marty, C., Prat-Pradal, D., Legaye, J., Duval-Beaupère, G., Pélissier, J., 2006. Sagittal alignment ofspine and pelvis regulated by pelvic incidence: standard values and predictionof lordosis. Eur. Spine J. 15 (4), 415–422.
Butterwick, D., Papp, S., Gofton, W., Liew, A., Beaulé, P.E., 2015. Acetabular fracturesin the elderly: evaluation and management. J. Bone Joint Surgery-Am. 97 (9),758–768.
Cameron, J.R. . J. G. S. & R. M., & Grant, 1999. Physics of the Body (2nd ed.). Madison,WI: Medical Physics Publishing.
Clarke, S.G., Phillips, A.T.M., Bull, A.M.J., 2013. Evaluating a suitable level of modelcomplexity for finite element analysis of the intact acetabulum. Comput.Methods Biomech. Biomed. Eng. 16 (7), 717–724.
Culemann, U., Holstein, J.H., Köhler, D., Tzioupis, C.C., Pizanis, A., Tosounidis, G.,Burkhardt, M., Pohlemann, T., 2010. Different stabilisation techniques fortypical acetabular fractures in the elderly—A biomechanical assessment. Injury41 (4), 405–410.
Dawson, J.M., Khmelniker, B.V., McAndrew, M.P., 1999. Analysis of the structuralbehavior of the pelvis during lateral impact using the finite element method.Accid. Anal. Prev. 31 (1-2), 109–119.
Du, W., Zhang, J., Hu, J., 2018. Method to determine cortical bone thickness ofhuman femur and tibia using clinical ct scans. Conference ProceedingsInternational Research Council on the Biomechanics of Injury, IRCOBI, 2018-April, 388–398.
Fleps, I., Enns-Bray, W.S., Guy, P., Ferguson, S.J., Cripton, P.A., Helgason, B., 2018. Onthe internal reaction forces, energy absorption, and fracture in the hip duringsimulated sideways fall impact. PLoS ONE, 13(8), 1–18. https://doi.org/10.1371/journal.pone.0200952
Ford, C.M., Keaveny, T.M., Hayes, W.C., 1996. The effect of impact direction on thestructural capacity of the proximal femur during falls. J. Bone Miner. Res. 11 (3),377–383.
13
Grassi, L., Schileo, E., Taddei, F., Zani, L., Juszczyk, M., Cristofolini, L., Viceconti, M.,2012. Accuracy of finite element predictions in sideways load configurations forthe proximal human femur. J. Biomech. 45 (2), 394–399.
Groen, B.E., Weerdesteyn, V., Duysens, J., 2007. Martial arts fall techniques decreasethe impact forces at the hip during sideways falling. J. Biomech. 40 (2), 458–462.
Henak, Corinne R., Kapron, Ashley L., Anderson, Andrew E., Ellis, Benjamin J., Maas,Steve A., Weiss, Jeffrey A., 2014. Specimen-specific predictions of contact stressunder physiological loading in the human hip: validation and sensitivitystudies. Biomech. Model Mechanobiol. 13 (2), 387–400.
Hewitt, John D., Glisson, Richard R., Guilak, Farshid, Vail, T. Parker, 2002. Themechanical properties of the human hip capsule ligaments. J. Arthroplasty 17(1), 82–89.
Hodge, W.A., Fijan, R.S., Carlson, K.L., Burgess, R.G., Harris, W.H., Mann, R.W., 1986.Contact pressures in the human hip joint measured in vivo. Proc. Natl. Acad. Sci.83 (9), 2879–2883.
Holzer, G., von Skrbensky, G., Holzer, L.A., Pichl, W., 2009. Hip fractures and thecontribution of cortical versus trabecular bone to femoral neck strength. J. BoneMiner. Res. 24 (3), 468–474.
Kannus, P., Parkkari, J., Niemi, S., Sievänen, H., 2015. Low-trauma pelvic fractures inelderly Finns in 1970–2013. Calcif. Tissue Int. 97 (6), 577–580.
Keyak, J.H., Skinner, H.B., Fleming, J.A., 2001. Effect of force direction on femoralfracture load for two types of loading conditions. J. Orthop. Res. 19 (4), 539–544.
Korhonen, N., Niemi, S., Parkkari, J., Sievänen, H., Palvanen, M., Kannus, P., 2013.Continuous decline in incidence of hip fracture: nationwide statistics fromFinland between 1970 and 2010. Osteoporos. Int. 24 (5), 1599–1603.
Laird, A., Keating, J.F., 2005. Acetabular fractures: A 16-year prospectiveepidemiological study. J. Bone Joint Surg. Br. Volume 87-B (7), 969–973.
Lemmon, David, Shiang, T.Y., Hashmi, Azfar, Ulbrecht, Jan S., Cavanagh, Peter R.,1997. The effect of insoles in therapeutic footwear—A finite element approach. J.Biomech. 30 (6), 615–620.
Leng, Huijie, Dong, X. Neil, Wang, Xiaodu, 2009. Progressive post-yield behavior ofhuman cortical bone in compression for middle-aged and elderly groups. J.Biomech. 42 (4), 491–497.
Letournel, E., 2019. Acetabulum fractures: classification and management. J. Orthop.Trauma 33, S1–S2.
Li, Zuoping, Alonso, Jorge E., Kim, Jong-Eun, Davidson, James S., Etheridge, BrandonS., Eberhardt, Alan W., 2006. Three-dimensional finite element models of thehuman pubic symphysis with viscohyperelastic soft tissues. Ann. Biomed. Eng.34 (9), 1452–1462.
Li, Z., Kim, J.-E., Davidson, J.S., Etheridge, B.S., Alonso, J.E., Eberhardt, A.W., 2007.Biomechanical response of the pubic symphysis in lateral pelvic impacts: Afinite element study. J. Biomech. 40 (12), 2758–2766.
Luo, Y., Nasiri Sarvi, M., Sun, P., Leslie, W.D., Ouyang, J., 2014. Prediction of impactforce in sideways fall by image-based subject-specific dynamics model. Int.Biomech. 1 (1), 1–14.
Luo, Y., Sarvi, M.N., 2015. A subject-specific inverse-dynamics approach forestimating joint stiffness in sideways fall. IJECB 3 (2), 137. https://doi.org/10.1504/IJECB.2015.070436.
Majumder, S., Roychowdhury, A., Pal, S., 2004. Dynamic response of the pelvis underside impact load – a three-dimensional finite element approach. Int. J.Crashworthiness 9 (1), 89–103.
Majumder, S., Roychowdhury, A., Pal, S., 2007. Simulation of hip fracture insideways fall using a 3D finite element model of pelvis–femur–soft tissuecomplex with simplified representation of whole body. Med. Eng. Phys. 29 (10),1167–1178.
Majumder, S., Roychowdhury, A., Pal, S., 2008. Effects of trochanteric soft tissuethickness and hip impact velocity on hip fracture in sideways fall through 3Dfinite element simulations. J. Biomech. 41 (13), 2834–2842.
Majumder, S., Roychowdhury, A., Pal, S., 2009. Effects of body configuration onpelvic injury in backward fall simulation using 3D finite element models ofpelvis–femur–soft tissue complex. J. Biomech. 42 (10), 1475–1482.
Mechlenburg, I., Nyengaard, J.R., Gelineck, J., Soballe, K., 2007. Cartilage thickness inthe hip joint measured by MRI and stereology – a methodological study.Osteoarthritis and Cartilage 15 (4), 366–371.
Mills, N.J., 2006. Finite element models for the viscoelasticity of open-cellpolyurethane foam. Cell. Polym. 25 (5), 293–316.
Nankaku, M., Kanzaki, H., Tsuboyama, T., Nakamura, T., 2005. Evaluation of hipfracture risk in relation to fall direction. Osteoporos. Int. 16 (11), 1315–1320.
Nasiri Sarvi, M., Luo, Y., 2017. Sideways fall-induced impact force and its effect onhip fracture risk: a review. Osteoporos. Int. 28 (10), 2759–2780.
O’Brien, Fergal J., Brennan, Orlaith, Kennedy, Oran D., Lee, T. Clive, 2005.Microcracks in cortical bone: How do they affect bone biology?. Curr.Osteoporos. Rep. 3 (2), 39–45.
O’Donnell, J.M., Devitt, B.M., Arora, M., 2018. The role of the ligamentum teres in theadult hip: redundant or relevant? A review. J. Hip Preservation Surg., 5(1), 15–22. https://doi.org/10.1093/jhps/hnx046
Papanicolaou, G.C., Zaoutsos, S.P., 2019. Viscoelastic constitutive modeling of creepand stress relaxation in polymers and polymer matrix composites. Creep andFatigue in Polymer Matrix Composites, 3–59. https://doi.org/10.1016/B978-0-08-102601-4.00001-1
Parashar, S.K., Sharma, J.K., 2016. A review on application of finite elementmodelling in bone biomechanics. Perspect. Sci. 8, 696–698.
Ramos, A., Simões, J.A., 2006. Tetrahedral versus hexahedral finite elements innumerical modelling of the proximal femur. Med. Eng. Phys. 28 (9), 916–924.

S. Khakpour, P. Tanska, S. Saarakkala et al. Journal of Biomechanics 114 (2021) 110156
Sarvi, M.N., Luo, Y., Sun, P., Ouyang, J., 2014. Experimental validation of subject-specific dynamics model for predicting impact force in sideways fall. JBiSE 07(07), 405–418.
Sebastian Giudice, J., Poulard, D., Nie, B., Wu, T., Panzer, M.B., 2018. A corticalthickness mapping method for the coxal bone using morphing. Front. Bioeng.Biotechnol. 6 (OCT), 1–9. https://doi.org/10.3389/fbioe.2018.00149.
Shim, V., Böhme, J., Vaitl, P., Klima, S., Josten, C., Anderson, I., 2010. Finite elementanalysis of acetabular fractures—development and validation with a syntheticpelvis. J. Biomech. 43 (8), 1635–1639.
Silvestri, C., 2008. Development and validation of a knee-thigh-hip LSDYNA modelof a 50 th percentile male.
van den Kroonenberg, A.J., Hayes, W.C., McMahon, T.A., 1996. Hip impact velocitiesand body configurations for voluntary falls from standing height. J. Biomech. 29(6), 807–811.
van der Zijden, A.M., Groen, B.E., Tanck, E., Nienhuis, B., Verdonschot, N.,Weerdesteyn, V., 2012. Can martial arts techniques reduce fall severity? Anin vivo study of femoral loading configurations in sideways falls. J. Biomech. 45(9), 1650–1655.
van der Zijden, A.M., Groen, B.E., Tanck, E., Nienhuis, B., Verdonschot, N.,Weerdesteyn, V., 2017. Estimating severity of sideways fall using a genericmulti linear regression model based on kinematic input variables. J. Biomech.54, 19–25.
Varga, P., Schwiedrzik, J., Zysset, P.K., Fliri-Hofmann, L., Widmer, D., Gueorguiev, B.,Blauth, M., Windolf, M., 2016. Nonlinear quasi-static finite element simulationspredict in vitro strength of human proximal femora assessed in a dynamicsideways fall setup. J. Mech. Behav. Biomed. Mater. 57, 116–127.
14
Vivanco, Juan F., Burgers, Travis A., García-Rodríguez, Sylvana, Crookshank, Meghan,Kunz, Manuela, MacIntyre, Norma J., Harrison, Mark M., Bryant, J. Tim, Sellens,Rick W., Ploeg, Heidi-Lynn, 2014. Estimating the density of femoral headtrabecular bone from hip fracture patients using computed tomography scandata. Proc. Inst. Mech. Eng. H 228 (6), 616–626.
Vleeming, A., Schuenke, M.D., Masi, A.T., Carreiro, J.E., Danneels, L., Willard, F.H.,2012. The sacroiliac joint: an overview of its anatomy, function and potentialclinical implications. J. Anat. 221 (6), 537–567.
Wang, G., Huang, W., Song, Q.i., Liang, J., 2017. Three-dimensional finite analysis ofacetabular contact pressure and contact area during normal walking. Asian J.Surg. 40 (6), 463–469.
Watson, P.J., Dostanpor, A., Fagan, M.J., Dobson, C.A., 2017. The effect of boundaryconstraints on finite element modelling of the human pelvis. Med. Eng. Phys. 43,48–57.
Westerling, L., 2002. A note on an erosion criterion in AUTODYN, (June).Wolfram, U., Schwiedrzik, J., 2016. Post-yield and failure properties of cortical bone.
BoneKEy Reports 5 (July), 1–10. https://doi.org/10.1038/bonekey.2016.60.Xiao, Y., Hu, Y., 2019. An extended iterative identification method for the GISSMO
model. Metals, 9(5). https://doi.org/10.3390/met9050568Zhang, Ning, Magland, Jeremy F., Rajapakse, Chamith S., Lam, ShingChun Benny,
Wehrli, Felix W., 2013. Assessment of trabecular bone yield and post-yieldbehavior from high-resolution mri-based nonlinear finite element analysis atthe distal radius of premenopausal and postmenopausal women susceptible toosteoporosis. Acad. Radiol. 20 (12), 1584–1591.
Zheng, N., Watson, L.G., Yong-Hing, K., 1997. Biomechanical modelling of thehuman sacroiliac joint. Med. Biol. Eng. Comput., 35(2), 77–82. https://doi.org/10.1007/BF02534134