The Anatomy Lesson of Dr. Nicolaes Tulp, Journal of Hand Surgery (2006)

of 10
description
Rembrandt’s The Anatomy Lesson of Dr. Nicolaes Tulp (1632) is considered a masterpiece and is a group portrait of the Amsterdam Guild of Surgeons in the form of an anatomy lesson. Dr. Nicolaes Tulp, Doctor of Medicine and Praelector Anatomiae to the Amsterdam Guild of Surgeons, showed an anatomic dissection of a forearm on the corpse of an executed criminal. The anatomic accuracy in Rembrandt’s famous painting has been discussed in the literature for decades without any general consensus. In 2006, on the 400th anniversary of Rem- brandt’s birth, a forearm dissection of a cadaver and a comparison with the anatomy in the painting are presented to analyze the anatomic accuracy of Rembrandt’s famous painting.
Transcript of The Anatomy Lesson of Dr. Nicolaes Tulp, Journal of Hand Surgery (2006)
-
HISTORY OF HAND SURGERY
mylae):itutberthD,
Medicherland
olaesof Su
aelectforeas pai
for decades without any general consensus. In 2006, on the 400th anniversary of Rem-brandts birth, a forearm dissection of a cadaver and a comparison with the anatomy in thepainting are presented to analyze the anatomic accuracy of Rembrandts famous painting. (J
AThLethewhce
beres
traDrtorshTuThdirDrleffor
88Hand Surg 2006;31A:882891. Copyright 2006 by the American Society for Surgery of theHand.)Key words: Amsterdam Guild of Surgeons, forearm dissection, Nicolaes Tulp, Rembrandt,17th century.
lmost 4 centuries ago Rembrandt painted agroup portrait of the Amsterdam Guild ofSurgeons in the form of an anatomy lesson.
e painting, dated 1632, known as The Anatomysson of Dr. Nicolaes Tulp, should be placed within
tradition of anatomy paintings from the Guild,ich began in 1601 and extended far into the 18th
ntury.1 The painting is considered a masterpiececause Rembrandt seemingly created a realistic rep-entation of an anatomy lesson and abandoned theditional formal and stiff arrangement of figures.. Nicolaes Tulp, Doctor of Medicine and Praelec-Anatomiae to the Amsterdam Guild of Surgeons,
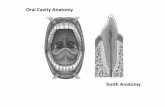
owed the dissection of a forearm (Fig. 1). To Dr.lps right side 7 members of the Guild are seated.2e Guild members facial expressions and visualections emphasize in a masterly way the climax of. Tulps demonstration.2 The gesture of Dr. Tulpst hand illustrates the function of the muscles in theearm and lends weight to his demonstration.2
Therefore, Tulps pose is that of a man who isspeaking to teach, and the members of the Guild arelistening to learn.2 Tulp presumably took the initia-tive to have himself painted with a group of Guildmembers in the tradition of his predecessors duringthe anatomic dissection, held on January 31, 1632, ofthe corpse of a 28-year-old executed criminal namedAdriaan Adriaansz, alias Aris t Kint (January 31,1632).13,513 Currently the painting is shown in theRoyal Picture Gallery Mauritshuis in The Nether-lands.
Public AnatomicLessons in the 17th CenturyFrom the beginning of the 16th century onward pub-lic anatomy lessons developed and spread acrossEurope.3 By the end of the century public anatomylessons were presented in many medical centers inEurope.3 In 1555 the Amsterdam Guild of Surgeonswas granted the privilege of dissecting the body of anThe Anatoof Dr. Nico
Rembrandt (1632of the Painting W
Left Forearm of a DFrank F. A. IJpma, MD, Ro
Jean-Philippe A. Nicolai, MD, P
From the Department of Plastic Surgery, UniversityThe Net
Rembrandts The Anatomy Lesson of Dr. Nicand is a group portrait of the Amsterdam GuildDr. Nicolaes Tulp, Doctor of Medicine and PrSurgeons, showed an anatomic dissection of aThe anatomic accuracy in Rembrandts famou2 The Journal of Hand SurgeryLessons Tulp byA Comparisonh a Dissectedch Male CadaverC. van de Graaf, MD,Marcel F. Meek, MD, PhD
al Center Groningen, University of Groningen,s.
Tulp (1632) is considered a masterpiecergeons in the form of an anatomy lesson.or Anatomiae to the Amsterdam Guild ofrm on the corpse of an executed criminal.nting has been discussed in the literature
-
ex
torelecitan
strgaleswe
wo
the1730hethethesiblocev
Gubeev
Letiocria c
bawe
thoint
DDran
of Leyden.1 The burial register on the death of one ofhishona
tenGuvo
boInma
tiosittheincimwr
taime
tieco
ea
looso
the
PrErThsec
Anbeforno
thepoan
hutombamu
thesee
huori19thetraistheex
thaof
Figofda
IJpma et al / The Anatomy Lesson of Dr. Nicolaes Tulp 883ecuted criminal to teach anatomy.57 The Praelec-, which literally means reader in anatomy, wascted by the city from among the physicians in they and would teach osteology, physiology, surgery,d zoology twice a week.1 Public anatomic demon-ations were given by the Praelector and were or-nized by the Guild once a year.1 Usually eachson would take longer than 1 day and the lessonsre held during the winter season so the corpseuld remain in relatively good condition because oflow temperatures.1,5 An anatomic theater of the
th century was designed to accommodate 200 to0 people.3,14 Even when no anatomic lesson wasld visitors were able to view the interior of theater with human and animal skeletons set up ongallery.1,14 Public anatomic lessons were acces-
le not only to members of the Guild but also toal citizens.1 Visitors paid admission to join the
ent.1 It is clear from the anatomy book of theild, which lists the public anatomic lessons held
tween 1631 and 1731, that they were popularents in Amsterdam.1 Rembrandts The Anatomysson of Dr. Nicolaes Tulp is considered the culmina-n of a series of events: the public execution of aminal, the public anatomic dissection of the corpse ofriminal hanged the day before, followed by a Guildnquet and a torch parade.3 Public anatomic lessonsre established initially for educational reasons, al-ugh by the end of the 16th century they had evolvedo popular events for the citizens.1
r. Nicolaes TulpNicolaes Tulp was born as Claes Pietersz in 15931
d he eventually studied medicine at the University
ure 1. Rembrandts painting (1632) The Anatomy LessonDr. Nicolaes Tulp. Reprinted with permission from Foun-tion Friends of the Mauritshuis, The Netherlands.children refers to a signboard with a tulip at hisuse.1 He choose a tulip for a coat of arms and theme Tulp became his family name.1 After hisure as Praelector Anatomiae of the Amsterdamild of Surgeons (16281653), Dr. Tulp was in-lved in politics later in his career and served asth city councilor and burgomaster of Amsterdam.1his medical career Tulp developed the first Phar-copoea Amstelredamensis, a book with descrip-ns for medication, as a result of the desperateuation in 1635 when Amsterdam was besieged by
plague and many people died as a result oforrectly prepared medication.1,57 Tulps mostpressive achievement in the medical field wasiting the book Observationes Medicae, which con-ns definite descriptions of the conditions, treat-nt, and recovery or cause of death of 231 pa-nts.1 He wrote about various forms of cancer, thennection between tobacco smoking and lung dis-ses, stones, a heart clot, palpitations, a head injury,se skin, cerebral palsy, and even a 2-headed per-
n.1 Tulp was the first person to describe and drawvalvula ileocecalis accurately.1
esumed Anatomicrors in Rembrandts Paintinge presumed mistakes in the anatomy of the dis-ted forearm in Rembrandts famous painting Theatomy Lesson of Dr. Nicolaes Tulp (1632) haveen discussed in medical and art-history literature
decades15,8,9,1113,1528; however, there is stillgeneral consensus about the observed structures indissected human forearm. In addition most view-
ints are based on comparisons of the painting withatomic atlases, not with a dissected forearm of aman cadaver. The discussion about presumed ana-ic errors in Rembrandts painting was initially
sed on the question of whether the flexor or extensorscles are represented.4 This is because the origin ofmuscles that Dr. Tulp is holding in the forceps
ms to appear from the lateral epicondyle of themerus; however, the flexor muscles of the forearmginate from the medial epicondyle of the humerus. In44 Wood Jones16 stated that Rembrandt had drawn
superficial flexor muscles of the right arm andnsferred them to the left arm. The lateral epicondylethe origin of the extensor muscles of the forearm;refore Heckscher4 argued that the painting represents
tensor muscles. Wolf-Heidegger17 concluded in 1967t the flexor muscles are represented. The intersectionsuperficial and deep flexor tendons, named Campers
-
chan
ma
strprostrstrtheco
sm
an
thedigradve
lenofthebraac
co
ma
AnthOnca
thearm
ingNiofne
The anatomic areas (Fig. 2), which were discussedma
folturPicscr
foran
ser
strsec
theforfouduSethi
ArReulnIt ithebywa
(F
thimu
Sobemu
flediatenlontheflaslo
theepco
fletraeqwi(Fthevo
so
Figpathaingtwlik
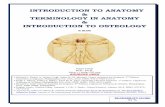
884 The Journal of Hand Surgery / Vol. 31A No. 6 JulyAugust 2006iasma, is visible clearly on the digits.9,18,19 Fouratomic areas in Rembrandts painting were discussedinly in the literature (Fig. 2): the sloping muscularucture that is prominent on the ulnar side of theximal aspect of the forearm (area 1), the muscular
uctures in Dr. Tulps forceps (area 2), the longaight muscular structure lying between the elbow andwrist on the ulnar side (area 3), and the longitudinal
rd-like white structure situated at the ulnar part of theall finger (area 4).15,8,9,1113,1528 Carpentier Altingd Waterbok18,19 reported in 1976 that the anatomy in
painting could be reproduced by lifting the flexoritorum superficialis together with the flexor carpiialis muscle in the forceps. In 1982, the 350th anni-
rsary of the painting, the editor of this Journal chal-ged readers to identify the anatomic error (the originthe flexor muscles from the lateral epicondyle) inpainting.15 In 2006, the 400th anniversary of Rem-ndts birth, we present this study to investigate the
curacy of the anatomy depicted in the painting bymparing the painting with the dissected forearm of ale cadaver.
atomic Comparison ofe Painting With a Cadaveric Dissectione left forearm from a 41-year-old preserved male
daver was dissected at the Department of Anatomy atUniversity of Groningen in The Netherlands. Thewas positioned and the skin was removed accord-
to Rembrandts painting The Anatomy Lesson of Dr.colaes Tulp. Muscles and tendons on the volar aspectthe forearm were isolated along with the lower armrves. Pictures were taken at every stage of dissection.
ure 2. Dissected forearm as depicted in Rembrandtsinting marked with 4 different areas of anatomic structurest have been discussed in the literature. Black arrow, slop-muscle; white arrow, single muscle belly situated be-
een the elbow and the wrist; red arrow, longitudinal cord-e white structure.inly in the literature, were analyzed according to thelowing 4 stages. In the first stage the anatomic struc-es in Rembrandts original painting at the Royalture Gallery Mauritshuis were observed and de-ibed without interpreting them. In the second stage aearm dissection was performed as described earlierd the anatomic structures in the cadaver were ob-ved and described. In the third stage the anatomicuctures of the painting were compared with the dis-ted forearm and analyzed. A detailed illustration ofdissected forearm in the original painting was usedcomparison during the anatomic dissection. In therth stage different approaches were used to repro-
ce the anatomy as depicted in Rembrandts paintingveral structures were dissected and transferred fors purpose.
ea 1mbrandts painting shows a sloping muscle on thear proximal side of the forearm (Fig. 2, black arrow).s a separate muscle belly that seems to originate frommedial epicondyle. Its insertion is partially covered
dissected skin. Once the forearm was dissected theres no sloping muscle observed as seen in the painting
ig. 3A).Because normally there is no muscular structure ins area we tried to transfer some superficial flexorscles to reconstruct area 1 similar to the painting.me investigators1719 believe the sloping muscle tothe palmaris longus muscle. The palmaris longusscle is a slender fusiform muscle situated ulnar to the
xor carpi radialis muscle. It originates from the me-l epicondyle of the humerus and courses as a longdon to insert at the palmar aponeurosis. The palmarisgus muscle was cut at the insertion and transferred toulnar side of the forearm. A muscle that was thin,
t, and not equal in bulkiness compared with theping muscle in the painting was shown (Fig. 3B).The flexor carpi radialis muscle is situated ulnar to
pronator teres muscle and arises from the medialicondyle. Its muscle belly is fusiform and forms ard-like tendon to the wrist. The palmaris longus andxor carpi radialis muscle insertions were cut andnsferred to the ulnar side of the forearm. An almostual amount of muscle tissue was created, comparableth the amount of muscle tissue visible in the paintingig. 3C). Removal of the palmaris longus muscle from
transferred muscle mass did not reduce the musclelume substantially.The pronator teres muscle has been suggested byme investigators2022 to be the sloping muscle;
-
holikthaprotheforThtheforma
co
tog
Figis cTh(C)to(Dsidlonthemusupparadtobemucopaco
IJpma et al / The Anatomy Lesson of Dr. Nicolaes Tulp 885wever, Bankl and Bankl20 stated that this is mostely the pronator teres muscle of the right arm andt it does not exist in this way in the left arm. Thenator teres muscle is situated at the radial part ofcubital region and passes obliquely across the
earm to insert on the lateral surface of the radius.e pronator teres muscle was cut at its insertion on
radius and transferred to the ulnar side of theearm along with the flexor carpi radialis and pal-ris longus muscles (Fig. 3D). Because of their
mmon origin these 3 muscles had to be transferredether. The volume of the transferred muscle mass
ure 3. (A) No sloping muscle is observed on the ulnar proximut at the insertion and transferred to the ulnar side of the fore
e flexor digitorum superficialis and the flexor carpi radialis mThe palmaris longus and the flexor carpi radialis muscles are
reconstruct the sloping muscle in the painting. Black arrow, fl) The pronator teres, flexor carpi radialis, and palmaris longue of the forearm in an attempt to recreate the sloping musclegus muscles; white arrow, pronator teres muscle. (E) The fleflexor digitorum superficialis muscle the insertion of the flexoscles are transferred to the ulnar side of the forearm to recreerficialis and the flexor digitorum profundus muscles are he
lmaris longus muscle transferred to the ulnar side of the foreialis muscles are held in the forceps. The palmaris longus m
recreate the sloping muscle in the painting. (H) The insertionlly to the proximal forearm with regard to its normal positioscle; white arrow, ulna; dotted line arrow, transfer directio
rd-like white structure was observed at the ulnar part of theinting a distal branch of the ulnar nerve is transferred to thiurse of the ulnar nerve.the dissection was much greater than the appear-ce of the muscle mass in the painting.According to Schupbach2 the sloping muscle shouldthe flexor carpi ulnaris muscle and the palmarisgus muscle is not shown in the painting because it is
sent in many human beings and, when present, iten comes off with the skin during dissection. Thexor carpi ulnaris muscle is the most ulnar-situatedscle of the superficial forearm flexors. It arises by 2
ads from the medial epicondyle of the humerus, thecranon, and the posterior border of the ulna. A thickdon forms its distal half and is attached to the pisi-
e of the dissected forearm. (B) The palmaris longus musclean attempt to recreate the sloping muscle in the painting.
s are held in the forceps. Arrow, palmaris longus muscle.d transferred to the ulnar side of the forearm in an attemptarpi radialis muscle; white arrow, palmaris longus muscle.cles are cut at their insertion and transferred to the ulnar
e painting. Black arrow, flexor carpi radialis and palmarisgitorum superficialis muscle is held in the forceps. To lifti radialis and the palmaris longus muscles were cut. Thesee sloping muscle in the painting. (F) The flexor digitorumhe forceps together, with the flexor carpi radialis and the(G) The flexor digitorum superficialis and the flexor carpis transferred to the ulnar side of the forearm in an attemptflexor carpi ulnaris tendon is cut and transfer of the muscleses the ulna. Black arrow, transferred flexor carpi ulnarise flexor carpi ulnaris muscle. (I) Initially no longitudinalfinger. To reproduce the white structure in Rembrandts
. Arrow, ulnar nerve; star, pisiform; dotted line, standardinan
belonaboftflemu
heoleten
al sidarm inusclecut anexor cs musin th
xor dir carpate thld in tarm.
uscle iof then expon of thsmall
s area
-
form, hamate, and fifth metacarpal bone. Transfer of theflesu
ev
is
obbrawa
flema
su
forthelikalimu
pa
ArThsev
sitfin
originate from muscle tissue centered between the
with id
886 The Journal of Hand Surgery / Vol. 31A No. 6 JulyAugust 2006xor carpi ulnaris muscle resulted in complete expo-re of the ulna. Because an exposed ulna was notident in Rembrandts painting the flexor carpi ulnarisnot likely the sloping muscle.It must be concluded that no muscular structure isserved at dissection as seen in area 1 on Rem-ndts painting. The presentation in the paintings represented most accurately by transferring thexor carpi radialis muscle with or without the pal-ris longus muscle. To elevate the flexor digitorum
perficialis muscle out of its natural bed with theceps (as depicted in the painting) the insertion offlexor carpi radialis muscle has to be cut. It is
ely that Dr. Tulp transferred the flexor carpi radi-s muscle to lift the flexor digitorum superficialisscle and created the sloping muscle as seen in the
inting (Figs. 3C, 4).
ea 2e structures held in Dr. Tulps forceps consist oferal muscle bellies (Fig. 2). The most radially
uated superficial muscle belly leads to an indexger tendon. Tendons to the middle and ring fingers
Figure 4. Dissected forearm in the paintingceps. The most ulnar superficial muscle bellyds to a small finger tendon. None of the depicteddons cross each other; they run straight towardmpers chiasm of each digit.The muscle in the forceps is believed to be thexor digitorum superficialis muscle.2,16 Other mus-s that have been proposed are the flexor carpi radialisether with the flexor digitorum superficialis mus-.18,19 The flexor digitorum superficialis muscle isuated deep to the flexor carpi radialis, palmaris lon-s, and pronator teres muscles. It is the largest of theperficial flexors and arises from 2 heads. The ulno-meral head arises from the medial epicondyle ofhumerus and the coronoid process of the ulna. Theial head originates from the proximal half of the
terior border of the radius. The flexor digitorum su-rficialis muscle gives rise to the tendons to the indexough small fingers. To lift the flexor digitorum su-rficialis muscle in our forceps we had to cut theertion of the flexor carpi radialis and palmaris longusscles (Fig. 3E). Dissection showed that the tendonsginate at different levels from the flexor digitorumperficialis muscle bellies. Tendons from the more
entification of the anatomic structures.forleatenCa
flecletogclesitgusu
hutheradan
pethrpeinsmu
orisu
-
volar bellies of the flexor digitorum superficialis musclepafrobeingflean
findigfortheob
ce
the(Ffletortogmu
thefroindoan
digdo(Cgeflefotisdigthe
fleca
wicleatithepa
en
mu
thamu
betherinsu
pa
Area 3Armu
wr
thesinthe
isulnfirItCuan
arm
ulnisan
no
3mu
ArAsco
levpalonsm
fleco
sen
Scciano
ser
tenprotendifstrno
insco
dothevo
oflikbraco
IJpma et al / The Anatomy Lesson of Dr. Nicolaes Tulp 887ss to the middle and ring fingers whereas tendonsm the deeper flexor digitorum superficial musclellies pass to the index and small fingers. In the paint-, however, tendons from the more volar bellies of the
xor digitorum superficialis muscle pass to the indexd small fingers instead of to the middle and ringgers and tendons from the deeper bellies of the flexoritorum superficialis muscle centered between theceps pass to the middle and ring fingers instead of toindex and small fingers (Figs. 3E, 4). The same
servation was made by Wolf-Heidegger and Cetto17In the painting more muscle volume in the for-ps is observed than would be anticipated from
flexor digitorum superficialis muscle aloneigs. 2, 3E). To recreate more muscle volume thexor digitorum superficialis and the flexor digi-um profundus muscles were held in the forcepsether (Fig. 3F). The flexor digitorum profundusscle arises deep to the superficial flexors fromanterior and medial surface of the ulna and
m the interosseous membrane. The muscle ends4 tendons that initially run inferior to the ten-ns of the flexor digitorum superficialis muscled the flexor retinaculum. In the hand the flexoritorum profundus tendons pass through the ten-
ns of the flexor digitorum superficialis muscleampers chiasm) to insert on the distal phalan-s. The flexor digitorum superficialis and thexor digitorum profundus muscles together in therceps resulted in greater bulkiness of musclesue but also exposed the tendons of the flexoritorum profundus muscle, which are not seen inpainting.
Previous publications18,19 have proposed that thexor digitorum superficialis together with the flexorrpi radialis muscle are held in Dr. Tulps forceps,th the palmaris longus muscle as the sloping mus-at the ulnar proximal side of the forearm. Recre-
ng this situation in the dissection did not result inanatomic appearance depicted in Rembrandts
inting (Fig. 3G).The muscle in Dr. Tulps forceps seems to be anlarged volume of the flexor digitorum superficialisscle alone (Fig. 4). Furthermore dissection showedt the tendons of the flexor digitorum superficialisscle originate at different levels from the muscle
llies compared with the painting. The position ofindex/small finger muscle bellies and the middle/
g finger muscle bellies of the flexor digitorumperficialis muscle are reversed in the painting com-red with the anatomic dissection.ea 3 in Rembrandts painting represents a singlescle belly situated between the elbow and theist (Fig. 2, white arrow). Its origin is covered by
sloping muscle and its insertion, consisting of agle tendon, is heading toward the ulnar aspect ofwrist.
There is debate as to whether the long straight musclethe flexor digitorum profundus2 or the flexor carpiaris.18,19 At dissection the flexor carpi ulnaris is the
st muscle to be seen at the ulnar side of the forearm.courses from the medial epicondyle to the pisiform.tting the insertion of the flexor carpi ulnaris tendond transferring the muscle belly to the proximal fore-
with regard to its normal position will expose thea (Fig. 3H). The flexor digitorum profundus muscle
situated radially from the flexor carpi ulnaris muscled courses to the digits. Because the exposed ulna ist seen in the painting the single muscle belly in areaof Rembrandts painting is the flexor carpi ulnarisscle (Fig. 4).
ea 4observed in Rembrandts painting a longitudinal
rd-like white structure appears proximally at theel of the distal forearm and courses to the ulnar
rt of the small finger (Fig. 2, red arrow). Thisgitudinal cord-like white structure has a slightlyaller diameter compared with the tendons of thexor digitorum superficialis but shares a similarlor.The structure has been proposed to be the dorsalsory branch of the ulnar nerve,18,19 although
hupbach2 believed the structure to be the superfi-l sensory branch of the ulnar nerve. At dissectionlongitudinal cord-like white structure was ob-
ved as shown in the painting resembling a nerve ordinous structure. It is not the flexor digitorumfundus tendon to the small finger because thatdon is much larger in diameter and is situated in aferent position than the longitudinal cord-likeucture depicted in the painting. The ulnar nerve isrmally situated radially from the pisiform and theertion of the flexor carpi ulnaris muscle and isvered by a slip of the flexor retinaculum. Thersal sensory branch of the ulnar nerve passes over
dorsum of the hand and is not visible from thelar aspect of the hand. With regard to the locationthe ulnar nerve at dissection the longitudinal cord-e white structure on the painting could not be anch of the ulnar nerve following its standard
urse (Fig. 4).
-
To reproduce the longitudinal cord-like white struc-turwr
theTuco
forstrtio
DThRelaehoepex
grotoistheshfrosec
visabforabforma
wiingproincce
mu
ofingabsitpaatoing
obdisno
icaberadlisthe
ature showed 5 general types of anomalies of thefletiotheser
diglumbeinthelesIt cthepava
oldmo
yedif
ca
su
Gusu
ne
pabraoftoman
Guco
see
locthetomprofrothedovisit gpaatmu
an
wipalikslico
ide
888 The Journal of Hand Surgery / Vol. 31A No. 6 JulyAugust 2006e in the painting we had to cut the ulnar nerve at theist and transpose its distal branch to the ulnar side ofpisiform (Fig. 3I). It seems highly unlikely that Dr.
lp transferred a nerve to recreate the longitudinalrd-like white structure as seen in the painting. There-e it must be concluded that the longitudinal cord-likeucture in the painting represents an anatomic varia-n of a branch of the ulnar nerve.
iscussione most apparent and well-known anatomic error inmbrandts painting The Anatomy Lesson of Dr. Nico-s Tulp is that the flexor muscles that Dr. Tulp islding in the forceps seem to originate from the lateralicondyle of the humerus.9,16,18,19,24 The forearm istended and supinated with the wrist placed in thein.18,19 The medial epicondyle of the humerus points
the corpse.18,19 The lateral epicondyle of the humerusturned away from the corpse in this position andrefore is not visible in the painting.18,19 Dr. Tulp
ows the flexor muscles of the forearm that originatem the medial epicondyle of the humerus The inter-tion of superficial and deep flexor tendons is clearlyible on the digits.9,18,19 The assumed anatomic errorout the lateral epicondyle of the humerus as the origin
the flexor muscles in Dr. Tulps forceps should beandoned with regard to the position of the dissectedearm in the painting. Dissection of the forearm of ale cadaver showed 4 anatomic differences comparedth Rembrandts painting: (1) the absence of the slop-
muscle that is prominent on the ulnar side of theximal aspect of the forearm in the painting, (2) anreased amount of muscle tissue in Dr. Tulps for-
ps, (3) the reversed position of the index/small fingerscle bellies and the middle/ring finger muscle belliesthe flexor digitorum superficialis muscle in the paint-compared with the anatomic dissection, and (4) the
sence of the longitudinal cord-like white structureuated at the ulnar part of the small finger in theinting. What is the explanation for the observed an-mic differences between the dissection and the paint-?Could anatomic variations be a reason for theserved differences between the painting and thesection? The sloping muscle (Fig. 2; area 1) hast been described as an anatomic variation in med-l literature. This muscular structure could haveen created by Dr. Tulp, transferring the flexor carpiialis muscle to lift the flexor digitorum superficia-muscle, or it can be considered an artistic error inpainting (Fig. 4). A review of the medical liter-xor digitorum superficialis muscle.29 These varia-ns include an associated muscle belly arising from
flexor digitorum superficialis tendon with rein-tion into the same tendon, attachment of the flexoritorum superficialis tendon to the flexor retinacu-, digastric muscles, distal extension of the muscle
llies, and anomalies of the superficial muscle layerthe distal forearm.29 However, the anomalies ofsuperficial muscle layer in the distal forearm are
s common and usually incompletely described.29annot be excluded that the observed differences offlexor digitorum superficialis muscle between the
inting and the dissection are based on anatomicriations. It should be mentioned that the 28-year-
executed criminal in Rembrandts painting has are muscular appearance compared with our 41-
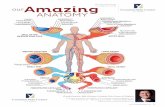
ar-old dissected corpse, which may explain theference in the amount of muscle tissue.Normally the ulnar nerve passes through Guyonsnal and divides into 2 branches at the carpus: aperficial sensory and a deep motor branch (Fig. 5A).yons canal is situated radial to the pisiform. The
perficial sensory branch divides into 2 compo-nts: an ulnar branch that forms the ulnar properlmar digital nerve of the small finger and a radialnch that forms the common palmar digital nervethe fourth intermetacarpal space.30 Several ana-ic variations have been described of the sensory
d motor branches of the ulnar nerve after passingyons canal.3032 At first sight the longitudinal
rd-like white structure in the painting does notm to be part of the ulnar nerve because it isated outside Guyons canal and is situated ulnar topisiform. Several case reports refer to an ana-ic variation of the ulnar nerve in which the ulnarper palmar digital nerve to the small finger arisesm the dorsal branch of the ulnar nerve instead of
superficial sensory branch (Fig. 5B).3336 Thersal branch of the ulnar nerve normally is notible on the volar aspect of the wrist. In these casesives off a branch that continues as the ulnar proper
lmar digital nerve to the small finger that emergesthe dorsomedial border of the flexor carpi ulnarisscle and the ulnar aspect of the pisiform. This
atomic variation of the ulnar nerve is in accordanceth the longitudinal cord-like white structure in theinting (Fig. 5C); however, the longitudinal cord-e white structure in the painting is coursingghtly toward Campers chiasma. The longitudinalrd-like white structure in the painting has beenntified as the dorsal branch of the ulnar nerve in
-
prean
bragitReofsliinco
sid
thetheofnitbrainaadbramo
hawhbeex
illusu
tomco
pasis
upsu
duorian
su
ticforbrash
Fig variatin tuatedan
IJpma et al / The Anatomy Lesson of Dr. Nicolaes Tulp 889vious literature.18,19 Without any reference to anatomic variation the standard course of the dorsalnch of the ulnar nerve could not explain the lon-udinal cord-like white structure in the painting.mbrandt could have painted an anatomic variationthe ulnar nerve, in which case the nerve coursingghtly toward Campers chiasma is an artistic errorthe painting (Fig. 4), or the entire longitudinal
rd-like white structure in the painting can be con-ered an artistic error.Could alterations or additions that have been made to
painting explain the anatomic difference betweenpainting and the dissected forearm? Restoration
the painting from 1996 to 1998 offered an opportu-y to analyze Rembrandts painting technique.1 Rem-ndt was an artist whose compositions gradually orig-ted on the canvas and during this process several
justments were made.1 All figures were part of Rem-ndts final composition.1 Frans van Loenen (seatedst superior) was portrayed initially wearing a black
t.1,2 The right hand from the corpse is painted onat initially was a stump.1,10 Aris t Kint could have
en punished by amputation of his right hand beforeecution.1,10 Rembrandt initially painted an anatomicstration of an arm on the paper held by one of the
rgeon observers. Rembrandts painting of an ana-ic illustration of an arm on the piece of paper was
vered by a second layer of paint, probably while theinting was being restored in the 18th century, con-ting of a list of names of the surgeon observers. The
ure 5. (A) Standard course of the ulnar nerve. (B) Anatomicwhich the longitudinal cord-like white structure (arrow) siatomic variation of the ulnar nerve.permost layer of paint with a list of names of thergeon observers has for the greater part been removedring the restoration from 1996 to 1998 so that theginal layer of paint with the anatomic illustration ofarm was made visible on the paper held by one of the
rgeon observers.1 There is no doubt about the authen-ity of the anatomic appearance of the dissected leftearm: its appearance is original as depicted by Rem-ndt in 1632.1 Research of the painting, however,
owed that Rembrandt had replaced the dissected fore-from a higher to a lower position in the painting.1
e adjustments to the painting that were made bymbrandt indicate that the painting went through therking process of the painter. It cannot be excludedt adjustments to the painting contributed to the ana-ic differences between the painting and the dis-
ted forearm.Is it possible to recall the circumstances in whichmbrandt made the painting? Did Rembrandt makewings during Dr. Tulps public anatomic lesson
d use them to create the painting later in his work-op? There are no records about Rembrandt beingeyewitness to the dissection1 and to our knowl-
ge no drawings that could have been made bymbrandt during the public anatomic lesson areailable. Did he use a real limb with or withoutditional anatomic illustrations to finish the paint-? Records about the corpse having been broughthis workshop are not available.1 The details andlistic colorful appearance of the original painting
ion of the ulnar nerve. (C) Dissected hand in the paintingat the ulnar side of the hand could be identified as anarm
ThRewo
thatomsec
Redraan
shan
edReav
adingtorea
-
suggests that Rembrandt used a real limb and theme
pleboan
beto(Dan
FaRearm
no
wh
hissitdidpuNoGuan
co
or
gerepLeinrepJanwa
om
viddisgrasininofthe
allthetoev
therea
rec
ratan
ora
rec
an
edge of God.13 Even moralizing inscriptions insidethetor
inaTupieSemu
plian
strrethiseyas
co
theinsTuteastumiforco
be
ThePicinghelme
ava
dedR
FebN
com
CPlae-m
C0d
Re1.
2.
3.
4.
890 The Journal of Hand Surgery / Vol. 31A No. 6 JulyAugust 2006mbers of the Guild posed for Rembrandt to com-te the painting.1,2,18,19 Attempts at identifying the
ok on the standard (Fig. 1; right corner) and theatomic illustration (Fig. 1; held by one of the mem-rs of the Guild) have been unsuccessful.1 Accordingprevious literature the anatomic works of Vesaliuse Humani Corporis Fabrica Libri Septem in 1543)d Adriaen van den Spieghel (De Humani Corporisbrica Libri Decem in 1627) are not consideredmbrandts direct model in creating the dissected
as seen in the painting1,2,9,1719,25; however, it ist possible to construct the exact circumstances inich Rembrandt created the painting.A portrait painters success depended heavily on
skills to produce an acceptable likeness of histers following existing visual conventions,37 but
Rembrandt record an exact representation of theblic anatomic lesson held on January 31, 1632?ne of the anatomy paintings of the Amsterdamild of Surgeons display an exact representation ofanatomic lesson.1 They are all group portraits and
mmemorate the tenure of a Praelector Anatomiaemembership of the Amsterdam Guild of Sur-
ons.1 Rembrandt seems to have painted a realisticroduction of an anatomy lesson.1 The Anatomy
sson of Dr. Nicolaes Tulp records a group portraitthe form of an anatomy lesson but not an exactresentation of Tulps anatomic dissection held onuary 31, 1632. In group portraits from 1684 on-rd it is even more obvious that the depicted anat-y is not the primary interest but rather the indi-uals themselves are The dissecting table with asected body of an executed criminal was replaceddually by a desk with, for example, a skull or agle dissected organ. The contribution of anatomythe collection of paintings of the Amsterdam GuildSurgeons decreased over time and the figuresmselves increasingly dominate the compositions.A public anatomic lesson in the 17th century usu-y started with dissecting the perishable organs ofabdomen and thorax; the extremities were the lastbe dissected.13 In Rembrandts painting, how-
er, the forearm already has been dissected whereasrest of the body still is intact. This is another
son to believe that Rembrandts painting does notord the real situation of Dr. Tulps dissection buther represents a symbolic interpretation.13 Publicatomic lessons were often preceded by a moralistiction in which the audience was encouraged toognize their own mortality.13 The science of
atomy was considered a path toward the knowl-anatomic theater reminded visitors of the transi-y of existence.1Andreas Vesalius (15141564), an anatomist orig-lly from Brussels, is believed to have influencedlps choice of pose through the woodcut frontce of his book De Humani Corporis Fabrica Libri
ptum with a portrait of himself showing the flexorscles of the forearm.13 Vesalius had accom-shed a revolution in the knowledge of humanatomy by studying the functionality of anatomicuctures in a practical way and refuting the theo-ic descriptions of the ancient anatomists.1,3,10 Inown book Tulp wrote that anatomy is the very
e of medicine and that it brought forth the truthit were out of the shadow into the light.2 Vesaliusnsidered the human hand a physical counterpart of
human psyche, an instrument for using furthertruments and a representation of Gods wisdom.2lp was familiar with Vesaliuss theories from hischer in Leyden (Pieter Pauw), who had been adent of Vesalius.1 One century later Dr. Tulpght have chosen to be depicted with a dissectedearm to be considered the Vesalius of his time andnfirmed a new era in establishing the connectiontween practical anatomy and functionality.
authors acknowledge Frederik J. Duparc, Director of the Royalture Gallery Mauritshuis, and Norbert Middelkoop, Curator of Paint-s, Prints, and Drawings of the Amsterdam Historical Museum for theirp and reviewing the manuscript. The authors also thank the Depart-nt of Anatomy of the University of Groningen for their help and theilability of the preserved body and A. Sterodimas for his help andication during the dissection.eceived for publication January 17, 2006; accepted in revised formruary 13, 2006.o benefits in any form have been received or will be received from amercial party related directly or indirectly to the subject of this articleorresponding author: Marcel F. Meek, MD, PhD, Department of
stic Surgery, Hanzeplein 1, 9700 RB Groningen, The Netherlands;ail: [email protected] 2006 by the American Society for Surgery of the Hand363-5023/06/31A06-0002$32.00/0oi:10.1016/j.jhsa.2006.02.014
ferencesMiddelkoop N, Noble P, Wadum J, Broos B. Rembrandtunder the scalpel. The Anatomy Lesson of Dr Nicolaes Tulpdissected. Amsterdam: Six Art Promotion BV, 1998;9-78.Schupbach W. The paradox of Rembrandts Anatomy ofDr. Tulp. Med Hist Suppl 1982;2:1110.Heckscher WS. Rembrandts Anatomy of Dr. Nicolaas Tulp:an iconological study. Washington: New York UniversityPress, 1958:40.Heckscher WS. Rembrandts Anatomy of Dr. Nicolaas Tulp:an iconological study. Washington: New York UniversityPress, 1958.
-
5. Goldwyn RM. Nicolaas Tulp (15931674). Med Hist 1961;5:270276.
6. Glazenburg J. Rembrandts anatomy of Dr. Nicolaas Tulp.Arch Chir Neerl 1977;29:8391.
7. Glazenburg J. Rembrandts Anatomy of Dr. Nicolaas Tulp.Int Surg 1976;61:586590.
8. Broos BPJ De anatomische les van Dr. Nicolaes Tulp. In:Broos BPJ, ed. Meesterwerken in het Mauritshuis. DenHaag: Staatsuitgeverij, 1987:277288.
9. Lindeboom GA. [Letter: dissection errors in RembrandtsAnatomy Lecture?] Ned Tijdschr Geneeskd 1976;120:7173.
10. Masquelet AC. The anatomy lesson of Dr. Tulp. J Hand Surg2005;30B:379381.
11. Mills AR. Rembrandts painting of the Anatomy lesson ofDr Tulp. Proc R Coll Phys Edinb 1989;19:327330.
12. Kruger L. The scientific impact of Dr. N. Tulp, portrayed inRembrandts Anatomy Lesson. J Hist Neurosci 2005;14:8592.
13. Bezerra AJ, DiDio LJ, Piva-Junior L. Dissection of Rem-brandts Anatomy of Dr. Nicolaas Tulp. Arch Ital AnatEmbriol 1991;96:153164.
14.
15.16.
17.
18.
19.
20.
21.
22. Scothorne RJ. Rembrandts painting of the anatomy lessonof Dr Tulp. Proc R Coll Phys Edinb 1989;19:330.
23. Scherer H. Rembrandts Dr. Tulps Anatomy Lesson.Minn Med 1990;73:2428.
24. Smeulers J. [Letter: dialogue between the clinician and thepreclinical student.]Ned Tijdschr Geneeskd 1975;119:18691870.
25. Lindeboom GA. [Letter: HogarthVesaliusRembrandt.]Ned Tijdschr Geneeskd 1975;119:18691870.
26. De Lint JG. Rembrandt. The Hague: J. Philip Kruseman,1930.
27. Cremone JC Jr. The anatomy lesson of Dr. Nicolaas Tulp.J Hand Surg 1982;7:530.
28. Meals RA. The anatomy lesson of Dr. Nicolaas Tulp. J HandSurg 1982;7:530.
29. Elliot D, Khandwala AR, Kulkarni M. Anomalies of theflexor digitorum superficialis muscle. J Hand Surg 1999;24B:570574.
30. Bonnel F, Vila RM. Anatomical study of the ulnar nerve inthe hand. J Hand Surg 1985;10B:165168.
31. Murata K, Tamai M, Gupta A. Anatomic study of variations
32.
33.
34.
35.
36.
37.
IJpma et al / The Anatomy Lesson of Dr. Nicolaes Tulp 891Duparc FJ. De kunst van de anatomie ontleed. In: Jansen I,Korevaart K, Korsten M, Molenaar J, Otterspeer W, eds.Kopstukken over topstukken, lezingenreeks Universiteit Lei-den. Leiden: Universiteit Leiden, 2001:118133.Light TR. Hands on stamps. J Hand Surg 1982;7:20.Wood Jones F. Principles of anatomy, as seen in the hand.London: Ballire, Tindall & Cox, 1944.Wolf-Heidegger G, Cetto AM. Die anatomische Sektion inbildlicher Darstellung. Bazel: Karger, 1967.Carpentier Alting MP, Waterbok TW. New light on theanatomical errors in Rembrandts Anatomy Lesson of Dr.Nicolaas Tulp. J Hand Surg 1982;7:632634.Carpentier Alting MP, Waterbok TW. [New lights on thedissecting errors in Rembrandts Anatomical lesson by Dr.Nicolaas Tulp.] Ned Tijdschr Geneeskd 1976;120:19001902.Bankl HC, Bankl H. [A critical view of Rembrandts Anat-omy Lesson.] Wien Klin Wochenschr 2000;112:368371.Romanes GJ. Rembrandts painting of the anatomy lesson ofDr Tulp. Proc R Coll Phys Edinb 1989;19:330.of hypothenar muscles and arborization patterns of the ulnarnerve in the hand. J Hand Surg 2004;29A:500509.Bas H, Kleinert JM. Anatomic variations in sensory inner-vation of the hand and digits. J Hand Surg 1999;24A:11711184.Bozkurt MC, Cezayirli E, Tagil SM. An unusual termi-nation of the ulnar nerve in the palm. Ann Anat 2002;184:271273.Konig PS, Hage JJ, Bloem JJ, Prose LP. Variations of theulnar nerve and ulnar artery in Guyons canal: a cadavericstudy. J Hand Surg 1994;19A:617622.McCarthy RE, Nalebuff EA. Anomalous volar branch of thedorsal cutaneous ulnar nerve: a case report. J Hand Surg1980;5:1920.Kaplan EB. Variation of the ulnar nerve at the wrist. BullHosp Joint Dis 1963;24:8588.Middelkoop N. Gezicht op Amsterdammers, Amsterdam-mers geportretteerd en verzameld. In: Middelkoop N, ed.Amsterdammers geportretteerd, 16001800. Amsterdam:Uitgeverij THOTH, Amsterdams Historisch Museum, 2002:1027.
The Anatomy Lesson of Dr. Nicolaes Tulp by Rembrandt (1632): A Comparison of the Painting With a Dissected Left Forearm of a Dutch Male CadaverPublic Anatomic Lessons in the 17th CenturyDr. Nicolaes TulpPresumed Anatomic Errors in Rembrandt's PaintingAnatomic Comparison of the Painting With a Cadaveric DissectionArea 1Area 2Area 3Area 4
DiscussionAcknowledgementReferences