The Burden and Contributors to Cardiovascular Disease and Diabetes in Indigenous Australians Alex...
24
The Burden and Contributors to Cardiovascular Disease and Diabetes in Indigenous Australians Alex Brown Baker IDI
-
Upload
harold-ward -
Category
Documents
-
view
219 -
download
5
Transcript of The Burden and Contributors to Cardiovascular Disease and Diabetes in Indigenous Australians Alex...

The Burden and Contributors to Cardiovascular Disease and
Diabetes in Indigenous Australians
Alex Brown
Baker IDI

Years of Life Lost (YLL) for the leading disease and injury categories – Indigenous persons 2003
CVD & Diabetes
The Health and Welfare of Australia’s Aboriginal and Torres Strait and Islander Peoples 2008 ABS Catalogue No. 4704.0 AIHW Catalogue No. IHW 21

Page 3: Baker IDI
Contributors to the Gap
16.7 years 1996-2000 19.0 years 1996-2000
B/w 1996-2000
NCD - 77% Gap in LE
Grp I - 15-16%
CVD – 33%
GUT – 9%
DM – 9%
Chronic Resp - 9%
Injury – 8%
Zhao and Dempsey, MJA 2006

Driving Life Expectancy Differentials
Source: AIHW Chronic Disease and Associated Risk Factors in Australia, 2006.

Page 5: Baker IDI
Risk factor prevalence in Australian populations - glucose intolerance
Daniel M, Rowley KG, McDermott R, O’Dea K. Diabetes and impaired glucose tolerance in Aboriginal Australians: prevalence and risk. Diab Res Clin Pract 2002; 57: 23-33.
Dunstan D et al. Diabesity and associated disorders in Australia 2000. International Diabetes Institute, Melbourne, 2000

DIABETES MORTALITY -AUSTRALIA
Male Death Rates - Diabetes Female Death Rates - Diabetes
The Health and Welfare of Australia’s Aboriginal and Torres Strait and Islander Peoples 2008 ABS Catalogue No. 4704.0 . AIHW Catalogue No. IHW 21

Cardiovascular Consequences of DM• Clustered risk factors –MetS, dyslipidaemia, behavioural• CHD - Diffuse /Multi-vessel Disease • Silent Ischaemia• Late diagnosis/recognition• Complications of MI more frequent in DM
– CHF• Diabetic Cardiomyopathy• PVD• CVA• Absolute risk equivalent to PMHx of CHD

Impact of DM on CHD Incidence – INTERHEART I
Page 9: Baker IDI
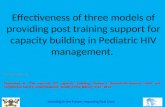
DM, CKD and CHD in Indigenous Australians
Wang and Hoy, Kidney Int 2005Wang and Hoy. MJA 2005

CAD and Diabetes in Aboriginal People

Risk of Incident CVD in Aboriginal People – Central Australia (n=739)
Rowley, Brown et al

DM AND CVD IN CENTRAL AUSTRALIA

Baseline Demographics and Clinical Characteristics, CASPA Cohort 2001-2002.
IndigenousN=214
Non-IndigenousN=278
p-Value
Mean age (± SD) years 50.1 (12.5) 59.3 (12.5) <0.001
Male (%) 57.0% 69.8% 0.003
History of CHD 39.3% 45.5% 0.166
Prior CABG 3.3% 9.4% 0.008
Hypertension 62.1% 45.0% <0.001
Smoker (current) 42.5% 35.3% 0.001
Dyslipidaemia 34.1% 38.5% 0.318
Diabetes Mellitus 55.6% 30.2% <0.001
CKD (GFR <60) 39.3% 24.7% 0.001
End stage renal failure 16.4% 1.8% <0.001
ACS Risk Stratification NSTEACS - High Risk STEMI
65.9%22.9%
49.3%20.5%
<0.0010.402
ACS onset in rural location 112 (47.7%) 23 (8.0%) < 0.001
Late Presentation >12hrs 63 (28.5%) 46 (17.1) 0.002
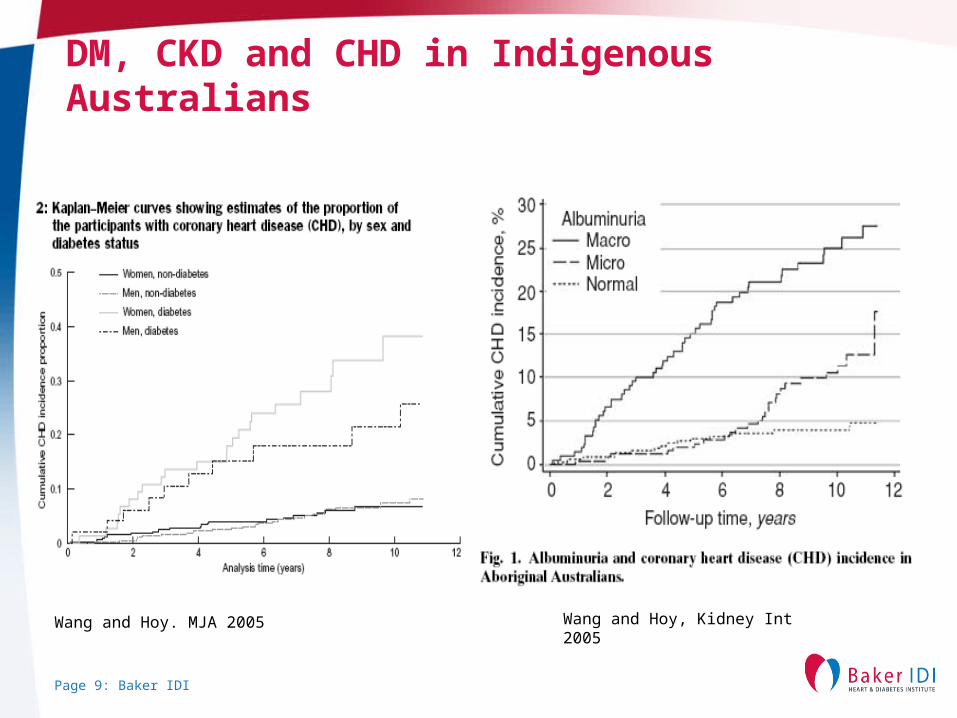
ACS Co-Morbidity by Ethnicity
64
29
74
68
Indigenous (n=235)
DMDM and CKD
CKD
24
51
63
149
DM DM and CKD
CKD
Non-Indigenous (n=287)
ACS and DM 59%
ACS + DM + CKD 27%
ACS + CKD 12%
ACS alone 29%
ACS + DM 30%
ACS + DM + CKD 8%
ACS + CKD 18%
ACS alone 52%
p=0.0001

Age Adjusted Survival and MACE-Free Survival – ACS [Males]
Indigenous
Non-Indigenous
HR = 3.762 [2.15 - 6.58]; p < 0.001 HR = 2.061 [1.40 - 3.02]; p < 0.001
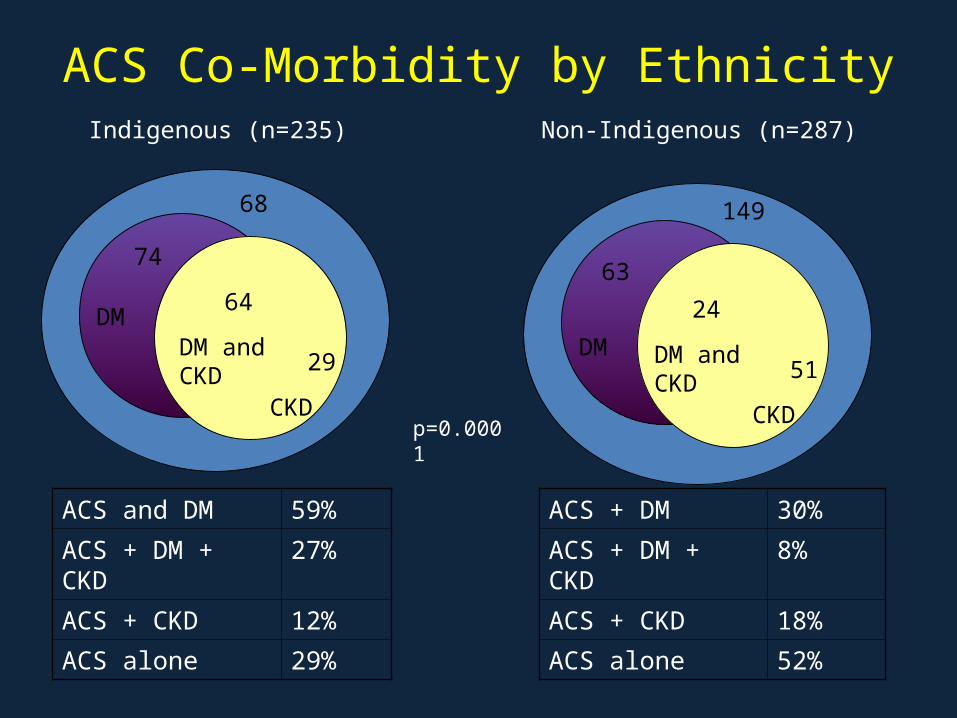
CVD RISK PREDICTION AND DM
WANG, ROWLEY, BROWN ET AL 2009

Page 17: Baker IDI
Potential Pathophysiological Pathways linking Chronic Stress, Depression and Atherogenesis. Adapted from Rozanski et al
Chronic Stress
Negative Emotional
States
CN
S M
ediated Effects
HPA Activation
SNS Activation
Adverse Behaviours
ANS Dysfunction
Insulin Resistance
Obesity
Inflammation
Platelet Activation
HPA Dysfunction
Endothelial Dysfunction

Depression in Aboriginal men -MHM


INDEPENDANT CORRELATES OF OBESITY IN ABORIGINAL MEN


Diabetes and Heart Disease -The Rumsfeld Criteria
“There are known knowns; there are things we know we know.
We also know there are known unknowns; that is to say there are some things we know we do not know.
But there are also unknown unknowns- the ones we don’t know we don’t know”
Fmr US Sec Defence, Donald Rumsfeld

The Known Known's – CVD AND DM
• Extremely common• DM is bad for your heart• Independent contributor to CVD in men and women • Independent predictor of adverse CVD outcomes• Commonly co-morbid in Indigenous populations• Accelerated atherogenesis the primary driver of excess death
and morbidity in DM• Same treatments are effective in DM• We know what we have to do• We know the system isn’t doing its job

Known Unknowns
• How to best deliver what needs to be done– Community based interventions– System level reforms– Reducing the evidence-practice gaps– Access
• Incorporating culture as a protective, preventative, management and palliative process
• SDIH • Racism/Stress/Marginalisation – biopsychosocial pathways to DM/CVD• Burden of CHF/interplay of DM among Indigenous peoples• How best to engage the family as the unit of intervention• Disadvantage across the life-course