The Center for Palliative Care Education Palliative Management of Dyspnea in HIV/AIDS.
30
The Center for Palliative Care Education Palliative Management of Dyspnea in HIV/AIDS
-
date post
22-Dec-2015 -
Category
Documents
-
view
227 -
download
1
Transcript of The Center for Palliative Care Education Palliative Management of Dyspnea in HIV/AIDS.
The Center for Palliative Care Education
Palliative Management of Dyspnea in HIV/AIDS
Learning objectives
Describe the primary causes of dyspnea at the end of life
Explain the process of evaluating a patient’s dyspnea
Give examples of treatments for dyspnea and their risks and benefits
Consider the causes, evaluation and treatment of dyspnea in patients with HIV/AIDS
Understand management of dyspnea during the last hours of life
Consider a case
42-year-old HIV positive man
Presents with progressive dypnea over 6 months
PMH otherwise unremarkable
–Physical exam normal
–Cutaneous Kaposi’s Sarcoma
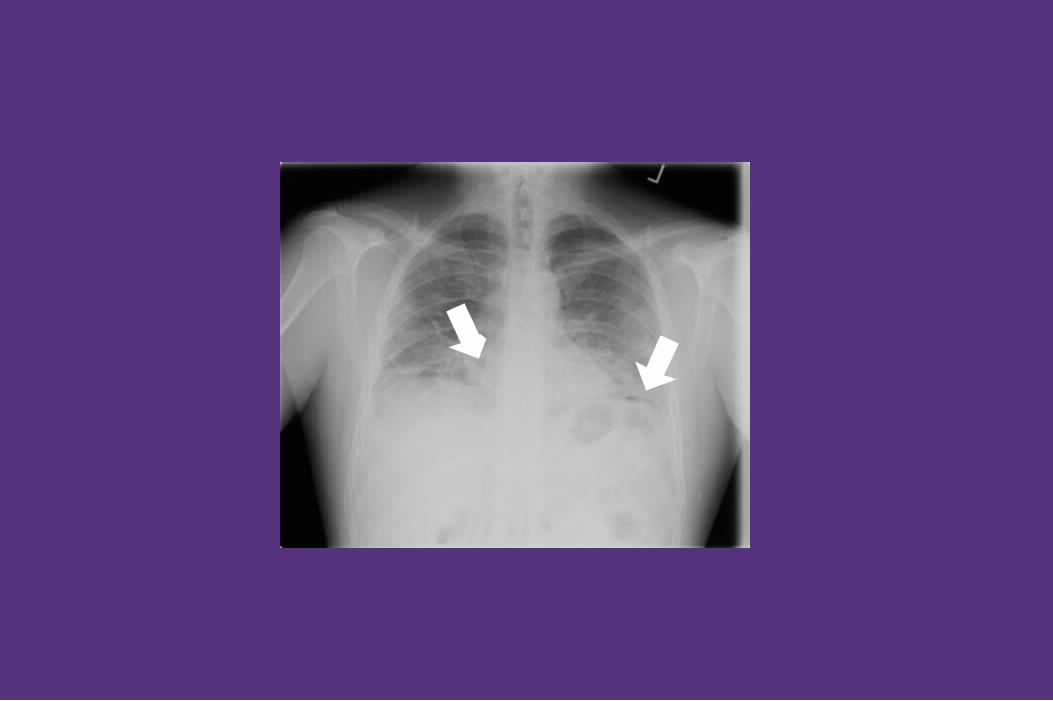
–CXR shows…


Outline
Causes of severe dyspnea in palliative care
Causes of dyspnea in HIV/AIDS patients
Treatment options for dyspnea
Dyspnea in the last hours of life

Causes of dyspnea
Many pulmonary and non-pulmonary diseases can cause dyspnea:–Pulmonary: COPD, asthma, pneumonia, PE, lung cancer, lymphoma, pneumothorax, pleural effusion
–Non-Pulmonary: Heart failure, anemia, acidosis
First step to managing dyspnea is to diagnose and treat underlying cause

Some causes of dyspnea in HIV/AIDS
Opportunistic Infections: PCP, Fungal, TB, Viral
Pulmonary Kaposi’s Sarcoma
Lymphoma
HIV-Related Myopathy



Initial evaluation for dyspnea
History, physical examination
Chest x-ray
Laboratory tests: CBC, chemistries, arterial blood gas
Spirometry
Approach to managing dyspnea
Identify the cause
Treat what is treatable
Manage with supportive measures
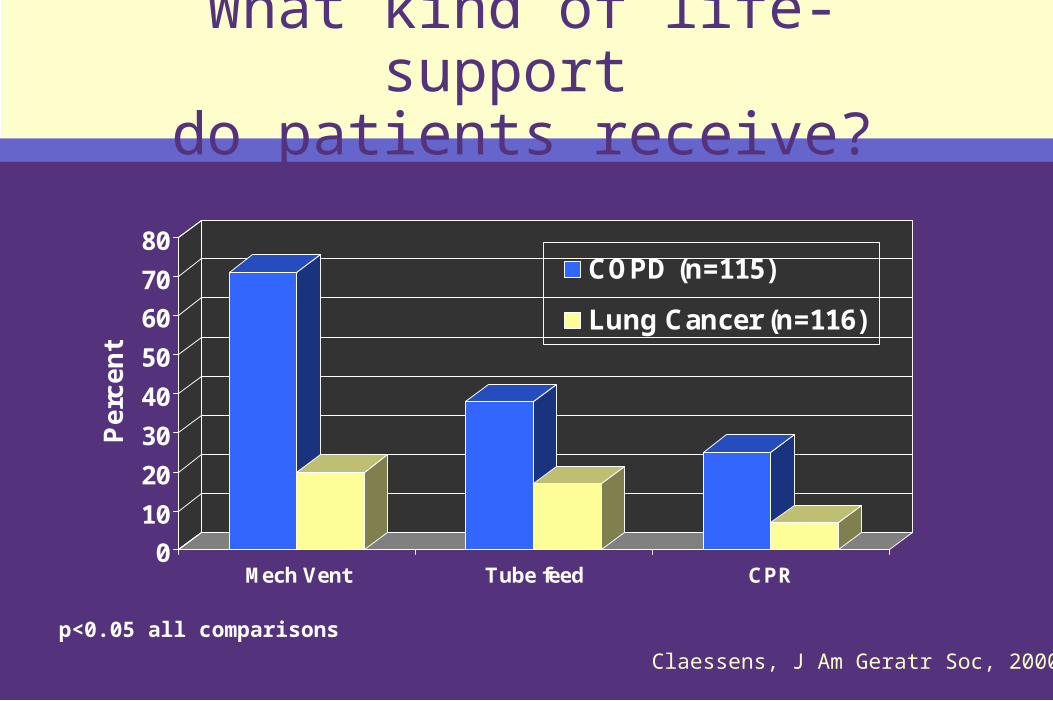
What kind of life-support do patients receive?
0
10
20
30
40
50
60
70
80
Pe
rce
nt
Mech Vent Tube feed CPR
COPD (n=115)
Lung Cancer (n=116)
Claessens, J Am Geratr Soc, 2000
p<0.05 all comparisons

What kind of life-support do patients want?
0
20
40
60
80
100
Pe
rce
nt
Prefer Comfort Prefer DNR No Mech Vent
COPDLung Cancer
Claessens, J Am Geratr Soc, 2000
p>0.05 all comparisons

Treatment of dyspnea
Oxygen
Opioids
Benxodiazepines
Anti-depressants
Non-pharmacologic measures

Oxygen
Many HIV+ patients with dyspnea do not have low O2 saturations
However, O2 therapy may relieve symptoms of dyspnea
Pro: Symptom relief, ease of use
Con: Uncomfortable, burdensome, expensive
Oxygen
Indication for oxygen therapy:
–PaO2 < 55 mmHgPaO2 55-59 + a) p pulmonale,
–b) clinical right heart failure, OR c) hct > 55%
–SaO2 < 89%
–SaO2 89% plus a, b, or c above
–Treatment of dyspnea in hospice care
Opioids
Primary pharmacologic therapy for dyspnea
Important central effects of analgesia and euphoria that palliate dyspnea
Choice of administration route (Patch, PO, parenteral)
Intermittent vs. continuous dosing
Pro: May be efficacious in improving breathlessness
Con: Sedating, may cause respiratory depression, constipation

Trials of oral opiates for dyspnea in severe COPD
Author- Year Drug Duration Dyspnea
Woodcock ’81 dh-codeine 1 dose improved
Johnson ’83 dh-codeine 1 wk improved
Light ’89 morphine 1 dose improved
Rice ’87 codeine 1 mo no change
Eiser ’91 diamorph. 2 wk no change
Poole ’98 MS-SR 6 wk no change
Manning, Resp Care, 2000; 45:1342

Other agents with little or no effect on dyspnea
Nebulized opiates:–1 positive, 4 negative controlled trials
Benzodiazepines:–1 positive, 3 negative controlled trials
Buspirone:–1 positive trial, very small effect
Phenothiazines:–1 positive, small effect; 1 negative trial

Depression and anxiety in severe COPD and stage III/IV lung cancer
0
2
4
6
8
10
12
Ho
spit
al A
nxi
ety
& D
epre
ssio
n
Sca
le
Depression Anxiety
COPD
Lung Cancer
Gore, Thorax, 2000
p<0.01 all comparisons
Benzodiazepines
Use may alleviate associated fear and anxiety
Start at low dose and titrate to dyspnea reduction
Once effective dose determined, schedule administration Q4-6H
Variety of dosing routes available

Treating depression in COPD
12-week randomized controlled trial
Two groups:
–Nortriptyline vs placebo
N=36
–Major depression (n=33)
–Residual depression (n=3)
Mean duration depression 39 months
Borson, Psychosomatics 1992
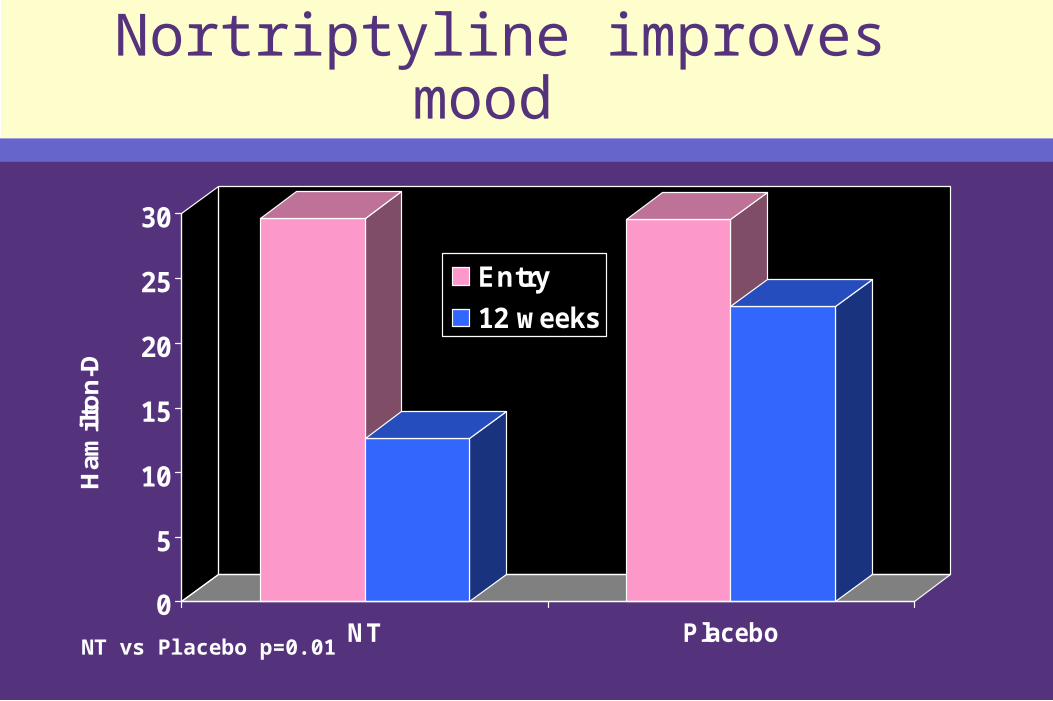
Nortriptyline improves mood
0
5
10
15
20
25
30
Ham
ilto
n-D
NT Placebo
Entry
12 weeks
NT vs Placebo p=0.01

Nortriptyline (NT) improves anxiety and somatic symptoms
0
10
20
30
40
50
60
PR
AS
ANXIETY PHYSICAL SX BREATHING SX
NT Entry
NT 12 Weeks
Placebo Entry
Placebo 12 Weeks
Differential NT treatment effects: All p < 0.05
Nonpharmacologic interventions
Minimize anxiety-producing factors in the environment
Address concerns of family members and caregivers as well as the patient
Relaxation techniques
Fan/cool air
Schwartzstein RM, et al (1987) Am Rev Respir Dis 136:58 -61

Dyspnea in the last hours of life
Same treatment modalites: oxygen, opioids, and benzodiazepines
Titrate opioid dose to patient’s respiratory signs
Consider anticholinergic agent for management of secretions
Re-consider case
42-year-old man with HIV presents with progressive dypnea over 6 months
PMH otherwise unremarkable
–Physical exam normal
–CXR consistent with KS

Summary
Dyspnea is common and disabling
Identify cause of dyspnea and treat underlying cause when possible
Trial of symptomatic treatments
–Oxygen, opiates
Recognize and treat anxiety and depression
Spend time communicating with patients and family

Contributors
The primary author of this module is Elizabeth Knauft, MD, MS, University of Washington Department of Pulmonary and Critical Care Medicine
Anthony Back, MD DirectorJ. Randall Curtis, MD, MPH Co-DirectorFrances Petracca, PhD EvaluatorLiz Stevens, MSW Project Manager
Visit our Website at uwpallcare.org
Copyright 2003, Center for Palliative Care Education, University of Washington
This project is funded by the Health Resources and Services Administration (HRSA) and the Robert Wood Johnson Foundation (RWJF).