The diagnosis and management of primary hypothyroidism · Boelaert et al. (2010) Am J Med 123,...
37
Underactive thyroid The diagnosis and management of primary hypothyroidism Kristien Boelaert Senior Clinical Lecturer and Consultant Endocrinologist University of Birmingham, UK [email protected]
Transcript of The diagnosis and management of primary hypothyroidism · Boelaert et al. (2010) Am J Med 123,...
-
Underactive thyroid The diagnosis and management of primary
hypothyroidism Kristien Boelaert
Senior Clinical Lecturer and Consultant Endocrinologist University of Birmingham, UK
http://images.google.co.uk/imgres?imgurl=http://postgrad.eee.bham.ac.uk/Schwirtza/index_files/unilogo4.jpg&imgrefurl=http://postgrad.eee.bham.ac.uk/Schwirtza/&usg=__nEI6zj8JA3YOwrQTHaz4ldDW9ec=&h=512&w=578&sz=46&hl=en&start=7&itbs=1&tbnid=KzmY3fxadUY7-M:&tbnh=119&tbnw=134&prev=/images?q=university+of+birmingham+uk&gbv=2&hl=en
-
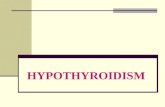
Thyroid gland
Located in neck
Brownish-red
25-30 g
Right and left lobe
Joined by isthmus
-
Thyroid gland
-
Thyroid hormones
Control of metabolism:
energy generation and use
Regulation of growth
Important in development
-
Thyroid hormones
T3 is biologically active hormone
T4 produced in highest quantity
Deiodinase enzymes convert T4 to T3 in tissues
-
Thyroid binding proteins
T4 T3
TBG
TBPA Albumin
Free T4: 0.03%
Deiodination
TBG
TBPA Albumin
Free T3: 0.3%
Thyroid hormones are bound to proteins
-
Control of thyroid hormone synthesis
Hypothalamus
Pituitary
TRH
TSH
-ve +ve
+ve
Thyroid
Target Tissue
T4 T3
-ve
-ve
T3
-
Serum TSH
Serum free T4
Serum free T3
Tests of thyroid function
Serum TSH
Serum free T4
Serum free T3
Serum TSH
Serum free T4
Serum free T3
Hyperthyroidism Hypothyroidism
Overactive Underactive
-
Hypothyroidism
-
Hypothyroidism
Occurs in 3.8-4.6% of population
Most common endocrine disease
10 times more common in women
Incidence rising
2010: 23 million prescriptions for levothyroxine in UK – 3rd most prescribed medication
-
Causes of hypothyroidism
Autoimmune – Hashimoto’s thyroiditis: genetic predisposition and antibodies (anti-TPO and anti-Tg)
Iodine deficiency
Following treatment for hyperthyroidism
Subacute/silent thyroiditis: inflammation of thyroid gland
Congenital (incomplete thyroid gland development/enzyme defects)
Drugs: amiodarone, lithium
-
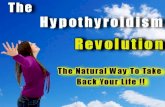
Hashimoto’s thyroiditis
-
Hashimoto’s thyroiditis
Normal thyroid gland
Inflammation and
goitre/swelling
Fibrosis and shrinkage
-
Iodine deficiency
Major cause of goitre and hypothyroidism world-wide
WHO identified in 7% of world’s population
Range from near 0% (Japan) to 80% (Andes, Zaire)
-
UK iodine deficiency Common in many areas
up to 1960’s
Main source of iodine is from milk and dairy products
Evidence for iodine deficiency in vegans
Daily iodine increased from 80 to 255g/day
-
UK Iodine status
Vanderpump et al. (2011) Lancet 377, 2007
-
Treatment options for hyperthyroidism
• Antithyroid drugs to block hormone synthesis
• Radioiodine (131I) therapy
• Surgical removal of thyroid
-
Outcome following 131I therapy
1278 patients treated with 131I for hyperthyroidism
Single fixed dose of 131I
Boelaert et al. (2009) Clin End 70, 129
-
Symptoms and signs of hypothyroidism
Cardiovascular
Slow heart rate
Heart failure
Gastrointestinal
Weight gain
Constipation
Skin
Myxoedema (puffiness of skin)
Hair loss
Dry skin
Neurological
Tiredness
Depression
Psychosis
-
Clinical features of hypothyroidism
-
Vitiligo
-
Diagnosis: symptoms
Sensitivity of individual symptoms: 2.9-24.5%
Likelihood increases with more symptoms
Absence of symptoms does not exclude diagnosis
Many symptoms are non-specific
-
Colorado Thyroid Prevalence Study
Canaris et al. (2000), Arch Int Med 160: 526
-
Biochemical diagnosis
Serum TSH
Serum free T4
Serum free T3
Normal TSH reference range: 0.4-4.5 mU/l
Use trimester-specific reference ranges in pregnancy
TSH distribution influenced by age
-
Upper serum TSH concentrations
Surks and Hollowell (2007) JCEM 92: 4575
Physiological changes to thyroid function with age
-
Biochemical diagnosis
Measure serum TFT not other bodily fluids
No evidence to support measurement of basal body temperature
Other illnesses may affect test results
Different methods may give different results
Support for harmonisation of reference ranges
RCP updated statement 2011
-
Treatment of hypothyroidism
Levothyroxine (T4) replacement
7 day half-life
Initiation at full dose safe except in elderly or patients with known heart disease (1.6μg/kg/day)
Take on empty stomach 30 mins before breakfast
-
Bedtime dosage of levothyroxine
Better biochemical control
No improvements in quality of life, blood pressure, lipid profiles
Bolk et al (2010) Arch Int Med 170: 1996
-
Monitoring of thyroid function
Stabilisation of TFT may take up to 4 months
Measure serum TSH 6-8 weeks after initiation/dose change
Annual TFT if on stable dose
Aim of treatment is to restore patient to euthyroid state
Symptoms usually recover
Fine-tuning may be required in individual patients
-
Causes of persistently raised serum TSH
Chakera et al (2011) Drug des, dev and therapy 6: 1
-
Drug interactions with L-T4
Chakera et al (2011) Drug des, dev and therapy 6: 1
-
Continued symptoms and biochemical euthyroidism
Investigate further for other causes
Think of associated autoimmune disorders
Hypothyroidism and dysphoria are common
-
Associated autoimmune disorders
Boelaert et al. (2010) Am J Med 123, 183.e1
-
Efficacy of T4 replacement
Audit of 18,944 prescribing records in general practice
Prevalence of T4 therapy 0.8% (3.6% > 60y)
Abnormal TFT in those prescribed T4
Low TSH in 20.6% (undetectable in 7%)
High TSH in 26.8%
T4 dose (g) High TSH Low TSH
150 25% 25%
Parle et al 1993 Br J Gen Pract, 43, 107
-
T3/T4 combination
Initial study from Lithuania: improvement in well-being
Meta-analysis of 11 RCT: no effect on bodily pain, depression, anxiety, quality of life, weight, lipid profile
Current T3 formulation does not result in normal physiological profile
Not recommended by national and international guidelines
? Genetic predisposition to benefiting from combination Rx
-
T3/T4 combination
Grozinsky-Glasberg JCEM 2006, 91, 2592
-
Desiccated pig thyroid extract
Contains T4:T3 in 4:1 ratio – physiological ratio 14:1
Higher than physiological doses of T3
No good evidence to support T3 mono therapy
Dangers of too much T3: heart, osteoporosis