The challenge of the changing health labor market G ILLES D USSAULT EUREGIO III 3 RD M ASTER C LASS...
19
The challenge of the changing health labor market GILLES DUSSAULT EUREGIO III 3RD MASTER CLASS PROGRAMME 23 MARCH, 2011
-
Upload
daniella-jennings -
Category
Documents
-
view
213 -
download
0
Transcript of The challenge of the changing health labor market G ILLES D USSAULT EUREGIO III 3 RD M ASTER C LASS...
The challenge of the changing health labor market
GILLES DUSSAULTEUREGIO III
3RD MASTER CLASS PROGRAMME23 MARCH, 2011

Overview
• Why discuss health workforce issues (HW) now?
• What needs to be done to find the right balance?

Why discuss HW issues now?
• Needs change • Demand changes• Supply changes• Many alerts: WHO reports, EU Green
paper/Conclusions• Time lag

Education pipeline
Nationals trained abroad
Immigration
Contracting
Stock/ supply of health workers
CompositionDistribution
Statutory retirement
Attrition
Emigration
Returners
A simple model of health labour market dynamics (stock and flows)
Socio-demographic, economic,organizational, legal determinants

Needs change
• Aging population• Epidemiological profile (chronic diseases, mental health, re/emerging diseases)• Values (religious requests, palliative care, euthanasia)• New diagnosis/treatment tools and strategies

Aging in the WHO-EUROPE Region, EU and CIS

Demand changes
• EU Health Policy, Cross-border directive• WHO renewed primary care policy• New organizational strategies: team work, integration of services, ambulatory/home care. Telemedicine • Medicalization of healthy life• Better informed, more demanding users (average time of consultations)

Supply changes
• Aging: Average/nurses = 41-45 in Den., Isl., Nor., Swe., Fra.
• Scaling-up of general practice, of nursing (expanded functions)
• Values and expectations (work-life balance, non-financial incentives)
• Mobility: within countries, between countries, im/emigration (freedom of movement, Bologna process, Blue EU Labour Card)

16%
4% 4% 5%
34%
19%11% 12%
19%
28%
17% 14%
11%
29%
25%20%
9% 12%
26%
24%
7%6%
14%20%
4% 2% 2% 4%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1987 1996 2004 2007
70+
65-69
60-64
55-59
50-54
45-49
40-44
35-39
30-34
GPs, Denmark

• England 2010: 14,000 nurses (Mooney H, 2007)• Netherlands: 7,000 nurses (Simoens et al 2005)• Norway: 3,300 nurses (Askildsen et al 2003)• Switzerland: 3000 nurses (Irving J 2001)
• USA– 500000 nurses (2025) (Buerhaus et al. in print)
– 44000 (2025) family practitioners (Colwill 2008)
Predicted shortages
12
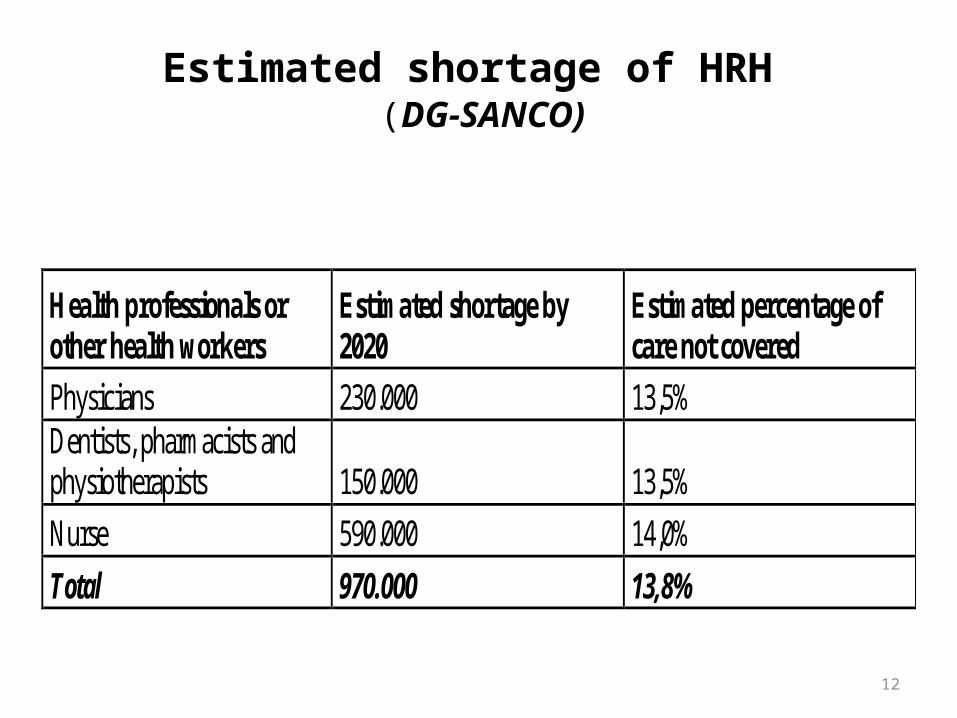
Estimated shortage of HRH (DG-SANCO)
Health professionals or other health workers
Estimated shortage by 2020
Estimated percentage of care not covered
Physicians 230.000 13,5% Dentists, pharmacists and physiotherapists 150.000 13,5%
Nurse 590.000 14,0%
Total 970.000 13,8%

Migratory flows: ‘push’ e ‘pull’
• Compensation• Working conditions• Working environment• Better career opportunities• Access to specialized training• More security and stability
• “Global Code of Practice on the International Recruitment of health personnel”
Source: Buchan J et al 2003
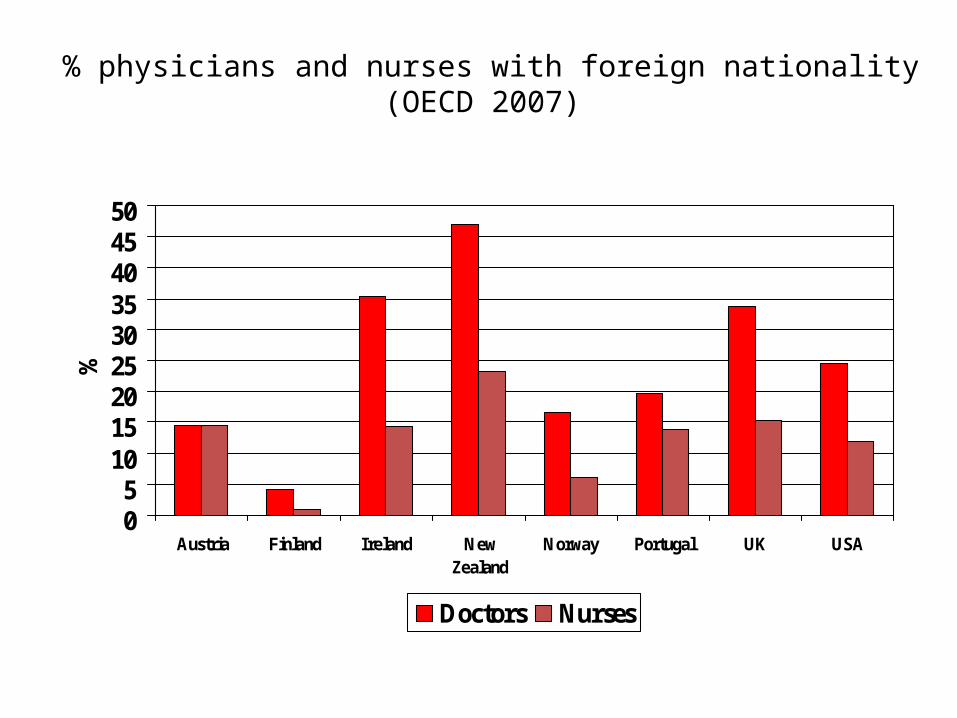
% physicians and nurses with foreign nationality(OECD 2007)
05
101520253035404550
Austria Finland Ireland NewZealand
Norway Portugal UK USA
%
Doctors Nurses
Which workforce?
• First, need to answer a few tricky questions:– Where do we start from?– Future health needs?– Which services? How will they be
organized? – Who will do what?– How will supply and labour market
evolve?– How much are we prepared to spend?
Which workforce?
• What is the capacity of the country, of individual organizations?– To attract/recruit the right type of future health
workers – To educate/train them– To employ them– To retain them

What countries can (should) do?
• HW policy in line with services and health policies
• Build the information base (numbers, availability, productivity, projections, expectations, multiple employment, private sector)
• Mobilize stakeholders in support of change• Mobilize resources and capacity

Conclusions
• The toughest challenge: building the workforce of tomorrow
• A global approach is needed• How to move from awareness to
effective action ?