The 2016 Jefferson Benefits Guidebook · IMPORTANT BENEFITS ENROLLMENT INFORMATION Open Enrollment...
42
The 2016 Jefferson Benefits Guidebook HOME OF SIDNEY KIMMEL MEDICAL COLLEGE
Transcript of The 2016 Jefferson Benefits Guidebook · IMPORTANT BENEFITS ENROLLMENT INFORMATION Open Enrollment...

The 2016
Jefferson BenefitsGuidebook
HOME OF SIDNEY KIMMEL MEDICAL COLLEGE

IMPORTANT BENEFITS ENROLLMENT INFORMATIONOpen Enrollment for the 2016 Plan Year is processed exclusively online from Oct. 20 – Nov. 3, 2015.
The benefits you elect during open enrollment will remain in effect for the entire plan year unless you experience a qualified life event. It’s the employee’s responsibility to contact the HR Service Center to report the qualified event. Changes must be made within 30 days of date of the event.
New hire elections are processed exclusively online and must be made within 30 days of hire.
The 2016 Jefferson Benefits Guidebook

BENEFITS AT A GLANCE ...........................................2
HUMAN RESOURCES SERVICE CENTER (HRSC) ........3
Online.............................................................................3
Access Employee Self-Service ...................................3
Your Campus Key and Password ..............................3
HRSC ..............................................................................3
Eligibility ....................................................................... 4
Part-Time Employee Benefit Program .............. 4
Eligibile Dependents ...................................................5
Proof of Dependents Status .................................5
HOW AND WHEN TO ENROLL FOR COVERAGE .... 6-7
Open Enrollment ........................................................ 6
Changing Your Benefits – Due to a Life Event ..... 6
When Coverage Ends ..................................................7
COBRA ...........................................................................7
LIVEWELL@JEFF ...........................................................8-9
MEDICAL PLANS ............................................... 10-17
Medical Plans at a Glance ....................................... 10
Terms to Know ..................................................... 10
Cost of Coverage .................................................. 11
ACO Plus PPO Plan ....................................................12
What is an ACO .....................................................12
How the ACO Plus Plan Works ..........................12
The ACO Plus Hospital Network .......................12
ACO PLUS PPO Plan Summary ........................ 13-14
JeffPLUS PPO Plan ....................................................15
How the JeffPLUS PPO Plan Works .................15
The JeffPLUS Hospital Network ........................15
JeffPLUS PPO Plan Summary ............................16-17
PRESCRIPTION PLAN ............................................. 18-20
How the Plan Works................................................. 18
Prescription Benefits at a Glance ..................... 18
Mandatory Generic Drugs ....................................... 19
Prescription Management Programs .................... 19
Smoking Cessation ................................................... 19
Filling Prescription While Away ............................. 20
Charges Not Covered .............................................. 20
Out-of-Pocket Maximum ........................................ 20
Save on Prescriptions .............................................. 20
Jefferson Pharmacy Locations .........................20
VISION PLAN .............................................................21-22
Davis Vision Benefits at a Glance ......................21
Davis Participating Partners ................................... 22
Out-of-Network Benefits ........................................ 22
Reimbursement Schedule .................................. 22
Cost of Coverage ................................................. 22
DENTAL PLAN .......................................................... 23-24
Dental Plan at a Glance ........................................... 23
Delta Dental of PA ............................................... 23
Aetna DMO ............................................................ 24
Cost of Coverage ................................................. 24
LIFE INSURANCE PLANS ........................................ 25-26
Basic Life and AD&D Insurance .............................. 25
Supplemental Life and AD&D Insurance .............. 25
Cost of Coverage ................................................. 25
Supplemental Insurance Rates ........................ 25
Converting to an Individual Policy ................... 26
Age Reduction ...................................................... 26
Medical Evidence of Insurability ....................... 26
Imputed Income .................................................. 26
Long Term Disability ............................................ 26
BUSINESS TRAVEL ACCIDENT INSURANCE ...............27
How the Plan Works................................................. 27
Cost of Coverage ................................................. 27
DISABILITY PLANS .................................................. 28-32
Short-Term Disability .........................................28-29
Your Short-Term Disability Choices ................. 28
How the Short-Term Disability Plan Works .... 28
Cost of Coverage ................................................. 28
Pre-Exsisting Conditions .................................... 29
Long Term Disability (LTD) ................................30-32
Your LTD Choices (Except Clinical Faculty) ...30
How the Long-Term Disability Plan Works ....30
Cost of Coverage .................................................30
Pre-Existing Conditions ......................................30
LTD Benefit Period .........................................30-31
LTD (Clinical Faculty) ........................................... 32
FLEXIBLE SPENDING ACCOUNTS ......................... 33-35
Flexible Spending Account at a Glance..........33-34
ADP Depit Card .................................................... 34
Discrimination ....................................................... 34
FSA Store ................................................................ 35
Additional Information ........................................ 35
VOLUNTARY BENEFITS ..................................................36
YOUR OTHER BENEFITS ......................................... 37-39
Retirement Plans ....................................................... 37
Tuition Assistance ..................................................... 38
Dependent Scholarship ........................................... 38
Vacation or Earned Time Off .................................. 39
BENEFITS SERVICE PROVIDER CONTACT LIST ........ 40
TABLE OF CONTENTS
For additional benefits information please view our website, hr.jefferson.edu. Click on benefits located in the menu on the left side of the page.

2
BENEFITS AT A GLANCEJefferson offers a wide variety of high quality benefits to meet your and your family’s individual needs. This chart provides a brief overview of the benefits available:
Medical PlansAll plans include Prescription Drug coverage
• Independence Blue Cross ACO Plus PPO Plan• Independence Blue Cross JeffPLUS PPO Plan
Vision Plan • Davis Vision Premier Plan
Dental Plans• Delta Dental of Pennsylvania PPO Plan• Aetna Dental Maintenance Organization (DMO)
Life and AD&D Insurance
• Basic Life and AD&D• Supplemental Life and AD&D• Spouse Life and AD&D• Child Life and AD&D
Disability • Short-Term Disability-Basic & Supplemental• Long-Term Disability-Basic & Supplemental
Flexible Spending Accounts• Health Care• Dependent Care
Retirement • Defined Contribution Programs
Voluntary Benefits
• Auto & Home Owners Insurance• Critical Illness & Accident Insurance• Gym discounts• Pet Insurance• Pre-Paid Legal Benefits• Shopping discounts & budgeting
Other Benefits
• Adoption Assistance• Blood Donor Center• Business Travel Accident Insurance• Cell Phone Discounts• Commuter Services & Discounts• Credit Union• Daycare Services & Discounts• Discount Entertainment Tickets• Earned Time Off/Paid Holidays• Employee Assistance Program• Exos• JeffConnect• LiveWell@Jeff Wellness Program• Tuition Assistance
3
HUMAN RESOURCES SERVICE CENTER (HRSC)
ONLINE
The Human Resources website, hr.jefferson.edu, provides you a wealth of benefit information and tools:
• Compare medical plans
• View benefit overviews and plan summaries
• Print forms
• Access policies
Through the website you can access Employee Self-Service (ESS) to:
• View your current benefits
• Enroll in benefits
• Select and update your beneficiary designations
• View your pay stub
• Review and update your address and phone number
YOUR CAMPUS KEY AND PASSWORD
New employees can look up their Campus Key online and select a password using a Jefferson computer. Contact your manager or IS&T at 215-955-7975 if you need assistance.
• Go to hr.jefferson.edu
• Click on Thomas Jefferson University at the top of the page
• Click on Blackboard on the right side of the page
• Select Campus Key Lookup on the left side of the page
• Follow the instructions to look up your Campus Key and Password information
HRSC
Can’t find an answer to your question on the HR website? Call the HRSC and speak with a representative about benefits, policies, employee self-service and general payroll issues. Contact the HRSC the way you prefer:
Send an email 24/7 to [email protected]
Call the HRSC Monday – Friday 7:30am – 5:00pm at (215) 503-4772 or dial 3-4772 from a Jefferson phone.
ACCESS EMPLOYEE SELF-SERVICE:
• From work: Using Google Chrome internet browser, go to hr.jefferson.edu and click on Employee Self-Service. Sign on with your campus key and password.
• From a non-work computer: go to connect.tjuh.org and enter your campus key and password. Click on Employee Self-Service and enter your campus key and password again.
4
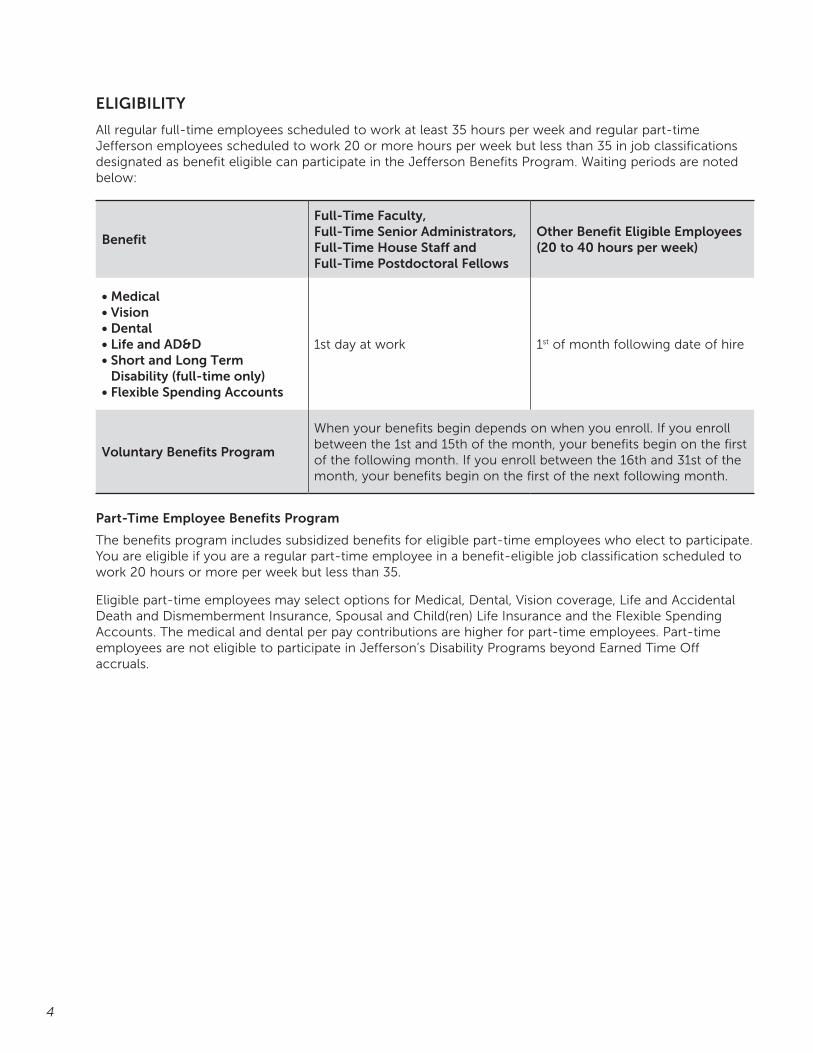
ELIGIBILITY
All regular full-time employees scheduled to work at least 35 hours per week and regular part-time Jefferson employees scheduled to work 20 or more hours per week but less than 35 in job classifications designated as benefit eligible can participate in the Jefferson Benefits Program. Waiting periods are noted below:
Benefit
Full-Time Faculty, Full-Time Senior Administrators, Full-Time House Staff and Full-Time Postdoctoral Fellows
Other Benefit Eligible Employees (20 to 40 hours per week)
• Medical• Vision • Dental • Life and AD&D• Short and Long Term
Disability (full-time only)• Flexible Spending Accounts
1st day at work 1st of month following date of hire
Voluntary Benefits Program
When your benefits begin depends on when you enroll. If you enroll between the 1st and 15th of the month, your benefits begin on the first of the following month. If you enroll between the 16th and 31st of the month, your benefits begin on the first of the next following month.
Part-Time Employee Benefits Program
The benefits program includes subsidized benefits for eligible part-time employees who elect to participate. You are eligible if you are a regular part-time employee in a benefit-eligible job classification scheduled to work 20 hours or more per week but less than 35.
Eligible part-time employees may select options for Medical, Dental, Vision coverage, Life and Accidental Death and Dismemberment Insurance, Spousal and Child(ren) Life Insurance and the Flexible Spending Accounts. The medical and dental per pay contributions are higher for part-time employees. Part-time employees are not eligible to participate in Jefferson’s Disability Programs beyond Earned Time Off accruals.
5
ELIGIBLE DEPENDENTS
You may enroll your eligible dependents in a Jefferson medical, dental, vision, life insurance or AD&D plan. Eligible dependents include your spouse and children up to age 26.
The Affordable Care Act regulations require us to report the social security number for all dependents covered under the medical plan. You will not be able to proceed with your online benefit enrollment unless you enter your dependent’s SSN.
Proof of Dependent Status
If you choose to enroll your dependents in benefits, you will need to submit dependent verification documentation within 30 days from the date you add them as a dependent. Acceptable documentation is a marriage certificate for a spouse and birth certificate for children. If either of these certificates is not available, the prior year tax return is acceptable. This information should be sent to:
[email protected]: 215-503-7455
If you do not provide the required documentation within 30 days of enrollment, that dependent will no longer be entitled to benefits and will be removed from coverage.
Who is not eligible for coverage?
• A former spouse
• A parent or grandchild who resides with you
• A legally domiciled adult and/or domestic partner
• Any other person who does not meet the eligibility requirements

6
HOW AND WHEN TO ENROLL FOR COVERAGENew hires must enroll in benefits within 30 days from date of hire. Employees that have a status change must enroll in benefits within 30 days of becoming eligible for benefits. You will need to enroll in benefits online using Employee Self-Service (ESS). The benefits you choose will remain in effect until December 31 of that year.
The Affordable Care Act has an automatic enrollment provision that requires employers to automatically enroll employees in employer medical benefits. If you do not want Jefferson medical coverage, you must go online and waive coverage every year. Otherwise, you will be enrolled in the ACO Plus PPO plan at employee only coverage.
OPEN ENROLLMENT
Every fall you will have an opportunity to make changes to your benefits during Open Enrollment. Any changes you make at Open Enrollment take effect on the upcoming January 1.
CHANGING YOUR BENEFITS DURING THE YEAR DUE TO A LIFE EVENT
You can only change your benefit elections during the year if you have a life event, as defined by the IRS. That is why it is important to review your choices carefully to ensure the benefits you choose will meet the needs of you and your family throughout the year. If you have a life event, you can only make a change to your coverage that is consistent with the life event. For example, if you get married, you may add your spouse to medical coverage, but may not switch medical plans. Any change you make must be made within 30 days of the event. Life Events include:
• Marital status change (marriage, divorce, death of spouse)
• Change in number of dependents (birth, adoption, death of dependent)
• You or one of your covered dependents gain or lose other benefits coverage
• Any other event recognized under applicable law and regulations as a reason to change an election under the Benefits Program
Marriage, birth or adoption life events can be submitted through Employee Self-Service. Any required documentation must be submitted to the HR Service Center within 30 days of the event. Contact the HR Service Center to report other life event changes.

7
WHEN COVERAGE ENDS
For You
Jefferson benefit coverage ends for you upon the following events:
• Medical, vision and dental benefits end on the last day of the month in which your employment ends or you no longer meet the applicable eligibility requirements of the plans
• Life insurance, disability and FSA benefits end on the date your employment ends or you no longer meet the applicable eligibility requirements of the plans
For Your Dependents
Jefferson benefit coverage ends for your dependents on the date:
• Your coverage ends
• Your dependent no longer meets the definition of an eligible dependent
• You remove a dependent from coverage due to a life event
Coverage may also end if you stop making required payments, you misrepresent your dependent’s eligibility status or the plan ends.
COBRA
COBRA requires continuation coverage to be offered to covered employees, their spouses, their former spouses and their dependent children when group health coverage would otherwise be lost due to certain specific qualifying events. The chart shows the specific qualifying events, the qualified beneficiaries and maximum coverage period.
Qualifying event Qualified BeneficiariesMaximum Period of Continuation Coverage
Termination (for reasons other than gross misconduct) or reduction in hours of employment
Employee, Spouse, Dependent Child
18 months
Employee enrollment in Medicare Spouse, Dependent Child 36 months
Divorce or legal separation Spouse, Dependent Child 36 months
Death of employee Spouse, Dependent Child 36 months
Loss of “dependent child” status under the plan Dependent Child 36 months
Once the qualifying event has been reported to the HR Service Center, the qualified beneficiary will receive a COBRA notice in the mail to the home address on record by our third party administrator, ADP. For more information on COBRA, visit the DOL website, “An Employees’ Guide to Health Benefits under COBRA” at www.dol.gov/ebsa/pdf/cobraemployee.pdf, contact ADP at 800-778-0043 or the HRSC at (215) 503-4772.
COBRA Rates
ACO Plus PPO JeffPLUS PPO Davis Vision Delta Dental Aetna DMO
Monthly Cost Monthly Cost Monthly Cost Monthly Cost Monthly Cost
Employee Only $628.60 $611.51 $6.32 $31.14 $21.82
Employee + 1 $1,257.16 $1,223.01 $10.85 $76.38 $40.65
Employee + 2 $1,885.75 $1,834.50 $15.67 $92.60 $75.55

8
LIVEWELL@JEFF
REDBRICK HEALTH
The LiveWell@Jeff program was established to enhance the quality of life of Jefferson employees by promoting healthy lifestyles and reducing the risk of illness by utilizing Jefferson’s wide range of educational and clinical resources. Jefferson has partnered with RedBrick Health to create a rewards program with an interactive online employee portal.
Basic requirements of the program:
1) Compass Health Assessment (online)
2) Health Screening (biometrics)
3) Earn 60 points through wellness activities – employees only
Eligibility
All benefits-eligible employees of Jefferson and their spouse, and members of 1199C enrolled in a Jefferson-sponsored health plan and their spouse are eligible to participate in RedBrick activities.
If two Jefferson employees are married to each other, both employees must each complete all three requirements of the program.
Wellness Credits
Employees and spouses that complete the wellness program requirements will earn wellness credits in their paycheck the following year. For example, the current wellness year is 10/01/2015-09/15/2016. If all requirements are met in this wellness year, credits will be applied in 2017. 2016 credits for employee completion is $15.00 per pay and a spouse is $10 per pay if enrolled in medical.
How the Portal Works
Employees and Spouses create an account on the RedBrick site and register and log in separately. When creating your account, both employee and spouse must enter your name exactly as it appears in PeopleSoft (Employee Self-Service).
MyRedBrick.com/Jefferson
The wellness portal is where you will complete the Compass Health Assessment. It also allows you to participate in RedBrick activities and record your Jefferson-sponsored activities for points.
9
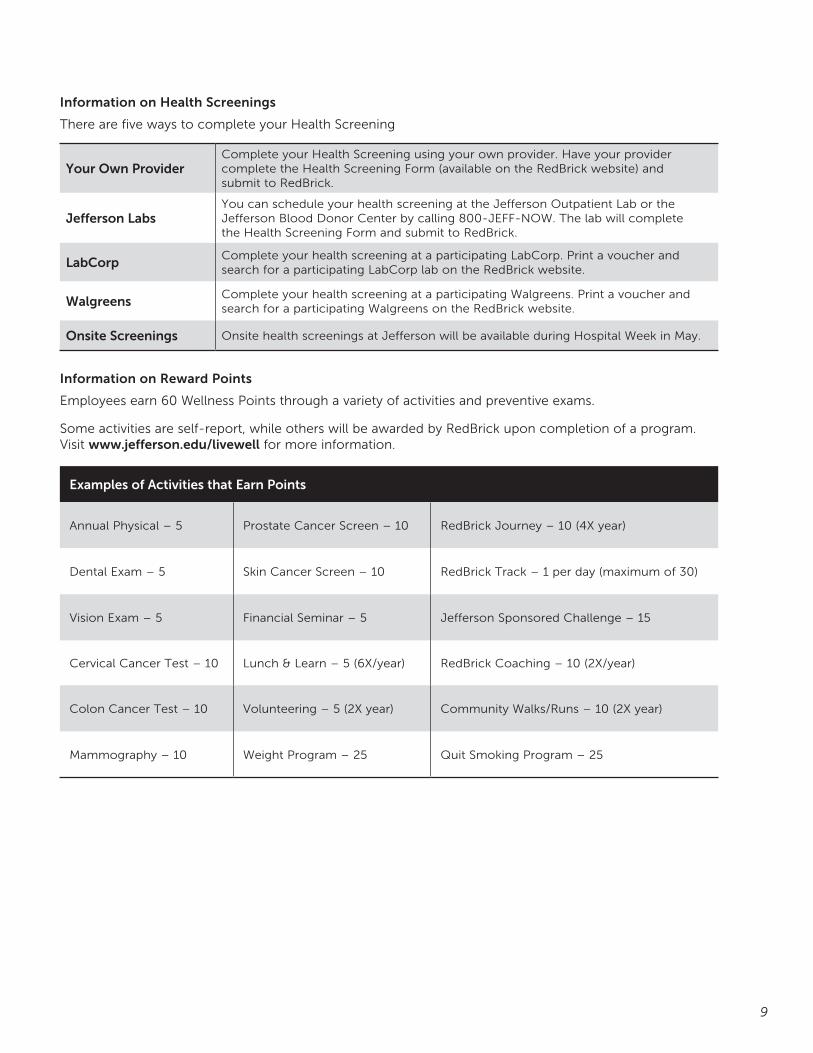
Information on Health Screenings
There are five ways to complete your Health Screening
Your Own ProviderComplete your Health Screening using your own provider. Have your provider complete the Health Screening Form (available on the RedBrick website) and submit to RedBrick.
Jefferson LabsYou can schedule your health screening at the Jefferson Outpatient Lab or the Jefferson Blood Donor Center by calling 800-JEFF-NOW. The lab will complete the Health Screening Form and submit to RedBrick.
LabCorpComplete your health screening at a participating LabCorp. Print a voucher and search for a participating LabCorp lab on the RedBrick website.
WalgreensComplete your health screening at a participating Walgreens. Print a voucher and search for a participating Walgreens on the RedBrick website.
Onsite Screenings Onsite health screenings at Jefferson will be available during Hospital Week in May.
Information on Reward Points
Employees earn 60 Wellness Points through a variety of activities and preventive exams.
Some activities are self-report, while others will be awarded by RedBrick upon completion of a program. Visit www.jefferson.edu/livewell for more information.
Examples of Activities that Earn Points
Annual Physical – 5 Prostate Cancer Screen – 10 RedBrick Journey – 10 (4X year)
Dental Exam – 5 Skin Cancer Screen – 10 RedBrick Track – 1 per day (maximum of 30)
Vision Exam – 5 Financial Seminar – 5 Jefferson Sponsored Challenge – 15
Cervical Cancer Test – 10 Lunch & Learn – 5 (6X/year) RedBrick Coaching – 10 (2X/year)
Colon Cancer Test – 10 Volunteering – 5 (2X year) Community Walks/Runs – 10 (2X year)
Mammography – 10 Weight Program – 25 Quit Smoking Program – 25

10
MEDICAL PLANS
MEDICAL PLANS AT A GLANCE
Jefferson gives you a choice of two medical plans administered through Independence Blue Cross:
• ACO Plus PPO
• JeffPLUS PPO
You have a choice of three coverage categories:
• Employee only
• Employee + 1
• Family
Terms to Know
Here are some important terms to help you understand how the plans pay benefits.
Allowable Amount Our benefit plans pay expenses based on the allowable amount. This is the average charge, or “going rate” for a specific service in a geographic area. Network providers have agreed to accept the allowable amount, while out-of-network providers may charge above the allowable amount. With an Out of Network provider, you may be responsible for the amount over the allowable amount, in addition to any deductibles, coinsurance or copays your plan requires.
Coinsurance The percentage of an eligible expense the plan pays (such as 80%). You pay the remaining percentage (such as 20%) and this counts toward the out-of-pocket maximum.
Copay The flat dollar amount you pay for some services (such as $20) at the time care is received. Copays count toward the out-of-pocket maximum.
Deductible The amount of eligible expenses you pay before the plan pays benefits. The deductible counts toward the out-of-pocket maximum.
Out of Pocket Maximum This is the maximum amount you or your family must pay in coinsurance, copays and deductibles toward eligible expenses in a calendar year. Generally, when you reach the out-of-pocket maximum the plan will pay 100% for most eligible expenses.
Pre-existing Limitations The medical plans do not restrict benefits based on pre-existing conditions.
The Affordable Care Act has an automatic enrollment provision that requires employers to automatically enroll employees in employer medical benefits. If you do not want Jefferson medical coverage, you must go online and waive coverage every year. Otherwise, you will be enrolled in the ACO Plus PPO plan at employee only coverage.
11
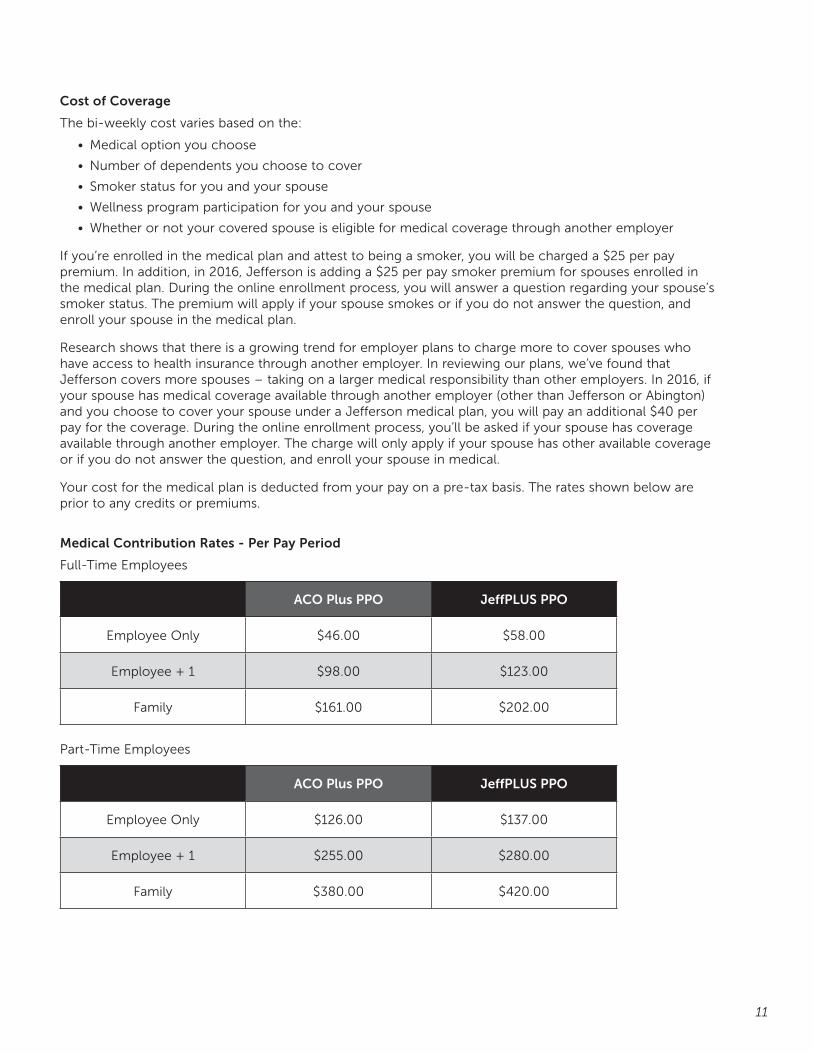
Cost of Coverage
The bi-weekly cost varies based on the:
• Medical option you choose
• Number of dependents you choose to cover
• Smoker status for you and your spouse
• Wellness program participation for you and your spouse
• Whether or not your covered spouse is eligible for medical coverage through another employer
If you’re enrolled in the medical plan and attest to being a smoker, you will be charged a $25 per pay premium. In addition, in 2016, Jefferson is adding a $25 per pay smoker premium for spouses enrolled in the medical plan. During the online enrollment process, you will answer a question regarding your spouse’s smoker status. The premium will apply if your spouse smokes or if you do not answer the question, and enroll your spouse in the medical plan.
Research shows that there is a growing trend for employer plans to charge more to cover spouses who have access to health insurance through another employer. In reviewing our plans, we’ve found that Jefferson covers more spouses – taking on a larger medical responsibility than other employers. In 2016, if your spouse has medical coverage available through another employer (other than Jefferson or Abington)and you choose to cover your spouse under a Jefferson medical plan, you will pay an additional $40 per pay for the coverage. During the online enrollment process, you’ll be asked if your spouse has coverage available through another employer. The charge will only apply if your spouse has other available coverage or if you do not answer the question, and enroll your spouse in medical.
Your cost for the medical plan is deducted from your pay on a pre-tax basis. The rates shown below are prior to any credits or premiums.
Medical Contribution Rates - Per Pay Period
Full-Time Employees
ACO Plus PPO JeffPLUS PPO
Employee Only $46.00 $58.00
Employee + 1 $98.00 $123.00
Family $161.00 $202.00
Part-Time Employees
ACO Plus PPO JeffPLUS PPO
Employee Only $126.00 $137.00
Employee + 1 $255.00 $280.00
Family $380.00 $420.00
12
ACO PLUS PPO PLAN
What is an ACO?
Accountable Care Organizations (ACOs) are a group of doctors, hospital, and other health care providers, who come together voluntarily to give coordinated high quality care. The goal of coordinated care is to ensure that patients, especially the chronically ill, get the right care at the right time, while avoiding unnecessary duplication of services and preventing medical errors. Jefferson is part of the Delaware Valley ACO (DVACO) and we are offering this employer ACO plan in partnership with the DVACO.
How the ACO Plus PPO Plan works
The ACO Plus PPO plan allows complete freedom of choice of providers. Primary Care Physician designation is not required, however, it is encouraged. Research shows that a patient with a relationship with a PCP has better coordinated care, better outcomes, with less cost and waste. Referrals are not required with the ACO Plus PPO plan.
You decide which network to choose a provider from when seeking medical care.
• Tier 1 Home ($): You receive care from a home ACO Plus provider
Non-Home ($$): You receive care from a non-home ACO Plus provider
• Tier 2 ($$$): You receive care from a Personal Choice provider
• Tier 3 ($$$$): You receive care from an out-of-network provider
If you receive care at an ACO Plus facility or an ACO Plus provider, you receive the highest level of benefits. This higher level of benefit is only available if the service is available through an ACO Plus provider.
The ACO Plus PPO Hospital Network
Visit www.jeffnetworks.org for the most up-to-date listing of facilities and providers in the ACO Plus network. Go to www.ibx.com to search for providers in the Personal Choice network.
ACO Plus Home Hospitals
• Jefferson Hospital
• Abington Hospital
• Main Line Health
- Bryn Mawr Hospital
- Bryn Mawr Rehab Hospital
- Lankenau Hospital
- Mirmont Treatment Center
- Paoli Memorial Hospital
- Riddle Memorial Hospital
ACO Plus non-home Hospitals
• Doylestown Hospital
• Magee Rehabilitation Hospital
• Nemours/Alfred I. duPont

13
ACO PLUS PPO – 2016 PLAN SUMMARYBENEFITS ACO Plus HOME ACO Plus NON-HOME PERSONAL CHOICE NETWORK OUT-OF-NETWORK *
Deductible
Individual None None $500 $1,000
Family None None $1,500 $3,000
Benefit Period Calendar Year Calendar Year Calendar Year Calendar Year
Coinsurance (percentage paid by plan except hearing aid benefit)
100% or 80% unless otherwise noted
100%, 90% or 80% unless otherwise noted
70% or 80% after deductible unless otherwise noted
60% after deductible unless otherwise noted
Out-of-Pocket Maximum***
Individual $2,000 4 $2,500 4 $3,500 4 $5,000
Family $4,000 4 $4,500 4 $5,500 4 $10,000
Lifetime Maximum Unlimited Unlimited Unlimited Unlimited
Doctor’s Office Visits
Primary Care Services $5 copayment $5 copayment $30 copayment 60% after deductible
Specialist Services $20 copayment $20 copayment $40 copayment 60% after deductible
Preventive Care for Adults and Children 100% 100% 100% 60% after deductible
Pediatric Immunizations 100% 100% 100% 60% after deductible
Routine Gynecological Exam/Pap One routine exam/pap test per calendar year for women of any age 1
100% 100% 100% 60% after deductible
Mammogram 100% 100% 100% 60%
Nutrition Counseling for Weight Management 6 visits per calendar year 1
100% 100% 100% 100% after deductible
Outpatient Diagnostic Services
Routine Radiology $15 Copayment $20 Copayment 70% after deductible 60% after deductible
MRI/MRA/CAT/PET $25 Copayment $30 Copayment 70% after deductible 60% after deductible
Outpatient Diagnostic Services
Laboratory 100% 100% $10 Copayment per occurrence 60% after deductible
Allergy Testing 100% 100% 80% after deductible 60% after deductible
Allergy Extract / Injections 100% 100% 80% after deductible 60% after deductible
Maternity
First OB Visit $20 Copayment $20 Copayment $40 Copayment 60% after deductible
Contraceptives 100% 100% 100% 60% after deductible
Infertility Diagnosis and Treatment $20,000 per lifetime 1
100% after applicable copayment
100% after applicable copayment 80% after deductible and applicable copayment
60% after deductible
Elective Abortion 100% 100% 80% after deductible 60% after deductible
Inpatient Hospital Services**
Facility 100% $300 Copayment per admission 3 $700 Copayment per admission 3 60% after deductible 2
Physician/Surgeon 100% 100% 80% after deductible 60% after deductible
Inpatient Hospital Days 1 365 365 365 70 2
Emergency Care $150 Copayment (Copayment waived if admitted)
$150 Copayment (Copayment waived if admitted)
$150 Copayment (Copayment waived if admitted)
$150 Copayment (Copayment waived if admitted)
Urgent Care Center $60 Copayment $70 Copayment $75 Copayment 60% after deductible
Retail Clinic Not Available Not Available $30 Copayment 60% after deductible
Tele Medicine $15 Not Covered Not Covered Not Covered
Benefits Outside USA Coverage in full for emergencies, applicable copay applies. Access to BlueCard Worldwide Program
Outpatient Surgery – Voluntary sterilization procedures included; Reversal of sterilization procedures excluded
Facility 100% $200 Copayment $300 Copayment per occurrence then 80% after deductible
60% after deductible
Physician/Surgeon 100% 100% 80% after deductible 60% after deductible
Ambulance
Emergency 100% 100% 100% 100%
Non-Emergency 80% 80% 80% 60% after deductible
14
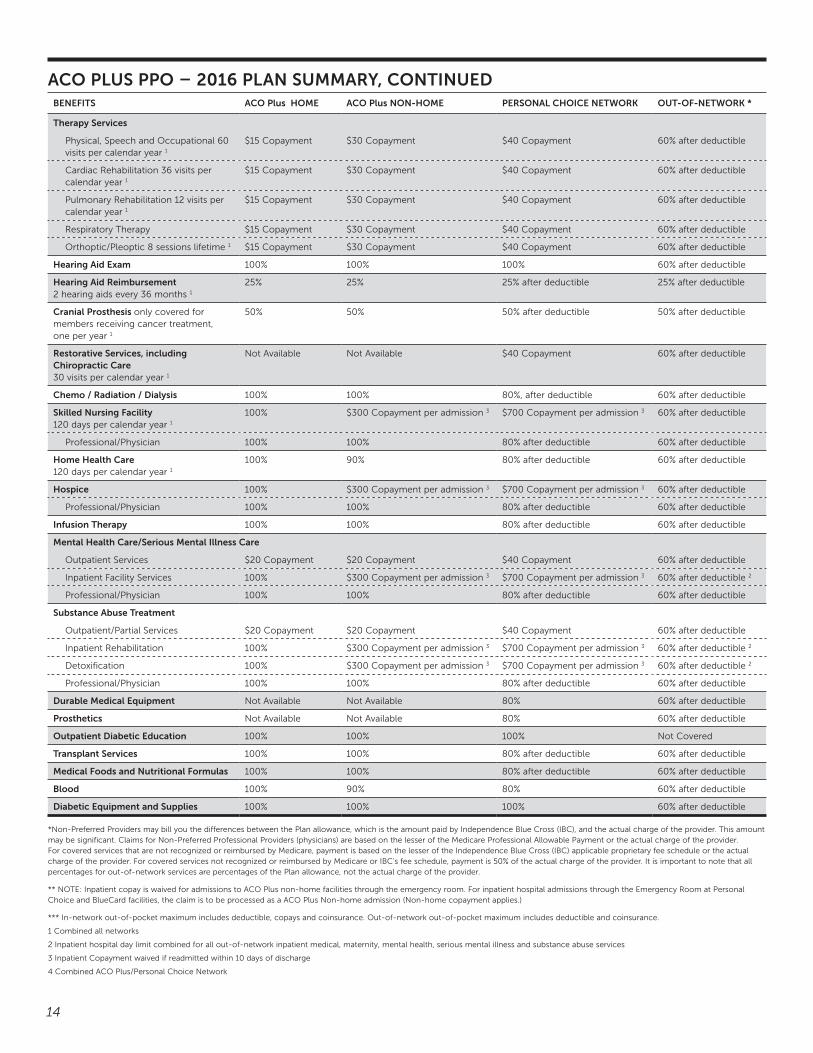
Therapy Services
Physical, Speech and Occupational 60 visits per calendar year 1
$15 Copayment $30 Copayment $40 Copayment 60% after deductible
Cardiac Rehabilitation 36 visits per calendar year 1
$15 Copayment $30 Copayment $40 Copayment 60% after deductible
Pulmonary Rehabilitation 12 visits per calendar year 1
$15 Copayment $30 Copayment $40 Copayment 60% after deductible
Respiratory Therapy $15 Copayment $30 Copayment $40 Copayment 60% after deductible
Orthoptic/Pleoptic 8 sessions lifetime 1 $15 Copayment $30 Copayment $40 Copayment 60% after deductible
Hearing Aid Exam 100% 100% 100% 60% after deductible
Hearing Aid Reimbursement 2 hearing aids every 36 months 1
25% 25% 25% after deductible 25% after deductible
Cranial Prosthesis only covered for members receiving cancer treatment, one per year 1
50% 50% 50% after deductible 50% after deductible
Restorative Services, including Chiropractic Care 30 visits per calendar year 1
Not Available Not Available $40 Copayment 60% after deductible
Chemo / Radiation / Dialysis 100% 100% 80%, after deductible 60% after deductible
Skilled Nursing Facility 120 days per calendar year 1
100% $300 Copayment per admission 3 $700 Copayment per admission 3 60% after deductible
Professional/Physician 100% 100% 80% after deductible 60% after deductible
Home Health Care 120 days per calendar year 1
100% 90% 80% after deductible 60% after deductible
Hospice 100% $300 Copayment per admission 3 $700 Copayment per admission 3 60% after deductible
Professional/Physician 100% 100% 80% after deductible 60% after deductible
Infusion Therapy 100% 100% 80% after deductible 60% after deductible
Mental Health Care/Serious Mental Illness Care
Outpatient Services $20 Copayment $20 Copayment $40 Copayment 60% after deductible
Inpatient Facility Services 100% $300 Copayment per admission 3 $700 Copayment per admission 3 60% after deductible 2
Professional/Physician 100% 100% 80% after deductible 60% after deductible
Substance Abuse Treatment
Outpatient/Partial Services $20 Copayment $20 Copayment $40 Copayment 60% after deductible
Inpatient Rehabilitation 100% $300 Copayment per admission 3 $700 Copayment per admission 3 60% after deductible 2
Detoxification 100% $300 Copayment per admission 3 $700 Copayment per admission 3 60% after deductible 2
Professional/Physician 100% 100% 80% after deductible 60% after deductible
Durable Medical Equipment Not Available Not Available 80% 60% after deductible
Prosthetics Not Available Not Available 80% 60% after deductible
Outpatient Diabetic Education 100% 100% 100% Not Covered
Transplant Services 100% 100% 80% after deductible 60% after deductible
Medical Foods and Nutritional Formulas 100% 100% 80% after deductible 60% after deductible
Blood 100% 90% 80% 60% after deductible
Diabetic Equipment and Supplies 100% 100% 100% 60% after deductible
*Non-Preferred Providers may bill you the differences between the Plan allowance, which is the amount paid by Independence Blue Cross (IBC), and the actual charge of the provider. This amount may be significant. Claims for Non-Preferred Professional Providers (physicians) are based on the lesser of the Medicare Professional Allowable Payment or the actual charge of the provider. For covered services that are not recognized or reimbursed by Medicare, payment is based on the lesser of the Independence Blue Cross (IBC) applicable proprietary fee schedule or the actual charge of the provider. For covered services not recognized or reimbursed by Medicare or IBC’s fee schedule, payment is 50% of the actual charge of the provider. It is important to note that all percentages for out-of-network services are percentages of the Plan allowance, not the actual charge of the provider.
** NOTE: Inpatient copay is waived for admissions to ACO Plus non-home facilities through the emergency room. For inpatient hospital admissions through the Emergency Room at Personal Choice and BlueCard facilities, the claim is to be processed as a ACO Plus Non-home admission (Non-home copayment applies.)
*** In-network out-of-pocket maximum includes deductible, copays and coinsurance. Out-of-network out-of-pocket maximum includes deductible and coinsurance.
1 Combined all networks
2 Inpatient hospital day limit combined for all out-of-network inpatient medical, maternity, mental health, serious mental illness and substance abuse services
3 Inpatient Copayment waived if readmitted within 10 days of discharge
4 Combined ACO Plus/Personal Choice Network
ACO PLUS PPO – 2016 PLAN SUMMARY, CONTINUEDBENEFITS ACO Plus HOME ACO Plus NON-HOME PERSONAL CHOICE NETWORK OUT-OF-NETWORK *
15
JEFFPLUS PPO PLAN
How the JeffPLUS PPO Plan works
The JeffPLUS PPO Plan allows complete freedom of choice of providers. Primary Care Physician designation and referrals are not required with the PPO.
You decide which network to choose a provider from when seeking medical care.
• Tier 1 Home ($): You receive care from a home JeffPLUS provider
Non-Home ($$): You receive care from a non-home JeffPLUS provider
• Tier 2 ($$$): You receive care from a Personal Choice provider
• Tier 3 ($$$$): You receive care from an out-of-network provider
If you receive care at a JeffPLUS facility or JeffPLUS provider, you receive the highest level of benefits. This higher level of benefit is only available if the service is available through a JeffPLUS provider.
The JeffPLUS Hospital Network
Visit www.jeffnetworks.org for the most up-to-date listing of facilities and providers in the JeffPLUS network. Go to www.ibx.com to search for providers in the Personal Choice network.
JeffPLUS Home Hospitals
• Jefferson Hospital
• Abington Hospital
• Main Line Health
- Bryn Mawr Hospital
- Bryn Mawr Rehab Hospital
- Lankenau Hospital
- Mirmont Treatment Center
- Paoli Memorial Hospital
- Riddle Memorial Hospital
JeffPLUS non-home Hospitals
• Magee Rehabilitation Hospital
• Nemours/Alfred I. duPont
• Virtua Hospitals (Inpatient services only)
- Berlin
- Marlton
- Memorial
- Voorhees
16
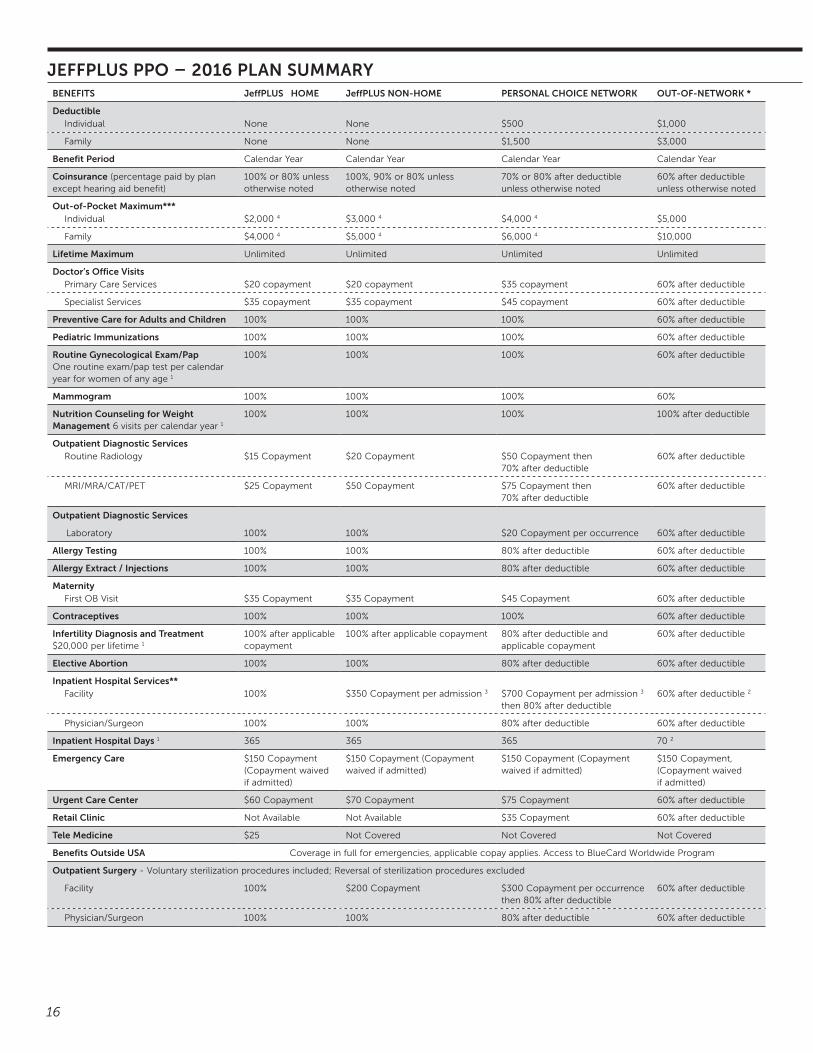
JEFFPLUS PPO – 2016 PLAN SUMMARYBENEFITS JeffPLUS HOME JeffPLUS NON-HOME PERSONAL CHOICE NETWORK OUT-OF-NETWORK *
Deductible Individual None None $500 $1,000
Family None None $1,500 $3,000
Benefit Period Calendar Year Calendar Year Calendar Year Calendar Year
Coinsurance (percentage paid by plan except hearing aid benefit)
100% or 80% unless otherwise noted
100%, 90% or 80% unless otherwise noted
70% or 80% after deductible unless otherwise noted
60% after deductible unless otherwise noted
Out-of-Pocket Maximum***Individual $2,000 4 $3,000 4 $4,000 4 $5,000
Family $4,000 4 $5,000 4 $6,000 4 $10,000
Lifetime Maximum Unlimited Unlimited Unlimited Unlimited
Doctor’s Office VisitsPrimary Care Services $20 copayment $20 copayment $35 copayment 60% after deductible
Specialist Services $35 copayment $35 copayment $45 copayment 60% after deductible
Preventive Care for Adults and Children 100% 100% 100% 60% after deductible
Pediatric Immunizations 100% 100% 100% 60% after deductible
Routine Gynecological Exam/Pap One routine exam/pap test per calendar year for women of any age 1
100% 100% 100% 60% after deductible
Mammogram 100% 100% 100% 60%
Nutrition Counseling for Weight Management 6 visits per calendar year 1
100% 100% 100% 100% after deductible
Outpatient Diagnostic ServicesRoutine Radiology $15 Copayment $20 Copayment $50 Copayment then
70% after deductible60% after deductible
MRI/MRA/CAT/PET $25 Copayment $50 Copayment $75 Copayment then 70% after deductible
60% after deductible
Outpatient Diagnostic Services
Laboratory 100% 100% $20 Copayment per occurrence 60% after deductible
Allergy Testing 100% 100% 80% after deductible 60% after deductible
Allergy Extract / Injections 100% 100% 80% after deductible 60% after deductible
MaternityFirst OB Visit $35 Copayment $35 Copayment $45 Copayment 60% after deductible
Contraceptives 100% 100% 100% 60% after deductible
Infertility Diagnosis and Treatment $20,000 per lifetime 1
100% after applicable copayment
100% after applicable copayment 80% after deductible and applicable copayment
60% after deductible
Elective Abortion 100% 100% 80% after deductible 60% after deductible
Inpatient Hospital Services**Facility 100% $350 Copayment per admission 3 $700 Copayment per admission 3
then 80% after deductible60% after deductible 2
Physician/Surgeon 100% 100% 80% after deductible 60% after deductible
Inpatient Hospital Days 1 365 365 365 70 2
Emergency Care $150 Copayment (Copayment waived if admitted)
$150 Copayment (Copayment waived if admitted)
$150 Copayment (Copayment waived if admitted)
$150 Copayment, (Copayment waived if admitted)
Urgent Care Center $60 Copayment $70 Copayment $75 Copayment 60% after deductible
Retail Clinic Not Available Not Available $35 Copayment 60% after deductible
Tele Medicine $25 Not Covered Not Covered Not Covered
Benefits Outside USA Coverage in full for emergencies, applicable copay applies. Access to BlueCard Worldwide Program
Outpatient Surgery - Voluntary sterilization procedures included; Reversal of sterilization procedures excluded
Facility 100% $200 Copayment $300 Copayment per occurrence then 80% after deductible
60% after deductible
Physician/Surgeon 100% 100% 80% after deductible 60% after deductible

17
AmbulanceEmergency 100% 100% 100% 100%
Non-Emergency 80% 80% 80% 60% after deductible
Therapy ServicesPhysical, Speech and Occupational 60 visits per calendar year 1
$25 Copayment $30 Copayment $40 Copayment 60% after deductible
Cardiac Rehabilitation 36 visits per calendar year 1
$25 Copayment $30 Copayment $40 Copayment 60% after deductible
Pulmonary Rehabilitation 12 visits per calendar year 1
$25 Copayment $30 Copayment $40 Copayment 60% after deductible
Respiratory Therapy $25 Copayment $30 Copayment $40 Copayment 60% after deductible
Orthoptic/Pleoptic 8 sessions lifetime 1 $25 Copayment $30 Copayment $40 Copayment 60% after deductible
Hearing Aid Exam 100% 100% 100% 60% after deductible
Hearing Aid Reimbursemen2 hearing aids every 36 months 1
25% 25% 25% after deductible 25% after deductible
Cranial Prosthesis only covered for members receiving cancer treatment, one per year 1
50% 50% 50% after deductible 50% after deductible
Restorative Services, including Chiropractic Care 30 visits per calendar year 1
Not Available Not Available $40 Copayment 60% after deductible
Chemo / Radiation / Dialysis 100% 100% 80%, after deductible 60% after deductible
Skilled Nursing Facility 120 days per calendar year 1
100% $350 Copayment per admission 3 $700 Copayment per admission 3 then 80% after deductible
60% after deductible
Professional/Physician 100% 100% 80% after deductible 60% after deductible
Home Health Care 120 days per calendar year 1
100% 90% 80% after deductible 60% after deductible
Hospice 100% $350 Copayment per admission 3 $700 Copayment per admission 3 then 80% after deductible
60% after deductible
Professional/Physician 100% 100% 80% after deductible 60% after deductible
Infusion Therapy 100% 100% 80% after deductible 60% after deductible
Mental Health Care/Serious Mental Illness CareOutpatient Services $35 Copayment $35 Copayment $40 Copayment 60% after deductible
Inpatient Facility Services 100% $350 Copayment per admission 3 $700 Copayment per admission 3 then 80% after deductible
60% after deductible 2
Professional/Physician 100% 100% 80% after deductible 60% after deductible
Substance Abuse TreatmentOutpatient/Partial Services $35 Copayment $35 Copayment $40 Copayment 60% after deductible
Inpatient Rehabilitation 100% $350 Copayment per admission 3 $700 Copayment per admission 3
then 80% after deductible60% after deductible 2
Detoxification 100% $350 Copayment per admission 3 $700 Copayment per admission 3 then 80% after deductible
60% after deductible 2
Durable Medical Equipment Not Available Not Available 80% 60% after deductible
Prosthetics Not Available Not Available 80% 60% after deductible
Outpatient Diabetic Education 100% 100% 100% Not Covered
Transplant Services 100% 100% 80% after deductible 60% after deductible
Medical Foods and Nutritional Formulas 100% 100% 80% after deductible 60% after deductible
Blood 100% 90% 80% 60% after deductible
Diabetic Equipment and Supplies 100% 100% 100% 60% after deductible
*Non –Preferred Providers may bill you the differences between the Plan allowance, which is the amount paid by Independence Blue Cross (IBC), and the actual charge of the provider. This amount may be significant. Claims for Non-Preferred Professional Providers (physicians) are based on the lesser of the Medicare Professional Allowable Payment or the actual charge of the provider. For covered services that are not recognized or reimbursed by Medicare, payment is based on the lesser of the Independence Blue Cross (IBC) applicable proprietary fee schedule or the actual charge of the provider. For covered services not recognized or reimbursed by Medicare or IBC’s fee schedule, payment is 50% of the actual charge of the provider. It is important to note that all percentages for out-of-network services are percentages of the Plan allowance, not the actual charge of the provider.
** NOTE: Inpatient copay is waived for admissions to JeffPLUS non-home facilities through the emergency room. For inpatient hospital admissions through the Emergency Room at Personal Choice and BlueCard facilities, the claim is to be processed as a JeffPLUS Non-home admission (deductible and coinsurance are waived, Non-home copayment applies.)
***In-network out-of-pocket maximum includes deductible, copays and coinsurance. Out-of-network out-of-pocket maximum includes deductible and coinsurance.
1 Combined all networks
2 Inpatient hospital day limit combined for all out-of-network inpatient medical, maternity, mental health, serious mental illness and substance abuse services
3 Inpatient Copayment waived if readmitted within 10 days of discharge
4 Combined JeffPLUS/Personal Choice Network
JEFFPLUS PPO – 2016 PLAN SUMMARY, CONTINUEDBENEFITS JeffPLUS HOME JeffPLUS NON-HOME PERSONAL CHOICE NETWORK OUT-OF-NETWORK *
18
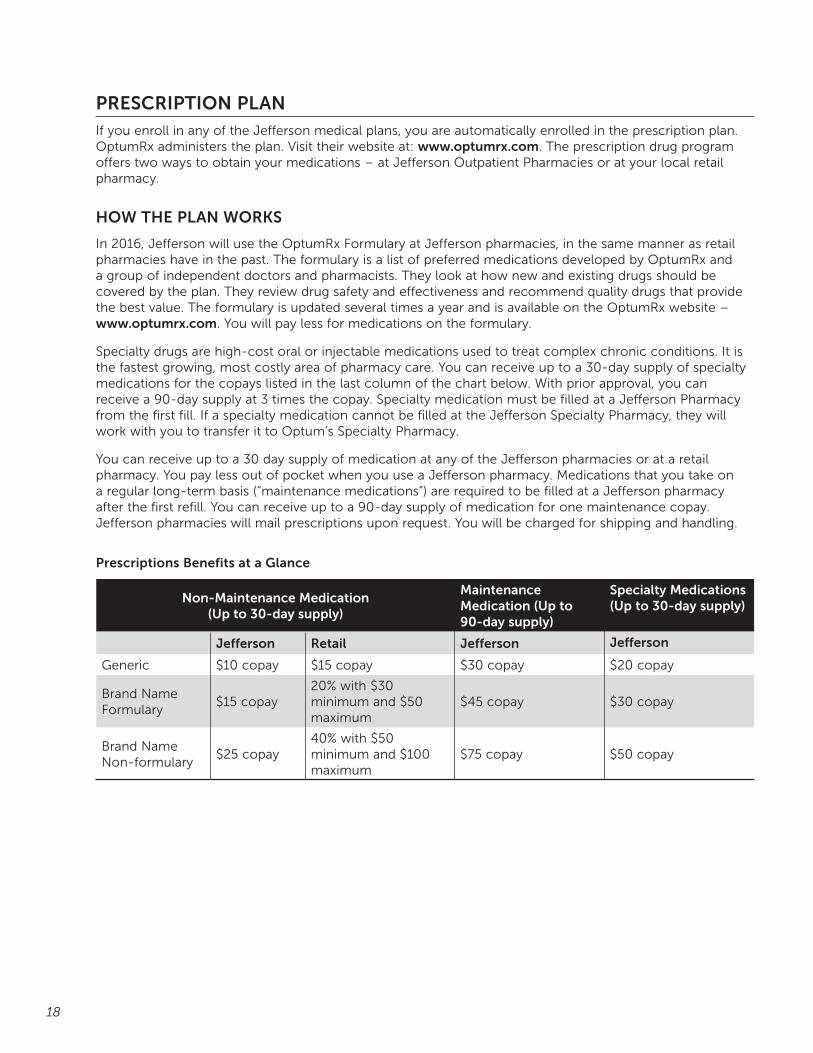
PRESCRIPTION PLANIf you enroll in any of the Jefferson medical plans, you are automatically enrolled in the prescription plan. OptumRx administers the plan. Visit their website at: www.optumrx.com. The prescription drug program offers two ways to obtain your medications – at Jefferson Outpatient Pharmacies or at your local retail pharmacy.
HOW THE PLAN WORKS
In 2016, Jefferson will use the OptumRx Formulary at Jefferson pharmacies, in the same manner as retail pharmacies have in the past. The formulary is a list of preferred medications developed by OptumRx and a group of independent doctors and pharmacists. They look at how new and existing drugs should be covered by the plan. They review drug safety and effectiveness and recommend quality drugs that provide the best value. The formulary is updated several times a year and is available on the OptumRx website – www.optumrx.com. You will pay less for medications on the formulary.
Specialty drugs are high-cost oral or injectable medications used to treat complex chronic conditions. It is the fastest growing, most costly area of pharmacy care. You can receive up to a 30-day supply of specialty medications for the copays listed in the last column of the chart below. With prior approval, you can receive a 90-day supply at 3 times the copay. Specialty medication must be filled at a Jefferson Pharmacy from the first fill. If a specialty medication cannot be filled at the Jefferson Specialty Pharmacy, they will work with you to transfer it to Optum’s Specialty Pharmacy.
You can receive up to a 30 day supply of medication at any of the Jefferson pharmacies or at a retail pharmacy. You pay less out of pocket when you use a Jefferson pharmacy. Medications that you take on a regular long-term basis (“maintenance medications”) are required to be filled at a Jefferson pharmacy after the first refill. You can receive up to a 90-day supply of medication for one maintenance copay. Jefferson pharmacies will mail prescriptions upon request. You will be charged for shipping and handling.
Prescriptions Benefits at a Glance
Non-Maintenance Medication (Up to 30-day supply)
Maintenance Medication (Up to 90-day supply)
Specialty Medications (Up to 30-day supply)
Jefferson Retail Jefferson Jefferson
Generic $10 copay $15 copay $30 copay $20 copay
Brand Name Formulary
$15 copay20% with $30 minimum and $50 maximum
$45 copay $30 copay
Brand Name Non-formulary
$25 copay40% with $50 minimum and $100 maximum
$75 copay $50 copay

19
MANDATORY GENERIC DRUGS
Whether you fill your prescriptions at a Jefferson or retail pharmacy, you are required to purchase generic drugs when they are available. If you or your doctor chooses a brand name drug when a generic is available, you will be required to pay the difference in cost between the generic and the brand, along with the applicable brand copay.
If you need to file an appeal to the Mandatory Generic program, you, or your covered dependent, must try a full prescription of the generic drug before requesting a brand name replacement. A Generic Exception Request form can be obtained from the Jefferson Apothecary.
PRESCRIPTION MANAGEMENT PROGRAMS
The prescription plan has several management programs to improve care and help manage costs:
• Prior Authorization Program requires authorization for some medications that are only approved or effective in treating specific illnesses, cost more or may be prescribed for conditions for which safety and effectiveness have not been well-established
• Quantity Limit Program sets limits based on the FDA approved indications, the manufacturer’s package labeling instructions and well-accepted or published clinical recommendations.
• Step Therapy Program encourages you to try first-line medications that deliver similar value, safety and effectiveness, but cost less than others.
SMOKING CESSATION
Support is available to help you and your family members quit smoking. Beginning in 2016, over-the-counter (OTC) and prescription smoking cessation products will be available at no cost. OTC products will require a prescription from your provider.

20
GETTING PRESCRIPTIONS FILLED WHILE AWAY FROM HOME
OptumRx is affiliated with over 63,000 pharmacies nationwide. You should have no problem filling a prescription at a participating pharmacy anywhere in the U.S. Simply present your I.D. card. OptumRx participating pharmacies are online via computer with OptumRx and will submit your claim electronically at the time the prescription is filled. You pay only your applicable copayment.
If you do not use a participating pharmacy, you must pay the full cost of the prescription, usually at the full retail cost – you will not benefit from the “plan discount.” You must complete and send a claim form to OptumRx no later than 365 business days from the date the prescription was dispensed. You will then be reimbursed only for the amount which OptumRx would have covered.
CHARGES NOT COVERED
Some prescription drugs and supplies are not covered under this plan. The plan does not cover:
• Allergy serum (covered under the medical plan if administered in your physician’s office)
• Dietary aids, cosmetics or other health and beauty aids
• Over-the-counter drugs
• Non-legend vitamins
• Medical appliances, such as back braces, bandages, cervical collars
• Ostomy products (covered under the medical plan)
• Charges for the administration of any drug
OUT-OF-POCKET MAXIMUM
The out-of-pocket maximum is $2,500 per person or $5,000 per family. Once you reach the out-of-pocket limit, all covered prescriptions will be paid by Jefferson at 100%.
SAVE ON PRESCRIPTIONS
Reduce your out-of-pocket expense when you use a Jefferson outpatient pharmacy.
Jefferson Apothecary Jefferson Pharmacy1st floor, Gibbon Building Lobby, 833 Chestnut Street 111 S. 11th Street 215-955-4400 215-955-8845 Hours: 8:30 a.m. - 5:30 p.m. M-F Hours: 7 a.m. - 6 p.m. M-F 9 a.m. - 1 p.m. Sat. 9 a.m. - 4 p.m. Sat.
Jefferson Pharmacy Walnut Street Methodist Hospital Apothecary908 Walnut Street 2301 S. Broad Street 215-503-1135 215-952-9385 Hours: 8:30 a.m. - 5:30 p.m. M-F Hours: 8:30 a.m. - 5 p.m. M-F 9 a.m. - 1 p.m. Sat.
Jefferson Specialty PharmacyMedications are hand-delivered to your home or office, as requested; remote locations are shipped. 215-955-8154 Hours: 8 a.m. - 5 p.m. M-F
21
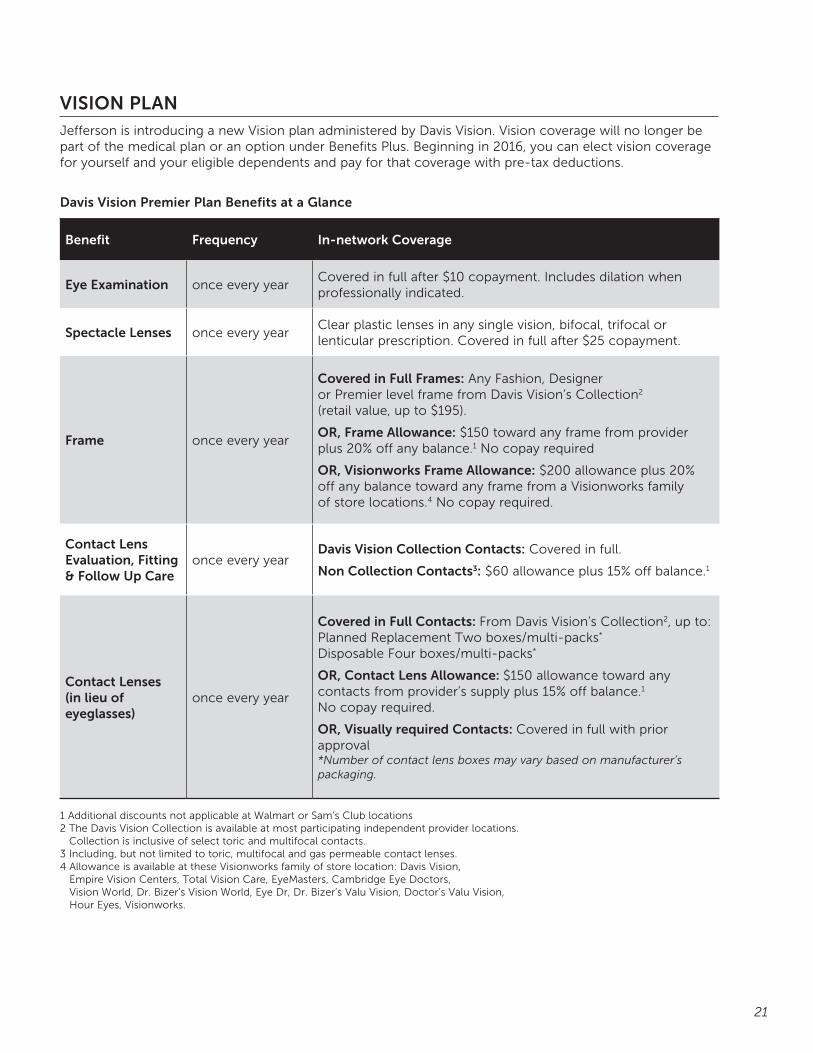
VISION PLANJefferson is introducing a new Vision plan administered by Davis Vision. Vision coverage will no longer be part of the medical plan or an option under Benefits Plus. Beginning in 2016, you can elect vision coverage for yourself and your eligible dependents and pay for that coverage with pre-tax deductions.
Davis Vision Premier Plan Benefits at a Glance
Benefit Frequency In-network Coverage
Eye Examination once every yearCovered in full after $10 copayment. Includes dilation when professionally indicated.
Spectacle Lenses once every yearClear plastic lenses in any single vision, bifocal, trifocal or lenticular prescription. Covered in full after $25 copayment.
Frame once every year
Covered in Full Frames: Any Fashion, Designer or Premier level frame from Davis Vision’s Collection2 (retail value, up to $195).
OR, Frame Allowance: $150 toward any frame from provider plus 20% off any balance.1 No copay required
OR, Visionworks Frame Allowance: $200 allowance plus 20% off any balance toward any frame from a Visionworks family of store locations.4 No copay required.
Contact Lens Evaluation, Fitting & Follow Up Care
once every yearDavis Vision Collection Contacts: Covered in full.
Non Collection Contacts3: $60 allowance plus 15% off balance.1
Contact Lenses (in lieu of eyeglasses)
once every year
Covered in Full Contacts: From Davis Vision’s Collection2, up to:Planned Replacement Two boxes/multi-packs*
Disposable Four boxes/multi-packs*
OR, Contact Lens Allowance: $150 allowance toward any contacts from provider’s supply plus 15% off balance.1 No copay required.
OR, Visually required Contacts: Covered in full with prior approval*Number of contact lens boxes may vary based on manufacturer’s packaging.
1 Additional discounts not applicable at Walmart or Sam’s Club locations2 The Davis Vision Collection is available at most participating independent provider locations.
Collection is inclusive of select toric and multifocal contacts. 3 Including, but not limited to toric, multifocal and gas permeable contact lenses.4 Allowance is available at these Visionworks family of store location: Davis Vision,
Empire Vision Centers, Total Vision Care, EyeMasters, Cambridge Eye Doctors, Vision World, Dr. Bizer’s Vision World, Eye Dr, Dr. Bizer’s Valu Vision, Doctor’s Valu Vision, Hour Eyes, Visionworks.
22
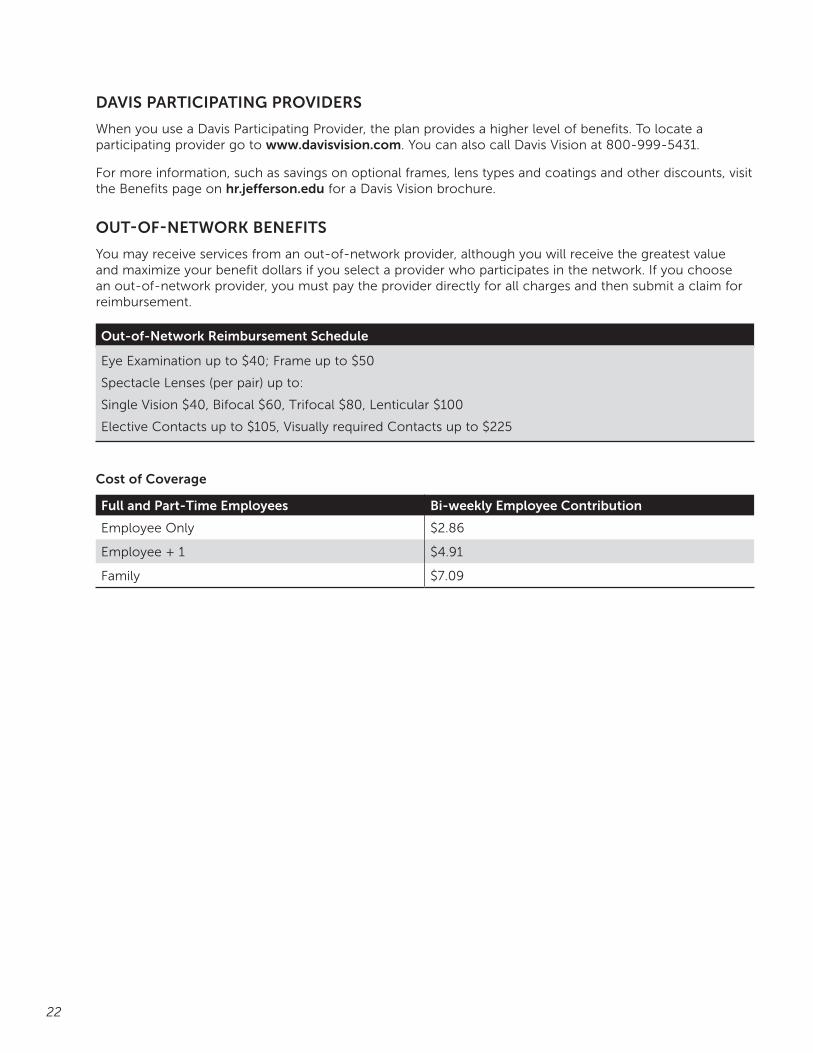
DAVIS PARTICIPATING PROVIDERS
When you use a Davis Participating Provider, the plan provides a higher level of benefits. To locate a participating provider go to www.davisvision.com. You can also call Davis Vision at 800-999-5431.
For more information, such as savings on optional frames, lens types and coatings and other discounts, visit the Benefits page on hr.jefferson.edu for a Davis Vision brochure.
OUT-OF-NETWORK BENEFITS
You may receive services from an out-of-network provider, although you will receive the greatest value and maximize your benefit dollars if you select a provider who participates in the network. If you choose an out-of-network provider, you must pay the provider directly for all charges and then submit a claim for reimbursement.
Out-of-Network Reimbursement Schedule
Eye Examination up to $40; Frame up to $50
Spectacle Lenses (per pair) up to:
Single Vision $40, Bifocal $60, Trifocal $80, Lenticular $100
Elective Contacts up to $105, Visually required Contacts up to $225
Cost of Coverage
Full and Part-Time Employees Bi-weekly Employee Contribution
Employee Only $2.86
Employee + 1 $4.91
Family $7.09
23
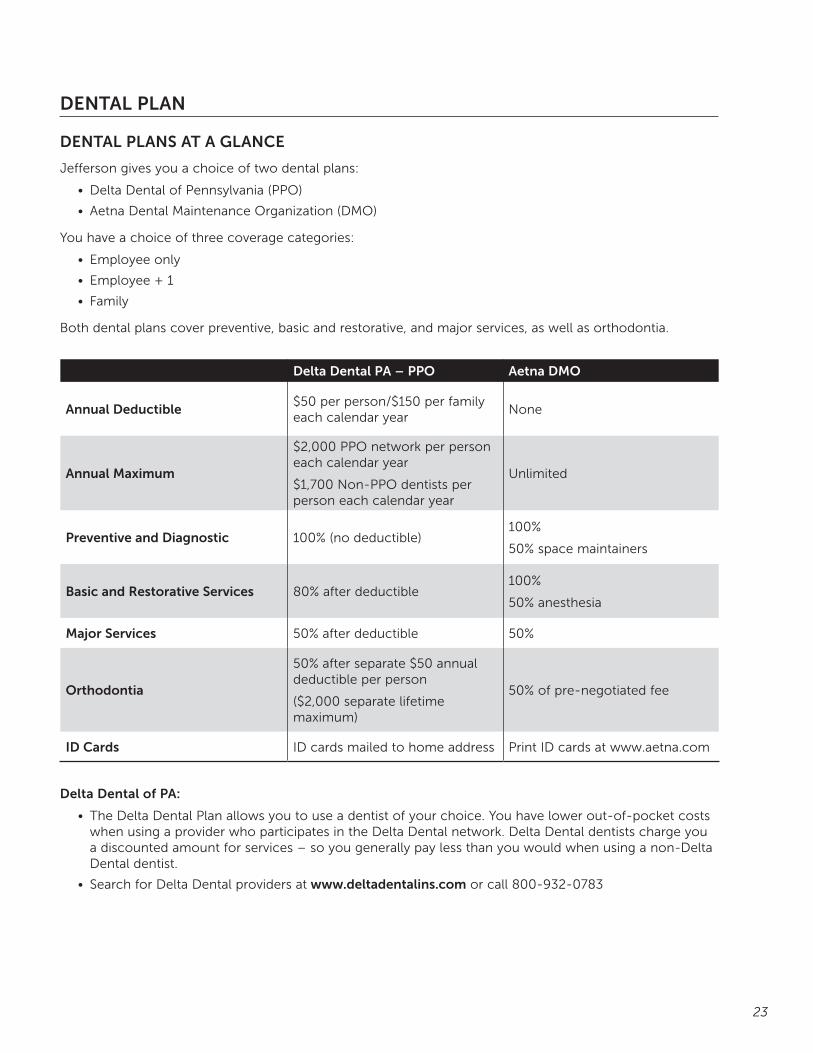
DENTAL PLAN
DENTAL PLANS AT A GLANCE
Jefferson gives you a choice of two dental plans:
• Delta Dental of Pennsylvania (PPO)
• Aetna Dental Maintenance Organization (DMO)
You have a choice of three coverage categories:
• Employee only
• Employee + 1
• Family
Both dental plans cover preventive, basic and restorative, and major services, as well as orthodontia.
Delta Dental PA – PPO Aetna DMO
Annual Deductible$50 per person/$150 per family each calendar year
None
Annual Maximum
$2,000 PPO network per person each calendar year
$1,700 Non-PPO dentists per person each calendar year
Unlimited
Preventive and Diagnostic 100% (no deductible)100%
50% space maintainers
Basic and Restorative Services 80% after deductible100%
50% anesthesia
Major Services 50% after deductible 50%
Orthodontia
50% after separate $50 annual deductible per person
($2,000 separate lifetime maximum)
50% of pre-negotiated fee
ID Cards ID cards mailed to home address Print ID cards at www.aetna.com
Delta Dental of PA:
• The Delta Dental Plan allows you to use a dentist of your choice. You have lower out-of-pocket costs when using a provider who participates in the Delta Dental network. Delta Dental dentists charge you a discounted amount for services – so you generally pay less than you would when using a non-Delta Dental dentist.
• Search for Delta Dental providers at www.deltadentalins.com or call 800-932-0783
24
Aetna Dental Maintenance Organization (DMO)
• The Aetna DMO provides benefits through a participating network of dental professionals. You must choose a Primary Care Dentist (PCD) for you and each family member. Once your enrollment has been processed, select a PCD by calling 800-THEDMO1
• Your PCD must provide dental care services, or a written referral for care by a DMO specialist, as appropriate. Otherwise, the plan will not pay benefits, except in an emergency.
• There are no claim forms to complete when you use an Aetna DMO provider
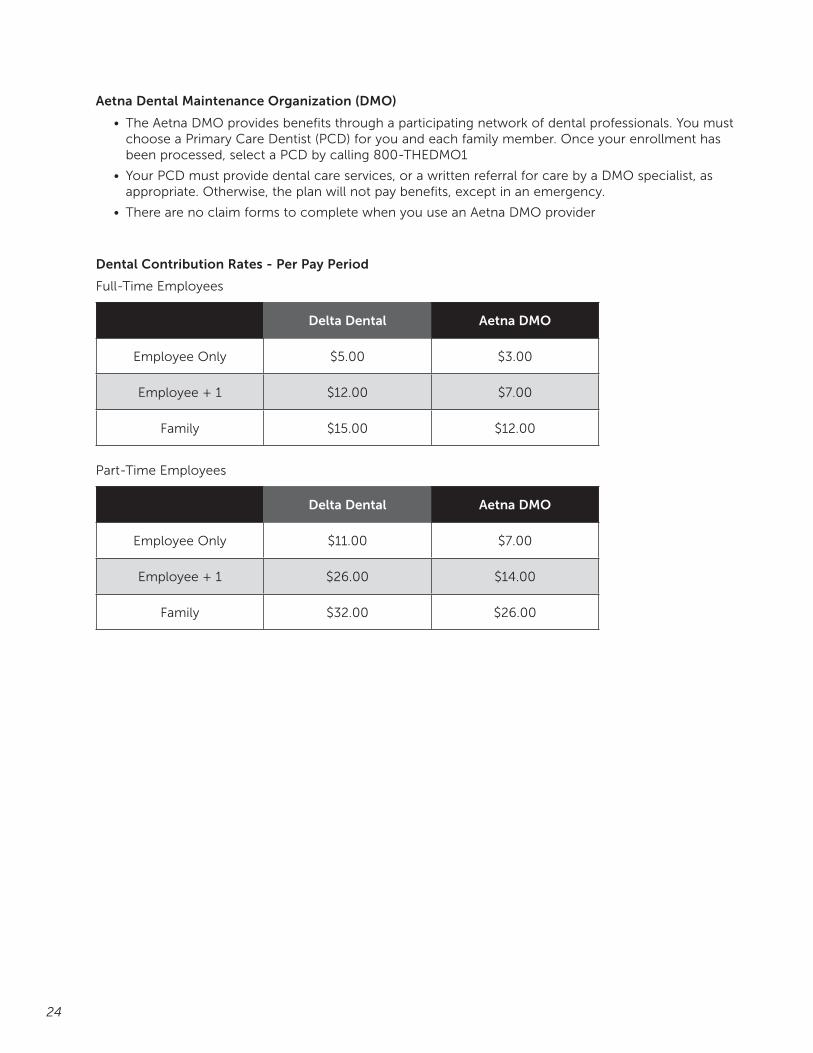
Dental Contribution Rates - Per Pay Period
Full-Time Employees
Delta Dental Aetna DMO
Employee Only $5.00 $3.00
Employee + 1 $12.00 $7.00
Family $15.00 $12.00
Part-Time Employees
Delta Dental Aetna DMO
Employee Only $11.00 $7.00
Employee + 1 $26.00 $14.00
Family $32.00 $26.00
25
LIFE INSURANCE PLANS
BASIC LIFE AND AD&D INSURANCE COVERAGE
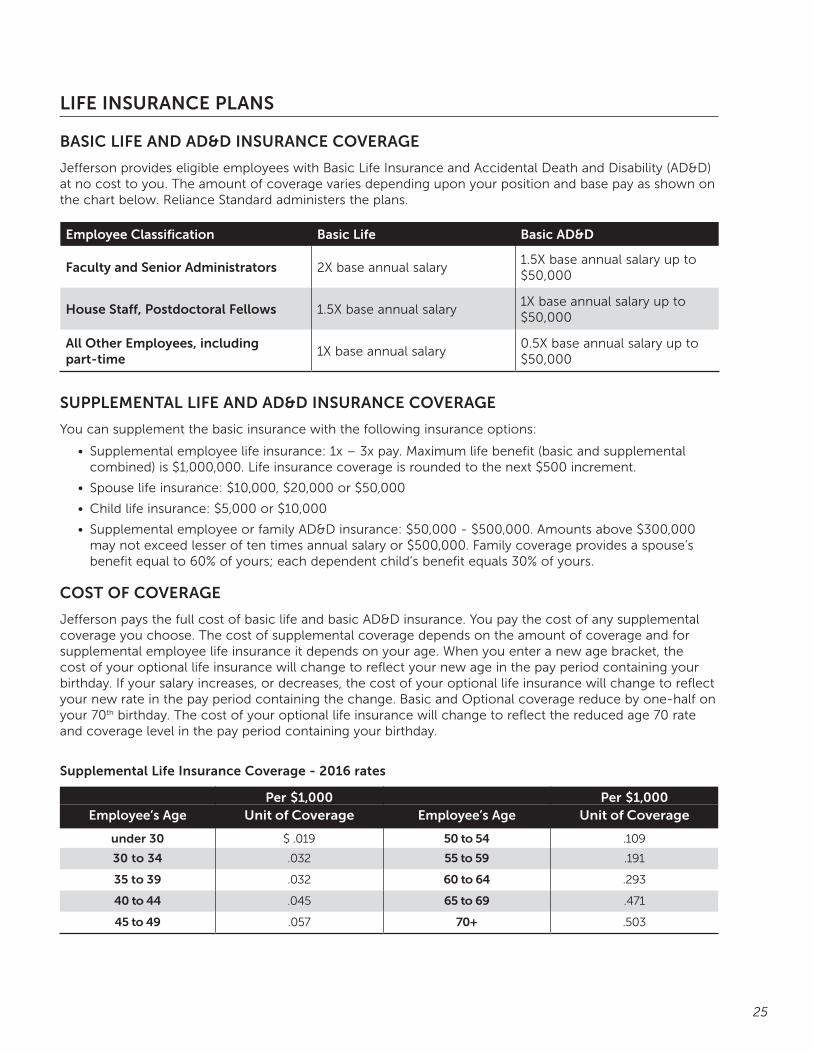
Jefferson provides eligible employees with Basic Life Insurance and Accidental Death and Disability (AD&D) at no cost to you. The amount of coverage varies depending upon your position and base pay as shown on the chart below. Reliance Standard administers the plans.
Employee Classification Basic Life Basic AD&D
Faculty and Senior Administrators 2X base annual salary1.5X base annual salary up to $50,000
House Staff, Postdoctoral Fellows 1.5X base annual salary 1X base annual salary up to $50,000
All Other Employees, including part-time
1X base annual salary0.5X base annual salary up to $50,000
SUPPLEMENTAL LIFE AND AD&D INSURANCE COVERAGE
You can supplement the basic insurance with the following insurance options:
• Supplemental employee life insurance: 1x – 3x pay. Maximum life benefit (basic and supplemental combined) is $1,000,000. Life insurance coverage is rounded to the next $500 increment.
• Spouse life insurance: $10,000, $20,000 or $50,000
• Child life insurance: $5,000 or $10,000
• Supplemental employee or family AD&D insurance: $50,000 - $500,000. Amounts above $300,000 may not exceed lesser of ten times annual salary or $500,000. Family coverage provides a spouse’s benefit equal to 60% of yours; each dependent child’s benefit equals 30% of yours.
COST OF COVERAGE
Jefferson pays the full cost of basic life and basic AD&D insurance. You pay the cost of any supplemental coverage you choose. The cost of supplemental coverage depends on the amount of coverage and for supplemental employee life insurance it depends on your age. When you enter a new age bracket, the cost of your optional life insurance will change to reflect your new age in the pay period containing your birthday. If your salary increases, or decreases, the cost of your optional life insurance will change to reflect your new rate in the pay period containing the change. Basic and Optional coverage reduce by one-half on your 70th birthday. The cost of your optional life insurance will change to reflect the reduced age 70 rate and coverage level in the pay period containing your birthday.
Supplemental Life Insurance Coverage - 2016 rates
Per $1,000 Per $1,000Employee’s Age Unit of Coverage Employee’s Age Unit of Coverage
under 30 $ .019 50 to 54 .109
30 to 34 .032 55 to 59 .191
35 to 39 .032 60 to 64 .293
40 to 44 .045 65 to 69 .471
45 to 49 .057 70+ .503
26
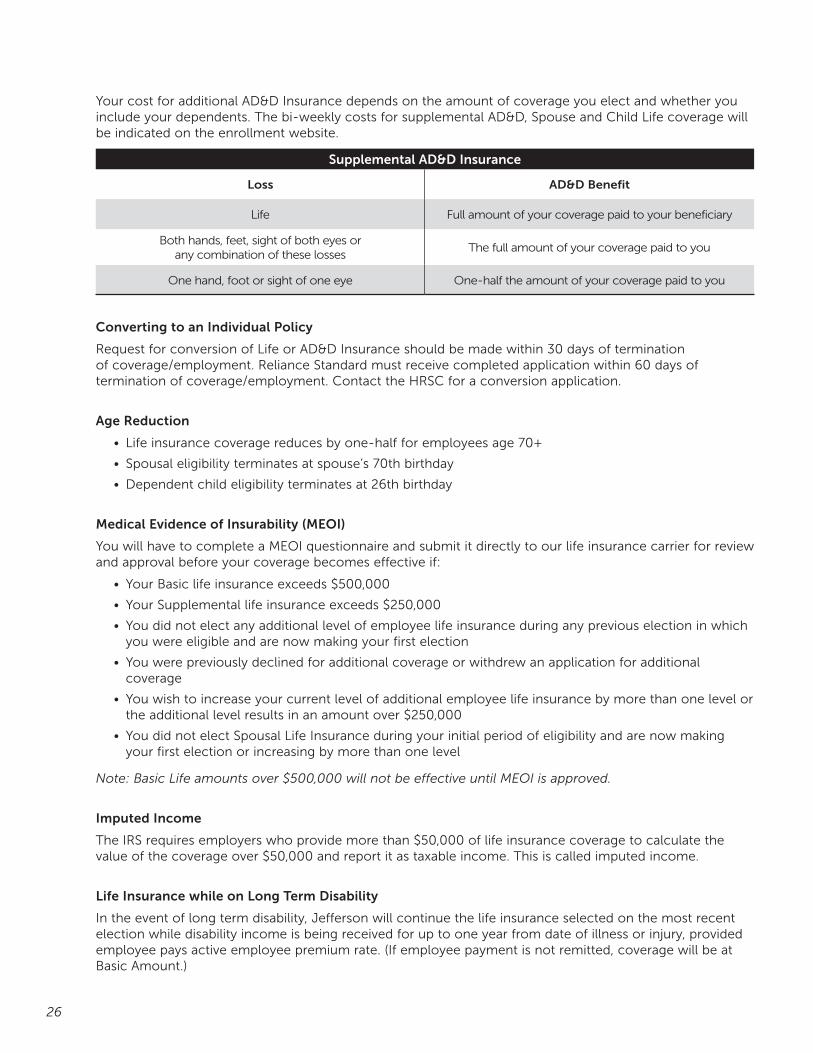
Your cost for additional AD&D Insurance depends on the amount of coverage you elect and whether you include your dependents. The bi-weekly costs for supplemental AD&D, Spouse and Child Life coverage will be indicated on the enrollment website.
Supplemental AD&D Insurance
Loss AD&D Benefit
Life Full amount of your coverage paid to your beneficiary
Both hands, feet, sight of both eyes or any combination of these losses
The full amount of your coverage paid to you
One hand, foot or sight of one eye One-half the amount of your coverage paid to you
Converting to an Individual Policy
Request for conversion of Life or AD&D Insurance should be made within 30 days of termination of coverage/employment. Reliance Standard must receive completed application within 60 days of termination of coverage/employment. Contact the HRSC for a conversion application.
Age Reduction
• Life insurance coverage reduces by one-half for employees age 70+
• Spousal eligibility terminates at spouse’s 70th birthday
• Dependent child eligibility terminates at 26th birthday
Medical Evidence of Insurability (MEOI)
You will have to complete a MEOI questionnaire and submit it directly to our life insurance carrier for review and approval before your coverage becomes effective if:
• Your Basic life insurance exceeds $500,000
• Your Supplemental life insurance exceeds $250,000
• You did not elect any additional level of employee life insurance during any previous election in which you were eligible and are now making your first election
• You were previously declined for additional coverage or withdrew an application for additional coverage
• You wish to increase your current level of additional employee life insurance by more than one level or the additional level results in an amount over $250,000
• You did not elect Spousal Life Insurance during your initial period of eligibility and are now making your first election or increasing by more than one level
Note: Basic Life amounts over $500,000 will not be effective until MEOI is approved.
Imputed Income
The IRS requires employers who provide more than $50,000 of life insurance coverage to calculate the value of the coverage over $50,000 and report it as taxable income. This is called imputed income.
Life Insurance while on Long Term Disability
In the event of long term disability, Jefferson will continue the life insurance selected on the most recent election while disability income is being received for up to one year from date of illness or injury, provided employee pays active employee premium rate. (If employee payment is not remitted, coverage will be at Basic Amount.)
27
BUSINESS TRAVEL ACCIDENT INSURANCE
HOW THE PLAN WORKS
Business Travel Accident insurance provides additional coverage when Full-Time employees regularly scheduled to work at least 35 hours a week travel off Jefferson premises on Jefferson business. If an eligible employee is injured or killed while traveling on Jefferson business, his/her beneficiary may receive an additional benefit based upon the nature of the injury. AIG administers the plan.
COST OF COVERAGE
Jefferson pays the full cost of business travel accident insurance.
• For more information on plan features see the Business Travel Accident Insurance Coverage Summary and AIG Benefits Travel Assist brochure on hr.jefferson.edu

28
DISABILITY PLANSThe Benefits Program offers you protection from income loss while you are out of work for a non-work related illness or injury. You are considered to be disabled when a treating health professional certifies that your illness, injury or medical condition keeps you from working. Disability benefits at Jefferson are made up of different programs, depending upon your position, including:
• Earned Time Off (ETO), Sick Pay or Salary Continuation
• Short Term Disability
• Long Term Disability
SHORT-TERM DISABILITY
Eligibility
Full-time employees and full-time Postdoctoral Fellows regularly scheduled to work at least 35 hours a week are eligible for short-term disability insurance. For regular staff, benefits begin on the first of the month following date of hire. Postdoctoral Fellows are eligible date of hire. Full-time Faculty, full-time Senior Administrators, and House Staff, benefits begin on date of hire, and have a separate salary continuation program.
Your Short-Term Disability Choices
• Basic STD Plan that pays 50% of your weekly pay. No premium cost to the employee
• Optional STD Plan pays 66 2/3% of your weekly pay. Employee pays cost of additional 16 2/3%
How the Short-Term Disability Plan Works
The Short-Term Disability (STD) plan provides benefits after seven consecutive calendar days of disability. All disabilities must be approved by Cigna, our third party administrator. STD continues for 26 weeks as long as you continue to be disabled. For the first seven calendar days of a disability, employees use Earned Time Off (ETO) or Sick Time based upon their position. Employees who have an Extended Illness Bank (EIB) will then be paid 100% of base pay until the bank is exhausted. If the employee remains on leave after EIB is exhausted, benefits will then be paid from the STD Plan(s). To qualify for short or long term disability you must be actively at work prior to your date of disability.
How Salary Continuation Works for Full-time Faculty, Senior Administrators and House Staff
Full-time faculty, senior administrators and house staff will receive salary continuation of 100% of base salary for up to 26 weeks in the event of disability. All salary continuations must be approved by Cigna for any absences over three calendar days under FMLA.
Cost of Coverage (Except Clinical Faculty)
Jefferson pays the full cost of Basic STD. You pay the cost of supplemental coverage. The cost of supplemental coverage depends on your salary. You can see the cost of optional STD when you enroll in benefits in Employee Self-Service.
You may wish to elect the Optional STD benefit if:
• The 50% Basic STD benefit will not meet your income needs while disabled; or
• You do not have enough EIB time to carry you in the event of a disability that lasts up to 26 weeks (6 months)

29
Pre-Existing Conditions
Pre-existing condition limits apply to the Optional STD Plan. A pre-existing condition exists if you have received medical treatment, consultations, diagnostic services or have taken prescription drugs for a condition in the three month period before your effective date of coverage. The pre-existing condition limitation applies for the next 12 months, unless you go without treatment or medication for any three month period within the same 12 month period. If you have a pre-existing condition, Optional STD benefits (662/3%) will be paid for the first four weeks of disability; then Basic STD benefits (50%) will be paid.
Filing an STD Claim
All employees covered by one of the STD plans; salary continuation, sick time or ETO must file an STD claim with Cigna, our Third Party Administrator. Cigna determines if the disability qualifies and initiates STD payments for employees covered by that plan. There are two ways to file a claim with Cigna:
1. Call 855-689-6673
2. File online at mycigna.com
It is recommended you file a claim as soon as you are aware that you will be out of work for an extended period of time, preferably within the first 30 days, but no later than 12 months after the date of disability. You may file an STD claim with Cigna at the same time you apply for FMLA or another leave. STD benefits may apply independent of the type of leave you qualify for. In all instances Cigna will review your application for STD and notify you whether your disability is approved or denied.
Attention employees working in New Jersey:
If you work in New Jersey, both you and Jefferson pay a tax to fund the New Jersey short-term disability plan. The New Jersey State Disability Plan is mandatory and covers approximately 662/3% of your salary up to a maximum of $604.00 per week. If you work in New Jersey, you may elect to waive the Jefferson optional short-term disability option on your online election due to coverage from the New Jersey State Plan, or you may choose to make a selection if you desire coverage over and above the New Jersey Plan limits. The benefit you receive from Jefferson will be offset automatically by your New Jersey State benefit. For example, if you choose option B, which is 662/3% of your weekly salary, and your present weekly salary is $1,000.00 you would be entitled to a benefit of $667.00 per week. You would receive the maximum benefit from the State of New Jersey which is presently $604.00 per week. The additional $63.00 per week would be paid to you from Jefferson’s Disability Plan.

30
LONG-TERM DISABILITY
Eligibility
Full-time employees, Postdoctoral Fellows, House Staff, Faculty and Senior Administrators regularly scheduled to work at least 35 hours a week are eligible for long-term disability insurance. For regular staff, benefits begin on the first of the month following date of hire. Postdoctoral Fellows, House Staff, Faculty and Senior Administrators are eligible date of hire. Clinical full-time Faculty has a separate Long-Term Disability program.
Your Long-Term Disability Choices (Except Clinical Faculty)
• Basic LTD that pays 50% of your base monthly salary. This plan is provided by Jefferson.
• Optional LTD that pays 60% of your base monthly salary if you elect optional coverage.
• Optional LTD Plan pays 66 2/3% of your base monthly salary if you elect optional coverage. (For this option House Staff is 70% coverage)
How the Long-Term Disability Plan Works (Except Clinical Faculty)
The Long-Term Disability (LTD) plan provides benefits after 180 initial days of disability. LTD benefits may continue for as long as you remain totally disabled until age 65 or older. To qualify for long term disability, you must be actively at work prior to your date of disability.
The maximum monthly benefit is $12,500 for most employees. $15,000 is the maximum for House Staff.
Cost of Coverage
Jefferson pays the full cost of Basic LTD. You pay the cost of any optional coverage you choose. The cost of supplemental coverage depends on your salary. You can see the cost of optional coverage when you enroll in benefits in Employee Self-Service.
Pre-Existing Conditions
Pre-existing condition limits apply to the LTD options. A pre-existing condition means any sickness or injury for which you received medical treatment, consultation, care or services, including diagnostic procedures, or took prescribed drugs or medicines, during the ninety (90) days immediately prior to your effective date of insurance.
LTD benefits will not be payable for any disability that results from a pre-existing medical condition, unless the disability begins:
• After the last day of 90 consecutive days during which you have received no medical care for the pre-existing condition; or
• After the last of 12 consecutive months during which you have been continuously insured under this plan.
LTD Benefit Period
LTD benefits are reduced by income from other sources of disability income such as Social Security, other government programs and Workers Compensation so that no more than 100% of the benefit due under the plan is paid when considering other payments.
All LTD benefits, except those for House Staff have a 24 month own occupation and mental illness limit. This chart shows the maximum length of time you may receive benefits through the LTD plan.
31
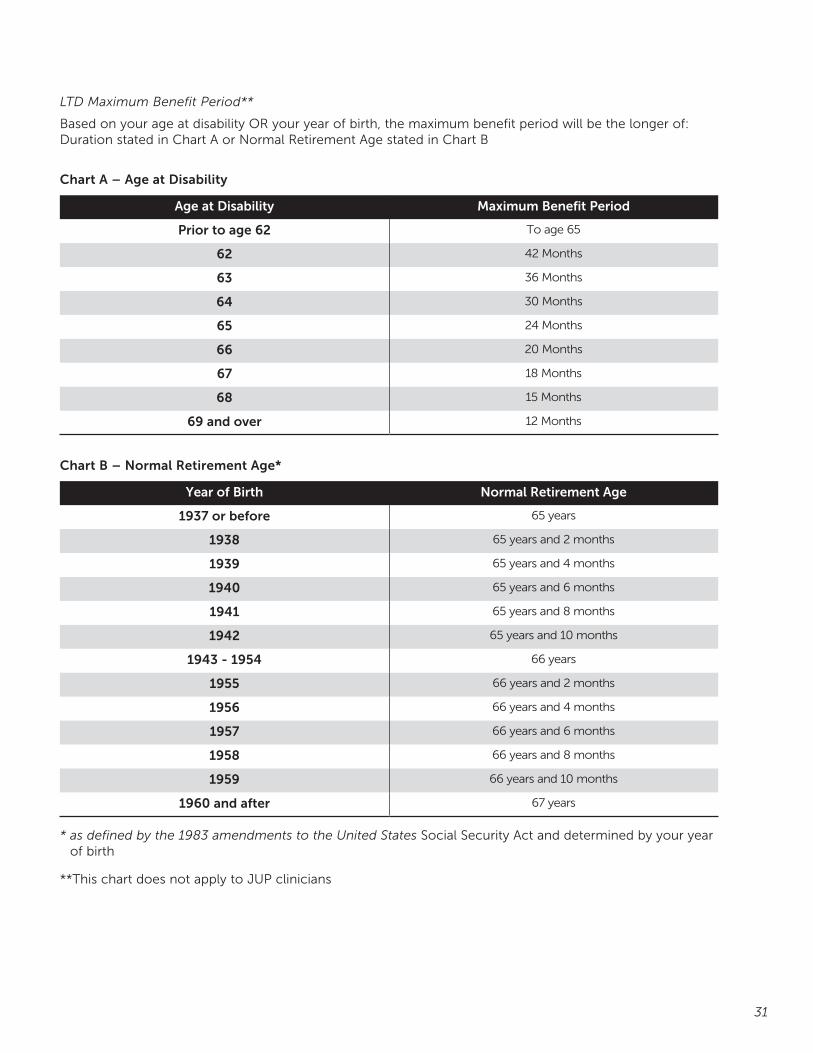
LTD Maximum Benefit Period**
Based on your age at disability OR your year of birth, the maximum benefit period will be the longer of: Duration stated in Chart A or Normal Retirement Age stated in Chart B
Chart A – Age at Disability
Age at Disability Maximum Benefit Period
Prior to age 62 To age 65
62 42 Months
63 36 Months
64 30 Months
65 24 Months
66 20 Months
67 18 Months
68 15 Months
69 and over 12 Months
Chart B – Normal Retirement Age*
Year of Birth Normal Retirement Age
1937 or before 65 years
1938 65 years and 2 months
1939 65 years and 4 months
1940 65 years and 6 months
1941 65 years and 8 months
1942 65 years and 10 months
1943 - 1954 66 years
1955 66 years and 2 months
1956 66 years and 4 months
1957 66 years and 6 months
1958 66 years and 8 months
1959 66 years and 10 months
1960 and after 67 years
* as defined by the 1983 amendments to the United States Social Security Act and determined by your year of birth
**This chart does not apply to JUP clinicians

32
Your Long-Term Disability Choices (Clinical Faculty)
Three levels of benefits available:
• Base benefit: Employer paid Group LTD 50% of pay up to $15,000 monthly benefit
Optional individual policies:
• Employer paid individual disability 60% less LTD to $2,500 monthly benefit
• Employee paid optional individual disability 60% less LTD to $7,500 monthly benefit. Eligibility subject to compensation
Aon Hewitt, our broker for the individual policies, will be in touch with newly eligible JUP Clinicians to offer more information and help with enrollment.
How the Long-Term Disability Plan Works (Clinical Faculty)
The Long-Term Disability (LTD) plan provides benefits after 180 initial days of disability. To qualify for long term disability, you must be actively at work prior to your date of disability.
Pre-Existing Conditions (Clinical Faculty)
Pre-existing conditions may apply.
LTD Benefit Period (Clinical Faculty)
The maximum benefit period is age 65. For disabilities occurring between ages 65 and 75, the maximum benefit period is 24 months. For disabilities occurring after age 75, the maximum benefit period is 12 months.

33
FLEXIBLE SPENDING ACCOUNTSJefferson offers two types of Flexible Spending Accounts (FSAs) to help you save tax dollars on certain health care and dependent care expenses. Based upon your annual election for contributions, money is deducted each pay from your paycheck, before taxes are calculated. This saves you money because you do not pay certain state and federal income tax on the contributions.
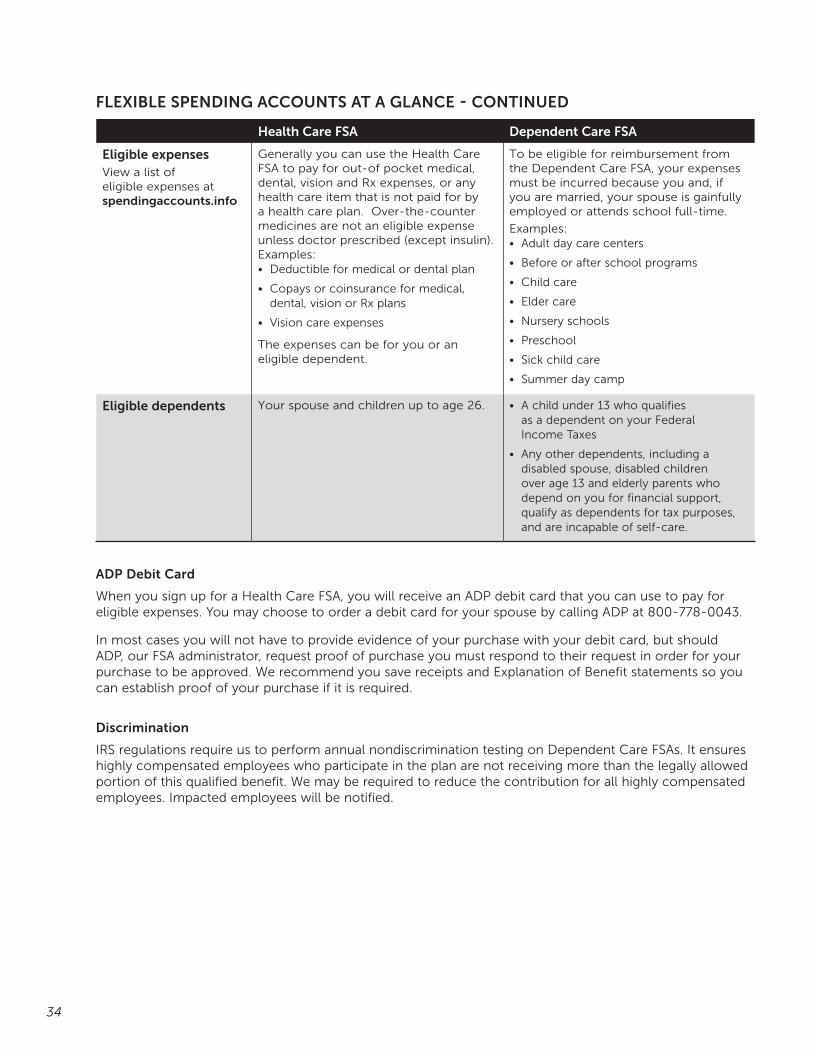
FLEXIBLE SPENDING ACCOUNTS AT A GLANCE
Health Care FSA Dependent Care FSA
How it works Enables you to use pre-tax earnings to pay for certain health care expenses for you and your eligible dependents.
Helps you pay for dependent care services that make it possible for you and your spouse, if applicable, to work. You can use your pre-tax earnings to pay for eligible child and adult day care services.
How much you can contribute each year
Minimum: $5.00 per pay
Maximum: $2,550
Minimum: $5.00 per pay
Maximum: Generally, $5,000:• If you are married and your spouse also
has a dependent care FSA, the combined limit is $5,000
• If you are married and file a separate tax return, your limit is $2,500
• If you are married, you cannot contribute more than the lower of your or your spouse’s annual salary
Getting reimbursed • Pay for services with your ADP debit card
• Prepay for the service and submit a claim form for reimbursement with proof of payment as well as an Explanation of Benefits from your health insurance company to ADP for reimbursement
• You may choose to receive a check or have money direct deposited to your bank account
• Submit a claim form with a copy of the paid receipt showing the Social Security number or tax ID number of the provider
• You may choose to receive a check or have money direct deposited to your bank account
Unused dollars In accordance with IRS regulations, if you have money left in your spending accounts at the end of the year, you will lose it. You have until March 15th of the following plan year to incur expenses. You have until June 30th of the following plan year to submit expenses for reimbursement.
Use the FSA accounts only if you can anticipate your qualified expenses for the coming Plan Year. If you are certain that you will have qualified expenses during the Plan Year, but are unsure of the amount, be conservative in the amount of salary you direct to your FSAs.
IRS regulations currently require that all salary directed to your FSA in any one year must be used to reimburse you for qualified expenses incurred during that plan year.
34
Health Care FSA Dependent Care FSA
Eligible expensesView a list of eligible expenses at spendingaccounts.info
Generally you can use the Health Care FSA to pay for out-of pocket medical, dental, vision and Rx expenses, or any health care item that is not paid for by a health care plan. Over-the-counter medicines are not an eligible expense unless doctor prescribed (except insulin). Examples:• Deductible for medical or dental plan
• Copays or coinsurance for medical, dental, vision or Rx plans
• Vision care expenses
The expenses can be for you or an eligible dependent.
To be eligible for reimbursement from the Dependent Care FSA, your expenses must be incurred because you and, if you are married, your spouse is gainfully employed or attends school full-time.
Examples:• Adult day care centers
• Before or after school programs
• Child care
• Elder care
• Nursery schools
• Preschool
• Sick child care
• Summer day camp
Eligible dependents Your spouse and children up to age 26. • A child under 13 who qualifies as a dependent on your Federal Income Taxes
• Any other dependents, including a disabled spouse, disabled children over age 13 and elderly parents who depend on you for financial support, qualify as dependents for tax purposes, and are incapable of self-care.
ADP Debit Card
When you sign up for a Health Care FSA, you will receive an ADP debit card that you can use to pay for eligible expenses. You may choose to order a debit card for your spouse by calling ADP at 800-778-0043.
In most cases you will not have to provide evidence of your purchase with your debit card, but should ADP, our FSA administrator, request proof of purchase you must respond to their request in order for your purchase to be approved. We recommend you save receipts and Explanation of Benefit statements so you can establish proof of your purchase if it is required.
Discrimination
IRS regulations require us to perform annual nondiscrimination testing on Dependent Care FSAs. It ensures highly compensated employees who participate in the plan are not receiving more than the legally allowed portion of this qualified benefit. We may be required to reduce the contribution for all highly compensated employees. Impacted employees will be notified.
FLEXIBLE SPENDING ACCOUNTS AT A GLANCE - CONTINUED

35
FSA Store
ADP has a relationship with FSA store. If you shop at the FSA Store you will have access to thousands of FSA-eligible products. You can pay for your purchases with your FSA debit card, or other major credit card. The FSA Store clearly designates which over-the-counter items for sale are available for purchase with and without a doctor’s prescription. Visit FSAStore.com for more information.
Additional Information
• You must re-enroll for FSA account(s) every plan year during open enrollment.
• You cannot change the amount of your contribution during the plan year unless you have a life event such as marriage, birth, or change of job that impacts benefits.
• You cannot be reimbursed for dependent care (i.e. daycare) from your Healthcare FSA nor can you be reimbursed for medical expenses from your Dependent Care account.
• Expenses are considered incurred on the date the services are provided, not when paid.
• For more information on FSAs consult spendingaccounts.info or call ADP Customer Service at 800-778-0043.
• Once you are enrolled in an FSA, you can manage your account online at myspendingaccount.adp.com, which includes filing claims online and setting up direct deposit.

36
VOLUNTARY BENEFITS
BENEFITS PLUS
Benefits Plus is a voluntary benefits program that provides employees with access to group rates on insurance and discounts - with the convenience of a single payroll deduction. The program offers:
• Critical Illness Insurance
• Accident Insurance
• Auto and home insurance
• Pre-paid Legal
• Pet insurance
• Purchasing Power for big-ticket items
• Shopping Discounts
• Membership Discounts at local gyms. Visit the Benefits Plus website and click on Sports & Fitness.
Cost of Coverage
You pay the full cost of coverage, but benefit from group discounted rates. You will have one Jefferson payroll deduction for all of the plans you choose through Benefits Plus. The cost of each coverage is available on the Benefits Plus website. www.jeffersonbenefitsplus.com
How to Get More Information
For more information, call Benefits Plus Customer Care (855) 515-5800.
Plan summaries and detailed information is available on the www.jeffersonbenefitsplus.com
37
YOUR OTHER BENEFITSOther benefits may include the following, depending on your employment status:
• Retirement Plan
• Tuition Assistance Program
• Dependent Scholarship for Faculty and Senior Administrators
• Vacation or Earned Time Off
Retirement Plans
Jefferson provides Retirement Plans for eligible employees.
Auto-Enrollment/Employee Contributions
All employees hired on or after January 1, 2016 will be automatically enrolled to make a biweekly employee contribution equal to 6% of base plus incentive compensation to the Jefferson Defined Contribution Retirement Plan or Jefferson University Physicians Voluntary 403b Program, unless employee instructs TIAA-CREF otherwise.
Once notified of eligibility following receipt of first paycheck, employees will have thirty days (30) from date of receipt of letter from TIAA-CREF to contact TIAA-CREF to waive, reduce, or increase this contribution level before auto-enrollment takes effect. Future contribution level may also then be changed at any time by contacting TIAA-CREF online or by phone.
All employees are eligible to make biweekly employee tax deferred contributions to the Jefferson Defined Contribution Retirement Plan or the Jefferson University Physicians Voluntary 403b Program.
Employer Contributions
The Jefferson Defined Contribution Retirement Plan and Jefferson University Physicians Retirement Plan provide biweekly employer contributions toward retirement to TJU Faculty, TJU/TJUH Senior Administrators, and JUP Employees and Clinicians.
The Jefferson Defined Contribution Retirement Plan provides annual fixed employer contributions and biweekly partial matching of employee contributions to eligible non-bargaining employees after one year of service.
The Jefferson Employees’ Pension Plan for other eligible non-bargaining employees hired prior to 2014 provides monthly benefits when an eligible participant reaches retirement age. Benefits are determined by the Plan’s formula, which takes into account earnings and length of service with Jefferson.
Tax Deferred Annuity Programs
All employees are eligible to participate in Jefferson’s Tax Deferred Annuity programs. Voluntary pre-tax contributions may be made to a 403(b) account to supplement your retirement income. For more information, please contact TIAA-CREF at 800-842-2888.

38
Tuition Assistance Program
Regular full-time non-bargaining employees are eligible for the Tuition Assistance Program.
Internal External
Calendar Year Maximum(Jan 1- Dec 31)
90% to maximum $5,000 undergraduate/$7,500 graduate per calendar year
80% to maximum $3,000 undergraduate/$5,000 graduate per calendar year
All courses that begin in the current calendar year are considered when calculating the maximum amount for the year.
Eligibility Full time, non-bargaining employees are eligible after 60 days of benefit eligible service
Full time, non-bargaining employees are eligible after 6 months of benefit eligible service
Requirements • Credited courses offered in a degree or certificate program
• Courses must be related to position at Jefferson
• Benefits provided for tuition charges only
• Credited courses taken in a program leading towards an Associate, Bachelor, Graduate or Doctorate degree
• Sponsored by an accredited institution through the Council for Higher Education Accreditation List (www.chea.org)
• Courses must be related to position at Jefferson
Repayment Terms • If you do not remain in the employ of Jefferson for one year subsequent to the completion of the courses, you will be required to reimburse Jefferson either through payroll deductions or personal check for the amount of tuition benefits received.
• If you do not satisfactorily complete all courses with a grade C or better, you will be required to reimburse Jefferson either through payroll deductions or personal check for the amount of tuition benefits received.
For additional information, contact the Human Resources Service Center at 215-503-HRSC (4772). The Tuition Assistance Program application can be found on the HR website hr.jefferson.edu
Dependent Scholarship Program
Full-time Faculty and Senior Administrators are eligible for Jefferson’s Dependent Scholarship Program, which provides eligible, unmarried dependent children up to age 30 with yearly assistance for educational expenses as undergraduate students at any CHEA accredited college, university or school of nursing. Dependent scholarship benefits are payable for up to four years of study towards an undergraduate degree.

39
Earned Time Off (ETO)
All eligible non-bargaining employees receive ETO based upon their job title and length of service. Generally, ETO is allotted to the following schedules:
Service ETO
up to 5 years 23 days
up to 10 years 28 days
10 or more years 33 days
ETO does not apply to Full-Time Faculty, Full-Time Senior Administrators, Postdoctoral Fellows and House Staff.
Vacation
Full-Time Faculty, Senior Administrators, Postdoctoral Fellows and House Staff receive vacation time based upon their job title and length of service. Generally, vacation time is allotted according to the following schedules:
• Faculty and Senior Administrators: 20 days a year
• House staff G-1 level, 10 days per year. All others, 20 days per year
• Postdoctoral Fellows, 10 days per year
Other Voluntary Programs and Facilities offered by Jefferson
More information on the following benefits can be found on the HR website hr.jefferson.edu
• Adoption Assistance
• Blood Donor Club
• Campus Currency
• Carebridge (Work/Life Balance assistance)
• Cell Phone Discounts
• Commuter Services and Discounts
• Daycare Services and Discounts
• Direct Payroll Deposit
• Discount Entertainment Tickets
• Exos
• First Call (Employee Assistance Program)
• Freedom Credit Union
• JeffConnect (telehealth)
• Jefferson Fitness & Recreation Center
• Library Privileges
Please Note: Specific eligibility requirements apply to the benefit plans identified in this booklet. Your entitlement to any of the benefits listed herein is expressly conditioned upon, and subject to, your meeting such eligibility requirements as provided in the plans. You may not rely upon this booklet as a determination as to your qualification or eligibility for such benefits. Detailed information is provided during the benefits orientation and enrollment session. If there is a difference between the statements in this booklet and in the contracts regarding the nature and extent of the benefits, the benefits will be determined in accordance with the language of the insurance contracts.

40
2016 BENEFITS SERVICE PROVIDER CONTACT LIST
Human Resources Service Center 215-503-4772 [email protected]
VENDOR PHONE WEBSITE
BANKING
Freedom Credit Union 215-612-5900 www.freedomcu.org
COBRA
ADP 800-778-0043
DENTAL
Aetna DMO
Delta Dental (group #2564)
800-THEDMO-1
800-932-0783
www.aetna.com
www.deltadentalins.com
DISABILITY
CIGNA (Short and Long Term Disability) 855-689-6673 mycigna.com
Aon Hewitt (Long Term Disability for Physicians) 877-815-6366
FMLA (FAMILY MEDICAL LEAVE ACT)
CIGNA 855-689-6673 mycigna.com
FLEXIBLE SPENDING ACCOUNT
ADP
ADP (pre-enrollment education)
800-778-0043 myspendingaccount.adp.com
spendingaccounts.info
LIFE INSURANCE
Reliance Standard (Life Insurance and AD&D) 800-351-7500 www.reliancestandard.com
MEDICAL
IBC Health Plans 800-ASK-BLUE www.ibx.com
JEFF NOW (Physician Referral Service for Employees) 855-JEFF-123 www.jeffersonhospital.org/finddoctor
Jeff Networks (Jefferson Health System’s link to ACO Plus and JeffPLUS) www.jeffnetworks.org
Blue Card PPO Network (National Blue Cross Network) 800-810-BLUE www.bcbs.com
MEDICARE SUPPLEMENTAL PLANS
Independence Blue Cross 877-393-6733 www.ibx.com
PRESCRIPTION
OptumRx 800-797-9791 www.optumrx.com
RETIREMENT
TIAA-CREF (TDAs and Retirement Plans) 800-842-2888 www.tiaa-cref.org/jefferson
TIAA-CREF (to schedule individual counseling sessions) 800-842-2888 www.tiaa-cref.org/schedulenow
Aon Hewitt Your Pension Resources™ (DB Pension Plans) 855-354-6942 www.yourbenefitresources.com/jeffersonretirement
Social Security Administration/Medicare 800-772-1213 www.ssa.gov
VISION
Davis Vision 800-999-5431 www.davisvision.com
WELLNESS (LIVEWELL@JEFF)
RedBrick Health 877-263-3554 MyRedBrick.com/Jefferson
OTHER VALUABLE BENEFITS
Benefits Plus (Voluntary Benefits) 855-515-5800 www.jeffersonbenefitsplus.com
Carebridge (Work-Life Support Services) Access Code W7SDF 800-437-0911 www.myliferesource.com
First Call (Employee Assistance Program) 800-382-2377 www.firstcalleap.org