THE CHALLENGE OF THE THIRD SECTOR: THE ROLE OF CIVIL SOCIETY IN HEALTH SYSTEMS REFORMS Aalborg, 2...
35
THE CHALLENGE OF THE CHALLENGE OF THE THIRD SECTOR: THE THIRD SECTOR: THE ROLE OF CIVIL SOCIETY IN THE ROLE OF CIVIL SOCIETY IN HEALTH SYSTEMS REFORMS HEALTH SYSTEMS REFORMS Aalborg, 2 November 2012 Aalborg, 2 November 2012 Prof. Guido Giarelli Prof. Guido Giarelli Department of Health Sciences Department of Health Sciences University ‘Magna Gr University ‘Magna Gr æcia’ æcia’ Catanzaro - Italy Catanzaro - Italy
-
Upload
sandra-banks -
Category
Documents
-
view
212 -
download
0
Transcript of THE CHALLENGE OF THE THIRD SECTOR: THE ROLE OF CIVIL SOCIETY IN HEALTH SYSTEMS REFORMS Aalborg, 2...

THE CHALLENGE OF THE CHALLENGE OF THE THIRD SECTOR: THE THIRD SECTOR:
THE ROLE OF CIVIL SOCIETY IN THE ROLE OF CIVIL SOCIETY IN HEALTH SYSTEMS REFORMSHEALTH SYSTEMS REFORMS
Aalborg, 2 November 2012Aalborg, 2 November 2012
Prof. Guido GiarelliProf. Guido GiarelliDepartment of Health Sciences Department of Health Sciences
University ‘Magna GrUniversity ‘Magna Græcia’ æcia’ Catanzaro - ItalyCatanzaro - Italy

CONTENTSCONTENTS
1.1. The rethoric of the Third SectorThe rethoric of the Third Sector
2.2. Third Sector or Civil Society?Third Sector or Civil Society?
3.3. A theoretical framework A theoretical framework
4.4. The role of civil society in health The role of civil society in health system reformssystem reforms
5.5. Conclusions: beyond the Third Conclusions: beyond the Third Sector?Sector?

1. 1. The rethoric of the Third SectorThe rethoric of the Third Sector

Self-help/mutual aid in ItalySelf-help/mutual aid in Italy
The same historical pattern, but delayedThe same historical pattern, but delayed1.1. 1970s1970s: first groups, opposition by : first groups, opposition by
medical and health professionals, medical and health professionals, difficulties with the institutions difficulties with the institutions
2.2. 1980s1980s: growing interest, : growing interest, institutionalization of groups into institutionalization of groups into associations, facilitating role by health associations, facilitating role by health professionals, substitution role in the professionals, substitution role in the delivery of social-health servicesdelivery of social-health services
3.3. 1990s-1990s-: ‘second generation’ groups, crisis : ‘second generation’ groups, crisis of welfare system and increasing role in of welfare system and increasing role in the governance of social-health arenathe governance of social-health arena

2. Beyond consumerism: active 2. Beyond consumerism: active citizenship and civil societycitizenship and civil society
A classical definition:A classical definition:Small groups ‘usually formed by peers who have come Small groups ‘usually formed by peers who have come together for mutual assistance in satisfying a common together for mutual assistance in satisfying a common need, overcoming a common handicap or life-disrupting need, overcoming a common handicap or life-disrupting problem, and bringing about desired social and/or problem, and bringing about desired social and/or personal change’ personal change’ (Katz & Bender 1976)(Katz & Bender 1976)
2 main characteristics:1. the ‘circle of sharing’: experiential learning by sharing of
personal stories of suffering to change the situation2.2. a pro-active orientation based on the a pro-active orientation based on the helper principle:helper principle: ‘ ‘You alone can do it, but you cannot do it alone’ You alone can do it, but you cannot do it alone’
(Riessman, 1965) (Riessman, 1965)

THE CONSUMERIST PARADIGMTHE CONSUMERIST PARADIGM The mainstream The mainstream consumerist paradigmconsumerist paradigm considers considers
the citizen as a the citizen as a consumerconsumer of medical care and of medical care and focuses on consumer’s focuses on consumer’s choicechoice in order to make in order to make social/health services more responsive to social/health services more responsive to consumers and to improve their qualityconsumers and to improve their quality
but ‘choice’ is within professionally/managerially but ‘choice’ is within professionally/managerially defined healthcare servicesdefined healthcare services
a market perspective & an individualised focus a market perspective & an individualised focus rooted in the dominant idelogical neo-liberal rooted in the dominant idelogical neo-liberal economy and policy trend economy and policy trend
‘‘consumer’s sovereignty or ‘supermarket model’? consumer’s sovereignty or ‘supermarket model’?

THE ACTIVE CITIZENSHIP THE ACTIVE CITIZENSHIP PARADIGMPARADIGM
A new emergent paradigm focused on the A new emergent paradigm focused on the personperson as a human being and not a role and as a human being and not a role and the the citizencitizen with rights and responsibilities with rights and responsibilities
the idea of ‘the idea of ‘active citizenactive citizen’ as ’ as the active citizen is athe active citizen is a co-producerco-producer of health of health
along with professionals allows patient-along with professionals allows patient-practitioner relationship to become a kind of practitioner relationship to become a kind of partnershippartnership
‘‘citizenship associations’ as a means to foster a citizenship associations’ as a means to foster a new new participatory-democraticparticipatory-democratic concept of concept of active active health citizenshiphealth citizenship in the governance of the in the governance of the health arena enhancing citizens’ political health arena enhancing citizens’ political awareness and empowerment (awareness and empowerment (community community health governancehealth governance))

2 key-concepts in the 2 key-concepts in the backgroundbackground
1.1. Civil societyCivil society: a significant historical evolution in : a significant historical evolution in Western thought from designating the political Western thought from designating the political sphere (polis) through the identification with the sphere (polis) through the identification with the market in liberal & Marxian thought, to a sphere market in liberal & Marxian thought, to a sphere of cultural hegemony & consensus building of cultural hegemony & consensus building (Gramsci), to a public sphere of representation (Gramsci), to a public sphere of representation and promotion of social rights and cultural and promotion of social rights and cultural pluralism (‘responsible freedom’ by pluralism (‘responsible freedom’ by homo homo civicuscivicus) )
2.2. Public spherePublic sphere: a non-state space of active : a non-state space of active citizenship and democratic life based on citizenship and democratic life based on recognition, tolerance and participation by recognition, tolerance and participation by voluntary associations, the space of the voluntary associations, the space of the ‘commons’ and of ‘communicative action’ ‘commons’ and of ‘communicative action’ (Habermas)(Habermas)

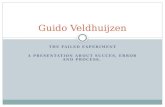
A CONCEPTUAL MAP OF THE SOCIETAL A CONCEPTUAL MAP OF THE SOCIETAL SPACESPACE
cultural Public Sphere medicalization assimilation of life
CIVIL SOCIETY (secondary groups & networks, associations, organizations, social movements)
LIFE WORLDS (person, family, primary social networks)
Private Sphere
POLITICAL-ADMINISTRATIVE
SYSTEM (State)
ECONOMIC SYSTEM (Market)
SOCIAL-CULTURAL SYSTEM
(Mass media technostructure)
mediatica)
SOCIAL-HEALTH SYSTEM
(Human services technostructure)

3. Third sector, citizenship 3. Third sector, citizenship associations and self-help mutual associations and self-help mutual
aidaid ‘‘Third sector’ as part of civil society, but Third sector’ as part of civil society, but
it does not include all of it in itself it does not include all of it in itself (Donati)(Donati)
the place of production & consumption of the place of production & consumption of ‘relational goods’ (Donati): the ‘relational goods’ (Donati): the manifestation of solidarity in social manifestation of solidarity in social relations, the good is relational since it is relations, the good is relational since it is (‘lies in’) the relationship (‘lies in’) the relationship
what is the place of citizenship what is the place of citizenship associations in the Third sector? associations in the Third sector?

A CLASSIFICATION OF THIRD SECTOR A CLASSIFICATION OF THIRD SECTOR COMPONENTS IN SOCIAL & HEALTH COMPONENTS IN SOCIAL & HEALTH
CARECARE
THIRD SECTOR COMPONENT
NON PROFIT
ORGANIZATIONS (FOUNDATIONS)
SOCIAL
ENTERPRISES (COOPERATIVES)
CITIZENSHIP
ASSOCIATIONS
Type of relational goods produced
solidarity aims or social
utility
comprehensive mutual
support
enactment of social rights
of citizernship

DIFFERENT TYPES OF DIFFERENT TYPES OF CITIZENSHIP ASSOCIATIONSCITIZENSHIP ASSOCIATIONS
1.1. ADVOCACY ORGANIZATIONSADVOCACY ORGANIZATIONS2.2. VOLUNTARY ASSOCIATIONSVOLUNTARY ASSOCIATIONS3.3. SELF-HELP GROUPS SELF-HELP GROUPS
((citizens-users/patients/carers citizens-users/patients/carers organizations) organizations)
inner vs outer focusedinner vs outer focused(Katz & Bender, 1976)(Katz & Bender, 1976)

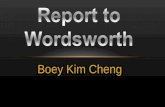
A typology of citizenship A typology of citizenship associationsassociations
TYPES OF CITIZENSHIP ASSOCIATIONS
VOLUNTARY ASSOCIATIONS
SELF-HELP ORGANIZATIONS/
GROUPS
ADVOCACY ORGANIZATIONS
sharing of a common personal/family problem
no
yes
no
main aim
delivery of free-of-charge, relational, solidaristic services to other people
promotion, prevention, rehabilitation of the health/ wellness of their members
information and enforcement of the weakest citizens’ rights
foundation principle
gift
helper
empowerment

THE DIFFERENT AREAS OF THE DIFFERENT AREAS OF INTERVENTIONINTERVENTION
OF SELF-HELP ORGANIZATIONSOF SELF-HELP ORGANIZATIONS
DRUG ADDICTION
PHYSICAL AND PSYCHIC
DISABILITIES
MENTAL HEALTH PSICO-SOCIAL DISCOMFORTS
CHRONIC AND RARE DISEAES

4. 4. A RESEARCH PROJECT ON THE ROLE OF A RESEARCH PROJECT ON THE ROLE OF
SELF-HELP MUTUAL AID IN THE GOVERNANCE SELF-HELP MUTUAL AID IN THE GOVERNANCE
OF HEALTH AND SOCIAL CARE OF HEALTH AND SOCIAL CARE FOR CHRONICALLY ILL IN ITALYFOR CHRONICALLY ILL IN ITALY
An inter-university project (Catanzaro, An inter-university project (Catanzaro, Padova and Ancona Universities) Padova and Ancona Universities)
funded by Italian Ministry of Health funded by Italian Ministry of Health aimed to aimed to analyse the role that self-help analyse the role that self-help
mutual aid associations play in promoting mutual aid associations play in promoting and/or representing the interests of and/or representing the interests of chronically ill within the local and regional chronically ill within the local and regional health services and to evaluate the actual health services and to evaluate the actual impact they have on the decision-making impact they have on the decision-making processes in all their phases (agenda processes in all their phases (agenda setting, policy development, planning, setting, policy development, planning, implementation and evaluation of services)implementation and evaluation of services)

PROJECT PHASESPROJECT PHASES Phases 1-2: Mapping of the self-help mutual aid Phases 1-2: Mapping of the self-help mutual aid
associations in the social-health care policy associations in the social-health care policy context at the national level by context at the national level by documentary documentary analysisanalysis and a and a surveysurvey with with 200 questionnaires200 questionnaires
Phases 3-4: An Phases 3-4: An in-depth studyin-depth study of of the origins, development, aims, activities, internal social structure and dynamics, culture of the different types of self-help mutual aid organizations of chronically ill and of their relationships with the other stakeholders (health professions, managers, politicians, scientific researchers, etc.) in the context of 3 regional health care systems (90 interviews90 interviews inin Calabria, Veneto and Marche Regions)
Phase 5: An international comparison at the European level (ENCUPO/ESHMS 4 meetings)

DISEASE
n.
%
Breast tumour 62 31,0 Alzheimer 36 18,0 Diabetes 22 11,0 Multiple sclerosis 19 9,5 Amyotrophic lateral sclerosis 13 6,5 Anticoagulation 12 6,0 HIV-AIDS Muscolar Dystrophy Epilepsy Crohn’s disease Rare metabolic diseases Nephropaties/dyalisis Others
12 10 5 5 2 1 1
6,0 5,0 2,5 2,5 1,0 0,5 0,5
Total 200 100,0
TYPES OF ORGANIZATIONTYPES OF ORGANIZATION14 chronic and rare diseases14 chronic and rare diseases

DISTRIBUTION OF THE DISTRIBUTION OF THE ORGANIZATIONS ACCORDING TO ORGANIZATIONS ACCORDING TO
TERRITORIAL AREA TERRITORIAL AREA OF ACTIVITIESOF ACTIVITIES
AREA OF ACITIVTIES
n. %
national 13 6.5 regional 36 18 provincial 109 54.5 municipal 24 12 other 18 9 TOTAL
200
100

GEOGRAPHICAL DISTRIBUTION GEOGRAPHICAL DISTRIBUTION OF THE ORGANIZATIONSOF THE ORGANIZATIONS
GEOGRAPHICAL AREA
%
North-West 32,5 North-East 39,0 Centre 15,5 South 9,0 Islands 4,0 Total
100,0

N. OF MEMBERS OF THE N. OF MEMBERS OF THE ORGANIZZATIONSORGANIZZATIONS
N. of members
N. %
cumulative %
Up to 50 47 24.5 24.5 From 51 to 100 39 20.3 44.8 From 101 to 200 46 24.0 68.8 From 201 to 300 19 9.9 78.6 From 301 to 500 18 9.4 88.0 More than 500 23 12.0 100.0 Total
192
100
100.0
Missing cases: 8

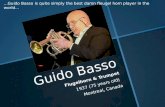
The self-help organizations according to the year of foundation (n.)
11 13
50
62 61
0
10
20
30
40
50
60
70
Prima del 1970 1970-1979 1980-1989 1990-1999 2000-2009

AVERAGE DIMENSIONS OF THE AVERAGE DIMENSIONS OF THE SELF-HELP GROUPSSELF-HELP GROUPS
Type of members of the self-help groups
Number of
groups
Average n. of
members
sick persons only family members/relatives only other caregivers only sick persons + family members/relatives sick persons + caregivers family members/relatives + other care givers sick persons + family members/relatives + other caregivers
104 50
3 60 12 14
43
10 11
7 16 12 11
14

WHICH SPECIFICITY ABOUT SELF-HELP WHICH SPECIFICITY ABOUT SELF-HELP FOR CHRONIC AND RARE DISEASES?FOR CHRONIC AND RARE DISEASES?
Expected duration of participation
Expected scope of change
short
long
small
short-term coping
long-term coping
extensive
short-term transformative
long-term transformative
A Self-help-mutual aid typology (Borkman, 1999:9)

5. External relationships with other 5. External relationships with other stakeholdersstakeholders
a.a. Other civil society organizations Other civil society organizations
b.b. health and social care services health and social care services managers and professionals managers and professionals
c.c. public institutions at local public institutions at local (municipalities), provincial (municipalities), provincial (provincial administration and (provincial administration and health authorities) and regional health authorities) and regional levelslevels

OTHER CIVIL SOCIETY OTHER CIVIL SOCIETY ORGANIZATIONSORGANIZATIONS
Only 20% of the organizations have Only 20% of the organizations have systematic relationships by participating systematic relationships by participating in coordination network in coordination network (vertical/horizontal) (vertical/horizontal)
but 70.4% occasionally collaborate with but 70.4% occasionally collaborate with other organizations other organizations
the nature of the relationship is mainly the nature of the relationship is mainly solidaristic (exchange of logistics, solidaristic (exchange of logistics, technical assistance, information) of for technical assistance, information) of for lobbying togetherlobbying together
some have become godmothers of new some have become godmothers of new associationsassociations
almost all participate in and have good almost all participate in and have good relations with the provincial Centers for relations with the provincial Centers for Voluntary Services (clearing houses)Voluntary Services (clearing houses)

HEALTH AND SOCIAL CARE SERVICES HEALTH AND SOCIAL CARE SERVICES
MANAGERS AND PROFESSIONALSMANAGERS AND PROFESSIONALS Over time, a significant change of attitude Over time, a significant change of attitude
by professionals and managers from by professionals and managers from distrust and skepticism to concern and distrust and skepticism to concern and collaboration collaboration
more problematic relationships with GPs more problematic relationships with GPs than with hospital doctorsthan with hospital doctors
good relationship with social workers, good relationship with social workers, psychologists and health educatorspsychologists and health educators
when a network is established, an when a network is established, an interchange between experiential versus interchange between experiential versus professional cultures is produced with a professional cultures is produced with a significant impact on the therapeutic significant impact on the therapeutic relationship (empowerment)relationship (empowerment)

Scale of professionals’ attitudes Scale of professionals’ attitudes towards self-help/mutual aidtowards self-help/mutual aid
hostile indifferent collaborative participant

PUBLIC INSTITUTIONSPUBLIC INSTITUTIONS Since there is no specific political Since there is no specific political
affiliation, the relationship depends from affiliation, the relationship depends from personal connections and friendshipspersonal connections and friendships
the level of the relationship is mostly the level of the relationship is mostly local/provincial (Municipality, Provincial local/provincial (Municipality, Provincial Administration, Local Health Authority)Administration, Local Health Authority)
a significant difference between the a significant difference between the North - where the relationship is more North - where the relationship is more formalized by protocols, agreements, formalized by protocols, agreements, etc. – and the South, where it is less etc. – and the South, where it is less formalized and more occasionalformalized and more occasional

PUBLIC INSTITUTIONS (2)PUBLIC INSTITUTIONS (2) Some of the associations formally and Some of the associations formally and
steadily participate in the local planning steadily participate in the local planning activities of social and health care activities of social and health care servicesservices
very few participate also in the very few participate also in the management and evaluation activitiesmanagement and evaluation activities
in spite of a certain lip service, the in spite of a certain lip service, the associations are generally fostered and associations are generally fostered and their action positively considered as their action positively considered as complementary to the institutionscomplementary to the institutions
problem of lack of funding by public problem of lack of funding by public administrations, expecially in the last administrations, expecially in the last years years

The participatory scale in The participatory scale in social-health governance social-health governance
lack of manipulative informational advisory structured participation participation participation participation participation

4 types of partnership4 types of partnershipFragmented PartnershipFragmented Partnership: : - limited relationships with the other Third Sector organizations- limited relationships with the other Third Sector organizations- occasional or no relationships with social and health care professionals - occasional or no relationships with social and health care professionals - occasional or no relationships with public institutions (supplementary role)- occasional or no relationships with public institutions (supplementary role)
Technocratic Partnership:Technocratic Partnership: - limited/structured relationships with the other Third Sector organizations- limited/structured relationships with the other Third Sector organizations- steady and structured relationships with social and health care professionals - steady and structured relationships with social and health care professionals - occasional or no relationships with public institutions (supplementary role)- occasional or no relationships with public institutions (supplementary role)
Co-opted PartnershipCo-opted Partnership:: - limited/structured relationships with the other Third Sector organizations- limited/structured relationships with the other Third Sector organizations- occasional or no relationships with social and health care professionals - occasional or no relationships with social and health care professionals - steady and structured relationships with public institutions (by cooptation)- steady and structured relationships with public institutions (by cooptation)
Network partnership:Network partnership: - Steady and structured relationships with the other Third Sector organizations- Steady and structured relationships with the other Third Sector organizations- steady and structured relationships with social and health care professionals - steady and structured relationships with social and health care professionals - steady and structured relationships with public institutions- steady and structured relationships with public institutions

4 types of partnerships within 4 types of partnerships within socio-health governancesocio-health governance
COLLABORATION WITH PUBLIC INSTITUTIONS
weak
fragmented technocratic partnership partnership COLLABORATION 4 17 WITH PROFESSIONALS weak strong
co-opted network partnership partnership 0 6
strong

FROM PARTNERSHIP TO FROM PARTNERSHIP TO HEALTH GOVERNANCEHEALTH GOVERNANCE
Fragmented partnership: Fragmented partnership: institutional institutional governancegovernance
Technocratic partnership: Technocratic partnership: corporate corporate governancegovernance
Co-opted partnership: Co-opted partnership: regulative regulative governancegovernance
Network partnership:Network partnership: community community governance governance

CONCLUSIONSCONCLUSIONS
Self-help/mutual aid organizationsSelf-help/mutual aid organizations have have the potential to play a significant role within the potential to play a significant role within the governance of the social and health care the governance of the social and health care system, particularly by steady and structured system, particularly by steady and structured forms of forms of ‘‘partnershippartnership’ ’ yielding forms ofyielding forms of ‘‘community healthcommunity health governancegovernance’, ’, which canwhich can help to overcome the traditionalhelp to overcome the traditional ‘deficit of ‘deficit of democracydemocracy’ of the social-health systems ’ of the social-health systems
However, this is still very embryonic, since the However, this is still very embryonic, since the actual situation found is mostly actual situation found is mostly technocratically orientedtechnocratically oriented, with a , with a dominant roledominant role still played by still played by managersmanagers and and professionalsprofessionals

THANK YOU FOR YOUR THANK YOU FOR YOUR ATTENTION!ATTENTION!