The Contractile Properties of Human Heart Muscle: Studies
12
Journal of Clinical Investigation Vol. 44, No. 6, 1965 The Contractile Properties of Human Heart Muscle: Studies on Myocardial Mechanics of Surgically Excised Papillary Muscles * EDMUND H. SONNENBLICK,t EUGENE BRAUNWALD, AND ANDREW G. MORROW (From the Cardiology Branch and the Clinic of Surgery, National Heart Institute, Bethesda, Md.) Previous studies of the performance character- istics of the heart have usually been directed to its function as a pump and, therefore, have been concerned principally with measurements of in- travascular and intracardiac pressures, flows, and derivatives of these variables. Over the past three decades, extensive studies of skeletal muscle have provided an understanding of the mechani- cal behavior and energetics of this tissue (1-5). Recent studies of isolated segments of mammalian heart muscle (6-8) have permitted extension of this approach to the myocardium and have sug- gested the feasibility of analyzing the perform- ance of the ventricle in terms of its properties as a muscle (9-12). Although efforts have been made to characterize normal and abnormal func- tion of the human heart from this point of view (13-15), a necessary first step is a detailed de- scription of the mechanical properties of human heart muscle. Such a description-is presented in this report, and a direct extension of these in- vestigations to the intact human ventricle is the subject of the companion paper (16). Methods Left ventricular papillary muscles were obtained at the time of mitral valve replacement in 19 patients. The pa- tients ranged in age from 21 to 64 years; 13 were males and 6 were females. The major hemodynamic abnor- mality in 8 patients was mitral regurgitation, in 5 pa- tients it was mitral stenosis, and in 6 patients combined stenosis and regurgitation were present. Five patients had associated aortic valve disease, and in 4 of the 19 pa- tients the aortic valve was also replaced with a prosthesis * Submitted for publication December 28, 1964; ac- cepted February 25, 1965. Presented in part before the American Society for Clinical Investigation, May 4, 1964, Atlantic City, N. J. t Address requests for reprints to Dr. Edmund H. Sonnenblick, National Heart Institute, Bethesda, Md. 20014. at the same operation. The valvular malformation re- sulted from rheumatic heart disease in 18 patients, and in the other mitral regurgitation was caused by ruptured chordae tendineae with an otherwise normal valve. All of the patients were in functional class III or class IV and were receiving maintenance digoxin therapy at the time of operation. The mitral valve was exposed during total cardiopul- monary bypass, and after the valve leaflets had been de- tached from the annulus, the papillary muscles were di- vided at their origins from the ventricular wall and the valve and muscles removed en bloc. The patients' tem- peratures were usually 34 to 350 C, and bypass had been in progress for 10 to 15 minutes when the papillary muscles were transected. Immediately upon removal, the papillary muscles were placed in Krebs solution into which a 95% 02 and 5% C02 gas mixture was bubbled. The thinnest discrete segment of papillary muscle was then selected and rapidly transferred to a myograph. If the papillary muscles were unduly thick, they were split longitudinally to provide a thin segment and to facilitate oxygenation. The lengths of the muscle segments, at the peak of the length-active tension curve, averaged 14.0 ± 3.9 (SD) mm, whereas the cross-sectional areas averaged 5.5 ± 3.9 mm'. The myograph in which the muscles were studied has previously been described in detail (7). The papillary muscle was held at its lower nontendinous end by a spring- loaded clip, forming the end of a rigid pin that penetrated the bottom of the bath and was directly attached to a Statham (GI-4-250) force transducer. The upper ten- dinous end of the muscle was attached to an isotonic lever for the measurement of muscle shortening, and the lever itself was mounted on a rigid Palmer stand. With this arrangement, when the position of the lever was fixed, the force of isometric contraction at any desired muscle length could be measured. The lever could also be freed and, by appropriate loading, the extent and velocity of shortening of the muscle at any preload (the small load that acts on the resting muscle and thereby establishes the initial length) and afterload (the load encountered by the contracting muscle when it attempts to shorten) could be measured. The muscles were stimulated super- maximally with square wave DC impulses of 5 msec dura- tion,' delivered through large platinum plates placed 'American Electronics stimulator, model 104A. 966
Transcript of The Contractile Properties of Human Heart Muscle: Studies

Journal of Clinical InvestigationVol. 44, No. 6, 1965
The Contractile Properties of Human Heart Muscle: Studieson Myocardial Mechanics of Surgically Excised
Papillary Muscles *EDMUND H. SONNENBLICK,t EUGENE BRAUNWALD, AND ANDREW G. MORROW
(From the Cardiology Branch and the Clinic of Surgery, National Heart Institute,Bethesda, Md.)
Previous studies of the performance character-istics of the heart have usually been directed toits function as a pump and, therefore, have beenconcerned principally with measurements of in-travascular and intracardiac pressures, flows, andderivatives of these variables. Over the pastthree decades, extensive studies of skeletal musclehave provided an understanding of the mechani-cal behavior and energetics of this tissue (1-5).Recent studies of isolated segments of mammalianheart muscle (6-8) have permitted extension ofthis approach to the myocardium and have sug-gested the feasibility of analyzing the perform-ance of the ventricle in terms of its properties asa muscle (9-12). Although efforts have beenmade to characterize normal and abnormal func-tion of the human heart from this point of view(13-15), a necessary first step is a detailed de-scription of the mechanical properties of humanheart muscle. Such a description-is presented inthis report, and a direct extension of these in-vestigations to the intact human ventricle is thesubject of the companion paper (16).
Methods
Left ventricular papillary muscles were obtained at thetime of mitral valve replacement in 19 patients. The pa-tients ranged in age from 21 to 64 years; 13 were malesand 6 were females. The major hemodynamic abnor-mality in 8 patients was mitral regurgitation, in 5 pa-tients it was mitral stenosis, and in 6 patients combinedstenosis and regurgitation were present. Five patientshad associated aortic valve disease, and in 4 of the 19 pa-tients the aortic valve was also replaced with a prosthesis
* Submitted for publication December 28, 1964; ac-cepted February 25, 1965.
Presented in part before the American Society forClinical Investigation, May 4, 1964, Atlantic City, N. J.t Address requests for reprints to Dr. Edmund H.
Sonnenblick, National Heart Institute, Bethesda, Md.20014.
at the same operation. The valvular malformation re-sulted from rheumatic heart disease in 18 patients, andin the other mitral regurgitation was caused by rupturedchordae tendineae with an otherwise normal valve. All ofthe patients were in functional class III or class IV andwere receiving maintenance digoxin therapy at the timeof operation.The mitral valve was exposed during total cardiopul-
monary bypass, and after the valve leaflets had been de-tached from the annulus, the papillary muscles were di-vided at their origins from the ventricular wall and thevalve and muscles removed en bloc. The patients' tem-peratures were usually 34 to 350 C, and bypass had beenin progress for 10 to 15 minutes when the papillarymuscles were transected. Immediately upon removal, thepapillary muscles were placed in Krebs solution intowhich a 95% 02 and 5% C02 gas mixture was bubbled.The thinnest discrete segment of papillary muscle wasthen selected and rapidly transferred to a myograph. Ifthe papillary muscles were unduly thick, they were splitlongitudinally to provide a thin segment and to facilitateoxygenation. The lengths of the muscle segments, at thepeak of the length-active tension curve, averaged 14.0 ±3.9 (SD) mm, whereas the cross-sectional areas averaged5.5 ± 3.9 mm'.The myograph in which the muscles were studied has
previously been described in detail (7). The papillarymuscle was held at its lower nontendinous end by a spring-loaded clip, forming the end of a rigid pin that penetratedthe bottom of the bath and was directly attached to aStatham (GI-4-250) force transducer. The upper ten-dinous end of the muscle was attached to an isotonic leverfor the measurement of muscle shortening, and the leveritself was mounted on a rigid Palmer stand. With thisarrangement, when the position of the lever was fixed,the force of isometric contraction at any desired musclelength could be measured. The lever could also be freedand, by appropriate loading, the extent and velocity ofshortening of the muscle at any preload (the small loadthat acts on the resting muscle and thereby establishesthe initial length) and afterload (the load encountered bythe contracting muscle when it attempts to shorten)could be measured. The muscles were stimulated super-maximally with square wave DC impulses of 5 msec dura-tion,' delivered through large platinum plates placed
'American Electronics stimulator, model 104A.
966

MECHANICS OF HUMAN HEART MUSCLE
parallel to the long axis of the muscle. Force, musclelength, the first derivatives of these variables, and thestimulus artifact were recorded on a multichannel oscil-lograph, and in some instances the transducer outputswere displayed on a dual-beam oscilloscope (Tektronixmodel 502) and photographed. The work performed bythe papillary muscle was calculated as the product ofafterload in grams and displacement in millimeters, andwas expressed in units of gram-millimeters; maximalpower was calculated as the product of the maximalshortening rate (dl/dt) and afterload, and it was ex-pressed in units of gram-millimeters per second.
Experiments were carried out at 300 C. In order tomaintain optimal performance of the muscles for pro-longed periods of time, frequencies of contraction of 6 to12 per minute were employed, except when the effects ofchanges of frequency of contraction were specificallystudied. To assure steady-state performance, a period of1 hour was allowed between the time the muscle wasplaced in the myograph and the initial recordings. Eachstudy was terminated when mechanical performance be-gan to deteriorate. Papillary muscles from three addi-tional patients did not maintain a steady state at the onsetof the experiment and were discarded.Four major aspects of myocardial mechanics were ana-
lyzed: 1) the passive and active length-tension curves,2) the force-velocity relation of the contractile componentof the muscle, with considerations of external work andpower, 3) the load-extension ("stress-strain") relation
A LENGTH-TENSION RELATION7 J.S. 05-13-75
34Y M. MITRAL REGURG.FUNCT. CLASS ME Moximumxfit
6 lmension of Lo
5 1To/of fension
of the series elastic component, and 4) the relationshipbetween the frequency of contraction and the performanceof the muscle, as reflected in force development, velocityof shortening, work, and power. The effects of thecardiac glycoside strophanthidin and of norepinephrineon the force-velocity relation of the muscles were alsodetermined.
Results
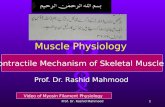
I. Length-tension relations. Isometric length-tension curves were determined in the papillarymuscles from all 19 patients, and the results of atypical experiment are shown in Figure IA. Inorder to allow comparisons among different ex-periments, all length-tension curves were per-formed at 300 C at a frequency of 12 contractionsper minute. The actively developed tension wascalculated as the difference between the peaksystolic (total) tension and the resting tension,and that muscle length at which both the restingand active tensions approached zero was definedas L. (Figure 1A). As muscle length was in-creased, both active and resting tensions rose;the peak of the length-active tension curve wasreached when the muscle was stretched to anaverage length of 151 ± 1% of Lo, and the maxi-
7
6C-5
zf40
1c:0"I.aC0
B
2F
00 10 20 30 40 50
%INCREASE IN LENGTH
0RATE
10 20OF FORCE DEVELOPMENT (g/sec)
Lo8MM 1IMM 12MM
FIG. 1. A. LENGTH-TENSION RELATIONS OF HUMAN PAPILLARY MUSCLE.Abscissa: Muscle length in millimeters and the per cent increase in musclelength above L4 (muscle length at which both the resting and active tensionsapproached zero). Frequency of contractions = 12 per minute. Cross-sec-tional area of muscle = 3.6 mm'. B. RELATIONSHIP BETWEEN ACTIVELY DE-VELOPED TENSION AND THE MAXIMAL RATE OF ISOMETRIC FORCE DEVELOPMENT,
967

E. H. SONNENBLICK, E. BRAUN\VALD, AND A. G. MORROW
o0 3 - @\ 0 500 1O-EEE
4-tz (IUi
0 X0
1 2 3 4 5 6 7LOAD (g)
FIG. 2. RELATION BETWNEEN INITIAL VELOCITY OF ISOTONIC SHORTEN-ING AND AFTERLOAD. F1reqluency of conltractionls =12 per minute.Muscle cross-sectional area =3.2 mmt2. Preload =1.4 g with a musclelength of 15 mmn. The insert inl the upper right showes several oscil-lo~scopic recordings from whlich the experimental psoinlts were calcu-lated, and the afterload for each of these contractions is indicated.
mal actively developed tension averaged 1.81 +
1.19 (SD) g per mm2. \Vith further increases innuiscle length, actively developed tension reacheda l)lateatu alnd then declined as resting tensionrose precil)itously. The time interval from theonset of contraction to the instant at which peaktension was achieved was independent of musclelength and, as a consequence, when muscle lengthwas increased the maximal rate of force develop-ment (dpl/dt) was found to be a linear functionof actively developed tension (Figure 1B). Nocorrelation between maximal developed tensionper ullit cross-sectional area and the actual cross-sectionial area of the muscle could be perceived.
I1. Forcc-vcloc'ity relahtouis. Force-velocity re-kit0ions wVcre determine(l in the papillary musclesof sevenl patients. A typical curve is depicted inFigure 2, and in the insert some of the originaloscilloscopic tracings from which the curve wasderived are reproduce(d. The initial length of
the muscle wXas set by a small preload, which wasmaintained constant for the entire curve. Theeffects on the velocity of shortening of progres-sively inicreasing afterload were then determined.The maximal velocity of shortening (Vma.x) couldnot be determined directly at zero load, since asmall preload was necessary to establish theinitial muscle lengths, and Vmax lwas, therefore,obtained by extrapolation. An inverse relationbetween the afterload and both the initial velocityand extent of shortening was observed in everymuscle. It weas also noted that the time from thestimnulus to maximal shortening was independentof the afterload.The effects of altering the initial muscle length
oni the force-velocity curve were examined by de-termininiihg 32 curv-es in 4 muscles. As seen inFigure 3A, Vnimax appeared to remain constant,but P0 (isometric tension) increased as a functionof initial length. P,) is used in this context as
968

MECHANICS OF HUMAN HEART MUSCLE
isometric force without implying tetanic force aswould be obtained in skeletal muscle. The effectsof altering the frequency of contraction on theforce-velocity curve were examined by determin-ing 13 curves in three muscles (Figure 3B). Inindividual muscles, contraction frequencies werevaried between 6 and 60 per minute, but all threemuscles were examined at rates of 12 and 30per minute. When the frequency of contractionwas increased at a constant initial muscle length,P. remained essentially unchanged, while Vmaxincreased strikingly. For the three muscles ex-amined, Vmax was 38%, 39%, and 23% greaterat 30 contractions per minute than at 12 con-tractions per minute.The effects of strophanthidin (0.5 ug per ml)
on the force-velocity relation were studied in themuscles obtained from three patients, and a rep-resentative pair of curves is shown in Figure 4A.
FORCE- VELOCITY
7 A. Increosing muscle /ength
6! Preload Length~~~~~~(g) (mm)
E (\00.4 8.0E 5 0 1.6 8.6z 0w
4 J.S.05-13-75 1-31-64\ 34y d'M it. Regurg
I Funct class mC')
0-3
>
The glycoside augmented both P. (39%o, 20%,and 84%o, respectively) and V... (15%o, 140%,and 125%, respectively) in each muscle. Nor-epinephrine (0.2 pg per ml) also shifted theforce-velocity relation upwards and to the right(Figure 4B); norepinephrine augmented P. by24%o + 6%o in the 14 muscles examined. In con-trast to the effects of changing initial musclelength, the shift in the force-velocity relation re-sulting from either norepinephrine or strophan-thidin was always accompanied by a decrease inthe time from stimulation to maximal force de-velopment. This time interval decreased from anaverage of 725 msec to 660 msec with strophan-thidin, and from an average of 720 msec to 530msec with norepinephrine.
Inspection of the force-velocity relation indi-cates that as V.ax and P0 are approached, externalwork and power approach zero, and these two
LOAD (g)
FIG. 3. A. EFFECTS OF INCREASING INITIAL MUSCLE LENGTH ON THE FORCE-VELOCITY RE-LATION. The maximal isometric force (PO) is augmented without a change in maximal velocityof shortening (Vmax). The time from stimulus to peak shortening was 440 msec for bothinitial lengths. Frequency of contractions = 12 per minute. B. EFFECTS OF INCREASING FRE-QUENCY OF CONTRACTION FROM 6 PER MINUTE TO 50 PER MINUTE. Vm.. is increased without achange in Po, while the time from stimulus to peak shortening decreased from 420 to 280 msec.The curves in A and B were derived from the same muscle, which had a cross-sectional areaof 3.6 mm'.
969

E. H. SONNENBLICK, E. BRAUNWALD, AND A. G. MORROW
EI-EE
zzwI-0
xUA.0
0-Jw
FORCE-VELOCITY IN HUMAN PAPILLARY MUSCLE
LOAD (g)
FIG. 4. A. EFFECT OF THE ADDITION OF STROPHANTHIDIN ON THE FORCE-VELOCITY RELATION.
Initial muscle length = 10.0 mm with a preload of 0.8 g. Muscle cross-sectional area = 3.6 mm'.The addition of strophanthidin increased both Vmax and PO while decreasing the time fromstimulation to maximal shortening from 390 to 340 msec. B. EFFECT OF THE ADDITION OF NOR-EPINEPHRINE ON THE FORCE-VELOCITY RELATION. Initial muscle length = 15.0 mm with a pre-
load of 1.4 g. Muscle cross-sectional area = 3.2 mm'. Norepinephrine augmented both Vmaxand PO while decreasing the time from stimulation to peak shortening from 730 to 540 msec.
variables reach a maximal value at some inter-mediate load. In the seven muscles in whichforce-velocity curves were obtained, it was ob-served that the peak values of work were achievedwith afterloads that ranged from 45% to 55%o ofisometric force (P.), while the peak values ofmaximal power were achieved with afterloadsranging from 50% to 60%o of the isometric force(P.). Increasing initial length of the muscle ele-vated the afterload-work and afterload-powercurves and raised the afterload at which the peakvalues of work and power were achieved (Figure5,A and B). At a constant initial muscle lengththe addition of norepinephrine also elevated andshifted the load-work and load-power curves tothe right (Figure 5,C and D). Increasing thefrequency of contraction did not significantly af-fect the load-work curve in the three musclesexamined (Figure 5E). However, in all in-stances a significant elevation of the load-powercurves resulted from increasing frequency (Fig-ure 5F), peak power rising by 40%o, 28%, and22%, respectively, in the three muscles as fre-
quency of contraction was elevated from 12 to30 per minute.
III. Load-extension curve of the series elasticcomponent. The series elastic component of thepapillary muscles was characterized in musclesfrom 5 patients by an analysis of afterloaded iso-tonic contractions relative to time after stimula-tion. In Figure 6A a typical force-velocity curveis shown, whereas in Figure 6B the velocities ofshortening (dl/dt) and the force for the samecontractions are plotted as functions of the timeafter stimulation. As described in detail else-where (17), at the time the muscle stops devel-oping force and begins to shorten, the serieselastic component is being stretched at a velocity(dl/dt) equal to but opposite in direction to thatof the contractile element. Therefore, the curverelating dl/dt to time after stimulation (Figure6B) applies to both the contractile element andthe series elastic component. By integrating dl/dtas a function of time, the extension of theseries elastic (SE) component with increasingforce (load) was determined (AL of SE = fptO°
970

MECHANICS OF HUMAN HEART MUSCLE
la0
P1
FIG. 5. RELATIONS OF WORK AND POWER WITH INCREASING AFTERLOAD, AS
INITIAL MUSCLE LENGTH WAS CHANGED (A AND B), NOREPINEPHRINE WAS
ADDED (C AND D), AND THE FREQUENCY OF CONTRACTION INCREASED (E AND
F).
dl/dt- dt). The load-extension curve of the serieselastic component obtained in this manner is re-produced in Figure 6C, and shows that withprogressive extension of the series elastic the forcedeveloped increased exponentially. In the fivemuscles in which this analysis was carried out,it was observed that during an isometric con-traction the series elastic was stretched by 8.4%o± 0.5%o of the initial length of the muscle atwhich the force-velocity curve was obtained.Further, the load-extension curve of the series
elastic component was not altered by changingfrequency of contraction nor by the addition ofnorepinephrine or strophanthidin.
IV. Force frequency relations. The effects ofchanging frequency of contraction were studied inpapillary muscles obtained from 16 patients. Arepresentative study on a muscle relating fre-quency to extent of shortening, time to maximalshortening, and velocity of shortening is shownin Figure 7A, whereas a representative study onan isometrically contracting muscle relating fre-
971

E. H. SONNENBLICK, E. BRAUNWALD, AND A. G. MORROW
A. FORCE -VELOCITY RELATION:B.FORCE AND VELOCITY AS
FUNCTIONS OF TIME C.LOAD-EXTENSION CURVE OF
0 2 4 6 0 400 800LOAD(g) TIME AFTER STIMULATION-msec
0 04 0.8 1.2EXTENSION OF SE-mm
FIG. 6. PROPERTIES OF THE SERIES ELASTIC COMPONENT OF A HUMAN HEART MUSCLE WITH
AN INITIAL MUSCLE LENGTH OF 13.5 MM AT A PRELOAD OF 1.0 G. Muscle cross-sectional area =
3.5 mm'. A. Velocity of isotonic shortening in millimeters per second as a function of increasingafterload. B. Velocity of shortening and force of contraction as functions of the time afterstimulation of the muscle. C. The load-extension relation of the series elastic component.
quency to isometric force, time to peak force,and rate of development of force is shown inFigure 7B. At a frequency of 6 contrac-tions per minute, the time from the onset ofcontraction to peak tension averaged 876 + 150msec, while the rate of force development aver-aged 20.8 g per second. At a frequency of 50
3.5 [
2.5[
A.
Shortenng-Frequency
-~~p
10 20 30 40 50FREQUENCY
contractions per minute, the time to peak tensiondecreased in every muscle to an average of 455± 89 msec, whereas the maximal rate of forcedevelopment increased in every muscle to an aver-age value of 35.0 g per second. Similarly, inevery muscle the time to peak shortening de-creased from an average of 410 ± 48 msec to
B.- 02 ;,,_C)
0o0
m :
<~0
-u0
ITS ,om
_C-1
FIG. 7. A. VELOCITY OF SHORTENING, THE EXTENT OF SHORTENING (AL), AND THE TIME
FROM STIMULATION TO PEAK SHORTENING ARE SHOWN AS FUNCTIONS OF FREQUENCY OF CON-
TRACTION. Preload = 0.4 g; afterload = 2.0 g. Muscle length = 15.0 mm; cross-sectional area
= 3.5 mm'. B. RELATION OF ISOMETRICALLY DEVELOPED FORCE, THE TIME FROM STIMULATION TO
PEAK FORCE DEVELOPMENT, AND THE RATE OF FORCE DEVELOPMENT AS FUNCTIONS OF FREQUENCY
OF CONTRACTION. Muscle length = 9.0 mm; cross-sectional area = 7.5 mm'.
,. 3.0
-!:
EO
;-; 2.0
crn
o= 1.0I--
-J
>-0
5
4
j.O1.6
4 E
4
1-
IAf
I-
0z)E
u Z
J ,|
60 10 21OF CONTRACTION /min.
972

MECHANICS OF HUMAN HEART MUSCLE
280 + 32 msec, while the velocity of shorteningincreased in every muscle, from an average of4.63 + 0.57 to 6.58 + 0.42 mm per second. Onthe other hand, alterations in frequency of con-traction produced little change either in isometricforce or in the extent of shortening of the iso-tonically contracting muscle. At 6 contractionsper minute, force averaged 12.4 g and at 50 con-tractions per minute 10.4 g. In the isotonicallycontracting muscle the extent of shortening atthese rates averaged 1.85 + 0.27 and 1.79 + 0.22mm.
Discussion
The left ventricular papillary muscles, whichmay be obtained from patients in the course ofcorrective cardiac operations, provide a uniqueopportunity for analyzing in vitro the contractileproperties of human heart muscle. Since thepreparation described in this report has not beenemployed previously, it is important to com-ment upon certain limitations inherent in its use.Perhaps the most important of these is thethickness of the human papillary muscle, whichmay not allow for adequate oxygenation at physi-ologic temperatures and frequencies of contrac-tion. For this reason, most of the experimentsdescribed herein were carried out at 30° C andat 6 to 12 contractions per minute. Fortunately,it is possible to recognize inadequate oxygenationof the muscle in relation to its energy require-ments since, when this occurs, the mechanicalperformance of the muscle deteriorates progres-sively. As noted previously, stable mechanicalactivity could not be achieved in several prepara-tions, and these muscles were discarded. Simi-larly, even in muscles that were initially stable, theexperiments were terminated when, in the courseof the study, a decrease in performance was ob-served.One meaningful way of characterizing a
muscle's performance is to measure the isometrictension that it develops at the apex of the length-active tension curve. In order to compare dif-ferent muscles, the maximal isometric tension iscorrected for the muscle's cross-sectional area.Abbott and Mommaerts observed a peak tensionof the order of 2.0 g per mm2 at 30° C in papil-lary muscles from normal cats (6). The averagepeak tension observed in the present study was
only slightly lower than 2.0 g per mm2, and twomuscles developed peak forces as high as 4.5 gper mm2. It is of interest that the cross-sec-tional area of the muscle did not appear to in-fluence the normalized maximal active tension.Furthermore, it must be appreciated that all ofthe muscles studied in this investigation were ob-tained from patients with serious organic heartdisease, and on analysis many of these muscleswere found to be depleted of norepinephrine (18).It is possible that the congestive heart failurestate or norepinephrine depletion (19), or both,might have depressed the mechanical perform-ance of certain muscles and thus account for thelower values of peak tension that were observedin them. The possible association of myocardialnorepinephrine concentration to the mechanicalperformance of papillary muscles is presently un-der investigation.The close resemblance between the length-active
tension curves of the papillary muscle, studied invitro, and the human ventricular myocardium,previously studied in vivo by means of a straingauge arch (20), lends further support to thevalidity of the human papillary muscle preparationand indicates the relevance of the data obtainedto the intact heart. The large elevations of ten-sion that occur consequent to small increases ininitial length (Figure 1) demonstrate the po-tential usefulness of the Frank-Starling mecha-nism when increases in force of contraction arerequired. From previous studies on intact pa-tients, it may be inferred that the left ventricleof a subject without heart failure operates onthe ascending limb of the Frank-Starling curve,but that the left ventricle of a patient with heartfailure operates near the peak or along the plateauof the curve (21, 22). When these observationsare taken together with the present findings thatthe peak of the length-active tension curve isreached at L0 + 51%, it would appear that theend-diastolic fiber lengths in the normal ventricleare less than this value, while the end-diastolicfiber lengths in the failing myocardium are prob-ably close to this value. Inspection of Figure 1also reveals that as the peak of the length-activetension is approached, the resting length-tensioncurve rises sharply. In this region of the curvenot only is further augmentation of ventricularperformance through the operation of the Frank-
973

E. H. SONNENBLICK, E. BRAUNWALD, AND A. G. MORROW
Starling mechanism not possible, but even smallincreases in initial length require substantial ele-vations of ventricular filling pressure.
Extensive investigations of skeletal muscle(1-5) have made it clear that a more completecharacterization of contraction requires a consid-eration not only of the force developed by themuscle, but also of its velocity of shortening. Therelation between these two variables comprisesthe force-velocity curve. In skeletal muscle, thisrelation is generally examined under tetanic con-ditions, while in heart muscle tetanus cannot ordi-narily be induced, and single contractions pro-vide the basis of the force-velocity relations thatare obtained. Previous investigations on thecat papillary muscle have demonstrated that, incontrast to skeletal muscle, the force-velocitycurve of myocardium does not remain fixed butmay be shifted by a variety of influences (6-8).If the duration of the active state of the contractilesystem is abbreviated, the force-velocity curvemay deviate from its expected hyperbolic form,so that as the load is progressively increased,velocity falls off more rapidly than anticipated(Figures 2 to 4). The isometric tension that isactually recorded may be less than that whichwould have occurred if the active state had con-tinued and the muscle had contracted tetanically.Factors tending to shorten the active state, suchas increasing the temperature of the bath, exag-gerated the deviation of the curve from a hyper-bolic form at higher loads.From the present study it is clear that an in-
crease in initial muscle length increases the maxi-mal force of isometric contraction (PO) withoutaltering the maximal velocity of shortening(Vmax). It is suggested that this type of shiftin the force-velocity curve does not represent achange in the fundamental contractile state of themyocardium, since it now appears that alterationsin initial muscle length change the total numberof active contractile sites, without affecting therate of their interaction (4, 8, 17). It has alsobeen shown that the force-velocity curve can beshifted by increasing the frequency of contraction(Figure 3) and by the administration of norepi-nephrine or strophanthidin (Figure 4). In con-trast to the effects of altering initial muscle length,these interventions augment Vmax (with or with-out elevating P.). It is suggested that this type
of shift in the force-velocity curve does representa change in the fundamental contractile state ofthe myocardium, since it is believed that the ele-vation of Vmax results from an increase in therate of interaction of the contractile sites, re-gardless of the number of sites involved (4, 8).A. V. Hill has provided evidence for the viewthat the force-velocity relation represents a funda-mental mechanical property of active muscle (1).This view, more recently expanded upon byPodolsky (4), derives from the observations madeon the frog sartorius muscle that the rate of heatproduction depends on the velocity of shortening(1). It has been concluded that there is a tightlink between the chemical processes that gen-erate force and the mechanical events, and thata change in Vmax (the intrinsic speed of themuscle) implies that a basic alteration has oc-curred in the mechanochemical coupling at thesites that generate force.
It is readily apparent that both the power andwork performed by the muscle may be consideredto be derivatives of the force-velocity relation.Just as the extent of shortening and the velocityof shortening are functions of the load, so arethe products of shortening and load (work) andvelocity of shortening and load (power). It isof interest that while an increase in the initiallength of the muscle augmented both work andpower at any given load, an increase in the fre-quency of contraction elevated the power but didnot affect the work performed (Figure 6, E andF), since velocity of shortening increased withoutincreasing extent of shortening (Figure 7). Sim-ilar observations have also been made in theintact dog heart (23). From these considerationsit is apparent that a change in the contractilestate of the muscle can occur and not be detectedin the relationship between initial length andwork, but be clearly apparent in the force-velocityand load-power relationships.The effects of altering the frequency of con-
traction on the mechanical performance of heartmuscle has been the subject of considerable in-terest and investigation. It is now clear thatthe force-frequency relation differs strikinglyamong various mammalian species and that evenin the same species atrial and ventricular musclemay behave differently (24-26). Accordingly,it was not possible, on the basis of existing in-
974

MECHANICS OF HUMAN HEART MUSCLE
formation, to predict the effects of altering fre-quency on the contractile properties of humanheart muscle. It was observed that as the fre-quency of contraction was increased, the durationof contraction diminished and the velocity ofshortening increased. An important consequenceof this reciprocal relationship is the relative con-stancy of the force or extent of shortening ob-served, within the range of frequencies examined.Since force remained constant at increasing fre-quency, there was no evidence that the humanmyocardium exhibited the classical Bowditch or"force staircase" (27), but the profound aug-mentation of the velocity of shortening (Figure7A) and increase of Vma. in the force-velocitycurve (Figure 3) indicate that this tissue doesexhibit what might be termed a "velocity stair-case." These data on the effect of frequency onthe duration of contraction of the isolated humanpapillary muscle also help to explain findings inthe intact heart. The abbreviation of contractiontime with increasing rate is reflected in the short-ening of the systolic ejection period and aug-mentation of the mean systolic ejection rate in thedog heart in which stroke volume is held con-stant (28). Similarly, the striking decrease inthe systolic ejection period observed when heartrate is increased by electrical stimulation of theright atrium in human subjects can be accountedfor primarily by the shortening of the contractiontime (29). Despite these apparent correlationsbetween the findings in the isolated muscle andin the intact heart with increasing frequency ofcontraction, certain limitations of the preparationmust be kept in mind. The findings obtained inthis investigation apply for frequencies belowphysiological levels, i.e., less than 50 contractionsper minute. Further, these muscles have, by defi-nition, been obtained from "failing" ventriclesand from patients being maintained on digoxin.Thus, the applicability of the observed "velocity"staircase requires further confirmation.
Since the development of force by muscle re-quires the interaction of contractile elements witha series elastic component (1), an understandingof the mechanical properties of the latter is es-sential to an analysis of myocardial contraction.As the contractile element shortens, the serieselastic component is extended. If the externalends of the muscle are fixed, i.e., in an isometric
contraction, the rate of force development by themuscle depends not only on the force-velocityrelations of the contractile element, but also uponthe stress-strain characteristics of the passive,springlike series elastic. Since the addition ofnorepinephrine to cat papillary muscle (8), andof both norepinephrine and strophanthidin tohuman muscle, does not alter the stress-straincharacteristics of the series elastic component, itmay be inferred that changes in the rate of forcedevelopment are dependent primarily on perform-ance of the contractile element. In the presentinvestigation it was calculated that during iso-metric contractions the series elastic componentis stretched by an average of 8.4%o of the entiremuscle length. Thus, it is apparent that signi-ficant shortening of the contractile elements oc-curs even during so-called isometric contractions.This observation is also relevant to an under-standing of the discrepancy between the actualwork performed by the contractile elements andthe calculated external work performed by theisolated muscle of the intact heart, a fact that isreceiving increasing attention in consideration ofenergy control in heart muscle (30).
Summary
The contractile properties of human heartmuscle were studied in left ventricular papillarymuscles excised from 19 patients at the time ofprosthetic replacement of the mitral valve. Anal-ysis of the isometric length-tension relations re-vealed that the peak of the active tension curvewas reached when the muscle was stretched toan average length that exceeded the initial lengthby 51 %. Further increases in muscle length pro-duced a precipitous rise in resting tension, whileactive tension declined. An inverse relation be-tween afterload and initial velocity of shorteningwas observed in every muscle, extending to humanheart muscle the concept of force-velocity rela-tions. When initial muscle length was increased,isometric tension was augmented but the maximalvelocity of shortening remained constant. Theaddition of strophanthidin or norepinephrine in-creased the maximal velocity of shortening as wellas the isometric tension, whereas increasing thefrequency of contraction augmented the maximalvelocity of shortening only. It is suggested that
975

E. I1. SONNENBLICK, E. 3RAUNWALD, AND A. G. MORROW
the contractile state of the myocardium can bedescribed by the force-velocity relation.An analysis of the series elastic component of
the muscle indicated that the series elastic com-
ponent was stretched an average of 8.4%o duringan isometric contraction, indicating that significantshortening of contractile elements occurs even inthe absence of external muscle shortening. Whenthe frequency of contraction was increased, theduration of contraction diminished, but the veloc-ity of shortening increased reciprocally. The re-
sultant force developed, or extent of shortening,remained relatively unchanged. Thus, at any
given muscle length, the improved contractilestate of the muscle resulting from increasing thefrequency of contraction was reflected by theaugmented power developed by the muscle, butwas not evident in the external work performed.
These studies on the contractile properties ofpapillary muscles provide a framework for an
analysis of the performance of the intact humanmyocardium in terms of fundamental musclemechanics.
References1. Hill, A. V. The heat of shortening and the dynamic
constants of muscle. Proc. roy. Soc. B 1938, 126,136.
2. Wilkie, D. R. Mechanical properties of muscle.Brit. med. Bull. 1956, 12, 174.
3. Jewell, B. R., and D. R. Wilkie. The mechanicalproperties of relaxing muscle. J. Physiol. (Lond.)1962, 152, 30.
4. Podolsky, R. J. Mechanochemical basis of muscularcontraction. Fed. Proc. 1962, 21, 964.
5. Hill, A. V. The effect of load on the heat of shorten-ing of muscle. Proc. roy. Soc. B 1964, 159, 297.
6. Abbott, B. C., and W. F. H. M. Mommaerts. A studyof inotropic mechanisms in the papillary musclepreparation. J. gen. Physiol. 1959, 42, 533.
7. Sonnenblick, E. H. Force-velocity relations in mam-malian heart muscle. Amer. J. Physiol. 1962, 202,931.
8. Sonnenblick, E. H. Implications of muscle mechanicsin heart muscle. Fed. Proc. 1962, 21, 975.
9. Sonnenblick, E. H., and S. E. Downing. Afterloadas a primary determinant of ventricular perform-ance. Amer. J. Physiol. 1963, 204, 604.
10. Levine, H. J., and N. A. Britman. Force-velocityrelations in the intact dog heart. J. clin. Invest.1964, 43, 1383.
11. Fry, D. L., D. M. Griggs, Jr., and J. C. Greenfield,Jr. Myocardial mechanics; tension-velocity-length
relationships of heart muscle. Circulat. Res. 1964,14, 73.
12. Downing, S. E., and E. H. Sonnenblick. Cardiacmuscle mechanics and ventricular performance:force and time parameters. Amer. J. Physiol. 1964,207, 705.
13. Gorlin, R., E. L. Rolett, P. M. Yurchak, W. C. El-liott, F. J. Lane, and R. H. Levy. Left ventricu-lar volume in man measured by thermodilution.J. clin. Invest. 1964, 43, 1203.'
14. Sonnenblick, E. H., G. Glick, A. G. Morrow, andE. Branuwald. Force-velocity relations in thehuman heart (abstract). J. clin. Invest. 1964, 43,1245.
15. Glick, G., E. H. Sonnenblick, J. F. Williams, Jr., andE. Braunwald. Effects of exercise performed atconstant heart rate on myocardial force-velocityrelations and ventricular dimensions in intact un-anesthetized man (abstract). Circulation 1964, 30(suppl. 3), 85.
16. Glick, G., E. H. Sonnenblick, and E. Braunwald.Myocardial force-velocity relations studied in in-tact unanesthetized man. J. clin. Invest. 1965, 44,978.
17. Sonnenblick, E. H. Series elastic and contractileelements in heart muscle. Changes in musclelength. Amer. J. Physiol. 1964, 207, 1330.
18. Chidsey, C. A., E. Braunwald, and A. G. Morrow.Catecholamine excretion and cardiac stores ofnorepinephrine in congestive heart failure. Amer.J. Med., in press.
19. Chidsey, C. A., G. A. Kaiser, E. H. Sonnenblick,J. F. Spann, and E. Braunwald. Cardiac nor-epinephrine stores in experimental heart failurein the dog. J. clin. Invest. 1964, 43, 2386.
20. Aygen, M. M., and E. Braunwald. Studies on Star-ling's law of the heart. VIII. Mechanical proper-ties of human myocardium studied in vivo. Circu-lation 1962, 26, 516.
21. Ross, J., Jr., and E. Braunwald. The study of leftventricular function in man by increasing resistanceto ventricular ejection with angiotensin. Circula-tion 1964, 29, 739.
22. Ross, J., Jr., and E. Braunwald. Studies on Starling'slaw of the heart IX: The effects of impeding ve-nous return on performance of the normal andfailing human left ventricle. Circulation 1964, 30,719.
23. Mitchell, J. H., A. G. Wallace, and N. S. Skinner, Jr.Intrinsic effects of heart rate on left ventricularperformance. Amer. J. Physiol. 1963, 205, 41.
24. Kruta, V., and P. Braveny. Differences physio-logiques entre le myocarde du rat et de certainsautres mammiferes. J. Physiol. (Paris) 1960, 52,137.
25. Hajdu, S., and E. Leonard. The cellular basis ofcardiac glycoside action. Pharmacol. Rev. 1959,11, 173.
9;76

MECHANICS OF HUMAN HEART MUSCLE
26. Koch-Weser, J., and J. R. Blinks. The influence ofthe interval between beats on myocardial con-
tractility. Pharmacol. Rev. 1963, 15, 601.27. Bowditch, H. P. 'Ober die Eigenthumlichkeiten der
Reizbarkeit, welche die Muskelfasern des Herzenszeigen. Ber. siichs. ges. (Akad.) Wiss. 1871, 652.
28. Braunwald, E., S. J. Sarnoff, and W. N. Stainsby.Determinants of duration and mean rate of ven-
tricular ejection. Circulat. Res. 1958, 6, 319.
29. Ross, J., Jr., J. W. Linhart, and E. Braunwald.Effects of altering heart rate by electrical stimu-lation of the right atrium in man: studies at rest,during muscular exercise, and isoproterenol infu-sion. Circulation, in press.
30. Britman, N. A., and H. J. Levine. Contractile ele-ment work: a major determinant of myocardialoxygen consumption. J. clin. Invest. 1964, 43,1397.
977