The complexity of intestinal permeability: Assigning the correct BCS classification through careful...
7
The complexity of intestinal permeability: Assigning the correct BCS classification through careful data interpretation Moran Zur, Allison S. Hanson, Arik Dahan ⇑ Department of Clinical Pharmacology, School of Pharmacy, Faculty of Health Sciences, Ben-Gurion University of the Negev, Beer-Sheva 84105, Israel article info Article history: Received 14 July 2013 Received in revised form 24 October 2013 Accepted 8 November 2013 Available online xxxx Keywords: BCS classification Biowaiver Intestinal absorption Drug solubility Segmental-dependent permeability abstract While the solubility parameter is fairly straightforward when assigning BCS classification, the intestinal permeability (P eff ) is more complex than generally recognized. In this paper we emphasize this complex- ity through the analysis of codeine, a commonly used antitussive/analgesic drug. Codeine was previously classified as a low-permeability compound, based on its lower Log P compared to metoprolol, a marker for the low–high permeability class boundary. In contrast, high fraction of dose absorbed (F abs ) was reported for codeine, which challenges the generally recognized P eff –F abs correlation. The purpose of this study was to clarify this ambiguity through elucidation of codeine’s BCS solubility/permeability class membership. Codeine’s BCS solubility class was determined, and its intestinal permeability throughout the small intes- tine was investigated, both in vitro and in vivo in rats. Codeine was found to be unequivocally a high-sol- ubility compound. All in vitro studies indicated that codeine’s permeability is higher than metoprolol’s. In vivo studies in rats showed similar permeability for both drugs throughout the entire small-intestine. In conclusion, codeine was found to be a BCS Class I compound. No P eff –F abs discrepancy is involved in its absorption; rather, it reflects the risk of assigning BCS classification based on merely limited physico- chemical characteristics. A thorough investigation using multiple experimental methods is prudent before assigning a BCS classification, to avoid misjudgment in various settings, e.g., drug discovery, for- mulation design, drug development and regulation. Ó 2013 Elsevier B.V. All rights reserved. 1. Introduction Amidon et al. (1995) revealed that the two fundamental param- eters controlling the rate and extent of drug absorption following oral administration are the permeability of the drug through the gastrointestinal (GI) membrane and the solubility/dissolution of the drug dose in the GI milieu, and developed the Biopharmaceu- tics Classification System (BCS). Based on this work, the FDA initi- ated the guidance for waiver of in vivo bioequivalence (BE) studies of immediate-release (IR) solid dosage forms for BCS Class I drugs (high-solubility and high-permeability) when formulated as rap- idly dissolved product (CDER/FDA, 2000). This initiative allowed to assure BE based on an in vitro dissolution test that provides a mechanistic proof for the continuing quality of the innovative and the generic products, rather than empirical in vivo human studies (Amidon et al., 1995, 2011; Dahan et al., 2009a; Lobenberg and Amidon, 2000; Martinez and Amidon, 2002; Yu et al., 2002). The solubility parameter is fairly straightforward when assign- ing a BCS classification. A drug is considered high-solubility when the highest dose strength is soluble in 250 mL or less of water over the pH range of 1–7.5 (CDER/FDA, 2000). These studies are fairly easy to perform, and in general most scientists agree when classi- fying a given drug as either high or low-solubility compound. How- ever, intestinal permeability is not routinely measured, and difficulties to prove high-permeability classification may limit the broad regulatory application of the BCS-based biowaiver concept. In this paper we emphasize the complexity behind and the care that must be taken with assigning a BCS permeability class. Human intestinal permeability (HIP), considering the whole of the human intestine, is more complex than generally recognized, and this can lead to misjudgment regarding F abs and P eff in various settings, e.g. drug discovery and development, formulation design, and drug regulation (Dahan et al., 2012, 2010a; Di et al., 2012; Lennernäs, 1998, 2007). Codeine is a commonly used antitussive/analgesic drug, either as a single active ingredient or in combination products. The loga- rithm of the partition coefficient between octanol and water of the unionized form of codeine (Log P) is 1.1 (Meylan and Howard, 1995). For comparison, the b-blocker metoprolol, which is the FDA marker for the low–high permeability class boundary, has a Log P value of 2.2 (Henchoz et al., 2009). Based on its lower Log P compared to metoprolol, codeine was previously classified as a low-permeability compound (Kasim et al., 2004; Lindenberg 0928-0987/$ - see front matter Ó 2013 Elsevier B.V. All rights reserved. http://dx.doi.org/10.1016/j.ejps.2013.11.007 ⇑ Corresponding author. Tel.: +972 8 6479483. E-mail address: [email protected] (A. Dahan). European Journal of Pharmaceutical Sciences xxx (2013) xxx–xxx Contents lists available at ScienceDirect European Journal of Pharmaceutical Sciences journal homepage: www.elsevier.com/locate/ejps Please cite this article in press as: Zur, M., et al. The complexity of intestinal permeability: Assigning the correct BCS classification through careful data interpretation. Eur. J. Pharm. Sci. (2013), http://dx.doi.org/10.1016/j.ejps.2013.11.007
Transcript of The complexity of intestinal permeability: Assigning the correct BCS classification through careful...

European Journal of Pharmaceutical Sciences xxx (2013) xxx–xxx
Contents lists available at ScienceDirect
European Journal of Pharmaceutical Sciences
journal homepage: www.elsevier .com/ locate/e jps
The complexity of intestinal permeability: Assigning the correctBCS classification through careful data interpretation
0928-0987/$ - see front matter � 2013 Elsevier B.V. All rights reserved.http://dx.doi.org/10.1016/j.ejps.2013.11.007
⇑ Corresponding author. Tel.: +972 8 6479483.E-mail address: [email protected] (A. Dahan).
Please cite this article in press as: Zur, M., et al. The complexity of intestinal permeability: Assigning the correct BCS classification through carefinterpretation. Eur. J. Pharm. Sci. (2013), http://dx.doi.org/10.1016/j.ejps.2013.11.007
Moran Zur, Allison S. Hanson, Arik Dahan ⇑Department of Clinical Pharmacology, School of Pharmacy, Faculty of Health Sciences, Ben-Gurion University of the Negev, Beer-Sheva 84105, Israel
a r t i c l e i n f o
Article history:Received 14 July 2013Received in revised form 24 October 2013Accepted 8 November 2013Available online xxxx
Keywords:BCS classificationBiowaiverIntestinal absorptionDrug solubilitySegmental-dependent permeability
a b s t r a c t
While the solubility parameter is fairly straightforward when assigning BCS classification, the intestinalpermeability (Peff) is more complex than generally recognized. In this paper we emphasize this complex-ity through the analysis of codeine, a commonly used antitussive/analgesic drug. Codeine was previouslyclassified as a low-permeability compound, based on its lower LogP compared to metoprolol, a marker forthe low–high permeability class boundary. In contrast, high fraction of dose absorbed (Fabs) was reportedfor codeine, which challenges the generally recognized Peff–Fabs correlation. The purpose of this study wasto clarify this ambiguity through elucidation of codeine’s BCS solubility/permeability class membership.Codeine’s BCS solubility class was determined, and its intestinal permeability throughout the small intes-tine was investigated, both in vitro and in vivo in rats. Codeine was found to be unequivocally a high-sol-ubility compound. All in vitro studies indicated that codeine’s permeability is higher than metoprolol’s. Invivo studies in rats showed similar permeability for both drugs throughout the entire small-intestine. Inconclusion, codeine was found to be a BCS Class I compound. No Peff–Fabs discrepancy is involved in itsabsorption; rather, it reflects the risk of assigning BCS classification based on merely limited physico-chemical characteristics. A thorough investigation using multiple experimental methods is prudentbefore assigning a BCS classification, to avoid misjudgment in various settings, e.g., drug discovery, for-mulation design, drug development and regulation.
� 2013 Elsevier B.V. All rights reserved.
1. Introduction
Amidon et al. (1995) revealed that the two fundamental param-eters controlling the rate and extent of drug absorption followingoral administration are the permeability of the drug through thegastrointestinal (GI) membrane and the solubility/dissolution ofthe drug dose in the GI milieu, and developed the Biopharmaceu-tics Classification System (BCS). Based on this work, the FDA initi-ated the guidance for waiver of in vivo bioequivalence (BE) studiesof immediate-release (IR) solid dosage forms for BCS Class I drugs(high-solubility and high-permeability) when formulated as rap-idly dissolved product (CDER/FDA, 2000). This initiative allowedto assure BE based on an in vitro dissolution test that provides amechanistic proof for the continuing quality of the innovativeand the generic products, rather than empirical in vivo humanstudies (Amidon et al., 1995, 2011; Dahan et al., 2009a; Lobenbergand Amidon, 2000; Martinez and Amidon, 2002; Yu et al., 2002).
The solubility parameter is fairly straightforward when assign-ing a BCS classification. A drug is considered high-solubility whenthe highest dose strength is soluble in 250 mL or less of water over
the pH range of 1–7.5 (CDER/FDA, 2000). These studies are fairlyeasy to perform, and in general most scientists agree when classi-fying a given drug as either high or low-solubility compound. How-ever, intestinal permeability is not routinely measured, anddifficulties to prove high-permeability classification may limitthe broad regulatory application of the BCS-based biowaiverconcept.
In this paper we emphasize the complexity behind and the carethat must be taken with assigning a BCS permeability class. Humanintestinal permeability (HIP), considering the whole of the humanintestine, is more complex than generally recognized, and this canlead to misjudgment regarding Fabs and Peff in various settings, e.g.drug discovery and development, formulation design, and drugregulation (Dahan et al., 2012, 2010a; Di et al., 2012; Lennernäs,1998, 2007).
Codeine is a commonly used antitussive/analgesic drug, eitheras a single active ingredient or in combination products. The loga-rithm of the partition coefficient between octanol and water of theunionized form of codeine (LogP) is 1.1 (Meylan and Howard,1995). For comparison, the b-blocker metoprolol, which is theFDA marker for the low–high permeability class boundary, has aLogP value of 2.2 (Henchoz et al., 2009). Based on its lower LogPcompared to metoprolol, codeine was previously classified as alow-permeability compound (Kasim et al., 2004; Lindenberg
ul data

2 M. Zur et al. / European Journal of Pharmaceutical Sciences xxx (2013) xxx–xxx
et al., 2004; Ramirez et al., 2010; Takagi et al., 2006). On the otherhand, codeine’s human fraction of dose absorbed (Fabs) was re-ported to be high (>90%) based on cumulative urinary excretionof drug-related material (chiefly codeine-6-glucuronide) followingoral administration (Bodd et al., 1987; Quiding et al., 1986; Skolniket al., 2010; Vree and Wissen, 1992; Yalkowsky et al., 2006; Zhaoet al., 2001). It is generally recognized that a high Fabs drug will ex-hibit high Peff in the human intestine, even though actual perme-ability data may not be available. The intestinal absorption ofcodeine, hence, allegedly represents a case of discrepancy betweenPeff and Fabs. This directly affects its BCS classification, which inturns dictates whether a generic immediate-release (IR) oral drugproduct containing this active ingredient may be eligible for aBCS-based biowaiver, a question of high scientific and financialimportance, that involves public health policy aspects as well(Amidon et al., 2011; Dahan et al., 2012, 2009a; Polli et al., 2008).
The purpose of this study was to elucidate the underlyingmechanisms behind the confusion in codeine’s BCS classification.We have determined the solubility class of codeine, and thoroughlyinvestigated its intestinal permeability, both in vitro and in vivo inrats, taking into consideration the complexity of the whole of thesmall intestine. The results were compared to metoprolol, theFDA reference drug for the low/high permeability class boundary.Overall, this study highlights the risk of assigning BCS classificationbased on limited physicochemical characteristics, and the merit ofusing multiple experimental methods to avoid misjudgment in BCSclassification.
2. Materials and methods
2.1. Materials
Codeine phosphate was generously donated by Rekah Pharma-ceutical Industry Ltd. (Holon, Israel). Metoprolol tartrate, phenolred, potassium chloride, potassium phosphate monobasic, sodiumchloride, octanol, hexadecane, and trifluoroacetic acid (TFA) werepurchased from Sigma Chemical Co. (St. Louis, MO). Acetonitrile,methanol and water (Merck KGaA, Darmstadt, Germany) wereUPLC grade. All other chemicals were of analytical reagent grade.
2.2. Solubility studies
The solubility class membership of codeine was determinedusing the shake-flask method (Miller et al., 2012a,b, 2011). Taking30 mg as the highest oral dose strength of an immediate-release(IR) codeine product, the minimal solubility to allow high-solubil-ity definition was calculated using the equation: D0 = M/V0/Cs
where the dose number (D0) was set at 1.0, M is the dose(30 mg), and the initial volume of water (V0) was set to be250 mL (CDER/FDA, 2000; Dahan and Amidon, 2009b; Dahanet al., 2009a). The minimal solubility value to allow high-solubilitydefinition for codeine was found to be 120 lg/mL. Tightly closedglass vials with 120 lg/mL, as well as 10-, 100- and 1000-fold high-er codeine concentrations (1.2, 12 and 120 mg/mL respectively)were placed at 37 �C and 100 rpm in triplicates. This procedurewas replicated in phosphate buffer pH 7.5, acetate buffer pH 4.5,and maleate buffer pH 1.0. Solubilization was monitored visually,followed by UPLC analysis.
2.3. Octanol-buffer partition coefficient studies
Experimental octanol-buffer partition coefficients, LogD, forcodeine and metoprolol at pH 6.5, 7.0 and 7.5 were determinedusing the traditional shake-flask method (Dahan et al., 2010a;Miller et al., 2010). Briefly, drug solutions were prepared in octanol
Please cite this article in press as: Zur, M., et al. The complexity of intestinal pinterpretation. Eur. J. Pharm. Sci. (2013), http://dx.doi.org/10.1016/j.ejps.2013.
saturated phosphate buffers with pH values of 6.5, 7.0 and 7.5.These aqueous solutions were equilibrated at room temperaturewith an equivalent volume of buffer saturated octanol for 48 h.The octanol and aqueous phases were then separated by centrifu-gation, and the drug concentration in the aqueous phase wasdetermined by UPLC. The drug concentration in the octanol phasewas obtained by mass balance. From these data, the apparent oct-anol/buffer partition coefficient was determined.
2.4. Parallel Artificial Membrane Permeability Assay (PAMPA)
Two different methods were used to determine the permeabil-ity of codeine and metoprolol through artificial membrane: thehexadecane-based PAMPA and the Pre-coated PAMPA assay (BDGentest™).
The hexadecane-based PAMPA studies were carried out as pre-viously described with minor modifications (Beig et al., 2012; Da-han et al., 2010b; Wohnsland and Faller, 2001). Briefly, three drugsolutions were prepared with different ratios of potassium phos-phate monobasic and sodium phosphate dibasic, to give pH valuesof 6.5, 7.0 and 7.5. Osmolality (290 mOsm/L) and ionic strengthwere similar in all buffers. Millipore (Danvers, MA) 96-well Multi-Screen-Permeability filter plates with 0.3 cm2 polycarbonate filtersupport (0.45 lm) were impregnated with 15 lL of a 5% hexadec-ane in hexane solution, and were then allowed to dry for 1 h, dur-ing which the hexane was completely evaporated resulting in auniform layer of hexadecane. Then, the donor wells were filledwith the different drug solutions (250 lL), the receiver wells werefilled with a matched blank buffer (300 lL), and the PAMPA sand-wich was incubated at room temperature. Receiver plates werecollected hourly for 4 h.
The Pre-coated PAMPA experiments (BD Gentest™, BD Biosci-ences, Bedford, MA) were carried out according to the manufac-turer instructions, with the addition of tracking the transportrate, as described for the hexadecane-based PAMPA. Receiverplates were collected hourly for 5 h.
Apparent permeability coefficient (Papp) values for both PAMPAmethods were calculated from the linear plot of drug accumulatedin the acceptor side vs. time using the equation:
Papp ¼dQ=dtA � C0
where dQ/dt is the steady-state appearance rate of drug on the re-ceiver side, C0 is the initial concentration of the drug in the donorside, and A is the membrane surface area (0.048 cm2). Linear regres-sion was carried out to obtain the steady-state appearance rate ofthe drugs on the receiver side.
2.5. Physicochemical analysis
The theoretical fraction extracted into octanol (fe) was calcu-lated using the following equation from Winne (1977) and Wagnerand Sedman (1973):
fe ¼fuP
1þ fuP
where P is the octanol–water partition coefficient of the unionizedform of the drug and fu is the fraction unionized of the drug at a gi-ven pH. Literature experimental LogP values of 1.14 for codeine(Meylan and Howard, 1995) and 2.2 for metoprolol (Henchozet al., 2009) were used. The fu vs. pH was plotted according to theHenderson–Hasselbalch equation, using the following literaturepKa values: 8.2 for codeine (Fuguet et al., 2008) and 9.68 for meto-prolol (Teksin et al., 2006).
ermeability: Assigning the correct BCS classification through careful data11.007

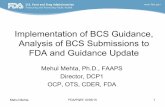
Fig. 1. The octanol–buffer partition coefficients, LogD, for codeine and metoprololat the three pH values 6.5, 7.0 and 7.5. Mean ± S.D.; n = 3 in each experimentalgroup.
M. Zur et al. / European Journal of Pharmaceutical Sciences xxx (2013) xxx–xxx 3
2.6. Rat intestinal perfusion studies
The in vivo effective permeability coefficient (Peff) of codeine vs.metoprolol was determined using the single-pass rat intestinalperfusion model. All animal experiments were conducted usingprotocols approved by Ben-Gurion University of the Negev AnimalUse and Care Committee (Protocol IL-60-11-2010). The animals(male Wistar rats weighing 230–260 g, Harlan, Israel) were housedand handled according to Ben-Gurion University of the Negev Unitfor Laboratory Animal Medicine Guidelines.
The experimental procedure followed previous reports (Dahanand Amidon, 2009a,c; Dahan et al., 2009b). Briefly, anesthetizedrats were placed on a 37 �C surface (Harvard Apparatus Inc., Holl-iston, MA), and a midline abdominal incision of 3 cm was made. Toaccount for the complexity of the whole of the small intestine, per-meability was determined in three different 10 cm segments; aproximal jejunal segment (starting 2 cm below the ligament of Tre-itz), mid-small intestinal segment (isolated between the end of theupper and the beginning of the lower segments), and a distal ilealsegment (ending 2 cm above the cecum) (Dahan and Amidon,2009b; Dahan et al., 2009c). Each intestinal segment was cannulat-ed on two ends, and was rinsed with blank perfusion buffer. Allsolutions were incubated in a 37 �C water bath.
Three perfusion buffers containing codeine, metoprolol andphenol red (a non-absorbable marker for water flux measure-ments) were prepared with different ratios of potassium phos-phate monobasic and sodium phosphate dibasic, to give pHvalues of 6.5, 7.0 and 7.5, while maintaining similar osmolarity(290 mOsm/L) and ionic strength in all buffers. The concentrationsof codeine and metoprolol in the perfusion buffers were 120 and400 lg/mL respectively, to represent the maximal dose of thedrugs (30 and 100 mg respectively) in 250 mL. The permeabilityin each intestinal segment was measured at the pH that corre-sponds to the physiological pH of that region: (1) proximal jeju-num, pH 6.5; (2) mid-small intestine, pH 7.0; and (3) distalileum, pH 7.5 (Dahan et al., 2010a; Mudie et al., 2010). The perfu-sion buffer was first perfused for 1 h, to ensure steady state condi-tions, followed by additional 1 h of perfusion with samples takenevery 10 min. The pH of the collected samples was measured atthe outlet, to verify that there was no pH change throughout theperfusion. All samples were immediately assayed by UPLC. At theend of the experiment, the length of each perfused intestinal seg-ment was accurately measured.
The effective permeability (Peff; cm/s) through the rat gut wallwas determined according to the following equation:
Peff ¼�QlnðC 0out=C 0inÞ
2pRL
where Q is the perfusion buffer flow rate (0.2 mL/min), C0out=C0in isthe ratio of the outlet and the inlet concentration of drug that hasbeen adjusted for water transport (Dahan and Amidon, 2010; Dahanand Miller, 2012), R is the radius of the intestinal segment (set to0.2 cm), and L is the length of the perfused intestinal segment.
2.7. Ultra Performance Liquid Chromatography (UPLC)
UPLC assays were performed on a Waters (Milford, MA) AcquityUPLC H-Class system equipped with photodiode array detector andEmpower software. Codeine, metoprolol and phenol red were as-sayed simultaneously using a Waters (Milford, MA) Acquity UPLCBEH C18 1.7 lm 2.1 � 100 mm column. The mobile phase consistedof 90:10 going to 20:80 (v/v) water:acetonitrile (both with 0.1%TFA) over 5 min (flow rate 0.5 mL/min). The detection wavelengthsand retention times for codeine, metoprolol and phenol red were285, 275 and 285 nm, and 2.1, 2.6 and 3.0 min, respectively. Injec-tion volumes for all UPLC analyses ranged from 5 to 50 lL.
Please cite this article in press as: Zur, M., et al. The complexity of intestinal pinterpretation. Eur. J. Pharm. Sci. (2013), http://dx.doi.org/10.1016/j.ejps.2013.
2.8. Statistical analysis
Log D determinations were performed in triplicates. All otherin vitro experiments were n = 4, and all animal experiments weren = 6. Values are expressed as means ± standard deviation (S.D.).To determine statistically significant differences among the exper-imental groups, the nonparametric Kruskal–Wallis test was usedfor multiple comparisons, and the two-tailed nonparametricMann–Whitney U-test for two-group comparison where appropri-ate. A p value of less than 0.05 was termed significant.
3. Results
3.1. Solubility
The solubility of codeine in the three pH values 1.0, 4.5 and 7.5,at 37 �C, exceeded 120 mg/mL. This data indicate that codeine isunequivocally a high-solubility compound; taking 30 mg as thehighest oral dose strength of an immediate-release (IR) codeineproduct, a minimum equilibrium solubility value of 120 lg/mLwould lead to a dose number (D0) value of 1, and hence to high-sol-ubility classification. By showing solubility of more than 120 mg/mL across the requested pH range 1–7.5 (CDER/FDA, 2000), a D0
lower than 0.001 is indicated, and a BCS high-solubility class mem-bership can be clearly designated.
3.2. Octanol–buffer partition coefficients
The Log D values for codeine and metoprolol at the three pHvalues 6.5, 7.0 and 7.5, representing the conditions throughoutthe small intestine, are presented in Fig. 1. It can be seen that forboth drugs, a clear pH dependent octanol–water partition coeffi-cient was found across the investigated pH range, with higher par-titioning at higher pH. While the octanol–water partitioncoefficient of the unionized form, LogP, of metoprolol (2.2) is dou-ble that of codeine (1.14), the opposite was evident when lookingat the Log D values; metoprolol’s Log D values at pH 6.5–7.5 werenegative and ranged between �0.8 to �0.2, whereas Log D valuesof codeine at these pHs were positive and ranged between 0.25and 0.6.
ermeability: Assigning the correct BCS classification through careful data11.007

4 M. Zur et al. / European Journal of Pharmaceutical Sciences xxx (2013) xxx–xxx
3.3. PAMPA
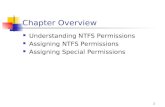
The accumulated amount transported vs. time plots of codeineand metoprolol in the hexadecane-based PAMPA and the Pre-coated PAMPA assay, at the three pH values 6.5, 7.0 and 7.5, arepresented in Figs. 2 and 3, respectively. The corresponding perme-ability values (Papp, cm/s) are plotted in Figs. 2 and 3 as well. It canbe seen that the results obtained from both systems were similar,indicating that codeine’s permeability is higher than metoprolol’s.The permeability of codeine and metoprolol through both artificialmembranes were pH-dependent at the investigated pH range, withhigher permeability at higher pH. Moreover, in both PAMPA sys-tems, the lowest permeability measured for codeine (i.e. at pH6.5) was higher than the highest permeability measured for meto-prolol (i.e. at pH 7.5). These results are in excellent agreement withthe octanol-buffer partition coefficients (Log D) data presented inFig. 1.
3.4. Physicochemical analysis
The theoretical fraction unionized (fu) and fraction extractedinto octanol (fe) plots as a function of pH for codeine and metopro-lol are presented in Fig. 4. The physicochemical properties used forthese analyses are summarized in Table 1. The fu of the basic com-pounds codeine and metoprolol is nil at low pH, and increases asthe pH rises, resulting in the classic sigmoidal shape. For bothdrugs, the fe vs. pH plot follows a similar pattern, but with a shiftto the left (lower pH values). The shift magnitude equals toLog(P�1) at the midpoint of the fe and fu sigmoidal curves (Wagnerand Sedman, 1973; Winne, 1977). Metoprolol has significantlyhigher LogP value than that of codeine, however, codeine has sig-nificantly lower pKa than that of metoprolol (Table 1). As a result,the rise in the fe of both drugs occurs at the same pH range, approx-imately between 6 and 8. Experimental octanol–buffer partitioningof the drugs at the three pH values 6.5, 7.0 and 7.5 are also pre-sented in Fig. 4, and were in good agreement with the theoreticalplots.
3.5. Rat intestinal permeability
The in vivo effective permeability coefficient (Peff) values ofcodeine vs. metoprolol determined using the single-pass rat intes-tinal perfusion model, in the three small intestinal segments the
Fig. 2. The transport flux of codeine and metoprolol at the three pH values 6.5, 7.0 andgroup.
Please cite this article in press as: Zur, M., et al. The complexity of intestinal pinterpretation. Eur. J. Pharm. Sci. (2013), http://dx.doi.org/10.1016/j.ejps.2013.
proximal jejunum (pH 6.5), mid-small intestine (pH 7.0) and thedistal ileum (pH 7.5), are presented in Fig. 5. The in vivo intestinalpermeability of both drugs was found to be segmental/pH depen-dent, with higher permeability at higher pH, in accordance withthe Log D and the PAMPA results. Throughout the entire smallintestine, similar permeability was revealed for codeine andmetoprolol.
4. Discussion
Due to the similar underlying mechanism, LogP (or CLogP) hasbeen widely used as a surrogate for passive intestinal permeability(Kasim et al., 2004; Takagi et al., 2006; Winiwarter et al., 1998),and based on codeine’s lower LogP compared to metoprolol (1.1and 2.2, respectively), this commonly used antitussive/analgesicdrug was previously classified as a low-permeability compound(Kasim et al., 2004; Lindenberg et al., 2004; Ramirez et al., 2010;Takagi et al., 2006). However, according to all experimental meth-ods used in this study, codeine is a high-permeability drug. To-gether with its unequivocal high-solubility classification, theresults presented in this paper indicate that codeine is a BCS classI compound, and should be a candidate for biowaiver when formu-lated in an IR rapidly-dissolving drug product. This conclusion is incorroboration with the human intestinal absorption characteristicsof codeine; cumulative urinary excretion of drug-related material(chiefly codeine-6-glucuronide) following oral administrationcould account for more than 90% of codeine’s dose, indicating highFabs for this drug. Hence, no discrepancy between Peff and Fabs is in-volved in its absorption. Rather, it reflects the risk of assigning BCSclassification based on merely limited physicochemicalcharacteristics.
Although high-permeability was indicated for codeine by allexperimental methods used in this study, the agreement betweenthe in vitro experiments and the rat study, as well as the agreementbetween the two PAMPA systems, was not complete; while thein vitro methods indicated that codeine has significantly higherpermeability than metoprolol, the rat data showed similar perme-ability throughout the entire small intestine for both drugs. Theo-retically, involvement of efflux transporters in the intestinalabsorption of codeine could explain this in vitro in vivo disparity,however, this does not seem to be likely; the high-solubility to-gether with the high passive permeability revealed in the PAMPAstudies in this paper (Figs. 2 and 3) indicate that transporters
7.5 in the hexadecane-based PAMPA assay. Mean ± S.D.; n = 4 in each experimental
ermeability: Assigning the correct BCS classification through careful data11.007

Fig. 3. The transport flux of codeine and metoprolol at the three pH values 6.5, 7.0 and 7.5 in the Pre-Coated PAMPA experiments (BD Gentest™). Mean ± S.D.; n = 4 in eachexperimental group.
Fig. 4. The theoretical fraction unionized (fu) and fraction extracted into octanol (fe)plots as a function of pH for codeine and metoprolol, and experimental buffer–octanol partitioning of the drugs in the three pH values 6.5, 7.0 and 7.5 (n = 3).
M. Zur et al. / European Journal of Pharmaceutical Sciences xxx (2013) xxx–xxx 5
may play minimal role in the in vivo intestinal absorption processof codeine, that will be primarily dominated by its native high pas-sive permeability (Cao et al., 2005; Custodio et al., 2008; Dahan andAmidon, 2009b; Giacomini et al., 2010). Moreover, codeine’s Caco-2 permeability was reported to be similar in the apical-to-basolat-eral and the basolateral-to-apical directions (Skolnik et al., 2010),indicating passive absorption as the primary transport mechanism.Also, similar oral vs. rectal absorption was reported for codeine,
Table 1Codeine and metoprolol physicochemical properties used for the fraction unionized (fu) a
Chemical structure pKa
Codeine8.2 Fuguet
Metoprolol9.68 Teksi
Please cite this article in press as: Zur, M., et al. The complexity of intestinal pinterpretation. Eur. J. Pharm. Sci. (2013), http://dx.doi.org/10.1016/j.ejps.2013.
further suggesting passive permeability as the primary absorptionmechanism (Moolenaar et al., 1983). Hence, differences betweenmethods are more likely to be responsible for the discrepancy be-tween the in vitro and the in vivo results reported in this paper.Skolnik et al. reported the in vitro permeability across Caco-2 cellmonolayers for codeine and metoprolol to be 22.9 � 10�6 and17.7 � 10�6 cm/s, respectively. Not only this agrees with thehigh-permeability classification indicated in this paper, it also cor-roborates our in vivo rats data that showed similar intestinal per-meability for codeine and metoprolol (Fig. 5).
When comparing the results obtained from the two PAMPA sys-tems, it seems that the structured layers of phospholipids serve asthe artificial membrane in the Pre-Coated PAMPA were able to cap-ture better the relatively small differences between codeine andmetoprolol at each given pH. On the other hand, the hexadecanePAMPA captured better the significant difference between the dif-ferent pH values. This highlights both the limitation of an artificialmembrane to predict the in vivo situation, and the merit of usingmultiple experimental methods.
An additional matter highlighted by this study is the impor-tance of regional differences in intestinal absorption (Bergstrandet al., 2012; Fairstein et al., 2013; Lennernäs, 2013; Sjöberg et al.,2013; Sjögren et al., 2013). In corroboration with the alkaline nat-ure of both codeine and metoprolol, the data presented in this pa-per indicate significant regional/pH-dependent absorption alongthe small intestine for these drugs, with higher permeability athigher pH (and more distal small intestinal regions). While in the
nd fraction extracted into octanol (fe) analyses.
LogP
et al. (2008) 1.14 Meylan and Howard (1995))
n et al. (2006) 2.2 Henchoz et al. (2009)
ermeability: Assigning the correct BCS classification through careful data11.007

Fig. 5. Effective permeability values (Peff, cm/s) obtained for codeine and meto-prolol after in situ single pass perfusion to the rat proximal jejunum at pH 6.5, mid-small intestine at pH 7.0, and to the distal ileum at pH 7.5. Mean ± S.D.; n = 6 in eachexperimental group.
6 M. Zur et al. / European Journal of Pharmaceutical Sciences xxx (2013) xxx–xxx
solubility classification there is an explicit recognition of thechanges in this parameter along the GI tract, demonstrated in therequirement to show that the drug dose is dissolved in 250 mL ofaqueous media in all luminal conditions, that is pH 1–7.5 (CDER/FDA, 2000), the permeability classification does not consider thechanges along the intestine and requires only the value in the jeju-num. This policy misses the complexity behind the permeabilitymeasure, considering the whole of the intestine; permeability islocation-dependent, and pertaining to each point throughout theGI tract. In fact, even the Peff values we report for the different seg-ment, proximal jejunum, mid-small intestine, and distal ileum, areaverage values; these values were calculated based on perfusionthrough a 10 cm intestinal segment, during which the permeabilitymay locally change at any point, and hence the overall value repre-sents the average permeability in this 10 cm segment. Within a10 cm intestinal segment with approximately similar characteris-tics the local Peff changes may be small, but when consideringthe many parameters that vary significantly from one region to an-other throughout the entire intestine, looking merely at one seg-ment can lead to misjudgment regarding Peff and Fabs in varioussettings.
In 2005, Wu and Benet have noticed that the high-permeabilityBCS class I and II drugs are eliminated by extensive metabolism(presumably having ready access to metabolizing enzymes withinthe hepatocytes), and observed that there may be a good correla-tion between the extent of drug metabolism and the permeabilityas defined in the BCS (Wu and Benet, 2005). This biopharmaceuticsdrug disposition classification system (BDDCS) suggested that ifthe major route of elimination of a given drug is metabolism, thenthe drug is high-permeable, and if the major route of elimination isrenal and biliary excretion of unchanged drug, then that drugshould be classified as low-permeability (Benet et al., 2008;Broccatelli et al., 2012; Custodio et al., 2008). With only �5% ofthe dose excreted unchanged in the urine, and �90% as metabo-lites, codeine is unequivocally an extensively metabolizedcompound, and is classified as Class I according to the BDDCS(Benet et al., 2011; Wu and Benet, 2005). Therefore, codeine is acase in which metabolism does a better job than LogP (or CLogP)in correctly assigning BCS permeability class. Again, this highlightsthe risk of assigning BCS classification based on limited physico-chemical characteristics, and the merit of using multiple experi-mental methods, e.g. Fabs data when available, intestinalperfusion studies, Caco-2 data, Ussing chambers experiments,PAMPA assay, and also metabolism information, before assigninga BCS classification.
Please cite this article in press as: Zur, M., et al. The complexity of intestinal pinterpretation. Eur. J. Pharm. Sci. (2013), http://dx.doi.org/10.1016/j.ejps.2013.
5. Conclusions
In conclusion, this study provides evidence to confirm that co-deine is a BCS Class I compound. No discrepancy between Peff
and Fabs is involved in its absorption, rather, it reflects the risk ofassigning a BCS classification based on merely limited physico-chemical characteristics. A thorough investigation using multipleexperimental methods is prudent before assigning a BCS classifica-tion, to avoid misjudgment in various settings, e.g., drug discovery,formulation design, drug development and regulation.
Acknowledgment
We thank Rekah Pharmaceutical Industry Ltd. (Holon, Israel) forthe generous donation of codeine.
References
Amidon, G.L., Lennernas, H., Shah, V.P., Crison, J.R., 1995. A theoretical basis for abiopharmaceutic drug classification: the correlation of in vitro drug productdissolution and in vivo bioavailability. Pharmaceutical Research 12, 413–420.
Amidon, K.S., Langguth, P., Lennernas, H., Yu, L., Amidon, G.L., 2011. Bioequivalenceof oral products and the biopharmaceutics classification system: science,regulation, and public policy. Clinical Pharmacology and Therapeutics 90, 467–470.
Beig, A., Miller, J.M., Dahan, A., 2012. Accounting for the solubility–permeabilityinterplay in oral formulation development for poor water solubility drugs: Theeffect of PEG-400 on carbamazepine absorption. European Journal ofPharmaceutics and Biopharmaceutics 81, 386–391.
Benet, L., Amidon, G.L., Barends, D., Lennernäs, H., Polli, J., Shah, V., Stavchansky, S.,Yu, L.X., 2008. The use of BDDCS in classifying the permeability of marketeddrugs. Pharmaceutical Research 25, 483–488.
Benet, L., Broccatelli, F., Oprea, T., 2011. BDDCS applied to over 900 drugs. The AAPSJournal 13, 519–547.
Bergstrand, M., Söderlind, E., Eriksson, U., Weitschies, W., Karlsson, M., 2012. ASemi-mechanistic modeling strategy for characterization of regional absorptionproperties and prospective prediction of plasma concentrations followingadministration of new modified release formulations. PharmaceuticalResearch 29, 574–584.
Bodd, E., Beylich, K.M., Christophersen, A.S., Mørland, J., 1987. Oral administration ofcodeine in the presence of ethanol: a pharmacokinetic study in man.Pharmacology and Toxicology 61, 297–300.
Broccatelli, F., Cruciani, G., Benet, L.Z., Oprea, T.I., 2012. BDDCS class prediction fornew molecular entities. Molecular Pharmaceutics 9, 570–580.
Cao, X., Yu, L.X., Barbaciru, C., Landowski, C.P., Shin, H.-C., Gibbs, S., Miller, H.A.,Amidon, G.L., Sun, D., 2005. Permeability dominates in vivo Intestinalabsorption of P-gp substrate with high solubility and high permeability.Molecular Pharmaceutics 2, 329–340.
CDER/FDA, 2000. Guidance for industry: Waiver of in vivo bioavailability andbioequivalence studies for immediate release dosage forms based on abiopharmaceutical slassification system. Center for Drug Evaluation andResearch.
Custodio, J.M., Wu, C.-Y., Benet, L.Z., 2008. Predicting drug disposition, absorption/elimination/transporter interplay and the role of food on drug absorption.Advanced Drug Delivery Reviews 60, 717–733.
Dahan, A., Amidon, G., 2009a. Grapefruit juice and its constituents augmentcolchicine intestinal absorption: potential hazardous interaction and the role ofP-gp. Pharmaceutical Research 26, 883–892.
Dahan, A., Amidon, G.L., 2009b. Segmental dependent transport of low permeabilitycompounds along the small intestine due to P-gp: the role of efflux transport inthe oral absorption of BCS class III drugs. Molecular Pharmaceutics 6, 19–28.
Dahan, A., Amidon, G.L., 2009c. Small intestinal efflux mediated by MRP2 and BCRPshifts sulfasalazine intestinal permeability from high to low, enabling its colonictargeting. American Journal of Physiology – Gastrointestinal and LiverPhysiology 297, G371–G377.
Dahan, A., Amidon, G.L., 2010. MRP2 mediated drug–drug interaction:Indomethacin increases sulfasalazine absorption in the small intestine,potentially decreasing its colonic targeting. International Journal ofPharmaceutics 386, 216–220.
Dahan, A., Miller, J., 2012. The solubility–permeability interplay and its implicationsin formulation design and development for poorly soluble drugs. The AAPSJournal 14, 244–251.
Dahan, A., Miller, J., Amidon, G.L., 2009a. Prediction of solubility and permeabilityclass membership: provisional BCS classification of the world’s top oral drugs.The AAPS Journal 11, 740–746.
Dahan, A., Sabit, H., Amidon, G.L., 2009b. Multiple efflux pumps are involved in thetransepithelial transport of colchicine: combined effect of P-gp and MRP2 leadsto decreased intestinal absorption throughout the entire small intestine. DrugMetabolism and Disposition 37, 2028–2036.
ermeability: Assigning the correct BCS classification through careful data11.007

M. Zur et al. / European Journal of Pharmaceutical Sciences xxx (2013) xxx–xxx 7
Dahan, A., West, B.T., Amidon, G.L., 2009c. Segmental-dependent membranepermeability along the intestine following oral drug administration:evaluation of a triple single-pass intestinal perfusion (TSPIP) approach in therat. European Journal of Pharmaceutical Sciences 36, 320–329.
Dahan, A., Miller, J.M., Hilfinger, J.M., Yamashita, S., Yu, L.X., Lennernäs, H., Amidon,G.L., 2010a. High-permeability criterion for BCS classification: segmental/pHdependent permeability considerations. Molecular Pharmaceutics 7, 1827–1834.
Dahan, A., Miller, J.M., Hoffman, A., Amidon, G.E., Amidon, G.L., 2010b. Thesolubility–permeability interplay in using cyclodextrins as pharmaceuticalsolubilizers: mechanistic modeling and application to progesterone. Journal ofPharmaceutical Sciences 99, 2739–2749.
Dahan, A., Lennernäs, H., Amidon, G.L., 2012. The fraction dose absorbed, in humans,and high jejunal human permeability relationship. Molecular Pharmaceutics 9,1847–1851.
Di, L., Artursson, P., Avdeef, A., Ecker, G.F., Faller, B., Fischer, H., Houston, J.B., Kansy,M., Kerns, E.H., Krämer, S.D., Lennernäs, H., Sugano, K., 2012. Evidence-basedapproach to assess passive diffusion and carrier-mediated drug transport. DrugDiscovery Today 17, 905–912.
Fairstein, M., Swissa, R., Dahan, A., 2013. Regional-dependent intestinalpermeability and BCS classification: elucidation of pH-related complexity inrats using pseudoephedrine. The AAPS Journal 15, 589–597.
Fuguet, E., Reta, M., Gibert, C., Rosés, M., Bosch, E., Ràfols, C., 2008. Criticalevaluation of buffering solutions for pKa determination by capillaryelectrophoresis. Electrophoresis 29, 2841–2851.
Giacomini, K., Huang, S., Tweedie, D., Benet, L., Brouwer, K., Chu, X., Dahlin, A., Evers,R., Fischer, V., Hillgren, K., Hoffmaster, K., Ishikawa, T., Keppler, D., Kim, R., Lee,C., Niemi, M., Polli, J., Sugiyama, Y., Swaan, P., Ware, J., Wright, S., Yee, S., Zamek-Gliszczynski, M., Zhang, L., 2010. Membrane transporters in drug development.Nature Reviews Drug Discovery 9, 215–236.
Henchoz, Y., Guillarme, D., Martel, S., Rudaz, S., Veuthey, J.-L., Carrupt, P.-A., 2009.Fast LogP determination by ultra-high-pressure liquid chromatography coupledwith UV and mass spectrometry detections. Analytical and BioanalyticalChemistry 394, 1919–1930.
Kasim, N.A., Whitehouse, M., Ramachandran, C., Bermejo, M., Lennernäs, H.,Hussain, A.S., Junginger, H.E., Stavchansky, S.A., Midha, K.K., Shah, V.P.,Amidon, G.L., 2004. Molecular properties of WHO essential drugs andprovisional biopharmaceutical classification. Molecular Pharmaceutics 1, 85–96.
Lennernäs, H., 1998. Human intestinal permeability. Journal of PharmaceuticalScinces 87, 403–410.
Lennernäs, H., 2007. Intestinal permeability and its relevance for absorption andelimination. Xenobiotica 37, 1015–1051.
Lennernäs, H., 2013. Regional intestinal drug permeation: Biopharmaceutics anddrug development. European Journal of Pharmaceutical Sciences (in press).
Lindenberg, M., Kopp, S., Dressman, J.B., 2004. Classification of orally administereddrugs on the World Health Organization model list of essential medicinesaccording to the biopharmaceutics classification system. European Journal ofPharmaceutics and Biopharmaceutics 58, 265–278.
Lobenberg, R., Amidon, G.L., 2000. Modern bioavailability, bioequivalence andbiopharmaceutics classification system. New scientific approaches tointernational regulatory standards. European Journal of Pharmaceutics andBiopharmaceutics 50, 3–12.
Martinez, M.N., Amidon, G.L., 2002. A mechanistic approach to understanding thefactors affecting drug absorption: a review of fundamentals. Journal of ClinicalPharmacology 42, 620–643.
Meylan, W.M., Howard, P.H., 1995. Atom/fragment contribution method forestimating octanol–water partition coefficients. Journal of PharmaceuticalSciences 84, 83–92.
Miller, J.M., Dahan, A., Gupta, D., Varghese, S., Amidon, G.L., 2010. Enabling theintestinal absorption of highly polar antiviral agents: Ion-pair facilitatedmembrane permeation of zanamivir heptyl ester and guanidino oseltamivir.Molecular Pharmaceutics 7, 1223–1234.
Miller, J.M., Beig, A., Krieg, B.J., Carr, R.A., Borchardt, T.B., Amidon, G.E., Amidon, G.L.,Dahan, A., 2011. The solubility–permeability interplay: mechanistic modelingand predictive application of the impact of micellar solubilization on intestinalpermeation. Molecular Pharmaceutics 8, 1848–1856.
Miller, J.M., Beig, A., Carr, R.A., Spence, J.K., Dahan, A., 2012a. A win–win solution inoral delivery of lipophilic drugs: Supersaturation via amorphous soliddispersions increases apparent solubility without sacrifice of intestinalmembrane permeability. Molecular Pharmaceutics 9, 2009–2016.
Please cite this article in press as: Zur, M., et al. The complexity of intestinal pinterpretation. Eur. J. Pharm. Sci. (2013), http://dx.doi.org/10.1016/j.ejps.2013.
Miller, J.M., Beig, A., Carr, R.A., Webster, G.K., Dahan, A., 2012b. The solubility–permeability interplay when using cosolvents for solubilization: revising theway we use solubility-enabling formulations. Molecular Pharmaceutics 9, 581–590.
Moolenaar, F., Grasmeijer, G., Visser, J., Meijer, D.K.F., 1983. Rectal versus oralabsorption of codeine phosphate in man. Biopharmaceutics & Drug Disposition4, 195–199.
Mudie, D.M., Amidon, G.L., Amidon, G.E., 2010. Physiological parameters for oraldelivery and in vitro testing. Molecular Pharmaceutics 7, 1388–1405.
Polli, J., Abrahamsson, B., Yu, L., Amidon, G., Baldoni, J., Cook, J., Fackler, P., Hartauer,K., Johnston, G., Krill, S., Lipper, R., Malick, W., Shah, V., Sun, D., Winkle, H., Wu,Y., Zhang, H., 2008. Summary workshop report: bioequivalence,biopharmaceutics classification system, and beyond. The AAPS Journal 10,373–379.
Quiding, H., Anderson, P., Bondesson, U., Boréus, L.O., Hynning, P.Å., 1986. Plasmaconcentrations of codeine and its metabolite, morphine, after single andrepeated oral administration. European Journal of Clinical Pharmacology 30,673–677.
Ramirez, E., Laosa, O., Guerra, P., Duque, B., Mosquera, B., Borobia, A.M., Lei, S.H.,Carcas, A.J., Frias, J., 2010. Acceptability and characteristics of 124 humanbioequivalence studies with active substances classified according to thebiopharmaceutic classification system. British Journal of ClinicalPharmacology 70, 694–702.
Sjöberg, Å., Lutz, M., Tannergren, C., Wingolf, C., Borde, A., Ungell, A.-L., 2013.Comprehensive study on regional human intestinal permeability and predictionof fraction absorbed of drugs using the Ussing chamber technique. EuropeanJournal of Pharmaceutical Sciences 48, 166–180.
Sjögren, E., Westergren, J., Grant, I., Hanisch, G., Lindfors, L., Lennernäs, H.,Abrahamsson, B., Tannergren, C., 2013. In silico predictions of gastrointestinaldrug absorption in pharmaceutical product development: Application of themechanistic absorption model GI-Sim. European Journal of PharmaceuticalSciences 49, 679–698.
Skolnik, S., Lin, X., Wang, J., Chen, X.-H., He, T., Zhang, B., 2010. Towards predictionof in vivo intestinal absorption using a 96-well Caco-2 assay. Journal ofPharmaceutical Sciences 99, 3246–3265.
Takagi, T., Ramachandran, C., Bermejo, M., Yamashita, S., Yu, L.X., Amidon, G.L.,2006. A provisional biopharmaceutical classification of the top 200 oral drugproducts in the United States, Great Britain, Spain, and Japan. MolecularPharmaceutics 3, 631–643.
Teksin, Z.S., Hom, K., Balakrishnan, A., Polli, J.E., 2006. Ion pair-mediated transport ofmetoprolol across a three lipid-component PAMPA system. Journal ofControlled Release 116, 50–57.
Vree, T.B., Wissen, C.P.W.G.M.V.-V., 1992. Pharmacokinetics and metabolism ofcodeine in humans. Biopharmaceutics & Drug Disposition 13, 445–460.
Wagner, J.G., Sedman, A.J., 1973. Quantitaton of rate of gastrointestinal and buccalabsorption of acidic and basic drugs based on extraction theory. Journal ofPharmacokinetics and Pharmacodynnamics 1, 23–50.
Winiwarter, S., Bonham, N.M., Ax, F., Hallberg, A., Lennernäs, H., Karlén, A., 1998.Correlation of human jejunal permeability (in vivo) of drugs withexperimentally and theoretically derived parameters. A multivariate dataanalysis approach. Journal of Medicinal Chemistry 41, 4939–4949.
Winne, D., 1977. Shift of pH-absorption curves. Journal of Pharmacokinetics andBiopharmaceutics 5, 53–94.
Wohnsland, F., Faller, B., 2001. High-throughput permeability pH profile and high-throughput alkane/water LogP with artificial membranes. Journal of MedicinalChemistry 44, 923–930.
Wu, C.-Y., Benet, L.Z., 2005. Predicting drug disposition via application of BCS:transport/absorption/elimination interplay and development of abiopharmaceutics drug disposition classification system. PharmaceuticalResearch 22, 11–23.
Yalkowsky, S.H., Johnson, J.L.H., Sanghvi, T., Machatha, S.G., 2006. A ‘rule of unity’ forhuman intestinal absorption. Pharmaceutical Research 23, 2475–2481.
Yu, L.X., Amidon, G.L., Polli, J.E., Zhao, H., Mehta, M.U., Conner, D.P., Shah, V.P., Lesko,L.J., Chen, M.L., Lee, V.H.L., Hussain, A.S., 2002. Biopharmaceutics classificationsystem: the scientific basis for biowaiver extensions. Pharmaceutical Research19, 921.
Zhao, Y.H., Le, J., Abraham, M.H., Hersey, A., Eddershaw, P.J., Luscombe, C.N., Boutina,D., Beck, G., Sherborne, B., Cooper, I., Platts, J.A., 2001. Evaluation of humanintestinal absorption data and subsequent derivation of a quantitativestructure–activity relationship (QSAR) with the Abraham descriptors. Journalof Pharmaceutical Sciences 90, 749–784.
ermeability: Assigning the correct BCS classification through careful data11.007