The causes and prevention of intestinal adhesions
3
Br. J. Surg. Vol. 69 (1982) 241-243 Printed in Great Britain Proffered review The causes and prevention of intestinal adhesions Although intestinal obstruction from intra-abdominal adhesions is a relatively common surgical emergency, the vast majority of adhesions are harmless and may be protective or even life-saving. The causes of intestinal adhesions are presented, and various methods advocated to prevent adhesions are discussed. The surgeon is advised to reduce unnecessary adhesion formation by meticulous surgical technique, control those adhesions which inevitably form to obtain their beneficial effects, and to avoid the risk of subsequent HAROLD ELLIS Professor of Surgery, Westminster Medical School, London SWI. obstruction. Intra-abdominal adhesions are almost inevitable after major abdominal surgery. Systematic studies at either post-mortem examination or laparotomy are surprisingly few, but these do reveal the high frequency of symptomless postoperative adhesions in the general population. Weibel and Majno (1) reviewed 298 subjects at post-mortem who had had previous laparotomies, and 67 per cent of these showed adhesions; after multiple operations, the incidence rose to 93 per cent. In a recent unpublished personal study of 50 consecutive patients submitted to laparotomy after previous abdominal surgery, no less than 44 had developed adhesions. Most surgeons regard these adhesions as a nuisance. They make reoperation upon the abdomen a tedious dissection, with risk of visceral damage, and they may precipitate intestinal obstruction. Indeed, adhesions now represent the commonest cause of small bowel obstruction in the Western World, replacing strangulated external hernia, which still holds pride of place for this emergency in developing countries where laparotomies are performed far less frequently. Analyses of large series of cases (Table l) demonstrate that approximately one-third of all intestinal obstructions are likely to be due to adhesions, and these are responsible for about 60 per cent of all small bowel obstructions. In a consecutive series of 253 intestinal obstructions in adult patients in my own unit, 26 per cent were due to adhesions and 21 per cent to strangulated hernia (7). In contrast, a recent study from Nigeria, typical of the many reports from emerging communi- ties, showed a 65 per cent incidence of strangulated hernia compared with only 11 per cent due to adhesions (8). Although postoperative adhesions may involve any viscus within the peritoneal cavity, obstruction from this cause nearly always implicates the small intestine, especially the ileum. For example, Miller and Winfield (9) reviewed a series of 43 cases of postoperative obstruction due to adhesions and found that 32 involved the ileum, 6 the ‘small intestine’ not specifically designated, and only 1 affected the large bowel (a patient in whom the sigmoid colon was obstructed by a fibrous band). Aetiology From the earliest days of abdominal surgery, surgeons became familiar with the fibrinous adhesions that develop within a few hours of operational trauma. This fibrin can either re-absorb completely, leaving a clear peritoneal cavity, or become organized by the ingrowth of fibroblasts to form established fibrous adhesions. It was soon apparent that the important thing to determine is the factor that decides whether the adhesions are to absorb completely or become organized into persistent, and potentially dangerous, fibrous strands. As I have pointed out in several essays on this subject (10-12), surgeons and pathologists, by armchair reasoning rather than experimental observations, and basing their analogy on the healing of cutaneous wounds, assumed that this factor was whether or not the peritoneal endothelium was intact. Text- book copied from textbook that anything which damages the endothelium-rough handling, retraction, surgical denudation and so on-will necessarily be followed by fibrous adhesions. This led to the surgical principle that peritoneal injury must be avoided at all costs, that raw damaged serosal surfaces must be eliminated within the peritoneal cavity and that peritoneal defects must be oversewn or patched wherever possible. However, when the armchair theory was put to the test, both by experiment and by careful clinical observation (lo), the results were very different. It is now well established that large peritoneal defects, left open and bleeding, heal within a few days into a smooth glistening new serosa. However, if the injury is accompanied by vascular damage, for example, if the tissues are crushed, sutured or ligated, then indeed adhesions develop, and injection studies show that these comprise active Table I: ADHESIONS AND BANDS AS CAUSES OF OBSTRUCTION ~~~ Total Author Year Place no. Nemir (2) 1952 Philadelphia 430 Perry et al. (3) 1955 Minneapolis 1252 Raf (4) 1969 Stockholm 2295 Playforth 1970 Lexington 111 Stewardson 1978 Chicago 238 Ellis (7) 1982 London 253 et al. (5) et al. (6) Adhesions (%I Notes 33 31 64 Small intestine only and excludes hernias, neoplasms and Crohn’s disease 54 Small intestine only 64 Small intestine only 26 Adults only
-
Upload
harold-ellis -
Category
Documents
-
view
214 -
download
1
Transcript of The causes and prevention of intestinal adhesions

Br. J . Surg. Vol. 69 (1982) 241-243 Printed in Great Britain
Proffered review
The causes and prevention of intestinal adhesions
Although intestinal obstruction from intra-abdominal adhesions is a relatively common surgical emergency, the vast majority of adhesions are harmless and may be protective or even life-saving. The causes of intestinal adhesions are presented, and various methods advocated to prevent adhesions are discussed. The surgeon is advised to reduce unnecessary adhesion formation by meticulous surgical technique, control those adhesions which inevitably form to obtain their beneficial effects, and to avoid the risk of subsequent
HAROLD ELLIS Professor of Surgery, Westminster Medical School, London SWI. obstruction.
Intra-abdominal adhesions are almost inevitable after major abdominal surgery. Systematic studies at either post-mortem examination or laparotomy are surprisingly few, but these do reveal the high frequency of symptomless postoperative adhesions in the general population. Weibel and Majno (1) reviewed 298 subjects at post-mortem who had had previous laparotomies, and 67 per cent of these showed adhesions; after multiple operations, the incidence rose to 93 per cent. In a recent unpublished personal study of 50 consecutive patients submitted to laparotomy after previous abdominal surgery, no less than 44 had developed adhesions.
Most surgeons regard these adhesions as a nuisance. They make reoperation upon the abdomen a tedious dissection, with risk of visceral damage, and they may precipitate intestinal obstruction. Indeed, adhesions now represent the commonest cause of small bowel obstruction in the Western World, replacing strangulated external hernia, which still holds pride of place for this emergency in developing countries where laparotomies are performed far less frequently.
Analyses of large series of cases (Table l) demonstrate that approximately one-third of all intestinal obstructions are likely to be due to adhesions, and these are responsible for about 60 per cent of all small bowel obstructions. In a consecutive series of 253 intestinal obstructions in adult patients in my own unit, 26 per cent were due to adhesions and 21 per cent to strangulated hernia (7). In contrast, a recent study from Nigeria, typical of the many reports from emerging communi- ties, showed a 65 per cent incidence of strangulated hernia compared with only 1 1 per cent due to adhesions (8).
Although postoperative adhesions may involve any viscus within the peritoneal cavity, obstruction from this cause nearly always implicates the small intestine, especially the ileum. For example, Miller and Winfield (9) reviewed a series of 43 cases of postoperative obstruction due to adhesions and found that 32
involved the ileum, 6 the ‘small intestine’ not specifically designated, and only 1 affected the large bowel (a patient in whom the sigmoid colon was obstructed by a fibrous band).
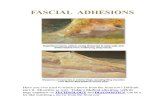
Aetiology From the earliest days of abdominal surgery, surgeons became familiar with the fibrinous adhesions that develop within a few hours of operational trauma. This fibrin can either re-absorb completely, leaving a clear peritoneal cavity, or become organized by the ingrowth of fibroblasts to form established fibrous adhesions. It was soon apparent that the important thing to determine is the factor that decides whether the adhesions are to absorb completely or become organized into persistent, and potentially dangerous, fibrous strands. As I have pointed out in several essays on this subject (10-12), surgeons and pathologists, by armchair reasoning rather than experimental observations, and basing their analogy on the healing of cutaneous wounds, assumed that this factor was whether or not the peritoneal endothelium was intact. Text- book copied from textbook that anything which damages the endothelium-rough handling, retraction, surgical denudation and so on-will necessarily be followed by fibrous adhesions. This led to the surgical principle that peritoneal injury must be avoided at all costs, that raw damaged serosal surfaces must be eliminated within the peritoneal cavity and that peritoneal defects must be oversewn or patched wherever possible.
However, when the armchair theory was put to the test, both by experiment and by careful clinical observation (lo), the results were very different. It is now well established that large peritoneal defects, left open and bleeding, heal within a few days into a smooth glistening new serosa. However, if the injury is accompanied by vascular damage, for example, if the tissues are crushed, sutured or ligated, then indeed adhesions develop, and injection studies show that these comprise active
Table I: ADHESIONS AND BANDS A S CAUSES OF OBSTRUCTION ~~~
Total Author Year Place no.
Nemir (2) 1952 Philadelphia 430 Perry et al. (3) 1955 Minneapolis 1252 Raf (4) 1969 Stockholm 2295
Play forth 1970 Lexington 1 1 1
Stewardson 1978 Chicago 238
Ellis (7) 1982 London 253
et al. (5)
et al. (6)
Adhesions (%I Notes
33 31 64 Small intestine only and excludes
hernias, neoplasms and Crohn’s disease
54 Small intestine only
64 Small intestine only
26 Adults only

242
vascular ingrowths of newly formed vessels into ischaemic tissue.
In many instances, these vascular grafts are undoubtedly life- saving, preserving the viability of an anastomosis, reinforcing the integrity of a traumatized segment of intestine or preventing an ischaemic appendix or gallbladder from perforating into the general peritoneal cavity. Experimentally, if we prevent adhesions from developing to a segment of intestine deprived of its blood supply by means of wrapping the segment in a sheet of polythene film, then gangrene of the segment will invariably take place. If, however, adhesions are allowed to develop, the bowel segment, up to a certain critical level, remains viable (10).
Buckman et al. (13, 14) have shown that peritoneal defects have a high plasminogen activity measured by the area of lysis produced on fibrin plates. This activity is lost in peritoneum which has been rendered ischaemic by grafting or by tight suturing and, moreover, such ischaemic tissue may actively inhibit fibrinolysis by normal tissues. This phenomenon also explains the failure of intact peritoneum to lyse fibrinous adhesions to adjacent ischaemic tissue.
Ischaemic tissues are not unique in stimulating an inflam- matory vascular response in neighbouring structures. Many of the substances which may contaminate the peritoneal cavity at the time of laparotomy may be responsible for the formation of granulomas and for the development of fibrous intra-abdomi- nal adhesions. The most detailed account of this is the study by Myllarniemi (1 5) of 309 cases of postoperative adhesions. Sixty-one per cent of these showed foreign body reactions, and this was particularly likely to occur after major surgery or repeated laparotomies. In half the cases, the foreign material was talc, in a quarter it was lint or thread and the remaining cases showed starch, extruded gut contents, sutures or a mixture of materials, usually talc associated with thread.
It is probable that the minor epidemic that we saw during the 1970s of starch reactions within the peritoneal cavity (16) was attributable to a change in the sterilization technique of the glove starch dusting powder. Capperauld (17) has shown that autoclaved starch is absorbed from the peritoneal cavity in about 48 hours, whereas irradiated starch persists for 70 days or more and produces a much greater incidence of adhesion formation in the experimental animal. Moreover, electron- microscopic studies showed that cracks may be seen on the surface of starch which has been autoclaved in contrast to the smooth surface of the irradiated material. Steroids have been advocated to speed the process of starch absorption, but we have been unable to show, in the experimental animal (18), that prednisone commenced at the time of the peritoneal con- tamination or after inoculation reduces the histological reaction to the starch.
Attempts to prevent adhesions This century has witnessed an enormous body of work on attempts to prevent adhesions, and hundreds of papers have been written on both the clinical and laboratory aspects of this subject. Extensive reviews have been published in the past by Boys in 1942 (19), Connolly and Smith in 1960 (20) and by myself in 1971 (21). These reviews include extensive biblio- graphies.
These attempts to prevent adhesions have been approached from a number of different aspects, which can be classified as follows: Prevention of jibrin deposition in the postoperative peritoneal exudate. This has involved the use of anticoagulants such as sodium citrate, heparin, dicoumarol and Dextran, and apro- tinin (Trasylol) as a possible antiplasmin agent. Removal ofjibrin exudate by means of intraperitoneal lavage, enzymes such as pepsin, trypsin and papain, and fibrinolytic agents such as streptokinase, actase and urokinase. Separation of surfaces has been advised by such methods as distension of the abdominal cavity with oxygen, stimulation of peristalsis with prostigmine to prevent prolonged contact between adjacent loops of intestine, and the use of such substances as olive oil, liquid paraffin, amniotic fluid, mem- branes of fish bladder, ox peritoneum, amniotic membrane, oiled silk, silver or gold foil, free grafts of omentum and silicones to separate damaged loops of bowel.
H. Ellis
Inhibition qf jibroblastic proliferafion has included the use of antihistamines, steroids and cytotoxic drugs.
The story for all these substances has been very much the same: initial enthusiasm, often actual use in clinical cases, then further investigations which showed either no effect at all or an actual increase in adhesion formation compared with controls, then finally the abandonment of that particular material.
Prophylaxis and treatment Armed with the knowledge of how adhesions develop, the surgeon needs to prevent unnecessary adhesions from develop- ing, control those adhesions which must inevitably form in order to obtain their beneficial effects but to avoid, wherever possible, the risk of subsequent obstruction; finally, in those patients who suffer from repeated episodes of obstruction, he must try to devise the best possible management following adhesion lysis.
Unnecessary adhesion formation can be reduced by meti- culous surgical technique, and this must include the prevention of granuloma formation from foreign materials such as gauze, glove powder or long and redundant ends of non-absorbable sutures. Wherever possible, peritoneal defects (such as the gallbladder bed or the pelvic floor) should be left open rather than pulled together under tension.
When adhesion formation is inevitable due to local tissue ischaemia (for example, to the peritoneal surface of the laparo- tomy incision or to an anastomotic line), the surgeon should try to ensure that such adhesions develop to structures other than the small intestine. Thus, the omentum should be drawn over the other abdominal organs before closing the laparotomy incision and it should be wrapped over any anastomotic line. For this reason, the omentum should be preserved, if at all possible, in carrying out a total colectomy. The reported high incidence of intestinal obstruction due to adhesions following this particular operation is almost certainly due to the fact that so many surgeons remove the omentum together with the colon, thus leaving only small bowel to adhere to the anterior abdominal wall along the line of closure. If adhesions have to form, let these be planned to safe vascular peritoneal grafts of omentum, falciform ligament or broad ligament without the risk of kinks and bands which such adhesions might produce if they involve coils of small intestine.
Fortunately, recurrent widespread adhesions causing re- peated episodes of intestinal obstruction are becoming less common. This is probably because of the greater care which is being taken in intra-abdominal surgery, and it is possible that in previous times many of these were due to extensive spillage of material such as talc into the peritoneal cavity. However, these dangerous and worrying problems are still seen from time to time. It may be possible to resect or short-circuit a localized coil of matted intestine. Personally, I do not believe that there is firm evidence that any substance instilled into the peritoneal cavity is of genuine clinical value.
A number of plication procedures have been advocated which are designed to avoid acute kinks of the matted bowel. The operation was first reported by the Finnish surgeon, Wichmann in 1934, but was popularized by Noble (22), after whom the operation is often, and rather unfairly, named (23). More recently, transmesenteric plication of loops of small intestine in a serpentine pattern has been advocated as a simpler and safer procedure by Childs and others (24,25).
Certainly, the Childs technique appears to be safer than the Noble plication (26), but several reports of series of patients show that there is a significant mortality with the procedure, and follow-up shows that further episodes of obstruction may still, unfortunately, occur (27-29).
I must confess that I have no personal experience whatsoever of these plication procedures, nor am I convinced from my reading of the results of others that the incidence of recurrent intestinal obstruction is any lower in their patients than in those subjected to simple division of the adhesive bands.
In 1959, Baker (30) described an ingenious technique of threading a tube down the whole length of the small intestine via a jejunostomy which, by its intrinsic stiffness, would prevent kinking while adhesions develop. Subsequent reports (31,32) described favourable results following the use of this technique.

Intestinal adhesions 243
Miller E. M. and Winfield J. M.: Acute intestinal obstruction secondary to post-operative adhesions. Arch. Surg. 1959: 78: 952-7. Ellis H.: The aetiology of postoperative abdominal adhesions. Br. J . Surg. 1962; 50: 10-16. Ellis H.: Wound repair-reaction of the peritoneum to injury. Ann. R. Coll. Surg. 1978; 60: 219-21. Ellis H.: Internal overhealing-the problem of intraperitoneal adhesions. World J . Surg. 1980; 4: 303-6. Buckman R. F., Woods M., Sargent L. et al.: A unifying pathogenetic mechanism in the etiology of intraperitoneal ad- hesions. J . Surg. Res. 1976; 2 0 1-5. Buckman R. F., Buckman P. D., Hufnagel H. V. et al.: A physiologic basis for the adhesion-free healing of deperitonealized surfaces. J . Surg. Res. 1976; 21: 67-76. Myllarniemi H.: Foreign material in adhesion formation after abdominal surgery. Acra Chir. Scand. 1967; Suppl. 377. Jagelman D. G. and Ellis H.: Starch and intraperitoneal adhesion formation. Br. J . Surg. 1973; 60: 1 11-14, Capperauld I . : Influence of sterilisation methods on the incidence of glove starch granuloma. Eur. Surg. Res. 1977; 9: Suppl. 1, 70. Cade D. and Ellis H.: The peritoneal reaction to starch and its modification by prednisone. Eur. Surg. Res. 1976; 8: 471479. Boys F.: The prophylaxis of peritoneal adhesions: a review of the literature. Surgery 1942; 11: 118-68. Connolly J. E. and Smith J. W.: The prevention and treatment of intestinal adhesions. Surg. Gynecol. Obstet. 1960; 110: 417-31. Ellis H.: The cause and prevention of post-operative intraperi- toneal adhesions. Surg. Gynecol. Obstet. 1971; 133: 497-51 1. Noble T. B.: Plication of small intestine as prophylaxis against adhesions. Am. J. Surg. 1937; 35: 41-4. Sivula A. and Asp K.: Wichmann's plication in the treatment of recurrent intestinal obstruction due to adhesions. Acra Chir.
Childs W. A. and Phillips R. R.: Experience with intestinal plication and a proposed modification. Ann. Surg. 1960; 152:
Ferguson A. T., Reihmer V. A. and Gaspar M. R. : Trans- mesenteric plication for small intestinal obstruction. Am. J. Surg.
Papadimitriou J., Marselos A., Kyriakou K. et al.: Childs versus Noble plication. Chir. Gastroenterol. 1972; 6: 29-36. Hollender L. F., Otteni F. and Klein A,: La plicature mes- enterique selon Childs et Phillips. Lyon Chir. 1971; 67: 24-9. McCarthy J. D.: Further experience with the Childs-Phillips plication operation. Am. J . Surg. 1975; 130: 15-19. Somell A.: Mesenteric plication in the treatment of adhesive intestinal obstruction. Acta. Chir. Scand. 1978; 144: 255-9. Baker J. W.: A long jejunostomy tube for decompressing in- testinal obstruction. Surg. Gynecol. Obstet. 1959; 109: 5 18-20. Baker J. W. and Ritter K. J.: Complete surgical decompression for late obstruction of the small intestine with reference to a method.,Ann. Surg. 1963; 157 759-69. Galibert C.: Intubation per-op6ratoire du grdle dans le traitement des occlusions intestinales primitives ou rbcidivantes. Ann. Chir.
Munro A. and Jones P. F.: Operative intubation in the treatment of complicated small bowel obstruction. Br. J . Surg. 1978; 65:
Close M. B. and Christensen N. M.: Transmesenteric small bowel plication or intraluminal tube stenting. Am. J. Surg. 1979; 138:
&and. 1966; 131: 99-106.
258-65.
1967; 114: 203-8.
1979; 3 3 26-3 1.
123-7.
89-96.
Munro and Jones (33) give a good technical account of operative intubation in the treatment of complicated small bowel obstruction, The value of intubation in preventing recurrent small bowel obstruction is not easily proved and only a long term follow-up of such patients and a comparison with a control group will give a definitive answer. Although not a controlled trial, the report by Close and Christensen (34) is of interest. They compare 28 plications with 37 patients subjected to tube stenting and 107 who underwent simple adhesion lysis. Of the plications, there were 3 unrelated deaths, 1 small bowel fistula and 3 reoperations for further obstruction. of the 37 Baker tube procedures, there was 1 unrelated death and 1 reoperation for obstruction. Of the 107 patients who had undergone division of adhesions only, there were 4 deaths and 7 late recurrences.
Obviously, where there is a single band or a few adhesions, simple division alone is all that is indicated. However, where multiple severe adhesions are present, we still need more in- formation regarding the wisest procedure to adopt-plication, intubation or simple lysis.
Conciusion It is my belief that the surgeon needs to change his attitude toward intra-abdominal adhesions. It is true that intestinal obstruction from adhesions is a relatively common surgical emergency, but this must be considered against the background of the enormous numbers of abdomens that are opened each year, in most of which it can be assumed that adhesions have developed. We should cease to regard them as evil. The vast majority are harmless and in many instances may well have been protective or even life-saving by the prevention of leakage from suture lines, obviating necrosis of damaged bowel or walling off inflammatory collections. It is time that the surgeon came to regard adhesions as his friends who occasionally misbehave, rather than his enemies!
References I .
2.
3.
4.
5 .
6.
7.
8.
Weibel M. A. and Majno G.: Peritoneal adhesions and their relation to abdominal surgery. Am. J . Surg. 1973; 126 345-53. Nemir P.: Intestinal obstruction: ten-year survey at the Hospital of the University of Pennsylvania. Ann Surg. 1952; 135: 367-71. Perry J. F.. Smith G . A. and Yonchiro E. G.: Intestinal obstruc- tion caused by adhesions; a review of 388 cases. Ann. Surg. 1955;
Raf L. E.: Causes of abdominal adhesions in cases of intestinal obstruction. Aria Chir. Scand. 1969; 135: 73-6. Playforth R. H.. Holloway .I. B. and Griffen W. 0.: Mechanical small bowel obstruction: a plea for earlier surgical intervention. Ann. Surg. 1970; 171: 783-8. Stewardson R. H., Bombeck T. and Nyhus L. M.: Critical operative management of small bowel obstruction. Ann. Surg.
142: 810-16.
1978: 187: 189-93. Ellis 'H.: Intestinal Ohstruction. New York: Appleton-Century- Crofts, 1982. Chiedozi L. C., Aboh 1 . 0 . and Piserchia N. E.: Mechanical bowel obstruction. Review of 3 16 cases in Benin City. Am. J. Surp 1980;
9.
10.
I I .
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
- 139: 389-93. Paper accepted 20 August 198 1