The bleeding time as a preoperative screening test
4
The Bleeding Time as a Preoperative Screening Test ANN BARBER, M.D.* DAVID GREEN, M.D., Ph.D. THERESA GALLUZZO, M.T. (A.S.C.P.) CHUNGHSIN TS’AO, Ph.D. Chicago, Illinois From the Deparbnems of Medicine and Pathology, Northwestern Mernoriil Hospital and Northwestern University Medical School, and the Atheroscle- rosis Program, Rehabilitation Institute of Chicago, Chicago, Illinois. Requests for reprints should be addressed to Dr. David Green, Atherosclerosis Program, Northwestern University, Rehabilitation Institute of Chicago, 345 East Superior Street, Room 1407, Chicago, Illinois 60611. Manuscript accepted October 8, 1984. l Current address: Medicine Branch, National Cancer Institute, National Institutes of Health, Building 10, Room 12N226, Bethesda, Maryland 20815. To examine the benefit of determination of the bleedlng time as a preoperative screening test, the medical records of all patients who had a prolonged bleeding time during a six-month period were re- viewed. At Northwestern Memorial Hospttal, where the bteeding time test is part of the presurgical panel, 1,941 bleedlng t/me determl- nations were performed during six months. Prolonged Meeding times were recorded in 110 preoperative patients, of whom 83 (75 per- cent) had bleeding risk factors, including drug ingestion, thrombo- cytopenia, and azotemia. In these patients, the bleeding time ranged unpredictably from 10 to more than 20 minutes. However, of the 27 patients without apparent risk factors, only two had bleeding times of more than 20 minutes. This small number probably does not justtfy the routine use of the test in all preoperative patients. Rather, the test should be used selectively for those subjects who, on the basis of history or laboratory evidence, are suspected of being at risk of hemorrhage. Moreover, even in these patients, prolongation of the bleeding time may not always bs associated wtth excessive surgical blood loss. The bleeding time has been used to identify both quantitative and qualitative disorders of primary hemostasis since 1910. when Duke [l] first described the test. Since then, improvements in the technique of determining the bleeding time have resulted in a reliable and re- producible method for measuring primary hemostasis [2-51. The test is influenced by platelet number, platelet function, and vascular tone, and is used to predict susceptibility to bleeding [6]. For this reason, the bleeding time is often determined as a preop- erative screening test. In 1980, Bowie and Owen [7] recommended that the test be performed in all preoperative patients. More recently, however, Rapaport [8] suggested that determination of the bleeding time be omitted if a preoperative screening history reveals no recent aspirin ingestion, easy bruising, or unusual bleeding. Since the bleeding time is a routine preoperative test at our institution, we decided to retrospectively review our experience with the test. If prolonged bleeding times were discovered frequently or unexpectedly in pre- operative patients, then performance of the test as a routine preop- erative measure would be appropriate. If, on the other hand, abnormal bleeding times were rare and usually predictable, the additional ex- penses and discomfort of the test would be unwarranted. PATIENTS AND METHODS All bleeding time tests performed by the Hemostasis Laboratory of North- western Memorial Hospital during fhe six-month period from May 1 to October 31, 1983, were surveyed to identify patients with prolonged bleeding times. The medical records of these patients were reviewed for the following in- formation: history of bleeding disorders, list of medications, platelet count, May 1995 The American Journal ol Medicine Volume 78 761
-
Upload
ann-barber -
Category
Documents
-
view
213 -
download
1
Transcript of The bleeding time as a preoperative screening test

The Bleeding Time as a Preoperative Screening Test
ANN BARBER, M.D.* DAVID GREEN, M.D., Ph.D. THERESA GALLUZZO, M.T. (A.S.C.P.) CHUNGHSIN TS’AO, Ph.D.
Chicago, Illinois
From the Deparbnems of Medicine and Pathology, Northwestern Mernoriil Hospital and Northwestern University Medical School, and the Atheroscle- rosis Program, Rehabilitation Institute of Chicago, Chicago, Illinois. Requests for reprints should be addressed to Dr. David Green, Atherosclerosis Program, Northwestern University, Rehabilitation Institute of Chicago, 345 East Superior Street, Room 1407, Chicago, Illinois 60611. Manuscript accepted October 8, 1984. l Current address: Medicine Branch, National Cancer Institute, National Institutes of Health, Building 10, Room 12N226, Bethesda, Maryland 20815.
To examine the benefit of determination of the bleedlng time as a preoperative screening test, the medical records of all patients who had a prolonged bleeding time during a six-month period were re- viewed. At Northwestern Memorial Hospttal, where the bteeding time test is part of the presurgical panel, 1,941 bleedlng t/me determl- nations were performed during six months. Prolonged Meeding times were recorded in 110 preoperative patients, of whom 83 (75 per- cent) had bleeding risk factors, including drug ingestion, thrombo- cytopenia, and azotemia. In these patients, the bleeding time ranged unpredictably from 10 to more than 20 minutes. However, of the 27 patients without apparent risk factors, only two had bleeding times of more than 20 minutes. This small number probably does not justtfy the routine use of the test in all preoperative patients. Rather, the test should be used selectively for those subjects who, on the basis of history or laboratory evidence, are suspected of being at risk of hemorrhage. Moreover, even in these patients, prolongation of the bleeding time may not always bs associated wtth excessive surgical blood loss.
The bleeding time has been used to identify both quantitative and qualitative disorders of primary hemostasis since 1910. when Duke [l] first described the test. Since then, improvements in the technique of determining the bleeding time have resulted in a reliable and re- producible method for measuring primary hemostasis [2-51. The test is influenced by platelet number, platelet function, and vascular tone, and is used to predict susceptibility to bleeding [6].
For this reason, the bleeding time is often determined as a preop- erative screening test. In 1980, Bowie and Owen [7] recommended that the test be performed in all preoperative patients. More recently, however, Rapaport [8] suggested that determination of the bleeding time be omitted if a preoperative screening history reveals no recent aspirin ingestion, easy bruising, or unusual bleeding. Since the bleeding time is a routine preoperative test at our institution, we decided to retrospectively review our experience with the test. If prolonged bleeding times were discovered frequently or unexpectedly in pre- operative patients, then performance of the test as a routine preop- erative measure would be appropriate. If, on the other hand, abnormal bleeding times were rare and usually predictable, the additional ex- penses and discomfort of the test would be unwarranted.
PATIENTS AND METHODS
All bleeding time tests performed by the Hemostasis Laboratory of North- western Memorial Hospital during fhe six-month period from May 1 to October 31, 1983, were surveyed to identify patients with prolonged bleeding times. The medical records of these patients were reviewed for the following in- formation: history of bleeding disorders, list of medications, platelet count,
May 1995 The American Journal ol Medicine Volume 78 761

PREOPERATIVE BLEEDING TIMES-BARBER ET AL
0
:
”
ETIOLOGIC FACTOR
and serum urea nitrogen, creatinine, glutamic-oxaloacetic transaminase, lactic dehydrogenase, alkaline phosphatase, and total bilirubin levels. In addition, the reason the bleeding time test was requested and any related changes in patient management were noted. Because many patients underwent surgery before a subsequent normal bleeding time was re- corded, we re-examined these 58 medical records for pre- operative transfusions, intraoperative complications, esti- mated surgical blood loss, postoperative bleeding compli- cations, and in-hospital deaths. To estimate the total number of preoperative bleeding time tests performed during the six-month period, we prospectively recorded the indication for bleeding time tests over a subsequent four-week period and considered the percentage of preoperative bleeding time tests as representative for the entire survey period.
The bleeding time test was performed by the standardized Ivy method [4] using the Simplate II (General Diagnostics, Morris Plains, New Jersey). In our laboratory, the bleeding times of 12 normal subjects who had not ingested aspirin- containing drugs in the preceding two weeks were 5.5 f 3.5 minutes (mean f 2 SD). We consider a bleeding time of 10 minutes or more to be abnormal, as recommended by the manufacturer of the testing device.
RESULTS
Over the six-month period of the study, 1,94 1 bleeding time tests were performed; an estimated 95 percent (1,800) were for preoperative screening. Abnormal test results were recorded in 110 preoperative patients (6 percent). In 53 patients, the abnormal bleeding times were associated with aspirin ingestion. Thirteen ab- normal test results were associated with other drugs known to affect platelets, namely, nonsteroidal anti- inflammatory drugs (eight patients), high-dose penicillins
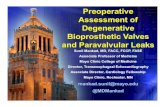
Figure 1. Prolonged bleeding times by etiologic factors in 110 preoperative pa- tients. NSAID = nonsteroidal anti-in- flammatory drugs other than aspirin.
(four patients), and intravenous nitroglycerin (one pa- tient). Eleven other subjects with prolonged bleeding times had platelet counts below lOO,OOO/~l, and six patients were uremic, with serum urea nitrogen levels above 60 mg/dl. No etiologic factors could be identified for the remaining 27 (25 percent). Bleeding time tests were repeated in 17 of these patients, and 12 gave normal results, suggesting previous but forgotten ex- posure to platelet-inhibiting substances. None of the patients in this series was found to have a primary he- mostatic disorder.
The distribution of the individual bleeding times by etiologic factor is shown in Figure 1. In patients with a history of aspirin ingestion, the median bleeding time was 11.5 minutes, but four subjects had values that exceeded 20 minutes. Similarly, in each of the other categories, there were subjects displaying markedly prolonged bleeding times. Overall, 23 of the 110 subjects (21 percent) had initial bleeding times in excess of 20 minutes. A repeated bleeding time was within normal range in eight of these and persistently pro- longed in five, and the test was not repeated in 10.
The effect of the initial abnormal bleeding time on subsequent surgical management was analyzed. Sur- gical management was not altered for 68 patients with abnormal bleeding times. For the remaining 42 patients, the abnormal bleeding time did change surgical plans, as surgery was canceled for three, delayed for 34, and carried out as scheduled for five but platelets were given or aspirin discontinued. As for the four patients with recent aspirin ingestion and bleeding times of more than 20 minutes, surgery was canceled because of myo-
702 May 1995 The American Journal of Medicine Volume 79

PREOPERATIVE BLEEDING TIMES-BARBER ET AL
MINOR MAJOR
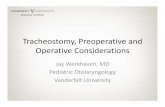
Figure 2. Estimated blood loss in patients with prolonged bleeding times undergoing minor and major surgical procedures (o”&n circles = preoperative platelet transfusiok). -
BLEEDING TIME (minutes)
cardial infarction in one, and aspirin was discontinued and a normal bleeding time recorded before surgery was performed in the other three.
Because surgery was performed in 58 patients without waiting for the bleeding time to normalize, the outcome of surgery was analyzed (Figure 2). In 12, the bleeding time had been measured days or weeks prior to surgery; however, in the remaining 46, it had been determined within 24 hours of surgery and was over 20 minutes in eight of these 46. Blood loss data were available for 39 of these 58 patients. Estimated surgical blood loss was 100 ml or less for all 12 patients having minor surgery and 500 ml or less for 21 of 27 patients having major surgery. The procedures associated with blood loss of more than 500 ml were placement of a hip prosthesis (600 ml), craniotomy (800 ml and 1,000 ml), renal transplantation (1,300 ml), femoropopliteal vas- cular grafting (1,500 ml), and spinal fusion (3,500 ml). The latter three patients had bleeding times of more than 20, 13, and 15.5 minutes, respectively. Another patient, whose bleeding time was more than 20 min- utes, had transient epistaxis during renal transplantation, but surgical blood loss was only 150 ml. There were no intraoperative deaths among the 58 patients. Postop- erative bleeding complications were noted in only seven patients, but three were receiving heparin and another was thrombocytopenic (5,000/& the remaining three
patients had hematoma, hematuria, or bleeding diver- ticuli, and these conditions required no further therapy. In summary, bleeding complications that could be at- tributed to prolonged preoperative bleeding times were recorded in only 10 of the 58 patients.
COMMENTS
This study set out to determine whether the bleeding time test is a valuable adjunct to the preoperative screening history and other routine laboratory tests such as platelet count, prothrombin time, and partial throm- boplastin time. Our results showed that 6 percent of 1,800 preoperative patients had prolonged bleeding times. Of these 110 patients, the abnormal bleeding times could have been suspected in 75 percent on the basis of medication intake, platelet count, or serum urea nitrogen level. Only two of the 27 patients whose pro- longed bleeding times could not have been suspected had values of more than 20 minutes. This small number probably does not justify the routine use of the bleeding time test in all preoperative patients.
Since aspirin ingestion was the most prominent single cause for the abnormal bleeding time observed in our survey, its use in connection with clinical bleeding merits some discussion. Michelson et al [9] and To- rosian et al [lo] reported significant increases in mediastinal blood loss in patients taking aspirin within
May 1995 The Amerkan Journal of Medicine Volume 79 783

PREOPERATIVE BLEEDING TIMES-BARBER ET AL
seven days of coronary bypass surgery. Stuart et al [ 1 l] observed bleeding tendencies in nine of 10 neonates whose mothers had ingested aspirin within five days of delivery. Six of the 10 mothers had excessive intra- partum and postpartum hemorrhage. In contrast, Amrein et al [ 121 gave a group of 129 patients 300 or 900 mg of aspirin four times daily beginning on the day before total hip replacement, but none on the day of surgery. Aspirin was continued for seven days after surgery. Although the mean bleeding time was significantly prolonged in these patients as compared with that in a control group, there was no correlation between in- creased bleeding time and excessive surgical blood loss. However, it should be noted that no patient in this series had a preoperative bleeding time greater than 12 minutes. In our retrospective review, all but two patients with bleeding times of up to 12 minutes underwent surgery without major hemorrhage, and bleeding in those having minor surgery was not excessive. Thus, enhanced bleeding in patients exposed to aspirin or other agents inhibiting platelet function probably de- pends on the extent of the prolongation of the bleeding time as well as on the degree of tissue trauma and other operative factors to which the patient is exposed. Al- though a carefully taken medical history may reveal that the patient has been exposed to a platelet-inhibiting
substance, the intensity of the effect of that substance on hemostasis is probably best indicated by the bleeding time test.
Several advantages of performing routine preoper- ative bleeding time tests can be cited: the detection of unanticipated abnormalities of primary hemostasis, the quantification of expected abnormal tests results, and the surgeon’s foreknowledge of the likelihood of de- fective hemostasis. On the other hand, the yield of ab- normal results with routine bleeding time tests is low (only 6 percent in our series). The number of patients with prolonged bleeding times without bleeding risk factors is quite small (27 of 1,800), and values over 20 minutes are infrequent (two of 27). If bleeding times were selectively determined only in patients with es- tablished risk factors, those most severely affected would be identified and excessive surgical bleeding avoided. However, only a prospective study, blinded so that the surgical team is unaware of the results of the screening bleeding time test, and with meticulous monitoring of bleeding during surgery, would define a “safe” bleeding time [ 131.
ACKNOWLEDGMENT
We thank Drs. Daniel Deykin and David Nahrwold for their helpful comments and suggestions.
REFERENCES
1. Duke WW: The relation of blood platelets to hemorrhagic erative hemostatic tests. Prog Hemost Thromb 1960; 5: disease: description of a method for determining the 179-209. bleeding time and coagulation time and report of three 6. Rapaport SI: Preoperative hemostasis evaluation: which test, cases of hemorrhagic disease relieved by transfusion. if any? Blood 1963; 61: 229-231. JAMA 1910; 55: 11651192. 9. Michelson EL, Morgenroth J, Torosian M, MacVaugh H Ill:
2. Ivy AC, Nelson 0, Bucher G: The standardization of certain Relation of preoperative use of aspirin to increased medi- factors in the cutaneous “venostasis” bleeding time astinal blood loss after coronary artery bypass graft sugary. technique. J Lab Clin Med 1941; 26: 1612-1622. J Thorac Cardiovasc Surg 1976; 76: 694-697.
3. Harker LA, Slichter SJ: The bleeding time as a screening test 10. Torosian M, Michelson EL, Morgenroth J, MacVaugh H Ill: for evaluation of platelet function. N Engl J Med 1972; 267: Aspirin- and coumadin-related bleeding after coronary ar- 155-159. tery bypass graft surgery. Ann Intern Med 1976; 69:
4. Mielke CH, Kaneshiro MM, Maher IA, et al: The standardized 325-326. normal Ivy bleeding time and its prolongation by aspirin. 11. Stuart MJ, Gross SJ, Elrod H, Graeber JE: Effects of acetyl- Blood 1969; 34: 204-215. salicyclic acid ingestion on maternal and neonatal hemo-
5. Kumar R, Ansell JE, Canoso RT. Deykin 0: Clinical trial of a stasis. N Engl J Med 1962; 307; 909-912. bleeding time device. Am J Clin Pathol 1976; 70: 642- 12. Arrrein PC, Ellman L, Harris WI-L Aspirininduced prolongation 645. of bleeding time and perioperative blood loss. JAMA 1961;
6. Quick AJ: The bleeding time as a test of hemostatic function. 245: 1625-1626. Am J Clin Pathol 1975; 64: 67-94. 13. Lind SE: Prolonged bleeding time. Am J Med 1964; 77:
7. Bowie EJW, Owen CA: The significance of abnormal preop- 305-312.
764 May 1985 The American Journal ol Yedlclne Volume 78