
The American Journal of Medicine
45
The American Journal of Medicine Volume 120, Issue 10, Supplement 2, Pages S1-S41 (October 2007) 1. Title Page Page i 2. Faculty List Page iv 3. Faculty Disclosures Page v 4. Introduction Page S1 Andrew F. Shorr 5. Newer Modalities for Detection of Pulmonary Emboli Pages S2-S12 Seth Clemens and Kenneth V. Leeper Jr. 6. Inferior Vena Cava Filters in the Management of Venous Thromboembolism Pages S13-S17 Mark A. Crowther 7. Outpatient Management of Stable Acute Pulmonary Embolism: Proposed Accelerated Pathway for Risk Stratification Pages S18-S25 Amjad AlMahameed and Teresa L. Carman 8. Prevention and Management of Venous Thromboembolism in Pregnancy Pages S26-S34 Andra H. James 9. The Pharmacoeconomics of Deep Vein Thrombosis Treatment Pages S35-S41 Andrew F. Shorr
Transcript of The American Journal of Medicine

The American Journal of Medicine Volume 120, Issue 10, Supplement 2, Pages S1-S41 (October 2007)
1. Title Page Page i
2. Faculty List Page iv
3. Faculty Disclosures Page v
4. Introduction Page S1 Andrew F. Shorr
5. Newer Modalities for Detection of Pulmonary Emboli Pages S2-S12 Seth Clemens and Kenneth V. Leeper Jr.
6. Inferior Vena Cava Filters in the Management of Venous Thromboembolism Pages S13-S17 Mark A. Crowther
7. Outpatient Management of Stable Acute Pulmonary Embolism: Proposed Accelerated Pathway for Risk Stratification Pages S18-S25 Amjad AlMahameed and Teresa L. Carman
8. Prevention and Management of Venous Thromboembolism in Pregnancy Pages S26-S34 Andra H. James
9. The Pharmacoeconomics of Deep Vein Thrombosis Treatment Pages S35-S41 Andrew F. Shorr

I
morPedt
ataftgtrJLlt
actbwlaad
vtctdF
np
P1
0d
The American Journal of Medicine (2007) Vol 120 (10B), S1
ntroductionodfia
miptAcricaw
aecctImtd
mtt
R
1
2
3
Pulmonary embolism (PE) remains a major challenge inedicine. Historically, any type of physician may be called
n to diagnose and manage PE. Frustratingly, mortalityates may approach 30% in medical patients with untreatedE. With rapid identification and appropriate therapy, how-ver, mortality is dramatically reduced.1 Early and accurateiagnosis of this potentially fatal condition is therefore ofhe utmost importance.
Although much has been written on risk assessment, lessttention has been given to the recent technologic advanceshat enable quick and accurate diagnosis of PE. Pulmonaryngiography has long been held to be the “gold standard”or definitive diagnosis, yet newer modalities have emergedo challenge this assumption. Recently, computed tomo-raphic pulmonary angiography with or without imaging ofhe lower extremities has all but replaced traditional angiog-aphy. In the first article of this supplement to The Americanournal of Medicine, Drs. Seth Clemens and Kenneth V.eeper review the evidence on the relative accuracies and
imitations of these newer modalities, concluding with howhey fit into an algorithm for first-line evaluation of PE.
Additionally, this supplement focuses on several areas ofctive controversy. The ease of introduction of inferior venaava filters and the advent of retrievable devices have led toheir expanded use. Yet, according to current evidence-ased guidelines, they are recommended only for patientsith proven venous thromboembolism (VTE) and an abso-
ute contraindication for anticoagulation, a complication ofnticoagulation, or recurrent VTE despite adequate antico-gulation.2 Dr. Mark A. Crowther reviews the limited evi-ence currently available on these devices.
Although outpatient management of patients with deepein thrombosis is becoming more widely accepted, outpa-ient treatment of persons with PE remains an area of un-ertainty. Yet, new data are emerging to show that outpa-ient treatment may be feasible for selected patients who areeemed to be at low risk based on careful risk stratification.ollowing an overview of the pathogenesis and epidemiol-
Statement of conflict of interest: Andrew F. Shorr, MD, MPH, reportso conflict of interest with the sponsor of this supplement article orroducts discussed in this article.
Requests for reprints should be addressed to Andrew F. Shorr, MD, MPH,ulmonary and Critical Care Medicine Service, Washington Hospital Center,10 Irving Street NW, Washington, District of Columbia 20010.
E-mail address: [email protected].
002-9343/$ -see front matter © 2007 Elsevier Inc. All rights reserved.oi:10.1016/j.amjmed.2007.07.013
gy of PE, Drs. Teresa L. Carman and Amjad AlMahameediscuss risk stratification and the available evidence, bene-ts, and therapeutic options pertaining to outpatient man-gement of these patients.
Thromboembolic disease is now the leading cause ofaternal death in the United States.3 Pregnant women are at
ncreased risk of thrombosis both during pregnancy andostpartum, due to a relative hypercoagulable state that ishought to have evolved to protect them from hemorrhage.nticoagulation in these patients is challenging, requiring
onsideration of both maternal and fetal issues. After aeview of risk factors for thrombosis in pregnancy andndications for VTE prophylaxis, Dr. Andra H. James dis-usses options for prophylaxis, initiation of anticoagulation,nd diagnosis and management of VTE in pregnancy, asell as management at parturition and postpartum.Finally, in today’s world of third-party payers and man-
ged care medicine, pharmacoeconomics is assuming anver-increasing role. The economic burden posed by VTE isonsiderable, and pharmacoeconomic analyses have be-ome a useful tool for helping clinicians select appropriateherapy from among similarly effective and safe therapies.n the last article of this supplement, I discuss factors thatay affect the relative costs of different approaches to
reatment and review recent clinical and pharmacoeconomicata comparing fondaparinux with enoxaparin.
We hope that readers will find the articles in this supple-ent both thought provoking and useful as a guide for detec-
ion and management of an important condition that is poten-ially devastating, yet treatable if detected in a timely manner.
Andrew F. Shorr, MD, MPHPulmonary and Critical Care Medicine Service
Washington Hospital CenterWashington, District of Columbia, USA
eferences
. Carson JL, Kelley MA, Duff A, et al. The clinical course of pulmonaryembolism. N Engl J Med. 1992;326:1240–1245.
. Buller HR, Agnelli G, Hull RD, Hyers TM, Prins MH, Raskob GE.Antithrombotic therapy for venous thromboembolic disease: the Sev-enth ACCP Conference on Antithrombotic and Thrombolytic Therapy.Chest. 2004;126(suppl 3):401S–428S.
. Chang J, Elam-Evans LD, Berg CJ, et al. Pregnancy-related mortalitysurveillance—United States, 1991–1999. MMWR Surveill Summ. 2003;
52:1–8.
Newer Modalities for Detection of Pulmonary EmboliSeth Clemens, MD, and Kenneth V. Leeper, Jr., MDDivision of Pulmonary, Allergy and Critical Care, Emory University, Atlanta, Georgia, USA
ABSTRACT
Pulmonary embolism (PE) is the third most common cardiovascular disease after myocardial infarction andstroke in the United States. Early and accurate diagnosis of this condition is imperative because manypatients die within hours of presentation. Clinical and laboratory tests can be used to accurately determinethe pretest probability of PE. When necessary, imaging techniques are then used to exclude or diagnose PE.Pulmonary angiography is the reference standard for the diagnosis of PE, but it is invasive and has a highmorbidity and mortality rate. Ventilation and perfusion (V/Q) scanning in the past has been recommendedas the initial diagnostic test for PE; however, this technique also has limitations. Recently, new modalitiesfor the diagnosis and exclusion of PE have been evaluated. These techniques include V/Q single photonemission computed tomography (SPECT), single- and multi-detected computed tomography, and magneticresonance angiography (MRA) including gadolinium-enhanced MRA, real-time magnetic resonance im-aging (RT-MR), and magnetic resonance perfusion imaging. © 2007 Elsevier Inc. All rights reserved.
KEYWORDS: Computed tomography; Diagnosis; Magnetic resonance angiography; Pulmonary embolism; Radio-nuclide imaging
Pulmonary embolism (PE) is the third most common car-diovascular disease in the United States.1 In 1999, 140,000individuals were discharged from the hospital with an acutePE diagnosis.2 Mortality rates range from 3.5% to 15% andcan be as high as 31% to 58% when shock is present.3,4
Early and accurate diagnosis of this condition is imperativebecause PE is unsuspected in 70% of patients who die of thedisease. Approximately 65% of patients will die within 1hour of presentation of PE and 92.9% expire within the first2.5 hours.5
Pulmonary angiography is the reference standard for thediagnosis and exclusion of PE. However, it is invasive(Table 1) and morbidity and mortality rates range from3.5% to 6% and 0.2% to 0.5%, respectively.6,7 In addition,data from a subanalysis of the landmark Prospective Inves-tigation of Pulmonary Embolism Diagnosis (PIOPED)study suggest only moderate reader agreement for identify-ing PE in smaller, subsegmental arteries.8 Because newer
tests with improved safety have been developed, pulmonaryangiography is rarely used as a first-line test for the diag-nosis or exclusion of PE.
Ventilation and perfusion (V/Q) scanning in the pastwas the recommended initial diagnostic test for the eval-uation for PE in guidelines last updated in 1999 by theAmerican Thoracic Society (ATS).9 The major benefit ofthe V/Q scan is its safety. It is not invasive and radiationexposure is �2.5 mSv.10 This is 3.76 to 11.2 times lowerthan the radiation exposure from a computed tomography(CT) scan of the chest.11 V/Q scanning is also the onlyimaging modality that does not pose a threat of end-organtoxicity. Because of its safety profile, it is still the rec-ommended study for pregnant or nursing women withsuspected PE.12
Many of the guidelines for the performance and inter-pretation of V/Q scans were established in the initialPIOPED study.13 A planar scanning technique with Xenongas for the ventilation component was used to collect 2-di-mensional (2D) images. Scans were classified into normal,high, intermediate, low, or very low probability categoriesaccording to predefined criteria. Clinical pretest probabilitywas also determined.
Please see the Author Disclosures section at the end of this article.Requests for reprints should be addressed to Kenneth V. Leeper, MD,
Crawford Long Hospital, 550 Peachtree Street NE, MOT, 6th Floor,Atlanta, Georgia 30365.
E-mail address: [email protected].
0002-9343/$ -see front matter © 2007 Elsevier Inc. All rights reserved.doi:10.1016/j.amjmed.2007.07.014
The American Journal of Medicine (2007) Vol 120 (10B), S2–S12

In patients without prior history of PE, a high-probabilityscan had a positive predictive value (PPV) of 88%. PPVimproved to 96% when combined with a high clinical prob-ability, effectively diagnosing PE. The negative predictivevalue (NPV) of a normal scan was 96%, high enough to ruleout PE regardless of clinical probability. Normal scans wereuncommon in this study, occurring in only 14% of patients.The NPV of a low-probability scan was 88% and improvedto 96% when combined with a low clinical probability.Thus, a low-probability scan with a low clinical probabilityscore rules out PE as definitively as a normal scan. Finally,39% of the patients had intermediate scans and 32% of thesepatients had angiographically proven PE.13 Although, asshown by the PIOPED study, indeterminate readings arecommon, the incidence of an indeterminate reading may beas low as 9% if patients present with a normal chest x-ray.14
The major limitation of the V/Q scan is that a clot is notdirectly visualized; its presence is assumed when a mis-matched defect is observed. Although a clot is the mostlikely cause of a mismatch, there are other extravascularcauses. These can often be detected with a recent chestx-ray. Also, in theory, a clot must be occlusive or a mis-match will not be visualized. Additional limitations of V/Q
scanning are that it captures only 2D images and the radio-labeled isotope used for the ventilation portion of the test isnot standardized.
Although there has been much debate on risk stratifica-tion and treatment, less attention has been given to thesignificant advances in the quick and accurate exclusion ordiagnosis of PE. Recently, new modalities for the diagnosisand exclusion of PE, particularly CT pulmonary angiogra-phy with or without additional imaging of the lower extrem-ities, have been evaluated. This technology has rapidlyexpanded from single-detector CT to multidetector ma-chines and technologies. The CT scan has some limitationsand is not available for all patients with suspected PE. Forthis reason, other modalities, such as pulmonary magneticresonance angiography (MRA), are being studied. This ar-ticle will review these new modalities and their benefits andlimitations in clinical practice.
PRETEST PROBABILITYThe concept of pretest probability is important because mostof the diagnostic modalities discussed in this article havetheir sensitivities, specificities, and predictive values ad-
Table 1 Imaging methods
Method Technology
Pulmonaryangiography
A catheter is advanced into the pulmonary arterial tree with serial injection of contrast into the main, right,and left pulmonary arterial vessels; when PE is present, distinct filling defects can be identified
V/Q Imaging is performed with a �-camera using technetium or xenon gas as the radioisotope to evaluateventilation and technetium-labeled albumin to evaluate perfusion; PE is diagnosed when an area of thelung is identified that is ventilated but has no perfusion, the so-called “mismatched defect”
V/Q SPECT 1–3 �-cameras are rotated around the patient with image acquisition every 3–6 degrees; a computer canperform a tomographic reconstruction to create a 3D image from the individual 2D images, which areinitially cross-sectional, but can be manipulated to display different axes of the body
CT An x-ray detector is rotated around the patient, producing a 2D axial image of the scanned area; the patientis moved past this detector on a moving bed, with the detector collecting images at set distances;multiple 2D images are formatted into a 3D image
Single-detector CT A single detector and x-ray source rotate around the patient, allowing multiple cross-sectional images to beobtained as the patient moves through the scanner
Multidetector CT Multiple (4–64), staggered detectors are rotated around the patient as they move through the scannerMRA The spin of the atomic nucleus of hydrogen is manipulated by electromagnetic pulses that systematically
excite the hydrogen protons; the relaxation time back to the steady state generated by the magnetic fieldis used to create a contrast between water and lipids
Gd-enhanced MRA Contrast is used to better visualize the pulmonary vasculature; the data collected are used to create a 3Dimage of the pulmonary vasculature; a 20- to 30-sec breath hold is required
RT-MR Technology is similar to that used for electrocardiographically gated CT scanners to acquire images ofmoving organs; RT-MR sequences produce T2-weighted images and the need for contrast is eliminated;when evaluating PE, RT-MR is timed to take images gated to a patient’s respiratory cycle, eliminating theneed for a breath hold
MR perfusionimaging
Contrast agents (frequently Gd) are used to cause local disturbances in a magnetic field that can bemeasured by an MR scanner; a signal is generated based on the volume of blood in a region rather thandirectly imaging vascular structures; areas of decreased or absent blood flow suggest the presence ofobstruction and act as indirect evidence of PE; can be performed immediately after Gd-MR, a breath holdis not required
CT � computed tomography; 2D � two dimensional; 3D � three dimensional; Gd � gadolinium; MRA � magnetic resonance angiography; PE �pulmonary embolism; RT-MR � real-time magnetic resonance imaging; SPECT � single photon emission CT; V/Q � ventilation perfusion.
Adapted with permission from Ann Intern Med.20
S3Clemens and Leeper Newer Modalities for Detection of Pulmonary Emboli

justed based on the probability of PE before testing. Thepretest probability for PE can be most useful when deter-mined using both clinical and laboratory methods.13,15,16
Two methods, the Wells score and the Geneva score,were devised and validated to generate a clinical pretestprobability in patients with suspected PE.17,18 Both methodsdivide patients into low, intermediate, and high PE proba-bility groups. Both methods have similar accuracy, butneither is accurate enough to reliably diagnose or excludePE on its own.19
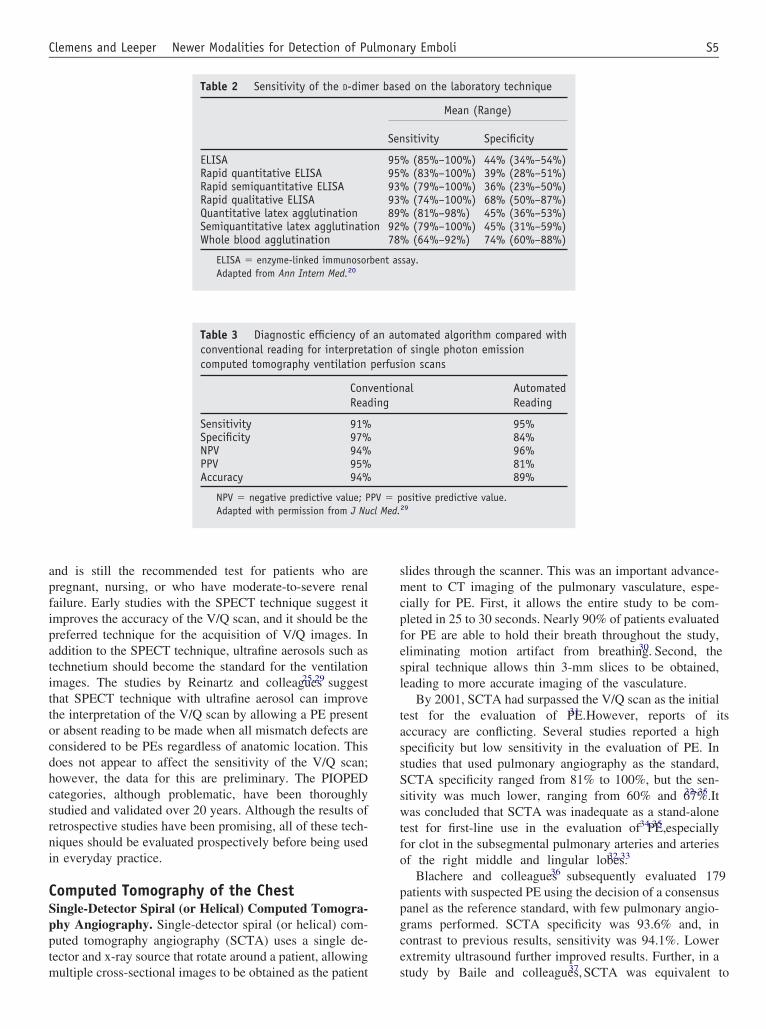
D-dimer testing is another method that has been used toevaluate patients with suspected PE. PE results in elevatedlevels of D-dimer, a fibrin degradation product. The D-dimeris elevated with increased clot lysis and suggests the pres-ence of thrombosis. D-dimer levels are often elevated inother conditions such as infection, active inflammatory dis-orders, malignancy, pregnancy, and liver failure. Therefore,the D-dimer assay has a very low specificity for PE, rangingfrom 38% to 83% depending on the assay used, and cannotrule in PE as a diagnosis.20 The D-dimer assay has excellentsensitivity; a normal D-dimer level can rule out PE withoutfurther work-up.
Many methods are available to measure D-dimer levelsand they are not all of equivalent utility (Table 2).20 Themajor methods include the enzyme-linked immunosorbentassay (ELISA); rapid quantitative ELISA; rapid semiquan-titative ELISA; rapid qualitative ELISA; and the quantita-tive, semiquantitative, and whole-blood latex agglutinationmethods.20 To date, only the VIDAS D -dimer assay(bioMérieux, Inc., Marcy l’Etoile, France), a rapid quan-titative ELISA, has been shown to have a high enoughsensitivity (96.4%)21 to rule out PE in the absence of acalculation of clinical pretest probability.21,22
Several studies have evaluated the sensitivity of a nega-tive D-dimer result combined with a low or intermediateclinical probability score.15,16,23 These studies demonstratedthat a negative D-dimer by rapid quantitative ELISA can becombined with a clinical probability score to exclude PE asa diagnosis and can eliminate further work-up in 32% to44% of patients with suspected PE.15,16 Caution should betaken with other, less sensitive D-dimer laboratory methods,and this rule may not apply to the latex agglutination assays.
NEWER MODALITIES FOR RADIOGRAPHICIMAGING FOR PULMONARY EMBOLISM
V/Q Single Photon Emission ComputedTomographyV/Q single photon emission computed tomography(SPECT) may improve both the sensitivity and specificity ofthe V/Q scan. In a study in artificially embolized pigs, lungSPECT scanning improved the sensitivity of planar scan-ning from 64% to 91% and the specificity from 79% to87%.24 In a retrospective study, Reinartz and colleagues25
analyzed 83 patients who had undergone 4-slice spiral CT,V/Q planar, and V/Q SPECT. Using the diagnosis of a
consensus panel as the reference standard, the sensitivity,specificity, NPV, and PPV for the SPECT technique were97%, 91%, 98%, and 90%, respectively.
This study used a protocol that differed from that used inthe PIOPED study. In addition to the SPECT technique,technetium aerosol was used for the ventilation portion ofthe V/Q scan. Technetium is believed to be superior to otherisotopes that have been used in the past for the ventilationportion of the V/Q scan. Xenon, the initial radioisotope usedfor V/Q scanning in PIOPED, has a low (1% to 3%) effi-ciency of pulmonary deposition.26,27 Technetium is approx-imately 5 times smaller in diameter (90 nm) than xenon andhas nearly a 20% efficiency of pulmonary deposition. Fewdata exist on the extent to which this may improve theresults of V/Q scanning. A study by Trujillo and col-leagues28 did demonstrate that the use of technetium de-creased the false-negative rate by 9% and the number ofindeterminate scans by 18% compared with PIOPED.
V/Q scan interpretation also differed from that proposedby the PIOPED investigators. In the Reinartz group’s study,all mismatched defects, regardless of level, were consideredto be PEs. Scans were read as either “embolism confirmed”or “embolism disproved,” eliminating the indeterminate in-terpretation. Indeterminate readings greatly limit the utilityof traditional V/Q scans. An indeterminate result is nondi-agnostic and requires further testing. This reading is fairlycommon, occurring in 39% of cases,13 delaying the time todiagnosis, decreasing the convenience to the patient andphysician, and increasing the cost of the work-up. Althoughnormal and high probability readings can be helpful in thecorrect clinical setting, these interpretations are less fre-quent, occurring 14% and 13% of the time, respectively.13
Improving the interpretation criteria is perhaps the singlemost important improvement that can be made to V/Qscanning. Eliminating or minimizing the indeterminatereading without sacrificing sensitivity and specificity wouldmake it a much more attractive test.
Finally, the SPECT technique also has the potential toimprove interpretation of the V/Q scan by incorporatingcomputerized interpretations. In a retrospective study of 53patients by Reinartz and colleagues,29 traditional reader andautomated computer algorithm interpretations were com-pared with the decision of a consensus panel as to whetherPE was present or absent (Table 3). As in their previousstudy, scans were read as either positive or negative for PE.
The computer algorithm resulted in the generation ofartifact in the area of the pulmonary recesses that resulted in5 false-positive results; however, when the automated andconventional methods were combined, there was only 1false-positive finding and the sensitivity and specificitywere 95% and 97%, respectively. Furthermore, the auto-mated technique correctly evaluated 12 patients who hadhighly heterogeneous scans because of restrictive or ob-structive disease.29
In sum, a normal V/Q scan remains the most sensitivetest in the evaluation of PE, continues to be the safest test,
S4 The American Journal of Medicine, Vol 120 (10B), October 2007
and is still the recommended test for patients who arepregnant, nursing, or who have moderate-to-severe renalfailure. Early studies with the SPECT technique suggest itimproves the accuracy of the V/Q scan, and it should be thepreferred technique for the acquisition of V/Q images. Inaddition to the SPECT technique, ultrafine aerosols such astechnetium should become the standard for the ventilationimages. The studies by Reinartz and colleagues25,29 suggestthat SPECT technique with ultrafine aerosol can improvethe interpretation of the V/Q scan by allowing a PE presentor absent reading to be made when all mismatch defects areconsidered to be PEs regardless of anatomic location. Thisdoes not appear to affect the sensitivity of the V/Q scan;however, the data for this are preliminary. The PIOPEDcategories, although problematic, have been thoroughlystudied and validated over 20 years. Although the results ofretrospective studies have been promising, all of these tech-niques should be evaluated prospectively before being usedin everyday practice.
Computed Tomography of the ChestSingle-Detector Spiral (or Helical) Computed Tomogra-phy Angiography. Single-detector spiral (or helical) com-puted tomography angiography (SCTA) uses a single de-tector and x-ray source that rotate around a patient, allowingmultiple cross-sectional images to be obtained as the patient
slides through the scanner. This was an important advance-ment to CT imaging of the pulmonary vasculature, espe-cially for PE. First, it allows the entire study to be com-pleted in 25 to 30 seconds. Nearly 90% of patients evaluatedfor PE are able to hold their breath throughout the study,eliminating motion artifact from breathing.30 Second, thespiral technique allows thin 3-mm slices to be obtained,leading to more accurate imaging of the vasculature.
By 2001, SCTA had surpassed the V/Q scan as the initialtest for the evaluation of PE.31 However, reports of itsaccuracy are conflicting. Several studies reported a highspecificity but low sensitivity in the evaluation of PE. Instudies that used pulmonary angiography as the standard,SCTA specificity ranged from 81% to 100%, but the sen-sitivity was much lower, ranging from 60% and 67%.32-35 Itwas concluded that SCTA was inadequate as a stand-alonetest for first-line use in the evaluation of PE,34,35 especiallyfor clot in the subsegmental pulmonary arteries and arteriesof the right middle and lingular lobes.32,33
Blachere and colleagues36 subsequently evaluated 179patients with suspected PE using the decision of a consensuspanel as the reference standard, with few pulmonary angio-grams performed. SCTA specificity was 93.6% and, incontrast to previous results, sensitivity was 94.1%. Lowerextremity ultrasound further improved results. Further, in astudy by Baile and colleagues,37 SCTA was equivalent to
Table 2 Sensitivity of the D-dimer based on the laboratory technique
Mean (Range)
Sensitivity Specificity
ELISA 95% (85%–100%) 44% (34%–54%)Rapid quantitative ELISA 95% (83%–100%) 39% (28%–51%)Rapid semiquantitative ELISA 93% (79%–100%) 36% (23%–50%)Rapid qualitative ELISA 93% (74%–100%) 68% (50%–87%)Quantitative latex agglutination 89% (81%–98%) 45% (36%–53%)Semiquantitative latex agglutination 92% (79%–100%) 45% (31%–59%)Whole blood agglutination 78% (64%–92%) 74% (60%–88%)
ELISA � enzyme-linked immunosorbent assay.Adapted from Ann Intern Med.20
Table 3 Diagnostic efficiency of an automated algorithm compared withconventional reading for interpretation of single photon emissioncomputed tomography ventilation perfusion scans
ConventionalReading
AutomatedReading
Sensitivity 91% 95%Specificity 97% 84%NPV 94% 96%PPV 95% 81%Accuracy 94% 89%
NPV � negative predictive value; PPV � positive predictive value.Adapted with permission from J Nucl Med.29
S5Clemens and Leeper Newer Modalities for Detection of Pulmonary Emboli
pulmonary angiography in a pig model with a methacrylatecast of the pulmonary vasculature as a standard. The sensi-tivity of pulmonary angiography was 87% and not statisti-cally different from that of single-detector CT scanning.
Several follow-up studies were performed to see whetherthe sensitivity of SCTA could be improved. A study byPerrier and colleagues38 found that SCTA combined withlower extremity ultrasonography (N � 299) had a sensitiv-ity of only 70%, despite the fact that ultrasonography im-proved the false-negative rate from 30% to 21%. In a similarstudy, when clinical probability was low or intermediateand SCTA and lower extremity ultrasonography were neg-ative, the incidence of venous thromboembolism (VTE) inthe absence of therapy was 1.8% at 3 months. Of concern,16% of patients with a negative SCTA had positive lowerextremity ultrasonography that resulted in treatment.39 Re-gardless, this study suggested that a negative SCTA withlower extremity ultrasound in the correct clinical settingwas sufficient for ruling out PE as a diagnosis.
Benefits and Limitations of SCTA. Despite its poor sensi-tivity, several factors make SCTA a desirable method forevaluating PE. SCTA does have high specificity, and apositive finding can be treated with confidence. Unlike theV/Q scan, SCTA directly identifies the presence of a clot,and false-positive results, such as extraluminal compres-sion, radiation effects, and others that may be reported withthe V/Q scan, are eliminated. In addition, SCTA allowsimaging of the lung parenchyma, chest wall, and mediasti-num, so that alternative diagnoses may be made when PE isabsent, eliminating the need for additional studies. Kim andcolleagues40 reported that 67% of patients in whom PE wasruled out by SCTA had a finding that suggested or con-firmed an alternative diagnosis such as pneumonia, pulmo-nary fibrosis, or trauma. Similar findings were reported in 2other studies in which SCTA identified an alternative diag-nosis in 31% and 21.2% of patients.16,33 Regardless of thediscrepancy in rates, these findings are important becauseneither the V/Q scan nor pulmonary angiography can reli-ably detect alternative conditions.
Contributing to the poor sensitivity of SCTA is its res-olution. Although it visualizes main, lobar, and segmentalarteries relatively well, it does not image the subsegmentalarteries well. Subsegmental PEs may account for 6% to 30%of all emboli.8,41 At best, SCTA detects 61% to 79% ofthese clots.32,42
CT scanning is a significant source of radiation exposurein the hospital setting. Although CT scans account for only4% of all radiologic examinations performed, they accountfor 40% to 75% of medical radiation exposure.43,44 Themeasured effective dose from CT scans has been estimatedat 7.5 mSv, and doses of 50 to 200 mSv begin to increasethe risk for cancer.45 This is especially true in patients whoreceive serial studies and in women who receive radiation tothe breast. Exposure of women aged �35 years to radiationfrom CT scanners may increase the risk for breast cancer by102%.11,45
Radiation exposure is also a concern in pregnancy. Stud-ies using Monte Carlo models have suggested that helicalCT scans can be used in pregnancy,12 but current guidelinesstill recommend V/Q scanning for the evaluation of PE.Although shielding with bismuth can be performed, it mayreduce the average dose to the female breast by only 57%.46
Reaction to the contrast used to perform the SCTA canalso limit its utility. Mild reactions to contrast media in-cluding flushing, nausea, vomiting, and pruritus occur in upto 15% of patients.47 Severe and very severe reactionsincluding convulsions, laryngeal edema, bronchospasm, andcardiovascular collapse occur much less frequently (0.22%and 0.04% of patients, respectively). The use of low-osmo-lality contrast media decreases the incidence of all of thesereactions.47 Contrast-induced nephropathy (CIN), a long-recognized complication from iodinated contrast exposure,is another limitation of CT scanning. It is the third mostcommon cause of acute renal failure in the hospital setting,and it is associated with increased inhospital mortality,1-year mortality, and increased length of hospital stay. Al-though generally self-resolving, CIN can result in the needfor dialysis.48
Finally, in a recent study of CT angiography of the chest,as many as 25% of patients had a contraindication for thetest. Preexisting renal failure and pregnancy were the pri-mary conditions that prevented this mode from being usedas the primary test for the evaluation of PE.49
Multidetector Spiral Computed Tomography: Improv-ing on an Improvement. Multidetector spiral computedtomography (MDCT) technology quickly followed SCTA,improving on the same concept. With MDCT, multipledetectors are staggered and rotated around the patient asthey slide through the CT scanner. Initially, 4 detectors wereused for MDCT, but this quickly progressed to 6-, 8-, 10-,16-, 32-, and 64-detector technology. The use of moredetectors shortens the time of the study to �10 seconds andallows for cuts as thin as 0.5 mm to be obtained. Thisgreatly improves the resolution of the study, allowing forimaging out to sixth-order pulmonary arteries.42 Conse-quently, MDCT improves the detection of segmental andsubsegmental PEs,50,51 decreasing false-negative results andimproving sensitivity.
Thinner slices have also allowed for computed recon-struction of the axial images into 3D models, which, al-though not yet demonstrated, may decrease the amount ofartifact and number of false-positive findings.52 Thin slicesalso allow CT images to be reconstructed retrospectivelyusing electrocardiographic reconstruction based on their re-lation to the R-R interval. This eliminates cardiac artifact,allowing better visualization of the coronary arteries andthoracic aorta.53,54
Several important articles published in recent years haveevaluated MDCT for the evaluation of PE. The primaryobjective of PIOPED II, published in 2006, was to deter-mine the accuracy of MDCT for the diagnosis and exclusionof PE in patients with suspected PE.49 PIOPED II enrolled
S6 The American Journal of Medicine, Vol 120 (10B), October 2007

824 patients with a component of a composite referencestandard (Table 4) that was either positive or negative forPE. Patients underwent MDCT of the chest followed by CTvenography (CTV) of the lower extremities. The majority ofMDCT studies were performed with 4-row detector scan-ners, but 8- and 16-row detector scanners were also used.Results were compared with a composite reference standard(Table 4).
The sensitivity and specificity of MDCT of the chestalone were 83% and 96%, respectively.49 Sensitivity andspecificity were 90% and 95%, respectively, with MDCT/CTV. These results suggest that MDCT has sufficient spec-ificity to diagnose PE without further testing, but, due to afalse-negative rate of 17%, it does not appear to be adequateas a stand-alone test to rule out PE as a diagnosis. However,MDCT/CTV may adequately rule out PE in most patients.When the clinical assessment does not agree with theMDCT/CTV findings, additional tests are necessary.
This study was important for its evaluation of MDCT inthe diagnosis and exclusion of PE, but was also important inthat it studied a set of tests, the composite reference standard(Table 4), that could be used in lieu of MDCT or pulmonaryangiography to diagnose or exclude PE. Because pulmonaryangiography is particularly poor at identifying PEs at thesubsegmental artery level8 and MDCT has an improvedability to visualize PEs at this level,50,55 MDCT could bepositive when pulmonary angiography is negative. To ad-dress this problem, the PIOPED investigators created acomposite standard that, when satisfied, could diagnose orexclude PE (Table 4). The study was not designed to cal-culate the specificity of the composite reference standard;however, of 590 patients with a composite reference stan-dard negative for PE, only 2 (�1%) had a follow-up eventin the next 6 months. This suggests that the compositestandard is a powerful set of tests that can be used toreliably exclude PE without pulmonary angiography orCT scanning.
Two studies have validated the use of MDCT. Perrierand colleagues56 evaluated patients with an abnormal D-dimer test or a high clinical probability for PE by theGeneva score. The majority of patients (89%) underwent4-detector MDCT; 11% underwent 16-detector MDCT. All
patients who underwent CT scanning also received lowerextremity ultrasonography. The CT scan was negative andanticoagulation was withheld in 292 patients. Three of thesepatients went on to have a thromboembolic event in the next3 months. The incidence of a thromboembolic event in thesepatients at 3 months was 1.7%. The authors concluded thatMDCT of the chest in patients with an elevated D-dimer orhigh clinical probability for PE by the Geneva score couldreliably evaluate patients for PE. Ultrasonography did notsignificantly improve the algorithm.
The second validation study evaluated inpatients andoutpatients with either an abnormal D-dimer or a PE-likelyclinical probability by the modified Wells score.16 Patientsunderwent CT scanning of the chest, with MDCT performedin 88% of patients. A total of 1,436 patients had negativeCT scans and were not treated. The incidence of a VTEevent in these patients at 3 months was 1.3%. An alternativediagnosis was found in 21.5% of patients with a scan thatwas negative for PE. Interestingly, the incidence of PE inthis population (20%) was comparable or even low com-pared with previous studies, suggesting that MDCT doesnot result in additional false-positive results or in the detec-tion of smaller, potentially clinically irrelevant PEs. Theseresults suggest that MDCT in patients with suspected PE,abnormal D-dimer, or high clinical probability is adequatefor the evaluation of PE without further diagnostic testing.
Limitations of MDCT. One concern with MDCT is that itdetects PE at the subsegmental level. PEs isolated to thesubsegmental level were found in 7% of the patients in thestudy by Perrier and colleagues,56 and smaller studies havereported detection of isolated subsegmental PEs withMDCT in as many as 36% of patients.32,41 The significanceof subsegmental PEs, especially those in arteries out to thefifth and sixth generation, is unknown, as is the importanceof treating them. Subsegmental PEs may not be acutelydangerous to the patient,3 but may predict the potential fora future, more severe embolism.57 It may also identifypatients at risk for the development of pulmonary hyperten-sion.58,59 Regardless of importance, MDCT does not seemto increase the diagnosis of PE even at the subsegmentallevel. If the use of MDCT did lead to an increased diagnosis
Table 4 Diagnostic reference standard for the Prospective Investigation of Pulmonary Embolism Disorders (PIOPED) II
PE Diagnosed PE Excluded
● High probability V/Q scan in a patient without priorhistory of PE
● Normal findings on digital subtraction pulmonary angiography
● Abnormal findings on pulmonary digital subtractionangiography
● Normal findings on the V/Q scan
● Abnormal findings on venous ultrasonography in a patientwith no prior history of DVT at that site and anondiagnostic V/Q scan (not normal and not highprobability)
● Low or very low probability V/Q scan in a subject with aclinical Wells score �2 and negative lower extremityultrasonography
DVT � deep vein thrombosis; PE � pulmonary embolism; V/Q � ventilation perfusion.Adapted from N Engl J Med.49
S7Clemens and Leeper Newer Modalities for Detection of Pulmonary Emboli

of isolated subsegmental clots, the incidence of PE inMDCT studies should be higher than those performed withother methods. In the original PIOPED study, the incidenceof PE was 33% with pulmonary angiography13 comparedwith 23.3%,49 26%,56 and 20.4%16 with MDCT in thePIOPED II, Perrier, and Christopher Studies, respectively. Itshould be noted that these studies used mostly 4-detectorscanners and more detectors should increase the detection ofsubsegmental PE and may affect the incidence of PE infuture studies.
As with SCTA, MDCT exposes patients to radiationexposure and the risk of CIN. It is worth noting that radi-ation exposure is significantly greater with MDCT. A 4-rowMDCT may increase radiation exposure by 30% to 100%when compared with SCTA. Additional detectors do notincrease exposure, mostly because they enable the scans tobe completed in a shorter time with more efficient use ofradiation.42 Finally, about 25% of patients with a suspicionof PE will have a contraindication for MDCT scanning,such as pregnancy or renal insufficiency that will requirealternative tests.
In sum, single- or multidetector CT scanning has anexcellent specificity for the diagnosis of PE, and patientswith a positive study should be treated with confidence.Overall, these studies demonstrate that, due to its low sen-sitivity, the utility of SCTA as the sole, initial test for theevaluation of PE is in question and further study is war-ranted. SCTA does not appear to have adequate sensitivityto exclude PE as a diagnosis, but imaging of the lowerextremities with either ultrasonography or CTV can im-prove its ability to exclude PE.
The advantages of MDCT over SCTA include decreasedtime to complete the study, and a negative 4-detector CTscan can be used to rule out PE as a diagnosis with a3-month risk for a subsequent VTE of only 1.3% to1.7%.16,56 CTV of the lower extremity would further de-crease this risk.49 At the same time, use of 4-detectorMDCT scans does not appear to increase the incidence ofPE and does not result in increased use of anticoagulationtherapy. However, in the near future, 4-detector MDCTs arelikely to be replaced by 16-, 32-, and 64-detector scannersthat will detect smaller PEs of unknown significance. Theresults of many of the studies that have been discussedlikely cannot be generalized to these new scanners. Thesesmaller PEs may not be acutely dangerous to the patient, butthey may predict the potential for a future, more severeembolism or for the development of pulmonary hyperten-sion from chronic thromboembolic disease. These patientswill likely need to be treated differently than a patient witha single acute PE.
Finally, although MDCT scanners are an excellent first-line test for the evaluation of PE, they are not without riskto the patient, and the number of CT scans should belimited. At the least, MDCT scanning should be reserved forpatients with either a high clinical Geneva score, PE-likely
modified Wells score, or those with an abnormal D-dimertest regardless of clinical probability.
Magnetic resonance angiographyRecent advances in magnetic resonance imaging (MRI)technology have made imaging of the chest, and particularlythe vascular structures, feasible. Specifically, the develop-ment of parallel imaging has greatly decreased the amountof time necessary to complete a study, allowing images tobe acquired during a short breath hold of 20 seconds.60 MRIis attractive for 2 reasons. First, it does not use ionizingradiation to generate images, and it is thought to be com-pletely harmless to a patient. Although not well established,it is felt to be safe for use during pregnancy. Second, thecontrast agent used is thought to be much less nephrotoxic.There are even some MRI techniques that can image thepulmonary vasculature without the use of contrast. Data onthe accuracy of these techniques is still limited but growing,and MRI with MRA of the pulmonary vasculature is makingits way into clinical practice.
The 3 most commonly used MRI techniques are gado-linium-enhanced MRA (Gd-MRA), real-time MRI (RT-MR), and magnetic resonance (MR) perfusion. The accu-racy for the evaluation of PE differs with the differenttechniques.
Gd-MRA. Gd-MRA is perhaps the most common MRAmethod currently used to evaluate a patient for PE. In thelargest study of Gd-MRA, conducted by Oudkerk and col-leagues,61 118 patients underwent Gd-MRA followed bypulmonary angiography, and 2 independent readers inter-preted the Gd-MRAs. Gd-MRA sensitivity was 77% andspecificity was 98%. Although Gd-MRA identified all em-boli in the central and lobar arteries, its sensitivity was only40% for isolated subsegmental emboli. Sensitivity im-proved to 72% when all subsegmental emboli were in-cluded. Similar results were reported in smaller studies62,63
and in a study that compared Gd-MRA with 16-row MDCTas the reference standard.64
The high specificity of Gd-MRA allows patients with apositive study to be treated for PE with confidence. How-ever, at this time, its sensitivity as a single test is not highenough to reliably exclude PE, particularly in the distal,subsegmental arteries. Larger, prospective studies areneeded before Gd-MRA gains routine use as the initial testfor the evaluation of PE. A study by the PIOPED investi-gators is currently underway that will compare Gd-MRAwith a composite reference standard in 710 patients.
RT-MR. RT-MR uses technology similar to that used forelectrocardiographically gated CT scanners to acquire im-ages of moving organs. When used for the evaluation of PE,RT-MR is timed to take images gated to a patient’s respi-ratory cycle. This modality has 2 advantages. First, it elim-inates the need for a breath hold. Second, RT-MR sequencesproduce T2-weighted images, which allow for imaging ofthrombus without the need for contrast.65
S8 The American Journal of Medicine, Vol 120 (10B), October 2007

In a study by Haage and colleagues,66 pigs with artifi-cially induced PE were evaluated by pulmonary angiogra-phy (standard), CT scanning using 3-mm slices, Gd-MRA,and RT-MR. The sensitivities for CT, Gd-MRA, andRT-MR were 71.0%, 80.3%, and 97.7%, respectively.RT-MR detected all but 1 of the emboli detected by pul-monary angiography. There were no subsegmental emboliin this study because the size of the artificial emboli wasgreater than the diameter of the subsegmental arteries.Based on these results, RT-MR for the evaluation of PE wasstudied in humans.
There are few published studies comparing RT-MR withother modalities. In a study by Kluge and colleagues,64 62patients with signs and symptoms of PE underwent 16-rowMDCT (standard), Gd-MRA, RT-MR, and MR perfusionimaging. The incidence of PE was 31% and the sensitivityand specificity of RT-MR were 85% and 98%, respectively.The sensitivity of RT-MR was superior to that of Gd-MRA(77%), and the specificities were essentially the same. Al-though RT-MR showed continued excellent specificity, itssensitivity was not nearly what might be expected based onthe preclinical study and does not appear to be high enoughto allow its use as a stand-alone test for the evaluation of PE.
Aside from a possible increased sensitivity, RT-MR pro-vides additional benefits over Gd-MRA. In a second study,Kluge and colleagues65 went on to compare RT-MR withGd-MRA for the evaluation of PE. There was no truereference standard for this study, and sensitivity and spec-ificity calculations should be viewed with caution and arenot discussed. The secondary objective of this study was todetermine which test was better tolerated by patients andless prone to artifact. Patients were staged based on theirlevel of dyspnea from asymptomatic to severe with de-creased blood pressure. Studies were defined as nondiag-nostic if �3 lobar arteries or �50% of the segmental arter-ies could not be visualized or could not be evaluated for PEsecondary to blurring of the vasculature. There were nonondiagnostic studies using RT-MR regardless of dyspneastage, whereas 36% of Gd-MRA studies in patients withdyspnea and agitation were nondiagnostic, as were 5 of 5Gd-MRA studies in patients with severe dyspnea and de-creased blood pressure. The nondiagnostic studies wereattributed to motion or breathing artifact. The results ofthese studies suggest that RT-MR has increased sensitivitycompared with Gd-MRA and produces fewer nondiagnosticstudies.
MR Perfusion. MR perfusion images use contrast agentsthat cause local disturbances in a magnetic field that can bemeasured by an MR scanner. Gadolinium is frequently thecontrast agent used, and perfusion studies can be performedimmediately after Gd-MRA. The patient does need to per-form a breath hold for an optimal study. Perfusion imagesdo not directly image vascular structures, but rather generatea signal based on the volume of blood in a region. MRperfusion studies act in a similar fashion as nuclear medi-cine perfusion studies, in that areas where blood flow is
decreased or absent suggest areas where blood flow is ob-structed. This acts as indirect evidence of PE. Althoughclinical studies of MR perfusion are limited, it is hoped thatMR perfusion will perform better with respect to identifyingperipheral thrombus in the subsegmental arteries than Gd-MRA and RT-MR.
Kluge and colleagues67 evaluated the agreement of MRperfusion with SPECT perfusion in 41 patients with sus-pected PE. MR perfusion identified 14 of 15 patients withPE by SPECT. The �-scores for agreement between themethods were 0.98, 0.83, and 0.69, at the lobar, segmental,and subsegmental levels, respectively. In a second studythat compared MR perfusion with 16-row MDCT in 62patients with suspected PE, the sensitivity and specificityfor MR perfusion were 100% and 91%, respectively.64
Contrast-enhanced perfusion studies frequently are per-formed in conjunction with Gd-MRA. Kluge and col-leagues64 evaluated this method in a study using 16-rowMDCT as the reference standard. The protocol called forinitial RT-MR followed by Gd-MRA and, finally, perfusionMR. The combined protocol results were defined as theconsensus interpretation between 2 blinded radiologists af-ter all 3 tests were reviewed. This combined protocol had asensitivity and specificity of 100% and 93%, respectively.The average time for a patient to complete all 3 studies was9 minutes and 56 seconds.
Advantages and Limitations with MRI. To date, MRI is notthought to be harmful. Although not thoroughly studied inpregnant women, it is thought to be safe in this populationas well. It is finding increasing utility for the diagnosis ofconditions in both the woman and the fetus that are notcompletely identified by ultrasound.68 In addition, there isno known end-organ toxicity from exposure to MRI.
The major concern with MRI for the evaluation of PE isits lack of sensitivity. Although there are few studies of thistechnique to date, there is already a trend toward a repro-ducible sensitivity in the range of 75% to 93%. In the future,combining MRI with imaging of the lower extremities mayprove to be adequate to rule out PE.
There are contraindications for MRI, the most importantof which is the presence of an electronic implanted device.Fatal arrhythmias have been attributed to cardiac pacemakermalfunctions during an MRI, and pacemakers are consid-ered an absolute contraindication. Nerve stimulators, con-tinuous medicine pumps (e.g., epoprostanol), cardiac defi-brillators, insulin pumps, cochlear implants, and someprosthetic devices should be considered contraindications asshould residual metallic fragments (shrapnel, bullets),which may move during the course of an MRI.69 Althoughrare, burns in patients with tattoos have been reported.69
Gadolinium-based contrast agents are thought to be lesstoxic than ionic contrast agents used for fluoroscopy and CTscanning. The incidence of adverse events associated withgadolinium contrast is 1.47%.70 At least 69% of these re-actions are mild in nature. Severe reactions, such as ana-phylaxis, occur in 0.0003% of patients. Gadolinium, a preg-
S9Clemens and Leeper Newer Modalities for Detection of Pulmonary Emboli

nancy class C drug, quickly crosses the placenta, is removedfrom the fetal bloodstream by the kidneys, released into theamniotic fluid, and is subsequently ingested by the fetus.68
The length of time that gadolinium contrast remains in thefetal circulation is unknown.
Although gadolinium was thought to be safe for use inpatients with renal failure at US Food and Drug Adminis-tration (FDA)–approved doses, gadolinium-containing agentsrecently have been implicated in the development of nephro-genic fibrosing dermopathy (NFD)/nephrogenic systemicfibrosis (NSF). NFD/NSF is a rare condition (only 215 caseshave been reported worldwide since 1997) that occurs ex-clusively in patients with chronic renal insufficiency, tendsto be progressive, and may be fatal.71
RT-MR and other techniques for direct thrombus visu-alization do not use contrast but report results similar tocontrast-enhanced studies. Therefore, it becomes importantto determine the additional benefit that occurs from theaddition of contrast with respect to the risk to the patient forthis condition.
In sum, MRI and MRA of the pulmonary vasculature isa rapidly developing technology for evaluating PE. Theaccuracy of MR for evaluating PE is dependent on thetechnique used. When these techniques are used as stand-alone tests, they have a high specificity for diagnosing PE,but sensitivity is not high enough to reliably exclude PEwithout additional testing. However, when combined toevaluate PE, these techniques have a sensitivity and speci-ficity that rivals 4-row MDCT.
Although encouraging, the data for MRI are insufficientto suggest this as a first-line study for the evaluation of PE.Although more attractive than V/Q scanning because thereis direct visualization of thrombus and no risk of an inde-terminate reading, it should probably be ranked below thismodality as well. Although not ideal, the reproducible de-pendability of readings such as normal, low-probability, andhigh-probability V/Q scans will allow the physician to maketreatment decisions with more confidence than with MRI.Additional large, prospective studies such as PIOPED IIImay provide data to better support MRI in the future.
Although MRI is very safe, the addition of gadoliniumcontrast adds additional risk to the study. Currently, RT-MRcan be performed without contrast. There are also MRperfusion techniques that eliminate the need for contrast aswell. Until these techniques are better studied, it is unlikelythat they will replace V/Q scanning as the test of choice forpregnant patients or patients with end-stage renal disease.
SUMMARYIn the past 10 years, a wealth of data have emerged con-cerning the best way to diagnose or exclude PE. The optimalmethod must be sensitive (important because untreated PEis often fatal) and specific (important to avoid unnecessaryanticoagulation). In addition, the number of tests required toachieve an adequate sensitivity and specificity must be min-imized for patient safety and improved cost-effectiveness.
Current evidence supports the use of an algorithm thatincorporates clinical probability, D-dimer testing, and MDCTscanning for first-line evaluation of suspected PE. When clin-ical probability is low or intermediate by the Geneva score orPE-unlikely by a modified Wells score, a D-dimer assay shouldbe obtained. If the D-dimer is negative, PE can be ruled out,preventing further testing in one third of patients with sus-pected PE. If the D-dimer is abnormal or the clinical probabilityis high, MDCT of the chest should be performed. The decisionto treat can be made based on the results of this study. Con-current CTV of the lower extremity may be performed tofurther improve the sensitivity of the study. No additionalcontrast is needed, and the additional time and risk to thepatient is negligible. This is a simple, efficient, and accuratestrategy for most patients; however, this algorithm will becontraindicated in one sixth to two thirds of patients, most ofwhom will be pregnant or have renal insufficiency.
In this population, D-dimer assay is still useful, and thispart of the algorithm should remain intact. V/Q scanning,ideally using SPECT technique, is probably the best test touse in these patients because of its well-documented safetyprofile. An indeterminate reading is still a possibility andwould likely require further work-up. If MRI is the chosenmodality, a combined study using RT-MR, Gd-MRA, andcontrast-enhanced MR perfusion seems to have an accuracythat is adequate for the evaluation of PE. However, this isbased on only 1 fairly small study; larger studies must beperformed.
Contrast studies should be avoided in patients who arepregnant or who have advanced renal failure and should beused with caution in those with moderate renal insuffi-ciency. RT-MR should be the preferred imaging techniquein this population so that gadolinium contrast can beavoided. In the absence of contrast, MRI is essentiallyharmless to a patient. In the few studies of this technique,the sensitivities and specificities have been shown to besimilar to those of SCTA. Intuitively, it stands that itsresults should be interpreted in a similar fashion. Specifi-cally, negative exams should not be satisfactory for rulingout PE, and additional testing, such as imaging of the lowerextremities, should be pursued to verify a negative finding.This may change as more data become available on MRI,but to date, there have been no clinical validation studiesthat determine treatment based on the result of MR tech-niques. Until that time, caution should be used when makingtreatment decisions based on their results.
AUTHOR DISCLOSURESThe authors who contributed to this article have disclosedthe following industry relationships: Seth Clements, MD,has received research/grant support from Kimberly-Clark;and honoraria from Kimberly-Clark. Kenneth V. Leeper,Jr., MD, has served as a member of the Speakers’ Bureaufor Ortho-McNeil and Pfizer Inc; has received research/grant support from Kimberly-Clark, Ortho-McNeil, and
S10 The American Journal of Medicine, Vol 120 (10B), October 2007

Pfizer Inc., and has received honoraria from Kimberly-Clark, Ortho-McNeil, and Pfizer Inc.
References1. Stein PD, Hull RD, Ghali WA, et al. Tracking the uptake of evidence:
two decades of hospital practice trends for diagnosing deep veinthrombosis and pulmonary embolism. Arch Intern Med. 2003;163:1213–1219.
2. Horlander KT, Mannino DM, Leeper KV. Pulmonary embolism mor-tality in the United States, 1979-1998: an analysis using multiple-causemortality data. Arch Intern Med. 2003;163:1711–1717.
3. Wood KE. The presence of shock defines the threshold to initiatethrombolytic therapy in patients with pulmonary embolism. IntensiveCare Med. 2002;28:1537–1546.
4. Konstantinides S, Geibel A, Olschewski M, et al. Association betweenthrombolytic treatment and the prognosis of hemodynamically stablepatients with major pulmonary embolism: results of a multicenterregistry. Circulation. 1997;96:882–888.
5. Stein PD, Henry JW. Prevalence of acute pulmonary embolism amongpatients in a general hospital and at autopsy. Chest. 1995;108:978–981.
6. Schoepf UJ, Goldhaber SZ, Costello P. Spiral computed tomographyfor acute pulmonary embolism. Circulation. 2004;109:2160–2167.
7. Stein PD, Athanasoulis C, Alavi A, et al. Complications and validityof pulmonary angiography in acute pulmonary embolism. Circulation.1992;85:462–468.
8. Stein PD, Henry JW, Gottschalk A. Reassessment of pulmonary an-giography for the diagnosis of pulmonary embolism: relation of inter-preter agreement to the order of the involved pulmonary arterialbranch. Radiology. 1999;210:689–691.
9. Tapson VF, Carroll BA, Davidson BL, et al, for the American Tho-racic Society. The diagnostic approach to acute venous thromboem-bolism [clinical practice guideline]. Am J Respir Crit Care Med.1999;160:1043–1066.
10. Valentin J. Radiation dose to patients from radiopharmaceuticals [ad-dendum 2 to ICRP publication 53]. Ann ICRP. 1998;28:1–126.
11. Schuemichen C. Pulmonary embolism: is multislice CT the method ofchoice? Against. Eur J Nucl Med Mol Imaging. 2005;32:107–112.
12. Winer-Muram HT, Boone JM, Brown HL, Jennings SG, Mabie WC,Lombardo GT. Pulmonary embolism in pregnant patients: fetal radi-ation dose with helical CT. Radiology. 2002;224:487–492.
13. The PIOPED Investigators. Value of the ventilation/perfusion scan inacute pulmonary embolism. Results of the prospective investigation ofpulmonary embolism diagnosis (PIOPED). JAMA. 1990;263:2753–2759.
14. Forbes KP, Reid JH, Murchison JT. Do preliminary chest X-rayfindings define the optimum role of pulmonary scintigraphy in sus-pected pulmonary embolism? Clin Radiol. 2001;56:397–400.
15. Ginsberg JS, Wells PS, Kearon C, et al. Sensitivity and specificity ofa rapid whole-blood assay for D-dimer in the diagnosis of pulmonaryembolism. Ann Intern Med. 1998;129:1006–1011.
16. van Belle A, Buller HR, Huisman MV, et al. Effectiveness of man-aging suspected pulmonary embolism using an algorithm combiningclinical probability, D-dimer testing, and computed tomography.JAMA. 2006;295:172–179.
17. Wicki J, Perneger TV, Junod AF, Bounameaux H, Perrier A. Assess-ing clinical probability of pulmonary embolism in the emergencyward: a simple score. Arch Intern Med. 2001;161:92–97.
18. Wells PS, Anderson DR, Rodger M, et al. Derivation of a simpleclinical model to categorize patients probability of pulmonary embo-lism: increasing the models utility with the SimpliRED D-dimer.Thromb Haemost. 2000;83:416–420.
19. Chagnon I, Bounameaux H, Aujesky D, et al. Comparison of twoclinical prediction rules and implicit assessment among patients withsuspected pulmonary embolism. Am J Med. 2002;113:269–275.
20. Stein PD, Hull RD, Patel KC, et al. D-dimer for the exclusion of acutevenous thrombosis and pulmonary embolism: a systematic review.Ann Intern Med. 2004;140:589–602.
21. Dunn KL, Wolf JP, Dorfman DM, Fitzpatrick P, Baker JL, GoldhaberSZ. Normal D-dimer levels in emergency department patients sus-pected of acute pulmonary embolism. J Am Coll Cardiol. 2002;40:1475–1478.
22. de Moerloose P, Desmarais S, Bounameaux H, et al. Contribution ofa new, rapid, individual and quantitative automated D-dimer ELISA toexclude pulmonary embolism. Thromb Haemost. 1996;75:11–13.
23. Wells PS, Anderson DR, Rodger M, et al. Excluding pulmonaryembolism at the bedside without diagnostic imaging: management ofpatients with suspected pulmonary embolism presenting to the emer-gency department by using a simple clinical model and D-dimer. AnnIntern Med. 2001;135:98–107.
24. Bajc M, Bitzen U, Olsson B, Perez de Sa V, Palmer J, Jonson B. Lungventilation/perfusion SPECT in the artificially embolized pig. J NuclMed. 2002;43:640–647.
25. Reinartz P, Wildberger JE, Schaefer W, Nowak B, Mahnken AH,Buell U. Tomographic imaging in the diagnosis of pulmonary embo-lism: a comparison between V/Q lung scintigraphy in SPECT tech-nique and multislice spiral CT. J Nucl Med. 2004;45:1501–1508.
26. Senden TJ, Moock KH, Gerald JF, et al. The physical and chemicalnature of technegas. J Nucl Med. 1997;38:1327–1333.
27. Hartmann IJ, Hagen PJ, Stokkel MP, Hoekstra OS, Prins MH. Tech-negas versus 81mKr ventilation-perfusion scintigraphy: a comparativestudy in patients with suspected acute pulmonary embolism. J NuclMed. 2001;42:393–400.
28. Trujillo NP, Pratt JP, Talusani S, Quaife RA, Kumpe D, Lear JL.DTPA aerosol in ventilation/perfusion scintigraphy for diagnosingpulmonary embolism. J Nucl Med. 1997;38:1781–1783.
29. Reinartz P, Kaiser HJ, Wildberger JE, Gordji C, Nowak B, Buell U.SPECT imaging in the diagnosis of pulmonary embolism: automateddetection of match and mismatch defects by means of image-process-ing techniques. J Nucl Med. 2006;47:968–973.
30. Herold CJ. Spiral computed tomography of pulmonary embolism. EurRespir J Suppl. 2002;35:13s–21s.
31. Stein PD, Kayali F, Olson RE. Trends in the use of diagnostic imagingin patients hospitalized with acute pulmonary embolism. Am J Cardiol.2004;93:1316–1317.
32. Goodman LR, Curtin JJ, Mewissen MW, et al. Detection of pulmonaryembolism in patients with unresolved clinical and scintigraphic diag-nosis: helical CT versus angiography. AJR Am J Roentgenol. 1995;164:1369–1374.
33. Garg K, Welsh CH, Feyerabend AJ, et al. Pulmonary embolism:diagnosis with spiral CT and ventilation-perfusion scanning–correla-tion with pulmonary angiographic results or clinical outcome. Radi-ology. 1998;208:201–208.
34. Drucker EA, Rivitz SM, Shepard JA, et al. Acute pulmonary embo-lism: assessment of helical CT for diagnosis. Radiology. 1998;209:235–241.
35. Jiménez D, Gómez M, Herrero R, et al. Thromboembolic events inpatients after a negative computed tomography pulmonary angiogram:a retrospective study of 165 patients [in Spanish]. Arch Bronconeumol.2006;42:344–348.
36. Blachere H, Latrabe V, Montaudon M, et al. Pulmonary embolismrevealed on helical CT angiography: comparison with ventilation-perfusion radionuclide lung scanning. AJR Am J Roentgenol. 2000;174:1041–1047.
37. Baile EM, King GG, Muller NL, et al. Spiral computed tomography iscomparable to angiography for the diagnosis of pulmonary embolism.Am J Respir Crit Care Med. 2000;161:1010–1015.
38. Perrier A, Howarth N, Didier D, et al. Performance of helical com-puted tomography in unselected outpatients with suspected pulmonaryembolism. Ann Intern Med. 2001;135:88–97.
39. Musset D, Parent F, Meyer G, et al. Diagnostic strategy for patientswith suspected pulmonary embolism: a prospective multicentre out-come study. Lancet. 2002;360:1914–1920.
40. Kim KI, Muller NL, Mayo JR. Clinically suspected pulmonary embo-lism: utility of spiral CT. Radiology. 1999;210:693–697.
S11Clemens and Leeper Newer Modalities for Detection of Pulmonary Emboli

41. Oser RF, Zuckerman DA, Gutierrez FR, Brink JA. Anatomic distri-bution of pulmonary emboli at pulmonary angiography: implicationsfor cross-sectional imaging. Radiology. 1996;199:31–35.
42. Schoepf UJ. Diagnosing pulmonary embolism: time to rewrite thetextbooks. Int J Cardiovasc Imaging. 2005;21:155–163.
43. Shrimpton PC, Edyvean S. CT scanner dosimetry. Br J Radiol. 1998;71:1–3.
44. Wiest PW, Locken JA, Heintz PH, Mettler FA, Jr.CT scanning: amajor source of radiation exposure. Semin Ultrasound CT MR. 2002;23:402–410.
45. Land CE, Tokunaga M, Tokuoka S, Nakamura N. Early-onset breastcancer in A-bomb survivors (Letter). Lancet. 1993;342:237.
46. Hopper KD, King SH, Lobell ME, TenHave TR, Weaver JS. The breast:in-plane x-ray protection during diagnostic thoracic CT—shielding withbismuth radioprotective garments. Radiology. 1997;205:853–858.
47. Thomsen HS, Morcos SK. Management of acute adverse reactions tocontrast media. Eur Radiol. 2004;14:476–481.
48. McCullough PA, Adam A, Becker CR, et al. Epidemiology and prog-nostic implications of contrast-induced nephropathy. Am J Cardiol.2006;98:5K–13K.
49. Stein PD, Fowler SE, Goodman LR, et al. Multidetector computedtomography for acute pulmonary embolism. N Engl J Med. 2006;354:2317–2327.
50. Schoepf UJ, Holzknecht N, Helmberger TK, et al. Subsegmentalpulmonary emboli: improved detection with thin-collimation multi-detector row spiral CT. Radiology. 2002;222:483–490.
51. Brunot S, Corneloup O, Latrabe V, Montaudon M, Laurent F. Repro-ducibility of multi-detector spiral computed tomography in detectionof sub-segmental acute pulmonary embolism. Eur Radiol. 2005;15:2057–2063.
52. Heuschmid M, Mann C, Luz O, et al. Detection of pulmonary embo-lism using 16-slice multidetector-row computed tomography: evalua-tion of different image reconstruction parameters. J Comput AssistTomogr. 2006;30:77–82.
53. Nieman K, Oudkerk M, Rensing BJ, et al. Coronary angiography withmulti-slice computed tomography. Lancet. 2001;357:599–603.
54. Hofmann LK, Zou KH, Costello P, Schoepf UJ. Electrocardiographi-cally gated 16-section CT of the thorax: cardiac motion suppression.Radiology. 2004;233:927–933.
55. Ghaye B, Szapiro D, Mastora I, et al. Peripheral pulmonary arteries:how far in the lung does multi-detector row spiral CT allow analysis?Radiology. 2001;219:629–636.
56. Perrier A, Roy PM, Sanchez O, et al. Multidetector-row computedtomography in suspected pulmonary embolism. N Engl J Med. 2005;352:1760–1768.
57. Morgenthaler TI, Ryu JH. Clinical characteristics of fatal pulmonaryembolism in a referral hospital. Mayo Clin Proc. 1995;70:417– 424.
58. Pengo V, Lensing AW, Prins MH, et al. Incidence of chronic throm-boembolic pulmonary hypertension after pulmonary embolism. N EnglJ Med. 2004;350:2257–2264.
59. Becattini C, Agnelli G, Pesavento R, et al. Incidence of chronicthromboembolic pulmonary hypertension after a first episode of pul-monary embolism. Chest. 2006;130:172–175.
60. Pedersen MR, Fisher MT, van Beek EJ. MR imaging of the pulmonaryvasculature—an update. Eur Radiol. 2006;16:1374–1386.
61. Oudkerk M, van Beek EJ, Wielopolski P, et al. Comparison of con-trast-enhanced magnetic resonance angiography and conventional pul-monary angiography for the diagnosis of pulmonary embolism: aprospective study. Lancet. 2002;359:1643–1647.
62. Meaney JF, Weg JG, Chenevert TL, Stafford-Johnson D, HamiltonBH, Prince MR. Diagnosis of pulmonary embolism with magneticresonance angiography. N Engl J Med. 1997;336:1422–1427.
63. Gupta A, Frazer CK, Ferguson JM, et al. Acute pulmonary embo-lism: diagnosis with MR angiography. Radiology. 1999;210:353–359.
64. Kluge A, Luboldt W, Bachmann G. Acute pulmonary embolism to thesubsegmental level: diagnostic accuracy of three MRI techniques com-pared with 16-MDCT. AJR Am J Roentgenol. 2006;187:W7–W14.
65. Kluge A, Muller C, Hansel J, Gerriets T, Bachmann G. Real-time MRwith TrueFISP for the detection of acute pulmonary embolism: initialclinical experience. Eur Radiol. 2004;14:709–718.
66. Haage P, Piroth W, Krombach G, et al. Pulmonary embolism: com-parison of angiography with spiral computed tomography, magneticresonance angiography, and real-time magnetic resonance imaging.Am J Respir Crit Care Med. 2003;167:729–734.
67. Kluge A, Gerriets T, Stolz E, et al. Pulmonary perfusion in acutepulmonary embolism: agreement of MRI and SPECT for lobar,segmental and subsegmental perfusion defects. Acta Radiol. 2006;47:933–940.
68. Levine D. Obstetric MRI. J Magn Reson Imaging. 2006;24:1–15.69. Kanal E, Borgstede JP, Barkovich AJ, et al, for the American College
of Radiology. ACR white paper of magnetic resonance (MR) safety:combined papers of 2002 and 2004 [ACR Practice Guidelines andClinical Standards]. Reston, VA: American College of Radiology,2004:1005–1030.
70. Niendorf HP, Haustein J, Cornelius I, Alhassan A, Clauss W. Safety ofgadolinium-DTPA: extended clinical experience. Magn Reson Med.1991;22:222–228; discussion 229–232.
71. US Food and Drug Administration, Center for Drug Evaluation andResearch. Gadolinium-based contrast agents for magnetic resonanceimaging scans [FDA Information for Healthcare Professionals.] Rock-ville, MD: US Food and Drug Administration, June 2006; updatedDecember 2006.
S12 The American Journal of Medicine, Vol 120 (10B), October 2007
Inferior Vena Cava Filters in the Management of VenousThromboembolismMark A. Crowther, MD, MScDivision of Hematology, McMaster University, Hamilton, Ontario, Canada
ABSTRACT
Inferior vena cava (IVC) filters, both retrievable and permanent, are indicated for the prevention ofpulmonary embolism (PE) in patients contraindicated for anticoagulant therapy, in those with anticoagulanttherapy complications, and perhaps for those with recurrent PE despite therapeutic anticoagulation.Because of the lack of randomized controlled trials (only 1 has been published), clinicians have littleevidence-based information to assist them in determining proper use of IVC filters. The introduction ofretrievable filters and the ease of insertion have stimulated increased use of these devices without strongevidence or follow-up to assess either efficacy or longer-term clinical outcomes. Current evidence-basedguidelines recommend IVC filter insertion only in patients with proven venous thromboembolism and anabsolute contraindication for anticoagulation. © 2007 Elsevier Inc. All rights reserved.
KEYWORDS: Deep vein thrombosis; Evidence based practice; Inferior vena caval filters; Pulmonary embolism;Recurrent thrombosis
Systemic anticoagulation is the therapy of choice for allforms of venous thromboembolism (VTE); however, anti-coagulant therapy is contraindicated in a small subgroup ofpatients. Without anticoagulation, patients with VTE are athigh risk for developing pulmonary embolism (PE), whichis fatal in as many as 25% of patients.1 Interruption of theinferior vena cava (IVC) with implantable filtering devicesshould be considered in patients with VTE in whom anti-coagulation is contraindicated.2 Filters are typically placedwithin the infrarenal IVC and function to capture embolithat would result in PE.3
Institution or resumption of anticoagulation is recom-mended as soon as possible in all patients in whom IVCfilters are placed2 because filters are not effective for deepvenous thrombosis (DVT) prevention and can, in fact, beassociated with recurrent DVT, presumably owing to in-creased outflow obstruction at the level of the filter.4
Both permanent and retrievable filters are approved in
the United States for the prevention of PE in individualswith acute DVT or PE. Despite their approval, there is astriking lack of rigorously performed clinical studies, andthere are known safety concerns that warrant careful con-sideration of the use of IVC filters.4–6 However, with theintroduction of retrievable filters, bedside insertion tech-niques, and ultrasound guidance, the use of IVC filters hasrapidly increased and expanded beyond the recommendedindications. The purpose of this article is to review therecommended and expanded indications for IVC filters inthe management of VTE and to discuss the lack of data tosupport expanded indications as well as the safety andefficacy concerns with their use.
INDICATIONS FOR INFERIOR VENA CAVAFILTERS
Recommended UseEvidence-based guidelines from the American College ofChest Physicians (ACCP) recommend IVC filter placementonly in those patients with proven VTE with a contraindi-cation for anticoagulation, a complication of anticoagula-tion treatment, or recurrent VTE despite adequate anticoag-
Please see the Conflict of Interest section at the end of this article.Requests for reprints should be addressed to Mark A. Crowther, MD,
MSc, St Joseph’s Hospital, Room L208, 50 Charlton Avenue East, Ham-ilton, Ontario L8N 4A6, Canada.
E-mail address: [email protected].
0002-9343/$ -see front matter © 2007 Elsevier Inc. All rights reserved.doi:10.1016/j.amjmed.2007.07.015
The American Journal of Medicine (2007) Vol 120 (10B), S13–S17
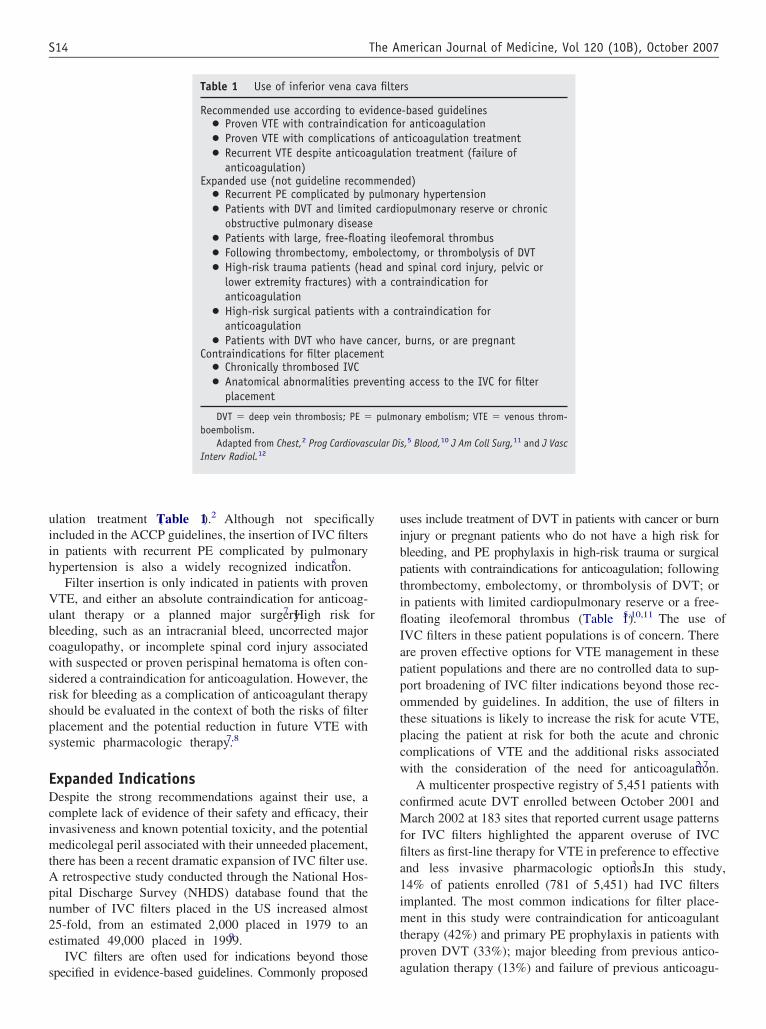
ulation treatment (Table 1).2 Although not specificallyincluded in the ACCP guidelines, the insertion of IVC filtersin patients with recurrent PE complicated by pulmonaryhypertension is also a widely recognized indication.5
Filter insertion is only indicated in patients with provenVTE, and either an absolute contraindication for anticoag-ulant therapy or a planned major surgery.7 High risk forbleeding, such as an intracranial bleed, uncorrected majorcoagulopathy, or incomplete spinal cord injury associatedwith suspected or proven perispinal hematoma is often con-sidered a contraindication for anticoagulation. However, therisk for bleeding as a complication of anticoagulant therapyshould be evaluated in the context of both the risks of filterplacement and the potential reduction in future VTE withsystemic pharmacologic therapy.7,8
Expanded IndicationsDespite the strong recommendations against their use, acomplete lack of evidence of their safety and efficacy, theirinvasiveness and known potential toxicity, and the potentialmedicolegal peril associated with their unneeded placement,there has been a recent dramatic expansion of IVC filter use.A retrospective study conducted through the National Hos-pital Discharge Survey (NHDS) database found that thenumber of IVC filters placed in the US increased almost25-fold, from an estimated 2,000 placed in 1979 to anestimated 49,000 placed in 1999.9
IVC filters are often used for indications beyond thosespecified in evidence-based guidelines. Commonly proposed
uses include treatment of DVT in patients with cancer or burninjury or pregnant patients who do not have a high risk forbleeding, and PE prophylaxis in high-risk trauma or surgicalpatients with contraindications for anticoagulation; followingthrombectomy, embolectomy, or thrombolysis of DVT; orin patients with limited cardiopulmonary reserve or a free-floating ileofemoral thrombus (Table 1).5,10,11 The use ofIVC filters in these patient populations is of concern. Thereare proven effective options for VTE management in thesepatient populations and there are no controlled data to sup-port broadening of IVC filter indications beyond those rec-ommended by guidelines. In addition, the use of filters inthese situations is likely to increase the risk for acute VTE,placing the patient at risk for both the acute and chroniccomplications of VTE and the additional risks associatedwith the consideration of the need for anticoagulation.2,7
A multicenter prospective registry of 5,451 patients withconfirmed acute DVT enrolled between October 2001 andMarch 2002 at 183 sites that reported current usage patternsfor IVC filters highlighted the apparent overuse of IVCfilters as first-line therapy for VTE in preference to effectiveand less invasive pharmacologic options.3 In this study,14% of patients enrolled (781 of 5,451) had IVC filtersimplanted. The most common indications for filter place-ment in this study were contraindication for anticoagulanttherapy (42%) and primary PE prophylaxis in patients withproven DVT (33%); major bleeding from previous antico-agulation therapy (13%) and failure of previous anticoagu-
Table 1 Use of inferior vena cava filters
Recommended use according to evidence-based guidelines● Proven VTE with contraindication for anticoagulation● Proven VTE with complications of anticoagulation treatment● Recurrent VTE despite anticoagulation treatment (failure of
anticoagulation)Expanded use (not guideline recommended)
● Recurrent PE complicated by pulmonary hypertension● Patients with DVT and limited cardiopulmonary reserve or chronic
obstructive pulmonary disease● Patients with large, free-floating ileofemoral thrombus● Following thrombectomy, embolectomy, or thrombolysis of DVT● High-risk trauma patients (head and spinal cord injury, pelvic or
lower extremity fractures) with a contraindication foranticoagulation
● High-risk surgical patients with a contraindication foranticoagulation
● Patients with DVT who have cancer, burns, or are pregnantContraindications for filter placement
● Chronically thrombosed IVC● Anatomical abnormalities preventing access to the IVC for filter
placement
DVT � deep vein thrombosis; PE � pulmonary embolism; VTE � venous throm-boembolism.
Adapted from Chest,2 Prog Cardiovascular Dis,5 Blood,10 J Am Coll Surg,11 and J VascInterv Radiol.12
S14 The American Journal of Medicine, Vol 120 (10B), October 2007
lation therapy (11%) were additional reasons for filter in-sertion.3
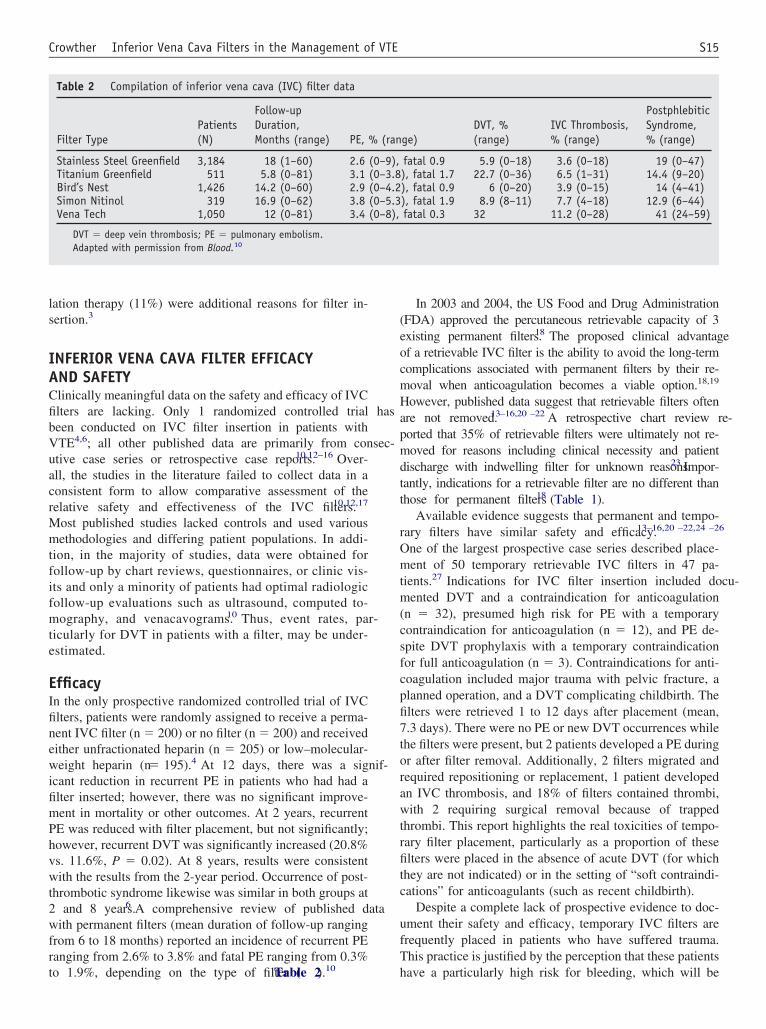
INFERIOR VENA CAVA FILTER EFFICACYAND SAFETYClinically meaningful data on the safety and efficacy of IVCfilters are lacking. Only 1 randomized controlled trial hasbeen conducted on IVC filter insertion in patients withVTE4,6; all other published data are primarily from consec-utive case series or retrospective case reports.10,12–16 Over-all, the studies in the literature failed to collect data in aconsistent form to allow comparative assessment of therelative safety and effectiveness of the IVC filters.10,12,17
Most published studies lacked controls and used variousmethodologies and differing patient populations. In addi-tion, in the majority of studies, data were obtained forfollow-up by chart reviews, questionnaires, or clinic vis-its and only a minority of patients had optimal radiologicfollow-up evaluations such as ultrasound, computed to-mography, and venacavograms.10 Thus, event rates, par-ticularly for DVT in patients with a filter, may be under-estimated.
EfficacyIn the only prospective randomized controlled trial of IVCfilters, patients were randomly assigned to receive a perma-nent IVC filter (n � 200) or no filter (n � 200) and receivedeither unfractionated heparin (n � 205) or low–molecular-weight heparin (n � 195).4 At 12 days, there was a signif-icant reduction in recurrent PE in patients who had had afilter inserted; however, there was no significant improve-ment in mortality or other outcomes. At 2 years, recurrentPE was reduced with filter placement, but not significantly;however, recurrent DVT was significantly increased (20.8%vs. 11.6%, P � 0.02). At 8 years, results were consistentwith the results from the 2-year period. Occurrence of post-thrombotic syndrome likewise was similar in both groups at2 and 8 years.6 A comprehensive review of published datawith permanent filters (mean duration of follow-up rangingfrom 6 to 18 months) reported an incidence of recurrent PEranging from 2.6% to 3.8% and fatal PE ranging from 0.3%to 1.9%, depending on the type of filter (Table 2).10
In 2003 and 2004, the US Food and Drug Administration(FDA) approved the percutaneous retrievable capacity of 3existing permanent filters.18 The proposed clinical advantageof a retrievable IVC filter is the ability to avoid the long-termcomplications associated with permanent filters by their re-moval when anticoagulation becomes a viable option.18,19
However, published data suggest that retrievable filters oftenare not removed.13–16,20 –22 A retrospective chart review re-ported that 35% of retrievable filters were ultimately not re-moved for reasons including clinical necessity and patientdischarge with indwelling filter for unknown reasons.23 Impor-tantly, indications for a retrievable filter are no different thanthose for permanent filters18 (Table 1).
Available evidence suggests that permanent and tempo-rary filters have similar safety and efficacy.13–16,20 –22,24 –26
One of the largest prospective case series described place-ment of 50 temporary retrievable IVC filters in 47 pa-tients.27 Indications for IVC filter insertion included docu-mented DVT and a contraindication for anticoagulation(n � 32), presumed high risk for PE with a temporarycontraindication for anticoagulation (n � 12), and PE de-spite DVT prophylaxis with a temporary contraindicationfor full anticoagulation (n � 3). Contraindications for anti-coagulation included major trauma with pelvic fracture, aplanned operation, and a DVT complicating childbirth. Thefilters were retrieved 1 to 12 days after placement (mean,7.3 days). There were no PE or new DVT occurrences whilethe filters were present, but 2 patients developed a PE duringor after filter removal. Additionally, 2 filters migrated andrequired repositioning or replacement, 1 patient developedan IVC thrombosis, and 18% of filters contained thrombi,with 2 requiring surgical removal because of trappedthrombi. This report highlights the real toxicities of tempo-rary filter placement, particularly as a proportion of thesefilters were placed in the absence of acute DVT (for whichthey are not indicated) or in the setting of “soft contraindi-cations” for anticoagulants (such as recent childbirth).
Despite a complete lack of prospective evidence to doc-ument their safety and efficacy, temporary IVC filters arefrequently placed in patients who have suffered trauma.This practice is justified by the perception that these patientshave a particularly high risk for bleeding, which will be
Table 2 Compilation of inferior vena cava (IVC) filter data
Filter TypePatients(N)
Follow-upDuration,Months (range) PE, % (range)
DVT, %(range)
IVC Thrombosis,% (range)
PostphlebiticSyndrome,% (range)
Stainless Steel Greenfield 3,184 18 (1–60) 2.6 (0–9), fatal 0.9 5.9 (0–18) 3.6 (0–18) 19 (0–47)Titanium Greenfield 511 5.8 (0–81) 3.1 (0–3.8), fatal 1.7 22.7 (0–36) 6.5 (1–31) 14.4 (9–20)Bird’s Nest 1,426 14.2 (0–60) 2.9 (0–4.2), fatal 0.9 6 (0–20) 3.9 (0–15) 14 (4–41)Simon Nitinol 319 16.9 (0–62) 3.8 (0–5.3), fatal 1.9 8.9 (8–11) 7.7 (4–18) 12.9 (6–44)Vena Tech 1,050 12 (0–81) 3.4 (0–8), fatal 0.3 32 11.2 (0–28) 41 (24–59)
DVT � deep vein thrombosis; PE � pulmonary embolism.Adapted with permission from Blood.10
S15Crowther Inferior Vena Cava Filters in the Management of VTE

exacerbated by pharmacologic prophylaxis. There is noevidence to support this practice.28 A large randomizedclinical trial supports the fact that pharmacologic prophy-laxis is both safe and effective in these patients,29 and thereare no randomized prospective evaluations of temporaryIVC interruption in this setting.
SafetyComplications related to insertion occur in 4% to 11% ofpatients with IVC filters, but result in death in only approx-imately 0.12% of patients.12 The most common adverseevents associated with IVC filter placement are thromboticcomplications. Thrombotic complications include insertion-site thrombosis (2% to 28%)12 and IVC thrombosis (3.6% to11.2%).10 An increased frequency of recurrent DVT (5.9%to 35.7%)4,6,10 and postphlebitic syndrome (12.9% to 41%)have also been reported, possibly because IVC filters canimpair lower extremity venous drainage.10 Other complica-tions include migration (in rare cases to the heart), penetra-tion of the IVC, filter fracture, vena caval obstruction, andguidewire entrapment.12
The use of retrievable filters can avoid some of thethrombotic complications with permanent filters; however,prolonged dwell times are commonly reported,19,30 –32 witha retrieval rate as low as 35% reported in 1 study.23 Thereis a notable paucity of published information on long-termoutcomes in patients implanted with retrievable filters thatwere not removed in a timely manner.30 Several case reportsof uneventful dwell times of nearly 1 year have been pub-lished31,32; however, prolonged dwell times can result inremoval problems due to adherence of fibrotic material tothe struts of the IVC filters. Epithelialization of the struts isa concern, and has been observed within 12 days,19,33 sug-gesting that wall damage might occur during the removalprocess. Repositioning or replacement of retrievable filterswith permanent filters may be required to prevent epitheli-alization.34 In addition, emboli captured within the filtersand documented residual IVC thrombus can prevent filterremoval.11,30,34
SUMMARYIVC filter placement, whether permanent or retrievable, isrecommended only in those patients with proven acute VTEand a current contraindication for anticoagulation, a complica-tion of anticoagulation (bleeding), or (perhaps) recurrent PEdespite adequate anticoagulation. Use of IVC filters for pre-vention of PE in patients who do not have an acute DVT hasnot been compared with pharmacologic prophylaxis, is likelyto result in clinicians not using proven prophylaxis in suchpatients, and is not supported by evidence-based treatmentrecommendation. The increased number of filters placed, par-ticularly with the introduction of retrievable IVC filters, is ofconcern. Given the lack of randomized controlled data, inva-siveness, the high cost of the devices and procedures, and theuncertainty around their complication rate, IVC filters shouldnot be used outside of those indications recommended in evi-
dence-based guidelines. To provide additional evidence to jus-tify current treatment practices, a randomized comparison oftemporary IVC interruption with pharmacologic prophylaxis isrequired in patients perceived to be at high risk for boththrombosis and bleeding.
CONFLICT OF INTERESTMark A. Crowther, MD, MSc, reports no conflict of interestwith the sponsor of this supplement article or productsdiscussed in this article.
References1. Barritt DW, Jordan SC. Anticoagulant drugs in the treatment of pul-
monary embolism: a controlled trial. Lancet. 1960;1:1309–1312.2. Buller HR, Agnelli G, Hull RD, Hyers TM, Prins MH, Raskob GE.
Antithrombotic therapy for venous thromboembolic disease: the Sev-enth ACCP Conference on Antithrombotic and Thrombolytic Therapy.Chest. 2004;126(suppl 3):401S–428S.
3. Jaff MR, Goldhaber SZ, Tapson VF. High utilization rate of vena cavafilters in deep vein thrombosis. Thromb Haemost. 2005;93:1117–1119.
4. Decousus H, Leizorovicz A, Parent F, et al, for the Prévention duRisque d’Embolie Pulmonaire par Interruption Cave Study Group. Aclinical trial of vena caval filters in the prevention of pulmonaryembolism in patients with proximal deep-vein thrombosis. N EnglJ Med. 1998;338:409–415.
5. Weichman K, Ansell JE. Inferior vena cava filters in venous throm-boembolism. Prog Cardiovasc Dis. 2006;49:98–105.
6. PREPIC Study Group. Eight-year follow-up of patients with perma-nent vena cava filters in the prevention of pulmonary embolism: thePREPIC (Prévention du Risque d’Embolie Pulmonaire par Interrup-tion Cave) randomized study. Circulation. 2005;112:416–422.
7. Geerts WH, Pineo GF, Heit JA, et al. Prevention of venous thrombo-embolism: the Seventh ACCP Conference on Antithrombotic andThrombolytic Therapy. Chest. 2004;126(suppl 3):338S–400S.
8. Levine MN, Raskob G, Beyth RJ, Kearon C, Schulman S. Hemor-rhagic complications of anticoagulant treatment: the Seventh ACCPConference on Antithrombotic and Thrombolytic Therapy. Chest.2004;126(suppl 3):287S–310S.
9. Stein PD, Kayali F, Olson RE. Twenty-one-year trends in the use ofinferior vena cava filters. Arch Intern Med. 2004;164:1541–1545.
10. Streiff MB. Vena caval filters: a comprehensive review. Blood. 2000;95:3669–3677.
11. Sarani B, Chun A, Venbrux A. Role of optional (retrievable) IVCfilters in surgical patients at risk for venous thromboembolic disease.J Am Coll Surg. 2005;201:957–964.
12. Kinney TB. Update on inferior vena cava filters. J Vasc Interv Radiol.2003;14:425–440.
13. Asch MR. Initial experience in humans with a new retrievable inferiorvena cava filter. Radiology. 2002;225:835–844.
14. Oliva VL, Szatmari F, Giroux MF, Flemming BK, Cohen SA, Soulez G.The Jonas study: evaluation of the retrievability of the Cordis OptEaseinferior vena cava filter. J Vasc Interv Radiol. 2005;16:1439–1445.
15. Grande WJ, Trerotola SO, Reilly PM, et al. Experience with therecovery filter as a retrievable inferior vena cava filter. J Vasc IntervRadiol. 2005;16:1189–1193.
16. Millward SF, Oliva VL, Bell SD, et al. Gunther Tulip Retrievable VenaCava Filter: results from the Registry of the Canadian InterventionalRadiology Association. J Vasc Interv Radiol. 2001;12:1053–1058.
17. Greenfield LJ, Rutherford RB, for the Vena Caval Filter ConsensusConference. Recommended reporting standards for vena caval filter place-ment and patient follow-up. J Vasc Interv Radiol. 1999;10:1013–1019.
18. Kaufman JA, Kinney TB, Streiff MB, et al. Guidelines for the use ofretrievable and convertible vena cava filters: report from the Society ofInterventional Radiology multidisciplinary consensus conference. JVasc Interv Radiol. 2006;17:449–459.
S16 The American Journal of Medicine, Vol 120 (10B), October 2007

19. Anderson RC, Bussey HI. Retrievable and permanent inferior venacava filters: selected considerations. Pharmacotherapy. 2006;26:1595–1600.
20. Bull PG, Mendel H, Schlegl A. Gunther vena caval filter: clinicalappraisal. J Vasc Interv Radiol. 1992;3:395–399.
21. Neuerburg JM, Gunther RW, Vorwerk D, et al. Results of a multi-center study of the retrievable Tulip Vena Cava Filter: early clinicalexperience. Cardiovasc Intervent Radiol. 1997;20:10–16.
22. Rosenthal D, Swischuk JL, Cohen SA, Wellons ED. OptEase retriev-able inferior vena cava filter: initial multicenter experience. Vascular.2005;13:286–289.
23. Kirilcuk NN, Herget EJ, Dicker RA, Spain DA, Hellinger JC, Brund-age SI. Are temporary inferior vena cava filters really temporary? Am JSurg. 2005;190:858–863.
24. Rousseau H, Perreault P, Otal P, et al. The 6-F nitinol TrapEaseinferior vena cava filter: results of a prospective multicenter trial. JVasc Interv Radiol. 2001;12:299–304.
25. Vos LD, Tielbeek AV, Bom EP, Gooszen HC, Vroegindeweij D. TheGunther temporary inferior vena cava filter for short-term protectionagainst pulmonary embolism. Cardiovasc Intervent Radiol. 1997;20:91–97.
26. Ponchon M, Goffette P, Hainaut P. Temporary vena caval filtration.Preliminary clinical experience with removable vena caval filters. ActaClin Belg. 1999;54:223–228.
27. Linsenmaier U, Rieger J, Schenk F, Rock C, Mangel E, Pfeifer KJ.Indications, management, and complications of temporary inferiorvena cava filters. Cardiovasc Intervent Radiol. 1998;21:464 – 469.
28. Geerts WH. Prevention of venous thromboembolism in high-riskpatients. Hematology Am Soc Hematol Educ Program. 2006:462–466.
29. Geerts WH, Jay RM, Code KI, et al. A comparison of low-doseheparin with low-molecular-weight heparin as prophylaxis againstvenous thromboembolism after major trauma. N Engl J Med. 1996;335:701–707.
30. Karmy-Jones R, Jurkovich GJ, Velmahos GC, et al. Practice patternsand outcomes of retrievable vena cava filters in trauma patients: anAAST multicenter study. J Trauma. 2007;62:17–24.
31. Binkert CA, Bansal A, Gates JD. Inferior vena cava filter removal after317-day implantation. J Vasc Interv Radiol. 2005;16:395–398.
32. Lipman JC. Removal of vena caval filter at 224 days. South Med J.2005;98:556–558.
33. Burbridge BE, Walker DR, Millward SF. Incorporation of the Gunthertemporary inferior vena cava filter into the caval wall. J Vasc IntervRadiol. 1996;7:289–290.
34. de Gregorio MA, Gamboa P, Gimeno MJ, et al. The Gunther Tulipretrievable filter: prolonged temporary filtration by repositioning withinthe inferior vena cava. J Vasc Interv Radiol. 2003;14:1259–1265.
S17Crowther Inferior Vena Cava Filters in the Management of VTE
Outpatient Management of Stable Acute PulmonaryEmbolism: Proposed Accelerated Pathway for RiskStratificationAmjad AlMahameed, MD, MPH,a and Teresa L. Carman, MDb
aDivision of Cardiology, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, Massachusetts, USA; and bSectionof Vascular Medicine, Department of Cardiovascular Medicine, Cleveland Clinic, Cleveland, Ohio, USA
ABSTRACT
Pulmonary embolism (PE) is a major health problem and a cause of worldwide morbidity and mortality.The current standard therapy for acute PE encourages admitting patients to the hospital for administrationof parenteral anticoagulation therapy as a bridge to oral vitamin K antagonists. Prognostic models thatidentify patients with stable (nonmassive) acute PE (SPE) who are at low risk for adverse outcome haverecently been reported. Based on these risk stratification models, hospital-based therapy is warranted forpatients with PE who meet the criteria associated with a high risk for adverse outcome. However, agrowing body of evidence suggests the feasibility of partial outpatient management and acceleratedhospital discharge (AHD) in a subset of patients with SPE. Prospective validation of these risk stratificationmodels for predicting patient suitability for AHD is needed. © 2007 Elsevier Inc. All rights reserved.
KEYWORDS: Anticoagulation; Pharmacotherapy; Pulmonary embolism; Risk stratification; Treatment; Venousthromboembolism
Deep vein thrombosis (DVT) and pulmonary embolism(PE) are manifestations of the same disease process re-ferred to collectively as venous thromboembolism(VTE). Despite increased awareness and wider employ-ment of reliable thromboprophylactic strategies, the in-cidence of first-time symptomatic VTE remains high at71 to 117 cases per 110,000 population.1 Up to 33% of allpatients with symptomatic DVT manifest PE at the timeof presentation. Nearly 50% of individuals with proximal(i.e., suprapopliteal or above-the-knee) DVT have radio-graphic evidence of a coexistent PE,2 and most fatalemboli are likely to arise from this region.3 Although therisk of embolization may be lower with untreated distal(i.e., calf vein or infrapopliteal) DVT, proximal propa-
gation is seen in as many as 25% of such thrombi, furtherincreasing the risk for PE. Patients with a history of PEare almost 4 times more likely to die of recurrent VTE inthe following year than are patients who are treated forDVT alone.4
It is estimated that about 237,000 nonfatal and294,000 fatal cases of PE occur in the United States eachyear.5 A total of 34% of VTE-related deaths were due tosudden massive PE and 59% followed undiagnosed PE.PE presents with a wide clinical spectrum and largelynonspecific symptoms; therefore, timely diagnosis re-quires a high degree of clinical suspicion. Studies suggestthat 55% to 94% of PEs in medical patients are notdiagnosed until autopsy.6,7 These numbers most likelyhave been underestimated because autopsies are not rou-tinely conducted in contemporary practice. It has beensuggested that up to 27% to 68% of fatal PE cases arepotentially preventable.8 Thus, rigorously screening forVTE risk factors and implementing effective thrombo-prophylaxis, along with prompt diagnosis and early ther-apy of suspected cases, is warranted.
Please see the Conflict of Interest section at the end of this article.Requests for reprints should be addressed to Amjad AlMahameed, MD,
MPH, Division of Cardiology, Beth Israel Deaconess Medical Center,Harvard Medical School, 1 Deaconess Road (Baker 4), Boston, Massachu-setts 02115.
E-mail address: [email protected].
0002-9343/$ -see front matter © 2007 Elsevier Inc. All rights reserved.doi:10.1016/j.amjmed.2007.08.010
The American Journal of Medicine (2007) Vol 120 (10B), S18–S25
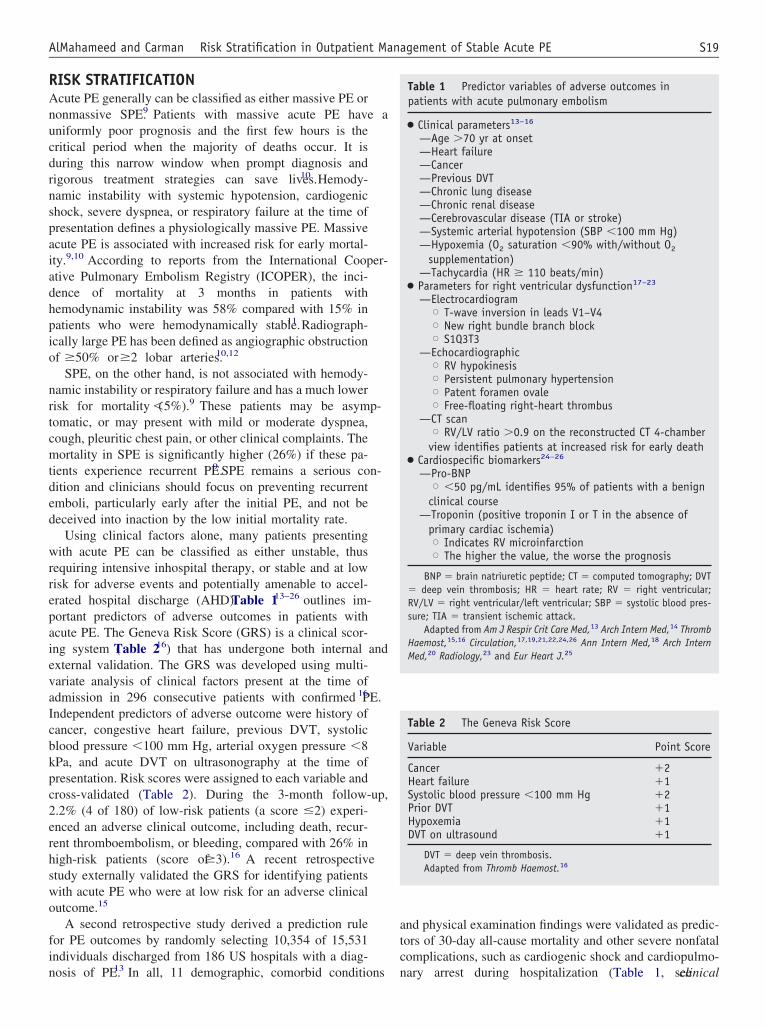
RISK STRATIFICATIONAcute PE generally can be classified as either massive PE ornonmassive SPE.9 Patients with massive acute PE have auniformly poor prognosis and the first few hours is thecritical period when the majority of deaths occur. It isduring this narrow window when prompt diagnosis andrigorous treatment strategies can save lives.10 Hemody-namic instability with systemic hypotension, cardiogenicshock, severe dyspnea, or respiratory failure at the time ofpresentation defines a physiologically massive PE. Massiveacute PE is associated with increased risk for early mortal-ity.9,10 According to reports from the International Cooper-ative Pulmonary Embolism Registry (ICOPER), the inci-dence of mortality at 3 months in patients withhemodynamic instability was 58% compared with 15% inpatients who were hemodynamically stable.11 Radiograph-ically large PE has been defined as angiographic obstructionof �50% or �2 lobar arteries.10,12
SPE, on the other hand, is not associated with hemody-namic instability or respiratory failure and has a much lowerrisk for mortality (�5%).9 These patients may be asymp-tomatic, or may present with mild or moderate dyspnea,cough, pleuritic chest pain, or other clinical complaints. Themortality in SPE is significantly higher (26%) if these pa-tients experience recurrent PE.9 SPE remains a serious con-dition and clinicians should focus on preventing recurrentemboli, particularly early after the initial PE, and not bedeceived into inaction by the low initial mortality rate.
Using clinical factors alone, many patients presentingwith acute PE can be classified as either unstable, thusrequiring intensive inhospital therapy, or stable and at lowrisk for adverse events and potentially amenable to accel-erated hospital discharge (AHD). Table 113–26 outlines im-portant predictors of adverse outcomes in patients withacute PE. The Geneva Risk Score (GRS) is a clinical scor-ing system (Table 216) that has undergone both internal andexternal validation. The GRS was developed using multi-variate analysis of clinical factors present at the time ofadmission in 296 consecutive patients with confirmed PE.16
Independent predictors of adverse outcome were history ofcancer, congestive heart failure, previous DVT, systolicblood pressure �100 mm Hg, arterial oxygen pressure �8kPa, and acute DVT on ultrasonography at the time ofpresentation. Risk scores were assigned to each variable andcross-validated (Table 2). During the 3-month follow-up,2.2% (4 of 180) of low-risk patients (a score �2) experi-enced an adverse clinical outcome, including death, recur-rent thromboembolism, or bleeding, compared with 26% inhigh-risk patients (score of �3).16 A recent retrospectivestudy externally validated the GRS for identifying patientswith acute PE who were at low risk for an adverse clinicaloutcome.15
A second retrospective study derived a prediction rulefor PE outcomes by randomly selecting 10,354 of 15,531individuals discharged from 186 US hospitals with a diag-nosis of PE.13 In all, 11 demographic, comorbid conditions
and physical examination findings were validated as predic-tors of 30-day all-cause mortality and other severe nonfatalcomplications, such as cardiogenic shock and cardiopulmo-nary arrest during hospitalization (Table 1, see clinical
Table 1 Predictor variables of adverse outcomes inpatients with acute pulmonary embolism
● Clinical parameters13–16
—Age �70 yr at onset—Heart failure—Cancer—Previous DVT—Chronic lung disease—Chronic renal disease—Cerebrovascular disease (TIA or stroke)—Systemic arterial hypotension (SBP �100 mm Hg)—Hypoxemia (O2 saturation �90% with/without O2
supplementation)—Tachycardia (HR � 110 beats/min)
● Parameters for right ventricular dysfunction17–23
—ElectrocardiogramX T-wave inversion in leads V1–V4X New right bundle branch blockX S1Q3T3
—EchocardiographicX RV hypokinesisX Persistent pulmonary hypertensionX Patent foramen ovaleX Free-floating right-heart thrombus
—CT scanX RV/LV ratio �0.9 on the reconstructed CT 4-chamberview identifies patients at increased risk for early death
● Cardiospecific biomarkers24–26
—Pro-BNPX �50 pg/mL identifies 95% of patients with a benignclinical course
—Troponin (positive troponin I or T in the absence ofprimary cardiac ischemia)X Indicates RV microinfarctionX The higher the value, the worse the prognosis
BNP � brain natriuretic peptide; CT � computed tomography; DVT� deep vein thrombosis; HR � heart rate; RV � right ventricular;RV/LV � right ventricular/left ventricular; SBP � systolic blood pres-sure; TIA � transient ischemic attack.
Adapted from Am J Respir Crit Care Med,13 Arch Intern Med,14 ThrombHaemost,15,16 Circulation,17,19,21,22,24,26 Ann Intern Med,18 Arch InternMed,20 Radiology,23 and Eur Heart J.25
Table 2 The Geneva Risk Score
Variable Point Score
Cancer �2Heart failure �1Systolic blood pressure �100 mm Hg �2Prior DVT �1Hypoxemia �1DVT on ultrasound �1
DVT � deep vein thrombosis.Adapted from Thromb Haemost.16
S19AlMahameed and Carman Risk Stratification in Outpatient Management of Stable Acute PE
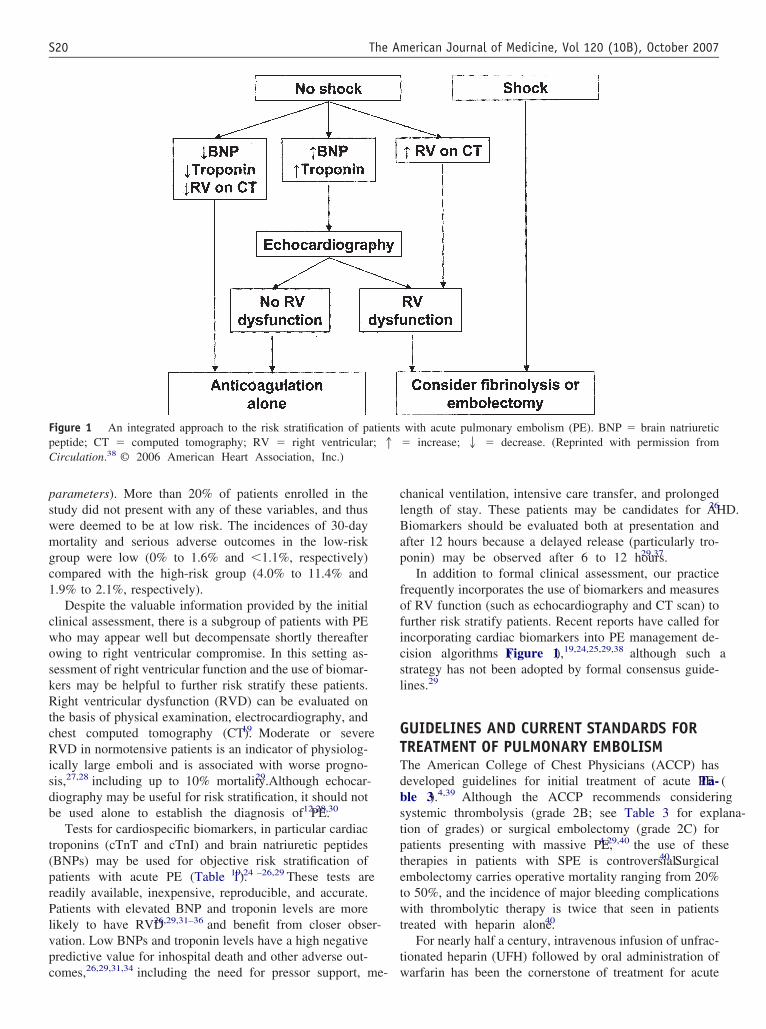
parameters). More than 20% of patients enrolled in thestudy did not present with any of these variables, and thuswere deemed to be at low risk. The incidences of 30-daymortality and serious adverse outcomes in the low-riskgroup were low (0% to 1.6% and �1.1%, respectively)compared with the high-risk group (4.0% to 11.4% and1.9% to 2.1%, respectively).
Despite the valuable information provided by the initialclinical assessment, there is a subgroup of patients with PEwho may appear well but decompensate shortly thereafterowing to right ventricular compromise. In this setting as-sessment of right ventricular function and the use of biomar-kers may be helpful to further risk stratify these patients.Right ventricular dysfunction (RVD) can be evaluated onthe basis of physical examination, electrocardiography, andchest computed tomography (CT).19 Moderate or severeRVD in normotensive patients is an indicator of physiolog-ically large emboli and is associated with worse progno-sis,27,28 including up to 10% mortality.29 Although echocar-diography may be useful for risk stratification, it should notbe used alone to establish the diagnosis of PE.12,28,30
Tests for cardiospecific biomarkers, in particular cardiactroponins (cTnT and cTnI) and brain natriuretic peptides(BNPs) may be used for objective risk stratification ofpatients with acute PE (Table 1).19,24 –26,29 These tests arereadily available, inexpensive, reproducible, and accurate.Patients with elevated BNP and troponin levels are morelikely to have RVD26,29,31–36 and benefit from closer obser-vation. Low BNPs and troponin levels have a high negativepredictive value for inhospital death and other adverse out-comes,26,29,31,34 including the need for pressor support, me-
chanical ventilation, intensive care transfer, and prolongedlength of stay. These patients may be candidates for AHD.26
Biomarkers should be evaluated both at presentation andafter 12 hours because a delayed release (particularly tro-ponin) may be observed after 6 to 12 hours.29,37
In addition to formal clinical assessment, our practicefrequently incorporates the use of biomarkers and measuresof RV function (such as echocardiography and CT scan) tofurther risk stratify patients. Recent reports have called forincorporating cardiac biomarkers into PE management de-cision algorithms (Figure 1),19,24,25,29,38 although such astrategy has not been adopted by formal consensus guide-lines.29
GUIDELINES AND CURRENT STANDARDS FORTREATMENT OF PULMONARY EMBOLISMThe American College of Chest Physicians (ACCP) hasdeveloped guidelines for initial treatment of acute PE (Ta-ble 3).4,39 Although the ACCP recommends consideringsystemic thrombolysis (grade 2B; see Table 3 for explana-tion of grades) or surgical embolectomy (grade 2C) forpatients presenting with massive PE,4,29,40 the use of thesetherapies in patients with SPE is controversial.40 Surgicalembolectomy carries operative mortality ranging from 20%to 50%, and the incidence of major bleeding complicationswith thrombolytic therapy is twice that seen in patientstreated with heparin alone.40
For nearly half a century, intravenous infusion of unfrac-tionated heparin (UFH) followed by oral administration ofwarfarin has been the cornerstone of treatment for acute
Figure 1 An integrated approach to the risk stratification of patients with acute pulmonary embolism (PE). BNP � brain natriureticpeptide; CT � computed tomography; RV � right ventricular; 1 � increase; 2 � decrease. (Reprinted with permission fromCirculation.38 © 2006 American Heart Association, Inc.)
S20 The American Journal of Medicine, Vol 120 (10B), October 2007
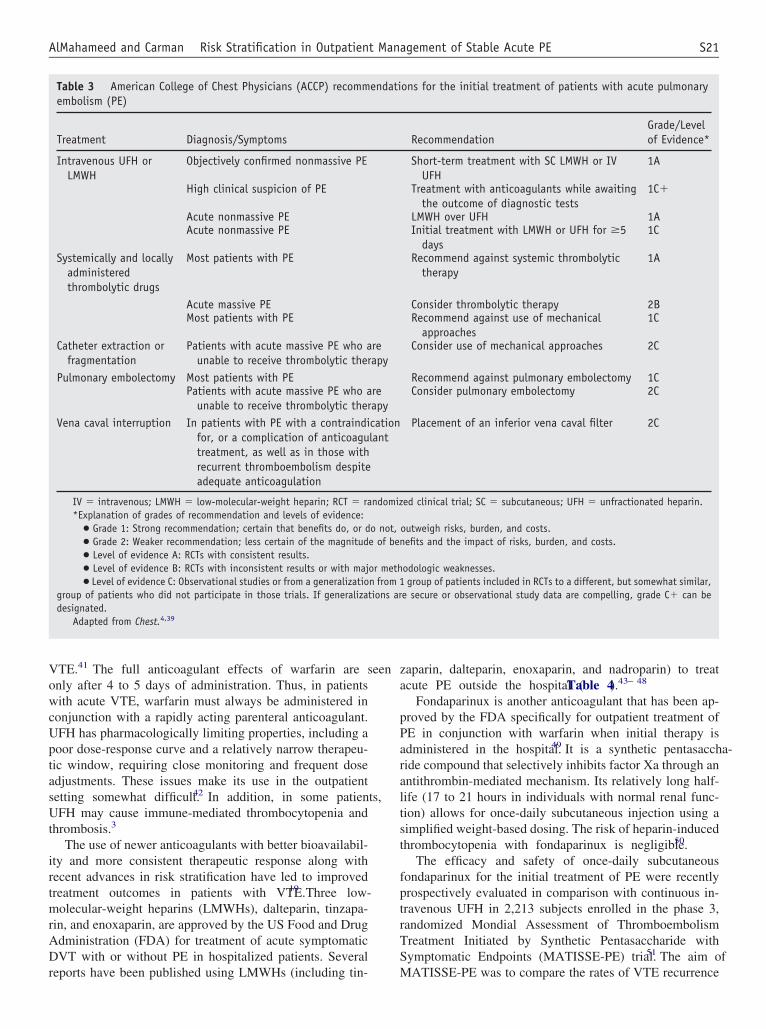
VTE.41 The full anticoagulant effects of warfarin are seenonly after 4 to 5 days of administration. Thus, in patientswith acute VTE, warfarin must always be administered inconjunction with a rapidly acting parenteral anticoagulant.UFH has pharmacologically limiting properties, including apoor dose-response curve and a relatively narrow therapeu-tic window, requiring close monitoring and frequent doseadjustments. These issues make its use in the outpatientsetting somewhat difficult.42 In addition, in some patients,UFH may cause immune-mediated thrombocytopenia andthrombosis.3
The use of newer anticoagulants with better bioavailabil-ity and more consistent therapeutic response along withrecent advances in risk stratification have led to improvedtreatment outcomes in patients with VTE.19 Three low-molecular-weight heparins (LMWHs), dalteparin, tinzapa-rin, and enoxaparin, are approved by the US Food and DrugAdministration (FDA) for treatment of acute symptomaticDVT with or without PE in hospitalized patients. Severalreports have been published using LMWHs (including tin-
zaparin, dalteparin, enoxaparin, and nadroparin) to treatacute PE outside the hospital (Table 4).43– 48
Fondaparinux is another anticoagulant that has been ap-proved by the FDA specifically for outpatient treatment ofPE in conjunction with warfarin when initial therapy isadministered in the hospital.49 It is a synthetic pentasaccha-ride compound that selectively inhibits factor Xa through anantithrombin-mediated mechanism. Its relatively long half-life (17 to 21 hours in individuals with normal renal func-tion) allows for once-daily subcutaneous injection using asimplified weight-based dosing. The risk of heparin-inducedthrombocytopenia with fondaparinux is negligible.50
The efficacy and safety of once-daily subcutaneousfondaparinux for the initial treatment of PE were recentlyprospectively evaluated in comparison with continuous in-travenous UFH in 2,213 subjects enrolled in the phase 3,randomized Mondial Assessment of ThromboembolismTreatment Initiated by Synthetic Pentasaccharide withSymptomatic Endpoints (MATISSE-PE) trial.51 The aim ofMATISSE-PE was to compare the rates of VTE recurrence
Table 3 American College of Chest Physicians (ACCP) recommendations for the initial treatment of patients with acute pulmonaryembolism (PE)
Treatment Diagnosis/Symptoms RecommendationGrade/Levelof Evidence*
Intravenous UFH orLMWH
Objectively confirmed nonmassive PE Short-term treatment with SC LMWH or IVUFH
1A
High clinical suspicion of PE Treatment with anticoagulants while awaitingthe outcome of diagnostic tests
1C�
Acute nonmassive PE LMWH over UFH 1AAcute nonmassive PE Initial treatment with LMWH or UFH for �5
days1C
Systemically and locallyadministeredthrombolytic drugs
Most patients with PE Recommend against systemic thrombolytictherapy
1A
Acute massive PE Consider thrombolytic therapy 2BMost patients with PE Recommend against use of mechanical
approaches1C
Catheter extraction orfragmentation
Patients with acute massive PE who areunable to receive thrombolytic therapy
Consider use of mechanical approaches 2C
Pulmonary embolectomy Most patients with PE Recommend against pulmonary embolectomy 1CPatients with acute massive PE who are
unable to receive thrombolytic therapyConsider pulmonary embolectomy 2C
Vena caval interruption In patients with PE with a contraindicationfor, or a complication of anticoagulanttreatment, as well as in those withrecurrent thromboembolism despiteadequate anticoagulation
Placement of an inferior vena caval filter 2C
IV � intravenous; LMWH � low-molecular-weight heparin; RCT � randomized clinical trial; SC � subcutaneous; UFH � unfractionated heparin.*Explanation of grades of recommendation and levels of evidence:
● Grade 1: Strong recommendation; certain that benefits do, or do not, outweigh risks, burden, and costs.● Grade 2: Weaker recommendation; less certain of the magnitude of benefits and the impact of risks, burden, and costs.● Level of evidence A: RCTs with consistent results.● Level of evidence B: RCTs with inconsistent results or with major methodologic weaknesses.● Level of evidence C: Observational studies or from a generalization from 1 group of patients included in RCTs to a different, but somewhat similar,
group of patients who did not participate in those trials. If generalizations are secure or observational study data are compelling, grade C� can bedesignated.
Adapted from Chest.4,39
S21AlMahameed and Carman Risk Stratification in Outpatient Management of Stable Acute PE
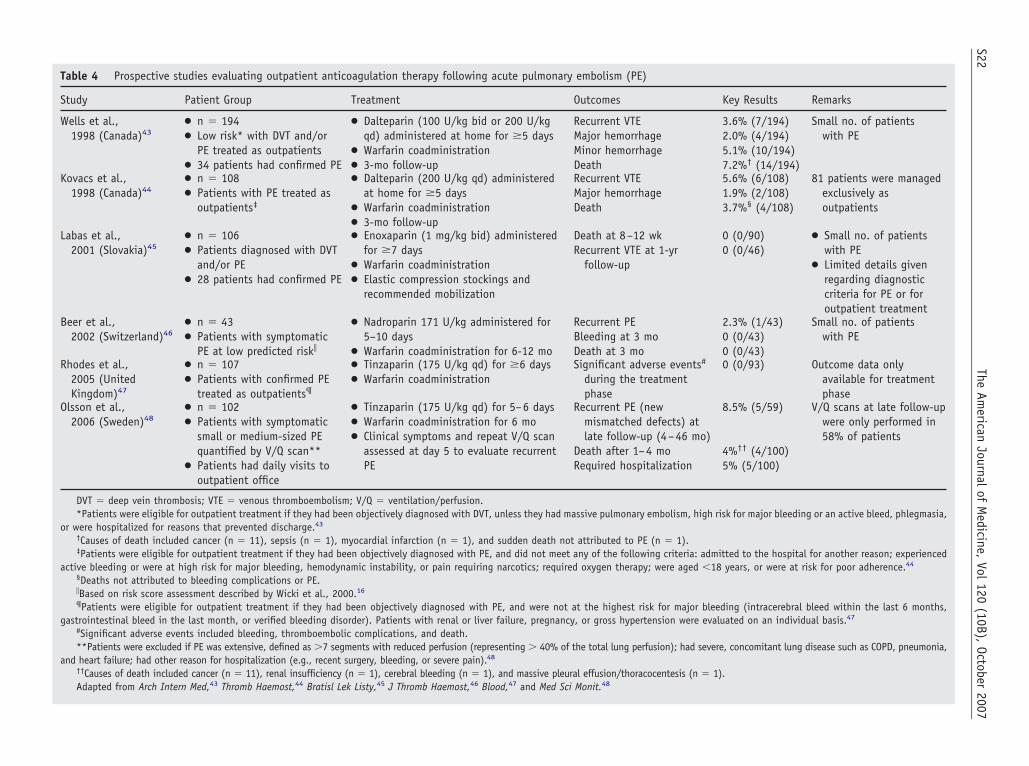
Table 4 Prospective studies evaluating outpatient anticoagulation therapy following acute pulmonary embolism (PE)
Study Patient Group Treatment Outcomes Key Results Remarks
Wells et al.,1998 (Canada)43
● n � 194● Low risk* with DVT and/or
PE treated as outpatients● 34 patients had confirmed PE
● Dalteparin (100 U/kg bid or 200 U/kgqd) administered at home for �5 days
● Warfarin coadministration● 3-mo follow-up
Recurrent VTEMajor hemorrhageMinor hemorrhageDeath
3.6% (7/194)2.0% (4/194)5.1% (10/194)7.2%† (14/194)
Small no. of patientswith PE
Kovacs et al.,1998 (Canada)44
● n � 108● Patients with PE treated as
outpatients‡
● Dalteparin (200 U/kg qd) administeredat home for �5 days
● Warfarin coadministration● 3-mo follow-up
Recurrent VTEMajor hemorrhageDeath
5.6% (6/108)1.9% (2/108)3.7%§ (4/108)
81 patients were managedexclusively asoutpatients
Labas et al.,2001 (Slovakia)45
● n � 106● Patients diagnosed with DVT
and/or PE● 28 patients had confirmed PE
● Enoxaparin (1 mg/kg bid) administeredfor �7 days
● Warfarin coadministration● Elastic compression stockings and
recommended mobilization
Death at 8–12 wkRecurrent VTE at 1-yr
follow-up
0 (0/90)0 (0/46)
● Small no. of patientswith PE
● Limited details givenregarding diagnosticcriteria for PE or foroutpatient treatment
Beer et al.,2002 (Switzerland)46
● n � 43● Patients with symptomatic
PE at low predicted risk�
● Nadroparin 171 U/kg administered for5–10 days
● Warfarin coadministration for 6-12 mo
Recurrent PEBleeding at 3 moDeath at 3 mo
2.3% (1/43)0 (0/43)0 (0/43)
Small no. of patientswith PE
Rhodes et al.,2005 (UnitedKingdom)47
● n � 107● Patients with confirmed PE
treated as outpatients¶
● Tinzaparin (175 U/kg qd) for �6 days● Warfarin coadministration
Significant adverse events#
during the treatmentphase
0 (0/93) Outcome data onlyavailable for treatmentphase
Olsson et al.,2006 (Sweden)48
● n � 102● Patients with symptomatic
small or medium-sized PEquantified by V/Q scan**
● Patients had daily visits tooutpatient office
● Tinzaparin (175 U/kg qd) for 5–6 days● Warfarin coadministration for 6 mo● Clinical symptoms and repeat V/Q scan
assessed at day 5 to evaluate recurrentPE
Recurrent PE (newmismatched defects) atlate follow-up (4–46 mo)
Death after 1–4 moRequired hospitalization
8.5% (5/59)
4%†† (4/100)5% (5/100)
V/Q scans at late follow-upwere only performed in58% of patients
DVT � deep vein thrombosis; VTE � venous thromboembolism; V/Q � ventilation/perfusion.*Patients were eligible for outpatient treatment if they had been objectively diagnosed with DVT, unless they had massive pulmonary embolism, high risk for major bleeding or an active bleed, phlegmasia,
or were hospitalized for reasons that prevented discharge.43
†Causes of death included cancer (n � 11), sepsis (n � 1), myocardial infarction (n � 1), and sudden death not attributed to PE (n � 1).‡Patients were eligible for outpatient treatment if they had been objectively diagnosed with PE, and did not meet any of the following criteria: admitted to the hospital for another reason; experienced
active bleeding or were at high risk for major bleeding, hemodynamic instability, or pain requiring narcotics; required oxygen therapy; were aged �18 years, or were at risk for poor adherence.44
§Deaths not attributed to bleeding complications or PE.�Based on risk score assessment described by Wicki et al., 2000.16
¶Patients were eligible for outpatient treatment if they had been objectively diagnosed with PE, and were not at the highest risk for major bleeding (intracerebral bleed within the last 6 months,gastrointestinal bleed in the last month, or verified bleeding disorder). Patients with renal or liver failure, pregnancy, or gross hypertension were evaluated on an individual basis.47
#Significant adverse events included bleeding, thromboembolic complications, and death.**Patients were excluded if PE was extensive, defined as �7 segments with reduced perfusion (representing � 40% of the total lung perfusion); had severe, concomitant lung disease such as COPD, pneumonia,
and heart failure; had other reason for hospitalization (e.g., recent surgery, bleeding, or severe pain).48
††Causes of death included cancer (n � 11), renal insufficiency (n � 1), cerebral bleeding (n � 1), and massive pleural effusion/thoracocentesis (n � 1).Adapted from Arch Intern Med,43 Thromb Haemost,44 Bratisl Lek Listy,45 J Thromb Haemost,46 Blood,47 and Med Sci Monit.48
S22The
American
Journalof
Medicine,
Vol120
(10B),October
2007

during the 3-month follow-up period and major bleedingand death during the initial treatment period. Fondaparinuxwas administered as a once-daily subcutaneous dose of 7.5mg (adjusted to 5 mg and 10 mg for patients weighing �50kg and �100 kg, respectively). Only 42 (3.8%) of 1,103patients who received fondaparinux had recurrent VTEevents compared with 56 (5.0%) of 1,110 patients assignedto receive UFH, for an absolute difference of �1.2 percent-age points in favor of fondaparinux (P � NS). Major andnonmajor bleeding, thrombocytopenia, and mortality weresimilar in both groups during the entire period of the study.
The current ACCP recommendations for SPE involvesadmitting all patients to the hospital for administration ofparenteral anticoagulation therapy, either UFH or LMWH,as a bridge to warfarin with a minimum of 5 days of overlapuntil a therapeutic international normalized ratio (INR)�2.0 is achieved.4 Warfarin should be continued for aminimum of 6 to 12 months. Fondaparinux was not yetapproved for treatment of DVT and PE when the SeventhACCP Conference on Antithrombotic and ThrombolyticTherapy developed treatment guidelines; therefore, this op-tion was not included when the guidelines were released in2004.
BENEFITS OF OUTPATIENT TREATMENTThere is growing evidence that AHD and partial outpa-tient therapy is feasible for patients with nonmassiveSPE.44 – 48,51–57 Partial outpatient treatment of PE via anAHD program may be offered to patients deemed to be atlow risk for mortality, recurrent PE, or major bleedingcomplications; who have a home environment with ade-quate support; and who are able to self-administer themedications (see Tables 1 and 2 for risk stratificationcriteria).53,54 In 1 study, up to 83% of VTE patientsqualified for outpatient treatment.43 Benefits of outpatientmanagement include improved quality-of-life mea-sures,58 increased physical activity and social function-ing,58 reduced length of stay,58,59 and substantial costsavings.52,60,61 Pharmacoeconomic analyses of outpatienttreatment for DVT reported cost reductions of 34% to64%.52 Agnelli and colleagues52 reported � $2,400 incost savings per patient when acute PE was treated on anoutpatient basis. However, despite these incentives, cli-nicians are rightfully disinclined to send home patientswho might be at risk for an unfavorable outcome.16
Several studies have demonstrated successful outpatienttherapy with LMWH as a bridge to warfarin for the treat-ment of acute SPE (Table 4).43– 48 In addition, 158 patientsin the fondaparinux group of the MATISSE-PE trial werepermitted early discharge and received fondaparinux partlyon an outpatient basis51,59; 5 of these patients had recurrentVTE, and none had major bleeding or died during initialtreatment.59 In light of the current data and the consider-ation for AHD with partial outpatient therapy of acute PE,there is a need to accurately predict patient suitability forthis type of therapy. It is likely that identification of low-risk
patients with acute PE will facilitate less complex treatmentand allow for earlier discharge without sacrificing efficacyor safety.
SUMMARYAcute PE has a wide clinical spectrum, ranging fromasymptomatic patients to those presenting with suddendeath. The clinical course in patients who survive an initialthromboembolic episode can be complicated by recurrentnonfatal VTE, fatal PE, postthrombotic syndrome, andchronic thromboembolic pulmonary hypertension. Earlyidentification of high-risk patients with acute PE who are atincreased risk for adverse outcomes remains a challenge inclinical practice. A substantial subset of patients with stablePE may be amenable to outpatient treatment; however,appropriate risk stratification is necessary to identify thesecandidates. Outpatient treatment in these patients can re-duce hospital stay, improve patient quality of life, anddecrease healthcare costs. Further studies are needed toestablish clear clinical pathways that prospectively use con-temporary risk stratification criteria for AHD of patientspresenting with acute SPE.
Treatment of acute PE with LMWH or fondaparinuxadministered in an outpatient setting for appropriately se-lected patients is at least as effective and safe as conven-tional inpatient treatment with UFH in preventing recurrentVTE, without increasing the risk for major bleeding whenpatients are closely monitored. Phase 3 clinical trials haveshown fondaparinux to be an effective alternative to LMWHsand UFH for the outpatient treatment of DVT62; addition-ally, these trials have shown it to be efficacious in inpatientand partial outpatient treatment of PE.51 Fondaparinux cur-rently is the only FDA-approved medication for partialoutpatient treatment of SPE.
CONFLICT OF INTERESTThese authors report the following conflicts of interest withthe sponsor of this supplement article or products discussedin this article. Teresa L. Carman, MD, has served as amember of the Speakers’ Bureau for Bristol-Myers SquibbCompany. Amjad AlMahameed, MD, has served as a mem-ber of the Speakers’ Bureau for sanofi-aventis and Glaxo-SmithKline.
References1. White RH. The epidemiology of venous thromboembolism. Circula-
tion. 2003;107(suppl 1):I4–18.2. Meignan M, Rosso J, Gauthier H, et al. Systematic lung scans reveal
a high frequency of silent pulmonary embolism in patients with prox-imal deep venous thrombosis. Arch Intern Med. 2000;160:159–164.
3. Bates SM, Ginsberg JS. Clinical practice: treatment of deep-veinthrombosis. N Engl J Med. 2004;351:268–277.
4. Buller HR, Agnelli G, Hull RD, Hyers TM, Prins MH, Raskob GE.Antithrombotic therapy for venous thromboembolic disease: the Sev-enth ACCP Conference on Antithrombotic and Thrombolytic Therapy.Chest. 2004;126(suppl 3):401S–428S.
S23AlMahameed and Carman Risk Stratification in Outpatient Management of Stable Acute PE

5. Heit J, Cohen A, Anderson FA. Estimated annual number of incidentand recurrent, non-fatal and fatal venous thromboembolism (VTE)events in the US [abstract]. Blood. 2005;102.
6. Pineda LA, Hathwar VS, Grant BJ. Clinical suspicion of fatal pulmo-nary embolism. Chest. 2001;120:791–795.
7. Stein PD, Henry JW. Prevalence of acute pulmonary embolism amongpatients in a general hospital and at autopsy. Chest. 1995;108:978–981.
8. Merli GJ. Pulmonary embolism in medical patients: improved diag-nosis and the role of low-molecular-weight heparin in prevention andtreatment. J Thromb Thrombolysis. 2004;18:117–125.
9. Douketis JD. Prognosis in pulmonary embolism. Curr Opin PulmMed. 2001;7:354–359.
10. Wood KE. Major pulmonary embolism: review of a pathophysiologicapproach to the golden hour of hemodynamically significant pulmo-nary embolism. Chest. 2002;121:877–905.
11. Goldhaber SZ, Visani L, De Rosa M. Acute pulmonary embolism:clinical outcomes in the International Cooperative Pulmonary Embo-lism Registry (ICOPER). Lancet. 1999;353:1386–1389.
12. Lim KE, Chan CY, Chu PH, Hsu YY, Hsu WC. Right ventriculardysfunction secondary to acute massive pulmonary embolism detectedby helical computed tomography pulmonary angiography. Clin Imag-ing. 2005;29:16–21.
13. Aujesky D, Obrosky DS, Stone RA, et al. Derivation and validation ofa prognostic model for pulmonary embolism. Am J Respir Crit CareMed. 2005;172:1041–1046.
14. Heit JA, Silverstein MD, Mohr DN, Petterson TM, O’Fallon WM,Melton LJ III. Predictors of survival after deep vein thrombosis andpulmonary embolism: a population-based, cohort study. Arch InternMed. 1999;159:445–453.
15. Nendaz MR, Bandelier P, Aujesky D, et al. Validation of a risk scoreidentifying patients with acute pulmonary embolism, who are at lowrisk of clinical adverse outcome. Thromb Haemost. 2004;91:1232–1236.
16. Wicki J, Perrier A, Perneger TV, Bounameaux H, Junod AF. Predict-ing adverse outcome in patients with acute pulmonary embolism: a riskscore. Thromb Haemost. 2000;84:548–552.
17. Konstantinides S, Geibel A, Kasper W, Olschewski M, Blumel L, JustH. Patent foramen ovale is an important predictor of adverse outcomein patients with major pulmonary embolism. Circulation. 1998;97:1946–1951.
18. Goldhaber SZ. Echocardiography in the management of pulmonaryembolism. Ann Intern Med. 2002;136:691–700.
19. Goldhaber SZ, Elliott CG. Acute pulmonary embolism: part II. Riskstratification, treatment, and prevention. Circulation. 2003;108:2834–2838.
20. Kucher N, Rossi E, De Rosa M, Goldhaber SZ. Prognostic role ofechocardiography among patients with acute pulmonary embolism anda systolic arterial pressure of 90 mm Hg or higher. Arch Intern Med.2005;165:1777–1781.
21. Quiroz R, Kucher N, Schoepf UJ, et al. Right ventricular enlargementon chest computed tomography: prognostic role in acute pulmonaryembolism. Circulation. 2004;109:2401–2404.
22. Schoepf UJ, Kucher N, Kipfmueller F, Quiroz R, Costello P, Gold-haber SZ. Right ventricular enlargement on chest computed tomogra-phy: a predictor of early death in acute pulmonary embolism. Circu-lation. 2004;110:3276–3280.
23. van der Meer RW, Pattynama PM, van Strijen MJ, et al. Right ven-tricular dysfunction and pulmonary obstruction index at helical CT:prediction of clinical outcome during 3-month follow-up in patientswith acute pulmonary embolism. Radiology. 2005;235:798–803.
24. Binder L, Pieske B, Olschewski M, et al. N-terminal pro-brain natri-uretic peptide or troponin testing followed by echocardiography forrisk stratification of acute pulmonary embolism. Circulation. 2005;112:1573–1579.
25. Kostrubiec M, Pruszczyk P, Bochowicz A, et al. Biomarker-based riskassessment model in acute pulmonary embolism. Eur Heart J. 2005;26:2166–2172.
26. Kucher N, Printzen G, Doernhoefer T, Windecker S, Meier B, HessOM. Low pro-brain natriuretic peptide levels predict benign clinicaloutcome in acute pulmonary embolism. Circulation. 2003;107:1576–1578.
27. Grifoni S, Olivotto I, Cecchini P, et al. Short-term clinical outcome ofpatients with acute pulmonary embolism, normal blood pressure, andechocardiographic right ventricular dysfunction. Circulation. 2000;101:2817–2822.
28. Ribeiro A, Lindmarker P, Juhlin-Dannfelt A, Johnsson H, Jorfeldt L.Echocardiography Doppler in pulmonary embolism: right ventriculardysfunction as a predictor of mortality rate. Am Heart J. 1997;134:479–487.
29. Kucher N, Goldhaber SZ. Cardiac biomarkers for risk stratification ofpatients with acute pulmonary embolism. Circulation. 2003;108:2191–2194.
30. Geibel A, Zehender M, Kasper W, Olschewski M, Klima C, Konstan-tinides SV. Prognostic value of the ECG on admission in patients withacute major pulmonary embolism. Eur Respir J. 2005;25:843–848.
31. Giannitsis E, Muller-Bardorff M, Kurowski V, et al. Independentprognostic value of cardiac troponin T in patients with confirmedpulmonary embolism. Circulation. 2000;102:211–217.
32. Meyer T, Binder L, Hruska N, Luthe H, Buchwald AB. Cardiactroponin I elevation in acute pulmonary embolism is associated withright ventricular dysfunction. J Am Coll Cardiol. 2000;36:1632–1636.
33. Tulevski I, Hirsch A, Sanson BJ, et al. Increased brain natriureticpeptide as a marker for right ventricular dysfunction in acute pulmo-nary embolism. Thromb Haemost. 2001;86:1193–1196.
34. Konstantinides S, Geibel A, Olschewski M, et al. Importance ofcardiac troponins I and T in risk stratification of patients with acutepulmonary embolism. Circulation. 2002;106:1263–1268.
35. Mehta NJ, Jani K, Khan IA. Clinical usefulness and prognostic valueof elevated cardiac troponin I levels in acute pulmonary embolism. AmHeart J. 2003;145:821–825.
36. Pruszczyk P, Bochowicz A, Torbicki A, et al. Cardiac troponin Tmonitoring identifies high-risk group of normotensive patients withacute pulmonary embolism. Chest. 2003;123:1947–1952.
37. Muller-Bardorff M, Weidtmann B, Giannitsis E, Kurowski V, KatusHA. Release kinetics of cardiac troponin T in survivors of confirmedsevere pulmonary embolism. Clin Chem. 2002;48:673–675.
38. Piazza G, Goldhaber SZ. Acute pulmonary embolism: part II. Treat-ment and prophylaxis. Circulation. 2006;114:e42–e47.
39. Guyatt G, Schunemann HJ, Cook D, Jaeschke R, Pauker S. Applyingthe grades of recommendation for antithrombotic and thrombolytictherapy: the Seventh ACCP Conference on Antithrombotic andThrombolytic Therapy. Chest. 2004;126(suppl 3):179S–187S.
40. Task Force on Pulmonary Embolism, European Society of Cardiology.Guidelines on diagnosis and management of acute pulmonary embo-lism. Eur Heart J. 2000;21:1301–1336.
41. Shapiro SS. Treating thrombosis in the 21st century. N Engl J Med.2003;349:1762–1764.
42. Hirsh J, Warkentin TE, Shaughnessy SG, et al. Heparin and low-molecular-weight heparin: mechanisms of action, pharmacokinetics,dosing, monitoring, efficacy, and safety. Chest. 2001;119(suppl 1):64S–94S.
43. Wells PS, Kovacs MJ, Bormanis J, et al. Expanding eligibility foroutpatient treatment of deep venous thrombosis and pulmonary em-bolism with low-molecular-weight heparin: a comparison of patientself-injection with homecare injection. Arch Intern Med. 1998;158:1809–1812.
44. Kovacs MJ, Anderson D, Morrow B, Gray L, Touchie D, Wells PS.Outpatient treatment of pulmonary embolism with dalteparin. ThrombHaemost. 2000;83:209–211.
45. Labas P, Ohradka B, Cambal M. Could deep vein thrombosis be safelytreated at home? Bratisl Lek Listy. 2001;102:458–461.
46. Beer JH, Burger M, Gretener S, Bernard-Bagattini S, Bounameaux H.Outpatient treatment of pulmonary embolism is feasible and safe in asubstantial proportion of patients. J Thromb Haemost. 2003;1:186–187.
S24 The American Journal of Medicine, Vol 120 (10B), October 2007

47. Rhodes S, Bond S, Green S, et al. Outpatient management of pulmo-nary embolism: results from the national multicentre PE study [ab-stract]. Blood. 2005;106:911.
48. Olsson CG, Bitzen U, Olsson B, et al. Outpatient tinzaparin therapy inpulmonary embolism quantified with ventilation/perfusion scintigra-phy. Med Sci Monit. 2006;12:PI9–PI3.
49. Nutescu EA, Shapiro NL, Chevalier A, Amin AN. A pharmacologicoverview of current and emerging anticoagulants. Cleve Clin J Med.2005;72(suppl 1):S2–S6.
50. Warkentin TE, Maurer B, Aster RH. Heparin-induced thrombocytopeniaassociated with fondaparinux. N Engl J Med. 2007;356:2653–2655.
51. Buller HR, Davidson BL, Decousus H, et al. Subcutaneous fondapa-rinux versus intravenous unfractionated heparin in the initial treatmentof pulmonary embolism. N Engl J Med. 2003;349:1695–1702.
52. Agnelli G, Becattini C. Clinical and economic aspects of managingvenous thromboembolism in the outpatient setting. Semin Hematol.2001;38:58–66.
53. Wells PS. Outpatient treatment of patients with deep-vein thrombosisor pulmonary embolism. Curr Opin Pulm Med. 2001;7:360–364.
54. Wells PS, Buller HR. Outpatient treatment of patients with pulmonaryembolism. Semin Vasc Med. 2001;1:229–234.
55. Segal JB, Bolger DT, Jenckes MW, et al. Outpatient therapy with lowmolecular weight heparin for the treatment of venous thromboembolism:a review of efficacy, safety, and costs. Am J Med. 2003;115:298–308.
56. Ong BS, Karr MA, Chan DK, Frankel A, Shen Q. Management ofpulmonary embolism in the home. Med J Aust. 2005;183:239 –242.
57. Wells PS, Anderson DR, Rodger MA, et al. A randomized trialcomparing 2 low-molecular-weight heparins for the outpatient treat-ment of deep vein thrombosis and pulmonary embolism. Arch InternMed. 2005;165:733–738.
58. Koopman MM, Prandoni P, Piovella F, et al, for the Tasman StudyGroup. Treatment of venous thrombosis with intravenous unfraction-ated heparin administered in the hospital as compared with subcuta-neous low-molecular-weight heparin administered at home. N EnglJ Med. 1996;334:682–687.
59. Buller H. for the MATISSE Investigators. Initial outpatient treatmentof venous thromboembolism with fondaparinux: the MATISSE tri-als. Poster presented at the Annual Meeting of The InternationalSociety on Thrombosis and Haemostasis; August 6, 2005; Sydney,Australia.
60. Aujesky D, Smith KJ, Cornuz J, Roberts MS. Cost-effectiveness oflow-molecular-weight heparin for treatment of pulmonary embolism.Chest. 2005;128:1601–1610.
61. Rodger MA, Gagne-Rodger C, Howley HE, Carrier M, Coyle D, WellsPS. The outpatient treatment of deep vein thrombosis delivers costsavings to patients and their families, compared to inpatient therapy.Thromb Res. 2003;112:13–18.
62. Buller HR, Davidson BL, Decousus H, et al. Fondaparinux orenoxaparin for the initial treatment of symptomatic deep venousthrombosis: a randomized trial. Ann Intern Med. 2004;140:867–873.
S25AlMahameed and Carman Risk Stratification in Outpatient Management of Stable Acute PE
Prevention and Management of Venous Thromboembolismin PregnancyAndra H. James, MD, MPHDepartment of Obstetrics and Gynecology, Duke University Medical Center, Durham, North Carolina, USA
ABSTRACT
Normal pregnancy is accompanied by an increase in clotting factors. The resulting hypercoagulable state haslikely evolved to protect women from hemorrhage at the time of miscarriage and childbirth. During pregnancy,women are 4 times more likely to suffer from venous thromboembolism (VTE) compared with when they arenot pregnant. Relative to pregnancy, the risk postpartum is even higher. The incidence of VTE is approximately2 per 1,000 births, and VTE accounts for 1 death per 100,000 births, or approximately 10% of all maternaldeaths. The most important risk factors during pregnancy are thrombophilia and a history of thrombosis. Ahistory of thrombosis increases the risk for VTE to 2% to 12%. Thrombophilia increases not only the risk formaternal thrombosis but also the risk of poor pregnancy outcome. Despite the increased risk for thrombosisduring pregnancy and the postpartum period, most women do not require anticoagulation. Those who do requireanticoagulation include women with current VTE, women on lifelong anticoagulation, and many women withthrombophilia or a history of thrombosis. Recommended options for anticoagulation in pregnancy are limitedto heparins, which do not cross the placenta. Low-molecular-weight heparin (LMWH) is preferred overunfractionated heparin because LMWH has a longer half-life and is presumed to have fewer side effects. Thelonger half-life is a disadvantage around the time of delivery, when unfractionated heparin, with its shorterhalf-life, is easier to manage. For women who develop or are at high risk for heparin-induced thrombocytopeniaor severe cutaneous reactions, fondaparinux is probably the agent of choice. Women who do not require lifelonganticoagulation, but require anticoagulation during pregnancy, will still require anticoagulation for the first 6weeks postpartum. © 2007 Elsevier Inc. All rights reserved.
KEYWORDS: Venous thromboembolism; Pregnancy; Deep vein thrombosis; Pulmonary embolism
Rudolf Virchow, the 19th century German pathologist, iscredited with describing the 3 factors contributing to throm-bosis—hypercoagulability, vascular injury, and stasis.1
Pregnant women are at an increased risk for venous stasis asa result of hormonally induced decreased venous capaci-tance and decreased venous outflow,2,3 possibly as a resultof mechanical obstruction by the uterus4 and questionablyas a result of decreased mobility.5-8 These factors, alongwith vascular injury,4 may have some importance, espe-cially during the postpartum period, but overall, the most
important factor contributing to the development of throm-bosis during pregnancy is hypercoagulability.
Normal pregnancy is accompanied by increased concen-trations of factors VII, VIII, X, and von Willebrand factorand by pronounced increases in fibrinogen.9 Factors II, V,and IX are relatively unchanged.9 Free protein S, the active,unbound form, is decreased during pregnancy secondary toincreased levels of its binding protein, the complementcomponent C4b.9 Plasminogen activator inhibitor (PAI)–1levels increase 5-fold.9 Levels of PAI-2, produced by theplacenta, increase dramatically during the third trimester.10
These changes, which may not return to baseline until �8weeks postpartum,9 begin with conception. So does the riskof thrombosis.11,12
The hypercoagulable state of pregnancy has likelyevolved to protect women from hemorrhage during miscar-
Please see the Conflict of Interest section at the end of this article.Requests for reprints should be addressed to Andra H. James, MD,
MPH, Division of Maternal and Fetal Medicine, Box 3967, Duke Univer-sity Medical Center Durham, North Carolina 27710.
E-mail address: [email protected]
0002-9343/$ -see front matter © 2007 Elsevier Inc. All rights reserved.doi:10.1016/j.amjmed.2007.08.011
The American Journal of Medicine (2007) Vol 120 (10B), S26–S34
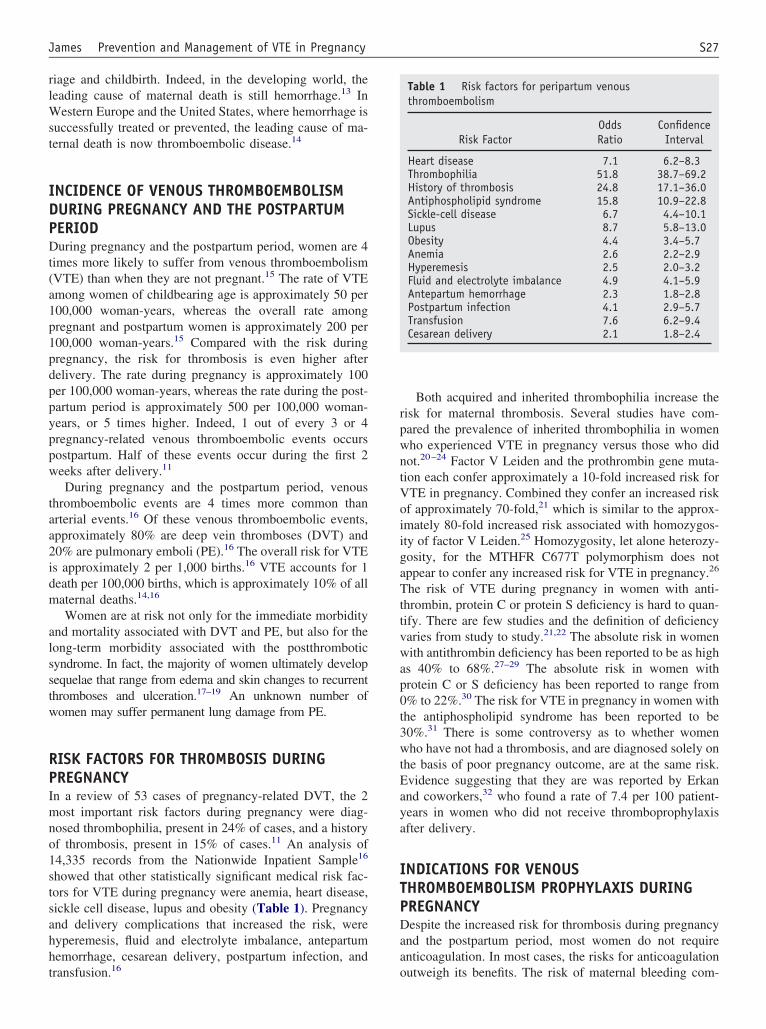
riage and childbirth. Indeed, in the developing world, theleading cause of maternal death is still hemorrhage.13 InWestern Europe and the United States, where hemorrhage issuccessfully treated or prevented, the leading cause of ma-ternal death is now thromboembolic disease.14
INCIDENCE OF VENOUS THROMBOEMBOLISMDURING PREGNANCY AND THE POSTPARTUMPERIODDuring pregnancy and the postpartum period, women are 4times more likely to suffer from venous thromboembolism(VTE) than when they are not pregnant.15 The rate of VTEamong women of childbearing age is approximately 50 per100,000 woman-years, whereas the overall rate amongpregnant and postpartum women is approximately 200 per100,000 woman-years.15 Compared with the risk duringpregnancy, the risk for thrombosis is even higher afterdelivery. The rate during pregnancy is approximately 100per 100,000 woman-years, whereas the rate during the post-partum period is approximately 500 per 100,000 woman-years, or 5 times higher. Indeed, 1 out of every 3 or 4pregnancy-related venous thromboembolic events occurspostpartum. Half of these events occur during the first 2weeks after delivery.11
During pregnancy and the postpartum period, venousthromboembolic events are 4 times more common thanarterial events.16 Of these venous thromboembolic events,approximately 80% are deep vein thromboses (DVT) and20% are pulmonary emboli (PE).16 The overall risk for VTEis approximately 2 per 1,000 births.16 VTE accounts for 1death per 100,000 births, which is approximately 10% of allmaternal deaths.14,16
Women are at risk not only for the immediate morbidityand mortality associated with DVT and PE, but also for thelong-term morbidity associated with the postthromboticsyndrome. In fact, the majority of women ultimately developsequelae that range from edema and skin changes to recurrentthromboses and ulceration.17–19 An unknown number ofwomen may suffer permanent lung damage from PE.
RISK FACTORS FOR THROMBOSIS DURINGPREGNANCYIn a review of 53 cases of pregnancy-related DVT, the 2most important risk factors during pregnancy were diag-nosed thrombophilia, present in 24% of cases, and a historyof thrombosis, present in 15% of cases.11 An analysis of14,335 records from the Nationwide Inpatient Sample16
showed that other statistically significant medical risk fac-tors for VTE during pregnancy were anemia, heart disease,sickle cell disease, lupus and obesity (Table 1). Pregnancyand delivery complications that increased the risk, werehyperemesis, fluid and electrolyte imbalance, antepartumhemorrhage, cesarean delivery, postpartum infection, andtransfusion.16
Both acquired and inherited thrombophilia increase therisk for maternal thrombosis. Several studies have com-pared the prevalence of inherited thrombophilia in womenwho experienced VTE in pregnancy versus those who didnot.20–24 Factor V Leiden and the prothrombin gene muta-tion each confer approximately a 10-fold increased risk forVTE in pregnancy. Combined they confer an increased riskof approximately 70-fold,21 which is similar to the approx-imately 80-fold increased risk associated with homozygos-ity of factor V Leiden.25 Homozygosity, let alone heterozy-gosity, for the MTHFR C677T polymorphism does notappear to confer any increased risk for VTE in pregnancy.26
The risk of VTE during pregnancy in women with anti-thrombin, protein C or protein S deficiency is hard to quan-tify. There are few studies and the definition of deficiencyvaries from study to study.21,22 The absolute risk in womenwith antithrombin deficiency has been reported to be as highas 40% to 68%.27–29 The absolute risk in women withprotein C or S deficiency has been reported to range from0% to 22%.30 The risk for VTE in pregnancy in women withthe antiphospholipid syndrome has been reported to be30%.31 There is some controversy as to whether womenwho have not had a thrombosis, and are diagnosed solely onthe basis of poor pregnancy outcome, are at the same risk.Evidence suggesting that they are was reported by Erkanand coworkers,32 who found a rate of 7.4 per 100 patient-years in women who did not receive thromboprophylaxisafter delivery.
INDICATIONS FOR VENOUSTHROMBOEMBOLISM PROPHYLAXIS DURINGPREGNANCYDespite the increased risk for thrombosis during pregnancyand the postpartum period, most women do not requireanticoagulation. In most cases, the risks for anticoagulationoutweigh its benefits. The risk of maternal bleeding com-
Table 1 Risk factors for peripartum venousthromboembolism
Risk FactorOddsRatio
ConfidenceInterval
Heart disease 7.1 6.2–8.3Thrombophilia 51.8 38.7–69.2History of thrombosis 24.8 17.1–36.0Antiphospholipid syndrome 15.8 10.9–22.8Sickle-cell disease 6.7 4.4–10.1Lupus 8.7 5.8–13.0Obesity 4.4 3.4–5.7Anemia 2.6 2.2–2.9Hyperemesis 2.5 2.0–3.2Fluid and electrolyte imbalance 4.9 4.1–5.9Antepartum hemorrhage 2.3 1.8–2.8Postpartum infection 4.1 2.9–5.7Transfusion 7.6 6.2–9.4Cesarean delivery 2.1 1.8–2.4
S27James Prevention and Management of VTE in Pregnancy

plications with heparin or low-molecular-weight heparin(LMWH) is reported to be as high as 2%.33,34 In addition tomaternal risks, anticoagulants may pose fetal risks, evenwith the use of agents that do not cross the placenta. Thereis a fine balance of hemostatic factors at the uteroplacentalinterface35 and, in most women, this balance is achievedwith the normal changes of pregnancy.
This is not necessarily true in women with a history ofthrombosis or thrombophilia. Women with a history of VTEwho receive anticoagulation have a 0% to 2% risk of arecurrent event in pregnancy,34,36,37 but women who do notreceive anticoagulation have a 2% to 12% risk.36,38,39 Be-cause pregnancy increases the risk of thrombosis 4-fold,including in women who have a history of thrombosis,40
women who are not on lifelong anticoagulation will likelyrequire anticoagulation during pregnancy, or, at a minimum,during the postpartum period. Women with a history ofrecurrent thrombosis will likely be on lifelong anticoagula-tion and will require conversion from warfarin to heparin orLMWH because of warfarin’s effects on the fetus.
Although some experts would recommend thrombopro-phylaxis for all pregnant women with inherited thrombo-philia, anticoagulation is probably not necessary if there isno personal history of thromboembolism or poor pregnancyoutcome.41 The exceptions, because of their especially highrisk for thrombosis, are women with antithrombin defi-ciency, homozygosity for the factor V Leiden mutation orthe prothrombin gene G20210A mutation, or heterozygosityfor both mutations (compound heterozygosity).42
In the antiphospholipid syndrome, an acquired thrombo-philia, several studies have demonstrated that anticoagula-tion improves the outcome of pregnancy.43 In inheritedthrombophilia, until very recently, only case reports andcase series demonstrated the role of anticoagulation in im-proving the outcome of pregnancy, but a recent randomizedtrial showed improved outcomes in women with inherited
thrombophilia and a history of a single fetal loss �10weeks’ gestation. A total of 69 of 80 women who tookenoxaparin 40 mg/day had a healthy live birth, comparedwith 23 of 80 who took low-dose aspirin.44
Although there are no large trials demonstrating thematernal or fetal benefits of anticoagulation in pregnancy,currently recommended indications include the conditionslisted below. Full-dose (adjusted dose) anticoagulation isrecommended41,45 for the prevention of VTE in womenwith a need for lifelong anticoagulation or with antiphos-pholipid syndrome with a history of thrombosis.
Full-dose (adjusted dose) or an intermediate or moderatedose, as described in Table 2, is recommended41,45 for womenwith antithrombin deficiency and women with homozygosityfor the factor V Leiden mutation, the prothrombin geneG20210A mutation or compound heterozygosity for both mu-tations.
Thromboprophylaxis with low-dose anticoagulation is rec-ommended41,46 for women with a history of unprovokedthrombosis, antiphospholipid syndrome with a history of poorpregnancy outcome as the only clinical criterion (plus use oflow-dose aspirin), or thrombophilia and poor pregnancy out-come.
Close observation (assessment of signs and symptoms ofthrombosis at routine prenatal visits) may be an option forwomen with thrombosis in the setting of transient risk factors41
or with thrombophilia but no history of thrombosis.41 None-theless, these women should be considered for thrombopro-phylaxis during the first 2 to 6 weeks postpartum.
OPTIONS FOR VENOUS THROMBOEMBOLISMPROPHYLAXIS IN PREGNANCYUnique aspects of anticoagulation in pregnancy includeboth maternal and fetal issues. During pregnancy, there is anincrease in blood volume of 40% to 50%2 and an increase in
Table 2 Protocols for thromboprophylaxis in pregnancy
Bates et al (2004)41 Duke Protocol42
Unfractionated heparinMini-dose“Low dose”
● 5,000 U sc q 12 hr ● 5,000 U sc q 12 hr � 8 wk● 7,500 U sc q 12 hr 8–28 wk● 10,000 U sc q 12 hr � 28 wk
Moderate dose“Low dose”
● q 12 hr to target anti-factor Xa level of0.1–0.3 U/mL
Adjusted dose“Full dose”
● q 12 hr to target mid-interval aPTT intherapeutic range
● q 8 or 12 hr to target mid-intervalaPTT in therapeutic range
Low-molecular-weight heparinProphylactic dose“Low dose”
● Enoxaparin 40 mg qd● Dalteparin 5,000 U qd● Tinzaparin 4,500 U qd
● Enoxaparin 40 mg qd or 30 mg bidbefore 28 wk, then
● Enoxaparin 40 mg bid after 28 wkAdjusted dose“Full dose”
● Enoxaparin 1 mg/kg bid or 1.5 mg/kg qd● Dalteparin 100 U/kg q 12 hr or 200 U/kg
q 24 hr● Tinzaparin 175 U/kg qd
● Enoxaparin 1 mg/kg bid withtarget of anti-factor Xa level of0.5–1.0
aPTT � acute partial thromboplastin time; sc � subcutaneous. Adapted from Chest41 and ACOG Practice Bulletin No. 19.45
S28 The American Journal of Medicine, Vol 120 (10B), October 2007
the volume of distribution. An increase in glomerular fil-tration2 results in increased renal excretion of drugs elimi-nated by this route. Additionally, there is an increase inprotein binding of heparin. The critical period for organo-genesis is from the 4th to the 8th week after conception.47
Because 45% of pregnancies are unintended,48 manywomen do not realize that they are pregnant. Warfarin takenduring this period is associated with a 14.6% to 56% re-ported risk for miscarriage49–55 and carries up to a 30% riskfor congenital anomalies.49–55 Placental transfer of warfarinlater in pregnancy can result in fetal bleeding55,56 or still-birth.50,52,53,57 Long-term sequelae include a 14% reportedrisk for adverse neurologic outcome and a 4% reported riskof low intelligence quotient (IQ).58
The preferred agents for anticoagulation in pregnancy areheparin compounds.41 Neither heparin59 nor LMWH59,60
crosses the placenta and both are considered safe inpregnancy.33,34 Disadvantages of unfractionated heparininclude the necessity of parenteral administration, a 2%risk for major bleeding,33 a 2% to 36% risk for reducedbone density,61– 63 a 2% risk for vertebral fracture64 anda risk for heparin-induced thrombocytopenia (HIT).41
Although the risk for HIT is low in pregnancy, and maybe lower than in nonpregnant patients,65 the actual risk isunknown.41
There are few comparative studies in pregnancy, but innonpregnant patients, LMWHs has been found to be as safeand effective as unfractionated heparin.41 Although paren-teral administration is still required, potential advantages ofLMWH over unfractionated heparin are less bleeding, amore predictable response, a lower risk for HIT, a longerhalf-life, and maybe less bone loss.41 However, in a recentlycompleted randomized trial of low-dose unfractionated hep-arin versus enoxaparin for thromboprophylaxis in preg-nancy, the incidence of clinically significant bone loss was2% to 2.5% and was no different in women who tookunfractionated heparin compared with those who took enox-aparin.63 Another study found that bone loss in women whotook LMWH was approximately 4%, no different than boneloss in controls.66 An advantage of LMWH over unfraction-ated heparin is less bruising at injection sites.67 A disadvan-tage of LMWH is that it is more expensive. Also, its longerhalf-life may be a problem at the time of delivery.
Long-term therapy with fondaparinux, the new selectivefactor Xa inhibitor, may result in less bone loss than eitherunfractionated or LMWH. In cell culture, osteoblasts havebeen shown to have significantly higher mitochondrial ac-tivity and protein synthesis when treated with fondaparinuxcompared with treatment with either unfractionated heparinor LMWH.68 Data on the use of fondaparinux in pregnancy,however, are limited. Although Lagrange et al69 observedno transplacental passage of fondaparinux using a perfusedcotyledon model, Dempfle et al70 found transplacental pas-sage of fondaparinux in 5 women who took it for 1 to 101days because of heparin allergy. Anti–factor Xa levels inumbilical cord plasma of newborns were found to be one
tenth the concentration of maternal plasma. The clinicalsignificance of this finding is unknown, but no adverseeffects were noted in the newborns.70 Fondaparinux is ef-fective in preventing VTE, but may not be effective inreducing the risk for pregnancy loss in women for whom itis prescribed for that indication, such as women with theantiphospholipid syndrome. Unlike heparin or LMWH,fondaparinux does not prevent fetal death in mice withantiphospholipid antibodies.71 At the present time there areinsufficient data to justify the routine use of fondaparinuxfor prophylaxis of VTE in pregnancy. Nonetheless,fondaparinux is probably the anticoagulant of choice incases of severe cutaneous allergies or HIT in pregnancy.70,72
INITIATING ANTICOAGULATION DURINGPREGNANCYWomen on lifelong anticoagulation may be converted fromwarfarin to LMWH before pregnancy or as soon as possibleafter conception. The problem with conversion before preg-nancy is the inconvenience and discomfort of parenteraladministration of heparins and the risks associated withtheir long-term use. The problem with conversion afterconception is that the half-life of warfarin is 36 to 42hours,73 and it may remain in the maternal circulation forseveral days, increasing the risk for miscarriage and con-genital anomalies. Only a few women are candidates forwarfarin rather than heparins during pregnancy. Candidatesinclude women with mechanical heart valves and certainother unusual conditions.
Women who are not on lifelong anticoagulation, but arecandidates for thromboprophylaxis in pregnancy, shouldstart soon after conception. An exception is women whowill be undergoing ovulation induction. Because hormonetherapy, including clomiphene, increases the risk for throm-bosis,74 these women should begin anticoagulation at thetime they start ovulation induction.
Because HIT manifests within the first 5 to 15 days ofexposure,75 platelet counts may be monitored for the first 2to 3 weeks after initiation of therapy. Although plateletcounts usually drop by 10% in pregnancy76 and thrombo-cytopenia affects up to 10% of all pregnancies,76 HIT stillmust be considered in women who develop thrombocyto-penia while taking heparins. If the diagnosis is confirmed,there are few data to guide treatment. Danaparoid has beenused most commonly to treat HIT in pregnancy,77-80 but itis not available in the United States. The use of recombinanthirudin has been reported in 1 case of HIT81 and 1 case ofheparin allergy in pregnancy.82 The use of argatroban inpregnancy has not been reported, and there are no publisheddata on placental transfer or fetal effects. Recently, the useof fondaparinux has been reported in 7 cases of heparinallergy in pregnancy.70,72,83
Anticoagulants that have been used during pregnancy aresummarized in Table 3.84-102
S29James Prevention and Management of VTE in Pregnancy
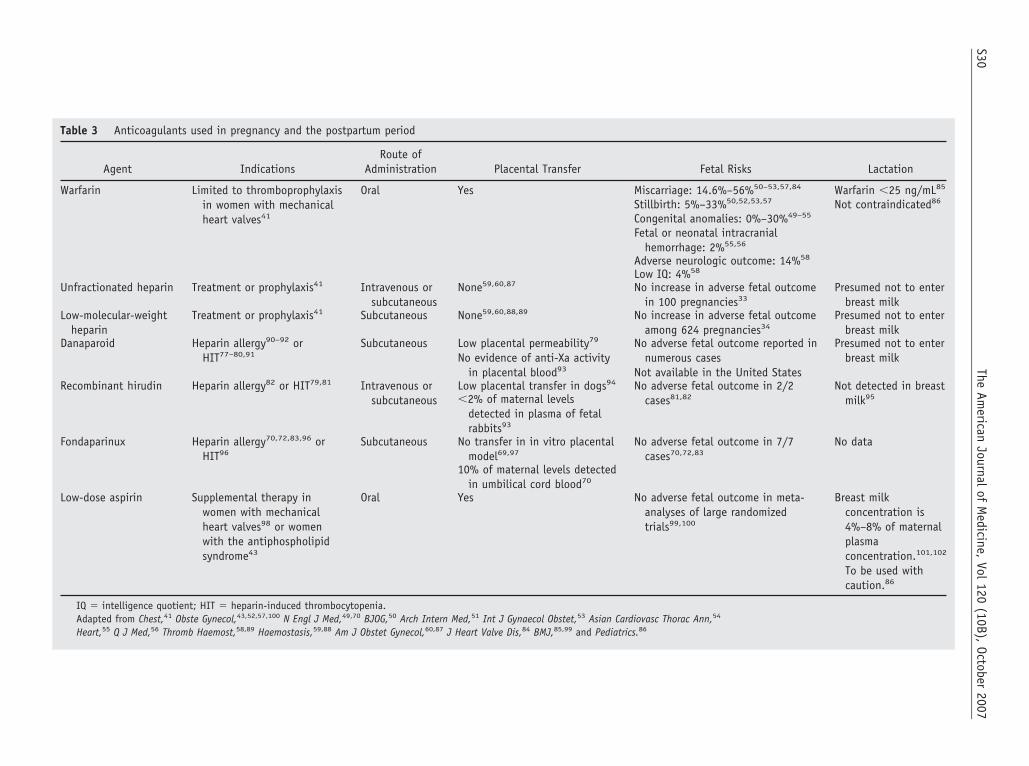
Table 3 Anticoagulants used in pregnancy and the postpartum period
Agent IndicationsRoute of
Administration Placental Transfer Fetal Risks Lactation
Warfarin Limited to thromboprophylaxisin women with mechanicalheart valves41
Oral Yes Miscarriage: 14.6%–56%50–53,57,84 Warfarin �25 ng/mL85
Stillbirth: 5%–33%50,52,53,57 Not contraindicated86
Congenital anomalies: 0%–30%49–55
Fetal or neonatal intracranialhemorrhage: 2%55,56
Adverse neurologic outcome: 14%58
Low IQ: 4%58
Unfractionated heparin Treatment or prophylaxis41 Intravenous orsubcutaneous
None59,60,87 No increase in adverse fetal outcomein 100 pregnancies33
Presumed not to enterbreast milk
Low-molecular-weightheparin
Treatment or prophylaxis41 Subcutaneous None59,60,88,89 No increase in adverse fetal outcomeamong 624 pregnancies34
Presumed not to enterbreast milk
Danaparoid Heparin allergy90–92 orHIT77–80,91
Subcutaneous Low placental permeability79
No evidence of anti-Xa activityin placental blood93
No adverse fetal outcome reported innumerous cases
Not available in the United States
Presumed not to enterbreast milk
Recombinant hirudin Heparin allergy82 or HIT79,81 Intravenous orsubcutaneous
Low placental transfer in dogs94 No adverse fetal outcome in 2/2cases81,82
Not detected in breastmilk95�2% of maternal levels
detected in plasma of fetalrabbits93
Fondaparinux Heparin allergy70,72,83,96 orHIT96
Subcutaneous No transfer in in vitro placentalmodel69,97
No adverse fetal outcome in 7/7cases70,72,83
No data
10% of maternal levels detectedin umbilical cord blood70
Low-dose aspirin Supplemental therapy inwomen with mechanicalheart valves98 or womenwith the antiphospholipidsyndrome43
Oral Yes No adverse fetal outcome in meta-analyses of large randomizedtrials99,100
Breast milkconcentration is4%–8% of maternalplasmaconcentration.101,102
To be used withcaution.86
IQ � intelligence quotient; HIT � heparin-induced thrombocytopenia.Adapted from Chest,41 Obste Gynecol,43,52,57,100 N Engl J Med,49,70 BJOG,50 Arch Intern Med,51 Int J Gynaecol Obstet,53 Asian Cardiovasc Thorac Ann,54
Heart,55 Q J Med,56 Thromb Haemost,58,89 Haemostasis,59,88 Am J Obstet Gynecol,60,87 J Heart Valve Dis,84 BMJ,85,99 and Pediatrics.86
S30The
American
Journalof
Medicine,
Vol120
(10B),October
2007

DIAGNOSIS AND MANAGEMENT OF VENOUSTHROMBOEMBOLISM DURING PREGNANCYWhen DVT occurs, it is more likely to be proximal18 andmassive18 and to be located in the left lower extremity. Intheir meta-analysis, Ray and coworkers12 reported that82.2% of DVTs occurred in the left lower extremity. Thisleft-sided predominance is associated with proximal throm-boses.103,104 Although distal thromboses are as likely tooccur on the right as on the left, proximal thrombosesoccurring under the influence of estrogen103,104 are morelikely to occur on the left. The predominance of left-sidedproximal or ileofemoral thrombosis is thought to be due toa relative stenosis of the left common iliac vein where it liesbetween the lumbar vertebral body and the right commoniliac artery,105 but the true mechanism is unknown.106 Pel-vic vein thrombosis, which accounts for �1% of all cases ofDVT,107 accounted for 11% in a series of cases amongpregnant or postpartum patients.11
The 2 most common initial symptoms, present in �80%of women with pregnancy-related DVT, are pain and swell-ing.11 When DVT is suspected, the first test recommendedis compression ultrasonography of the proximal veins.108
When results are equivocal or an iliac vein thrombosis issuspected, magnetic resonance venography (MRV) may beused.109 MRV does not carry the radiation risk of contrastvenography. The diagnosis of PE is similar to that in thenonpregnant individual. Ventilation/perfusion (V/Q) scan-ning gives relatively low radiation exposure to the fetus.109
With an indeterminate study in a woman without a DVT, aconfirmatory test, such as angiography or spiral computedtomography, is necessary to prevent the woman from un-necessary exposure to anticoagulation during pregnancy, atdelivery, or in future pregnancies.109
The initial management of VTE in pregnancy is withintravenous unfractionated heparin or subcutaneousLMWH. Pregnant women are generally admitted to thehospital. Those started on intravenous unfractionated hepa-rin are converted to LMWH before discharge. LMWH isadministered twice daily, as the half-life of LMWH isshorter in pregnancy.110-113 The shorter half-life may be dueto the higher glomerular filtration rate, greater volume ofdistribution, or placental heparinase that accompanies preg-nancy.110 Due to the shorter half-life, dosing requirementsincrease during pregnancy.110,114-116 Monitoring withmonthly anti–factor Xa levels is recommended with dosesadjusted accordingly. Thrombolysis, associated with a 6%rate of fetal loss,117 an 8% rate of maternal hemorrhage,117
and a 1% risk of maternal mortality,117 is reserved for casesof life- or limb-threatening VTE.
MANAGEMENT AT THE TIME OF DELIVERYWomen are often converted from LMWH to unfraction-ated heparin at 36 to 37 weeks of gestation or sooner ifthere is preterm labor, preeclampsia, fetal (intrauterine)growth restriction, oligohydramnios or other evidence ofimminent delivery. The purpose of converting women to
the shorter-acting unfractionated heparin has less to dowith any risk for bleeding at the time of delivery, thanwith the rare possibility of an epidural or spinal hema-toma with regional anesthesia.118 Due to this possibility,anesthesiologists will not place a regional anesthetic if awoman has received LMWH within 12 to 24 hours.Because of the benefits of regional analgesia and anes-thesia over other analgesia and anesthesia for labor anddelivery,118 every effort should be made to assure thatwomen have not received LMWH within 12 to 24 hoursof needing regional anesthesia. Because women with ahistory of VTE or thrombophilia are at an increased riskof poor pregnancy outcome, they should be delivered by39 weeks’ gestation. Depending on the risk of thrombo-sis, unfractionated heparin should be held for 6 to 24hours prior to delivery. Should a woman go into laborwhile taking unfractionated heparin, the heparin will usu-ally clear within 6 hours. Although the benefit of pneu-matic compression devices for the prevention of preg-nancy-related thrombosis has not been studied,extrapolating from perioperative data,119 the placementof pneumatic compression devices in labor or beforecesarean delivery is recommended.
POSTPARTUM MANAGEMENTPneumatic compression devices are left in place until thepatient is ambulatory and until anticoagulation is re-started after delivery. To minimize bleeding complica-tions, resumption of anticoagulation should be postponeduntil 12 hours after vaginal delivery, 12 hours after epi-dural removal, or 24 hours after cesarean delivery. Afterthe risk of postpartum hemorrhage has subsided, unless awoman prefers to remain on unfractionated heparin orLMWH, she may be bridged to warfarin for the remain-der of the 6-week postpartum period. Women who had athrombotic event during pregnancy should be continuedon warfarin for at least another 3 to 6 months afterdelivery. Women on lifelong anticoagulation will be con-tinued indefinitely. Although warfarin is contraindicatedduring pregnancy, it is not contraindicated during breast-feeding. In a study of the transfer of warfarin into breastmilk, �25 ng/mL of warfarin was detected.85 The Amer-ican Academy of Pediatrics (AAP) Committee on Drugssupports breastfeeding for women who take warfarin.86
Since there are no data about whether fondaparinuxenters breast milk, at the present time it should not beused routinely in women who are breastfeeding. It is anoption, however, for women who are not breastfeeding.Fondaparinux may be used until a woman is bridged towarfarin. For women who have to be fully anticoagulatedfor only 6 weeks postpartum, an advantage of fondapa-rinux over warfarin is that it does not require monitoring.An advantage of fondaparinux over LMWH is that itrequires only daily, as opposed to twice-daily, dosing.
S31James Prevention and Management of VTE in Pregnancy

SUMMARYDuring pregnancy and the postpartum period, women are 4times more likely to suffer from VTE than when they arenot pregnant. Relative to pregnancy, the risk is even higherpostpartum. The overall risk of VTE is approximately 2 per1,000 births. The most important risk factors during preg-nancy are thrombophilia and a history of thrombosis. De-spite the increased risk for thrombosis during pregnancy andpostpartum, most women do not require anticoagulation.Those who do include women with a current VTE, womenon lifelong anticoagulation, and many women with throm-bophilia or a history of thrombosis. Warfarin crosses theplacenta and is associated with miscarriage, congenitalanomalies, stillbirth, fetal bleeding, and poor neurologicoutcome. Therefore, recommended options for anticoagula-tion in pregnancy are limited to heparins, which do not crossthe placenta. LMWH is preferred over unfractionated hep-arin because LMWH has a longer half-life and is presumedto have fewer side effects. The longer half-life is a disad-vantage around the time of delivery when unfractionatedheparin, with its shorter half-life, is easier to manage. Forwomen who develop HIT or severe cutaneous reactions,fondaparinux is probably the agent of choice. Women whodo not require lifelong anticoagulation, but do require anti-coagulation during pregnancy, will still require anticoagu-lation for the first 6 weeks postpartum.
CONFLICT OF INTERESTAndra H. James, MD, MPH, reports no conflict of interestwith the sponsor of this supplement article or productsdiscussed in this article.
References1. Dickson B. Venous thrombosis: on the history of Virchow’s Triad.
University of Toronto Medical Journal. 2004;81:166–171.2. Gordon M. Maternal physiology in pregnancy. In: Gabbe S, Niebyl J,
Simpson J, eds. Normal and Problem Pregnancies, 4th ed. NewYork: Churchill Livingstone, 2002:63–92.
3. Macklon NS, Greer IA, Bowman AW. An ultrasound study of ges-tational and postural changes in the deep venous system of the leg inpregnancy. Br J Obstet Gynaecol. 1997;104:191–197.
4. Whitty J, Dombrowski M. Respiratory diseases in pregnancy. In:Gabbe S, Niebyl J, Simpson J, eds. Normal and Problem Pregnan-cies, 4th ed. New York,: Churchill Livingstone, 2002:1033–1064.
5. Danilenko-Dixon DR, Heit JA, Silverstein MD, et al. Risk factors fordeep vein thrombosis and pulmonary embolism during pregnancy orpost partum: a population-based, case-control study. Am J ObstetGynecol. 2001;184:104–110.
6. Carr MH, Towers CV, Eastenson AR, Pircon RA, Iriye BK, AdashekJA. Prolonged bedrest during pregnancy: does the risk of deep veinthrombosis warrant the use of routine heparin prophylaxis? J MaternFetal Med. 1997;6:264–267.
7. Kovacevich GJ, Gaich SA, Lavin JP, Hopkins MP, Crane SS, StewartJ, et al. The prevalence of thromboembolic events among womenwith extended bed rest prescribed as part of the treatment for prema-ture labor or preterm premature rupture of membranes. Am J ObstetGynecol. 2000;182:1089–1092.
8. Sikovanyecz J, Orvos H, Pal A, et al. Leiden mutation, bed rest andinfection: simultaneous triggers for maternal deep-vein thrombosisand neonatal intracranial hemorrhage? Fetal Diagn Ther. 2004;19:275–277.
9. Bremme KA. Haemostatic changes in pregnancy. Best Pract Res ClinHaematol. 2003;16:153–168.
10. Medcalf RL, Stasinopoulos SJ. The undecided serpin: the ins and outsof plasminogen activator inhibitor type 2. FEBS J. 2005;272:4858–4867.
11. James AH, Tapson VF, Goldhaber SZ. Thrombosis during pregnancyand the postpartum period. Am J Obstet Gynecol. 2005;193:216–219.
12. Ray JG, Chan WS. Deep vein thrombosis during pregnancy and thepuerperium: a meta-analysis of the period of risk and the leg ofpresentation. Obstet Gynecol Surv. 1999;54:265–271.
13. Postpartum Hemorrhage: Postpartum Hemorrhage Initiative, Officeof Health, Infectious Diseases and Nutrition, Bureau for GlobalHealth, US Agency for International Development. http://www.pphprevention.org/pph.php. Accessed September 3, 2007.
14. Chang J, Elam-Evans LD, Berg CJ, et al. Pregnancy-related mortalitysurveillance—United States, 1991–1999. MMWR Surveill Summ.2003;52:1–8.
15. Heit JA, Kobbervig CE, James AH, Petterson TM, Bailey KR, Mel-ton LJ III. Trends in the incidence of venous thromboembolismduring pregnancy or postpartum: a 30-year population-based study.Ann Intern Med. 2005;143:697–706.
16. James AH, Jamison MG, Brancazio LR, Myers ER. Venous thrombo-embolism during pregnancy and the postpartum period: incidence, riskfactors, and mortality. Am J Obstet Gynecol. 2006;194:1311–1315.
17. Bergqvist A, Bergqvist D, Lindhagen A, Matzsch T. Late symptomsafter pregnancy-related deep vein thrombosis. Br J Obstet Gynaecol.1990;97:338–341.
18. Ulander VM, Lehtola A, Kaaja R. Long-term outcome of deepvenous thrombosis during pregnancy treated with unfractionated hep-arin or low molecular weight heparin. Thrombosis Research. 2003;111:239–242.
19. Rosfors S, Noren A, Hjertberg R, Persson L, Lillthors K, Torngren S.A 16-year haemodynamic follow-up of women with pregnancy-re-lated medically treated iliofemoral deep venous thrombosis. Eur JVasc Endovasc Surg. 2001;22:448–455.
20. Grandone E, Margaglione M, Colaizzo D, D’Andrea G, Cappucci G,Brancaccio V, et al. Genetic susceptibility to pregnancy-related ve-nous thromboembolism: roles of factor V Leiden, prothrombinG20210A, and methylenetetrahydrofolate reductase C677T muta-tions. Am J Obstet Gynecol. 1998;179:1324–1328.
21. Gerhardt A, Scharf RE, Beckmann MW, et al. Prothrombin and factorV mutations in women with a history of thrombosis during pregnancyand the puerperium. N Engl J Med. 2000;342:374–380.
22. McColl MD, Ellison J, Reid F, Tait RC, Walker ID, Greer IA.Prothrombin 20210 G-- �A, MTHFR C677T mutations in womenwith venous thromboembolism associated with pregnancy. BJOG.2000;107:565–569.
23. Dilley A, Austin H, El-Jamil M, et al. Genetic factors associated withthrombosis in pregnancy in a United States population. Am J ObstetGynecol. 2000;183:1271–1277.
24. Martinelli I, De Stefano V, Taioli E, Paciaroni K, Rossi E, MannucciPM. Inherited thrombophilia and first venous thromboembolism dur-ing pregnancy and puerperium. Thromb Haemost. 2002;87:791–795.
25. Rosendaal FR, Koster T, Vandenbroucke JP, Reitsma PH. High riskof thrombosis in patients homozygous for factor V Leiden (activatedprotein C resistance). Blood. 1995;85:1504–1508.
26. Robertson L, Wu O, Langhorne P, Twaddle S, Clark P, Lowe GD, etal. Thrombophilia in pregnancy: a systematic review. Br J Haematol.2006;132:171–196.
27. Pabinger I, Schneider B, for the Gesellschaft fur Thrombose- undHamostaseforschung (GTH) Study Group on Natural Inhibitors.Thrombotic risk in hereditary antithrombin III, protein C, or proteinS deficiency: a cooperative, retrospective study. Arterioscler ThrombVasc Biol. 1996;16:742-–748.
28. Conard J, Horellou MH, Van Dreden P, Lecompte T, Samama M.Thrombosis and pregnancy in congenital deficiencies in AT III,protein C or protein S: study of 78 women. Thromb Haemost. 1990;63:319–320.
S32 The American Journal of Medicine, Vol 120 (10B), October 2007
29. Hellgren M, Tengborn L, Abildgaard U. Pregnancy in women withcongenital antithrombin III deficiency: experience of treatment withheparin and antithrombin. Gynecol Obstet Invest. 1982;14:127–141.
30. Girling J, de Swiet M. Inherited thrombophilia and pregnancy. CurrOpin Obstet Gynecol. 1998;10:135–144.
31. Krnic-Barrie S, O’Connor CR, Looney SW, Pierangeli SS, HarrisEN. A retrospective review of 61 patients with antiphospholipidsyndrome: analysis of factors influencing recurrent thrombosis. ArchIntern Med. 1997;157:2101–2108.
32. Erkan D, Merrill JT, Yazici Y, Sammaritano L, Buyon JP, LockshinMD. High thrombosis rate after fetal loss in antiphospholipid syn-drome: effective prophylaxis with aspirin. Arthritis Rheum. 2001;44:1466–1467.
33. Ginsberg JS, Kowalchuk G, Hirsh J, Brill-Edwards P, Burrows R.Heparin therapy during pregnancy: risks to the fetus and mother.Arch Intern Med. 1989;149:2233–2236.
34. Lepercq J, Conard J, Borel-Derlon A, et al. Venous thromboembo-lism during pregnancy: a retrospective study of enoxaparin safety in624 pregnancies. BJOG. 2001;108:1134–1140.
35. Roberts D, Schwartz RS. Clotting and hemorrhage in the placenta—adelicate balance. N Engl J Med. 2002;347:57–59.
36. Brill-Edwards P, Ginsberg JS, Gent M, et al, for the Recurrence ofClot in This Pregnancy Study Group. Safety of withholding heparinin pregnant women with a history of venous thromboembolism.N Engl J Med. 2000;343:1439-–1444.
37. Sanson BJ, Lensing AW, Prins MH, et al. Safety of low-molecular-weight heparin in pregnancy: a systematic review. Thromb Haemost.1999;81:668–672.
38. Pabinger I, Grafenhofer H, Kaider A, et al. Risk of pregnancy-associated recurrent venous thromboembolism in women with a his-tory of venous thrombosis. J Thromb Haemost. 2005;3:949–954.
39. De Stefano V, Martinelli I, Rossi E, et al. The risk of recurrent venousthromboembolism in pregnancy and puerperium without antithrom-botic prophylaxis. Br J Haematol. 2006;135:386–391.
40. Pabinger I, Grafenhofer H, Kyrle PA, et al. Temporary increase in therisk for recurrence during pregnancy in women with a history ofvenous thromboembolism. Blood. 2002;100:1060–1062.
41. Bates SM, Greer IA, Hirsh J, Ginsberg JS. Use of antithromboticagents during pregnancy: the Seventh ACCP Conference on Anti-thrombotic and Thrombolytic Therapy. Chest. 2004;126:627S–644S.
42. James AH, Brancazio LR, Ortel TL. Thrombosis, thrombophilia, andthromboprophylaxis in pregnancy. Clin Adv Hematol Oncol. 2005;3:187–197.
43. Branch DW, Khamashta MA. Antiphospholipid syndrome: obstetricdiagnosis, management, and controversies. Obstet Gynecol. 2003;101:1333–1344.
44. Gris JC, Mercier E, Quere I, Lavigne-Lissalde G, Cochery-NouvellonE, Hoffet M, et al. Low-molecular-weight heparin versus low-doseaspirin in women with one fetal loss and a constitutional thrombo-philic disorder. Blood. 2004;103:3695–3699.
45. American College of Obstetricians and Gynecologists. Thromboem-bolism in pregnancy. ACOG Practice Bulletin No. 19.2000ACOG-Washington, DC.
46. Lockwood CJ. Inherited thrombophilias in pregnant patients: detec-tion and treatment paradigm. Obstet Gynecol. 2002;99:333–341.
47. Moore KL. Organogenetic period: The fourth to eighth weeks. In:The Developing Human: Clinically Oriented Embryology, 6th ed.Philadelphia: WB Saunders Company; 1998:83–106.
48. Naimi TS, Lipscomb LE, Brewer RD, Gilbert BC. Binge drinking in thepreconception period and the risk of unintended pregnancy: implicationsfor women and their children. Pediatrics. 2003;111:1136–1141.
49. Iturbe-Alessio I, Fonseca MC, Mutchinik O, Santos MA, Zajarias A,Salazar E. Risks of anticoagulant therapy in pregnant women withartificial heart valves. N Engl J Med. 1986;315:1390–1393.
50. Sadler L, McCowan L, White H, Stewart A, Bracken M, North R.Pregnancy outcomes and cardiac complications in women with me-chanical, bioprosthetic and homograft valves. BJOG. 2000;107:245–253.
51. Chan WS, Anand S, Ginsberg JS. Anticoagulation of pregnantwomen with mechanical heart valves: a systematic review of theliterature. Arch Intern Med. 2000;160:191–196.
52. Nassar AH, Hobeika EM, Abd Essamad HM, Taher A, Khalil AM,Usta IM. Pregnancy outcome in women with prosthetic heart valves.Am J Obstet Gynecol. 2004;191:1009–1013.
53. Blickstein D, Blickstein I. The risk of fetal loss associated withwarfarin anticoagulation. Int J Gynaecol Obstet. 2002;78:221–225.
54. Srivastava AK, Gupta AK, Singh AV, Husain T. Effect of oralanticoagulant during pregnancy with prosthetic heart valve. AsianCardiovasc Thorac Ann. 2002;10:306–309.
55. Meschengieser SS, Fondevila CG, Santarelli MT, Lazzari MA. An-ticoagulation in pregnant women with mechanical heart valve pros-theses. Heart. 1999;82:23–26.
56. Chen WW, Chan CS, Lee PK, Wang RY, Wong VC. Pregnancy inpatients with prosthetic heart valves: an experience with 45 pregnan-cies. Q J Med. 1982;51:358–365.
57. Cotrufo M, De Feo M, De Santo LS, et al. Risk of warfarin duringpregnancy with mechanical valve prostheses. Obstet Gynecol. 2002;99:35–40.
58. Wesseling J, Van Driel D, Heymans HS, et al. Coumarins duringpregnancy: long-term effects on growth and development of school-age children. Thromb Haemost. 2001;85:609–613.
59. Harenberg J, Schneider D, Heilmann L, Wolf H. Lack of anti-factorXa activity in umbilical cord vein samples after subcutaneous admin-istration of heparin or low molecular mass heparin in pregnantwomen. Haemostasis. 1993;23:314–320.
60. Schneider D, Heilmann L, Harenberg J. Placental transfer of low-molecular weight heparin [in German]. Geburtshilfe Frauenheilkd.1995;55:93–98.
61. Dahlman TC, Sjoberg HE, Ringertz H. Bone mineral density duringlong-term prophylaxis with heparin in pregnancy. Am J Obstet Gy-necol. 1994;170:1315–1320.
62. Barbour LA, Kick SD, Steiner JF, et al. A prospective study ofheparin-induced osteoporosis in pregnancy using bone densitometry.Am J Obstet Gynecol. 1994;170:862–869.
63. Casele H, Haney EI, James A, Rosene-Montella K, Carson M. Bonedensity changes in women who receive thromboprophylaxis in preg-nancy. Am J Obstet Gynecol. 2006;195:1109–1113.
64. Dahlman TC. Osteoporotic fractures and the recurrence of thrombo-embolism during pregnancy and the puerperium in 184 women un-dergoing thromboprophylaxis with heparin. Am J Obstet Gynecol.1993;168:1265–1270.
65. Fausett MB, Vogtlander M, Lee RM, et al. Heparin-induced throm-bocytopenia is rare in pregnancy. Am J Obstet Gynecol. 2001;185:148–152.
66. Carlin AJ, Farquharson RG, Quenby SM, Topping J, Fraser WD.Prospective observational study of bone mineral density during preg-nancy: low molecular weight heparin versus control. Hum Reprod.2004;19:1211–1214.
67. Casele H, Haney E. Bruising in women undergoing thromboprophy-laxis in pregnancy [abstract]. Am J Obstet Gynecol. 2006;193:S81.
68. Matziolis G, Perka C, Disch A, Zippel H. Effects of fondaparinuxcompared with dalteparin, enoxaparin and unfractionated heparin onhuman osteoblasts. Calcif Tissue Int. 2003;73:370–379.
69. Lagrange F, Brun JL, Vergnes MC, et al. Fondaparinux sodium doesnot cross the placental barrier: study using the in-vitro human duallyperfused cotyledon model. Clin Pharmacokinet. 2002;41:47–49.
70. Dempfle CE. Minor transplacental passage of fondaparinux in vivo.N Engl J Med. 2004;350:1914–1915.
71. Girardi G, Redecha P, Salmon JE. Heparin prevents antiphospholipidantibody-induced fetal loss by inhibiting complement activation. NatMed. 2004;10:1222–1226.
72. Mazzolai L, Hohlfeld P, Spertini F, Hayoz D, Schapira M, DuchosalMA. Fondaparinux is a safe alternative in case of heparin intoleranceduring pregnancy. Blood. 2006;108:1569–1570.
73. Ansell J, Hirsh J, Poller L, Bussey H, Jacobson A, Hylek E. Thepharmacology and management of the vitamin K antagonists: the
S33James Prevention and Management of VTE in Pregnancy
Seventh ACCP Conference on Antithrombotic and ThrombolyticTherapy. Chest. 2004;126:204S–233S.
74. Stewart JA, Hamilton PJ, Murdoch AP. Thromboembolic diseaseassociated with ovarian stimulation and assisted conception tech-niques. Hum Reprod. 1997;12:2167–2173.
75. Warkentin TE, Levine MN, Hirsh J, et al. Heparin-induced throm-bocytopenia in patients treated with low-molecular-weight heparin orunfractionated heparin. N Engl J Med. 1995;332:1330–1335.
76. McCrae KR, Bussel JB, Mannucci PM, Remuzzi G, Cines DB.Platelets: an update on diagnosis and management of thrombocyto-penic disorders. Hematology (Am Soc Hematol Educ Program).2001;282:305.
77. Macchi L, Sarfati R, Guicheteau M, et al. Thromboembolic prophy-laxis with danaparoid (Orgaran) in a high-thrombosis-risk pregnantwoman with a history of heparin-induced thrombocytopenia (HIT)and Widal’s disease. Clin Appl Thromb Hemost. 2000;6:187–189.
78. Woo YL, Allard S, Cohen H, Letsky E, de Swiet M. Danaparoidthromboprophylaxis in pregnant women with heparin-induced throm-bocytopenia. BJOG. 2002;109:466–468.
79. Lindhoff-Last E, Bauersachs R. Heparin-induced thrombocytopenia-alternative anticoagulation in pregnancy and lactation. Semin ThrombHemost. 2002;28:439–446.
80. Gill J, Kovacs MJ. Successful use of danaparoid in treatment ofheparin-induced thrombocytopenia during twin pregnancy. ObstetGynecol. 1997;90:648–650.
81. Huhle G, Geberth M, Hoffmann U, Heene DL, Harenberg J. Man-agement of heparin-associated thrombocytopenia in pregnancy withsubcutaneous r-hirudin. Gynecol Obstet Invest. 2000;49:67–69.
82. Aijaz A, Nelson J, Naseer N. Management of heparin allergy inpregnancy. Am J Hematol. 2001;67:268–269.
83. Wijesiriwardana A, Lees DA, Lush C. Fondaparinux as anticoagulantin a pregnant woman with heparin allergy. Blood Coagul Fibrinoly-sis. 2006;17:147–149.
84. Vural KM, Ozatik MA, Uncu H, et al. Pregnancy after mechanicalmitral valve replacement. J Heart Valve Dis. 2003;12:370–376.
85. Orme ML, Lewis PJ, de Swiet M, et al. May mothers given warfarinbreast-feed their infants? BMJ. 1977;1:1564–1565.
86. American Academy of Pediatrics Committee on Drugs. Transfer ofdrugs and other chemicals into human milk. Pediatrics. 2001;108:776-–789.
87. Flessa HC, Kapstrom AB, Glueck HI, Will JJ. Placental transport ofheparin. Am J Obstet Gynecol. 1965;93:570–573.
88. Dimitrakakis C, Papageorgiou P, Papageorgiou I, Antzaklis A,Sakarelou N, Michalas S. Absence of transplacental passage of thelow molecular weight heparin enoxaparin. Haemostasis. 2000;30:243–248.
89. Melissari E, Parker CJ, Wilson NV, Monte G, Kanthou C, PembertonKD, et al. Use of low molecular weight heparin in pregnancy.Thromb Haemost. 1992;68:652–656.
90. Taylor AA. Successful use of heparinoids in a pregnancy complicatedby allergy to heparin. BJOG. 2001;108:1011–1012.
91. de Saint-Blanquat L, Simon L, Toubas MF, Hamza J. Treatment withdanaparoid during pregnancy for a woman with a cutenous allergy tolow-molecular-weight heparin [in French]. Ann Fr Anesth Reanim.2000;19:751-–754.
92. Myers B, Westby J, Strong J. Prophylactic use of danaparoid inhigh-risk pregnancy with heparin-induced thrombocytopaenia-posi-tive skin reaction. Blood Coagul Fibrinolysis. 2003;14:485–487.
93. Dager WE, White RH. Treatment of heparin-induced thrombocyto-penia. Ann Pharmacother. 2002;36:489–503.
94. Markwardt F, Fink G, Kaiser B, Klocking HP, Nowak G, Richter M,et al. Pharmacological survey of recombinant hirudin. Pharmazie.1988;43:202–207.
95. Lindhoff-Last E, Willeke A, Thalhammer C, Nowak G, BauersachsR. Hirudin treatment in a breastfeeding woman. Lancet. 2000;355:467–468.
96. Parody R, Oliver A, Souto JC, Fontcuberta J. Fondaparinux (ARIX-TRA) as an alternative anti-thrombotic prophylaxis when there is
hypersensitivity to low molecular weight and unfractionatedheparins. Haematologica. 2003;88:147–148.
97. Lagrange F, Vergnes C, Brun JL, et al. Absence of placental transferof pentasaccharide (Fondaparinux, Arixtra) in the dually perfusedhuman cotyledon in vitro. Thromb Haemost. 2002;87:831–835.
98. Rowan JA, McCowan LM, Raudkivi PJ, North RA. Enoxaparintreatment in women with mechanical heart valves during pregnancy.Am J Obstet Gynecol. 2001;185:633–637.
99. Duley L, Henderson-Smart D, Knight M, King J. Antiplatelet drugsfor prevention of pre-eclampsia and its consequences: systematicreview. BMJ. 2001;322:329–333.
100. Coomarasamy A, Honest H, Papaioannou S, Gee H, Khan KS.Aspirin for prevention of preeclampsia in women with historical riskfactors: a systematic review. Obstet Gynecol. 2003;101:1319–1332.
101. Bailey DN, Weibert RT, Naylor AJ, Shaw RF. A study of salicylateand caffeine excretion in the breast milk of two nursing mothers. JAnal Toxicol. 1982;6:64–68.
102. Findlay JW, DeAngelis RL, Kearney MF, Welch RM, Findlay JM.Analgesic drugs in breast milk and plasma. Clin Pharmacol Ther.1981;29:625–633.
103. Kierkegaard A. Side and site of deep vein thrombosis in women usingoral contraceptives. Acta Obstet Gynecol Scand. 1985;64:399–402.
104. Kierkegaard A. Deep vein thrombosis and the oestrogen content inoral contraceptives: an epidemiological analysis. Contraception.1985;31:29–41.
105. Cockett FB, Thomas ML. The iliac compression syndrome. Br JSurg. 1965;52:816–821.
106. Ginsberg JS, Brill-Edwards P, Burrows RF, et al. Venous thrombosisduring pregnancy: leg and trimester of presentation. Thromb Hae-most. 1992;67:519–520.
107. Goldhaber SZ, Tapson VF. A prospective registry of 5,451 patientswith ultrasound-confirmed deep vein thrombosis. Am J Cardiol.2004;93:259–262.
108. Bates SM, Ginsberg JS. How we manage venous thromboembolismduring pregnancy. Blood. 2002;100:3470–3478.
109. Schafer AI, Levine MN, Konkle BA, Kearon C. Thrombotic disor-ders: diagnosis and treatment. Hematology (Am Soc Hematol EducProgram). 2003;X:520-–539.
110. Barbour LA, Oja JL, Schultz LK. A prospective trial that demon-strates that dalteparin requirements increase in pregnancy to maintaintherapeutic levels of anticoagulation. Am J Obstet Gynecol. 2004;191:1024–1029.
111. Casele HL, Laifer SA, Woelkers DA, Venkataramanan R. Changes inthe pharmacokinetics of the low-molecular-weight heparin enoxaparinsodium during pregnancy. Am J Obstet Gynecol. 1999;181:1113–1117.
112. Blomback M, Bremme K, Hellgren M, Lindberg H. A pharmacoki-netic study of dalteparin (Fragmin) during late pregnancy. BloodCoagul Fibrinolysis. 1998;9:343–350.
113. Brancazio LR, Roperti KA, Stierer R, Laifer SA. Pharmacokinetics andpharmacodynamics of subcutaneous heparin during the early third tri-mester of pregnancy. Am J Obstet Gynecol. 1995;173:1240–1245.
114. Jacobsen AF, Qvigstad E, Sandset PM. Low molecular weight hep-arin (dalteparin) for the treatment of venous thromboembolism inpregnancy. BJOG. 2003;110:139–144.
115. Sephton V, Farquharson RG, Topping J, et al. A longitudinal study ofmaternal dose response to low molecular weight heparin in preg-nancy. Obstet Gynecol. 2003;101:1307–1311.
116. Smith MP, Norris LA, Steer PJ, Savidge GF, Bonnar J. Tinzaparinsodium for thrombosis treatment and prevention during pregnancy.Am J Obstet Gynecol. 2004;190:495–501.
117. Turrentine MA, Braems G, Ramirez MM. Use of thrombolytics forthe treatment of thromboembolic disease during pregnancy. ObstetGynecol Surv. 1995;50:534–541.
118. Horlocker TT. Low molecular weight heparin and neuraxial anesthe-sia. Thromb Res. 2001;101:141–154.
119. Baker WH, Mahler DK, Foldes MS, et al. Pneumatic compressiondevices for prophylaxis of deep venous thrombosis (DVT). Am Surg.1986;52:371–373.
S34 The American Journal of Medicine, Vol 120 (10B), October 2007
The Pharmacoeconomics of Deep Vein ThrombosisTreatmentAndrew F. Shorr, MD, MPHPulmonary and Critical Care Medicine Service, Washington Hospital Center, Washington, DC, USA
ABSTRACT
Venous thromboembolism (VTE), encompassing both deep vein thrombosis (DVT) and pulmonaryembolism, remains a common and costly condition that is associated with significant morbidity andmortality. Treatment options for initial management of DVT include unfractionated heparin (UFH),low-molecular-weight heparins (LMWHs), and fondaparinux, which is the first of a new class of pen-tasaccharide antithrombotic agents with anti–factor Xa activity. LMWHs are an important tool in DVTmanagement, offering advantages over UFH such as ease of dosing, lack of need for coagulationmonitoring, and reduced risk for heparin-induced thrombocytopenia (HIT). Fondaparinux is also charac-terized by a simple dosing regimen, no need for coagulation monitoring, and potentially a lower risk of HITcompared with LMWH. In a recent clinical trial of DVT management, efficacy and bleeding rates withfondaparinux appeared similar to those observed with LMWH. In contrast to LMWH, fondaparinux isgenerally given as a fixed dose across a range of patient weights rather than calculated per individualpatient weight. Given the increasing economic burden of VTE, particularly due to its increased rate amongthe elderly, pharmacoeconomic analyses have become a particularly useful tool to aid in selecting amongsimilarly effective and safe agents for VTE treatment. A recent cost-effective analysis demonstrated thatfondaparinux use offers an attractive economic alternative to other agents for initial DVT therapy thatcould yield cost savings without compromising clinical outcomes or patient safety. © 2007 Elsevier Inc.All rights reserved.
KEYWORDS: Anticoagulation; Deep vein thrombosis; Pharmacoeconomics; Venous thromboembolism
Venous thromboembolism (VTE), encompassing both deepvein thrombosis (DVT) and pulmonary embolism (PE),remains a common condition in the United States. Moreimportant, VTE is associated with significant morbidity andmortality. Reflecting this, VTE is responsible for approxi-mately 250,000 hospitalizations in the United States eachyear.1 Of the �200,000 new cases of VTE that occur an-nually, 20% of persons with an acute PE present withsudden death and 30% of those with other VTE syndromesdie within the subsequent 30 days. Survivors face an ap-proximately 30% risk for recurrent VTE over the next 10years.
Limited data exist regarding the economic burden ofVTE. Published estimates suggest that the direct costs ofVTE approach $3 to $4 billion annually.2,3 These estimatesdo not reflect the additional indirect cost of lost workdaysand productivity that often accompany a VTE diagnosis.2
Furthermore, a number of other so-called “hidden” costconsiderations arise in relation to VTE and its treatment.Depending on the anticoagulant agent used for VTE ther-apy, there are additional costs potentially associated withtherapeutic monitoring and with the agents used to reversethe pharmacologic effect in the event of overanticoagulation(e.g., protamine for overanticoagulation with unfractionatedheparin [UFH]). Furthermore, management of potential sideeffects of anticoagulants, including bleeding and heparin-induced thrombocytopenia (HIT) are expensive.4,5 Finally,the costs related to long-term complications of VTE, includ-ing clot recurrence and postthrombotic syndrome, can ac-
Please see the Conflict of Interest section at the end of this article.Requests for reprints should be addressed to Andrew F. Shorr, MD,
MPH, Pulmonary and Critical Care Medicine Service,Washington HospitalCenter, 110 Irving Street NW, Washington, District of Columbia 20010.
E-mail address: [email protected].
0002-9343/$ -see front matter © 2007 Elsevier Inc. All rights reserved.doi:10.1016/j.amjmed.2007.08.012
The American Journal of Medicine (2007) Vol 120 (10B), S35–S41
count for up to approximately 75% of the overall costs oftreating the primary event.6
Although there have been many advances in VTE diag-nosis and management, the primary goals of anticoagulationtherapy in the treatment of DVT remain the same: to preventclot propagation and recurrence.7 Presently, treatment op-tions for initial management of DVT include UFH, low-molecular-weight heparins (LMWHs), and fondaparinux,which is the first of a new class of pentasaccharide anti-thrombotic agents with anti–factor Xa activity. Since theiradvent in the 1980s, LMWHs have evolved as an importanttool in DVT management. LMWHs offer advantages overUFH, which include ease of dosing, no need for coagulationmonitoring, and a reduced risk for HIT.4,5,7,8 In addition,clinical trials and various meta-analyses indicate thatLMWHs are either equivalent or superior to UFH withrespect to efficacy for initial treatment of VTE.9,10 LMWHsmay also reduce bleeding complications when comparedwith UFH. Because of these attributes, LMWHs have beenshown to be cost-effective for DVT therapy when comparedwith UFH.11,12
Similar to LMWHs, fondaparinux use is characterized bya simple dosing regimen and does not require coagulationmonitoring.8 In addition, the risk of HIT is potentially lowerwith fondaparinux compared with both UFH and LMWH.13
Fondaparinux prevents thrombus formation by selectivelybinding to the pentasaccharide binding site on antithrombinIII and enhancing its inactivation of factor Xa, with a re-sultant decrease in thrombin generation.14 In a recent clin-ical trial of DVT management, efficacy and bleeding rateswith fondaparinux appeared similar to those observed withLMWH.15 In contrast to LMWHs, fondaparinux is gener-ally given as a fixed dose across a range of patient weightsrather than calculated per individual patient weight.
When selecting an anticoagulant for use either in anindividual patient or adoption in a healthcare system, clini-cians and healthcare policy makers must consider a numberof factors. In the absence of data indicating that a particularagent is superior to others in terms of efficacy, cost andimplementation concerns become important. Economicanalyses, therefore, are particularly useful when weighinganticoagulant options for DVT management.
To facilitate this process, it is necessary to review recentclinical and pharmacoeconomic data comparing fondapa-rinux with enoxaparin for the treatment of VTE and DVT.Additionally, it is important to evaluate factors that mayaffect the relative financial consequences of different ap-proaches to DVT therapy.
EFFICACY OF FONDAPARINUX VERSUSENOXAPARIN FOR DEEP VEIN THROMBOSISTREATMENTIn a recent randomized, multicenter, double-blind clinical trialMondial Assessment of Thromboembolism Treatment Initi-ated by Synthetic Pentasaccharide With Symptomatic End-points-Deep Vein Thrombosis (MATISSE-DVT), Buller and
associates15 determined that once-daily subcutaneousfondaparinux was at least as effective and as safe as twice-daily, body-weight–adjusted enoxaparin in the initial treat-ment of patients with symptomatic DVT. A total of 2,205patients with acute symptomatic DVT were randomized totreatment with either fondaparinux once-daily subcutane-ously dosed by weight category: 5.0 mg (body weight �50kg), 7.5 mg (body weight 50–100 kg), and 10 mg (bodyweight �100 kg), or enoxaparin 1 mg/kg of body weight,subcutaneously dosed twice daily. Treatment was continuedfor �5 days and until vitamin K antagonists induced aninternational normalized ratio �2.0 for 2 consecutive days.Patients excluded from this study included those with symp-tomatic PE, a contraindication for anticoagulation, or ele-vated serum creatinine levels (�2 mg/dL).
A total of 43 (3.9%) patients randomly assigned tofondaparinux and 45 (4.1%) patients randomly assigned toenoxaparin experienced symptomatic recurrent VTE duringthe 3-month study period (absolute difference, �0.15 per-centage points [95% confidence interval (CI), �1.8 to1.5]), indicating comparable efficacy between the 2agents (Figure 1).15 The incidence of major bleedingduring initial treatment was also similar between thetreatment groups, occurring in 12 (1.1%) patients receiv-ing fondaparinux and 13 (1.2%) patients receiving enox-aparin (absolute difference, �0.1 percentage points [95%CI, �1.0 to 0.8]) (Figure 1). Bleeding contributed to deathin 2 patients in the fondaparinux group. Mortality ratesduring the 3-month study period were 3.8% and 3.0% in thefondaparinux and enoxaparin groups, respectively (absolutedifference, 0.8 percentage points [95% CI, �0.8 to 2.3]).Subgroup analysis indicated that both treatment groups hadsimilar efficacy and safety independent of body weight.Also, among the approximately 33% of patients in eachgroup who received some or all of their initial treatment athome, the incidence of clinical outcomes was low andsimilar in each group.
COST-EFFECTIVENESS OF FONDAPARINUXVERSUS ENOXAPARIN FOR DEEP VEINTHROMBOSIS TREATMENTA recent cost-effective analysis determined that use offondaparinux for initial DVT therapy may offer substantialcost savings relative to enoxaparin from a healthcare systemperspective.16 The researchers created a decision model thatevaluated a cohort of 1,000 hypothetical subjects with acuteDVT who required injectable DVT treatment for 5 days(with once-daily enoxaparin 1.5 mg/kg or once-dailyfondaparinux 7.5 mg). Estimates for model inputs werecreated based on values identified in a review of the litera-ture and a meta-analysis of bleeding rates across the VTEtrials with fondaparinux (Table 1).13,15–22 Incremental costsfor DVT therapy and the economic outcomes of the com-plications associated with DVT management served as theprimary end point. The authors purposefully biased themodel against fondaparinux. This was achieved through
S36 The American Journal of Medicine, Vol 120 (10B), October 2007
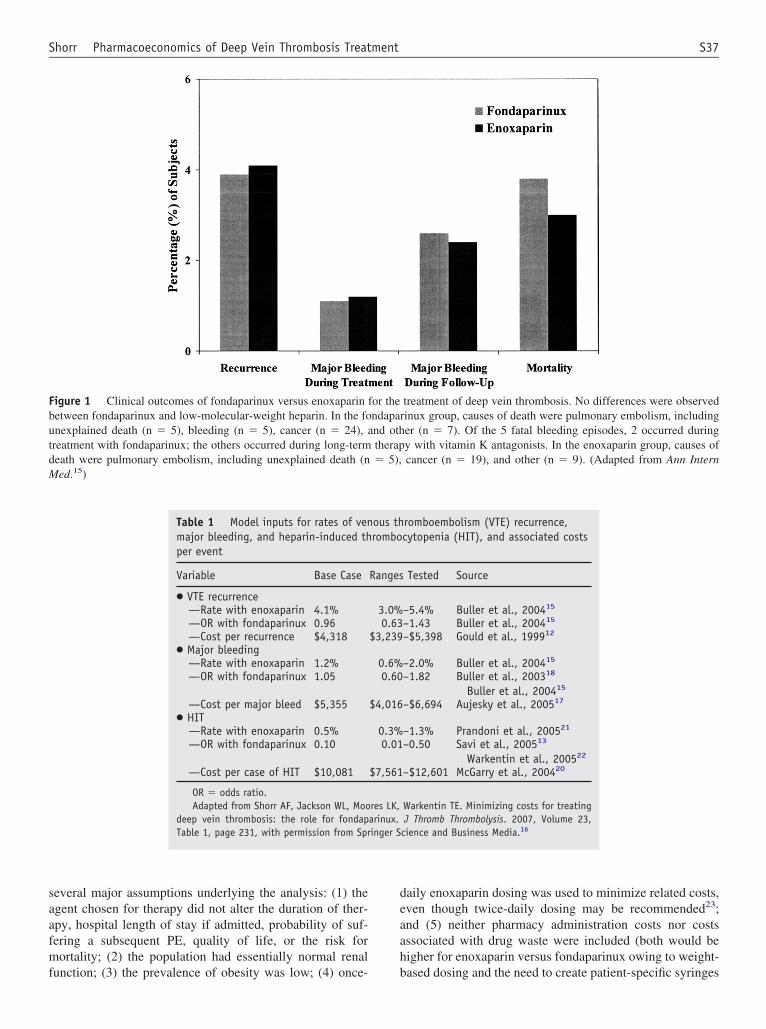
several major assumptions underlying the analysis: (1) theagent chosen for therapy did not alter the duration of ther-apy, hospital length of stay if admitted, probability of suf-fering a subsequent PE, quality of life, or the risk formortality; (2) the population had essentially normal renalfunction; (3) the prevalence of obesity was low; (4) once-
daily enoxaparin dosing was used to minimize related costs,even though twice-daily dosing may be recommended23;and (5) neither pharmacy administration costs nor costsassociated with drug waste were included (both would behigher for enoxaparin versus fondaparinux owing to weight-based dosing and the need to create patient-specific syringes
Figure 1 Clinical outcomes of fondaparinux versus enoxaparin for the treatment of deep vein thrombosis. No differences were observedbetween fondaparinux and low-molecular-weight heparin. In the fondaparinux group, causes of death were pulmonary embolism, includingunexplained death (n � 5), bleeding (n � 5), cancer (n � 24), and other (n � 7). Of the 5 fatal bleeding episodes, 2 occurred duringtreatment with fondaparinux; the others occurred during long-term therapy with vitamin K antagonists. In the enoxaparin group, causes ofdeath were pulmonary embolism, including unexplained death (n � 5), cancer (n � 19), and other (n � 9). (Adapted from Ann InternMed.15)
Table 1 Model inputs for rates of venous thromboembolism (VTE) recurrence,major bleeding, and heparin-induced thrombocytopenia (HIT), and associated costsper event
Variable Base Case Ranges Tested Source
● VTE recurrence—Rate with enoxaparin 4.1% 3.0%–5.4% Buller et al., 200415
—OR with fondaparinux 0.96 0.63–1.43 Buller et al., 200415
—Cost per recurrence $4,318 $3,239–$5,398 Gould et al., 199912
● Major bleeding—Rate with enoxaparin 1.2% 0.6%–2.0% Buller et al., 200415
—OR with fondaparinux 1.05 0.60–1.82 Buller et al., 200318
Buller et al., 200415
—Cost per major bleed $5,355 $4,016–$6,694 Aujesky et al., 200517
● HIT—Rate with enoxaparin 0.5% 0.3%–1.3% Prandoni et al., 200521
—OR with fondaparinux 0.10 0.01–0.50 Savi et al., 200513
Warkentin et al., 200522
—Cost per case of HIT $10,081 $7,561–$12,601 McGarry et al., 200420
OR � odds ratio.Adapted from Shorr AF, Jackson WL, Moores LK, Warkentin TE. Minimizing costs for treating
deep vein thrombosis: the role for fondaparinux. J Thromb Thrombolysis. 2007, Volume 23,Table 1, page 231, with permission from Springer Science and Business Media.16
S37Shorr Pharmacoeconomics of Deep Vein Thrombosis Treatment
of enoxaparin). In addition, it was assumed that the devel-opment of HIT did not increase the risk for death or signif-icantly decrease quality of life. By limiting the potentialclinical consequences of HIT and because HIT should notoccur with fondaparinux,13 the model favored enoxaparin.16
Multiple sensitivity analyses were conducted to assessthe impact of the assumptions. To evaluate the overalluncertainty in the model and to generate 95% CIs aroundthe estimated cost differential, the authors performed aMonte Carlo simulation.16 The analysis made 2 additionalassumptions: (1) the base-case patient weight was 80 kg and(2) the base-case cost of acquisition was $96 and $50 forenoxaparin and fondaparinux, respectively. Model inputsfor rates of VTE recurrence, major bleeding, and HIT, aswell as the costs associated with these events are listed inTable 1.
Results of the base-case analysis are summarized inTable 2. Total costs per patient treated associated with theuse of fondaparinux were $472 compared with $769 withuse of enoxaparin.16 This difference resulted in a 40%reduction in composite system costs. Drug acquisition costwas the major driver of overall costs. Univariate sensitivityanalysis indicated that the model was mildly sensitive to thecosts of the agents, particularly enoxaparin, and to patientweight (Figure 2). The 95% CI around the overall costdifference per patient ranged from $48 to $401, favoringcost savings with fondaparinux. Break-even analysis indi-cated the findings to be robust over a wide range of likelyclinical scenarios.
DOSING AND OTHER CONSIDERATIONS:POTENTIAL COST IMPACT ON CHOICE OF DEEPVEIN THROMBOSIS THERAPYSeveral considerations, in addition to those addressed in thiscost analysis, can substantially affect the relative costs as-sociated with different approaches to DVT therapy. Oneimportant consideration is dosing regimen differences be-tween agents. For VTE treatment fondaparinux is dosedonce daily by subcutaneous injection based on patientweight category: 5 mg (body weight �50 kg), 7.5 mg (bodyweight 50–100 kg), or 10 mg (body weight �100 kg).24
Data from the MATISSE-DVT trial and a post-hoc analysisof data from obese and nonobese patients in both theMATISSE-DVT and MATISSE-PE trials demonstrate thatefficacy and safety outcomes remained comparable betweenfondaparinux dosed once daily based on weight categoryversus either LMWH or UFH regardless of body weight (upto 217 kg) or body mass index (BMI; up to 80).25
Enoxaparin dosing for VTE treatment is based directlyon the patient’s weight and, unlike fondaparinux, is indi-cated for inhospital treatment for patients with acute DVT(with or without PE) and outpatient treatment for acuteDVT only (without PE).26 The approved enoxaparin regi-mens are: 1 mg/kg twice daily or 1.5 mg/kg once daily forinpatients, and 1 mg/kg twice daily for outpatient treatmentof DVT. Notably, results of a controlled trial of enoxaparin
versus UFH for treatment of VTE suggested reduced effi-cacy in obese patients (BMI �27) with a once-daily (1.5mg/kg) versus twice-daily (1 mg/kg) enoxaparin regimen(VTE recurrence rates: 7.3% vs. 3.4%, respectively).23 Likeenoxaparin, the LMWH tinzaparin is dosed by specificpatient weight: 175 IU/kg subcutaneously once daily.27 Thefollowing calculation is required to determine the correctvolume to be withdrawn from the 20,000 IU/mL vial withan appropriately calibrated syringe for the correct dose:patient weight (in kilograms) � 0.00875 mL/kg � volume(milliliters) to be administered.
These dose regimen differences among the various anti-coagulant agents have significant cost implications for VTEmanagement. Since fondaparinux is dosed based on weightcategory with prefilled syringes available in the exact dosesneeded (5 mg, 7.5 mg, and 10 mg doses), drug waste isavoided. Furthermore, pharmacy administration costs areminimized because dosing is once daily and no pharmacisttime is needed for syringe preparation. A simplified regimenand once-daily dosing also promote outpatient therapy withfondaparinux, which can drastically reduce costs from ahealthcare system perspective. This nearly 1-size-fits-allaspect of fondaparinux also enhances patient safety as itminimizes the chance that a patient will receive an overdosebecause of an error made during syringe preparation. Incontrast, enoxaparin dosing is subject to drug waste andhigher pharmacy administration costs relative to fondapa-rinux because it is dosed based on patient weight. Forexample, doses for odd weights do not readily fall within therange for prefilled enoxaparin syringes, resulting in waste ofpart of the premeasured dose and requiring additional phar-macy time to prepare the syringe. Also, doses �150 mgmust be prepared from a multidose vial. Twice-daily dosing(indicated for outpatients and, possibly, obese patients) alsoincreases pharmacy administration costs. These issues mayalso complicate outpatient treatment with enoxaparin ortinzaparin because many patients may have limited capabil-ity to titrate prefilled syringes or withdraw dosages frommultidose vials.15
As the investigators of the abovementioned cost analysisobserved, their analysis likely underplayed the cost impli-cations of enoxaparin’s weight-based dosing, given theirassumptions of no drug waste, little obesity, and once-dailyenoxaparin dosing.16 Particularly noteworthy is the risingincidence of obesity in the United States, which currentlyaffects approximately 33% of the adult population and hasa direct impact on the cost of specific weight-based medi-cations such as enoxaparin.16,28
While playing only a minor role in determining theoverall financial outcomes of DVT management, the differ-ence in risk of HIT between fondaparinux and enoxaparin ispotentially clinically meaningful. LMWH is associated witha much lower prevalence of HIT versus UFH (0% to 0.8%vs. 1% to 5%, respectively).29 Use of fondaparinux, how-ever, should theoretically be completely devoid of a risk forHIT. The absence of HIT with fondaparinux relates to its
S38 The American Journal of Medicine, Vol 120 (10B), October 2007
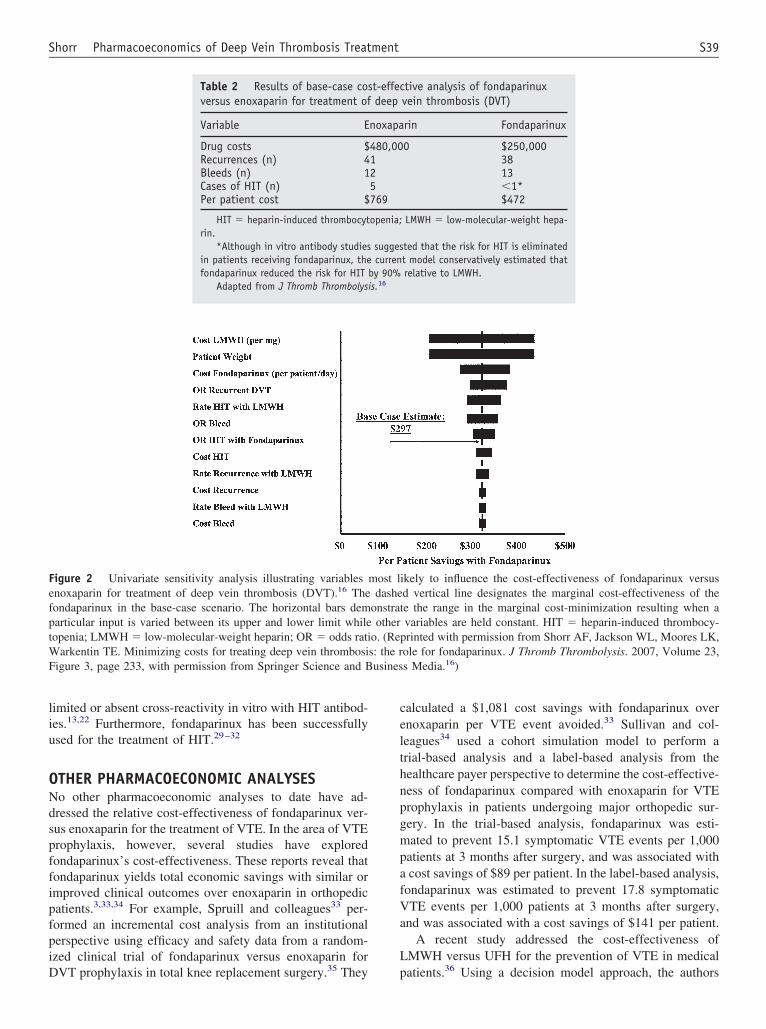
limited or absent cross-reactivity in vitro with HIT antibod-ies.13,22 Furthermore, fondaparinux has been successfullyused for the treatment of HIT.29–32
OTHER PHARMACOECONOMIC ANALYSESNo other pharmacoeconomic analyses to date have ad-dressed the relative cost-effectiveness of fondaparinux ver-sus enoxaparin for the treatment of VTE. In the area of VTEprophylaxis, however, several studies have exploredfondaparinux’s cost-effectiveness. These reports reveal thatfondaparinux yields total economic savings with similar orimproved clinical outcomes over enoxaparin in orthopedicpatients.3,33,34 For example, Spruill and colleagues33 per-formed an incremental cost analysis from an institutionalperspective using efficacy and safety data from a random-ized clinical trial of fondaparinux versus enoxaparin forDVT prophylaxis in total knee replacement surgery.35 They
calculated a $1,081 cost savings with fondaparinux overenoxaparin per VTE event avoided.33 Sullivan and col-leagues34 used a cohort simulation model to perform atrial-based analysis and a label-based analysis from thehealthcare payer perspective to determine the cost-effective-ness of fondaparinux compared with enoxaparin for VTEprophylaxis in patients undergoing major orthopedic sur-gery. In the trial-based analysis, fondaparinux was esti-mated to prevent 15.1 symptomatic VTE events per 1,000patients at 3 months after surgery, and was associated witha cost savings of $89 per patient. In the label-based analysis,fondaparinux was estimated to prevent 17.8 symptomaticVTE events per 1,000 patients at 3 months after surgery,and was associated with a cost savings of $141 per patient.
A recent study addressed the cost-effectiveness ofLMWH versus UFH for the prevention of VTE in medicalpatients.36 Using a decision model approach, the authors
Figure 2 Univariate sensitivity analysis illustrating variables most likely to influence the cost-effectiveness of fondaparinux versusenoxaparin for treatment of deep vein thrombosis (DVT).16 The dashed vertical line designates the marginal cost-effectiveness of thefondaparinux in the base-case scenario. The horizontal bars demonstrate the range in the marginal cost-minimization resulting when aparticular input is varied between its upper and lower limit while other variables are held constant. HIT � heparin-induced thrombocy-topenia; LMWH � low-molecular-weight heparin; OR � odds ratio. (Reprinted with permission from Shorr AF, Jackson WL, Moores LK,Warkentin TE. Minimizing costs for treating deep vein thrombosis: the role for fondaparinux. J Thromb Thrombolysis. 2007, Volume 23,Figure 3, page 233, with permission from Springer Science and Business Media.16)
Table 2 Results of base-case cost-effective analysis of fondaparinuxversus enoxaparin for treatment of deep vein thrombosis (DVT)
Variable Enoxaparin Fondaparinux
Drug costs $480,000 $250,000Recurrences (n) 41 38Bleeds (n) 12 13Cases of HIT (n) 5 �1*Per patient cost $769 $472
HIT � heparin-induced thrombocytopenia; LMWH � low-molecular-weight hepa-rin.
*Although in vitro antibody studies suggested that the risk for HIT is eliminatedin patients receiving fondaparinux, the current model conservatively estimated thatfondaparinux reduced the risk for HIT by 90% relative to LMWH.
Adapted from J Thromb Thrombolysis.16
S39Shorr Pharmacoeconomics of Deep Vein Thrombosis Treatment

concluded that despite higher acquisition costs, the use ofLMWH in hospitalized patients was cost-saving, primarilydue to the lower rate of HIT associated with the use ofLMWH. According to this analysis, routine use of LMWHwould save approximately $89 per patient (95% CI, $7 to$373). No cost-effective analyses evaluating the use offondaparinux for VTE prevention in medically ill patientshave been reported.
No studies have directly addressed the cost-effectivenessof fondaparinux versus UFH for the management of VTE.However, a number of cost-effective analyses, includingone based on a meta-analysis of randomized trials ofLMWH versus UFH for the treatment of DVT, have dem-onstrated the economic superiority of LMWH over UFH forthis indication.11,12,37 Based on available pharmacoeco-nomic and clinical data, therefore, it would seem reasonableto conclude that fondaparinux for VTE management wouldlikely result in significant cost savings over UFH as well.Furthermore, most economic comparisons have used enox-aparin as the representative LMWH. Given the varying costof different LMWHs, it is unclear how the findings fromcost studies evaluating enoxaparin might differ if a lessexpensive LMWH were used as the alternative strategy.
SUMMARYVTE and its subsequent management remain costly irre-spective of whether it arises de novo or as a complication ofsurgery or hospitalization. New options for VTE therapyand prevention are available that offer at least comparableefficacy and safety to standard agents, as well as dosing andconvenience advantages that may translate into enhancedsavings. Given the increasing economic burden of VTE,particularly due to its increased rate among the elderly,38
pharmacoeconomic analyses have become a particularlyuseful tool to aid in selecting among similarly effective andsafe agents for VTE treatment. A recent cost-effective anal-ysis demonstrated that fondaparinux use offers an attractiveeconomic alternative to other agents for initial DVT therapythat could yield cost savings without compromising clinicaloutcomes or patient safety.
CONFLICT OF INTERESTThe author reports the following conflicts of interest withthe sponsor of this supplement article or products discussedin this article. Andrew F. Shorr, MD, MPH, has served as amember of the Speakers’ Bureau for GlaxoSmithKline andsanofi-aventis; has served as a consultant/advisory boardmember for GlaxoSmithKline and sanofi-aventis; and hasreceived research/grant support from GlaxoSmithKline andsanofi-aventis.
References1. Thom T, Haase N, Rosamond W, et al. Heart disease and stroke
statistics—2006 update: a report from the American Heart AssociationStatistics Committee and Stroke Statistics Subcommittee. Circulation.2006;113:e85–e151.
2. de Lissovoy G. Economic issues in the treatment and prevention ofdeep vein thrombosis from a managed care perspective. Am J ManagCare. 2001;7(suppl 17):S535–S538.
3. Dranitsaris G, Kahn SR, Stumpo C, et al. Pharmacoeconomic analysisof fondaparinux versus enoxaparin for the prevention of thromboem-bolic events in orthopedic surgery patients. Am J Cardiovasc Drugs.2004;4:325–333.
4. Jones TE, Smith BJ, Polasek JF. Pharmacoeconomics of low-molec-ular-weight heparins: limitations of studies comparing them to unfrac-tionated heparin. Expert Opin Pharmacother. 2004;5:1887–1897.
5. Martel N, Lee J, Wells PS. Risk for heparin-induced thrombocytopeniawith unfractionated and low-molecular-weight heparin thrombopro-phylaxis: a meta-analysis. Blood. 2005;106:2710–2715.
6. Bergqvist D, Jendteg S, Johansen L, Persson U, Odegaard K. Cost oflong-term complications of deep venous thrombosis of the lowerextremities: an analysis of a defined patient population in Sweden. AnnIntern Med. 1997;126:454–457.
7. Buller HR, Agnelli G, Hull RD, Hyers TM, Prins MH, Raskob GE.Antithrombotic therapy for venous thromboembolic disease: the Sev-enth ACCP Conference on Antithrombotic and Thrombolytic Therapy.Chest. 2004;126(suppl 3):401S–428S.
8. Nutescu EA, Shapiro NL, Chevalier A, Amin AN. A pharmacologicoverview of current and emerging anticoagulants. Cleve Clin J Med.2005;72(suppl 1):S2–S6.
9. Siragusa S, Cosmi B, Piovella F, Hirsh J, Ginsberg JS. Low-molecu-lar-weight heparins and unfractionated heparin in the treatment ofpatients with acute venous thromboembolism: results of a meta-anal-ysis. Am J Med. 1996;100:269–277.
10. van Dongen CJ, van den Belt AG, Prins MH, Lensing AW. Fixed dosesubcutaneous low molecular weight heparins versus adjusted doseunfractionated heparin for venous thromboembolism. Cochrane Da-tabase Syst Rev. 2004;(4):CD001100.
11. Spyropoulos AC, Hurley JS, Ciesla GN, de Lissovoy G. Managementof acute proximal deep vein thrombosis: pharmacoeconomic evalua-tion of outpatient treatment with enoxaparin vs inpatient treatmentwith unfractionated heparin. Chest. 2002;122:108–114.
12. Gould MK, Dembitzer AD, Sanders GD, Garber AM. Low-molecular-weight heparins compared with unfractionated heparin for treatment ofacute deep venous thrombosis: a cost-effectiveness analysis. Ann In-tern Med. 1999;130:789–799.
13. Savi P, Chong BH, Greinacher A, et al. Effect of fondaparinux onplatelet activation in the presence of heparin-dependent antibodies: ablinded comparative multicenter study with unfractionated heparin.Blood. 2005;105:139–144.
14. Reynolds NA, Perry CM, Scott LJ. Fondaparinux sodium: a review ofits use in the prevention of venous thromboembolism following majororthopaedic surgery. Drugs. 2004;64:1575–1596.
15. Buller HR, Davidson BL, Decousus H, et al. Fondaparinux or enox-aparin for the initial treatment of symptomatic deep venous thrombo-sis: a randomized trial. Ann Intern Med. 2004;140:867–873.
16. Shorr AF, Jackson WL, Moores LK, Warkentin TE. Minimizing costsfor treating deep vein thrombosis: the role for fondaparinux. J ThrombThrombolysis. 2007;23:229–236.
17. Aujesky D, Smith KJ, Cornuz J, Roberts MS. Cost-effectiveness oflow-molecular-weight heparin for treatment of pulmonary embolism.Chest. 2005;128:1601–1610.
18. Buller HR, Davidson BL, Decousus H, et al. Subcutaneous fondapa-rinux versus intravenous unfractionated heparin in the initial treatmentof pulmonary embolism. N Engl J Med. 2003;349:1695–1702.
19. Gould MK, Dembitzer AD, Doyle RL, Hastie TJ, Garber AM. Low-molecular-weight heparins compared with unfractionated heparin fortreatment of acute deep venous thrombosis: a meta-analysis of ran-domized, controlled trials. Ann Intern Med. 1999;130:800–809.
20. McGarry LJ, Thompson D, Weinstein MC, Goldhaber SZ. Cost effec-tiveness of thromboprophylaxis with a low-molecular-weight heparinversus unfractionated heparin in acutely ill medical inpatients. Am JManag Care. 2004;10:632–642.
S40 The American Journal of Medicine, Vol 120 (10B), October 2007

21. Prandoni P, Siragusa S, Girolami B, Fabris F. The incidence of hep-arin-induced thrombocytopenia in medical patients treated with low-molecular-weight heparin: a prospective cohort study. Blood. 2005;106:3049–3054.
22. Warkentin TE, Cook RJ, Marder VJ, et al. Anti-platelet factor 4/hep-arin antibodies in orthopedic surgery patients receiving antithromboticprophylaxis with fondaparinux or enoxaparin. Blood. 2005;106:3791–3796.
23. Merli G, Spiro TE, Olsson CG, et al. Subcutaneous enoxaparin once ortwice daily compared with intravenous unfractionated heparin fortreatment of venous thromboembolic disease. Ann Intern Med. 2001;134:191–202.
24. ARIXTRA [package insert]. Research Triangle Park, NC: Glaxo-SmithKline; 2005.
25. Davidson BL, Buller HR, Decousus H, et al. Outcomes in obesepatients of pulmonary embolism and deep vein thrombosis treatmentwith fondaparinux or low–molecular-weight heparins: the MATISSEtrials. Poster presented at the Annual Meeting of the InternationalSociety on Thrombosis and Haemostasis; August 5, 2005; Sydney,Australia.
26. LOVENOX [package insert]. Bridgewater, NJ: Aventis Pharmaceuti-cals Inc.; 2005.
27. Innohep [package insert]. Boulder, CO: Pharmion Corporation; 2003.28. Michota F, Merli G. Anticoagulation in special patient populations: are
special dosing considerations required? Cleve Clin J Med. 2005;72(suppl 1):S37–S42.
29. Efird LE, Kockler DR. Fondaparinux for thromboembolic treatmentand prophylaxis of heparin-induced thrombocytopenia. Ann Pharma-cother. 2006;40:1383–1387.
30. Harenberg J, Jorg I, Fenyvesi T. Treatment of heparin-induced throm-bocytopenia with fondaparinux. Haematologica. 2004;89:1017–1018.
31. Kovacs MJ. Successful treatment of heparin induced thrombocytope-nia (HIT) with fondaparinux. Thromb Haemost. 2005;93:999–1000.
32. Kuo KH, Kovacs MJ. Fondaparinux: a potential new therapy for HIT.Hematology. 2005;10:271–275.
33. Spruill WJ, Wade WE, Leslie RB. A cost analysis of fondaparinuxversus enoxaparin in total knee arthroplasty. Am J Ther. 2004;11:3–8.
34. Sullivan SD, Davidson BL, Kahn SR, Muntz JE, Oster G, Raskob G.A cost-effectiveness analysis of fondaparinux sodium compared withenoxaparin sodium as prophylaxis against venous thromboembolism:use in patients undergoing major orthopaedic surgery. Pharmacoeco-nomics. 2004;22:605–620.
35. Bauer KA, Eriksson BI, Lassen MR, Turpie AG. Fondaparinuxcompared with enoxaparin for the prevention of venous thrombo-embolism after elective major knee surgery. N Engl J Med. 2001;345:1305–1310.
36. Shorr AF, Jackson WL, Weiss BM, Moores LK. Low-molecularweight heparin for deep vein thrombosis prophylaxis in hospitalizedmedical patients: results from a cost-effectiveness analysis. BloodCoagul Fibrinolysis. 2007;18:309–316.
37. Knight KK, Wong J, Hauch O, Wygant G, Aguilar D, Ofman JJ.Economic and utilization outcomes associated with choice of treatmentfor venous thromboembolism in hospitalized patients. Value Health.2005;8:191–200.
38. Stein PD, Hull RD, Kayali F, Ghali WA, Alshab AK, Olson RE.Venous thromboembolism according to age: the impact of an agingpopulation. Arch Intern Med. 2004;164:2260–2265.
S41Shorr Pharmacoeconomics of Deep Vein Thrombosis Treatment

Management of Venous Thromboembolism
GUEST EDITOR
Andrew F. Shorr, MD, MPHAssociate Section Director
Pulmonary and Critical Care Medicine ServiceWashington Hospital Center
Associate Professor of MedicineGeorgetown University
Washington, District of Columbia
This publication was supported by an unrestricted educational grant from GlaxoSmithKline. Editorial support was provided byDorland Global Health Communications, Philadelphia, Pennsylvania.
Statement of Peer Review: All supplement manuscripts submitted to The American Journal of Medicine for publication arereviewed by the Guest Editor(s) of the supplement, by an outside peer reviewer who is independent of the supplement project,and by the Journal’s Supplement Editor (who ensures that questions raised in peer review have been addressed appropriately andthat the supplement has an educational focus that is of interest to our readership).
Author Disclosure Policy: All authors contributing to supplements in The American Journal of Medicine are required to fullydisclose any primary financial relationship with a company that has a direct fiscal or financial interest in the subject matter orproducts discussed in the submitted manuscripts, or with a company that produces a competing product. These relationships(e.g., ownership of stock or significant honoraria or consulting fees) and any direct support of research by a commercial companymust be indicated on the title page of each manuscript. This information will be published in the frontmatter of each supplement.
Editor-in-Chief: Joseph S. Alpert, MDEditor, Supplements: William H. Frishman, MDPublishing Director: Pamela Poppalardo
Executive Supplements Editor: Brian JenkinsSenior Production Editor: Mickey KramerProof/Production Editor: Mary Crowell
THE AMERICANJOURNAL ofMEDICINE ®
October 2007
Volume 120 (10B)
Management of Venous Thromboembolism
Guest Editor
Andrew F. Shorr, MD, MPHAssociate Section DirectorPulmonary and Critical Care Medicine ServiceWashington Hospital CenterAssociate Professor of MedicineGeorgetown UniversityWashington, District of Columbia
Faculty
Amjad AlMahameed, MD, MPHDivision of CardiologyBeth Israel Deaconess Medical CenterHarvard Medical SchoolBoston, Massachusetts
Teresa L. Carman, MDSection of Vascular MedicineDepartment of Cardiovascular MedicineCleveland ClinicCleveland, Ohio
Seth Clemens, MDDivision of Pulmonary, Allergy and Critical CareEmory UniversityAtlanta, Georgia
Mark A. Crowther, MD, MScDivision of HematologyMcMaster UniversityHamilton, Ontario, Canada
Andra H. James, MD, MPHDepartment of Obstetrics and GynecologyDuke University Medical CenterDurham, North Carolina
Kenneth V. Leeper, Jr., MDDivision of Pulmonary, Allergy, and Critial CareEmory UniversityAtlanta, Georgia
Faculty Disclosures
The authors who contributed to this publication have disclosed the following industry relationships:
Amjad AlMahameed, MD, is a member of the Speakers’ Bureau for GlaxoSmithKline and sanofi-aventis; serves as aconsultant to GlaxoSmithKline and sanofi-aventis; is an advisory board member for GlaxoSmithKline; has receivedresearch/grant support from GlaxoSmithKline and sanofi-aventis; and is the recipient of honoraria from GlaxoSmithKline andsanofi-aventis.
Teresa L. Carman, MD, has served as a member of the Speakers’ Bureau for Bristol-Myers Squibb and sanofi-aventis; andhas served as a consultant to Bristol-Myers Squibb and sanofi-aventis.
Seth Clemens, MD, receives research/grant support from Kimberly-Clark; and honoraria from Kimberly-Clark
Mark A. Crowther, MD, MSc, has no financial arrangement or affiliation with a corporate organization or a manufacturerof a product discussed in this supplement.
Andra H. James, MD, MPH, has no financial arrangement or affiliation with a corporate organization or a manufacturer ofa product discussed in this supplement.
Kenneth V. Leeper, Jr., MD, is a member of the Speaker’s Bureau for Ortho-McNeil and Pfizer Inc; serves as a consultantfor Ortho-McNeil and Pfizer Inc; receives research/grant support from Kimbery-Clark; and receives honoraria from KimberlyClark, Ortho-McNeil, and Pfizer Inc.
Andrew F Shorr, MD, MPH, is a member of the Speaker’s Bureau for GlaxoSmithKline and sanofi-aventis; serves as aconsultant/advisory board member for GlaxoSmithKline and sanofi-aventis; and has received research/grant support fromGlaxoSmithKline and sanofi aventis.


















