
The Characteristics of Asthma Patients And Evaluation of the
78
1 CHAPTER I INTRODUCTION A. Background Globally, asthma is one of the most common chronic diseases and currently affects approximately 300 million people worldwide. The prevalence of asthma has risen in affluent countries over the last 30 years but now appears to have stabilized, with approximately 10-12% of adults and 15% of children affected by the disease (Longo et al, 2012). Asthma is a syndrome characterized by airflow obstruction that varies markedly, both spontaneously and with treatment (Longo et al, 2012). Asthma is a disease of increasing prevalence that is a result of genetic predisposition and environmental interactions; it is one of the most common chronic diseases of childhood (DiPiro et al, 2008). Usually, asthma can present at any age, with a peak age of 3 years. In childhood, twice as many males as females are asthmatic, but by adulthood the sex ratio is equalized. The commonly held belief that children "grow out of their asthma" is justified to some extent. Long term studies that have followed children until they reach the age of 40 years suggest that many with asthma become asymptomatic during adolescence but that asthma can reoccur at some point during adulthood, particularly in those with persistent symptoms and severe asthma (Longo et al, 2012).
-
Upload
sohbana-pillai-murali-dharan -
Category
Documents
-
view
13 -
download
0
Transcript of The Characteristics of Asthma Patients And Evaluation of the

1
CHAPTER I
INTRODUCTION
A. Background
Globally, asthma is one of the most common chronic diseases and
currently affects approximately 300 million people worldwide. The
prevalence of asthma has risen in affluent countries over the last 30 years
but now appears to have stabilized, with approximately 10-12% of adults
and 15% of children affected by the disease (Longo et al, 2012).
Asthma is a syndrome characterized by airflow obstruction that
varies markedly, both spontaneously and with treatment (Longo et al,
2012). Asthma is a disease of increasing prevalence that is a result of
genetic predisposition and environmental interactions; it is one of the
most common chronic diseases of childhood (DiPiro et al, 2008).
Usually, asthma can present at any age, with a peak age of 3 years.
In childhood, twice as many males as females are asthmatic, but by
adulthood the sex ratio is equalized. The commonly held belief that
children "grow out of their asthma" is justified to some extent. Long term
studies that have followed children until they reach the age of 40 years
suggest that many with asthma become asymptomatic during adolescence
but that asthma can reoccur at some point during adulthood, particularly
in those with persistent symptoms and severe asthma (Longo et al, 2012).
2
The exact cause of asthma still remains unknown, but it is thought
to be caused by allergy to some foreign substance (allergen) or irritant, no
extrinsic trigger can be found in some types of asthma. Allergens include
(but are not limited to) pollen, dust mites, feathers, animal dander, molds,
some drugs such as aspirin, and rarely foods. Asthma may also occur in
association with other allergic conditions, such as eczema or hay fever.
Other precipitants of asthma attacks include cold or dry air, smoke, air
pollution, bronchitis and other lung infections, vigorous exercise,
emotional excitement, or stress. A predisposition to asthma may be
hereditary (Margolis et al, 2006). Symptoms include difficulty breathing,
wheezing, coughing tightness in the chest. In severe cases, asthma can be
fatal.
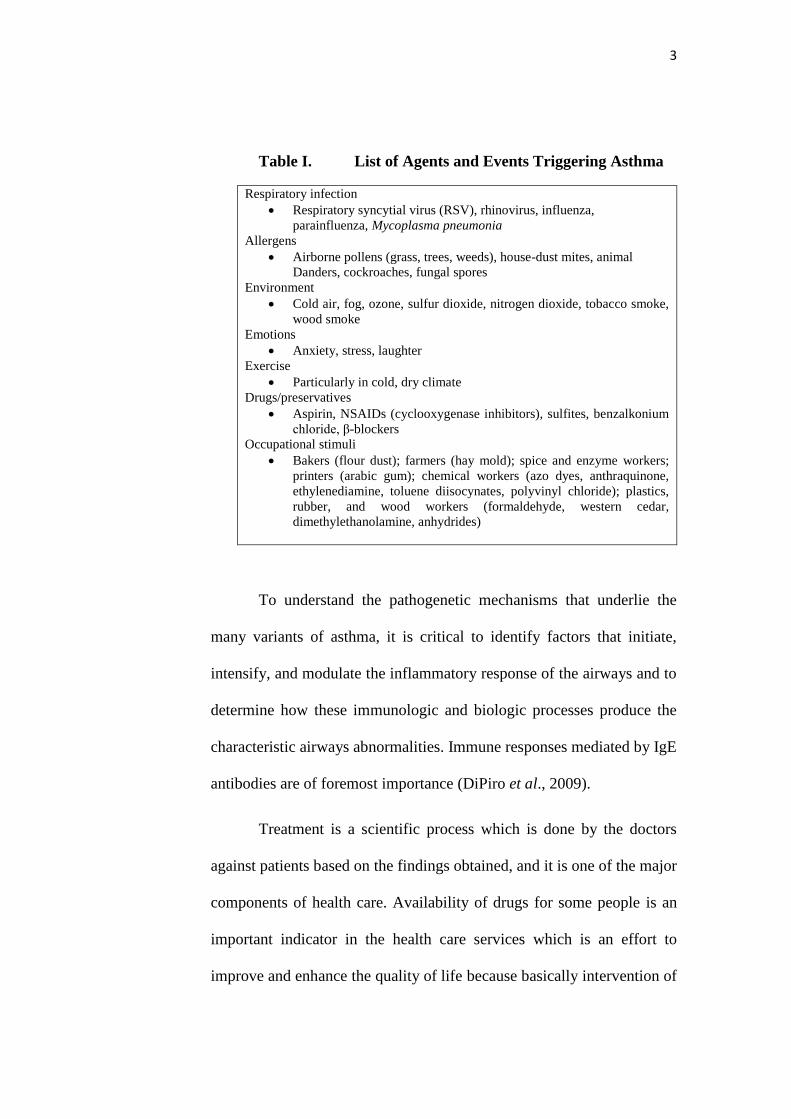
Furthermore, the major characteristics of asthma include a
variable degree of airflow obstruction (related to bronchospasm, edema,
and hypersecretion), bronchial hyper-responsiveness (BHR), and airways
inflammation. Evidence of inflammation depicted in the studies of
nonspecific BHR, bronchoalveolar lavage (BAL), bronchial biopsies, and
induced sputum, as well as from postmortem observations of patients with
asthma who died from an attack of asthma or from other causes. List of
the agents and events triggering asthma have been summarized into a
table below:
3
Table I. List of Agents and Events Triggering Asthma
To understand the pathogenetic mechanisms that underlie the
many variants of asthma, it is critical to identify factors that initiate,
intensify, and modulate the inflammatory response of the airways and to
determine how these immunologic and biologic processes produce the
characteristic airways abnormalities. Immune responses mediated by IgE
antibodies are of foremost importance (DiPiro et al., 2009).
Treatment is a scientific process which is done by the doctors
against patients based on the findings obtained, and it is one of the major
components of health care. Availability of drugs for some people is an
important indicator in the health care services which is an effort to
improve and enhance the quality of life because basically intervention of
Respiratory infection
Respiratory syncytial virus (RSV), rhinovirus, influenza,
parainfluenza, Mycoplasma pneumonia
Allergens
Airborne pollens (grass, trees, weeds), house-dust mites, animal
Danders, cockroaches, fungal spores
Environment
Cold air, fog, ozone, sulfur dioxide, nitrogen dioxide, tobacco smoke,
wood smoke
Emotions
Anxiety, stress, laughter
Exercise
Particularly in cold, dry climate
Drugs/preservatives
Aspirin, NSAIDs (cyclooxygenase inhibitors), sulfites, benzalkonium
chloride, β-blockers
Occupational stimuli
Bakers (flour dust); farmers (hay mold); spice and enzyme workers;
printers (arabic gum); chemical workers (azo dyes, anthraquinone,
ethylenediamine, toluene diisocynates, polyvinyl chloride); plastics,
rubber, and wood workers (formaldehyde, western cedar,
dimethylethanolamine, anhydrides)

4
a therapy is by using drugs. Drugs are chemical substance that can affect
the process of life. For instance, a drug will enter the body's circulatory
system and produce an effect (Sastramihardja et al, 1997).
Many different medications are used to manage and control
asthma. The two types of asthma medications used to treat asthma include
long-term control medication and short-term, or also known as quick-
relief medication. Though the goal of both medications is to treat asthma
symptoms, they are used for different purposes. Furthermore there is also
presence of surgical methods in controlling asthma apart from
medications such as bronchial thermoplasty. Long-term control
medication is usually taken every day to control asthma symptoms and to
prevent the occurrence of asthma attacks, for example inhaled
corticosteroids, long acting β2-agonist, leukotriene modifiers and Anti Ig-
E. Quick-relief medication is primarily taken to relieve the sudden onset
of asthma symptoms (such as during an asthma attack), and in cases in
which the asthma symptoms only occur occasionally, for example short-
acting beta2-agonists and anticholinergics. Surgery such as bronchial
thermoplasty can reduce the size of the smooth muscle allowing many
patients to cut back on medication and lead more active lives through
inserting a bronchoscope with a thermoplasty device inside into the
asthmatic patient’s mouth or nose as far as possible down each airway.
Electrodes on the tip are then heated with radiofrequency energy,
shrinking the muscle and creating a larger opening in the airway.

5
A clear picture of the treatment patterns for asthma in RSUP Dr.
Sardjito, Yogyakarta are hopefully to be used as a reference to increase
the quality of medical services towards asthmatic patients which can
cause improvement in patient’s quality of life.
B. Statement of Problem
Based on the background, the problem in this research can be:
1. What is the characteristics of asthmatic patients seen from their age, sex,
comorbid illness, occupation, level of education and medical history in
RSUP Dr. Sardjito for the period of January 2013 till December 2013?
2. What is the pattern of drug therapy given to asthma patients in RSUP Dr.
Sardjito, Yogyakarta based on the type of drugs for respiratory tract
disorders (anti-inflammatory drugs and broncodilators) and whether the
treatment is polytherapy or monotherapy?
3. How is the outcome of the patient after the therapy?
C. Objective
1. The objective of this study is to understand the characteristics of asthma
patients in RSUP Dr. Sardjito, Yogyakarta from aspects such as their age,
sex, comorbid illness, and medical history for the period of January 2013
till December 2013.

6
2. Besides that, the study is also meant to evaluate the drug pattern in asthma
patients and to compare it to Clinical Practice Guideline of The Diagnosis
and Management of Asthma.
3. At the same time, this study will also observe the outcome of the patient
after the treatment with the drugs for respiratory tract disorders (anti-
inflammatory drugs and bronchodilators).
D. Benefit
The benefit of this study is to be able to understand the seriousness
of this new growing disease in our society and the risk factors that
contributes towards the disease which is to help provide information about
asthma with more in depth, so to expect to work together with the
government or related parties in reducing the number of incidence of
asthma cases. Also, this study will help me and others such as health care
providers to have a better understanding on pattern of drugs used in
asthmatic patients and the outcome of the therapy towards the patients.
Furthermore this study will increase the quality of pharmacy healthcare
services in hospitals nevertheless to increase knowledge on medical
sciences and to apply those knowledge obtained.
E. Literature Review
1. Asthma
a. Definition of Asthma
Asthma is defined as a chronic inflammatory disease of the
airways. The chronic inflammation is associated with airway

7
hyperresponsiveness (an exaggerated airway narrowing response
to triggers, such as allergens and exercise), that leads to recurrent
symptoms such as wheezing, dyspnea (shortness of breath), chest
tightness and coughing. Symptom episodes are generally
associated with widespread, but variable, airflow obstruction
within the lungs that is usually reversible either spontaneously or
with appropriate asthma treatment (Kim et al, 2011). There are
seven types of asthma which are (Crosta et al, 2013):
1). Child onset Asthma
Asthma that begins during childhood is called child-onset
asthma. This type of asthma happens because a child becomes
sensitized to common allergens in the environment - most likely due
to genetic reasons. The child is atopic – a genetically determined
state of hypersensitivity to environmental allergens. The airway
cells are sensitive to particular materials making an asthmatic
response more likely if the child is exposed to a certain amount of
an allergen.
2). Adult onset Asthma
This term is used when a person develops asthma after
reaching 20 years of age. Adult-onset asthma affects women more
than men, and it is also much less common than child-onset
asthma. It can also be triggered by some allergic material or an
allergy. It is estimated that up to perhaps 50% of adult-onset
8
asthmas are linked to allergies. However, a substantial proportion
of adult-onset asthma does not seem to be triggered by exposure
to allergen(s); this is called non-allergic adult-onset asthma. This
non-allergic type of adult onset asthma is also known as intrinsic
asthma. Exposure to a particle or chemical in certain plastics,
metals, medications, or wood dust can also be a cause of adult-
onset asthma.
3). Exercise induced Asthma
If you cough, wheeze or feel out of breath during or after
exercise, you could be suffering from exercise-induced asthma.
As with other types of asthma, a person with exercise-induced
asthma will experience difficulty in getting air in and out of the
lungs because of inflammation of the bronchial tubes (airways)
and extra mucus.
4). Cough induced Asthma
Cough-induced asthma is one of the most difficult asthmas
to diagnose. The doctor has to eliminate other possibilities, such
as chronic bronchitis, post nasal drip due to hay fever, or sinus
disease. In this case the coughing can occur alone, without other
asthma-type symptoms being present. The coughing can happen
at any time of day or night. If it happens at night it can disrupt
sleep.
5). Occupational Asthma
9
This type of asthma is triggered by something in the
patient's place of work. Factors such as chemicals, vapors,
gases, smoke, dust, fumes, or other particles can trigger
asthma. It can also be caused by a virus (flu), molds, animal
products, pollen, humidity and temperature. Another trigger
may be stress.
6). Nocturnal Asthma
Nocturnal asthma occurs between midnight and 8 AM. It
is triggered by allergens in the home such as dust and pet dander
or is caused by sinus conditions. Nocturnal or nighttime asthma
may occur without any daytime symptoms recognized by the
patient. The patient may have wheezing or short breath when lying
down and may not notice these symptoms until awoken by them
in the middle of the night - usually between 2 and 4 AM. Nocturnal
asthma may occur only once in a while or frequently during the
week. Nighttime symptoms may also be a common problem in
those with daytime asthma as well. However, when there are no
daytime symptoms to suggest asthma is an underlying cause of the
nighttime cough, this type of asthma will be more difficult to
recognize - usually delaying proper therapy. The causes of this
phenomenon are unknown, although many possibilities are
under investigation.
7). Steroid – resistant Asthma (Severe Asthma)

10
While the majority of patients respond to regular inhaled
glucocorticoid (steroid) therapy, some are steroid resistant.
Airway inflammation and immune activation play an important
role in chronic asthma. Current guidelines of asthma therapy have
therefore focused on the use of anti- inflammatory therapy,
particularly inhaled glucocorticoids (GCs). By reducing airway
inflammation and immune activation, glucocorticoids are used to
treat asthma. However, patients with steroid resistant
asthma have higher levels of immune activation in their
airways than do patients with steroid sensitive (SS) asthma.
Furthermore, glucocorticoids do not reduce the eosinophilia (high
concentration of eosinophil granulocytes in the blood) or T cell
activation found in steroid resistant asthmatics. This persistent
immune activation is associated with high levels of the immune
system molecules IL-2 (interleukin 2), IL-4 and IL-5 in the
airways of these patients.
b. Epidemiology of Asthma
According to WHO, Asthma is one of the major non-
communicable diseases. WHO estimates that 235 million
people currently suffer from asthma. Asthma is the most
common non-communicable disease among children.
Asthma is a public health problem not just for high-income
countries; it occurs in all countries regardless of the level of
11
development. Most asthma-related deaths occur in low- and
lower-middle income countries.
Based on AAAAI, the number of people with asthma
continues to grow. One in 12 people (about 25 million, or 8% of
the U.S. population) had asthma in 2009, compared with 1 in 14
(about 20 million, or 7%) in 2001. More than half (53%) of people
with asthma had an asthma attack in 2008. More children (57%)
than adults (51%) had an attack. 185 children and 3,262
adults died from asthma in 2007. About 1 in 10 children (10%)
had asthma and 1 in 12 adults (8%) had asthma in 2009.
Women were more likely than men and boys more likely than girls
to have asthma. For the period 2008–2010, asthma prevalence was
higher among children than adults.
Asthma is one of the major causes of death in many
countries. The prevalence of asthma in different countries
varies widely, but the disparity is narrowing due to rising
prevalence in low and middle income countries and plateauing in
high income countries (Anonymous, 2011). An estimated 300
million people worldwide suffer from asthma, with 250,000
annual deaths attributed to the disease. It is estimated that the
number of people with asthma will grow by more than 100 million
by 2025. Workplace conditions, such as exposure to fumes, gases
or dust, are responsible for 11% of asthma cases worldwide. About

12
70% of asthmatics also have allergies. Approximately 250,000
people die prematurely each year from asthma. Almost all of
these deaths are avoidable. Occupational asthma contributes
significantly to the global burden of asthma, since the condition
accounts for approximately 15% of asthma amongst adults
(Anonymous, 2007a).
There are still no accurate statistics in Indonesia, but
according on the latest WHO data published in April 2011,
asthma deaths in Indonesia reached 14,624 or 1.03% of total
deaths. The age adjusted death rate is 8.25 per 100,000 of
population and ranks Indonesia as the no 69th in the world and
asthma as one of the top 20 causes of death in Indonesia.
c. Etiology of Asthma
The cause of Asthma has not been clearly identified
till date. The causes of Asthma are multifactorial. Some of them
cannot be changed such as age and genetic. Asthma is a
heterogeneous disease with interplay between genetic and
environmental factors. Several risk factors have been
implicated (Longo et al, 2012):
1). Genetic predisposition
2). Atopy
3). Airway hyperresponsiveness
4). Gender

13
5). Ethnicity
6). Obesity
7). Early viral infections
8). Indoor and outdoor allergens
9). Occupational sensitizers
10). Passive smoking
11). Respiratory infections
12). Drugs (β-blockers, aspirin)
13). Stress
14). Irritants (household sprays, paint fumes)
15). Cold air
16). Exercise and hyperventilation
17). Sulfur dioxide and irritant gases
d. Pathogenesis and Pathophysiology of Asthma
1). Pathogenesis
Asthma is associated with a chronic inflammation of the
mucosa of the lower airways. One of the main aims of treatment
is to reduce this inflammation (Longo et al, 2012).
2). Pathology
The pathology of asthma has been revealed through the
examining the lungs at autopsy of patients who have died of
asthma and from bronchial biopsies in patients with usually mild
asthma. The airway mucosa is infiltrated with activated

14
eosinophils and T lymphocytes, and there is activation of mucosal
mast cells. The degree of inflammation is poorly related to disease
severity and may be found in atopic patients without asthma
symptoms. The inflammation is reduced by treatment with ICS. A
characteristic finding is thickening of the basement membrane due
to subepithelial collagen deposition. This feature is also found in
patients with eosinophilic bronchitis presenting as cough who do
not have asthma and is therefore, likely to be a marker of
eosinophilic inflammation in the airway as eosinophils release
fibrogenic factors. The epithelial is often shed or friable, with
reduced attachments to the airway wall and increased numbers
of epithelial cells in the lumen. The airway wall itself may be
thickened and edematous, particularly in fatal asthma.
Another common finding in fatal asthma is occlusion of
the airway lumen by a mucous plug, which is comprised of
mucous glycoproteins secreted from goblet cells and plasma
proteins from leaky bronchial vessels. There is also vasodilation
and increased number of blood vessels (angiogenesis). Direct
observation by bronchoscopy indicates that the airways may be
narrowed, erythematous, and edematous. The pathology of asthma
is remarkably uniform in different types of asthma, including
atopic, non-atopic, occupational, aspirin-sensitive, and pediatric
asthma. These pathologic changes are found in all airways, but do

15
not extend to the lung parenchyma; peripheral airway
inflammation is found particularly in patients with severe
asthma. The involvement of airways may be patchy and this is
consistent with bronchographic findings of uneven narrowing of
the pathways (Longo et al, 2012).
3). Pathophysiology
Asthma is associated with T helper cell type-2 (TH2)
immune responses, which are typical of other atopic conditions.
Various allergic (e.g., dust mites, cockroach residue, furred
animals, moulds, pollens) and non-allergic (e.g., infections,
tobacco smoke, cold air, exercise) triggers produce a cascade of
immune-mediated events leading to chronic airway inflammation.
Elevated levels of TH2 cells in the airways release specific
cytokines, including interleukin (IL)-4, IL-5, IL-9 and IL-13,
that promote eosinophilic inflammation and immunoglobulin E
(IgE) production by mast cells. IgE production, in turn, triggers
the release of inflammatory mediators, such as histamine and
cysteinyl leukotrienes, that cause bronchospasm (contraction of
the smooth muscle in the airways), edema (swelling) and
increased mucous secretion (mucous hypersecretion), which lead
to the characteristic symptoms of asthma. The mediators and
cytokines released during the early phase of an immune response
to an inciting allergen, trigger a further inflammatory response

16
(late-phase asthmatic response) that leads to further airway
inflammation and bronchial hyperreactivity.
Evidence suggests that there may be a genetic
predisposition for the development of asthma. A number of
chromosomal regions associated with asthma susceptibility have
been identified, such as those related to the production of IgE
antibodies, expression of airway hyperresponsiveness, and the
production of inflammatory mediators. However, further study
is required to determine specific genes involved in asthma as well
as the gene-environment interactions that may lead to expression
of the disease (Kim et al, 2011).
Figure 1. The many inflammatory cells which are
known to be involved in Asthma with no
key cell that is predominant (Longo et al,
2012).

17
e. Classification of Asthma
Classification of asthma is done based on the severity and
the control of the disease. Firstly, it occurs with an intermittent
stage of asthma and continued by persistent asthma which can be
divided into 3 groups such as mild, moderate and severe whereas
when based on the control of asthma, it can be divided into 3
aspects, which are well controlled, not well controlled and very
poorly controlled (Anonymous, 2012a).
1). Severity of the Disease
a). Intermittent asthma
b). Persistent asthma
(1). Mild
(2). Moderate
(3). Severe
Table II. The classification of Asthma based on severity
of the disease (Anonymous, 2012a)
2). Control of the disease
a). Well controlled
b). Not well controlled
c). Very poorly controlled
Components of
Severity
Classification of Asthma Severity
≥12 years of age
Intermittent
Persistent
Mild
Moderate
Severe

18
Table III. The classification of Asthma based on
components of control (Anonymous, 2012a).
f. Sign and Symptoms of Asthma
Presence of any of these signs and symptoms should
increase the suspicion or indicate that the patient is suffering from
asthma (Anonymous, 2012c):
1). Wheezing high-pitched whistling sounds when breathing out
especially in children. (A normal chest examination does not
exclude asthma)
2). History of any of the following:
a). Cough, worse particularly at night
b). Recurrent wheeze
c). Recurrent difficult breathing
d). Recurrent chest tightness
3). Symptoms occur or worsen at night, awakening the patient.
4). Symptoms occur or worsen in a seasonal pattern.
5). The patient also has eczema, hay fever, or a family history of
asthma or atopic diseases.
Components of
Control
Classification of Asthma Control
≥12 years of age
Well
Controlled
Not Well
Controlled
Very Poorly
Controlled

19
6). Symptoms occur or worsen in the presence of:
a). Animals with fur
b). Aerosol chemicals
c). Changes in temperature
d). Domestic dust mites
e). Drugs (aspirin, beta blockers)
f). Exercise
g). Pollen
h). Respiratory (viral) infections
i). Smoke
j). Strong emotional expression
7). Symptoms respond to anti-asthma therapy.
8). Patients colds “go to chest” or take more than 10 days to clear
up.
g. Diagnosis
The diagnosis of asthma is based on the recognition of a
characteristic pattern of symptoms and signs and the absence of
an alternative explanation for them (see Table IV). The key is to
take a careful clinical history. In many cases this will allow a
reasonably certain diagnosis of asthma, or an alternative
diagnosis, to be made. If asthma does appear likely, the
history should also explore possible causes, particularly
occupational.

20
Table IV. The recognition of a characteristic pattern of
symptoms and signs and the absence of an
alternative explanation.
In view of the potential requirement for treatment over
many years, it is important even in relatively clear cut cases, to try
to obtain objective support for the diagnosis. Whether or not this
should happen before starting treatment depends on the certainty
of the initial diagnosis and the severity of presenting symptoms.
Repeated assessment and measurement may be necessary before
confirmatory evidence is acquired. Confirmation hinges on
demonstration of airflow obstruction varying over short periods of
time.
Spirometry, which is now becoming more widely
available, is preferable to measurement of peak expiratory flow
because it allows clearer identification of airflow obstruction, and

21
the results are less dependent on effort. It should be the preferred
test where available (although some training is required to obtain
reliable recordings and to interpret the results). Of note, a normal
spirogram (or PEF) obtained when the patient is not symptomatic
does not exclude the diagnosis of asthma. Results from spirometry
are also useful where the initial history and examination leave
genuine uncertainty about the diagnosis. In such cases, the
differential diagnosis and approach to investigation is different in
patients with and without airflow obstruction (see Figure 2 and
Table V). In patients with a normal or near-normal spirogram
when symptomatic, potential differential diagnoses are mainly
non-pulmonary; these conditions do not respond to inhaled
corticosteroids and bronchodilators. In contrast, in patients with
an obstructive spirogram the question is less whether they will
need inhaled treatment but rather exactly what form and how
intensive this should be.
Other tests of airflow obstruction, airway responsiveness
and airway inflammation can also provide support for the
diagnosis of asthma, but to what extent the results of the tests alter
the probability of a diagnosis of asthma has not been clearly
established, nor is it clear when these tests are best performed.

22
Figure 2. The presentation with suspected asthma in
adults (Anonymous, 2012b)
Furthermore, there are also other diagnosis methods such
as hematologic tests, imaging like chest roentgenography, skin
test and also exhaled nitric oxide (Longo et al, 2012).
23
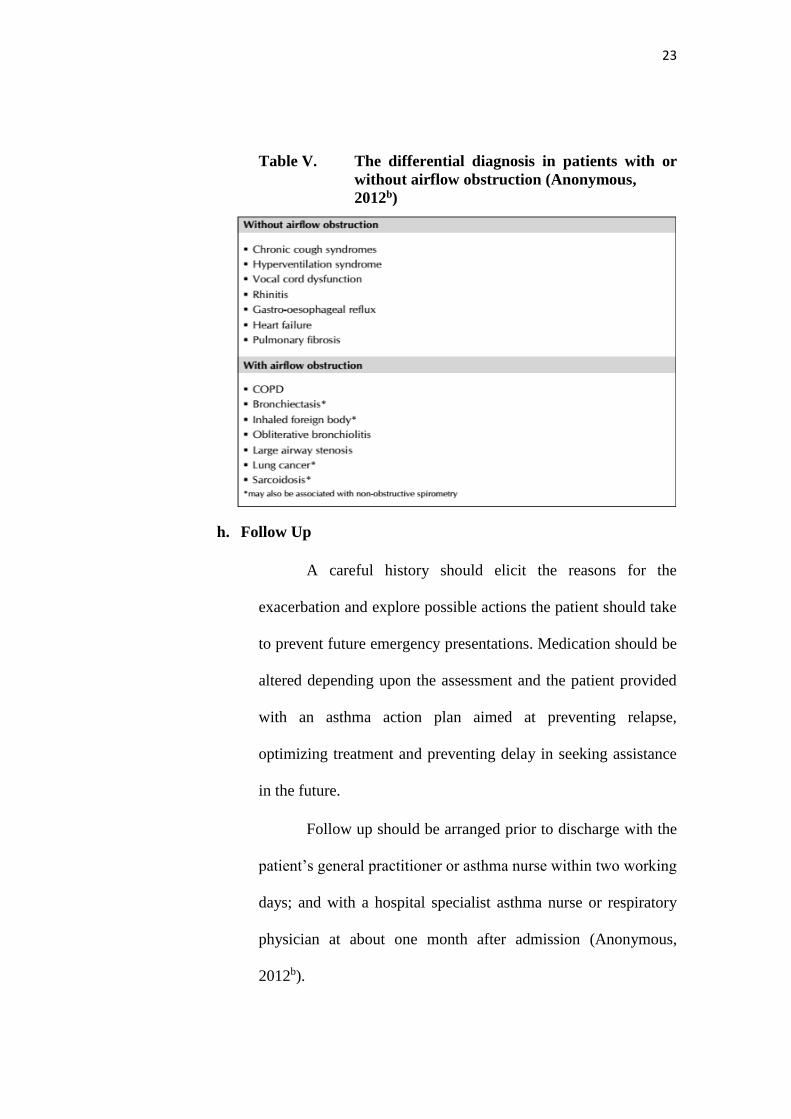
Table V. The differential diagnosis in patients with or
without airflow obstruction (Anonymous,
2012b)
h. Follow Up
A careful history should elicit the reasons for the
exacerbation and explore possible actions the patient should take
to prevent future emergency presentations. Medication should be
altered depending upon the assessment and the patient provided
with an asthma action plan aimed at preventing relapse,
optimizing treatment and preventing delay in seeking assistance
in the future.
Follow up should be arranged prior to discharge with the
patient’s general practitioner or asthma nurse within two working
days; and with a hospital specialist asthma nurse or respiratory
physician at about one month after admission (Anonymous,
2012b).
24
i. Therapy of Asthma
1). Objective of Therapy
Treatments of asthma can be said as effective if certain
objectives are achieved such as (Anonymous, 2010a):
a). Minimal or no chronic symptoms day or night
b). Minimal or no exacerbations
c). No limitations on activities/no school/parent’s
work missed
d). Maintain (near) normal pulmonary function in
adults and children
e). Minimal use of short-acting inhaled beta2-agonist
f). Minimal or no adverse effects from medications
2). Algorithm of Therapy
The treatment of asthma is straightforward and the
majority of patients are now managed by internists and family
doctors with effective and safe therapies. There are several aims
of therapy. Most emphasis has been placed on drug therapy, but
several non-pharmacologic approaches have also been used

25
(Longo et al, 2012). All diseases have their own specific algorithm
so do asthma.
Figure 3. The main algorithm therapy for Diagnosis and
Management of Asthma (Sveum et al, 2012).

26
3). Anti-asthmatic Drug
Medications for asthma are categorized into two general
classes: long-term control medication and quick-relief medication.
Selection of medications includes consideration of the general
mechanisms and role of the medication in therapy, delivery
devices, and safety. Long-term control medications are used daily
to achieve and maintain control of persistent asthma. The most
effective are those that attenuate the underlying inflammation
characteristic of asthma.
a). Long-term control medications include the following
(listed in alphabetical order) (Anonymous, 2007b):
(1). Corticosteroids are anti-inflammatory medications
that reduce airway hyperresponsiveness, inhibit
inflammatory cell migration and activation, and block
late phase reaction to allergen. Inhaled
Corticosteriods (ICSs) are the most consistently
effective long-term control medication at all steps of
care for persistent asthma. Short courses of oral
systemic corticosteroids are often used to gain prompt
control of asthma and are used long term to treat
patients with severe persistent asthma.
(2). Cromolyn sodium and nedocromil stabilize mast cells
and interfere with chloride channel function. They are

27
used as alternative, but not preferred, medication for
patients with mild persistent asthma. They also can be
used as preventive treatment before exercise or
unavoidable exposure to known allergens.
(3). Immunomodulators. Omalizumab (anti-IgE) is a
monoclonal antibody that prevents binding of IgE to
the high-affinity receptors on basophils and mast
cells. Omalizumab is used as adjunctive therapy for
patients 12 years of age who have sensitivity to
relevant allergens (e.g., dust mite, cockroach, cat, or
dog) and with severe persistent asthma. Clinicians
who administer omalizumab should be prepared and
equipped to identify and treat anaphylaxis that may
occur.
(4). Leukotriene modifiers interfere with the pathway of
leukotriene mediators, which are released from mast
cells, eosinophils, and basophils. These medications
include LTRAs (montelukast and zafirlukast) and a 5-
lipoxygenase inhibitor (zileuton). LTRAs are
alternative, but not preferred, therapy for the
treatment of patients with mild persistent asthma.
(5). LABAs (salmeterol and formoterol) are inhaled
bronchodilators that have a duration of

28
bronchodilation of at least 12 hours after a single
dose. LABAs are not to be used as monotherapy for
long-term control of asthma.
(6). Methylxanthines. Sustained-release theophylline is a
mild to moderate bronchodilator used as alternative,
not preferred, therapy for mild persistent asthma or as
adjunctive therapy with ICS in patients ≥5 years of
age. Theophylline may have mild anti-inflammatory
effects. Monitoring of serum theophylline
concentration is essential.
b). Quick-relief medications are used to treat acute symptoms
and exacerbations. They include the following (listed in
alphabetical order) (Anonymous, 2007b):
(1). Anticholinergics inhibit muscarinic cholinergic
receptors and reduce intrinsic vagal tone of the
airway. Ipratropium bromide provides additive
benefit to SABA in moderate or severe exacerbations
in the emergency care setting, not the hospital setting.
Ipratropium bromide may be used as an alternative
bronchodilator for patients who do not tolerate
SABA.
(2). SABAs—albuterol, levalbuterol, and pirbuterol—are
bronchodilators that relax smooth muscle. They are
29
the treatment of choice for relief of acute symptoms
and prevention of EIB. Increasing use of SABA
treatment or the use of SABA >2 days a week for
symptom relief (not prevention of EIB) generally
indicates inadequate asthma control and the need for
initiating or intensifying anti-inflammatory therapy.
Regularly scheduled, daily, chronic use of SABA is
not recommended.
(3). Systemic corticosteroids. Although not short-acting,
oral systemic corticosteroids are used for moderate
and severe exacerbations in addition to SABA to
speed recovery and to prevent recurrence of
exacerbations.
4). Surgery
Bronchial thermoplasty (BT), a new concept in the
treatment of asthma, aims to reduce the airway smooth muscle
(ASM) mass with the goal of diminishing bronchial constriction
and ameliorating asthma symptoms. The reduction in ASM is
accomplished by delivering controlled thermal energy to the
airway walls during a series of three bronchoscopies. The thermal
energy is delivered via the Alair system (Boston Scientific,
Natick, MA), which consists of a radiofrequency electrical

30
generator and a single-use catheter with an expandable four-
electrode basket at its distal tip (Figure III) (Wahidi et al, 2011).
Bronchial thermoplasty has been shown to reduce the
ASM mass via radiofrequency ablation in healthy animal and
human airways; whether the reduction in ASM mass can be
reproduced in the airways of patients with asthma or is the only
mechanism responsible for the clinical benefits seen in patients
with severe asthma requires further study. Alternative or
contributing mechanisms of BT may include modification in the
extracellular matrix that can lead to fixed airway structure,
reduction of mucus gland hyperplasia with an accompanying
decrease in mucus production, or change in the autonomic tone of
the airway (Wahidi et al, 2011).
Figure 4. The thermoplasty catheter with a distal shaft
marked at 5-mm intervals and an expandable
basket carrying four electrodes (Wahidi et al,
2011).

31
Table VI. The Usual Dosages for Long-Term Control
Medications (Anonymous, 2005).

32
Table VII. The Usual Dosages for Quick-Relief Medications
(Anonymous, 2005)
33
F. Empirical Expectations
1. Characteristics of patients play a vital role in developing asthma.
2. There could be different patterns of treatment for patients based
on effectiveness of drugs used for respiratory disorders (anti-
inflammatory drugs and bronchodilators) in controlling the
severity of asthma.

34
CHAPTER II
RESEARCH METHODOLOGY
A. Study Design
This is an observational study performed retrospectively.
B. Sample
The target population in this study is patients diagnosed with asthma
from the age of 1 to 90 years. Samples will be selected according to the
inclusion and exclusion criteria. Data will be collected retrospectively and
will be obtained from patients’ medical record from RSUP Dr. Sardjito,
Yogyakarta for 1 year (January 2013 – December 2013).
C. Sample Size
To determine the minimum sample size for this study, simple random
sampling method is used (Sudigdo et al, 1995).
To estimate sample size of a population, 3 information needed:
i. Disease proportion that to be found, P (from literature)
ii. Standard error needed. D (estimated)
iii. Confidence level, α (estimated)
Note:
P = 0.5, d = 0.10, zα = 1.960
n = (1.96)2 (0.5)(1-0.5) = 97
(0.1)2

35
Therefore, the minimal sample size is 97.
D. Inclusion Criteria
1. Patients from the age of 1 to 90 years who are having asthma.
2. Patients who received only out-patient treatment from RSUP Dr.
Sardjito.
3. Patients whose medical records have complete data.
E. Exclusion Criteria
1. Patients who are having COPD.
2. Unclear record of therapy.
3. Unclear record of examination and diagnosis.
4. Mistake in classification.
F. Course of Study
The course of study is carried out using 2 steps, which is:
1. Obtaining data based on medical records from the Medical Installation of
that specific hospital.
Data obtained from the patient’s medical records will consist of the
patient’s age, medical history and the history of drugs used. Besides that,
the drugs that are currently being used by the patient and its outcome is
also taken into account. All these data’s are made as the resources of this
study without having to choose a specific sampling method.
2. Analyzing and processing data.
Data obtained from this study will be analyzed descriptively through a
non- experimental design by analyzing with further details such as the

36
characteristic of asthmatic patient, treatment patterns and also the
outcome of the treatment plan.
D. Definition of Operational Variable
1. The asthmatic patients which are being studied are patients whom are
suffering from asthmatic and is currently obtaining their treatment from
RSUP Dr. Sardjito, Yogyakarta.
2. Patient medical record, health record, and medical chart are used
somewhat interchangeably to describe the systematic documentation of a
single patient's medical history and medical care across time. The
medical record includes a variety of types of "notes" entered over time by
health care professionals, recording observations and administration of
drugs and therapies, orders for the administration of drugs and therapies,
lab test results, x-rays, reports, etc.
3. The characteristics of asthmatic patients comprise of age, sex, history of
comorbid illness, occupation, residence, education level, complication,
degree of asthma, and medical history.
4. Treatment patterns are models or forms of therapies which is provided for
the asthmatic patients through local therapy (surgery or radiotherapy).
5. The outcome at the end of a therapy is the condition of the patient after
the treatment plan has ended, or the presence or absence of complains
from the patient and the side effects experienced by the patient after
receiving the treatment (post-treatment).

37
E. Data Analysis
Based on the data obtained from the treatment of Asthma in RSUP Dr.
Sardjito, it was further processed and analyzed as follow:
1. Characteristics of Asthma patient
The distribution of the total percentage were calculated from the
total number of patients according to the distribution of age of the patient,
sex, history of combined illness with asthma, complications, degree of
asthma, and medical history and its divided to the total number of
asthmatic patient which are being treated and being the subject of study
in RSUP Dr. Sardjito, Yogyakarta.
2. Treatment pattern for asthmatic patient
The patients will be divided into groups according to monotherapy
or polytherapy and each group will be analysed for the pattern of
antiasthmatic drug for asthma treatment. The analysis will be in the form
of descriptive according to the group of antiasthmatic drugs and
combination used for each group. Subsequently, the data will be analysed
by comparing the usage of antiasthmatic drugs by asthma patients with
standard guideline which included the parameter of right drugs, right dose
and right patients.
3. Outcome of therapy
Patients grouping were performed based on their therapy outcome
as in those who improved after receiving treatment were grouped as one
and the others who did not show any improvement after receiving therapy

38
and those who died were grouped in separate groupings respectively.
Thus, each groups were calculated the total amount of patient and divided
with the total amount of patients overall before grouping to obtain a
percentage. Side effects from surgery also were analyzed and the side
effects which occurs frequently by the patient is calculated. Furthermore,
patients were also grouped based on their level of control which are
controlled patients and uncontrolled patients where uncontrolled patients
experience exacerbations.

39
CHAPTER III
RESULTS AND DISCUSSION
A. Characteristics Of Asthma Patients
The data collection of this study took exactly two months. As it
was mentioned previously, the subjects of the study were outpatients with
RSUP Dr. Sardjito, Yogyakarta period 2013. A total number of 120
asthma patients have been used in this study. The subjects were matched
according to the inclusion and exclusion criteria as exact as possible.
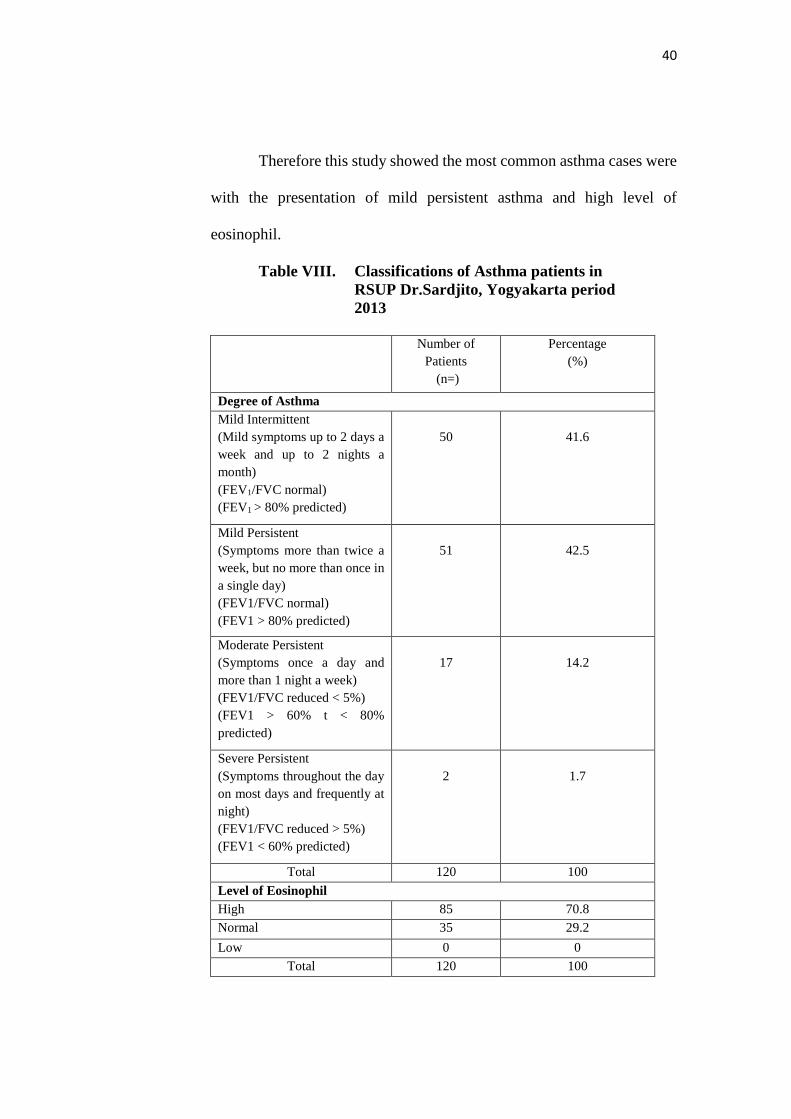
As can be seen in Table VIII, 120 patients were diagnosed with
asthma according to the degree of asthma and the presence of significant
eosinophil levels. Out of 120 patients, 41.6% (n=50) of them were with
mild intermittent asthma, 42.5% (n=51) patients with mild persistent
asthma, 14.2% (n=17) patients with moderate persistent and 1.7% (n=2)
patients with severe persistent asthma.
To strengthen the diagnosis of asthma, there must be the presence
of test for the levels of eosinophil. In this study out of 120 patients, 70.8%
(n=85) patients were with the level of high eosinophil, 29.2% (n=35)
patients with the level of normal eosinophil and 0% (n=0) with the level
of low eosinophil. Approximate equivalence to the above description are
high = more than 0 – 0.45 [103/µL] for adults, more than 0.2 – 0.3 [103/µL]
for infants aging 1 week to 6 months, more than 0.3 [103/µL] for infants
aging 1 year and more than 0 – 0.6 [103/µL] for children.
40
Therefore this study showed the most common asthma cases were
with the presentation of mild persistent asthma and high level of
eosinophil.
Table VIII. Classifications of Asthma patients in
RSUP Dr.Sardjito, Yogyakarta period
2013
Number of
Patients
(n=)
Percentage
(%)
Degree of Asthma
Mild Intermittent
(Mild symptoms up to 2 days a
week and up to 2 nights a
month)
(FEV1/FVC normal)
(FEV1 > 80% predicted)
50
41.6
Mild Persistent
(Symptoms more than twice a
week, but no more than once in
a single day)
(FEV1/FVC normal)
(FEV1 > 80% predicted)
51
42.5
Moderate Persistent
(Symptoms once a day and
more than 1 night a week)
(FEV1/FVC reduced < 5%)
(FEV1 > 60% t < 80%
predicted)
17
14.2
Severe Persistent
(Symptoms throughout the day
on most days and frequently at
night)
(FEV1/FVC reduced > 5%)
(FEV1 < 60% predicted)
2
1.7
Total 120 100
Level of Eosinophil
High 85 70.8
Normal 35 29.2
Low 0 0
Total 120 100

41
1. Age Group
The classifications of age among asthma patients in RSUP
Dr.Sardjito, Yogyakarta period 2013 is shown in Figure 5. This study
consists of 120 patients aged from 1 to 90 years old. This age range was
chosen because it is more likely for asthma to occur and are divided into
6 classes to differentiate the incidence of asthma.
Figure 5. Frequency and percentage of age group in
RSUP Dr.Sardjito, Yogyakarta period 2013
As can be seen on Figure 5 above, majority of patients belong to
the age group of 16-30 years old, 35.8% (n=43). This is gradually
followed by 31-45 years old with 22.5% (n=27), 46-60 years old with
18.3% (n=22), 61-75 years old with 13.3% (n=16), 1-15 years old with
8.3% (n=10) and finally 76-90 years old with 1.7% (n=2). From this
figure, it is clearly seen that asthma is more prone to occur in people
from the age group of 16-30 years old.
0
5
10
15
20
25
30
35
40
45
50
1 to 15 16 to 30 31 to 45 46 to 60 61 to 75 76 to 90
FREQ
UEN
CY
AGE
AGE

42
The National Health Interview Survey (NHIS) is a multi-purpose
health survey conducted by the National Center for Health Statistics
(NCHS), Centers for Disease Control and Prevention (CDC). It is the
principle source of information on the health of the civilian, non-
institutionalized, household population of the United States. Based on the
2011 NHIS sample, it was estimated that 39.5 million Americans, or
129.1 per 1,000 persons, had been diagnosed with asthma by a health
professional within their lifetime. Since 1999, children 5-17 years of age
have had the highest prevalence rates. In 2011, 8.7 million children ages
5-17 had been diagnosed with asthma in their lifetime (Anonymous,
2012d). Based on another study in Finland, there is a relationship between
age and the incidence of asthma where in the year 1996 to 1993, data was
collected from two national registers which cover practically all new cases
of occupational asthma and persistent asthma showed that the annual
incidence in the age group of 15 to 29 years increased by 87% (Reijula et
al., 1996). So, younger age is a common risk factor for asthma.
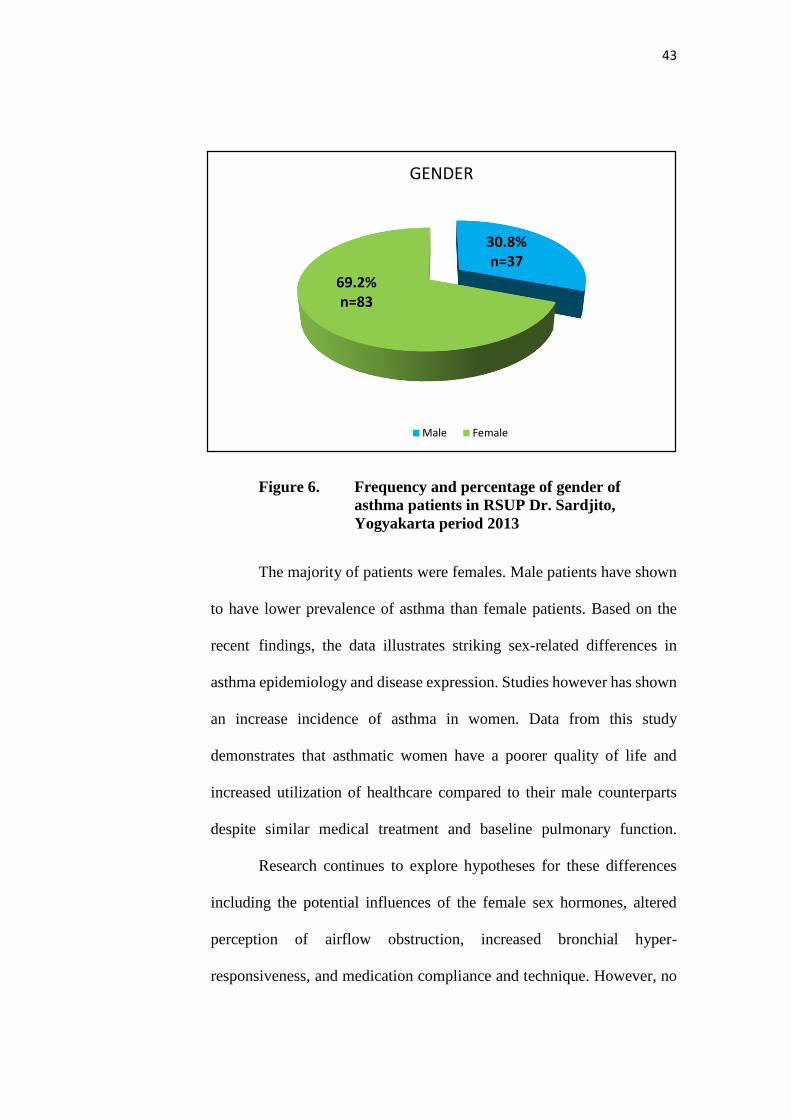
2. Gender
As Figure 6 shows below, it is obvious that the incidence of
asthma occurred more in female 69.2% (n=83).
43
Figure 6. Frequency and percentage of gender of
asthma patients in RSUP Dr. Sardjito,
Yogyakarta period 2013
The majority of patients were females. Male patients have shown
to have lower prevalence of asthma than female patients. Based on the
recent findings, the data illustrates striking sex-related differences in
asthma epidemiology and disease expression. Studies however has shown
an increase incidence of asthma in women. Data from this study
demonstrates that asthmatic women have a poorer quality of life and
increased utilization of healthcare compared to their male counterparts
despite similar medical treatment and baseline pulmonary function.
Research continues to explore hypotheses for these differences
including the potential influences of the female sex hormones, altered
perception of airflow obstruction, increased bronchial hyper-
responsiveness, and medication compliance and technique. However, no
30.8%n=37
69.2%n=83
GENDER
Male Female

44
single explanation has been able to fully explain the disparities. A 2009
National Health Interview Survey in the United States demonstrate a
prevalence of asthma in those less than 15 years of age of 11.9% in boys
and 7.7% in girls. In young adults aged 15 to 34 years, the pattern shifts,
with a prevalence of 6.3% in men and 9.6% in women. The difference
continues to widen in adults older than 35 years with prevalence of 5.6
versus 10.1% in men and women respectively (Kynyk et al., 2011).
3. Residence
As Figure 7 shows below, it is obvious that the incidence of
asthma occurred more in rural residence 64.2% (n=77).
Figure 7. Frequency and percentage of residence in
asthma patients in RSUP Dr. Sardjito,
Yogyakarta period 2013
The majority of patients were from ruralized area. Urban residents
have shown to have lower prevalence of asthma than rural residents. This
35.8%n=43
64.2%n=77
RESIDENCE
URBAN RURAL

45
could be due to the beneficial effect of the air humidity, effect of physical
activity, a more sedentary lifestyle, the level of education, the level of
hygiene in the area and a level of stress among the urbanized residents.
4. Types of Occupation
Figure 8 shows that out of 120 patients in RSUP Dr. Sardjito,
29.2% (n=35) were privates. Private has the highest percentage among
other occupations. Due to incomplete information in the patient’s medical
record, it is unclear if the privates were doing any other jobs to earn extra
income for the family and most probably the privates has higher
workloads compared to other occupation thus causing increase in the
stress level causing them to be more prone to asthma.
Figure 8. Frequency and percentage of types of
occupation in asthma patients in RSUP Dr.
Sardjito, Yogyakarta period 2013
23.3%
27.5%29.2%
2.5%
17.5%
0
5
10
15
20
25
30
35
Housewife Student Private Farmer Unknown
FR
EQ
UE
NC
Y
OCCUPATION
OCCUPATION
46
Even though some authors have not found any difference in
asthma outcomes between privates and other occupations, most
publications state that workers have adverse outcomes. Based on an
article by the American Lung Association State of Lung Diseases in
Diverse Communities published in the year 2010 which included four
states in their study which are California, New Jersey, Massachusetts, and
Michigan which tracked cases of occupational asthma over a seven-year
period. During this time, the occupations with the highest percentage of
asthma cases were operators, fabricators, and laborers (32.9%) where they
were most associated with miscellaneous chemicals (19.7%), cleaning
materials (11.6%), mineral and inorganic dust (11.1%) and indoor air
pollutants (9.9%) (Anonymous, 2010b). Therefore we can say that most
probably the patients from RSUP Dr. Sardjito suffering from asthma who
are working in the private sector has the highest percentage of incidence
most probably due to higher association with asthma allergens.
5. Obesity and Overweight
According to the Figure 9 below, showed out of 120 asthma
patients in RSUP Dr. Sardjito, Yogyakarta period 2013 41.7% (n=50)
were in the normal body mass index (BMI), followed by overweight
37.5% (n=45), underweight 15% (n=18) and lastly obese 5.8% (n=7).

47
Figure 9. Frequency and percentage of the body mass
index in asthma patients in RSUP Dr. Sardjito,
Yogyakarta period 2013
Based on a recent study in the United States, the rate of asthma
increased with increasing body mass index (BMI), with obese man or
women having the highest incidence. Compared with normal weight
people, obese people (BMI ≥ 30 kg/m2) had a higher risk for asthma.
Based on a study done is Brazil, it is observed that asthma causes
an alarming concomitant increase in obesity, which prevalence reaches
epidemic proportions (Saude et al., 2011). A survey data (POF
2008/2009) showed that asthma patients being overweight affects 50.1%
of men and 48% of adult women, and of that group, 12.4% of men and
16.9% of women are obese (IBGE et al., 2010). This is because, an
increasing body of literature suggests that there is an association between
obesity and asthma (Nystad et al., 2004). Moreover, studies report that
15%
41.7%
37.5%
5.8%
0
10
20
30
40
50
60
Underweight Normal weight Overweight Obese
FREQ
UEN
CY
BMI
BMI

48
individuals with persistent asthma are significantly limited in the practice
of physical activity, thus reducing energy expenditure, a fact that
contributes to the growing increase in the prevalence of overweight and
obesity (Ford et al., 2005).
Based on my study in asthma patients in RSUP Dr. Sardjito, the
highest number of patients were from the normal body mass index (BMI)
which ranged from 18.5 – 24.9 kg/m2 and this does not tally with the
previous studies. Most probably this is because, most of the asthma
patients in RSUP Dr. Sardjito are from the rural areas and can be
considered as low income people and are not able to spend a lot of money
on food and having heavy workload to earn little amount of money
causing them to have a normal body mass index (BMI) or low body mass
index (BMI) where the underweight (<18.5 kg/m2) and normal as stated
above.
B. Complications in Asthma
Based on an article published in Medline Plus there are certain
possibilities of complications occurring in an asthma patient. The
complications of asthma as stated can be severe and may include death,
decreased ability to exercise and take part in other activities, lack of sleep
due to nighttime symptoms, permanent changes in the function of the
lungs, persistent cough and trouble breathing that requires breathing
assistance such as ventilator (Busse, 2013).
49
However, the study performed were done retrospectively and thus
no interview with the patients were required to obtain the quality of life
of the patients from RSUP Dr. Sardjito and the data were just collected
based on the medical records of the patients. Therefore precise
information of whether there were decreased ability to exercise or lack of
sleep due to nighttime symptoms and other complications were not able
to be obtained. Besides that, based on the medical records, there were no
deaths recorded due to complications in RSUP Dr. Sardjito thus shows us
a 0% (n=0) mortality rate due to asthma complications. On the other hand,
the lack of complete data of the follow ups and visits to the hospital in the
medical record of RSUP Dr. Sardjito was a limiting factor to conduct
further analysis on the complications of asthma.
C. Asthma with other Combined Illness
Figure 10 shows that, out of 120 patients 78 patients were reported
to have combined illness with asthma in RSUP Dr. Sardjito, Yogyakarta.
Hypertension has the highest percentage among the group with 25.8%
(n=31). Hypertension is defined as systolic blood pressure of > or = 140
mmHg and or diastolic blood pressure of > or = 90 mm Hg.

50
Figure 10. Percentage of asthma patients with combined
illness in RSUP Dr. Sardjito, Yogyakarta period
2013
Based on a study, it is stated that both asthma and hypertension
are spastic disorders of smooth muscle, also asthmatics and hypertensives
have been found to be salt sensitive. Therefore, there is a suspicion that
the similarities between these two diseases may predispose the individuals
with one disease to the other, as pulmonary hypertension has been
described during exercise-induced bronchoconstriction. In this study, the
blood pressure pattern during and after acute severe asthma (ASA) along
with the frequency of hypertension in stable asthmatic patients were
studied. Two groups of patients were studied. Group 1 consisted of 12
patients with ASA (2 males, 10 females) with a mean age of 30 +/- 9.9
years. The mean blood pressure during attack of ASA (147 +/- 16.9/100
+/- 8.2 mmHg) was higher than the mean BP (132 +/- 8.3/82 +/- 7 mmHg)
25.80%
6.70%
20.80%
11.70%
8.30%
7.50%
5.80%
35%
Hypertension
Diabetes Mellitus Type 2
Brochitis
Allergic Rhinitis
Heart Diseases
GERD
Dislipidemia
None
CO
MB
INED
ILLN
ESS
Percent (%)

51
2 weeks after discharge from hospital without treatment in all patients (P
< 0.05). Group 2 included 134 asthmatic subjects in stable state (54 males,
80 females) with a mean age of 45 +/- 15 years and a range of 15-90 years.
The overall frequency of hypertension was 37% with a proportion of 39%
in males and 35% in females. There was no difference between the
frequency of attack of ASA in hypertensives (5.7 +/- 5.6 per year) and
non-hypertensives (5.5 +/- 3.8 per year), P < 0.05. From that, it was
concluded that the transient elevation of blood pressure may occur during
ASA. This shows that the frequency of hypertension among asthmatics is
quite high (Salako et al, 2000).
Besides that there are also stress induced asthma, therefore due to
high levels of stress can cause increase in the incidence of hypertension
due to increase in blood pressure.
Based on another study performed in Italy, a population-based
retrospective study using information obtained from the Health Search
Database (HSD) showed that asthma appeared to be also associated with
cardiovascular and hypertensive diseases as hypertension was the second
highest at 28.33% in the demographic characteristics of study population
by prevalence of comorbidities. Although asthma appeared to be weakly
associated with cardiovascular and hypertensive diseases and more
strongly associated with gastro-oesophageal reflux disease (GORD) and,
particularly, allergic rhinitis, it doesn’t mean that the disease prevalence
is not significant thus most probably the focus of study for comorbid

52
illness associated with asthma were more focused on diseases related to
the respiratory system such as bronchitis, allergic rhinitis and pneumonia
and the side effects of the use of anti-asthmatic drug such as theophylline
which is more responsible to the cause of GORD and the higher
prevalence of this disease (Cazzola et al, 2010).
D. Treatment And Management Of Asthma
Below are the results of 120 asthma patients in RSUP Dr. Sardjito,
Yogyakarta period 2013 during their visits to the hospital as outpatients:
1. Pattern of anti-asthmatic therapy based on monotherapy or
polytherapy
Data was taken by observing the pattern of anti-asthmatic
therapy in outpatients and are presented in Figure 11. The main
purpose here is to evaluate the differences in the pattern of therapy
among outpatients. From Figure 11 out of 120 asthma patients
during outpatient, 81.7% (n=98) were on polytherapy (consuming
two or more drugs) while 18.3% (n=22) were on monotherapy
(consuming a single drug). This study shows that most asthmatic
patients are on polytherapy.
The main aim of asthma management is control of the
disease. Therefore complete control of asthma can be defined as
no daytime symptoms, no night-awakening due to asthma, no need
for rescue medication, no exacerbations, no limitations on activity
including exercise, normal lung function (in practical terms FEV1

53
and/or PEF >80% predicted or best) and minimal side effects from
medication (Anonymous, 2012b). Therefore this study shows
that polytherapy is more frequently utilized than monotherapy.
Figure 11. Pattern of therapy in asthma patients in
RSUP Dr. Sardjito, Yogyakarta period
2013
There is a small number of patients on monotherapy and
this could be due to the number of asthma attacks occurred and
how controlled the asthma is in the patients and most probably due
to the effectiveness of a single drug to control the symptoms of
asthma. For patients without underlying medical problems, anti -
asthmatics drug therapy should be used to keep the asthma
symptoms under control as in less number of symptom episodes
per week, less number of nocturnal symptoms per month, and
improvement in the lung function (Anonymous, 2012a).
81.7%
n=98
18.3%
n=22
Type of Therapy
Polytherapy Monotherapy

54
Table IX. Single anti-asthmatics according to group given
to asthma patients in RSUP Dr. Sardjito,
Yogyakarta period 2013
Agent Frequency
(n=)
Percentage
(%)
Glucocorticosteroid
1. Inhaled Corticosteroid
2. Systemic Corticosteroid
69
33
57.5
27.5
Long Acting Beta2-Agonist 35 29.2
Short Acting Beta2-Agonist 99 82.5
Theophylline 52 43.3
For patients without underlying medical problems, anti-asthmatics
drug therapy should be used to keep the asthma symptoms under control
as in less number of symptom episodes per week, less number of
nocturnal symptoms per month, and improvement in the lung function
(Anonymous, 2012a).
In RSUP Dr. Sardjito, short acting beta2-agonist (SABA) was
administered 82.5% (n=99) if the asthma symptoms occurred and act as
relievers in the form of nebulizers or metered dose inhalers (MDI)/spacer
with dosage of 2 to 4 puffs as needed for symptoms every 4 to 6 hours
depending on the severity.
Based on an article in WebMD, it was stated that short-acting
beta2-agonists are bronchodilators and they relax the muscles lining the
airways that carry air to the lungs (bronchial tubes) within 5 minutes. This

55
increases airflow and makes it easier to breathe. They relieve asthma
symptoms for 3 to 6 hours. This group is most used due to the quick relief
symptoms that it provides during asthma attacks and acts as a reliever
before other steps could be taken. Furthermore, it is also stated that fewer
side effects are caused throughout the body than the oral forms
(Anonymous, 2012e). Examples of short acting beta2-agonists used in
RSUP Dr. Sardjito are albuterol/salbutamol, terbutaline and levalbuterol.
In this study, it is observed that inhaled corticosteroid was
administered 57.5% (n=69) in the form of nebulizers and inhalers with the
dosage varying on the severity of the disease, the drugs and the age of the
patient as in there is an adult dose for ≥12 years old and child dose for
<12 years old. The types of inhaled corticosteroid commonly used in
RSUP Dr. Sardjito were Budesonide DPI (Pulmicort Turbuhaler), and
Fluticasone DPI (Flixotide).
In this study, theophylline was administered 43.3% (n=52) in the
form of tablet and a dosage of 150 mg with frequency of three times a
day.
Besides that, long acting beta2-agonist were also one of the drug
groups administered by patients in RSUP Dr. Sardjito 29.2% (n=35) in
the form of nebulizers and inhalers with the dosage varying on the severity
of the disease, the drugs and the age of the patient as in there is an adult
dose for ≥12 years old and child dose for <12 years old. The types of long
56
acting beta2-agonists commonly used in RSUP Dr. Sardjito is formoterol
DPI and salmeterol DPI.
Lastly but not least, systemic corticosteroid was administered
27.5% (n=33) in the form of tablet and a dosage of 8, 16, and 32 mg
with frequency of three to four times a day depending on severity of the
disease.
2. Comparison with British Guideline on the Management of
Asthma 2012: A national clinical guideline
As based on the 2012, British Guideline On The
Management Of Asthma, there are several steps in controlling
asthma symptoms. As for step one which is known as the mild
intermittent asthma, the first drug of choice are the following
medications which act as short-acting bronchodilators which are
inhaled short-acting inhaled short-acting β2 agonists, inhaled
ipratropium bromide (anticholinergics), β2 agonists tablets or
syrup and theophylline. These short acting β2 agonists work more
quickly and/or with fewer side effects than the alternatives. Using
short-acting β2 agonists as required is at least as good as regular (four
times a day) administration. Good asthma control is associated with little
or no need for short-acting β2 agonist. Using two or more canisters of
β2 agonists per month or >10-12 puffs per day is a marker of poorly
controlled asthma that puts patients at risk of fatal or near-fatal asthma.

57
Therefore patients should have their asthma management reviewed
(Anonymous, 2012b).
As for step two, three, and four, treatments have been judged
on their ability to improve symptoms, lung function, and prevent
exacerbations, with an acceptable safety profile. Step two states the
introduction of regular preventer therapy for an asthma patient. In this
step, inhaled steroids can be said as the most effective preventer drug for
adults and older children for achieving overall treatment goals. There is
increasing body of evidence demonstrating that, at recommended
doses, they are also safe and effective in children under five years with
asthma. Inhaled steroids should be considered for adults, children aged 5-
12 and children under the age of five with any of the following features:
using inhaled β2 agonists three times a week or more; symptomatic three
times a week or more; or waking one night a week. In addition, inhaled
steroids should be considered in adults and children aged 5-12 who have
had an exacerbation of asthma requiring oral corticosteroids in the last
two years. In a mild to moderate asthma, starting at very high doses of
inhaled steroids and stepping down confers no benefit, therefore it is said
that patients should be started with a dose of inhaled steroids which is
appropriate to the severity of the disease. In adults, a reasonable starting
dose will usually be 400 micrograms BDP per day and in children 200
micrograms BDP per day. In children under five years, higher doses may
be required if there are problems in obtaining consistent drug delivery.

58
Later the dose of inhaled steroid should be titrated to the lowest dose at
which effective control of asthma is maintained. Regarding the frequency
of dosing of inhaled steroids, most current inhaled steroids are slightly
more effective when taken twice rather once daily, but may be used once
daily in some patients with milder disease and good or complete control
of their asthma (Anonymous, 2012b) .
Comparing the types of inhaled steroids, BDP and budesonide
are approximately equivalent in clinical practice, although there may be
variations with different delivery devices. There is limited evidence from
two open studies of less than ideal design that budesonide via the
turbohaler is more clinically effective. However, at present a 1:1 ratio
should be assumed when changing between BDP and budesonide.
Fluticasone provides equal clinical activity to BDP and budesonide at half
the dosage. The evidence that it causes fewer side effects at doses with
equal clinical effect is limited. Mometasone appears to provide equal
clinical activity to BDP and budesonide at half the dosage. The relative
safety of mometasone is still not fully established.
Based on Table X below, it shows the types of inhaled
steroids with its equivalent doses and the current licensed age
indications. The safety of inhaled steroids for adults shows that there is
little evidence that doses below 800 micrograms BDP per day cause any
short term detrimental effects apart from the local side effects of
dysphonia and oral candidiasis. However, the possibility of long term
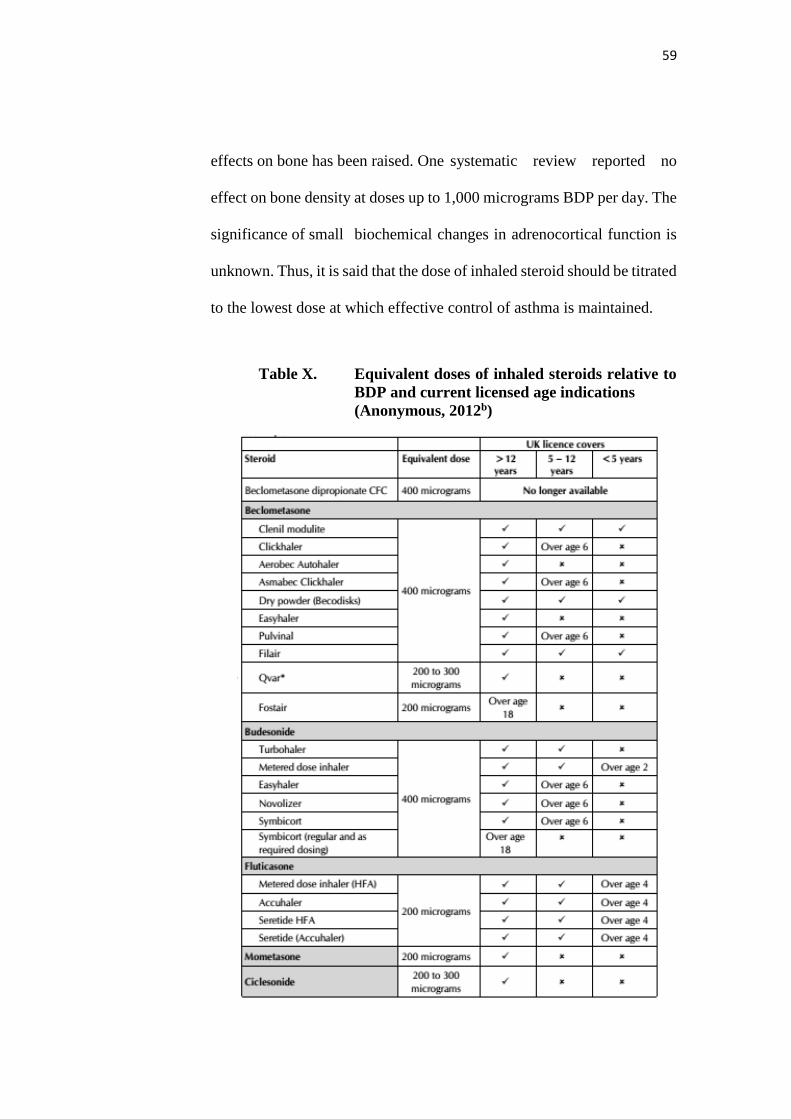
59
effects on bone has been raised. One systematic review reported no
effect on bone density at doses up to 1,000 micrograms BDP per day. The
significance of small biochemical changes in adrenocortical function is
unknown. Thus, it is said that the dose of inhaled steroid should be titrated
to the lowest dose at which effective control of asthma is maintained.
Table X. Equivalent doses of inhaled steroids relative to
BDP and current licensed age indications
(Anonymous, 2012b)
60
Based on this guideline, it is also stated that administration of
inhaled steroids at or above 400 micrograms BDP a day or equivalent
may be associated with systemic side effects. These may include growth
failure and adrenal suppression. Isolated growth failure is not a
reliable indicator of adrenal suppression and monitoring growth cannot be
used as a screening test of adrenal function. Clinical adrenal insufficiency
has been identified in a small number of children who have become
acutely unwell at the time of intercurrent illness. Most of these children
had been treated with high doses of inhaled corticosteroids. The dose or
duration of inhaled steroid treatment required to place a child at risk of
clinical adrenal insufficiency is unknown but is likely to occur at ≥800
micrograms BDP per day or equivalent. The low-dose ACTH test is
considered to provide a physiological stimulation of adrenal
responsiveness but it is not known how useful such a sensitive test is at
predicting clinically relevant adrenal insufficiency. In addition, it is
unknown how frequently tests of adrenal function would need to be
repeated if a child remained on high-dose inhaled corticosteroid. At
higher doses, add-on agents, for example, long-acting β2 agonists, should
be actively considered. While the use of inhaled corticosteroids may be
associated with adverse effects (including the potential to reduced bone
mineral density) with careful inhaled steroid dose adjustment, this risk is
likely to be outweighed by their ability to reduce the need for multiple
bursts of oral corticosteroids. Due to this, there should be monitoring of

61
the growth (height and weight centile) of the children with asthma on
annual basis. Furthermore, the lowest dose of inhaled steroids compatible
with the maintaining disease control should be used. As for children
treated with ≥ 800 micrograms BDP per day or equivalent, specific
written advice about steroid replacement (e.g. Steroid Alert Card) in the
event of a severe intercurrent illness or surgery should be part of the
management plan and the child should be under the care of a specialist
pediatrician for the duration of treatment (Anonymous, 2012b).
Other preventer therapies are also available but inhaled steroids
are the first choice preventer drug. It is also known that long-acting β2
agonists should not be used without inhaled corticosteroids. Patients
taking short-acting β2 agonists alone are a less effective preventer
therefore it is suggested that theophylline should be taken as well as
theophylline have some beneficial effect. Moreover, in children under
five years who are unable to take inhaled corticosteroids, leukotriene
receptor antagonists are an effective first line preventer (Anonymous,
2012b).
Step three states the initial add-on therapy for asthma treatment.
A proportion of patients with asthma may not be adequately controlled at
step two. Therefore, before initiating a new drug therapy, practitioners
should recheck adherence, inhaler technique and eliminate trigger factors.
The duration of a trial of add-on therapy will depend on the desired
outcome. For instance, preventing nocturnal awakening may require a

62
relatively short trial of treatment (days or weeks), whereas preventing
exacerbations of asthma or decreasing steroid tablet use may require a
longer trial of therapy (weeks or months). If there is no response to the
treatment the drug should be discontinued. Options for add-on therapy are
summarized in Figure 12 below (Anonymous, 2012b).
Figure 12. Summary of the Add-on therapy in adults and
children > 5 years (Anonymous, 2012b)
Following a review in 2007 of LABA in the treatment of adults,
adolescents, and children with asthma, the Medicines and Healthcare
products Regulatory Agency (MHRA) further reviewed the use of LABA,
specifically in children younger than age 12 years and concluded that the
benefits of these medicines used in conjunction with inhaled
corticosteroids in the control of asthma symptoms outweigh any apparent
risks. Long-acting inhaled β2 agonists should only be started in patients
who are already on inhaled corticosteroids, and the inhaled corticosteroid

63
should be continued. In efficacy studies, where there is generally good
compliance, there is no difference in efficacy in giving inhaled steroid and
a long-acting β2 agonist in combination or in separate inhalers. In clinical
practice, however it is generally considered that combination inhalers aid
compliance and also have the advantage of guaranteeing that the long-
acting β2 agonist is not taken without the inhaled steroids.
As for step four, it is all about poor control on moderate dose of
inhaled steroid plus add-on therapy which means there is an addition of a
fourth drug. In a small proportion of patients, asthma is not adequately
controlled on a combination of short-acting β2 agonist as required, inhaled
steroid (800 micrograms BDP daily), and an additional drug, usually a
long-acting β2 agonist. There are very few clinical trials in this specific
patient group to guide management. The following recommendations are
largely based on extrapolation from trials of add-on therapy to inhaled
steroids alone. If control remains inadequate on 800 micrograms BDP
daily (adults) and 400 micrograms daily (children) with an inhaled steroid
plus a long-acting β2 agonist, the following interventions are considered
as in increasing inhaled steroids to 2000 micrograms BDP/day (adults) or
800 micrograms BDP/day (children 5-12 years), adding a leukotriene
receptor antagonists, a theophylline, and a slow release β2 agonist tablets,
though caution needs to be used in patients already on long-acting β2
agonists. There are no controlled trials indicating which one of these is
the best option, although the potential for side effects is greater with

64
theophylline and β2 agonist tablets. If a trial of an add-on treatment is
ineffective, stop the drug (or in the case of increased dose of inhaled
steroid, reduce to the original dose). Before proceeding to step five, the
patients with inadequately controlled asthma, especially children, should
be referred to specialist care.
The last but not least is step five which is about continuous
or frequent use of oral steroids. The aim of treatment is to control asthma
using the lowest possible doses of medication. Some patients with very
severe asthma which are not controlled at step four with high dose of
inhaled corticosteroids, and who have also been tried on or are still taking
long-acting β2 agonists, leukotriene antagonists or theophylline, require
regular long term steroid tablets. For the small number of patients not
controlled at step four, use daily steroid tablets in the lowest dose
providing adequate control. Figure 13 and 14 below summaries the
stepwise management in adults and children with asthma. As for steroid
formulations prednisolone and methyl prednisolone are the most widely
used steroid for maintenance therapy in chronic asthma. There is no
evidence that other steroids offer an advantage. Patients on long term
steroid tablets (e.g. longer than three months) or requiring frequent
courses of steroid tablets (e.g. three to four per year) will be at risk of
systemic side effects.

65
Figure 13. Stepwise management of Asthma in adults
(Anonymous, 2012b)

66
Figure 14. Stepwise management of Asthma in children
aged 5-12 years (Anonymous, 2012b)

67
Table XI. Combination of anti-asthmatics given to asthma
patients in RSUP Dr. Sardjito, Yogyakarta period
2013
Combinations Frequency
(n=)
Percentage
(%) SABA’s + Theophylline 13 12.7
SABA’s + SCS 7 6.9
LABA’s + ICS 9 8.8
ICS + Theophylline 2 2.0
SABA’s + ICS 12 11.7
SABA’s + Anticholinergic 1 1.0
SABA’s + Theophylline + Anticholinergic 1 1.0
SABA’s + LABA’s + Theophylline 2 2.0
SABA’s + ICS + SCS 8 7.8
SABA’s + ICS + Anticholinergic 1 1.0
SABA’s + SCS + Anticholinergic 2 2.0
SABA’s + ICS + Theophylline 10 9.8
SABA’s + SCS + Theophylline 5 4.9
LABA’s + SCS + ICS 1 1.0
LABA’s +ICS + Theophylline 4 3.9
LABA’s + SABA’s + ICS 7 6.8
LABA’s + SABA’s + ICS + Anticholinergic 1 1.0
SABA’s + LABA’s + Theophylline + SCS 1 1.0
SABA’s + LABA’s + Theophylline + ICS 6 5.8
LABA’s + ICS + SCS + Theophylline 1 1,0
SABA’s + ICS + SCS + Anticholinergic 3 2.9
SABA’s + ICS + SCS + Theophylline 1 1.0
ICS + SCS + Theophylline + Anticholinergic 1 1.0
SABA’s + LABA’s + ICS + SCS 1 1.0
SABA’s + LABA’s + ICS + SCS +
Theophylline
2 2.0
Total 102 100 *ICS = Inhaled Corticosteroid; SCS = Systemic Corticosteroid; SABA’s = Short-acting β2 Agonist;
LABA’s = Long-acting β2 Agonist.
As seen in Table 11 above, in terms of dual anti-asthmatic
therapy, the most widely used combination in RSUP Dr. Sardjito was
short-acting β2 agonist and theophylline, which represented around 12.7%
(n=13) of dual therapy combinations with dosage of short-acting β2
agonist which can vary from 2 to 4 puffs as needed for symptoms and up
to 3 treatments at 20-minute intervals or a single nebulizer treatment as
needed and theophylline 10 mg/kg/day.

68
Based on a recent study, a total of eight studies were included. In
comparing the effect of theophylline combined with beta2-agonists to that
of a placebo, we found a statistically significant improvement in mean
FEV1 (0.27 L; 95% CI: 0.11 to 0.43) and mean dyspnea (-0.78; 95% CI:
-1.26 to -0.29). None of the Meta analyses performed detected any
difference between the results obtained using theophylline combined with
beta2-agonists and those obtained using beta2-agonists alone. When the
administration of theophylline combined with beta2-agonists was
compared to that of theophylline alone, there was a statistically significant
improvement in mean dyspnea (0.19; 95% CI: -0.34 to 0.04) (Zacarias et
al, 2007).
The second highest combination therapy administered in RSUP
Dr. Sardjito was dual combination of short-acting β2 agonist with inhaled
corticosteroid 11.7% (n=12).
As for the triple combination therapy administered in RSUP Dr.
Sardjito, the highest was the combination of short-acting β2 agonist with
inhaled corticosteroid and theophylline 9.8% (n=10).
The addition of theophylline in a combination therapy may be
used as a long term controllers for asthma symptoms as a second or third-
line agent or in patients whose asthma control is still inadequate therefore
trial of other add-on therapy such as leukotriene receptor antagonist or
theophylline is suggested. It is also known that theophylline may improve

69
lung function and symptoms, but side effects occur more commonly
(Anonymous, 2012b).
There were also combination of four types of anti-asthmatic
agents used in RSUP Dr. Sardjito and the highest number of usage were
short-acting β2 agonist with long-acting β2 agonist with inhaled
corticosteroid and theophylline 5.8% (n=6). The addition of the fourth
drug is also due to inadequate control of asthma symptoms (Anonymous,
2012b).
Furthermore, there were also combination of five types of anti-
asthmatics from different groups which consist of short-acting β2 agonist
with long-acting β2 agonist with inhaled corticosteroid, systemic
corticosteroid as well as theophylline 2% (n=2). This treatment was most
probably due to exacerbation of the disease and only two patients were
prescribed with these combinations of five different groups of anti-
asthmatic.
Inhaled corticosteroid are mostly contraindicated in children < 2
years as we can see according to the guideline. Most of the inhaled
corticosteroid are only administered for patients over age 2 because
consuming these group of drugs for infants < 2 years of age might affect
their metabolic organs such as liver due to the lack of full organ function.
Besides that, corticosteroids can also cause systemic side effects such as
growth failure and adrenal suppression (DiPiro et al, 2009).

70
Therefore, since there were one prescription involving inhaled
corticosteroids it can be considered as high risked decision taken by the
responsible physician in RSUP Dr. Sardjito, Yogyakarta.
E. Management On Prevention Of Asthma
Prevention of asthma can be performed by performed by surgery
which is also known as bronchial thermoplasty. This is a new concept in
the management on prevention of asthma, where aims to reduce the
airway smooth muscle (ASM) mass with the goal of diminishing
bronchial constriction and ameliorating asthma symptoms (Wahidi et al,
2011).
Sadly, this procedure has not reached this country and therefore
none have performed the surgery. Therefore, it couldn’t be analyzed
further due to insufficient resources and data.
F. Outcome of Therapy
Since the ultimate treatment for asthma is the control and
management of the symptoms and the quality of life besides
administration of anti-asthmatic drugs, based on Figure 15 within the
visits as outpatient in RSUP Dr. Sardjito 60.8% (n=73) controlled
symptoms were reported and has the highest percentage of outcome.

71
Figure 15. Frequency and percentage on outcome of
therapy in asthma patients in RSUP Dr.
Sardjito, Yogyakarta period 2013
This is followed by uncontrolled 35% (n=42) and 4.2% (n=5) for
non-stated outcomes respectively. Controlled outcomes can be defined as
when there is no daytime symptoms, no night-time awakening due to
asthma, no need for rescue medication, no exacerbations, no limitations
on activity including exercise, normal lung function and minimal side
effects from medication.
Based on a study, the relationship between baseline ACQ-5 and
exacerbations was investigated. A Markov analysis examined the
transitional probability of change in control status throughout the studies.
From this study, the percentage of patients achieving asthma control
increased with time, irrespective of treatment; the percentage
Controlled/Partly Controlled at study end was at least similar to
budesonide/formoterol maintenance and reliever therapy versus the 3
60.8%
35%
4.2%
0
10
20
30
40
50
60
70
80
Controlled Uncontrolled Not Stated
Freq
uen
cy
Outcome
Outcome

72
maintenance therapies: higher dose ICS (56% vs 45%), same dose
ICS/LABA (56% vs 53%), and higher dose ICS/LABA (54% vs 54%).
Baseline ACQ-5 score correlated positively with exacerbation rates. A
Controlled or Partly Controlled week predicted at least Partly Controlled
asthma the following week (≥80% probability). The better the control, the
lower the risk of an uncontrolled week. The probability of an exacerbation
was related to current state and was lower with budesonide/formoterol
maintenance and reliever therapy (Bateman et al, 2010).
Outcome based on quality of life were not been able to be
evaluated due to the type of study carried out which was a retrospective
study and no questionnaire were done and used to carry out interviews to
obtain precise information on the improvement of the patients quality of
life.

73
CHAPTER IV
CONCLUSION AND SUGGESTIONS
A. Conclusion
1. During the 1st of January 2013 to 31st December 2013, common
risk factors of asthma found were at the age of 16 to 30 years
35.8%, gender 69.2% for females, residence 64.2% for rural
residency, and occupation 29.2% for privates. Uncommon risk
factors found were obesity.
2. Evaluation of treatment in asthma patients showed results of
81.7% patients were under polytherapy with the most common
dual anti-asthmatics which are short-acting β2 agonist +
theophylline 12.7% as the most common combination anti-
asthmatic drugs given.
3. Management on prevention of asthma is through the procedure of
having a surgery called Bronchial Thermoplasty but due to
insufficient technology in this country, this procedure is yet to be
introduced therefore it cannot be evaluated.
4. Overall, the drug pattern and management of asthma patients in
RSUP Dr. Sardjito, Yogyakarta were correct according to the
British Guideline On Management Of Asthma (2012) with
outcome therapy of 60.8% controlled symptoms but there were
several high risked decision taken by the responsible physician in

74
RSUP Dr. Sardjito, Yogyakarta prescribing inhaled corticosteroid
for an infant below the age of 2 years.
B. Suggestions
1. For future researcher
For this study it is best to be performed as prospective
study because data collected will be more accurate and
researcher will have detailed information about patient’s
condition.
2. For hospital
a. Regarding the patient’s medical record, physicians should
write in detail of patient’s characteristics, such a family
history and outcome after receiving treatment as the lack
of complete data limits further analysis on risk factors.
This will help researchers in future to obtain complete data
and significant risk factors.
b. Physicians should also fill the treatment and management
sheet with great detail and not leaving any detail blank for
example pharmaceutical form of drugs given. This will help
researchers to understand physicians’ choices and decisions.
75
BIBLIOGRAPHY
Anonymous, 2005, Clinical Guideline for the Diagnosis, Evaluation, and
Management of Adults and Children with Asthma, retrieved from
www.health.ny.gov/diseases/asthma/pdf/2005_asthma_guidelines.pdf,
29th November 2013.
Anonymous, 2007a, World Health Organization (WHO). Global surveillance,
prevention and control of chronic respiratory diseases: a comprehensive
approach, 2007.
Anonymous, 2007b, National Asthma Education and Prevention Program Exper
panel Report 3. Guidelines for the Diagnosis and Management of Asthma,
NIH Publication Number 08-5846, retrieved from
http://www.nhlbi.nih.gov/guidelines/asthma/asthsumm.pdf , 26
November 2013.
Anonymous, 2010a, Asthma Medicine Care Guide, retrieved from
https://host1.medcohealth.com/art/corporate/pdf/Asthma_Medicines_Ca
re_Guide.pdf , 28th November 2013.
Anonymous, 2010b, Occupational Lung Disease, American Lung Association
State of Lung Disease in Diverse Communities 2010, retrieved from
http://www.lungusa.org 1-800-LUNG-USA , 24th March 2014.
Anonymous, 2011, World Allergy Organization (WAO) White Book on
Allergy, retrieved from
http://www.worldallergy.org/UserFiles/file/WAO-White-Book-on-
Allergy_web.pdf , 29th November 2013.
Anonymous, 2012a, Clinical Practice Guideline for Providers: Management of
Asthma in Children and Adults, retrieved from
https://www.wellcare.com/WCAssets/corporate/assets/HS1001CPG_Ast
hma.pdf , 29th November 2013.
Anonymous, 2012b, British Guideline on the Management of Asthma, A
national clinical guideline, retrieved from http://www.brit-
thoracic.org.uk/Portals/0/Guidelines/AsthmaGuidelines/sign101%20Jan
%202012.pdf , 28th November 2013.
Anonymous, 2012c, Global Initiative For Asthma. Pocket Guide For Asthma
Management And Prevention (for Adults and Children Older than 5
Years), retrieved from
http://www.ginasthma.org/local/uploads/files/GINA_Pocket2013_May1
5.pdf , 29th November 2013.

76
Anonymous, 2012d, Trends in Asthma Morbidity and Mortality, American
Lung Association, Epidemiology and Statistics Unit, Research and Health
Education Division retrieved from http://www.lung.org/finding-
cures/our-research/trend-reports/asthma-trend-report.pdf , 23rd March
2014.
Anonymous, 2012e, Bronchodilators and Asthma, retrieved from
http://www.webmd.com/asthma/guide/asthma_inhalers_bronchodilators,
21st March 2014.
Bateman E.D, Reddel H.K, Eriksson G, Peterson S, Ostlund O, Harrison T.W,
Quirce S, O’Byrne P.M, 2010, Overall asthma control: The relationship
between current control and future risk, J Allergy Clin Immunol, Volume
125, Number 3, retrieved from
http://download.journals.elsevierhealth.com/pdfs/journals/0091-
6749/PIIS0091674909017709.pdf , 13th April 13, 2014.
Busse P.J, MD, 2013, Asthma, retrieved from http:// http://www.nlm.nih.gov/medlineplus/ency/article/000141.htm , 13th
April 2013.
Cazzola M, Calzetta L, Bettoncelli G, Novelli L, Cricelli C, Rogliani P., 2010,
Asthma and comorbid medical illness, Eur Respir J 2011; 38: 42-49.,
ISSN 1399-3003.
Crosta P., 2013: All about Asthma- Types of Asthma, retrieved from
http://www.medicalnewstoday.com/info/asthma/types-of-asthma.php ,
29th November 2013.
Dipiro, J.T., Wells B.G., Schwinghammer, T.L., Dipiro, C.V., 2008,
Pharmacotherapy A Pathophysiologic Approach 7th Ed., 2121-2153, Mc
Graw Hill, United States.
Dipiro, J.T., Wells B.G., Schwinghammer, T.L., Dipiro, C.V., 2009,
Pharmacotherapy Handbook 7th Edition, 679-688, Mc Graw Hill, United
States.
Ford ES., 2005, The epidemiology of obesity and asthma. J Allergy Clin
Immunol. 2005;115:897-909.
IBGE. Instituto Brasileiro de Geografia e Estatística. Análise da disponibilidade
domiciliar de alimentos e do estado nutricional no Brasil: pesquisa de orc¸
amentos familiars 2008-2009. Rio de Janeiro; 2010.
Kim H., Mazza J., 2011. Asthma. Allergy, Asthma & Clinical Immunology 2011
7(Suppl 1):S2, retrieved from

77
http://www.aacijournal.com/content/pdf/1710-1492-7-S1-S2.pdf , 29th
November 2013.
Kynyk J.A, Mastronarde J.G, McCallister J.W, 2011, Asthma, the Sex
Difference, Curr Opin Pulm Med. 2011;17(1):6-11.
Longo D.L, Fauci A.S, Kasper D.L, Hauser S.L, Jameson J.L, Loscalzo J, 2012,
Harrison’s Principles of Internal Medicine 18th Edition Volume 2, ISBN
978-0-07-174887-2 (vol. 2).
Margolis S., 2006. John Hopkins Symptoms and Remedies. The Complete
Home Medical Reference, ISBN 1-933087-16-1.
Nystad W, Meyer HE, Nafstad P, Tverdal A, Engeland A., 2004, Body mass
index in relation to adult asthma among 135,000 Norwegian men and
women. Am J Epidemiol. 2004;160:969-76.
Reijula K, MD; Haahtela T, MD; Klaukka T, MD; Rantanen J, MD., 1996,
Incidence of Occupational Asthma and Persistent Asthma in Yong Adults
Has Increased in Finland, CHEST 1996; 110:58-61.
Sastramihardja, S., 1997, Penggunaan Obat Rasional di Tempat Pelayanan
Kesehatan, Majalah Kedokteran Indonesia, 47:4 532-536.
Salako B.L, Ajayi S.O, 2000, Bronchial asthma: a risk factor for hypertension?,
Afr J Med Med Sci. 2000 Mar;29(1):47-50, retrieved from http:// http://www.ncbi.nlm.nih.gov/pubmed/11379468 , 21 March 2013.
Portal da Saude, 2011, Ministerio da Saude [citado 2 set 2011], retrieved from
http://portal.saude.gov.br , 13th April 2014.
Sveum R, Bergstrom J, Brottman G, Hanson M, Heiman M, Johns K,
Malkiewicz J, Manney S, Moyer L, Myers C, Myers N, O’Brien M,
Rethwill M, Schaefer K, Uden D., 2012. Institute for Clinical Systems
Improvement. Diagnosis and Management of Asthma. Updated July
2012.
Sudigdo,S., Bambang, M., Sunoto, P., Alan, R., 1995, Perkiraan Besar Sampel, Dasar-dasar Methodologi Penelitian Klinis, Binarupa Akasara, Jakarta.
Wahidi, M.M., Kraft M., 2011, Concise Clinical Review- Bronchial
Thermoplasty for Severe Asthma. Division of Allergy, Pulmonary, and
Critical Care Medicine, Department of Medicine, Duke University
Medical Center, Durham, North Carolina. Originally Published in Press
as DOI: 10.1164/rccm.201105-0883CI on November 10, 2011.
Zacarias E.C, Castro A.A, Cendon S., 2007, Effect of theophylline associated
with short-acting or long-acting inhaled beta2-agonists in patients with

78
stable asthma: a systematic review, J Bras Pneumil. 2007 Mar-
Apr;33(2):152-60.













![FUTURE ASTHMA RISK: Using real-life patient records to help … · approximately 350,000 patients with asthma (and 100,000 patients with chronic obstructive pulmonary disease [COPD])](https://static.fdocuments.us/doc/165x107/5cd8e64288c99341128c90bb/future-asthma-risk-using-real-life-patient-records-to-help-approximately-350000.jpg)



