The CQUIN Learning Network 3 Annual Meeting Fostering...
22
Poster Abstract Book – 3 rd CQUIN Annual Meeting, Johannesburg, South Africa | November 10-14, 2019 1 The CQUIN Learning Network 3 rd Annual Meeting: Fostering Scale-Up of Differentiated HIV Service Delivery to Achieve Sustainable Epidemic Control Poster Abstracts
Transcript of The CQUIN Learning Network 3 Annual Meeting Fostering...

Poster Abstract Book – 3rd CQUIN Annual Meeting, Johannesburg, South Africa | November 10-14, 2019
1
The CQUIN Learning Network 3rd Annual Meeting:
Fostering Scale-Up of Differentiated HIV Service Delivery to
Achieve Sustainable Epidemic Control
Poster
Abstracts

Poster Abstract Book – 3rd CQUIN Annual Meeting, Johannesburg, South Africa | November 10-14, 2019
2
CQUIN Annual Meeting Posters CQUIN network participants responded with enthusiasm to the CQUIN Annual Meeting call for
posters. In order to accommodate all 38 posters, they will be presented in three tracks, which
correspond to the days on which posters will be presented.
Track A posters will be displayed from November 11 – 14
Track B posters will be displayed on November 11 – 12
Track C posters will be displayed on November 13 – 14
Electronic versions of posters will be available on the CQUIN Annual Meeting website, at
www.cquin.icap.columbia.edu
Track A: November 11-14
1. Taking DSD to Scale in Zimbabwe: Championing Data for Decision-Making Clorata Gwanzura, Takura Matare, Tsitsi Apollo
Ministry of Health and Child Care
Corresponding author: Clorata Gwanzura, [email protected]
2. Taking DSD to Scale in Zambia: Innovating, Adapting and Scaling Up DSD Priscilla Lumano-Mulenga1, Mpande Mukumbwa Mwenechanya2, Muhau Mubiana2, Felton Mpasela3, Maureen Simwenda4, Linah Mwango5, Ernest Mwila16, Tamara Choola6, Zumbe Siwale7, Mercy Nalwamba8, Nantembwa Chellah15, Linkson Zulu9, Nancy Zyongwe10, Owen Mulenga11, Chimuka Sianyinda 1 ,Fred Chungu12, Keith Mweebo13, Musonda Musonda14, Joseph Kayaya17, Christopher Mbinji17, Alex Makupe
1. Zambian Ministry of Health (MoH), 2. CIDRZ, 3. Clinton Health Access Initiative, 4. JSI USAID SAFE, 5. University of Maryland, 6. Howard University, 7. EQUIP, 8. FHI360, 9. CHAZ, 10. ICAP, 11. TALC, 12. NZP+, 13. CDC, 14. USAID, 15. AIDS Health Care Foundation, 16. JSI USAID Discover Health, 17. Broadreach
Corresponding author: Priscilla Lumano-Mulenga, [email protected]
3. Taking DSD to Scale in Uganda: A Maturing National Program Josen Kiggundu, Cordelia Katureebe, Hudson Balidawa, Ivan Lukabwe
Ministry of Health AIDS Control Program
Corresponding author: Josen Kiggundu, [email protected]
Poster Abstract Book – 3rd CQUIN Annual Meeting, Johannesburg, South Africa | November 10-14, 2019
3
4. Taking DSD to Scale in Tanzania: Diversifying DSD Models Leads to Increased Coverage Mastidia Rutaihwa1, Anath Rwebembera1, Veryhe Sambu1, Syliverster Kwilasa1, Boniface Silvan1, James Kamuga1, Stella Chale2 Angela Ramadhani1
1. National AIDS Control Program, Tanzania Ministry of Health 2. I -TECH Tanzania
Corresponding authors: Mastidia Rutaihwa, [email protected] & Angela Ramadhani [email protected]
5. Taking DSD to Scale in South Africa Lillian Diseko, Romy Overmeyer, Tshepo Molapo, Magogodi Mkhize, Mokgadi Phokojoe, Zukiswa Pinini National Department of Health Corresponding author: Lillian Diseko, [email protected]
6. Taking DSD to Scale in Mozambique: Putting Quality at the Center Irénio Gaspar¹, Hélder Macul,¹ Aleny Couto,¹ Orlando Munguambe¹, Dario Ali2
1. Ministry of Health, Mozambique, 2. ICAP Mozambique
Corresponding author: Irénio Gaspar, [email protected]
7. Taking DSD to Scale in Malawi: Accelerating 6-month Multi-Month Dispensing (6-MMD) Rose Nyirenda, Stanley Ngoma, Andreas Jahn, Ackim sankhani, Paul Nyasulu, Tiwonge Chimpandule
Department of HIV/AIDS, Ministry of Health
Corresponding author: Stanley Ngoma, [email protected]
8. Taking Differentiated Service Delivery to Scale in Kenya: Moving to Scale Maureen Kimani, Rose Ayugi, Muthoni Karanja, Faith Ngare, Maureen Inimah, Mburu Muiyuro, Nicholas Sewe, Franklyn Songok, Mohamud Mohamed NASCOP, MoH, Kenya Corresponding author: Maureen Inimah, [email protected]
9. Taking Differentiated Service Delivery to Scale in Ethiopia: A Focus on 6-month Multi-Month Dispensing (6-MMD) Alemtsehay Abebe1, Mirtie Getachew1, Tamrat Assefa2, Zenebe Melaku2, Frehiwot Nigatu3 1.Ministry of Health-Ethiopia, 2. ICAP Ethiopia, 3. Project Hope Corresponding author: Alemtsehay Ababe, [email protected]

Poster Abstract Book – 3rd CQUIN Annual Meeting, Johannesburg, South Africa | November 10-14, 2019
4
10. Taking Differentiated Service Delivery to Scale in Eswatini: Focusing on Quality and Coverage Hervé Nzereka Kambale1, Simangele Mthethwa1, Thabo Motsa2, Nobuhle Mthethwa1, Thembie Dlamini1, Sindi Matse1, Gugulethu Madonsela1 Nompilo Gwebu1, Nondumiso Ncube1, Harrison Njoroge Kamiru6, Nxumalo Nkosinathi6, Arleta Ndlela6, Bridget Mugisa4, Victoria Masuku4, Hugben Byarugaba4, Lydia Mpango3, Christopher Makwindi3, Edwin Mabena5, Patrick Nyema5, Laura Muzart7, and Philisiwe Dlamini7.
Eswatini National AIDS Programme (SNAP) 1, Ministry of Health Monitoring and Evaluation Unit2, AIDS Free3, University Research Co. LLC (URC) 4, Médecins Sans Frontières (MSF) 5, ICAP at Columbia University6, FHI 3607
Corresponding author: Hervé Nzareka Kambale, [email protected]
11. Taking DSD to Scale in Cote d’Ivoire: Building National Leadership to Catalyze DSD Scale-up Franck Boraud1, Simplice Bohoussou2, Maturin Kouadjale2, Alain Somian3, Thibaut Brou4, Jean Jacques M'Bea Kouaasi1, Aoua Camara epse Aka5, Patrice Ladji2, Greet Vanderbriel1, Stephania Koblavi1 1. ICAP at Columbia University, 2. Programme National de la Lutte Contre le Sida (PNLS), 3. RIP+, 4. SEVCI, 5. DIIS
Corresponding author: Franck Boraud, [email protected]
12. Accelerating DSD with CQUIN South-to-South Learning Exchange Visits Peter Preko, Siphiwe Shongwe, Miriam Rabkin, ICAP/CQUIN Corresponding author: Peter Preko, [email protected]
The CQUIN network continues to encourage and support peer-to-peer demonstration of successful differentiated service delivery (DSD) implementation strategies. CQUIN’s south-to-south (S2S) learning visits are an effective forum to collaborate, review progress, and empower participants to advocate for implementation and adaptation of new approaches in their home settings. This poster summarizes the CQUIIN south-to-south visits to date, including outcomes and impact on visiting country policies and practice.
13. CQUIN Communities of Practice: Co-Creation and Knowledge Exchange Peter Preko, Bill Reidy, Andrea Schaaf, Siphiwe Shongwe, Martin Msukwa, Cassia Wells, Bactrin Killingo, Laura Block, Joanne Mantell, Miriam Rabkin Corresponding author: Peter Preko, [email protected]
CQUIN’s Communities of Practice (CoPs) are a growing element of the learning network, convening country teams to work on shared challenges and opportunities. Countries can opt into the CoP most relevant to their context, participating remotely via teleconference and email and in person at CQUIN workshops. Most CoPs focus on co-creating resources and tools and many are time limited. New CoPs are formed ‘on demand’ when CQUIN member countries identify a new area for collaboration. This poster summarizes the activities of CQUIN’s 7 CoPs and key lessons learned.
Poster Abstract Book – 3rd CQUIN Annual Meeting, Johannesburg, South Africa | November 10-14, 2019
5
Track B: Monday, November 11 - Tuesday, November 12
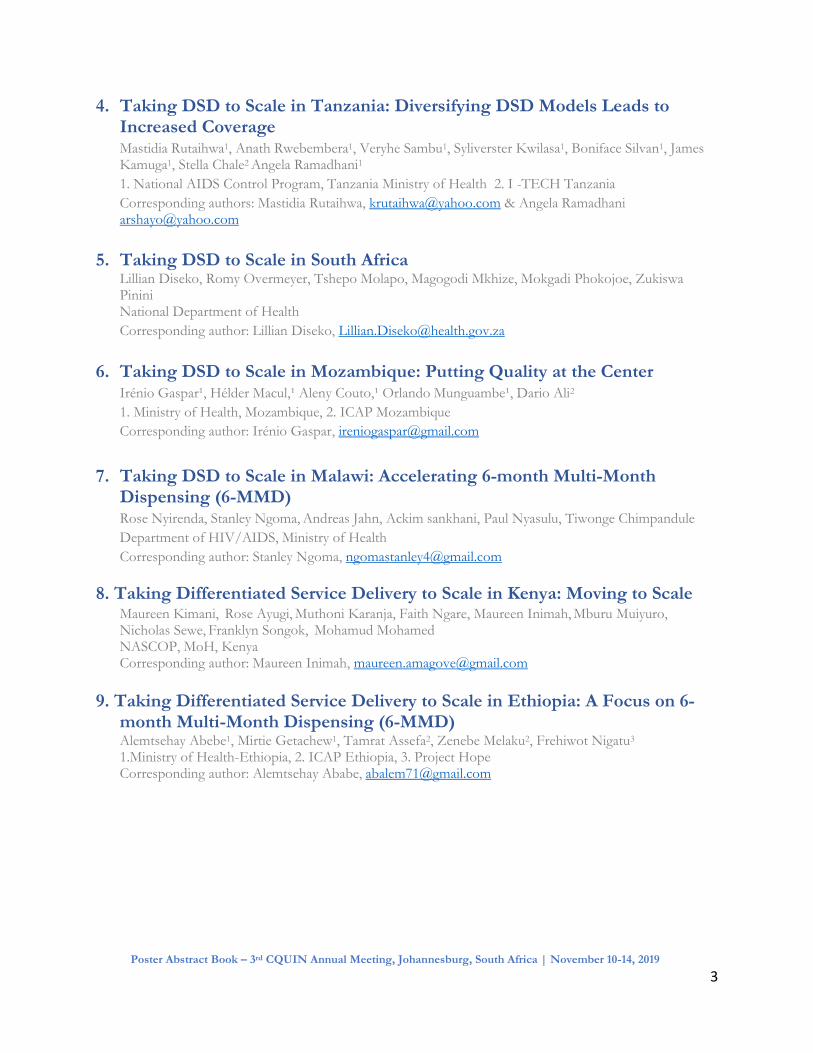
14. Patient and provider costs associated with differentiated models of service delivery for HIV treatment in sub-Saharan Africa Salome Kuchukhidze1, Brooke Nichols1,2, Lawrence Long1,2, Sophie Pascoe2, Amy Huber2, Matt Fox1,2, Sydney Rosen1,2 1 Department of Global Health, Boston University School of Public Health, Boston, MA, USA 2 Health Economics and Epidemiology Research Office (HE2RO), Johannesburg, South Africa Corresponding author: Sydney Rosen, [email protected]
As part of a larger rapid review of the published and gray literature on the observed outcomes of differentiated service delivery (DSD) models for HIV treatment since 2016, we synthesized sources that reported empirical information on patient and/or provider costs of DSD models. We searched PubMed, Embase, and Web of Science for articles published since 2016 and used Google’s advanced search to identify unpublished abstracts, posters, presentations, and reports from websites of DSD implementing partners and ministries of health. Thirteen out of 85 published and unpublished sources reporting on DSD implementation provided patient and/or provider cost estimates. DSD models consistently reduced travel and time costs for patients. The table below summarizes provider cost findings.
Country Model Outcome metric DSD cost or burden (USD)
SOC cost or burden (USD)
% difference
Empirical costing (patient-level data) Kenya
Streamlined care model Total ART treatment cost/patient/yr
(2016 USD) $285.52
Uganda $309.08
Resource utilization quantification Nigeria Multi-month scripting Decreased facility patient burden/day
due to DSD
32%
DRC ART support group, community-based point of ART distribution (PODI+), fast-track ART refill circuit
Number of patients/provider 202 patients
409 patients 51%
Guidelines-based costing Malawi Multi-month scripting Total ART treatment cost/patient/yr
(2016 USD) $121.41 $135.33 10%
Fast-track refills $120.73 $135.33 11%
Community ART groups $122.30 $135.33 10%
Malawi Teen club Incremental program costs/patient/yr (excludes ARVs, labs, clinic visits)
$30
South Africa
Youth care clubs Incremental DSD visit costs/patient/yr (excludes ARVs, labs, clinic visits)
$48
Tanzania Community and facility HIV support services cost/patient/yr (excludes ARVs, labs, clinic visits)
$45 $108 58%
Community $20 $108 81%

Poster Abstract Book – 3rd CQUIN Annual Meeting, Johannesburg, South Africa | November 10-14, 2019
6
15. The Cost of Differentiated HIV Antiretroviral Therapy Delivery Strategies n Sub-Saharan Africa: A Systematic Review D Allen Roberts MPH1, Nicholas Tan BS2, Nishaant Limaye BA2, Elizabeth Irungu MBChB MPH2, Ruanne V. Barnabas MBChB DPhil1,2,3* 1Department of Epidemiology, University of Washington, Seattle, Washington, USA 2Department of Global Health, University of Washington, Seattle, Washington, USA 3Department of Medicine, University of Washington, Seattle, Washington, USA Corresponding author: Allen Roberts, [email protected]
Introduction: Scalable models for HIV treatment are needed to maximize health outcomes with available resources. Differentiated antiretroviral therapy (DART) models may improve service delivery efficiency. We conducted a systematic review of studies assessing the cost of DART in sub-Saharan Africa.
Methods: We searched bibliographic databases and the grey literature for studies published between 2005 and 2019 that assessed the cost of DART. We extracted the annual per-patient service delivery cost and incremental cost of DART compared to standard of care in 2018 USD.
Results: We identified 12 articles that reported costs for 16 DART models in seven countries. Most models were facility-based (n=12) and located in Uganda (n=7). The annual cost per patient within DART models (excluding drugs) ranged from $27 to $889 (2018 USD). Of the 11 models reporting incremental costs, seven found DART to be cost saving. The median incremental savings per patient per year among cost-savings models was $67. Personnel was the most common driver of reduced costs, but savings were sometimes offset by higher overheads or utilization.
Conclusions: DART models can save personnel costs by task shifting and reducing visit frequency. To decrease costs, programs will need to match DART models to client needs without incurring substantial overheads.

Poster Abstract Book – 3rd CQUIN Annual Meeting, Johannesburg, South Africa | November 10-14, 2019
7
16. Optimizing treatment models for people living with HIV in urban
Zimbabwe: Findings from a mixed methods study
Michael Strauss1, Gavin George1, Munyaradzi Mapingure2, Joanne E. Mantell3, Tsitsi B. Masvawure4, Matthew R. Lamb5, Godfrey Musuka2, Jennifer M. Zech5, Innocent Chingombe2, Martin Msukwa6, Rodrigo Boccanera7, ClorataGwanzura8; TsitsiApollo8, Miriam Rabkin5 Health Economics and HIV and AIDS Research Division (HEARD), University of KwaZulu-Natal1, ICAP Zimbabwe2, New York State Psychiatric Institute and Columbia University, Division of Gender, Sexuality and Health3, Center for Interdisciplinary Studies, College of the Holy Cross4, ICAP at Columbia University, Mailman School of Public Health5, ICAP South Africa6, Health Resources and Services Administration (HRSA) 7, Ministry of Health and Child Care, Zimbabwe8 Corresponding author: Michael Strauss, [email protected]
Zimbabwe is scaling up differentiated HIV service delivery to improve patient and healthcare worker (HCW) satisfaction, HIV treatment outcomes, and program efficiencies. We designed a mixed-methods study to explore the treatment preferences of urban people living with HIV (PLHIV) in 7 health facilities in Harare [35 key informant interviews (KII) with HCWs; 8 focus group discussions (FGD) with 54 PLHIV; a discrete choice experiment (DCE) in which 500 adult DART-eligible PLHIV selected their treatment preferences; and a survey with the 500 DCE participants exploring DART knowledge and preferences].
Participants strongly preferred HF-based services, individual DART models, respectful and understanding HCWs, and services costing < $3/visit. Patients also preferred less frequent visits and shorter wait times. They were indifferent to variations in HCW cadre and distances from home to HF. These preferences were mostly homogenous, with only minor differences between male vs. female and older vs. younger patients. In KII, HCWs characterized the fast track/visit spacing model (a facility-based individual model) as the one most favoured by patients; HCW also preferred this model, which they felt decompressed HF and decreased HCW workload. Prioritizing these models for scale-up in urban areas may be the most efficient way to sustain positive patient outcomes and increase health system performance.

Poster Abstract Book – 3rd CQUIN Annual Meeting, Johannesburg, South Africa | November 10-14, 2019
8
17. Applying Client Centered Design Processes to Optimize DSD Edward Bitarakwate1, Eliab Natumanya1, Julius Mugaya1, Lawrence Mugumya1, Assumpta Bibaze1, Jacqueline Muyama1, Dan Mugisha1, Caroline Tiri1, Ivan Teri1. Elizabeth Glaser Pediatric AIDS Foundation1 Corresponding author: Edward Bitarakwate, [email protected]
Despite initial gains following adoption of DSD, retention on ART progressively decreased to 94% with a related net reduction in clients on ART across sites in in the EGPAF-led USAID RHITES-SW project in Uganda. Root cause analysis (RCA) was implemented to understand and address barriers among clients who missed ARV drug pick up appointments. Input was sought from the PLHIV to design site specific actions to address identified issues. There was a concomitant increase in net of new ART clients as enrollment on DSD increased each quarter. The benefits of DSD can be optimized through appropriate iteration in programming.

Poster Abstract Book – 3rd CQUIN Annual Meeting, Johannesburg, South Africa | November 10-14, 2019
9
18. The landscape of differentiated service delivery models in Malawi, South Africa, and Zambia: insights from AMBIT stakeholder interviews Amy Huber1, Sophie Pascoe1, Lawrence Long1,2, Brooke Nichols1,2, Salome Kuchukhidze2, Idah Mokhele1, Nkgomeleng Lekodeba1, Sydney Rosen1,2 1 Health Economics and Epidemiology Research Office (HE2RO), Johannesburg, South Africa 2 Department of Global Health, Boston University School of Public Health, Boston, MA, USA Corresponding author: Sophie Pascoe, [email protected].
Most countries lack current, comprehensive data on the scale and status of differentiated service delivery (DSD) models for ART. In 2019, AMBIT interviewed the main nongovernmental organizations supporting the implementation of DSD models in Malawi, South Africa, and Zambia about the design, characteristics, and scale of currently implemented models. We interviewed 28 implementing partners supporting a total of 87 DSD models. Most common
(42%) were models delivering services to individual patients outside of facilities (mainly medication pickup points in communities). Also common were facility-based individual models
(e.g. fast-track services and specialized clinics for different kinds of patients) (26%) and
various forms of adherence clubs (24%). The few client-led groups were largely CAGs. Dispensing duration is summarized below.
Average months of ARVs dispensed in model* Number of
models reported**
Malawi South Africa
Zambia
1 month 10 5 3 2 2 months 32 1 31 0 3 months 11 4 2 5 1 or 3 months (patients typically start with 1 month, then move to
3 months) 2 1 0 1
6 months 9 3 1 5 3 or 6 months (typically previously dispensed 3 months but
transitioning to 6 months in line with national policy) 14 2 1 11
Not reported 9 6 2 1
Total reported in interviews 87 22 40 25 *Includes DSD models for both suppressed and unsuppressed patients, all ages and risk groups, excluding PMTCT programs. **Specific models of care are present more than once in this table, as each instance of an implementing partner supporting a given model is counted separately. For example, multiple partners in South Africa support CCMDD; each is counted as a separate model in this table.
19. Early warning system to reduce ARV ruptures and other laboratory inputs in ARV treatment centers in Côte d'Ivoire: Experience of the Ivorian Network of Organizations of People Living with HIV (RIP +) in 2015 and 2016
Management Sciences for Health, USAID/ Supply Chain Management System (SCMS), Alain SOMIAN, Directeur Exécutif du RIP+ Corresponding author: Alain Somian, [email protected]

Poster Abstract Book – 3rd CQUIN Annual Meeting, Johannesburg, South Africa | November 10-14, 2019
10
20. Experience of the DRC HIV/TB Observatory of the UCOP+ : A Mixed Methods Study from First Quarter of 2019 Ange Mavula Ndeke, Maurice Felo, Richard Chuy Ingwe, Comité de Pilotage l’UCOP+, Membres des Organisations de la Société Civile de lutte contre le VIH/TB) qui valident le rapport. Corresponding author: Ange Mavula, [email protected]
The Observatory is an arrangement for monitoring civil society organizations engaged in the fight against AIDS and TB, to provide evidence for advocacy to improve access to care.
Information is gathered from users of services and health care providers (primary information sources), with the help of an electronic questionnaire (via the mobile application “KoBoCollect”) by a network of trained survey staff. The latter have come from Congolese civil society organizations fighting HIV and TB.
For the qualitative survey, the data gathered by survey staff are stored in a (virtual and physical) server, which is managed by UCOP+. The processing and analysis of the data are done in Excel.
These questionnaires focus on :
• Geographic accessibility (the time it takes a user to get to the place where care is administered).
• Availability of HIV & TB services (Screening, Care, Viral load, etc.)
• Financial accessibility (fees paid for access to services)
• Stigmatization & discrimination (violation of rights)
• Availability of strategic inputs (ARV, INH, Screening tests, anti-TB, cotrimoxazole, fluconazole, ceftriaxone)
• Participation of civil society organizations at Steering Committee meetings
MONTHLY DATA COLLECTION
DATA PROCESSING (SPSS, EPI INFO &
EXCEL)
DISSEMINATION & RESPONSE
FEEDBACK
COLLECTE MENSUELLE DES
DONNEES
TEMENT DES DONNEES (SPSS,
EPI INFO & EXCEL)
DIFFUSION & FEEDBACK
RETROACTION
Poster Abstract Book – 3rd CQUIN Annual Meeting, Johannesburg, South Africa | November 10-14, 2019
11
21. Differentiated ART delivery in West and Central Africa: policy, practice and plans for scale up Anna Grimsrud, Lynne Wilkinson, Lina Golob International AIDS Society Corresponding author: Anna Grimsrud, [email protected]
Major progress has been made globally to move towards the UNAIDS 90-90-90 targets by 2020, but countries in West and Central Africa (WCA) are lagging. In 2016, UNAIDS launched a WCA catch-up plan to set the 25 countries in the region on the fast track to achieving the 90-90-90 targets by 2020.
The poster content is based on programme experiences and best practices from West and Central African countries shared during a consultation on differentiated ART delivery in WCA in Accra, Ghana, on 17 May 2019, convened by the International AIDS Society. The consultation brought together more than 40 representatives from ministries of health, implementing partners, community organizations and global normative agencies.
The poster will:
• Share five priority actions needed to facilitate implementation and scale up of differentiated ART delivery models in WCA for clinically stable clients on ART,
• Promote examples from the region, both related to policy and implementation,
• Assess the level of differentiated ART delivery implementation in specific countries in the region.
22. Peri-Natal Adherence Clubs in Maputo, Mozambique Irénio Gaspar¹, Aleny Couto1, Assmita Mutisse1, Ana Gabriela Gutierrez2, Natalia Tamayo Antabak2, Anne Loarec 2 ¹Ministry of Health, Maputo, Mozambique; 2Médecins Sans Frontières, Maputo, Mozambique Corresponding author: Irénio Gaspar, [email protected]
Vertical transmission of HIV in Mozambique remains very high, at an estimated 15% and the HIV PCR positivity rate for exposed babies < 8 weeks is 8% and > 8 weeks, 19%.
Mozambique launched Option B+ in 2013, offering all HIV-positive pregnant women ART for life regardless of CD4 count. In addition, HIV testing coverage during pregnancy is 98%; and 97% of women testing positive are initiated on ART. Despite this high coverage, it is clear that PMTCT is still a major challenge during pregnancy and breastfeeding. This poster will present
outcomes from a pregnant and breastfeeding cohort included in a Differentiated Model of Care, Adherence Clubs, at a Ministry of Health – Médecins Sans Frontières supported primary health care facility in Maputo, Mozambique.

Poster Abstract Book – 3rd CQUIN Annual Meeting, Johannesburg, South Africa | November 10-14, 2019
12
23. Uptake of ART Health Post Dispensation model in Lusaka district ART facilities. A Differentiated Service Delivery H. Bwalya Mulenga1, M. Muhau1, M. Mukumbwa-Mwenechanya1, C. Lyembele1 , I.Sikazwe1, T. Savory1, M. Wa Mwanza1, D. Mwamba1,V. Kamanga1, C. Bolton1,2, M. Herce1,3
1Center for Infectious Disease Research in Zambia, Lusaka, Zambia. 2University of Alabama at Birmingham, Birmingham, United States, 3University of North Carolina at Chapel Hill, Chapel Hill, United States Corresponding author: Helen Bwalya Mulenga, [email protected]
The Health Post model is a DSD model in which stable clients pick up refills at local Health Posts within their communities; aimed at addressing distance and transport challenges faced by the stable clients in accessing ART services. In this poster, we demonstrate the uptake of the model in 18 facilities.
Methods: Main facility pharmacy personnel dispensed medicines for three months and advised patients to collect the next three months refill from the assigned health post within their community. We analyzed uptake of the services between October 2017 and April 2019.
Results: 8% of 75,271 clients in all DSD models were enrolled on the HP model where 65% were female. Enrollments by age were 18% in the >50 years ,45-50 years 21%, 40-44 years 22%, 35-39 years 19%, 30-34 years 12%, 25-29 years 6%, 20-24years 2% and < 20 years 0.3%. Enrollments were highest among the 40-44 age group and lowest among the below 20 age group.
Conclusion: Health Post remains an option model for recipient of care who stay far from the main ART clinic.

Poster Abstract Book – 3rd CQUIN Annual Meeting, Johannesburg, South Africa | November 10-14, 2019
13
24. Male-focused Strategies: Promising Community-based Approaches to Identify Men Living with HIV in Tanzania Macdonald Mahiti, Vanessa Anyoti, Damian Laki, Hawa Mziray, Shabani Kingazi, Omari Msumi, Fernando Morales, Cassia Wells, Brenda Senyana, Haruka Maruyama, Julie Franks ICAP at Columbia University Corresponding author: Macdonald Mahiti, [email protected]
Throughout sub-Saharan Africa, men living with HIV are less likely than women to know their HIV status; in Tanzania this gap is at 13%. ICAP-Tanzania sought to improve male engagement in community-based HIV testing while also improving the proportion of tests performed on men resulting in new HIV diagnoses (“yield”). Approaches included reaching male-centric venues (permanent and seasonal workplaces, guesthouses, brothels); male community outreach volunteers; training peer female sex worker community outreach volunteers to engage male clients of HIV-positive female sex workers for testing; screening for HIV risk; and follow-through on index-based testing. These approaches improved yield over four quarters (see Figure below)
Trends in Male Testing and Positive Yield over Time
114,231
135,208
76,502
46,473
2.9%3,272
3.3%4,404
6.9%5,281 10.1%
4,684
0
1,000
2,000
3,000
4,000
5,000
6,000
-
20,000
40,000
60,000
80,000
100,000
120,000
140,000
160,000
Oct-Dec 18 Jan-Mar 19 Apr-June 19 Jul-Sep 19
HTS_TST HTS_POS (% Yield)

Poster Abstract Book – 3rd CQUIN Annual Meeting, Johannesburg, South Africa | November 10-14, 2019
14
25. Taking DSD to scale while responding to recipient of care specific needs;
Integration of NCDs treatment into Facility Based Treatment Clubs at
Pigg’s Peak Hospital, Eswatini Hervé Nzereka Kambale1, Thembie Dlamini1, Simangele Mthethwa1, Ntombi Ginindza1, Nompilo Gwebu1, Hugben Byarugaba2 Lydia Mpango3, Mazwi Mavuso3, Maria Makhanya, Vuyisile Dlamini, Dumsile Mhlanga, Aimé Makengo4 SNAP1, URC2, AIDS Free3, Pigg’s Peak Hospital4 Corresponding author: Hervé Nzereka Kambale, [email protected]
The Eswatini MOH would like to share its best practice in responding to specific recipient of care needs. NCDs has been considered as one of the factors limiting enrollment into DSD because clients with NCDs were considered as not eligible for DSD, this was not making justice to recipient of care affected with NCDs despite the fact that the incidence of NCDs is progressively increasing because of the aging of clients of ART. One of the high-volume facility of the country has successfully integrated NCDs screening and management into the facility based treatment clubs. NCDs treatment has since been aligned with HIV treatment, Clients are able to refill their NCDs treatment together with their ARVs within their treatment clubs.
This initiative is in line with the core principle of differentiating care as described by WHO as way of providing ART that acknowledges specific barriers identified by clients and empowers them to manage their disease with the support of the health system. WHO highlight the need for client-centered care to improve the quality of HIV care services.
26. The Young People and Adolescent Peer Support (YAPS) Model of differentiated care for adolescents and Young people living with HIV in Uganda: Adaptation of the Zvandiri CATS model T N. Chimulwa, C. Katureebe Mboijana, E. N Magongo, Ivan Lukabwe, J. Kiggundu, Dr. Hudson Balidawa, J Musinguzi1, R. Nasaba2, B. Asire3, V. Nabitaka4, E. Nazziwa, J. Kabanda, C. Muwanga5, A. Tsitsi6, Angella Mushavi7, Nicola Willis, April Ricotta8 Ministry of Health Uganda1, ANECCA2, UNICEF Uganda Office3, CHAI4, PEPFAR5, WHO, Zimbabwe Office6, Ministry of Health Zimbabwe7, AFRICAID Zvandiri8 Corresponding author: Teddy Chimulwa, [email protected]
The Young people and Adolescent Peer support (YAPS) model is an adapted peer support intervention of differentiated HIV care for Adolescents and young people living with HIV in Uganda. It was adapted from the Zvandiri CATS model of Zimbabwe. This came after a learning visit was conducted by Ministry of Health and Partners to Zimbabwe after learning about the CATS model from the CQUIN Adolescent Consultative meeting in 2017 in South Africa. We propose to share the processes and experiences to-date.

Poster Abstract Book – 3rd CQUIN Annual Meeting, Johannesburg, South Africa | November 10-14, 2019
15
27. Zvandiri—Bringing a Differentiated Service Delivery Program to Scale for Children, Adolescents, and Young People in the Region April Ricotta, Nicola Willis, Kuda Madzeke1, Clorata Gwanzura, Shephard Bobo2, Norman Manzi3, Teddy Chimulwa4, Cecilia Kihara5 Africaid1, Ministry of Health and Child Care2, Dream Village3, Ugandan Ministry of Health,4 Frontline AIDS5 Corresponding author: April Ricotta, [email protected]
The Zvandiri model brings to scale peer-led, holistic support of children, adolescents and young people living with HIV (CAYPLHIV) ages 0-24 years that is responsive to their medical, developmental, and psychosocial needs. Led by Zimbabwe’s Ministry of Health and Child Care and Africaid, a local Private Voluntary Organisation, and in partnership with the World Health Organisation, regional Ministries of Health and multiple funding partners, this model is now being adopted or adapted in the region. We will share the journey of south-to-south collaboration and technical assistance as well as lessons learned and recommendations for the way forward.

Poster Abstract Book – 3rd CQUIN Annual Meeting, Johannesburg, South Africa | November 10-14, 2019
16
Track C: Wednesday, November 13-Thursday, November 14
28. Using quality improvement approaches to improve uptake of Determined, Resilient, Empowered, AIDS-Free, Mentored and Safe (DREAMS) adolescent care package in six health facilities in Blantyre, Malawi L Nyirenda1, T Musukwa1, F. Gent1, R. Mogha1, A. Sorgi2, I. Teri2, T. Maphosa1, A. Ahimbisibwe1 1Elizabeth Glaser Pediatric AIDS Foundation (EGPAF), Malawi. 2 Elizabeth Glaser Pediatric AIDS Foundation, (EGPAF), Washington Corresponding author: Allan Ahimbisbwe, [email protected]
Background: In DREAMS initiative among adolescent girls and young women (AGYW), we share a quality improvement model to identify critical pathway bottlenecks for care.
Methods: Orientation of facility staff on the package and collaboration sessions followed by monthly reviews to address root causes and, introduction of additional tools to the original DREAMS tools was done.
Results: We observed a progressive increase in the number registered, eligible clients tested for HIV and newly identified HIV- positives (See figure 1)
Conclusion: Quality Improvement is a critical approach to improving access to HIV testing rates and linkage to HIV treatment among the AGYW.
Figure 1: Graph showing cascade of DREAMS adolescent care package in Five health facilities (Malawi)
184369
1119
2332
177
351 321 360177 194
321 329
16 16 11 3815 16 11 35
010
00
20
00
30
00
Jul-Sep 18 Oct-Dec 18 Jan-Mar 19 Apr-Jun 19
# o
f adole
scents
Registered Eligible for Testing Tested for HIV
Uptake of DREAMS services increasing

Poster Abstract Book – 3rd CQUIN Annual Meeting, Johannesburg, South Africa | November 10-14, 2019
17
29. Leveraging the family care clinic initiative to improve management of viral load among children (0-14yrs) from six health facilities using Quality improvement approaches L Nyirenda1, M Botomani1, W Kaminyoge1, JL Sunguti1 A sorgi2 I. Teri2, A Ahimbisibwe1
1Elizabeth Glaser Pediatric AIDS Foundation (EGPAF), Malawi.2 Elizabeth Glaser Pediatric AIDS
Foundation (EGPAF)
Corresponding author: Allan Ahimbisbwe, [email protected]
Background: EGPAF Malawi in collaboration with Ministry of Health established family-centered clinics to address challenges regarding managing children with High Viral Load (HVL) using a quality improvement implementation model.
Methods: A dedicated clinic day in the week was set for children 0-14years and their family members.
Results: Of the children enrolled in HVL clinics, there was an observed increase in those completing IAC sessions, received VL results as well as switched to 2nd line ARVS. (See Figure 1 below)
Conclusion: Establishing family care clinics has facilitated completion of adherence counselling sessions, collection of VL sample and switching of children failing first line regimen.
Figure 1: HVL management milestones for infants 0-14yrs from six EGPAF supported facilities (Dec 18 - June 19)
112 108
67
47
28 23170 166 108 99 78 73
100% 96%
62%70%
60%
82%
100% 98%
65%
92%
79%
94%
0%
20%
40%
60%
80%
100%
120%
0
20
40
60
80
100
120
140
160
180
Child (0-14) HVL Enrolled in EAC Completed EAC Results received HVL after EAC Switchedregimen
Feb-19 Jun-19 Coverage coverage

Poster Abstract Book – 3rd CQUIN Annual Meeting, Johannesburg, South Africa | November 10-14, 2019
18
30. Using Quality Improvement Methodology to Scale up Differentiated Service Delivery at three high volume facilities in the Kingdom of Eswatini Hervé Nzereka Kambale, Thembie Dlamini, Simangele Mthethwa1, Hugben Byarugaba, Yvonne Makwabarara2, Lydia Mpango, Mazwi Mavuso3, Arleta Ndlela, Jonasi Solom4, Maria Makhanya, Dumsile Mhlanga5, Makhosini Mpanza, Auggy Ndlovukzi6, Sithembakuye Moyo, David Tumuhairwe7 SNAP1, URC2, AIDS Free3, ICAP4, Pigg’s Peak Hospital5, Good Shepard Hospital6, AHF Clinic7 Corresponding author: Hervé Kambale, [email protected]
The poster showcases how a quality improvement project can be used to increase coverage of DSD. The aim statement of the project was to increase the proportion of eligible ART clients enrolled in DSD in three health facilities (Pigg’s Peak, Good Shepherd, and AHF) of Eswatini from 16% to 50% from October 2018 to May 2019.
The following were the key steps for this QI project:
- Identification and training of a facility focal person
- Development of a facility’s specific SOPs
- Collection of baseline data
- Annotate or Flag files of clients that were eligible for DSD
- Implementation of an active system to offer and enroll eligible clients into DSD
The result of the steps above was an increase of DSD Coverage in the three health facilities as demonstrated in the figure below:
Poster Abstract Book – 3rd CQUIN Annual Meeting, Johannesburg, South Africa | November 10-14, 2019
19
31. Utilizing Quality Improvement interventions in Fast Track Model to promote Viral Load coverage (VLC) in Lusaka, Zambia M. Muhau1 , H. Bwalya Mulenga1, M. Mukumbwa-Mwenechanya1, C. Lyembele1 , M. Chitala1 , I.Sikazwe1, T. Savory1, M. Wa Mwanza1, D. Mwamba1,V. Kamanga1, C. Bolton1,2, M. Herce1,3
1Center for Infectious Disease Research in Zambia, Lusaka, Zambia. 2University of Alabama at Birmingham, Birmingham, United States, 3University of North Carolina at Chapel Hill, Chapel Hill, United States Corresponding author: Muhau Mubiana, [email protected]
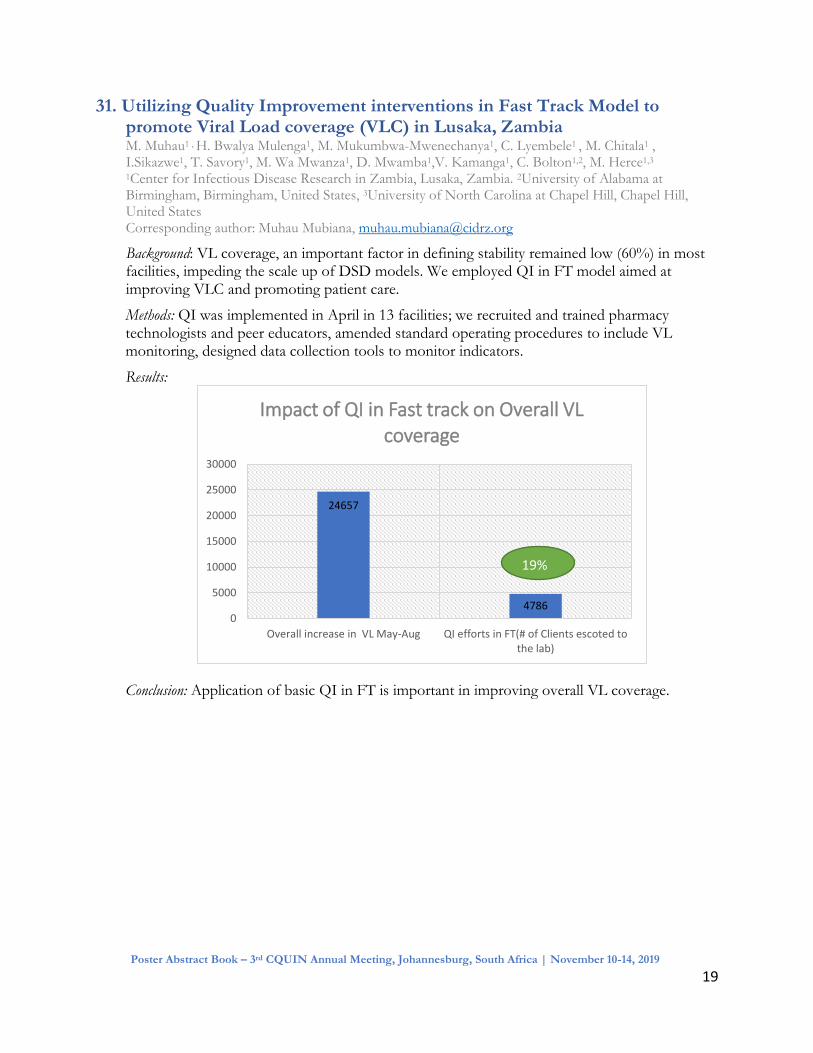
Background: VL coverage, an important factor in defining stability remained low (60%) in most facilities, impeding the scale up of DSD models. We employed QI in FT model aimed at improving VLC and promoting patient care.
Methods: QI was implemented in April in 13 facilities; we recruited and trained pharmacy technologists and peer educators, amended standard operating procedures to include VL monitoring, designed data collection tools to monitor indicators.
Results:
Conclusion: Application of basic QI in FT is important in improving overall VL coverage.
24657
47860
5000
10000
15000
20000
25000
30000
Overall increase in VL May-Aug QI efforts in FT(# of Clients escoted tothe lab)
Impact of QI in Fast track on Overall VL coverage
19%

Poster Abstract Book – 3rd CQUIN Annual Meeting, Johannesburg, South Africa | November 10-14, 2019
20
32. Sharing Tanzania Best Practices: Strides Made in Strengthening HIV Monitoring and Evaluation Systems for Improving Implementation of Differentiated Services Delivery Models Sambu V1; Rutaihwa M1, Rwebembera A1, Mzaga D1 Maokola W1, Faustine P1, Ramadhani A1 1Ministry of Health, Community development, Gender, Elderly and Children Corresponding author: Mastidia Rutaihwa, [email protected]
33. Feasibility and acceptability of iThemba - A mobile health application to support engagement in HIV care and viral load suppression ST. Lalla-Edward1*, N. Mashabane1, K. Chugh 2, M. Singh2, B. Haile2, D. Duncan3
1 Ezintsha, a sub-division of Wits Reproductive Health and HIV Institute, Johannesburg, South Africa 2 Roche, Clinical Operations and Biometrics, Pleasanton, California, USA 3 Roche, Medical and Scientific Affairs, Pleasanton, California, USA Corresponding author: ST Lalla-Edward, [email protected]
Introduction: Ithemba is a mobile health application(app) designed to promote engagement with HIV care and improve clinical outcomes. The study objective was to evaluate the feasibility and acceptability of this app which provides electronic return of HIV viral load(VL) results.
Methods: Using purposive sampling in two Johannesburg healthcare facilities, counsellors recruited people waiting for a routine HIV VL test. Eligible patients were consented and iThemba was installed on their phones. Study nurses completed processes related to the blood draw and facility shipping of samples.
Results: 706 people were screened to enroll 500(71%) participants. Technical issues with cellphones was the primary reason for screen failure. 91.6%(458/500) of results were released to participant phones of which 75.2%(344) were viewed. The median days from blood draw to receiving their VL result was 6 days compared to 56 days standard of care. The median time from results sent to the phone to results viewed was 12 hours. Majority of users responding to an in-app survey had positive ratings of the barcode scanning and VL result viewing experience(72% and 83% respectively).
Conclusion: iThemba can increase the speed of HIV VL result return to accelerate clinical decision-making and empower patients to remain adherent and engaged in care.

Poster Abstract Book – 3rd CQUIN Annual Meeting, Johannesburg, South Africa | November 10-14, 2019
21
34. Tracking Scale up of Quality Differentiated Service Delivery Through Supportive Supervision Ivan Lukabwe1, Hudson Balidawa1, Cordelia Katureebe1, Josen Kiggundu1, Edgar Kansiime2, Joshua Musinguzi1 1. Ministry of Health, Uganda
2. Makerere University School of Public Health
Corresponding author: Ivan Lukabwe, [email protected]
Background/introduction: In 2016, Ministry of Health adapted Differentiated Service Delivery (DSD) models for testing, care and treatment for Persons Living with HIV or Tuberculosis. Site supervision is being used to monitor scale up.
Methods Two rounds of supervision were conducted in September 2018 and March 2019 with 85 and 56 sites visited respectively to assess level of implementation against standards.
Results: Demonstrated in figure below.
Discussion: Marked increase in sites with policies, leadership for DSD and patients correctly categorisation. Human resource, governance, M&E and CQI for DSD still sub optimal. Next steps/way forward: Scale up of quality DSD by addressing identified gaps through routine coaching, mentorship and supervision.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Sep
-18
Mar
-19
Sep
-18
Mar
-19
Sep
-18
Mar
-19
Sep
-18
Mar
-19
Sep
-18
Mar
-19
Sep
-18
Mar
-19
Sep
-18
Mar
-19
Sep
-18
Mar
-19
Sep
-18
Mar
-19
Sep
-18
Mar
-19
Policies HR Leadership Governance HTS Care & Rx Supply Chain M&E CQI Categorisation

Poster Abstract Book – 3rd CQUIN Annual Meeting, Johannesburg, South Africa | November 10-14, 2019
22
35. A Research Agenda for Differentiated ART delivery Anna Grimsrud, Lynne Wilkinson, Lina Golob International AIDS Society1 Corresponding author: Anna Grimsrud, [email protected]
Many countries, particularly in sub-Saharan Africa, have adopted policies on differentiated service delivery (DSD) for antiretroviral therapy (ART) and have begun implementing models. However, there are unanswered research questions on how best to meet the diverse needs of people living with HIV as DSD is scaled up. This poster outlines a research agenda for differentiated ART delivery based on a think tank discussion that brought together key stakeholders from eight countries, including ministries of health, HIV service providers and HIV implementation scientists.
The research gaps presented will be according to the four groups of people living with HIV as described by the World Health Organization: 1) For individuals who are clinically stable, 2) individuals receiving an ART regimen that is failing, 3) individuals presenting or returning to care when clinically well, 4) individuals presenting or returning to are with advanced HIV disease.
36. Direct Service Delivery (DSD) models to strengthen retention in care through Community ART Refill groups (CARGs) TA Tafuma1 , A Muchedzi1 , R Dhliwayo1, T Nyagura2 , M Mayanga1 , C Gwanzura3, T Zulu1 , T Mavimba1 , T Samushonga1, D Harbick1, FH Mudzengerere1 1FHI 360, Harare, Zimbabwe 2 United States Agency for International Development, Harare, Zimbabwe 3Ministry of Health and Child Care, Harare, Zimbabwe Corresponding author: Taurayi Tafuma, [email protected]