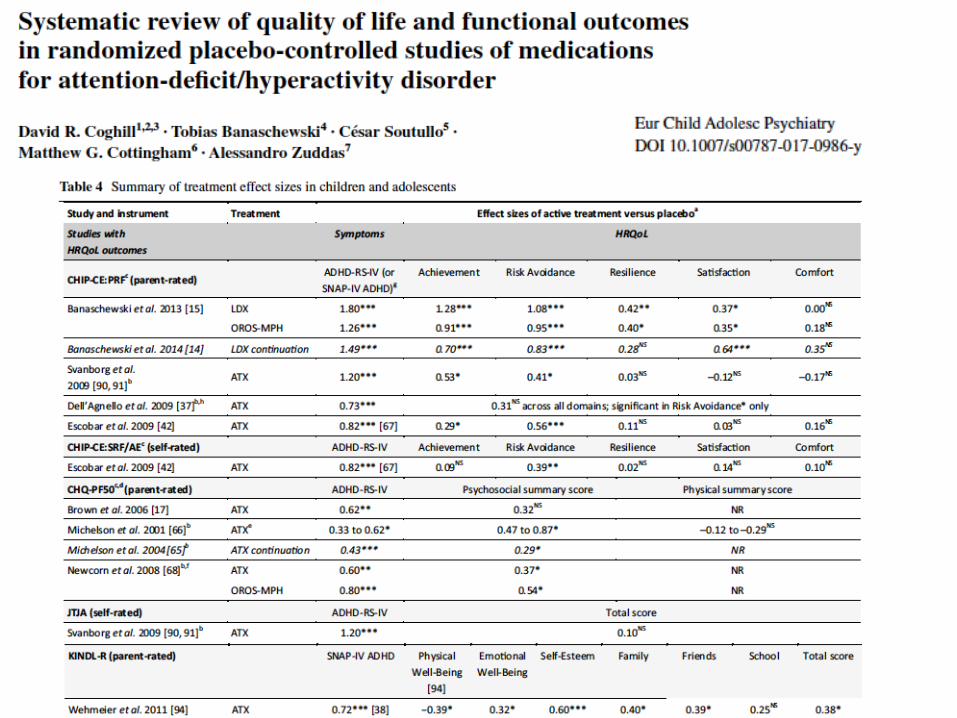
Cognitive Neuropsychiatry Varieties of confabulation and delusion
Alessandro ZuddasChild & Adolescent Neuropsychiatry
Department of Biomedical Sciences, University of Cagliari,
& “A Cao” Paediatric Hospital, “G. Brotzu” Hospital Trust
Cagliari, Italy
The Clinical Global Impression score:a widely used instrument in psychiatry
A discussion of Benedetto Vitiello presentation
AO Brotzu
Financial Disclosure (2013-2017)
Research grants• Shire• Vifor• Roche• Lundbeck• Janssen• EU 7 Framework Program (PERS, STOP, ADDUCE, MATRICS), • Assessorato Sanità Regione Sardegna
RoyaltiesGiunti.OS, Oxford University Press
Speaker or advisory relationship with: Angelini, Lilly, Astra Zeneca, Servier, Shire, Takeda, Vifor.
Member of Data Safety Monitory BoardsOtsuka, Lundbek,
European rules forapproval of new ADHD medications
The EMA has developed the only formal guideline on ADHD clinical trial design – Guideline on clinical investigation of medicinal products for the treatment of attention deficit hyperactivity disorder1
Recommendations include: Three-arm studies (inclusion of an active comparator)
Both symptomatic and functional efficacy outcomes
Measures of clinical response
Monitoring of treatment-emergent adverse events (TEAEs), vital signs, ECG parameters and suicidal ideation and behaviours
Evidence of the maintenance of effect which may be assessed via randomized withdrawal design
1. EMA, 2010. Available from: www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2010/08/WC500095686.pdf (Accessed 17 January 2014)ADHD, attention-deficit/hyperactivity disorder; EMA, European Medicines Agency
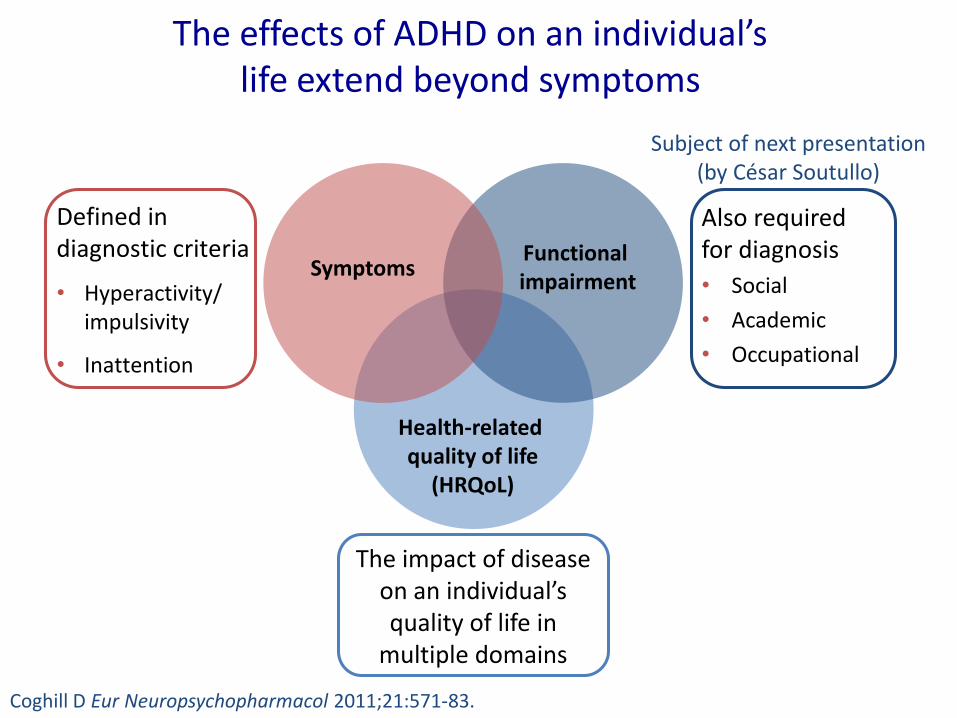
Defined in diagnostic criteria
• Hyperactivity/ impulsivity
• Inattention
The effects of ADHD on an individual’s life extend beyond symptoms
Functional impairment
Health-related quality of life
(HRQoL)
Also required for diagnosis
• Social
• Academic
• Occupational
Symptoms
The impact of disease on an individual’s quality of life in
multiple domains
Subject of next presentation (by César Soutullo)
Coghill D Eur Neuropsychopharmacol 2011;21:571-83.

Defined in diagnostic criteria
• Hyperactivity/ impulsivity
• Inattention
The effects of ADHD on an individual’s life extend beyond symptoms
Functional impairment
Health-related quality of life
(HRQoL)
Also required for diagnosis
• Social
• Academic
• Occupational
Symptoms
The impact of disease on an individual’s quality of life in
multiple domains
Symptoms do not capture the range of outcomes and impact of ADHD
Impact of behaviour on daily life is the
major motivation for seeking treatment
Coghill D Eur Neuropsychopharmacol 2011;21:571-83.
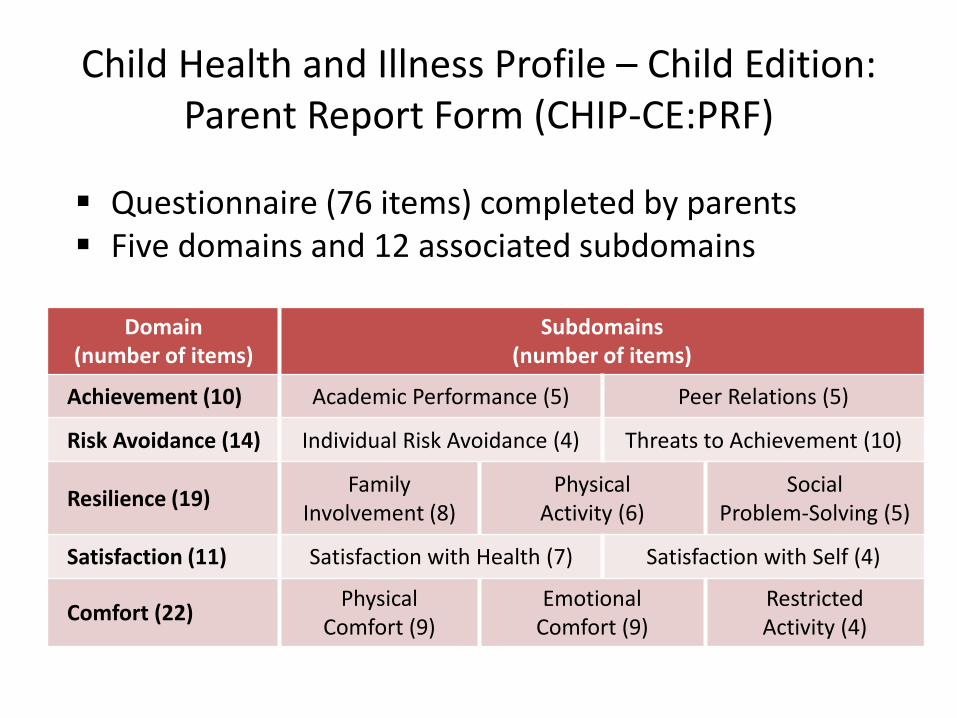
Questionnaire (76 items) completed by parents Five domains and 12 associated subdomains
Domain (number of items)
Subdomains (number of items)
Achievement (10) Academic Performance (5) Peer Relations (5)
Risk Avoidance (14) Individual Risk Avoidance (4) Threats to Achievement (10)
Resilience (19)Family
Involvement (8)Physical
Activity (6)Social
Problem-Solving (5)
Satisfaction (11) Satisfaction with Health (7) Satisfaction with Self (4)
Comfort (22)Physical
Comfort (9)Emotional
Comfort (9)RestrictedActivity (4)
Child Health and Illness Profile – Child Edition: Parent Report Form (CHIP-CE:PRF)

Interpreting T-scores: normal distribution, mean = 50 and standard deviation (SD) = 10
50.0%
15.9%
0.1%
84.1%
Cumulative frequency
50(Mean)
40(−1 SD)
30(−2 SD)
20(−3 SD)
60(+1 SD)
Representation in this talk
T-score
70(+2 SD)
80(+3 SD)
97.7%
99.9%
Black circle at 50
2.3% of normative reference population have a T-score ≤ 30
2.3%
20 50 6030 40
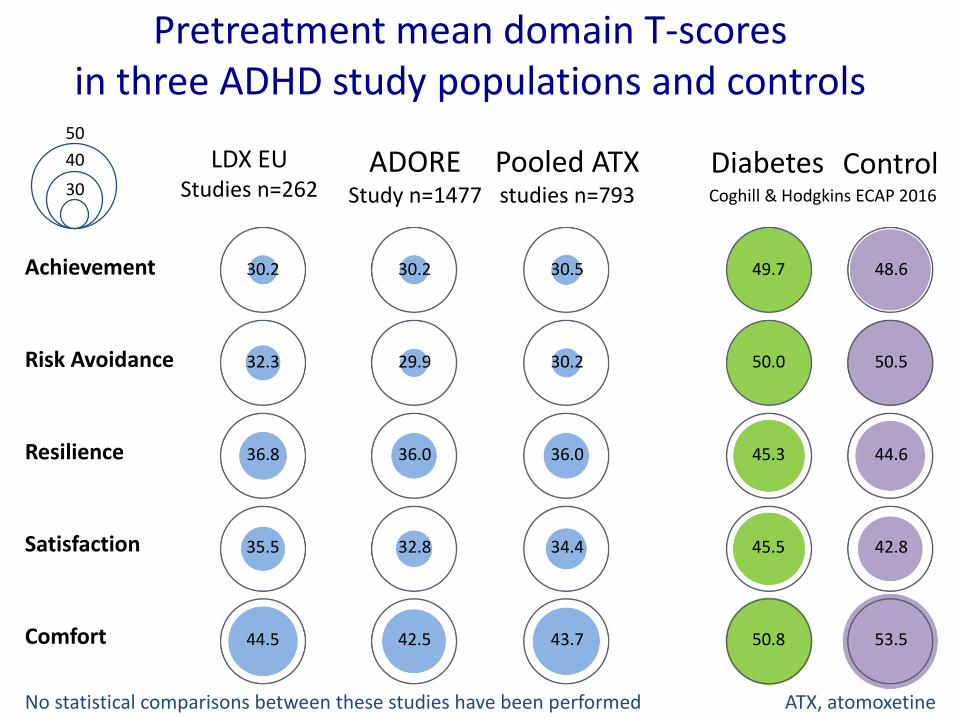
Pretreatment mean domain T-scores in three ADHD study populations and controls
30.2 30.2 30.5
32.3 29.9 30.2
36.8 36.0 36.0
35.5 32.8 34.4
44.5 42.5 43.7
49.7 48.6
50.0 50.5
45.3 44.6
45.5 42.8
50.8 53.5
Diabetes ControlLDX EU Studies n=262
ADOREStudy n=1477
Pooled ATX studies n=793
50
40
30
Achievement
Risk Avoidance
Resilience
Satisfaction
Comfort
No statistical comparisons between these studies have been performed ATX, atomoxetine
Coghill & Hodgkins ECAP 2016
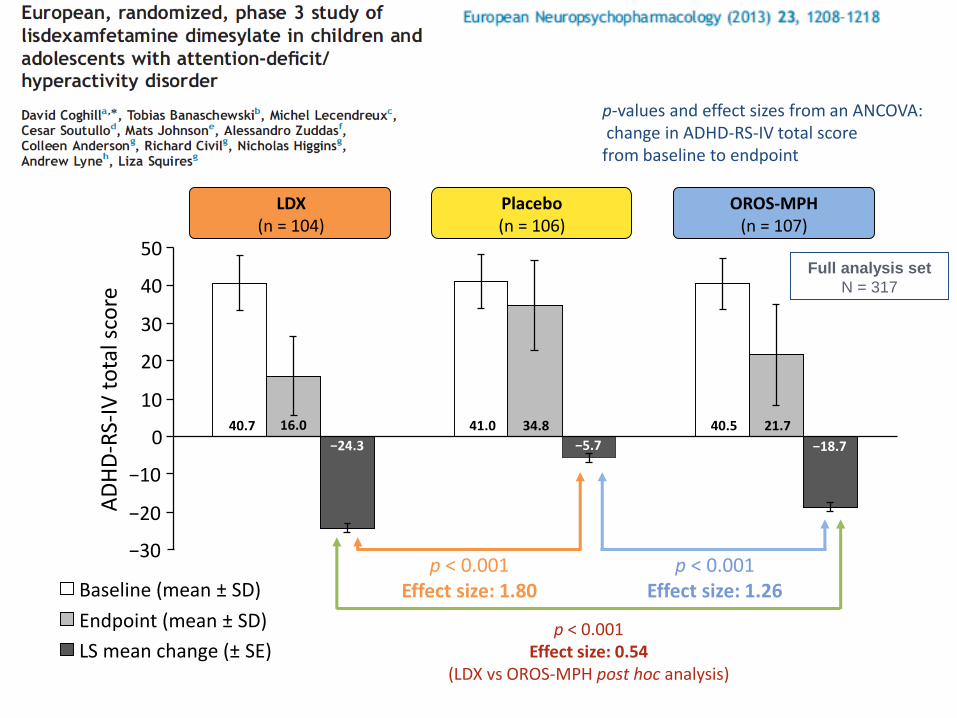
Placebo(n = 106)
LDX(n = 104)
OROS-MPH(n = 107)
−20
Baseline (mean ± SD)
Endpoint (mean ± SD)
LS mean change (± SE)
AD
HD
-RS-
IV t
ota
l sco
re
40.7 41.0 40.534.8 21.716.0
−5.7
−30
−10
0
10
20
30
40
50
−24.3 −18.7
p < 0.001Effect size: 1.80
p < 0.001Effect size: 1.26
Full analysis set
N = 317
p < 0.001Effect size: 0.54
(LDX vs OROS-MPH post hoc analysis)
p-values and effect sizes from an ANCOVA:change in ADHD-RS-IV total score from baseline to endpoint
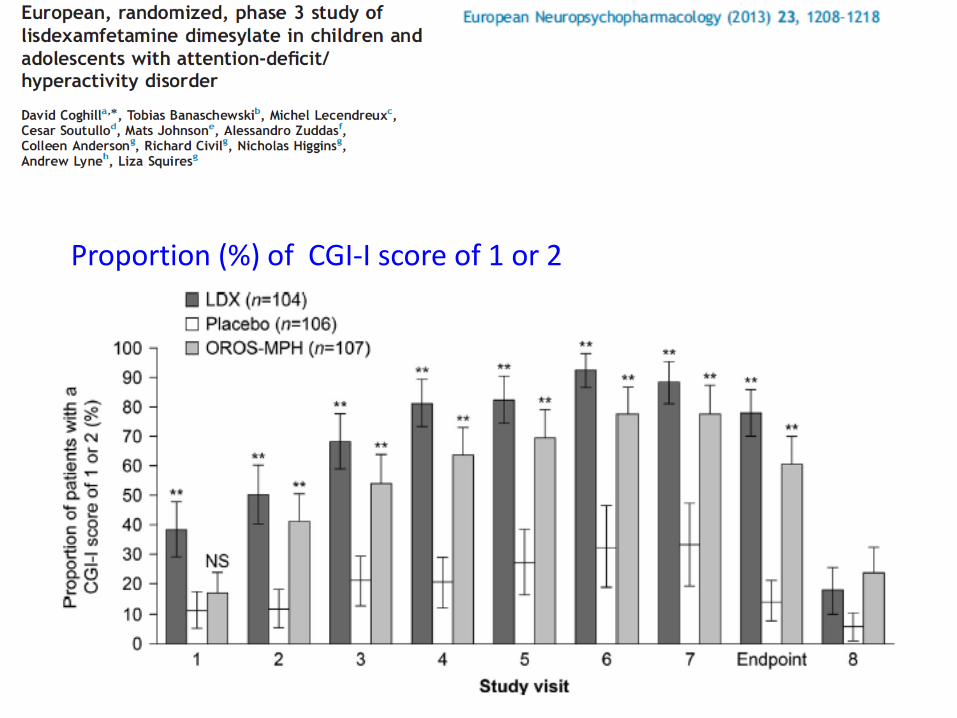
Proportion (%) of CGI-I score of 1 or 2
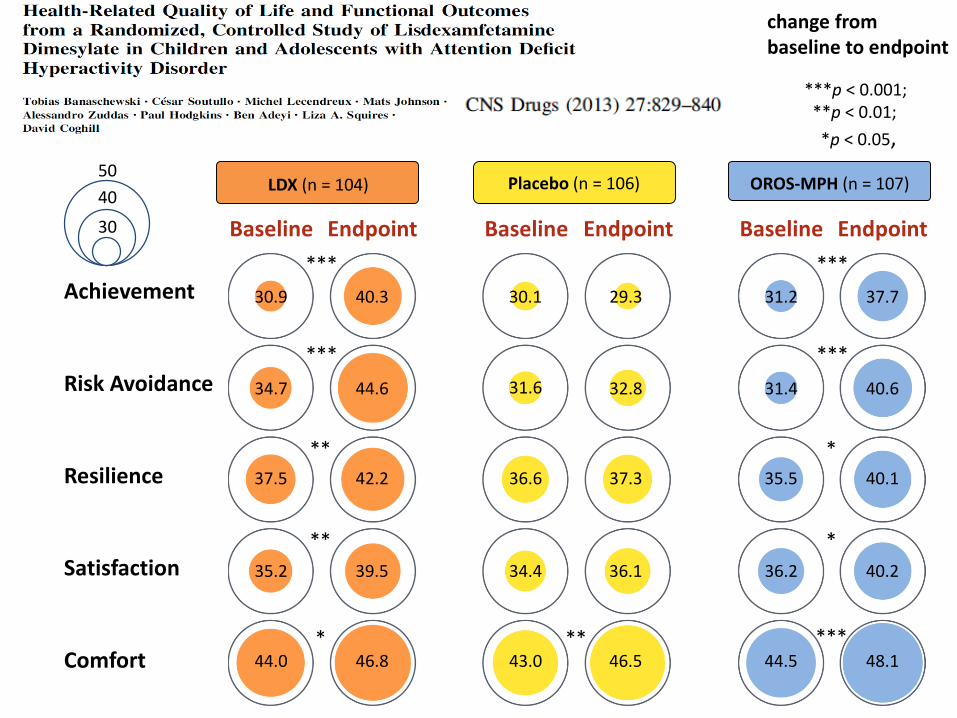
30.9 40.3 30.1
34.7 44.6 31.6
37.5 42.2 36.6
35.2 39.5 34.4
44.0 46.8 43.0
31.2 37.7
31.4 40.6
35.5 40.1
36.2 40.2
44.5 48.1
29.3
32.8
37.3
36.1
46.5
LDX (n = 104) Placebo (n = 106) OROS-MPH (n = 107)
EndpointBaseline EndpointBaseline EndpointBaseline
***p < 0.001; **p < 0.01; *p < 0.05, change from baseline to endpoint (not adjusted for multiplicity)
***
***
**
**
*
***
***
*
*
*****
50
40
30
Achievement
Risk Avoidance
Resilience
Satisfaction
Comfort
***p < 0.001; **p < 0.01;
*p < 0.05,
change from baseline to endpoint
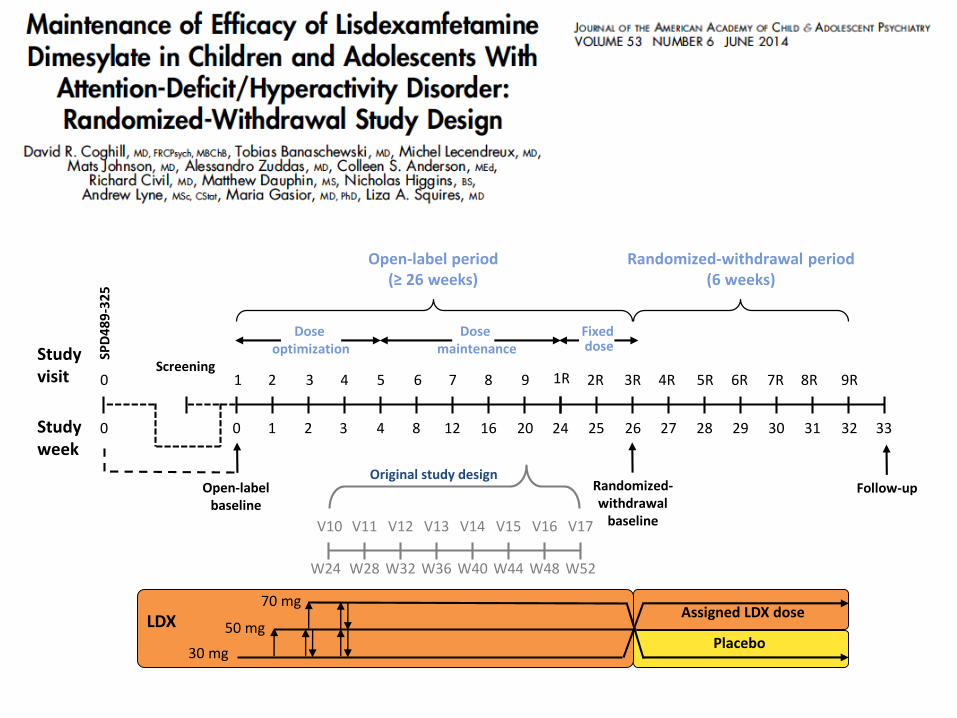
3R 9R
Follow-up
Studyvisit 1
Open-labelbaseline
Fixed dose
Randomized-withdrawal period (6 weeks)
2 3 4 5 6
V10
7 8 9 1R 2R 4R 5R 6R 7R 8R
V11 V12 V13 V14 V15 V16 V17
0 1 2 3 4 8 12 16 20 24 25 26 27 28 29 30 31 32
W24 W28 W32 W36 W40 W44 W48 W52
Dose maintenance
Dose optimization
Open-label period(≥ 26 weeks)
Studyweek
Original study designRandomized-withdrawal
baseline
LDX
30 mg
50 mg
70 mg
Placebo
Assigned LDX dose
Screening
33
0
0
SPD
48
9-3
25
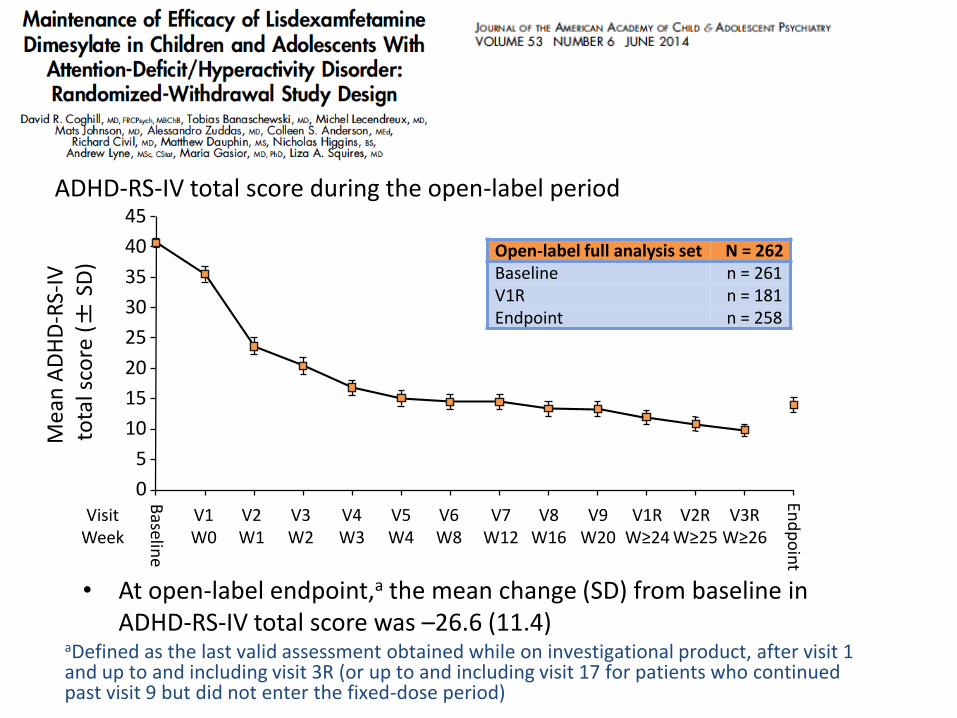
ADHD-RS-IV total score during the open-label period
• At open-label endpoint,a the mean change (SD) from baseline in ADHD-RS-IV total score was –26.6 (11.4)
Open-label full analysis set N = 262Baseline n = 261V1R n = 181Endpoint n = 258
45
40
35
30
25
0
Mea
n A
DH
D-R
S-IV
to
tal s
core
(±
SD)
20
15
10
5
Baselin
e
V1W0
V2W1
V3W2
V4W3
V5W4
V6W8
V7W12
V8W16
V9W20
V1RW≥24
V2RW≥25
V3RW≥26
End
po
int
VisitWeek
aDefined as the last valid assessment obtained while on investigational product, after visit 1 and up to and including visit 3R (or up to and including visit 17 for patients who continued past visit 9 but did not enter the fixed-dose period)
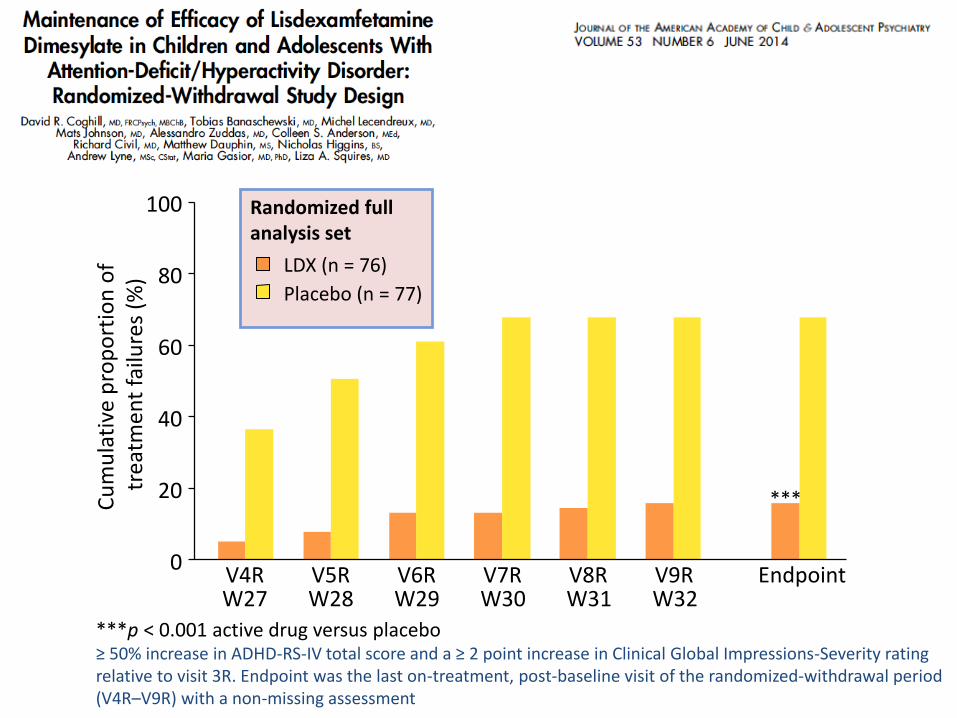
***p < 0.001 active drug versus placebo≥ 50% increase in ADHD-RS-IV total score and a ≥ 2 point increase in Clinical Global Impressions-Severity rating relative to visit 3R. Endpoint was the last on-treatment, post-baseline visit of the randomized-withdrawal period (V4R–V9R) with a non-missing assessment
Randomized full analysis set
LDX (n = 76)
Placebo (n = 77)
Cu
mu
lati
ve p
rop
ort
ion
of
trea
tmen
t fa
ilure
s (%
)
***
V4R V5R V6R V7R V8R V9R EndpointW27 W28 W29 W30 W31 W32
0
20
40
60
80
100

30.2 38.9 39.6
32.3 44.1 45.8
36.8 40.5 42.0
35.5 40.3 41.9
44.5 49.4 51.0
41.2 35.3
46.8 41.3
42.6 40.2
43.3 39.3
51.1 48.5
40.1
47.5
43.3
44.9
51.1
LDX (n = 76)
EndpointBaseline EndpointBaseline EndpointBaseline
LDX (n = 262)
Open label (≤ 26 weeks) Randomized withdrawal (6 weeks)50
40
30
Achievement
Risk Avoidance
Resilience
Satisfaction
Comfort
Placebo (n = 77)