The C.A.R.E. Connection. Patient- and Family-Centered Care: C.A.R.E. Patient- and Family-Centered...
59
The C.A.R.E. Connection
-
Upload
basil-townsend -
Category
Documents
-
view
232 -
download
9
Transcript of The C.A.R.E. Connection. Patient- and Family-Centered Care: C.A.R.E. Patient- and Family-Centered...
The C.A.R.E. Connection
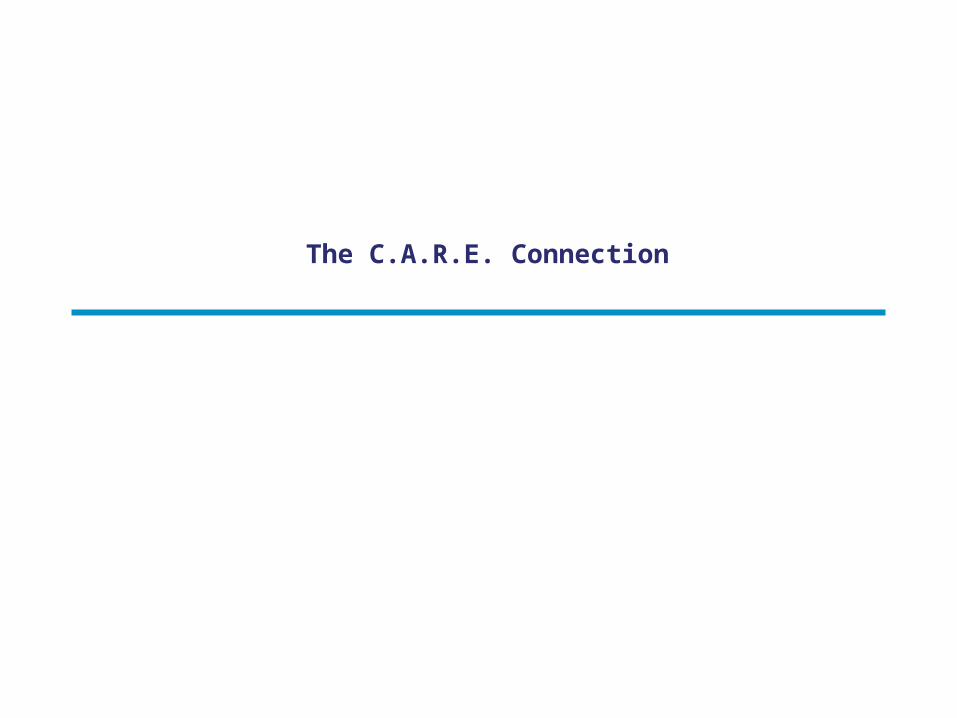
Patient- and Family-Centered Care: C.A.R.E.
Patient- and Family-Centered Care• RESPECT and DIGNITY
• INFORMATION
• PARTICIPATION
• COLLABORATION
C.A.R.E.• CONNECT: Make a personal
connection to the Veteran as a person.
• APPRECIATE: Let the Veteran know that you see their health care situation and how it affects them.
• RESPOND: Listen, clarify, and co-create solutions.
• EMPOWER: Empower the Veteran as a partner in their health and health care.
Exercise 1
1. You are making your initial rounds on a new patient.
2. You enter a room and find a distraught family member.
3. You encounter a Veteran in the hallway who is upset about being late for his clinic appointment because he couldn't find parking.
4. You answer the telephone and a Veteran is asking to re-schedule a clinic appointment at the last minute.
Exercise 2
▼ Jean, age 56, has just had knee surgery and has been brought to her room in the surgery unit. She has been very nervous and waited a long time for this surgery, but happy to finally have the replacement done. She is in pain and uncomfortable, and is anxious to see her husband Shawn.
▼ The first person who comes into her room after her arrival on the unit is her bedside nurse, Mary. Mary comes in to do her initial nursing assessment, but Jean interrupts to ask her when her husband can visit her. She also wants to know what Mary can do about her pain.
As You Play Out the Scene, the Objectives Are to Make Sure that Jean:
• Learns who Mary is and her role in her care.• Learns that Shawn, her husband, is welcome to her
bedside and can visit her any time.• Gets support for relieving her pain and discomfort
(verbal and/or actual physical and medication assistance).
• Feels reassured that Mary is there for her, will answer both her and Shawn’s questions as well as she can, and connect her to anyone else who can help her better than she can.
• Feels as if she and Shawn are welcomed members of her health care team.
Also make sure that: Mary gets her nursing assessment finished.
Debrief
For “Mary” and “Jean”▼ How did you feel during this interaction?▼ What went well?▼ What could have been done differently?▼ Anything else?
BREAK
Patient- and Family-Centered Approaches to Clinical Practice
Promising Nursing Practices
• Nurse Bedside Change of Shift Report and Plan of Care
• Introduction to Patient and Family-Centered Clinical Practices
• Self Management Support
• Team-Based Practices
▼ Pain Management
▼ Medication Reconciliation
▼ Family Presence in Multidisciplinary Rounds
▼ Nurse Bedside Change of Shift Report and Plan of Care
Introduction to Patient- and Family-Centered Clinical Practices
Nurse Bedside Change of Shift Report
toFrom Exclusive… Inclusive
“Communication breakdowns are a leading cause of medical errors…in 2005, a Joint Commission analysis found that 70 percent of sentinel events were caused by communication breakdowns, and half of those occurred during handoffs. To address the problem, the Joint Commission instituted a National Patient Safety Goal in 2006 calling on hospitals to implement a standardized approach to patient handoffs…”
Anderson, C. D., & Mangino, R. R. (2006). Nurse shift report: Who says you can’t talk in front of the patient? Nursing Administration Quarterly, 30(2), 112-122.
Nurse Bedside Change of Shift Report
• A safe, standardized approach to “hand offs,” (meeting the National Patient Safety Goal for communication.)
• Encourages patients and families to partner in their own care.
• Serves as an example of patient- and family-centered nursing practice.
“Nothing About Me Without Me.”
Nurse Change of Shift Report:Is This Your Current State?
▼ Change of shift report is an integral part of the nurses' daily workflow which often takes place in the nurses' station or break room.
▼ Impersonal (goals are directed by nursing; it is not a collaborative process with patients and families.)
▼ Limited, and sometimes inaccurate information is shared (report often does not reflect the actual status of the patient.)
Implementing Nurse Change of Shift Report at the Bedside
▼ The purpose is to share accurate, useful information between nurses and with patients and families and to engage patients and families in their care.
▼ Nursing staff conducts shift change reports at the patient’s bedside with the patient and family, in accordance with patient preference.
▼ The patient defines his/her family and/or other support person(s) and how they will be involved in care and care planning.
▼ Patient can share important information with nurses.▼ Report should take 3-5 minutes per patient.▼ Some units have an initial 3-5 minute huddle to provide an
overview of key issues for the unit that day.
Nurse Bedside Change of Shift
Nurse Bedside Change of Shift Report
Discussion questions:▼ What are the overall impressions of the bedside shift
report?▼ What went well?▼ What could have been done differently?▼ How is this practice change helpful to the nurse?▼ What questions or concerns do you have about bedside
shift report?
Benefits
• Better information and improved visibility to describe the patient's condition
• Accountability• Improved time management• Patient safety• Return to care at the bedside• Efficiency
Bedside Shift Report Improves Patient Safety and Nurse Accountability▼ Enhances patient and family involvement in and
understanding of care.
▼ Builds trust with the patient and family.
▼ Enhances safety.
▼ Builds teamwork, accountability, and commitment to quality work among nursing staff.
▼ Opportunity for real-time conversations.
▼ Saves time after becoming comfortable with change in practice.
▼ Practical tips for implementation included in the article.
Baker, S. J. (2010). Bedside shift report improves patient safety and nurse
accountability, Journal of Emergency Nursing, 36(4), 355-358.
Other Benefits to Nurses, Patients, and Families
▼ Provides nurses across shifts with hands-on, face-to-face interaction with the patient…key to individualizing care, building relationships, and avoiding misunderstandings.
▼ Offers up-to date information about the patient’s care to the patient and family, resulting in less anxiety, less uncertainty.
▼ Makes the nurse’s role in care transparent to patients and families.
▼ Increases patient, family, and nurse satisfaction.
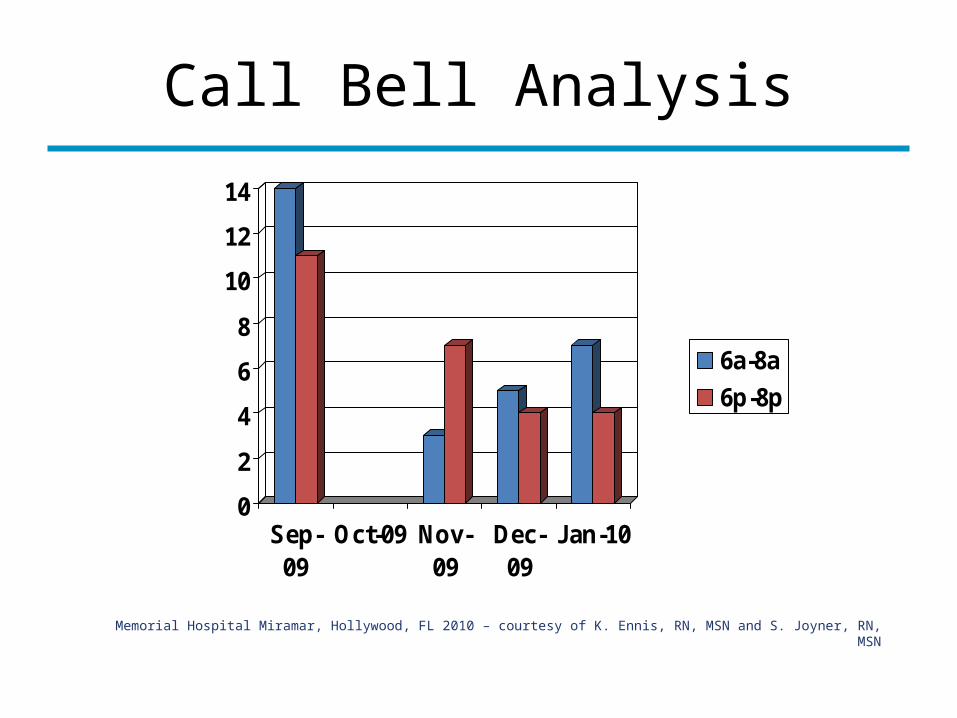
Call Bell Analysis
0
2
4
6
8
10
12
14
Sep-09
Oct-09 Nov-09
Dec-09
Jan-10
6a-8a
6p-8p
Memorial Hospital Miramar, Hollywood, FL 2010 – courtesy of K. Ennis, RN, MSN and S. Joyner, RN, MSN
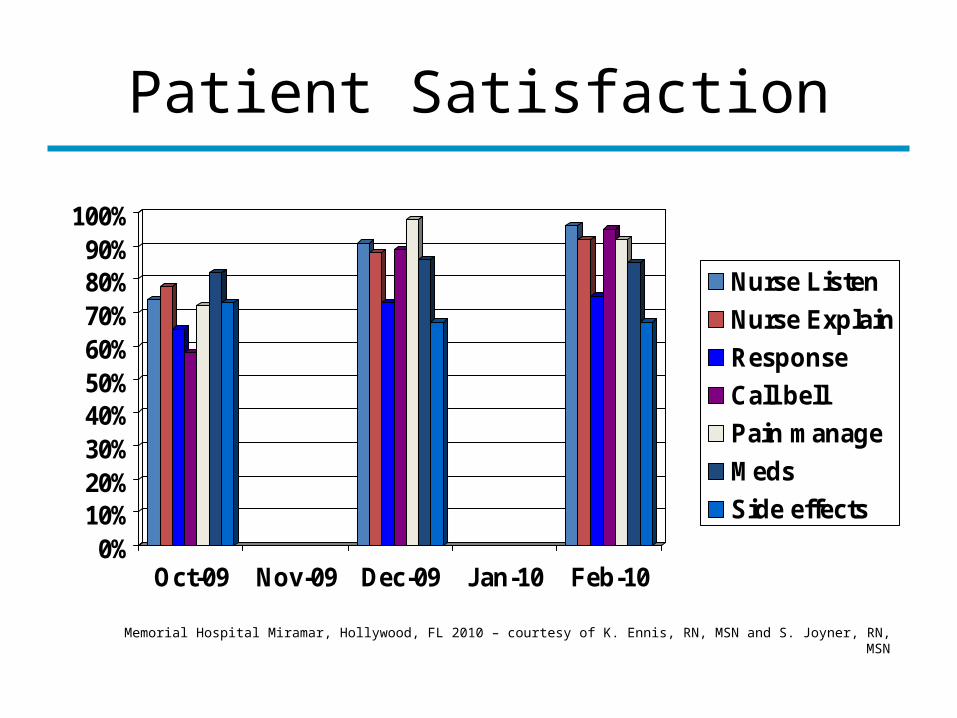
Patient Satisfaction
0%10%20%30%40%50%60%70%80%90%
100%
Oct-09 Nov-09 Dec-09 Jan-10 Feb-10
Nurse Listen
Nurse Explain
Response
Call bell
Pain manage
Meds
Side effects
Memorial Hospital Miramar, Hollywood, FL 2010 – courtesy of K. Ennis, RN, MSN and S. Joyner, RN, MSN
Nurses’ Concerns About Bedside Report
• Unknown visitors or family members in the room.• New diagnosis/information patient is not yet aware of
(waiting for doctor to discuss.)• Patient and/or family are asleep.• Patient is not following plan of care and you need to share this
information with the incoming nurse.• Patient or loved ones have complex questions that require
lengthy clarification.• Semi-private rooms/HIPAA concerns.
Semi-Private Rooms/HIPAA Concerns
• Health information can be disclosed for:TreatmentHealth care operationsPayment
• HIPAA acknowledges incidental disclosures may occur. This is not a HIPAA violation as long as you:Take reasonable safeguards to protect privacy.Only disclose or use the minimum information necessary.
HIPAA Concerns (cont’d)
• Can health care providers engage in confidential conversations with other providers or with patients, even if there is a possibility that they could be overheard?
• Yes. HIPAA does not prohibit providers from talking to each other and to their patients. Providers’ primary consideration is the appropriate treatment of their patients. Patient access to their health care information is important to quality, safety, and achieving the best outcomes.
• Patient access to their health information is important to quality, safety, and achieving the best outcomes. This must be balanced with the need to protect privacy.
HIPAA Concerns (cont’d.)
Oral communications often must occur freely and quickly. Providers are free to engage in communications as required for quick, effective, and high-quality health care. For example, when:• Coordinating services at nursing stations.• Discussing a patient’s condition or treatment regimen in the
patient’s semi-private room.• Discussing a patient’s condition during training rounds in an
academic or training institution.
Exercise 1
Glenda, a 55-year-old female with asthma and type 2 diabetes, was admitted to the unit this afternoon from the Emergency Department. Her symptoms were severe wheezing and vomiting for two days, abdominal pain, and dizziness. She received a multitude of treatments with Albuterol and steroids before admission. Her blood glucose is 200 and ketones are negative.
At evening shift change, Glenda says her breathing is better but her nausea is still present.
Debrief
• How did you each feel during this interaction?• What went well?• What could have been done differently?• Anything else?
Wrap Up
“Increased patient satisfaction was seen with the implementation of bedside shift report. By involving the patients in their plan of care and keeping all caregivers updated on that plan, patients feel more secure, and are more likely to participate in their own care and follow recommended health care options.”Acute care patients want more active involvement in their illness trajectory…today patients want to be involved or at least informed about health care options and alternatives (collaborative model). Bedside nurse reporting supports this model of informed choice and active patient participation.”
- Anderson, C. & Mangino, R. Nursing Administration Quarterly, 2006
Self Management Support
Chief Nurse of Mental Health Tuscaloosa VAMC
Self-Management Support▼ The assistance caregivers give to patients with chronic disease in order to
encourage and support patient’s daily decisions that improve health-related behaviors and clinical outcomes.
▼ A portfolio of techniques and tools that help patients choose healthy behaviors.▼ A fundamental transformation of the patient-caregiver relationship into a
collaborative partnership.▼ “The purpose of self-management support is to aid and inspire patients to
become informed about their conditions and take an active role in their treatment.”
Tom Bodenheimer, Helping Patients Manage Their Chronic Conditions, www.chcf.org, 2005
Encouraging Engagement
▼ This means inviting patients and their loved ones– clearly, explicitly, and probably over and over again–to: Ask questions until they get answers they understand. Participate in their care to the extent they want. Provide you with information only they have. Share their observations and concerns. Become a valued member of the health care team.
New Health Partnerships:
Improving Care by Engaging Patients
May 2009
Partnering in Self-Management
Support:A Toolkit for Clinicians
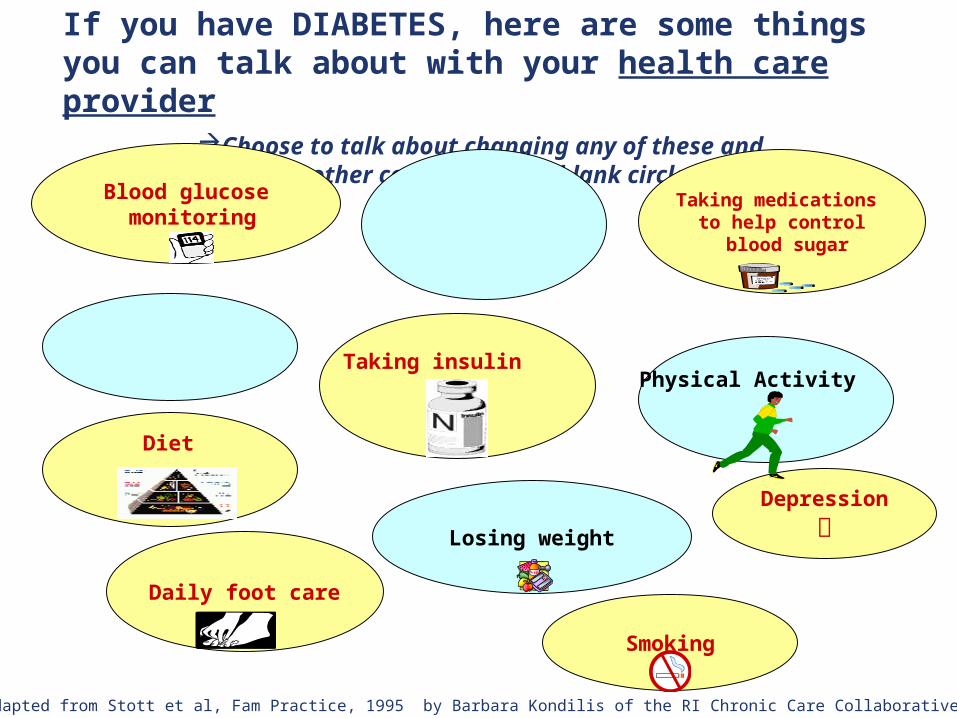
If you have DIABETES, here are some things you can talk about with your health care provider
Choose to talk about changing any of these and add other concerns in the blank circles.
Blood glucose monitoring
Taking medications to help control blood sugar
Losing weight
Daily foot care
Depression
Smoking
Taking insulin
Diet
Adapted from Stott et al, Fam Practice, 1995 by Barbara Kondilis of the RI Chronic Care Collaborative
Physical Activity
Self-Management Support• Describes and promotes the patient as the expert in managing
his or her chronic condition.• Emphasizes the patient’s central role in managing his/her
health.• Shares information and communication in a way that meets
patients’ and families’ needs and preferences. Explores and creates the plan based on the patient’s values, preferences, cultural, and personal beliefs.
• Collaboratively sets goal(s) and develops action plans; uses skill building and problem-solving strategies that help patients and families identify and overcome barriers to reaching goals.
• Provides follow-up on action plans and connects patients with community programs to sustain healthy behaviors.
Working as a Team
There's No 'I' in Team
Health care is a team sport, but all too often practitioners act as individual players. They're siloed from the time they walk into medical, nursing, or pharmacy schools to the time they touch their first patient. And while they may interact with each other in the care of a patient or a group of patients, those collaborations typically occur in short bursts and can result in communication lapses.
Matthew Weinstock, HHN Magazine, March 2010
Team Approaches
• Crew Resource Management (CRM)• Huddles• Briefings before handoff• Timeouts before surgery• SBAR (Situation, Background, Assessment, Recommendation)• TeamSTEPPS
The You CAN Campaign: Teamwork Training forPatients and Families in Ambulatory Oncology
Patient Aligned Care Team –Teamwork In Action
The Stockbridge Community-
Based Outpatient
ClinicExperience
Social Worker—Tuscaloosa
Coach and Mentor – Individualizing Care and
Communications
Nursing Director—Tuscaloosa VAMC
When a nurse or other caregiver enters a patient's room to give a medication, deliver a meal, or complete any task, what really takes place?
Clinical quality is seen as a measure of how skillfully and efficiently each task is performed.
But from the patient's perspective, every task is more than the delivery of health care. It is an opportunity for human interaction.
(Putting Patients First, p. 5)
I CARE PLANS Changing the Culture of Care
Planning• Medical Model
Staff know you by diagnosis
Staff write care plan based on what they think is best for your diagnosis
Interventions are based on standards of practice per diagnosis
▼ Community Model Staff have personal
relationship with resident and family
Resident, family, and staff develop care plan that reflects what resident desires for him/herself
Individualized interventions which meet the needs, priorities and preferences of that resident
Changing the Culture of Care Planning
• Medical ModelCare plan written in
the third personCare plan attempts
to fit resident into facility routine
Nursing assistants not part of interdisciplinary team
Care conference scheduled at facility convenience
▼ Community ModelCare plan written in first
person “I” formatCare plan identifies
resident’s lifelong routine and how to continue it in the nursing home
Nursing assistants present at each care plan conference
Care conference scheduled at resident and family convenience
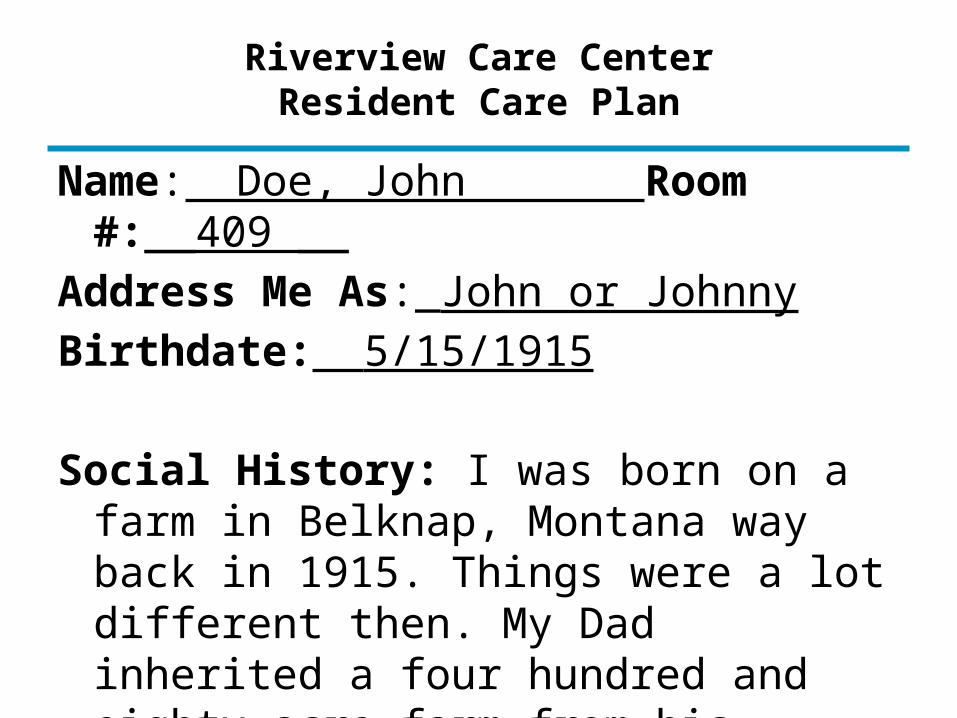
Riverview Care CenterResident Care Plan
Name: Doe, John Room #:__409 __Address Me As:_John or JohnnyBirthdate: 5/15/1915
Social History: I was born on a farm in Belknap, Montana way back in 1915. Things were a lot different then. My Dad inherited a four hundred and eighty acre farm from his father and this is where I grew up. We raised beef cattle and hay. After graduating from High School, I joined the Army Infantry and fought during WW II in France. My life changed for the better when in 1956, I met and married Jane. After we started our family, I took a position with Standard Oil as a regional manager. In 1980 I retired after 30 years of service.
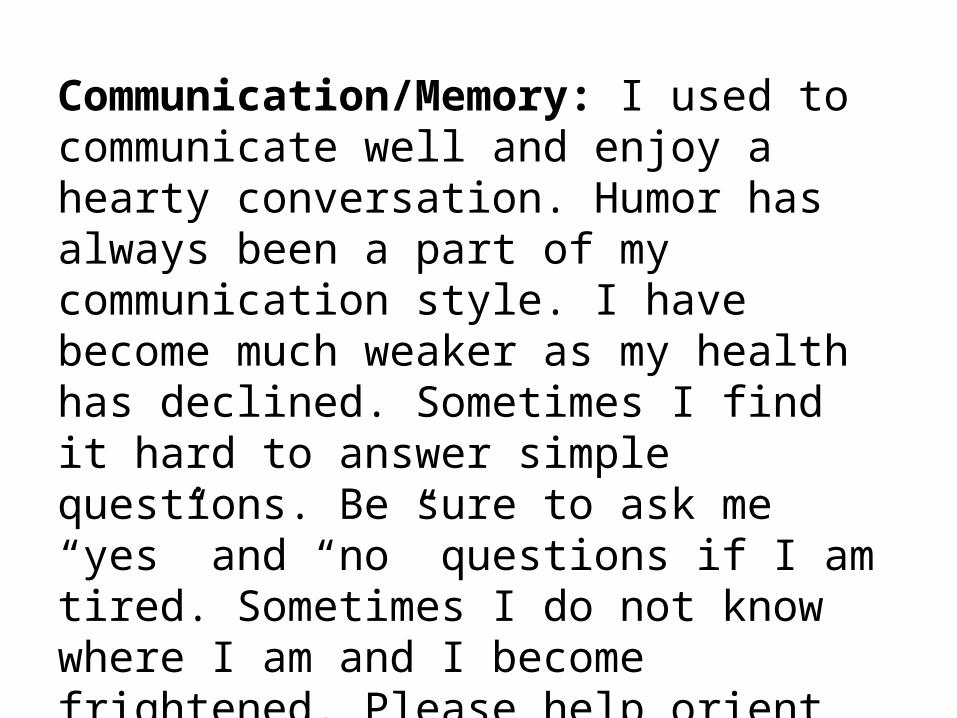
Communication/Memory: I used to communicate well and enjoy a hearty conversation. Humor has always been a part of my communication style. I have become much weaker as my health has declined. Sometimes I find it hard to answer simple questions. Be sure to ask me “yes” and “no” questions if I am tired. Sometimes I do not know where I am and I become frightened. Please help orient me during these times of confusion. Let me know who you are and what you are going to be doing. I usually recognize my children and my wife. Holding my wife's hand comforts me. When I am confused and frightened, I may strike out at you. Use calm gentle touch and hand massage while providing me reassurance.
Goal: I don't want my memory loss and confusion to interfere with my ability to accept the care I need.
I do not want to hurt my caregivers.
Why Stories?
“Facts bring us to knowledge, but stories lead to wisdom.”
Rachel Naomi Remen MD, “Kitchen Table Wisdom”
• Stories often bring us closer to our own buried wisdom and remind us of our courage.
• Stories can be powerful medicine. Sharing experiences and feelings through stories helps us make sense of our lives.
Tell A Story From Your Personal or Professional
Experience
Real Stories – Role Plays
• Real stories from your peers.• Break into groups of 4-5. • One or two will be observers, and will provide
feedback.• Listen to the situation–the transcript will be
on the screen after the video.• Using the Write Your Own Script worksheet,
take 3-4 minutes to determine how you will talk with the patient/family.
• Take 7-8 minutes to play out the scenario. • Debrief with the observers on your team.
Nurse--VAMC
Transcript• I think it's very important for the patient's
family member or significant other to be present during the hospital stay or the clinic visit.
• One example I can think of, we had a patient who came in, who had a GI surgery. The patient wasn't doing so well. He was feeling a little sick. We had to put down an NG tube to decompress the abdomen.
• The patient, he gave us this scenario. He had been to Vietnam, had all of these bombs dropped on him and all of these other really manly duties that he had done in his life previously and was really, really scared of what was going to happen when the nurse inserted the tube to go down into his stomach.
Nurse—Atlanta VAMC
Questions?
Reference Toolkit and How To Use
What Are Next Steps?

After the call to serve, many Veterans continue to pay a high price for the sacrifices they made at home and abroad.
Getting to know their stories becomes part of the healing.
“Let us not forget.”
Adapted from: Jillian Van Ens CNE, “Our Veteran Population”,
Spokane VAMC, June 2010