The 2012 Digital Edition of General Surgery News Special Edition
48
The Independent Newspaper for the General Surgeon INTERNATIONAL EDITION Vo l ume 1 • 201 2 GE NE RALSURGE RYNE WS.COM Surgeons Discuss Bariatric Options For GERD and Hiatal Hernias Optimal Approach in Some Patients; Insurance Challenge BY MONICA J. SMITH SAN DIEGO—Should bariatric surgery be a part of treatment options for gas- troesophageal reflux disease (GERD) and/or large hiatal hernias in obese patients? “Yes!” said Jon C. Gould, MD, emphatically, at the 2012 meeting of the American Society of Gastro- intestinal and Endoscopic Surgeons (SAGES). Dr. Gould, associate professor of surgery , Medical College of Wiscon- sin and chief, Division of General Surgery, Froedtert Hospital, Milwau- kee, specializes in bariatric surgery, but a large part of his practice is foregut Study T racks Pain 10 Years After Open Hernia Re pai r Proper Nerve Handling the Key BY CHRISTINA F RANGOU NEW YORK—One in six patients who K K reported chronic pain six months after an open inguinal hernia repair still suf- fers from chronic pain 10 years later, according to a prospective German study reported at the Fifth International Her- nia Congress. Others develop late-onset pain, even after five years. “Patients reporting chronic pain vary with time. This is a very important mes- sage,” said lead author Wolfgang Rein- pold, MD, director of the Department of surgery of Gross Sand Hospital and director of the Hernia Center, Hamburg, Germany. The study was initially published in Annals of Surgery in 2011, at which point, only five-year data were available. At this spring’s international hernia meet- ing, Dr. Reinpold presented updated results after conducting a 10-year fol- low-up of the prospective two-phase study. The prospective cohort study fol- lowed 736 patients who underwent 781 elective primary inguinal hernia opera- tions at the Hernia Centre of Reinbek Hospital, Germany, from April 2000 to April 2002. Patients underwent pain Controversy Swi rl s Over Efficacy and Safety of Procedure for Acalashia POEM Procedure Shows Promise, As Experts Urge Caution BY CHRISTINA F RANGOU SAN DIEGO—A new endoscopic ther- apy for achalasia has been dubbed a “ promising new treatment” that could rival conventional methods, after a series of reports from Asia, Europe and North America indicated that peroral endoscopic myotomy (POEM) is safe and effective. Speaking at Digestive Disease Week 2012, Horst Neuhaus, MD, said, “[POEM] promises to be as effective as laparoscopic myotomy or pneu- matic dilation.” Dr. Neuhaus, profes- sor of medicine and head of internal medicine, Evangelisches Kranken- haus Düsseldorf Teaching Hospital of the University Breast Cancer Susceptibility Gene Identified BY GEORGE OCHOA A n international team of researchers has identified a new breast cancer susceptibility gene, XRCC2 (Am J Hum ( ( Genet 2012;90:734-739). In an interview, senior author Melis- sa C. Southey, PhD, Grad Dip Law, FHGSA, FFSc (RCPA), professorial fellow and head of Genetic Epidemiol- ogy Laboratory, and group leader at the Victorian Breast Cancer Research Con- sortium, National Health and Medical Research Council, Australia, stated, “We found a gene that when mutated predis- poses to breast cancer, and this adds to the small collection of breast cancer sus- ceptibility genes previously identified.” By exome sequencing families with multiple individuals affected by breast cancer, the researchers identified two families with XRCC2 mutations. Sub- sequently, two further studies were conducted: One a population-based case-control mutation screening study of XRCC2 and the other additional mutation screening of XRCC2 in index cases from multiple-case families and in male breast cancer cases. The research- ers identified six distinct rare vari- ants in the gene that were predicted to INSIDE ® 40 th ANNIVERSARY YEAR 1972-2012 Opinion In the News The Surgeons’ Lounge: Hernia and Epiphrenic Diverticula. ........................ 6 International Fellowship Program in Laparoscopic Colorectal Surgery......... 18 New App Predicts Chronic Pain After Inguinal Hernia Surgery ............................ 20 see GENE page 8 see HERNIA REPAIR PAIN page 10 see GERD AND HERNIA page 12 see POEM page 26 T echnol ogi cal Advancements i n T issue-Sealing Devices Benefits of GORE® DUALMESH® Biomaterial in Herni a Repai r: A Case-based Presentation REPORT REPORT See insert at page 6 See insert at page 14
-
Upload
mcmahon-group -
Category
Documents
-
view
233 -
download
5
description
The 2012 Digital Edition of General Surgery News Special Edition
Transcript of The 2012 Digital Edition of General Surgery News Special Edition

The Independent Newspaper for the General Surgeon
INTERNATIONAL EDITION Volume 1 • 2012GENERALSURGERYNEWS.COM
Surgeons Discuss Bariatric Options For GERD and Hiatal Hernias
Optimal Approach in Some Patients; Insurance Challenge
BY MONICA J. SMITH
SAN DIEGO—Should bariatric surgery be a part of treatment options for gas-troesophageal reflux disease (GERD) and/or large hiatal hernias in obese patients?
“Yes!” said Jon C. Gould, MD, emphatically, at the 2012 meeting
of the American Society of Gastro-intestinal and Endoscopic Surgeons (SAGES).
Dr. Gould, associate professor of surgery, Medical College of Wiscon-sin and chief, Division of General Surgery, Froedtert Hospital, Milwau-kee, specializes in bariatric surgery, but a large part of his practice is foregut
Study Tracks Pain 10 Years After Open
Hernia RepairProper Nerve Handling the Key
BY CHRISTINA FRANGOU
NEW YORK—One in six patients who KK
reported chronic pain six months after an open inguinal hernia repair still suf-fers from chronic pain 10 years later, according to a prospective German study reported at the Fifth International Her-nia Congress. Others develop late-onset pain, even after five years.
“Patients reporting chronic pain vary with time. This is a very important mes-sage,” said lead author Wolfgang Rein-pold, MD, director of the Department of surgery of Gross Sand Hospital and director of the Hernia Center, Hamburg, Germany.
The study was initially published in Annals of Surgery in 2011, at which point,only five-year data were available. At this spring’s international hernia meet-ing, Dr. Reinpold presented updated results after conducting a 10-year fol-low-up of the prospective two-phase study. The prospective cohort study fol-lowed 736 patients who underwent 781 elective primary inguinal hernia opera-tions at the Hernia Centre of Reinbek Hospital, Germany, from April 2000 to April 2002. Patients underwent pain
Controversy Swirls Over Efficacy and Safety of
Procedure for AcalashiaPOEM Procedure Shows Promise, As Experts Urge Caution
BY CHRISTINA FRANGOU
SAN DIEGO—A new endoscopic ther-apy for achalasia has been dubbed a “promising new treatment” that could rival conventional methods, after a series of reports from Asia, Europe and North America indicated that
peroral endoscopic myotomy (POEM) is safe and effective.
Speaking at Digestive Disease Week 2012, Horst Neuhaus, MD, said, “[POEM] promises to be as effectiveas laparoscopic myotomy or pneu-matic dilation.” Dr. Neuhaus, profes-sor of medicine and head of internal medicine, Evangelisches Kranken-haus Düsseldorf Teaching Hospital of the University
Breast Cancer Susceptibility
Gene Identified
BY GEORGE OCHOA
An international team of researchershas identified a new breast cancer
susceptibility gene, XRCC2 (Am J Hum((Genet 2012;90:734-739).t
In an interview, senior author Melis-sa C. Southey, PhD, Grad Dip Law,FHGSA, FFSc (RCPA), professorialfellow and head of Genetic Epidemiol-ogy Laboratory, and group leader at theVictorian Breast Cancer Research Con-sortium, National Health and MedicalResearch Council, Australia, stated, “Wefound a gene that when mutated predis-poses to breast cancer, and this adds tothe small collection of breast cancer sus-ceptibility genes previously identified.”
By exome sequencing families withmultiple individuals affected by breast cancer, the researchers identified twofamilies with XRCC2 mutations. Sub-sequently, two further studies wereconducted: One a population-basedcase-control mutation screening study of XRCC2 and the other additionalmutation screening of XRCC2 in indexcases from multiple-case families and inmale breast cancer cases. The research-ers identified six distinct rare vari-ants in the gene that were predicted to
INSIDE
®
40th ANNIVERSARY YEAR 1972-2012
Opinion In the News
The Surgeons’ Lounge:Hernia and Epiphrenic Diverticula. ........................ 6
International Fellowship Program in Laparoscopic Colorectal Surgery.........18
New App Predicts Chronic Pain After Inguinal Hernia Surgery ............................ 20
see GENE page 8
see HERNIA REPAIR PAIN page 10
see GERD AND HERNIA page 12
see POEM page 26
Technological Advancements inTissue-Sealing Devices
Benefits of GORE® DUALMESH® Biomaterial inHernia Repair: A Case-based Presentation
REPORT REPORT
See insert at page 6 See insert at page 14

Proven Rel iabi l i ty
GORE® DUALMESH® Biomaterial is a soft, conformable, ePTFE material.
Gore. Because material really does matter.
GORE®, CORDUROY, DUALMESH®
® DUALMESH® Biomaterial
the choice for laparoscopic ventral hernia repair

The staff of General Surgery News at the office in New York City. From left, Victoria Stern (Associate Edi-tor), Michael Enright (Publication Director), Deanna Cosme (Art Director), Kevin Horty (Group Publication Editor) and Kate Carmody (Manager of Publication Sales).
Dear Reader,General Surgery News is pleased to present its first internationals
issue, and welcome you as our reader. The vision for this editionemerged after speaking with several surgeons about the need for comprehensive coverage of surgery news from around the world.This issue includes news and feature articles, as well as expert opinions focused on clinical and technological innovations in arange of areas, including hernia repair, breast cancer and bariat-ric surgery. Many of the pieces highlight clinical research done by surgeons worldwide.
Included within these pages is an article that discusses the con-troversy over the safety and efficacy of peroral endoscopic myot-omy (POEM), research that examines chronic pain after inguinalhernia repair and an article exploring how surgeons are chang-ing their practice after the Z0011 data were published last year.The issue also contains a section called The Surgeons’ Lounge inwhich surgeons tackle case-based questions submitted by read-ers. In this section, surgeons from the United Kingdom discuss apatient with a complex abdominal wall hernia, and a surgeon fromIsrael explains his surgical approach to epiphrenic diverticula. Wehope that you enjoy reading this edition and the topics featuredhere engender a lively discussion and debate. We look forward toany and all comments and feedback (please find enclosed survey),and we hope this is the first of many issues to come.
Sincerely,
The Editors,Kevin Horty [email protected] Stern
3GENERALSURGERYNEWS.COM / GENERAL SURGERY NEWS INTERNATIONAL EDITION 2012 From the Editors
McMahon Publishing isa family-owned medical publishing and medical
education company. McMahon publishes seven clinical news papers and nine annual orsemiannual Special Editions.
mcmahonmed.com © 2012 by McMahon Publishing, New York, NY 10036. All rights reserved. General Surgery News
(ISSN 1099-4122) is published monthly by McMAHON PUBLISHING,Sales, Pro duction and Editorial Offices: 545 W. 45th St., 8th Floor,New York, NY 10036, Tel. (212) 957-5300. Corporate Office: 83Peaceable St. West Redding, CT 06896. Periodicals postage paidat New York, NY, and at additional mailing offices. POSTMASTER:Please send address changes to General Surgery News, 545 W.45th St., 8th Floor, New York, NY 10036.
Senior Medical Adviser
Frederick L. Greene, MDCharlotte, NCGeneral Surgery, Laparoscopy, Surgical Oncology
Editorial Advisory Board
Maurice E. Arregui, MDIndianapolis, INGeneral Surgery, Laparoscopy, Surgical Oncology, Ultrasound,Endoscopy
Kay Ball, RN, CNOR, FAANLewis Center, OHNursing
Philip S. Barie, MD, MBANew York, NYCritical Care/Trauma, Surgical Infection
L.D. Britt, MD, MPHNorfolk, VAGeneral Surgery, Trauma/Critical Care
David Earle, MDSpringfield, MAGeneral Surgery, Laparoscopy
James Forrest Calland, MDPhiladelphia, PAGeneral Surgery, Trauma Surgery
Edward Felix, MDFresno, CAGeneral Surgery, Laparoscopy
Robert J. Fitzgibbons Jr., MDOmaha, NEGeneral Surgery, Laparoscopy, Surgical Oncology
David R. Flum, MD, MPHSeattle, WAGeneral Surgery, Outcomes Research
Michael Goldfarb, MDLong Branch, NJLaparoscopy, Telemedicine
Leo A. Gordon, MDLos Angeles, CAGeneral Surgery, Laparoscopy, Surgical Education
Gary Hoffman, MDLos Angeles, CAColorectal Surgery
Namir Katkhouda, MDLos Angeles, CALaparoscopy
Michael Kavic, MDYoungstown, OHGeneral Surgery, Laparoscopy
Peter K. Kim, MDBronx, NYEmergency General Surgery
Raymond J. Lanzafame, MDRochester, NYGeneral Surgery, Laparoscopy, Surgical Oncology, Laser Surgery, New Technology
John Maa, MDSan Francisco, CASurgical Hospitalist
Gerald Marks, MDWynnewood, PAColon and Rectal Surgery, Colonoscopy
J. Barry McKernan, MDMarietta, GALaparoscopy
Joseph B. Petelin, MDShawnee Mission, KSLaparoscopy
Richard Peterson, MDSan Antonio, TXGeneral Surgery, Bariatric Surgery
Joseph J. Pietrafitta, MDMinneapolis, MNGeneral Surgery, Laparoscopy, Colon and Rectal Surgery,Laser Surgery
David M. Reed, MDNew Canaan, CTGeneral Surgery, Laparoscopy,Medical Technology Development/Assessment
Barry A. Salky, MD New York, NYLaparoscopy
Paul Alan Wetter, MDMiami, FLOb/Gyn, Laparoscopy
Editorial Staff
Kevin HortyGroup Publication Editor ([email protected])
Victoria SternAssociate Editor ([email protected])
James PruddenGroup Editorial Director
Robin B. WeisbergManager, Editorial Services
Elizabeth ZhongAssociate Copy Chief
Sales
Michael EnrightGroup Publication Director (212) 957-5300, ext. [email protected]
Kate CarmodyManager of Publication Sales (212) 957-5300, ext. [email protected]
Alina DasguptaClassified Advertising (212) 957-5300, ext. [email protected]
Art/MAX Graphics & Production Staff
Michele McMahon VelleCreative Director
Deanna CosmeArt Director
James O’NeillSenior Systems Manager
Dan RadebaughDirector of Production and Technical Operations
Brandy WilsonCirculation Coordinator
McMahon Group
Raymond E. McMahon, Publisher & CEO,
Managing Partner
Van Velle, President, Partner
Matthew McMahon, General Manager, Partner
Lauren Smith, Michael McMahon,Michele McMahon Velle, Rosanne C.McMahon, Partners
Change of Address ProcedureAll U.S. general surgeons, colorectal sur-
geons, vascular surgeons, surgical oncolo-gists and trauma/critical care surgeons should receive General Surgery News free of charge. If you are changing your address or name, you must notify the AMA at (800) 262-3211 or the AOA (if appropriate) at (800) 621-1773 to continue receiving GSN. You need not be a member; however, they maintain the ultimate source of our mailing addresses.
If you are not a general surgeon or otherspecialist listed above and would like to sub-scribe, please send a check payable to Gen-eral Surgery News. Please allow 8-12 weeks for the first issue. Subscription: $70 per year (outside U.S.A., $90). Single copies, $7 (out-side U.S.A., $10).
Send checks and queries to: Circulation Coordinator, General Surgery News, 545 West45th Street, 8th Floor, New York, NY 10036.Fax: (212) 664-1242.
INFECTIOUS DISEASE SPECIAL EDITION
Please send letters to:[email protected].
Mission StatementIt is the mission of General Surgery News
to be an independent and reliable source of news and analysis about the current state ofsurgery. It strives to provide a venue for dis-cussion and opinions, from all viewpoints, on the issues most important to surgeons.
DisclaimerOpinions and statements published in
General Surgery News are those of thesindividual author or speaker and do not necessarily represent the views of the editorial advisory board, editorial staff or reporters.

Study Offers Glimpse on How Surgeons Are Applying Z0011 DataBY MONICA SMITH
PHOENIX—After results of the American XX
College of Surgeons Oncology Group’s ACOSOG Z0011 trial were released—first the local recurrence data in 2010 (JAMA(( 2011;305:569-575) and then the Asurvival data in April 2011 at a meeting of the American Surgical Association—it has been unclear how the trial’s find-ings have influenced practice. Research
presented at the annual meeting of the American Society of Breast Surgeons shows that surgeons at one large institu-tion have grown increasingly comfortable applying the Z0011 data to their patients (Ann Surg Onc;(( July 2012, Epub ahead of print).
In August 2010, the University of Texas MD Anderson Cancer Center, in Houston, assembled a multidisciplinary team of surgeons, radiation oncologists, pathologists and medical oncologists to
determine how to use the Z0011 findings, that showed no difference in local recur-rence or survival between selected patients with positive sentinel lymph nodes (SLN) who omitted axillary lymph node dissec-tion (ALND) and patients who under-went ALND.
“We discussed the results of the trial and the relevant literature and came up with a group consensus on how to apply this data in our clinical practice,” said Abi-gail S. Caudle, MD, assistant professor of
surgical oncology at MD Anderson Can-cer Center.
Subsequently, Dr. Caudle and col-leagues sought to determine the impact of Z0011 on surgeon practice patterns, and tosee which patients’ surgeons seemed most comfortable applying the data. The retro-spective review involved 17 surgeons andtwo cohorts of patients: those seen in theyear before the release of Z0011 and those seen in a 12-month peri-od after their interdisciplinary yconference. The investiga-tors used only patients who met eligibility criteria for Z0011, excluding thosewho had neoadjuvant chemotherapy, those who underwent mas-tectomy and those with tumors larger than 5 cm on surgical pathology.
The investigators included 658 patients:335 in the pre-Z0011results group, of whom 62 (19%) were SLN-positive, and 323 in the post-Z0011 results group, of whom 42 (13%) were SLN-positive.In the pre-Z0011 cohort, 85% of SLN-positive patients underwent ALND,compared with 24% of those in the post-Z0011 cohort. Given that the propor-tion of post-Z0011 patients undergoing ALND dropped from 28% in the first sixmonths of the post-Z0011 time frameto 18% in the subsequent six monthssuggests that surgeons became more
comfortable applying the Z0011 dataover time.
One purpose of this study was todetermine if there were patient groups towhich surgeons were not applying Z0011data, and how they were distinguishing those patients. “In the pre-Z0011 group,the decision to omit ALND appears tobe driven by SLN characteristics, whilein the post-Z0011 group, the decision toperform ALND appears to be driven by primary tumor features,” Dr. Caudle said.
In the post-Z0011 cohort, surgeonswere more likely to perform ALND onpatients who had larger tumors, lobu-lar histology, fewer SLNs retrieved, larg-er SLN metastasis, evidence of extranodalextension, and those in whom a validatednomogram predicted a higher probability of positive non-SLNs.
The researchers also examined theimpact of Z0011 on adjuvant therapy andfound that the radiation oncologists at
4 In the News GENERALSURGERYNEWS.COM / GENERAL SURGERY NEWS INTERNATIONAL EDITION 2012
It has been unclear how the trial’s findings have
influenced practice.

MD Anderson had been adjusting radi-ation fields to add high tangents for those who do not undergo ALND.
“In the pre-Z0011 cohort, 10% had high tangents versus 43% in the post-Z011 cohort,” Dr. Caudle said. “We feel that this is a reflection of changing sur-gical practices, since only 2% of patients who underwent ALND had high tan-gents compared with 88% who did not have an ALND.”
They also found that surgeons were less likely to perform intraoperative nodal assessment in the post-Z0011 cohort; assessment fell from 69% in the pre-Z0011 cohort to 26% in the post-Z0011 group. This change led to a decrease in operative time, from a medi-an of 92 down to 79 minutes.
“This was definitely a well-received paper,” said Judy Boughey, MD, asso-ciate professor of surgery, Mayo Clinic, in Rochester, Minn. “I think it’s always important for people to hear that the big institutions have accepted and altered their practice based on the findings. In particular, people are interested in how surgeons and institutions have incorpo-rated the study findings into their every-day clinical practice.
“One of the critical things this abstract showed was that it is still a lim-ited proportion of patients you see who fit the exact criteria for Z0011. Sur-geons are more likely to do dissections for patients with larger tumors, fewer SLN removed or larger lymph node
metastasis—the more worrisome cases,” Dr. Boughey added. “It is also important to note that the findings are not being extrap-olated to women undergoing mastectomy, or receiving partial breast radiation or neoadjuvant chemotherapy.”
Dr. Boughey also noted the inclusion of intraoperative nodal assessment and its impact on operating time. “In this day and age, people are more in tune with trying to cut down on unneces-sary additive costs if it doesn’t
benefit the patient or alter the patient’s treatment; decreased intraoperative assessment lowers cost and allows short-er operating time for the patient.”
In her practice, Dr. Boughey said she and her colleagues still perform frozen section analyses on all SLNs. In particu-lar, it remains important for surgeons to perform intraoperative analysis of SLNs when they encounter a node that they are concerned will be positive by palpa-tion because it’s more likely that there will be several additional positive nodes.
“But, in nodes you think will be neg-ative, I think it’s reasonable not to do
intraoperative nodal assessment in thosecases where the patient meets Z0011criteria, is undergoing breast conserva-tion, doesn’t have a very large tumor anddidn’t have neoadjuvant chemothera-py, if you plan not to do a dissection innode-positive cases,” she said.
Drs. Boughey and Caudle had no relevant disclosures.
5GENERALSURGERYNEWS.COM / GENERAL SURGERY NEWS INTERNATIONAL EDITION 2012 In the News
‘This was definitely a well-received paper. I think it’s
always important for people to hear that the big institutions
have accepted and altered their practice based on the findings.’
—Judy Boughey, MD
www.cookmedical.com
Unlike synthetic mesh and other biologic grafts, Biodesign is completely remodeled by the patient’s body into strong, well vascularized patient tissue.
The evolution of a proven techonlogy, Biodesign can help provide reduced recurrence rates when compared to other biologic grafts. That’s because Biodesign is completely remodeled into tissue that maintains long-term strength.
Learn more: visit www.cookbiodesign.com
Move beyondto the next generation.
© COOK 2012 SUR-BADV-MBNG-EN-201209
BIODESIGN®
A D VA N C E D T I S S U E R E PA I R
PROVENT E C H N O LO GY
REDUCEDR E C U R R E N C E
COSTE F F E C T I V E

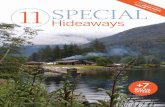
A68-year-old woman had a history of regurgitation, halitosis and recurrent
aspirations over the past few years. She underwent a barium swallow that revealed epiphrenic esophageal diverticula. What is your preferred workup for this patient? Do you always perform a preoperative manom-etry? Are asymptomatic patients candi-dates for surgery? What is the likelihood of malignancy in the diverticula? What is your preferred surgical approach?
From Tamar Abramovich, MD Department of Surgery B, Carmel Medical Center, Haifa, Israel
Question for Dr. Hazzan
Epiphrenic diverticula are found adja-cent to the diaphragm in the distal thirdof the esophagus. They are false diver-ticula that often are related to achala-sia and diffuse esophageal spasm. They most often are related to thickenedesophageal musculature or increasedintraluminal pressure.
A barium swallow is the best diag-nostic tool to detect the presence of
epiphrenic diverticula. The size, posi-tion and proximity of the diverticulato the diaphragm can be clearly delin-eated. The underlying motility disor-der often is identified as well; however, manometric studies need to be under-taken to evaluate the overall motility of the esophageal body and lower esopha-geal sphincter. An endoscopy is alwaysperformed to detect mucosal lesions,including esophagitis, Barrett’s esopha-gus and distal cancer.
Treatment is recommended for patients who have moderate to severesymptoms. There is no consensus as to whether asymptomatic patients
should undergo treatment as well.Despite the finding that asymptom-atic patients do not usually developsymptoms during many years of fol-low-up, the fact that minimally inva-sive approaches are available for themanagement of epiphrenic divertic-ula may make surgical therapy moreappealing.
The incidence of cancer in an epi-phrenic diverticulum is less than1%. Risk factors for malignancy areadvanced age, male gender, long-standing history of cancer and larg-er diverticula. Outcomes usually arequoted as dismal because of a delayeddiagnosis but several cases of super-ficial carcinoma have been described.
In this particular case, becausethe diverticulum is wide-mouthed,I would perform a diverticulectomy,contralateral myotomy and Toupet fundoplication. In some cases whenthe diverticulum is small, surgeonsmight recommend diverticulopexy to prevent creating a stapler line that is at risk for leakage. In both cases, along esophageal myotomy is a crucialstep in the treatment of this patholo-gy. The extent of the myotomy is anissue of debate: Most authors recom-i f d b t M t thmend starting from the level of thebase of the diverticulum and extend-ing the myotomy 1 to 2 cm distal tothe esophagogastric junction.
For many decades, the tradition-al approach was through a left tho-racotomy; more recently, minimally invasive techniques by video-assistedthoracic surgery or laparoscopy havebeen used successfully and are now theprocedures of choice in most cases. Istrongly believe that the laparoscop-ic approach is ideal for the treatment of this pathology. The esophageal hia-tus is approached, the distal esopha-gus is mobilized and the diverticula isidentified and cleared of surrounding
tissue to expose the mucosa at the neck of the diverticula. After inserting a 56 to 60 Fr bougie down through the esophagus, a linear cutting stapler is used to excise the diverticula. The overlying muscle is closed. A myoto-my is then performed on the opposite side of the esophagus, the hiatus is closed and a partial fundoplication—either Dor or Toupet—is performed. The postoperative morbidity should be less than 5%. Most patients can be discharged by postoperative day 2 and the long-term results in terms of dys-phagia or reflux are similar to those of patients after Heller myotomy due to achalasia.
Suggested Reading
1. Vicentine FP, Herbella FA, Silva LC, Patti MG. High resolution manometry findings in patients with esophageal epiphrenic diverticula. Am Surg. 2011;77:1661-1664.
2. Fisichella PM, Pittman M, Kuo PC. Lap-aroscopic treatment of epiphrenic divertic-ula: preoperative evaluation and surgical technique. How I do it. J Gastrointest Surg..2011;15:1866-1871.
3. Zaninotto G et al. Therapeutic strate-gies for epiphrenic diverticula: systematic review. World J Surg. 2011;35:1447-1453.
4. Rosati R et al. Long-term results of min-imally invasive surgery for symptomat-i ll i i f t tic epiphrenic diverticulum. Am J Surg.2011;201:132-135.
5. D’Journo XB et al. Lower oesophageal sphincter dysfunction is part of the func-tional abnormality in epiphrenic diverticu-lum. Br J Surg. 2009;96:892-900.
6. Melman L et al. Esophageal manomet-ric characteristics and outcomes for lap-aroscopic esophageal diverticulectomy, myotomy, and partial fundoplication for epiphrenic diverticula. Surg Endosc.2009;23:1337-1341.
7. Varghese TK Jr et al. Surgical treatment of epiphrenic diverticula: a 30-year experi-ence. Ann Thorac Surg. 2007;84:1801-1809.
8. Reznik SI et al. Assessment of a patho-physiology-directed treatment for symp-tomatic epiphrenic diverticulum. Dis Esophagus. 2007;20:320-327.
Dear Readers,Welcome to the The Surgeons’ Lounge with experts from our International Seriese . This
issue features David Hazzan, MD, director of minimally invasive surgery, Carm-el Medical Center in Haifa, Israel, who will be discussing the case of epiphren-ic diverticula. The issue also includes Steve Hornby, BMBS, MRCS, upper GIclinical research fellow, General Surgical Registrar in the South Peninsula, and director of education for the Association of Surgeons in Training, London, andAndrew Kingsnorth, MD, consultant surgeon and honorary professor of surgery at the Peninsula College of Medicine and Dentistry, president of the surgical sec-tion of the Royal Society of Medicine, and past president of the European Hernia Soci-ety and the British Hernia Society, London, who have prepared a detailed case report of a patient with an abdominal wall hernia and describe here how they managed this very complex case. I want to give special mention to commander Rory Rickard, MD, a consultant plastic and reconstructive surgeon based in London.
We look forward to your comments and questions.
Sincerely,Samuel Szomstein, MD, FACSEditor, The Surgeons’ [email protected]
6 Surgeons’ Lounge GENERALSURGERYNEWS.COM / GENERAL SURGERY NEWS INTERNATIONAL EDITION 2012
Dr. Szomstein is associate director,nBariatric Institute, Section of Minimally Invasive Surgery, Department of General and Vascular Surgery, Cleveland Clinic Florida, Weston.
Dr. Hazzan’s
Reply
Figure. Epiphrenic esophageal diverticula seen on barium swallow.

Figure 1. Front view.
Figure 2. Side view.
Figure 3. Previous mesh material.
Figure 4. Rectus femoris fascia reconstruction.
Figure 5. Biological mesh.
A62-year-old man presents as a national refer-ral to your specialist complex hernia clinic. He
has massive lower abdominal wall herniation. The patient was initially treated several years ago for bilateral inguinal hernias and since then has had at least five attempts to repair recurrences. A variety of mesh materials and tissue planes have been used, including laparoscopic approaches.
On physical examination, the entire abdominal wall below the umbilicus is affected, and with the patient in standing position, the hernia reaches his knees (Figures 1 and 2). With the patient in lying position, the hernia appears to be completely reduc-ible, and several of the previously implanted meshes are palpable.
It appears from the examination and the evidence provided from a magnetic resonance imaging (MRI) scan that the right inguinal ligament is destroyed. This patient’s quality of life is so adversely affect-ed by his hernia that he is desperate for a further attempt at repair.
How is this complex problem managed?
Description of Case ManagementA key first step in patients such is this one is to
manage their expectations. This patient should be informed that the risk for further failure of the repair is approximately 50% and that there would be a sig-nificant risk for mortality associated with a recon-struction of this scale. The patient is not overweight, but if he were, he would be strongly advised to lose weight and, if necessary, referred to a specialized dietetic team.
Given the high likelihood he will require tissue replacement of the inguinal ligaments, it is recom-mended he receive the help of a specialist plastic sur-geon. A theater (operating room) slot of at least eight hours should be set aside.
The patient was taken to theater with two consul-tant surgeons specializing in abdominal wall recon-struction, a herniologist and a plastic surgeon. The operation required six hours and 40 minutes to com-plete. On opening the redundant skin, several large pieces of mesh were found and excised (Figure 3). The abdominal wall consisted of only atrophied rec-tus abdominis muscles about 2 cm wide, and the right inguinal ligament was absent. The redundant skin was excised and adhesiolysis was performed. The right inguinal ligament was reconstructed by mobilizing a strip of rectus femoris fascia and securing it using nonabsorbable sutures between the anterior superior iliac spine and the pubic tubercle (Figure 4).
When completed, this reconstruction was used as a platform to place an underlapping biological mesh to close the hernia defect (Figure 5). This region was further reinforced with an onlay polypropylene mesh (Figure 6). Both meshes were affixed with a
nonabsorbable suture. Drains were placed on top of the mesh with instructions not to remove for five days and to only drain less than 50 mL every 24 hours.
The patient initially had an unstable recovery. He developed pulmonary edema and right lower lobe collapse, and required a two-day intensive care unit admission for noninvasive ventilation. After these issues were dealt with, recovery was steady and he was discharged on day 13 postsurgery.
The patient has been followed up for nine months. At this stage, he has complained of several aches and pains as well as gastroesophageal reflux, but his her-nia repair remains intact and this has been confirmed on MRI scan (Figures 7 and 8).
In summary, here are several points to consider when treating this patient:
• Multidisciplinary teamwork: This patient benefited from specialist care by a hernia sur-geon, a plastic surgeon, an anesthetist, an intensivist, physiotherapists and nursing staff, all of whom had roles to play in his repair and recovery
• Considered use of mesh• Biological mesh for tissue reconstruction• Synthetic mesh for reinforcement and strength• Drain management: The drains in our cases
are left until the postsurgical collection is drained to dryness. Seromas remain an unsolved problem, but the use of tissue glues and talc products may offer solutions
Autologous tissue repair techniques, such as the components separation and rectus femoris fascia flaps, should be in the armamentarium of any sur-geon tackling these complex reconstructions.
Case Study of a Difficult Hernia
7GENERALSURGERYNEWS.COM / GENERAL SURGERY NEWS INTERNATIONAL EDITION 2012 Surgeons’ Lounge
Andrew Kingsnorth, MD Mr. Steve Hornby
Figure 6. Synthetic mesh.
Figure 7. Postoperative follow-up, front view.
Figure 8. Postoperative follow-up, side view.

severely affect protein function: Two of these variants were protein-truncating mutations and four resulted in missensechanges.
Dr. Southey, also senior research fel-low and deputy head in the Department of Pathology, University of Melbourne,Australia, said the study would be rel-evant to “clinical oncologists who work with families with multiple cases of breast cancer. This is another gene they can test for.”
No commercially available tests haveyet been developed based on these find-ings; however, Dr. Southey said, “Iimagine there will be [tests] soon, tohelp women determine their personalrisk for breast cancer. Some treatment choices might be influenced by knowing if a woman has a mutation in XRCC2.”
In the paper, the researchers notedthat specific targeted treatments such aspoly(ADP-ribose) polymerase (PARP)inhibitors might benefit patientswhose breast cancer is associated with
homologous-recombination DNA repair dysfunction, as is the case with deleteri-ous XRCC2 mutations.
The study is the first report of mas-sively parallel sequencing being used in the discovery of a breast cancer sus-ceptibility gene, said Dr. Southey, who called this “one of the really exciting things about this paper.” She added, “We anticipate finding more genes related to susceptibility to breast cancer by applying this methodology.”
Massively parallel sequencing has been used previously to identify the genetic explanation for relatively sim-ple autosomal-dominant diseases, Dr. Southey stated. “This is the first report applying it to a complex disease. Now the world’s our oyster.” Dr. Southey is currently using the technique to study genetic predisposition to prostate and colorectal cancers. “A large number of genetic research groups are applying this technology.”
Nasal MRSA a Risk Factor for Post-op Surgical Site InfectionsFirst Study To Document Link in
Gastrointestinal Surgery
BY DAVID WILD
SAN DIEGO—Preoperative methicillin-resistant Staph-ylococcus aureus (MRSA) colonization increases the risk for surgical site infections (SSIs) and increases hospi-tal length of stay (LOS) following major gastrointes-tinal (GI) surgery, according to a study presented at the 2012 Digestive Diseases Week. Investigators said the results may justify a policy of universal preoperative nasal swabbing and MRSA decolonization.
“Preoperative nasal swab testing with decolonization of MRSA-positive patients could decrease lengths of stay and reduce the incidence of MRSA-associated SSI after major gastrointestinal surgery,” said lead researcher Harry Papaconstantinou, MD, who is chief of colorec-tal surgery at Scott and White Memorial Hospital, in Temple, Texas.
Dr. Papaconstantinou and colleagues conducted nasal swab tests for MRSA and methicillin-sensitive S. aureus (MSSA) in 1,137 patients who underwent major GI surgery between December 2007 and August 2009 (abstract 374). Patients were swabbed within 48 hours of hospital admission. Swabs showed 6.4% (73 patients) were MRSA-positive, 14.7% (167) were MSSA-posi-tive and 78.9% (897) were S. aureus-negative on admis-sion. Demographic traits of the three groups were similar.
The researchers found 13.7% (10) of MRSA-positive patients developed an SSI, compared with 4.2% (seven) of MSSA-positive patients and 9.4% (84) of uninfected patients (P<0.05 for MRSA vs. MSSA and uninfected).
Patients with SSIs (aggregated across MRSA,
MSSA and uninfected groups) had an LOS of 15.7 days, compared with 6.2 days among those with no SSIs (P<0.001). Including individuals with and without SSIs, MRSA-positive patients had significantly lon-ger hospital stays (mean, 12.5 days for MRSA-positive vs. 8.8 and 7.6 days for MSSA-positive and uninfect-ed, respectively; P<0.001). However, when the investi-gators examined only those with SSIs, they found no significant differences in LOS between patients with wound MRSA colonization and those with MRSA-free SSIs. Mortality rates also did not differ among the three groups, with each approximately 4%.
Dr. Papaconstantinou was surprised that 70% of MRSA-positive patients also had MRSA-positive wound cultures. He said that he expected most post-GI surgery wound pathogens to originate from the gut. In contrast, only 8.5% of patients who had negative nasal swabs had MRSA-positive wound cultures (P<0.0001).
Philip S. Barie, MD, MBA, professor of surgery and professor of public health at Weill Cornell Medical College, in New York City, who was not involved in the study, said that MRSA colonization has been linked to an increased risk for SSIs in cardiac and orthopedic surgery patients (J Am Acad Orthop Surg(( 2012;20:94-g101). He said that this is the first study to document a link in the GI surgery patient population.
“These findings get the message out that MRSA-related SSIs can occur after a broader spectrum of oper-ations than was previously believed,” Dr. Barie told General Surgery News. “The question remains as to what is the best course of preventive action. This retrospec-tive study makes an important observation, but does not constitute proof that screening and decolonization will be effective before GI surgery.”
Dr. Papaconstantinou had nothing to disclose. Dr. Barie is a consultant to Forest Laboratories, Merck and Pfizer.
8 In the News GENERALSURGERYNEWS.COM / GENERAL SURGERY NEWS INTERNATIONAL EDITION 2012
GENEContinued from page 1
‘This is the first report applying it to a complex disease. Now the world’s our oyster.’—Melissa C. Southey, PhD, Grad Dip Law, FHGSA, FFSc
‘The question remains as to what is the best course
of preventive action.’—Philip S. Barie, MD, MBA

MCGSN1166.indd 1 7/11/12 4:58 PM

assessments on the day of surgery, the first, second and seventh day postsur-gery, and at six months and five years after surgery.
The chronic pain was 16.4% and sen-sory disorder rate was 15.9% after six months. At the five-year mark, 16.1% of patients reported chronic pain and 20.3% had sensory disorder of the groin. Independent significant predictors of chronic pain were preoperative pain, chronic pain after six months, sensory disorder after five years and ilioinguinal nerve neurolysis in Lichtenstein repair due to mobilization of the nerve from its natural bed and nerve preservation.
Based on the results of the study, Dr. Reinpold and colleagues called on sur-geons to avoid ilioinguinal nerve mobi-lization in the Lichtenstein technique. “The inguinal nerves should either be left untouched in their natural bed or if this is not possible a neurrectomy and proximal end implantation … should be performed,” they said.
At the meeting, the investigators pre-sented their 10-year outcomes data. They had sent a questionnaire to 736 patients, and received responses from 55%. Eight patients in the cohort died
over the course of the study.Among the respondents, 13.6%
reported chronic pain 10 years after surgery. Most patients with pain clas-sified it as mild without an effect on daily activities or quality of life. How-ever, eight patients (1.8%) had relevant pain, defined as a score greater than 3 on the visual analog scale. No patient described the sensation as very strong. Five of the eight reported a slight inter-ference with daily activities.
Among the eight patients with relevant pain, five had under-gone a Lichten-stein repair andthree had aShouldice repair. Seven of the eight patientshad neurolysis of the ilioinguinal nerve with preser-vation of the nerve.Significant predictors of chronic pain were young-er than age 50 years, sensory disorder of the groin after five years and chronic pain after six months.
Dr. Reinpold said the 10-year results confirm their earlier recommendations. They called on surgeons to visualize the
nerves and handle with care; to leave the inguinal nerves untouched in their natural bed or, if this is not possible, to perform a neurectomy and proximal end implantation; to leave the cremas-teric muscle and spermatic fascia in tact; and to avoid mesh suture fixation to the internal oblique muscle.
The investigators believe that a chronic inflammatory reaction occurs between the conventional polypropyl-ene mesh and mobilized nerve, leading
to long-term post-herniorrhaphy chronic pain. Another hypothesis is that chronic scar formation with fibrotic nerve traction leads to chronic pain.
Dr. Reinpold’s study comes on the heels of international guidelines pub-lished in 2011. Both reports stress what some specialists have argued for years: A mesh repair is not the same as a tradition-al tissue repair with the addition of mesh. Mesh repairs are a completely different
operation and the nerves need to be treat-ed carefully, left in their natural beds andnot exposed to contact with the mesh.
“Mesh repair has its own principlesthat have to be followed. For many years, surgeons had a mindset that wasotherwise,” said Parviz K. Amid, MD,clinical professor of surgery, David Gef-fen School of Medicine at University of California, Los Angeles and director of the Lichtenstein Amid Hernia Clinic at the university.
Dr. Amid said patients persistently hung onto three “cardinal mistakes fromthe past”: removing the ilioinguinal nervefrom its natural bed, roughly mobilizing the spermatic cord by finger instead of
doing it gently under direct visionand removing the cremasteric lay-ers that protect the genital branchof the genitofemoral nerve and thevas deferens.
Based on the current evidence,the rate of chronic pain can bereduced to less than 1% by care-ful nerve handling, Dr. Amid
said, and surgeons are growing morecognizant of nerve management. “Sur-geons are beginning to understand that they have to deprogram their memory bank and not rely on teachings of thepast,” said Dr. Amid.
New Fixation Technique Cuts Tacks Needed In Hernia Repair May Lessen Postoperative Pain
BY CHRISTINA FRANGOU
NEW YORK—Spanish surgeons have reported a new KK
method of mesh fixation for laparoscopic ventral her-nia repair that significantly reduces the number of tacksrequired and may diminish patients’ postoperative pain.This new technique uses a combination of tacks andfibrin glue placed in a double-crown technique.
“I think with this study, we have shown the feasibili-ty of this technique, which decreases mechanical fixationand should reduce acute and postoperative chronic painwithout increasing the recurrence rate,” said lead author Salvador Morales-Conde, MD, chief of the AdvancedLaparoscopic Unit of the University Hospital Virgen delRocío in Sevilla, Spain. Dr. Morales-Conde presentedthe results at the Fifth Inter-national Hernia Congress (session 7C abstracts).
Previous studies have drawn a link between pain and the number of tacks (Br J Surg 2011;98:1537-1545), which is why Dr. Morales-Conde and her team set out to develop a technique that would reduce the number of tacks required. For this tech-nique, surgeons put the mesh
in place and deposited four tacks into the mesh at cardi-nal points around the mesh perimeter. They then marked all the spots where they would usually put tacks, leav-ing less than 1 cm between each mark. After marking the exterior and inner ring of the double crown, the sur-geons placed a tack at every third or every fourth mark and filled in the gaps with fibrin glue. Lab studies have shown that fibrin glue has a chemotactic effect, increas-ing the collagen, spurring new vessel growth and con-sequently causing a biological rather than mechanical fixation.
In a series of 38 patients, Dr. Morales-Conde and her team showed they could reduce the number of tacks by 66% by using this technique. All patients included in the study had primary or secondary ventral hernias, located at the midline, far from bones and sizes ranging between 3×3 and 17×12 cm.
There were no intraoperative complications; postop-erative days in the hospital aver-aged 1.62 days with a range of one to seven. Two patients (5.7%) were readmitted due to paralytic ileus. None of the patients report-ed chronic pain at a median fol-low-up of 24 months. Without a control group, however, the team could not demonstrate any chang-es in pain compared with standard fixation techniques.
To date, none of the patients has developed a recurrence after
a median follow-up of 24 months. One patient wasdiagnosed with a “tack hernia,” a condition that’s beendescribed in the literature as a fascial defect related tothe tack site (JSLS(( 2003;7:383-387).S
The Spanish research team is continuing to add toits series. The team currently is using plastic permanent tacks, rather than titanium spiral tacks, in the sametechnique. The researchers hypothesize that plastic per-manent tacks will create less adhesions.
Surgeons who heard the study presented say thetechnique is promising but longer follow-up with morepatients is needed. “We have a long way to go, but this iscertainly something to watch,” said Karl LeBlanc, MD,MBA, past president of the American Hernia Society and director and program chair of Fellowship Program,Minimally Invasive Surgery Institute, Baton Rouge, La.
One surgeon present questioned the “tack hernia,” saying he felt that it was a form of recurrence. How-ever, both Drs. Morales-Conde and LeBlanc, who first reported on tack hernias, said that it represents a new hernia.
The surgical team is following a watch and wait approach for the tack hernia because it is small andasymptomatic, said Dr. Morales-Conde.
Several groups in Spain and Italy have adopted thenew technique but there are no reports of surgeons using it in the United States.
Dr. Morales-Conde reported no relevant disclosures. The glue used in the study is Tissucol (Tisseel in the United
States), which is manufactured by Baxter.
10 In the News GENERALSURGERYNEWS.COM / GENERAL SURGERY NEWS INTERNATIONAL EDITION 2012
HERNIA REPAIR PAINContinued from page 1
‘Surgeons are beginning to understand that they have to
deprogram their memory bank and not rely on teachings of the past.’
—Paviz K. Amid, MD
‘I think with this study, we have shown the feasibility of this technique, which decreases
mechanical fixation and should reduce acute and postoperative chronic pain without increasing
the recurrence rate.’—Salvador Morales-Conde, MD

Study Shows Apparent Safety of Biologic Mesh for Hiatal Hernias Conflicts With Earlier Studies;
Long-Term Effects Still Uncertain
BY CHRISTINA FRANGOU
Alarge single-center series report-AAed no major complications associ-ated with use of biologic mesh to repair large hiatal hernias. This finding con-trasts with other recent studies that haveshown an increased risk for morbidity related to prosthetic and biologic meshesin these patients.
“Given the potential benefits of bio-logic mesh, we believe that surgeonswho pay careful attention to its place-ment should feel reassured in the safety of using these meshes during hiatal her-nia repair,” wrote Eelco B. Wassenaar,MD, and colleagues from the Universi-ty of Washington, in Seattle (Surg Endosc2012;26:1390-1396). They caution, how-ever, that the low complication rate may
reflect their own technique and not that of the general community.
Use of biologic mesh for repair of par-aesophageal hernia has been increasing ever since studies showed that, when used to reinforce hiatal closure, these mesh-es decrease short-term recurrence (Ann ((Surg 2006;244:481-490). But over the gpast few years, surgeons reported serious complications following biologic mesh repair, including erosion, dense fibro-sis and esophageal stenosis (Surg Endosc 2009;23:1219-1226).
After the 2009 study was published, the research team at the University of Washington decided to review its insti-tution’s experience. The group had used biologic mesh extensively for compli-cated hernia repair and led the original randomized trial. The study included all patients who had a biologic mesh placed at the hiatus and who were followed for at least one year. The investigators adminis-tered a questionnaire to identify any cases
of symptoms of gastroesophageal reflux disease, dysphagia and all other operative or endoscopic interventions that occurred after mesh implantation.
Of 126 eligible patients, 73 (58%) returned a questionnaire. Of those who did not respond, four patients (3%) had died from causes unrelated to the opera-tion, four patients (3%) did not want to participate and 47 patients (36%) were unreachable. The surveyed group had a median follow-up of 45 months.
Surveys showed that no patient report-ed mesh-related complications and no patient had an erosion, stricture or indi-cation from radiographic or endoscopic evaluation. No patient required a reoper-ation except one man for recurrent reflux symptoms with a recurrent sliding hiatal hernia.
The surveyed patients reported an overall improvement in all symptoms after their hernia repairs. No restriction or mild restriction in what they could eat was reported by 89% of patients. Two-thirds of patients graded their operative result as “excellent,” 23% as “good,” 6% as “fair” and 5% as “poor.” Among patients with poor results, one experienced severe dysphagia, one was dissatisfied with post-operative follow-up but did not have any symptoms, and another had “pain in the diaphragm” that was also recorded on the preoperative questionnaire.
The risk for dysphagia was a major focus for the investigators. When the prosthesis is placed at the hiatus, it can induce inflammation and scarring lead-ing to fibrosis, stenosis and eventually dysphagia. In this series, six patients (9%) had worsened dysphagia after surgery. Of these, two patients said the dysphagia was severe. Follow-up studies performed else-where revealed that one of these patients had a “tight wrap” but without stricture or erosion, and dilation did not improve the patient’s symptoms. “It is possible that mesh could be a contributing factor,” the authors said.
Overall, the rate of dysphagia in the study was 2%. This rate compared favor-ably to other studies of patients who underwent Nissen fundoplication with-out the use of mesh.
The study provides some reassur-ance about the safety of biologic meshes but concerns remain, said Emanuele Lo Menzo, MD, PhD, associate professor of surgery, University of Maryland Medi-cal Center, in Baltimore. “This study has long-term follow-up, which gives us a lit-tle bit of breathing room to say that bio-logic meshes seem to be safe. Certainly, at the University of Washington, it seems to be.”
He added, however, that there are flaws in the study. More than one-third
of patients treated could not be contact-ed and among those who were contacted,no patients underwent firsthand endo-scopic or radiologic evaluation at their treating institution. Furthermore, theinstitution has very experienced surgeons;thus, the results are likely to be difficult to reproduce.
Dr. Wassenaar said the surgical team uses three key strategies that may reducethe risk for complications. They advocatethe use of a U-shaped, rather than a key-hole configuration, which leaves an open area in the anterior aspect of the esopha-gus, and recommend covering the hiatusposterior to the esophagus, taking careto avoid pulling the mesh anteriorly andlifting the esophagus posteriorly to avoidnarrowing the esophagus. They also sug-gest leaving a small space between theedge of the mesh and the esophageal wallto avoid excessive contact of the mesh with the esophagus. The team developed this technique after studies conducted indogs revealed some fibrosis and scarring, leading to an esophageal stricture.
Despite the study’s findings, uncer-tainty remains about the long- and short-term success of biologic mesh repair in large hernias, other surgeons noted.
“It’s very confusing [because of ] mixed results from the studies. We still don’t know how biologic meshes are going to hold up long-term for large hiatal herniarepairs,” said Constantine T. Frantzides, MD, PhD, director of the advanced lapa-roscopic and bariatric fellowship program,Saint Francis Hospital, and director of the Chicago Institute of Minimally Inva-sive Surgery, in Skokie, Ill.
In 2011, surgeons reported results from a multicenter randomized trial of laparo-scopic paraesophageal hernia repair that compared primary diaphragm repair withprimary repair buttressed with a biolog-ic prosthesis (JACS (( 2011;213:461-468). The study showed that repair using bio-logic mesh was not associated with high-er rates of complications or side effectsbut that there was no benefit in reducing hiatal hernia recurrence with follow-up of more than five years.
Dr. Frantzides said more time and more studies are needed to settle theissue of synthetic versus biologic meshrepair. A randomized controlled study,led by Dr. Frantzides, confirmed thebenefit of mesh in large hiatal herniarepair (Arch Surg(( 2002;137:649-652);ghowever, there is little agreement about the ideal material of the mesh in theserepairs, he said.
“Personally, with large defects, I don’t think the biologic mesh will hold. But this is something that we cannot set-tle without having time to follow thesepatients long-term,” he said.
11GENERALSURGERYNEWS.COM / GENERAL SURGERY NEWS INTERNATIONAL EDITION 2012 In the News
‘This study has long-term follow-up, which gives us a little bit of
breathing room to say that biologic meshes seem to be safe.’
—Emanuele Lo Menzo, MD, PhD

surgery, and he sees many patients with severe GERD, an increasing number of whom are obese.
Although procedures specifically for the treatment of GERD and/or hiatal hernia may address those problems, they do nothing to address the underlying obesity that contributes to or exacerbates those problems and may increase risk for recurrence. The patient with a body mass index (BMI) of 40 kg/m2 who receives a fundoplication at age 35 is likely to be
just as heavy if not heavier 10 years later, and to accumulate the comorbidities asso-ciated with obesity. “If they are interest-ed then in pursuing bariatric surgery, it’s going to be much more difficult,” Dr. Gould said. “You’ve burned a few bridg-es by that point.”
Dr. Gould frames the context of bariat-ric surgery for these patients in three dif-ferent scenarios. First is the obese patient with GERD who wants help for reflux. “They have been sent to you to talk about fundoplication, but you need to bring up the fact that bariatric surgery is probably the better choice once they get into that
BMI category,” Dr. Gould said. “Fun-doplication has a higher failure rate [in
obese patients], and in my experience, it’s much more difficult to do a Nissen than a gastric bypass on patients with a BMI in the 40s and 50s.”
As a surgeon who does a lot of reoper-ative anti-reflux surgery, Dr. Gould gets a bit frustrated when he sees obese patients with failed fundoplications who were not informed about the option of bariat-ric surgery. “Even more frustrating is the patient who has a Nissen for GERD and later enrolls in a bariatric program and wants surgery,” he said. “They could have had one operation up front. Now it’s a risky procedure because you have to take down the Nissen before doing a gastric bypass.”
The second scenario Dr. Gould sees is the patient interested in and indicated for the patient interested in and indicated forbariatric surgery who turns out to have rns ou
GERD with or without a hiatal hernia.In this case, the question is whether
the choice of bariatric surgery should be guided by the presence of the hernia or the diagnosis of GERD.
The third scenario is an obese patient with a large, symptomatic paraesophageal hernia who may or may not have GERD but is experiencing symptoms related to the hernia such as chest pains or dyspha-gia. “Should you do a traditional lapa-roscopoic paraesophageal hernia repair, or manage that hernia with a gastric bypass or sleeve gastrectomy?”
For patients from the first scenario, Dr. Gould suggests gastric bypass as an ideal procedure for a variety of reasons (Ann Surg (( 2010;251:244). After the gas-tric pouch is created and the stomach is divided, most of the parietal cells remain in the bypassed stomach, so the acid, as well as pepsin and bile, are for the most part mechanically diverted away from the esophagus.
“I’ve done gastric bypasses on people with GERD and they are better imme-diately. Also, as they lose weight, the ele-vated intra-abdominal pressure associated with obesity starts to decrease,” lower-ing one of the risk factors for GERD, Dr. Gould said.
The evidence is less clear for gas-tric banding and GERD. In a review of 20 studies of 3,200 patients, “resolu-tion versus improvement, versus worsen-ing of GERD symptoms, versus newly developed GERD symptoms after band
12 In the News GENERALSURGERYNEWS.COM / GENERAL SURGERY NEWS INTERNATIONAL EDITION 2012
GERD AND HERNIAContinued from page 1
‘I’ve done gastric bypasses on people with GERD and
they are better immediately. Also, as they lose weight,
the elevated intra-abdominal pressure associated with
obesity starts to decrease.’—Jon C. Gould, MD
MINIMALLY INVASIVESURGERY WEEK
A U G U S T 2 8 - 3 1 , 2 0 1 3
WASHINGTON D.C.
RESTON ~ VA
Presented by SLS Affiliated Societies & Annual Meeting & Endo Expo
ORREADY
ORReady is a worldwide, multi-Specialty initiative to encourage steps that are known to improve surgical outcomes and save lives. If the guidelines suggested here, which include Check Lists, Time Outs and Warm Ups are
followed routinely, we estimate that Six Million patients around the world could have better outcomes.
2
1
3
1 Ready - Warm Up & Check List
2 Set - Stop & Time Out
3 Go - OK to begin
Go to www.SLS.org for more information about MIS Week
The Multidisciplinary Approach - "It's the Outcome"
Find out how your department and hospital canbe ORReady and improve outcomes at ORREADY.org
Robotic Societies
Society of Laparoendoscopic Surgeons (SLS)
American Institute of Minimally Invasive Surgery (AIMIS)
Chinese Journal of Minimally Invasive Surgery (CJMIS)
International Pelvic Pain Society (IPPS)
International Society of Gynecological Endoscopy (ISGE)
New European Surgical Academy (NESA)
Society for Medical Innovation and Technology (SMIT)
Surg ica l Endoscopy Gyn Laparoscopy Endouro logy Robot ic Surgery
Preliminary Listing of Participating Organizations

placement, it’s all over the map,” Dr. Gould said (Aliment Pharmacol Ther(( 2009;30:11-r12). “Data suggests short-term resolu-tion or improvement of symptoms, but in the long term, there are concerns about worsening or newly developing symptoms with the band.”
Sleeve gastrectomy is probably not the best option. “There’s data out there sug-gesting that patients who have GERD at the time of sleeve gastrectomy are very likely to continue to have GERD, and there is a fair number of people who do not have symptoms prior to sleeve who develop those symptoms later,” Dr. Gould said.
In the obese patient with a hiatal her-nia, gastric banding could be feasible. “Hiatal hernia has been considered a con-Hiatal hernia has been considered a con
traindication for a band, but that’s less nowadays,” Dr. Gould said. In past stud-ies examining the repair of small hia-tal hernias (1-2 cm), at the time of band placement, the incidence of band slippage is low.
Sleeve gastrectomy may be a good option for the patient with a large, symp-tomatic paraesophageal hernia and asso-ciated short esophagus in whom it is difficult to mobilize the gastroesophage-al junction below the diaphragm during surgery.
“A sleeve gastrectomy is like a really long neo-esophagus, a tube that goes all the way down to the pre-pyloric area of the stomach,” Dr. Gould said. “It’s a pret-ty radical esophageal-lengthening proce-dure, and it minimizes the opportunity for the stomach to herniate back through the diaphragm into the chest for a recur-rent paraesophageal hernia.”
Although there are no long-term data to support sleeve gastrectomy in patients with paraesophageal hernias, Dr. Gould thinks it makes sense. “It’s analogous to the lengthening procedure we would do.”
The flip side of success in treating these three patient scenarios with bariat-ric surgery is the agony of getting insur-ance to pay for it.
“That’s the difficult part,” Dr. Gould said. “You and the patient decide bariat-ric surgery is the right thing to do, but the insurance company says no and the only thing they’ll pay for is the fundoplication. That’s not an uncommon scenario in my
practice and it’s really frustrating.”
Failed FundoplicationDimitrios Stefanidis, MD, PhD, who
has been using bariatric surgery to treat patients after prior failed fundoplica-tions, also usually gets stonewalled at first by insurance companies that reject his
request to perform a gastric diversion, which is much like a gastric bypass.
“When I think a patient needs to have a gastric diversion done, I submit to insurance and typically they
reject it,” said Dr. Stefanidis, who is med-ical director, Carolinas Simulation Cen-ter, Carolinas Medical Center, Charlotte, N.C.
“Then I have to talk to one of the med-ical directors, and most of the time they approve it. They understand the rationale of why it’s important,” said Dr. Stefanidis,
noting that this approach does not always work with Medicare, which does not fol-low a precertification process.
Dr. Stefanidis started performing gas-tric diversions instead of redo fundo-plications after noting the high rate of fundoplication failure in obese patients and high recurrence rates of reflux after redo fundoplications.
In research presented at the 2012 SAGES meeting, Dr. Stefanidis and col-leagues assessed outcomes and quality of life in 25 patients who underwent gastric diversions, which is like a gastric bypass
13GENERALSURGERYNEWS.COM / GENERAL SURGERY NEWS INTERNATIONAL EDITION 2012 In the News
see GERD AND HERNIA PAGE 14
‘When I think a patient needs to have a gastric diversion done, I submit to insurance and typically they reject it.’—Dimitrios Stefanidis, MD, PhD

but includes removal of the gastric fun-dus, after one or more failed fundoplica-tions (S051).
The mean BMI was 34.4 kg/m2 (22-50 kg/m2). The patients had undergonea total of 40 prior anti-reflux operations,and 23 had associated hiatal hernias.There were no deaths, but 11 patientshad complications, and five requiredreoperation.
At 14 months, mean excess weight loss was 60%, and 96% of patientsreported being free of reflux and feeling better about their appearance. Many felt the operation had improved their socialand sexual lives, and 96% indicated they would do it again. There was no differ-ence in quality of life between the obeseand nonobese patients.
The researchers concluded that gas-tric diversion results in excellent con-trol of reflux and improved quality of life, but noted that the procedure can bequite challenging, especially in patientswhose anatomy has been severe-ly compromised by scarring from past operations.
“We did the vast majority of thesecases laparoscopically; many of those
patients had two or three prior surger-ies, and about 50% had had open sur-geries,” Dr. Stefanidis said. “It can take five to seven hours to do these proce-dures laparoscopically.”
A frequent challenge he has faced has had more to do with bowel obstructions due to previous scar tissue and less to do with taking down the Nissen. “Espe-cially after prior open surgeries, a lot of these patients have incisional hernias in the abdominal wall,” Dr. Stefanidis said.
In addition to the technical chal-lenges is the difficulty in working with patients who may have trouble adjusting to the impositions of bariatric surgery.
“When we do a gastric bypass on obese patients, they know what they’re having and why,” he said. “But the bypass requires a big adjustment phase. You can only eat about one ounce after the sur-gery, and some of the patients who have the procedure for reflux have difficulty adjusting initially despite the counseling we have given them beforehand.”
He often will place a feeding tube in the gastric remnant of normal-weight and/or more complicated patients to help them stay hydrated and avoid hos-pitalization. Incidentally, although the normal-weight patients also lose some weight early on, they tend to gain most
of it back and stabilize at normal.Bipan Chan, MD, of the Cleveland
Clinic in Ohio, and colleagues consid-ered an entirely different population in their research on longitudinal gastrecto-my—following the principles of a Collis procedure with some elements of sleeve gastrectomy—in obese patients with GERD and/or hiatal hernia.
“Most people would agree that the best operation for these patients is a gas-tric bypass, but there is a patient popu-lation that either doesn’t like the idea of gastric bypass or who don’t qualify based on their insurance,” said John H. Rodri-guez, MD, a postgraduate year 4 resident with Dr. Chang’s group who presented the research at SAGES (S106). “That leaves these patients untreated because we don’t want to do an anti-reflux pro-cedure that is likely to fail, and we can’t do a gastric bypass.”
Under institutional review board pro-tocol, the researchers performed longi-tudinal gastrectomy in 19 patients with a mean BMI of 37.8 kg/m2 and type III or IV paraesophageal hernias. Of the 17 who completed follow-up question-naires on weight loss, patient satisfac-tion, use of proton pump inhibitors and/or H2 blockers at a 13-month follow-up, there was a significant decrease in
symptoms and use of medication. Meanexcess weight loss was 29%, with threepatients losing no weight, and some los-ing quite a bit.
In the question-and-answer session following Dr. Rodriguez’s presentation,the procedure was criticized for both destroying the hiatus and for resulting in little weight loss.
“Anytime you try something new, you get a lot of criticism,” Dr. Rodriguez said. “Our operation tries to reproducethe anatomic and physiologic compo-nents that prevent reflux. It also adds the benefits of weight loss, which reducesthe risk for a symptomatic recurrence.”
Dr. Rodriguez explained that they reconstruct the hiatus as they would with any other patient, doing a primary clo-sure and reinforcing with mesh depend-ing on how the defect looks. As for thesleeve portion, which is less restrictivethan a traditional sleeve gastrectomy and doesn’t reach as far, the creation of a tubular stomach eliminates the risk for a volvulus in the event of a recurrence.
“I don’t think we’re combining the worst of both worlds—I think we’re doing the exact opposite, combining thebest of both worlds,” Dr. Rodriguez said.
Patients Prefer Colonoscopy to CT Colonography, Study Shows BY DAVID WILD
SAN DIEGO—Patients undergoing screening for colorectal cancer (CRC) experience less pain and have less anxiety with colonoscopy than patients undergoing computed tomographic colonography (CTC) screen-ing, according to findings from a prospective ques-tionnaire-based study presented at the 2012 Digestive Disease Week meeting (abstract 445).
Researchers asked 90 patients being screened for CRC to undergo both CTC and colonoscopy on the same day and found that 77% said they would prefer colonoscopy for repeat screening.
The findings are important “in that they allow me say with confidence that colonoscopy is not less comfortable thanCTC, but that most patients would findit more comfortable,” said Douglas Fai-gel, MD, professor of medicine at Mayo Clinic in Scottsdale, Ariz., who was not involved in the study.
“Along with these findings, and given that colonoscopy has been shown to prevent CRC inci-dence and mortality while similar data are lacking on CTC, I would recommend colonoscopy as the best test for detecting and preventing CRC,” Dr. Faigel added. “I would reserve CTC for the subset of patients who are truly unwilling to undergo colonoscopy but [are] willing to have a CTC.”
Patient preference may affect adherence to a CRC
screening schedule, said lead investigator Greg Rosen-feld, MD, clinical assistannt professor in the Departmentof Family Practice and a gastroenterology fel-low at the University of f BritishColumbia’s Depart-ment of Medicine in Vancouver. To better understand the ques-tion, Dr. Rosenfeld anddhis colleagues enrolleed90 patients (mean age, 555years) to undergo CTC aand
subsequent colonoscopy on the same day. Participants received midazolam and fentanyl or meperidine during colonoscopy, but no sedation or analgesia during CTC. The subjects completed a 13-item patient satisfaction questionnaire following each procedure.
The findings showed that 36% of patients felt less anxious during colonoscopy, whereas 14% report-ed experiencing less anxiety with CTC (P<0.0001).
ly, 69% of patients Additionallfelt less pain or dis-said they fduring colonoscopy, comfort donly 4% said they whereas
re comfortable dur-felt morTC (ing CT P<0.0001). In PPof overall satisfac-terms
30% of participants tion, 3erred colonoscopy prefeer than CTC in con-rathet to 4% who were tras
ore satisfied with moTC (CT P<0.0001). PP
The remainder of Trespondents to the rhree questions did thtrate a strong pref-not demonst
erence either way.they would rather Notably, 77% of patients said t
undergo colonoscopy for repeat screening.undergo colonoscopy for repeat screAlthough the palatability of CTC may be improved
if patients were to receive sedation and analgesia, Dr. Rosenfeld insisted the conclusions point to the con-tinued place of colonoscopy as the gold standard in screening for CRC.
“I think that, overall, colonoscopy is a better test than CTC for screening, and CTC should be reserved for cases where patients are unwilling to undergo colo-noscopy or it cannot be safely completed,” Dr. Rosen-feld concluded.
Drs. Faigel and Rosenfeld have no conflicts of interest.
14 In the News GENERALSURGERYNEWS.COM / GENERAL SURGERY NEWS INTERNATIONAL EDITION 2012
‘I think that, overall, colonoscopy is a better test than CTC for screening and CTC should be reserved for cases where patients are unwilling to undergo colonoscopy or it cannot be safely completed.’ —Greg Rosenfeld, MD
GERD AND HERNIAContinued from page 13

Experts Discuss Endoscopic Repair of Colonic PerforationsBY MONICA J. SMITH
NEW YORK —The time may have arrived when endosco-KK
pists can, and should, treat perforations in some patients who would have been referred to surgery, according to G.S. Raju, MD, professor in the Department of Gastro-enterology, Hepatology and Nutrition at the University of Texas MD Anderson Cancer Center, Houston, who spoke at the annual course of the New York Society for Gastrointestinal Endoscopy, held in December.
“You could actually manage these patients by endoscopy,” Dr. Raju toldmeeting attendees, sum-marizing his review of thetopic that was publishedin the December issue of Gastrointestinal Endoscopy(2011;74:1380-1388).
“Over the past couple of decades, we have learnedto control bleeding, and it is now extremely rare for apatient to go to surgery to control that complication,” Dr. Raju said. “But we have not done the same thing for per-forations. So in this past decade, we are making progress to treat that complication.”
Colonoscopy-related perforations generally result from mechanical or thermal injury during polypectomy. They are relatively rare—depending on the type of resec-tion used to remove polyps, the risk for perforation can vary from 0.1% to 5%, with endoscopic mucosal resection (EMR) and endoscopic submucosal dissection (ESD) carrying the highest risk. When perforations do occur, they result in an air leak within seconds. If the leak is not recognized and repaired quickly, the injury can result in tension pneumoperitoneum. After time, fluid will leak and lead to peritonitis and sepsis.
Traditionally, upon recognizing that a perforation has occurred, an endoscopist would refer the patient to a sur-geon, who would likely take the patient to the operat-ing room. The patient would undergo general anesthesia, a laparotomy or thoracotomy, and dissection to identify the perforation, followed by repair of the perforation and a fairly extensive recovery.
“This approach has a significant morbidity and mor-tality, which could be avoided if we take a different route of endoscopy closure,” Dr. Raju explained. “That per-foration is going to be small, and we can close it with clips so that the patient doesn’t need surgery. That’sa paradigm shift from surgical to nonsurgical management.”
Moving Toward NonsurgicalManagement
Only a decade ago, surgery was theonly option for patients who suffered perforation—the tools and tech-niques had not yet been developed to allow endoscopists to manageperforations on the spot.
“We started [laboratory animalresearch] to answer the questions:Could perforations be closed? If so,could we create a leakproof sealing?
How far could we push ourselves in terms of the size of the polyp perforation we could close, and how does it compare with surgery?” Dr. Raju said.
Dr. Raju and his team found that indeed they could apply a leakproof seal on perforations, and that these repairs, along with sidestepping all the risks associated with major surgery, also resulted in fewer adhesions than surgery.
“We know now how to close a perforation that is lin-ear and a perforation that is horizontal,” he said.
Of course, prevention is the most important factor in managing perforations. Preventative measures include ensuring thorough bowel preparation, maintaining a dry field and proper colonoscope technique. Examination of any resection site is essential to identify any perforation that might have occurred and to gauge the next step.
“One-third of perforations can be diagnosed at the time of the procedure, and this gives us an opportunity to close a perforation,” Dr. Raju said.
It is also important to identify those patients who will develop post-polypectomy syndrome or a perforation after the procedure, and to recog-nize which patients will benefit from prophylac-
tic closure of a defect. Delayed perforations usually occur within the first day or two, and up to two weeks after the procedure. After two weeks, the patient is in the clear.
“If we want to catch all the perforations that happen in endoscopy, we should set up a system whereby you con-tact the patients within 14 days after the procedure,” Dr. Raju said.
A Surgeon’s PerspectiveGeorge Chang, MD, MS, associate professor of sur-
gical oncology and associate medical director of the Colorectal Center at MD Anderson Cancer Center, commended Dr. Raju and his colleagues for their work in the endoscopic management of perforations.
“We’ve long identified that patients with small per-forations who are clinically asymptomatic and identified with minimal pneumoperitoneum or pneumatosis after endoscopic procedures often can be managed without an operation. Obviously, the goal of treating patients is to treat them in as minimally invasive a way as possible, but without compromising safety, and that’s the key,” said Dr. Chang, who is director of clinical operations in the Minimally Invasive and New Technologies in Oncologic
Surgery Program, at MD Anderson.“I would recommend engaging surgical consultation
earlier rather than later,” he noted. “Patients will need to be very closely monitored to ensure that a more signifi-cant complication has not occurred.”
Close monitoring is also important in the event that the endoscopic repair fails, despite initially appearing to have worked.
“The closure may be attempted and may appear to be technically successful, but the patient could have a clini-cal deterioration,” Dr. Chang explained. “You cannot do this [repair] and then forget about the patient.”
Another point Dr. Chang stressed is that an endosco-pist faced with a complex polyp should take careful stock of his or her own skills in EMR or ESD before attempt-ing to remove the lesion.
“In the heat of the battle, it can sometimes be dif-ficult to make some of those decisions. This is clearly an advanced technique that only appropriately trained endoscopists should attempt. We must remember to first, do no harm.”
Dr. Chang added that the endoscopic management of perforations is not for everyone: “not for every patient, not for every polyp and not for every endoscopist.”
Training OpportunitiesConsidering the rarity of colonoscopy-related perfo-
rations and the challenges of endoscopic management, some may wonder what would motivate an endoscopist to learn these techniques.
“I think, like anything else, this takes time for people to get used to,” Dr. Raju said. “You don’t lose anything if you try to close it; if you can’t, the patient needs to go to surgery. It’s not much different from using a biopsy for-ceps—it’s a bit of a technical detail. The way I look at this is that you need to learn the technique of clip closure so that you can push yourself to do additional things you would not have otherwise undertaken.”
In other words, endoscopists who learn to close per-forations may be able to apply that knowledge to other challenges in endoscopy.
“Learning the techniques to close a perforation will equip you to do a little more, to take the extra steps to remove the large, flat lesions that would tradition-ally have been sent to surgery,” he said, noting that he and his colleagues found this to be true for themselves as they gained confidence in managing perforations endoscopically.
As with learning any new skill or technique, it does take time and practice to manage perforations with through-the-scope or, less commonly, over-the-scope clips. Fur-thermore, gaining experience may be difficult considering
the relative rarity of perforations. Dr. Raju suggests starting small, such as managing routine defects
after polyp removal, to gain skill and confidence with using endoscopic clips.
“When we remove polyps, we often cre-ate defects, which are not through and through. You can try to close those defects [with a clip] and gain experience that way,” he suggested. “If you have a deep defect, you could reinforce the wall and prevent a delayed perforation. This is something you can work on in your practice.”
Drs. Chang and Raju reported no relevant conflicts of interest.
15GENERALSURGERYNEWS.COM / GENERAL SURGERY NEWS INTERNATIONAL EDITION 2012 In the News
‘In the heat of battle, it can sometimes be
difficult to make some of those decisions ... We must remember to first,
do no harm.’—George Chang, MD

An Evolution in the Management of Colonoscopic PerforationsOne Surgeon’s Experience
BY GARY H. HOFFMAN, MD
Endoscopic management using through-the-scope
clips is a proven tool for both preventing a perforation after polypectomy and for treating a recognized perforation (see
“Endoscopic Management of Colonic Perforation,” page 11). However, a more common clinical situation is the presen-tation and recognition of the perforation in the recovery room or after the patient has been discharged. At this point, the patient is in severe pain. The abdominal exam, a mainstay of physical diagnosis, is of no value as the abdomen is distend-ed and tense, rendering the exam useless in following the patient’s clinical course. Operative intervention is commonly the next step.
I would suggest an additional approach in the management of many of these patients with an endoscopic per-foration: immediate, ultrasound-guid-ed abdominal paracentesis, followed by vigilant, nonoperative observation. The patient will be relatively pain-free after the paracentesis, allowing the surgeon to better use the abdominal exam as a guide to continuing close observation or pro-ceeding to the operating room. To fol-low this course, the surgeon must possess surgical fortitude, vigilance and the flex-ibility to change course should the clini-cal findings warrant a change.
Painful ExperiencesIn my experience with more than
13,000 colonoscopies performed over 28 years, four of my patients have expe-rienced perforations, a rate of 0.03%. National rates for colonoscopic perfora-tions range from 0.1% to 0.3%. All four perforations occurred in patients who had undergone a complete colon prepa-ration prior to the colonoscopy. All per-forations were recognized in the recovery room. All of the procedures had been performed without difficulty and with-out a concomitant polypectomy. None of these patients had a large, gaping, scope-induced colotomy.
The first patient underwent an imme-diate laparotomy. Upon opening the abdomen, there was a rush of free air, but a site of perforation or other abnormal-ity was not found. No other intervention was undertaken and the patient did well.
I began to re-evaluate the treat-ment approach to an endoscopic per-foration. I wondered if the cause of the patient’s abdominal pain was secondary to the abdominal free air with peritoneal
distention, or due to either a leak of colonic contents or the actual coloto-my itself. Was an immediate laparotomy really necessary?
An endoscopic perforation might be analogous to a self-sealing, diverticular perforation. In many pain-free patients with a diverticular perforation and an unprepared or “dirty” bowel, treatment is often expectant and nonoperative. I came to believe that it might be possi-ble to avoid operative intervention in patients with post-colonoscopy perfora-tions. I postulated that the intense post-perforation abdominal pain was a result of abdominal distention and peritone-al membrane distention from the intra-abdominal free air and not from the perforation itself or from the leak of any colonic contents.
The Nonoperative Approach BeginsThe next two patients whose perfo-
rations were diagnosed in the recovery room had extensive diverticulosis with thin, fragile diverticular walls. I suspected that the insufflation of air, or the move-ment of the scope through the colon had caused the perforation. I immediately hospitalized these two patients, ordered nothing by mouth and prescribed antibi-otics and liberal amounts of pain medi-cation. I opted then for close observation without immediate surgical interven-tion. I watched these two patients closely, knowing that I could handle the problem if there was a turn for the worse. Initial-ly, I evaluated them three times each day in the hospital and awaited signs of nor-mal flatus production, signaling the return of bowel function. I was fully prepared to operate with even the smallest worrisome physical finding or with worsening labo-ratory data. Both patients did well, with resolution of abdominal pain in four to six days. The abdominal bloating lasted lon-ger but eventually resolved. I took heart that I had been correct in my treatment logic and in my patient care.
The Nonoperative Approach EvolvesThe decision to operate often is driv-
en by the sight of a patient who is in
intense abdominal pain. Urgent oper-ative intervention for a perforated vis-cus is the most common method of treatment. This is one of the first les-sons learned during residency. Howev-er, most surgeons do not perform a highvolume of colonoscopies and thereforedo not have a wide breadth of experi-ence in this specific area. When you area hammer, everything looks like a nail.Surgeons are often hammers. However,not all patients are nails and not all post-colonoscopy perforations require surgicalintervention.
What if I could monitor a pain-freepatient with an iatrogenic perforation? Would I better be able to follow thepatient’s clinical course without being adversely influenced by a tense, painfulabdomen? This situation would be sim-ilar to that of observing a patient whohas a perforated, self-sealing colon-ic diverticulum and minimal abdominalpain. Perhaps not all nails would requireimmediate hammering.
Ultrasound, Paracentesis and Close Observation
When I encountered my fourthpatient with a post-colonoscopy perfo-ration, I asked the radiologist to removeall of the intra-abdominal free air using ultrasound guidance. With this accom-plished, my patient simply sat in thehospital, pain-free and bored. After thereturn of bowel function, the patient was started on a clear liquid diet, whichwas accompanied by mild cramping that quickly resolved. The patient was dis-charged home four days later on a pro-gressive diet.
Rather than using the distended andtender abdomen as reason to operate,I had been able to monitor a pain-freepatient and use any new onset of painas a marker for a worsening situation,possibly requiring surgical intervention.This did not happen and no other inter-vention was necessary.
A Question for You To PonderAlthough I have a new perspective on
the evaluation and treatment of post-colonoscopy perforations, I hope never to need to use this knowledge or expe-rience. A nonoperative treatment pro-tocol requires extreme vigilance anddiligence with frequent examinationsof the patient, the vital signs and labsas well as in-depth training in the careof abdominal emergencies. I knew that I could successfully handle the problemno matter the clinical course, and I couldalways turn quickly to the scalpel if any-thing were to change. I was willing toshoulder the load of watchful waiting,
while gaining some new gray hairs inthe process.
A surgeon is often the final treating physician or consultant responsible for adecision to operate or not. In the end,the surgeon must decide if he or she hasthe experience, the skills and the surgi-cal fortitude to follow a patient who tra-ditionally, and most commonly, is takento the operating room immediately. Thesurgeon will experience considerableanxiety while pursuing this nonoperativepath. Obviously, the anxiety will lessenwith an improving clinical course, but the wait can be trying for the surgeon. Acomfortable, pain-free patient will allow ethe surgeon some increased measure of objectivity, so that the patient can befollowed, and the symptom of pain canbe used more objectively as a signpost,rather than an indication for immediateoperative intervention.
Finally, a fifth patient underwent a rather large cecal polypectomy, at which time I placed three prophylacticthrough-the-scope clips for added pro-tection against a perforation. The patient called the day after the procedure, com-plaining of right lower quadrant pain. Acomputed tomography scan showed twosmall extraluminal air bubbles. The painresolved almost immediately with hos-pitalization, bed rest, intravenous fluidsand antibiotics. The patient was dis-charged home.
Through-the-scope clips havebecome a major adjunct in our arma-mentarium and the authors are to becommended for their analysis of theendoscopic management of colonic per-forations. But, as always and in any situation, experience, planning and pre-paredness are our best tools.
Dr. Hoffman is an attending surgeon,in the Divisions of Colorectal Surgery and General Surgery, and an instructor in the Colon and Rectal Surgical Fellowship at
Cedars-Sinai Medical Center, Los Angeles.He is a senior member of Los Angeles Colon and Rectal Surgical Associates
(www.lacolon.com).
16 Opinion GENERALSURGERYNEWS.COM / GENERAL SURGERY NEWS INTERNATIONAL EDITION 2012
What if I could monitor a pain-free patient with an iatrogenic perforation?
Would I better be able to follow the patient’s clinical
course without being adversely influenced by a tense, painful abdomen?
I asked the radiologist to remove all of the
intra-abdominal free air using ultrasound guidance.
With this accomplished, my patient simply sat in the
hospital pain-free and bored.

Finally – a cost-effective alternative to biologics! GORE® BIO-A® Tissue Reinforcement
is a unique non-biologic scaffold that is gradually absorbed by the body. The open,
highly interconnected 3D pore structure facilitates cell infiltration and growth.
Vascularization begins quickly within one to two weeks.
With a three-year shelf life and no soaking, refrigeration or tracking required,
this versatile material is the easy-to-use, performance-proven alternative that
offers value for surgeons and hospitals alike.
Gore. Because material really does matter.
Products listed may not be available in all markets.
GORE®, BIO-A®
and designs are trademarks of W. L. Gore & Associates.
new choice for complex soft tissue reinforcement.
A Valuable Alternative to Biologics

International Fellowship Programs Open a World of OpportunityBY CHRISTINA FRANGOU
In summer 1997, young German surgeon Hermann Kessler, MD, PhD, arrived in Cleveland, Ohio, to
begin a fellowship in laparoscopic colorectal surgery.Over the next 24 months, Dr. Kessler enhanced
his laparoscopic skills, studying computer program-ming and database management on the weekends. Heimproved his English so much that the Cleveland Clin-ic eventually asked him, with his slight British inflec-tions, to do voice-overs for their medical videos.
Fifteen years later, Dr. Kessler said that international fellowship set the trajectory for the course of his career. “Those two years of fellowship gave me a platform to learn, and the opportunity to build up a network all the way around the world.”
Dr. Kessler returned home to the University of Erlangen in northern Bavaria and set up a laparoscop-ic colorectal program and a database for tracking out-comes. “As soon as I got home, the chairman asked me to do a laparoscopic sigmoid on one of his private patients. They watched me very carefully to make sure that I hadn’t been partying the two years I’d been away. It was a very big event in the department. Even the chair of orthopedic surgery came in to watch,” said Dr. Kessler, now a professor of surgery at the University of Erlangen.
Since then, Dr. Kessler has completed more than 800 laparoscopic colorectal cases, and has presented all over the world, including Japan and Australia. He recom-mends that all surgeons try to get international experi-ence. “It can only be an advantage.”
Evolving International FellowshipsSurgeons have been going outside of their home
countries for centuries to observe other surgical practic-es. Even in the 19th century, surgeons from the United States would travel to Europe for training. According to a 2010 report in the Journal of the American College of Surgeons, about 15,000 American physicians traveled to Europe to train between 1870 and 1914 (211:279-284).
Over the past decade, the number of available inter-national fellowships has grown and is continuing to do so. Although no one tracks all available surgical fel-lowships internationally, there is no question that more professional societies and institutions now fund inter-national fellowships than ever before.
Today, many types of inter-national fellowships exist. They can be clinical or research-based, or both, as short as onemonth or as long as severalyears. Surgeons can travel toall seven continents (in Ant-arctica, contract positions areavailable as medical and surgi-cal officers, but no fellowships per se). Fellowships exist for surgeons just starting out in their career, and those inmid or even late careers. Most are designed to enhancea surgeon’s skills and allow them to gain new culturalexperience. Others, like the Paul Farmer Global Sur-gery Fellowship, are designed to address surgical care inresource-poor settings throughout the world.
A 2010 survey of former recipients of the Ameri-can College of Surgeons’ international scholars program
offers some insight into the benefit of an internation-al fellowship (JACS (( 2010;211:279-284). Participants in the program may be North Americans who trav-el abroad, or surgeons who come to the United States or Canada to train. Many scholars said that the pro-gram had a positive influence on their careers: 38% felt it provided opportunities not otherwise possible, 47% felt it was extremely helpful and 12% believed it was somewhat helpful. Respondents said their trips direct-ly affected their clinical care. Scholars said they learned new techniques, which they now practice in their home departments, and their contact with leading surgeons led to improvements in their work and practice.
Fellowships bring hardships, too. Trainees are away from family and friends; they often work in a second language; the financing can be difficult; and, for some, they worry about putting themselves out of the job mar-
ket in their home country.Sonal Nagra, MD, is cur-
rently spending one year away from his home in Fiji while he finishes a surgical fellowship in Dunedin, New Zealand. He left to gain experience in laparoscopic techniques that are not rou-tinely available in Fiji but it was a tough decision to leave
even for a year. His wife left her job as a general prac-titioner at Fiji’s largest hospital to join him. The cli-mate took some getting used to as well. As warm as New Zealand can be, it doesn’t compare with Fiji. And he had to work to reestablish the confidence of peers, supervisors and staff.
Overall, however, fellows said their internation-al experience helped their careers by enhancing clinical skills and knowledge and developing relationships with
surgeons around the globe.Dr. Nagra said he will return to Fiji better able to
deal with the unique challenges of practicing “Pacif-ic Medicine.” “Being able to gain more experience andbring this back to the Pacific in any form possible wouldbe an asset to the health system locally.”
Dr. Kessler noted, “The relationships that I built dur-ing my fellowship continue to help me, and gave me theopportunity to build up a network all the way aroundthe world.”
Even in the era of Internet, Skype and online educa-tional opportunities, there is tremendous value in train-ing abroad. “There’s a famous quote that sums it up quitenicely: ‘Whenever you can take a walk in someone else’sshoes, the world becomes a better place,’” said Mark Carlson, MD, professor of surgery, University of Nebras-ka Medical Center, Omaha.
In 2007, Dr. Carlson studied in Germany for four weeks as an American College of Surgeons Traveling Fellow. He toured different hospitals and met with sur-geon-researchers, several of whom he continues to work with today.
A traveling fellow can see how other surgeons approach similar problems. They see that there oftenis more than one way to treat a disease and get stilldecent outcomes, said Dr. Carlson. “[This experience]can enhance the fellow’s understanding or tolerancefor doing things differently. Sometimes, because of our training, we fall into a mindset and if anything falls out of that mindset, it might be looked on with disapprov-al. Being abroad enhances the fellow’s ability to keep an open mind.”
The American College of Surgeons, the AustralasianCollege of Surgeons and the Royal College of Surgeons,as well as individual institutions, offer multiple interna-tional fellowships. Application information is availableon the Colleges’ Web sites.
18 In the News GENERALSURGERYNEWS.COM / GENERAL SURGERY NEWS INTERNATIONAL EDITION 2012
‘The relationships that I built during my fellowship continue to help me,
and gave me the opportunity to build up a network all the way
around the world.’—Hermann Kessler, MD, PhD
‘Being abroad enhances the fellow’s ability to keep
an open mind.’—Mark Carlson, MD

Discover Tri-Staple™ Technology
INTELLIGENT DESIGNFOR INTELLIGENT† TISSUE COMPRESSION
With its stepped cartridge face, Tri-Staple™ technology delivers graduated compression, optimizing interaction between the tissue and stapler because it:
Generates less stress on tissue during compression and clamping1
2
Stapling Made Smarter
Compared with uniform compression, graduated compression produces less tissue stress1
UNIFORM COMPRESSION GRADUATED COMPRESSION
1. When compared to Echelon Flex™ green reloads in computer-generated Aachen model to demonstrate stress imparted on porcine GI tissue during compression. 2. When compared to Echelon Flex™ green reloads in bench top model using a porous medium and saline solution.†Benefits are due to graduated tissue compression technology. Device is not software controlled.
See Tri-Staple™ technology in action at www.tristapletechnology.com
Always refer to Instructions for Use supplied with the product for complete Indications, contraindications, warnings, precautions and instructions.
MCGSN1171.indd 1 7/24/12 1:45 AM

New App Predicts Chronic Pain After Inguinal Hernia SurgeryBY CHRISTINA FRANGOU
NEW YORK —Surgeons and patients con-KK
sidering hernia surgery can now use a free app that predicts a person’s chance of experiencing chronic pain after ingui-nal hernia repair, based on the outcomes of nearly 1,700 patients treated over the last five years. The app, the Carolinas Equation of Quality of Life (CeQOL), was officially launched at the 5th Inter-national Hernia Congress and can be
downloaded for free on smartphones and computers.
The app will help educate patients about the risks for chronic pain, an issue some-times glossed over in preoperative discus-sions between physicians and patients, said B. Todd Heniford, MD, senior researcher of the team that designed theapp and chair of gastrointestinal and min-imally invasive surgery at Carolinas Med-ical Center, Charlotte, N.C. “This app opens up the discussion about the chance
of chronic discomfort following inguinal hernia surgery and gives patients a very specific idea of risk,” said Dr. Heniford. “It sets the stage for what we should strive for with every operation: an objective plan to obtain personal quality-of-life [QOL] outcomes for post-operation and therapy.”
Between 8% and 40% of patients who undergo inguinal hernia repair have chronic pain after surgery, according to previous studies. That pain often trig-gers legal action against physicians and
hospital systems. In the Unit-ed Kingdom, chronic pain fol-lowing hernia repair is the No.1 cause of malpractice suits. In the United States, 35%of all malpractice case law that relates to hernia repair is related to chronic pain or discomfort.
Bruce Ramshaw, MD, a her-nia surgeon and chief medical officer for the Transformative Care Institute, in Daytona Beach, Fla., who won the World Hernia Congress Resi-dent/Fellow Research Award for 2012 for this project, said the app marks a change in the way outcomes after medical and surgical care are measured.
“This app is great because it’s focused on patient QOL and outcomes from the patient perspective. That’s the direction we are going as a hernia society.”
The app is based on an algorithm developed by Igor Belyansky, a fellow in laparoscopic surgery at Carolinas Medi-cal Center. Dr. Belyansky and colleagues studied data collected between September 2007 and September 2011 by the Interna-tional Hernia Mesh Registry, a prospec-tively collected multicenter database that includes data on patients from 30 sites in Canada, the United States, Europe and Australia. Patients submit data to the reg-istry, by mail or email, and answer ques-tions regarding QOL, Carolinas Comfort Scale scores and postoperative complica-tions. Researchers studied 2,146 ingui-nal hernia patients, after excluding cases where more than 10 tacks were used in the repair. [An earlier study, from the same group, showed that the use of more than 10 tacks increases long-term pain (Ann Surg(( 2011;254:709-714).]g
The average age of the patients was 56.4±14.6 years; 94% were male and 38% underwent laparoscopic repair. Overall, 20% of patients had bilateral repair and 12% were treated for a recurrent hernia. Almost 58% of patients reported preop-erative pain. Patients were queried at reg-ular intervals for a year after their hernia repair (77.7% follow-up rate). One month after surgery, just over one-fourth of patients (26.1%) reported postoperative pain, which dropped by more than half over the next year, with 12.5% reporting postoperative pain one year after surgery.
The investigators found that younger age, female gender, bilateral repair, recur-rent inguinal hernia repair, preoperative pain, postoperative hematoma, postop-erative recurrence and postoperative uri-nary tract problems all were predictive of chronic pain. Based on these results, the researchers developed an algorithm to predict chronic pain. They used a ran-dom sample of 80% of patients in the
20 In the News GENERALSURGERYNEWS.COM / GENERAL SURGERY NEWS INTERNATIONAL EDITION 2012
12-1
5 M
AY 2
013
12 - 15 May 2013Polish Baltic Philharmonic | Gdansk | Poland
Congress Secretariat
PO Box 24285202 CK ‘s-HertogenboschThe NetherlandsTel +31 73 700 [email protected] www.EHS2013.eu

database to develop the algorithm and confirmed the results in the remaining 20% of patients. A Harvard statistician independently tested the equation, and confirmed its sensitivity and specificity. The app was developed to make the algo-rithm more practical for use by physicians and patients. It is the first app for medical and surgical outcomes, said Dr. Heniford.
According to CeQOL, a young asymp-tomatic patient with no preoperative pain has about a 10% risk for discomfort one year after surgery. Patients with preoper-ative pain, bilateral inguinal hernias and recurrent hernias have an increased risk of developing chronic pain after surgery. Interestingly, older patients are less like-ly tohave symptoms of chronic pain than younger patients.
Dr. Belyansky said the app will help identify high-risk individuals who may benefit from a multidisciplinary treatment approach. “Furthermore, in a preoperative or pretreatment setting, full disclosure of postoperative QOL expectations should become a standard part of the counseling and consent process for surgery and major medical treatments,” he said.
Surgeons at Carolinas currently use the app for all inguinal hernia patients who come into the clinic. Surgeons fill in the app as they speak to patients, or patients do it themselves on an iPad. New prod-ucts come into the hernia field at rapid speed but data on outcomes follow much more slowly, said Shirin Towfigh, MD, associate professor of surgery, Cedars-Sinai Medical Center, in Los Angeles,
and assistant professor of surgery at the University of Southern California.
The new app keeps the focus on patients, she said. “What this app helps quantify in very real terms, and for the first time ever, is how much chronic pain a typical patient may suffer based on simple preoperative symptoms,” said Dr. Tow-figh. “Surgeons can help use this app to educate their patients about the risks and benefits of hernia repair.”
Dr. Heniford, who is the outgo-ing president of the American Hernia Society, encouraged surgeons and their patients to use the app. Currently, the app
applies only to men, because of a shortage of outcomes data following hernia repair in women. He said CeQOL represents a paradigm shift in which the success of a procedure is judged not only by recur-rence rates, which are quite low, but also by patients’ QOL.
“The team should be congratulated for pioneering an app that bridges evolving technology and patient care outcomes. As CeQol gets used by multiple surgeons and patients, its validity and usefulness will be tested,” said Brian Jacob, MD, attending surgeon at Mount Sinai Medical Center, in New York City. “Pain complaints after
hernia surgery, in general, are very subjec-tive, and often factor in many variables that are dependent on any given surgeon's technique, patient population and follow-up regimen,” he said. “Such variables make it tough for an app to reliably account for things like the type of hernia repair being performed, the surgeon's experience with the technique and the location or type of pain complaint being reported. Therefore,the risks that CeQol produces might havea chance to overestimate or generalize.” Dr. Jacob said he plans to use the app inhis own practice and see “how reliable it is with my patients.”
21GENERALSURGERYNEWS.COM / GENERAL SURGERY NEWS INTERNATIONAL EDITION 2012 In the News
‘It’s a tool that sets the stage
for what we should strive for with every operation:
an objective plan to obtain personal quality-of-life
outcomes for post-operation and therapy.’
—B. Todd Heniford, MD
Get concise medical education videos at your fi ngertips.

MCGSNSE118.indd 1 7/24/12 1:49 AM

MCGSNSE118.indd 1 7/24/12 1:49 AM

Lap Subtotal Gastrectomy Could Be Primary Gastroparesis TherapySimilar Morbidity, Mortality As
GES; More Symptom Improvement
BY MONICA SMITH
SAN DIEGO—Gastric electrical stimulation (GES) can improve symptoms in patients with gastropare-sis, but after retrospectively reviewing patient outcomes, researchers at the University of Southern California are now offering laparoscopic subtotal gastrectomy to these patients as a primary treatment option.
“Our initial algorithm for patients with medically refractory gastroparesis who needed surgery was place-ment of a stimulator as a first-line of treatment, and if that fails, a laparoscopic subtotal gastrectomy,” said Joerg Zehetner, MD, assistant professor of surgery in the Department of Surgery, Keck School of Medicine, University of California, Los Angeles, who presented the research at 2012 meeting of the Society of Ameri-can Gastrointestinal and Endoscopic Surgeons (SAGES; S101). “But now, after our study, we think we should tell patients right away that the laparoscopic sub-total gastrectomy also can be seen as a pri-mary therapy because it has a significantly higher rate of symptom improvement, accept-able morbidity and comparable mortality tothe GES.”
The researchers, led by John C. Lipham,MD, evaluated outcomes in 103 patients whoreceived treatment at their center for medi-cally refractory gastroparesis between January 2003 and January 2012; 72 patients receivedGES by either laparoscopy (n=20) or mini-incision (n=52), and 31 patients received alaparoscopic subtotal (n=27), total (n=1) or completion gastrectomy (n=3). Thirty-day morbidity was significantly greater in the gas-trectomy groups than in those who receivedGES (23% vs. 8%) but this difference leveledout over time; in-hospital mortality was about 3% for both groups.
About two-thirds (63%) of the patientsin the GES group achieved symptom improvement as assessed by the Gastroparesis Cardinal Symptom Index, whereas 87% of those in the gastrectomy group report-ed significant improvement in nausea, vomiting, epigas-tric pain and other symptoms that plague gastroparesis patients. In the GES group, 19 (26%) had the device removed due to device malfunction, infection or failure to respond; these patients received laparoscopic subtotal gas-trectomies, and 100% reported symptom improvement.
Of the patients who failed GES, 80% had diabetes-related gastroparesis. “This was a little unusual because you would expect those with diabetes gastroparesis to respond better,” than patients with idiopathic or postsur-gical gastroparesis, Dr. Zehetner said.
The researchers recommended laparoscopic subtotal gastrectomy as a primary treatment, and to reserve GES for patients who don’t want a gastrectomy or a more inva-sive procedure. “The good thing about the stimulator is that we can see it as a breaching treatment; it does not prevent us from doing a gastrectomy,” said Dr. Zehetner.Daniel J. Deziel, MD, Helen Shedd Keith Professor and chair of the Department of General Surgery, Rush Uni-versity, Chicago, noted there was no statistically signifi-cant difference in morbidity and mortality between the
two groups. “One might intuitively think GES a safer approach. Perhaps the number of patients in each group was too small to detect a difference, or this is a seriously compromised patient population to start with,” he said. “It would be important to know the factors that might predict which patients would be more likely to improve following GES, resection or other procedures that have been used.” Dr. Deziel continued, “Is success related to the etiology of the disease? If we knew this, we might be more effective in our initial therapeutic recommenda-tions, and could perhaps identify patients who would not benefit from any major operative intervention other than jejunostomy placement.”
Researchers from the United Kingdom attempted to answer some of these questions by seeing if placement of temporary GES (tGES) could predict which patients would benefit from a permanent GES. “We know now that GES works, and that it works better in some sub-groups,” said N.V. Jayanthi, MD, who presented the research at SAGES (S102). “But we don’t know who fails to improve with GES. So that brings us to tGES.”
Temporary GES: Another OptionThe idea of using tGES to predict who will benefit
from permanent GES is not new. “Dr. Thomas Abell proposed this several years ago,” said Abeezar I. Sare-la, MD, FRCS, Department of Upper Gastrointestinal, Metabolic and Bariatric Surgery, St. James’s Universi-ty Hospital, Leeds, United Kingdom. “But the uptake on tGES has been quite low.” Dr. Abell’s initial research showed a 97% response rate in patients selected by tGES (Digestion 2002;66:204-212). Subsequent research showed a strong correlation between symptom improve-ment in tGES and permanent GES (Gastrointest Endosc 2005;61:455-461), and tGES is used as a treatment for nausea and vomiting in patients who do not have gastro-paresis (Digestion 2011;83:1-2).
Dr. Sarela has long been interested in GES for gastro-paresis, a condition he thinks is far too often under- or misdiagnosed. “The vast majority of patients with gas-troparesis are lost among the diagnosis of functional dys-pepsia,” he said. “I think this is due to lack of awareness. But even if we do make a diagnosis of gastroparesis, there are few definitive treatments.”
The most problematic patients are those who do not improve with dietary changes and prokinetics, and whose
condition is so severe that they cannot tolerate oral intake and require jejunostomy tubes. “That is a miserable exis-tence for these patients,” Dr. Sarela said. “For patients with gastroparesis of this sort, the treatment options are very limited.”
As far as the mechanism by which GES works in gas-troparesis, “we do not know; it is not as simplistic as it improves gastric emptying, and there have been conflict-ing studies,” Dr. Sarela said. “We had positive experi-ences with GES, but one dilemma is that not everyone benefits. It is a fairly straightforward procedure, but still invasive and carries some risk for side effects and compli-cations. It also is very expensive so it’s important to select the patients most likely to have a good response.”
Dr. Sarela’s team set out to see if they could establish a role for tGES in patient selection. Of 71 patients with medically refractory gastroparesis referred to their cen-ter, 51 received tGES.
“We endoscopically placed an electrode into the stom-ach lining, which then runs through the patient’s nose and connects to the stimulator on the outside. During the two weeks this is kept in place the patient maintains a
symptom diary and we assess how well they do,” Dr. Sarela said.
Overall, 39 (74%) patients improved, and 31 received a permanent GES. At 10 months follow-up, 22 (71%) showed significant sus-tained improvement compared with a 50% improvement associated with GES in the longest series to date (Clinical Gastroenterol Hepatol 2011;9:314-319). It is not yet clear lwhether transmucosal stimulation is equiva-lent to GES. Also, not all patients tolerate the stimulation, and leads can dislodge inside the stomach without patients or phy-sicians realizing it. “But lacking other tools, tGES is less invasive and shows that in selected patients, it can improve GES suc-cess rate,” Dr. Javanthi said.
Although the results were promising,the follow-up was fairly short. “We have to keep in mind how durable and significant is the clinical response,” Dr. Deziel noted.
The improvement was based on patient self-reporting. “We didn’t really have any objective physiologic measures of improvement—it would be interesting to know if they had any objective data to quantify the effect of the pac-ing on gastric emptying, and whether it is gastric emp-tying of solids or liquids and how that correlated with symptom improvement,” Dr. Deziel said, adding “One question I have is why some patients responded to tGES and not GES.” The answer may have to do with differ-ences between tGES and permanent GES in terms of how electrodes are placed, and perhaps in other differ-ence between the two modalities that are not well under-stood at this time.
Regardless, “there seems to be a good increase in suc-cess that we see with tGES,” Dr. Sarela said. “Once we are to the stage of treating someone with GES, we should consider a tGES as a selection parameter.”
Most important, however, is managing patient expec-tations. “When they come to our service, they are des-perate and will try anything you want,” Dr. Javanthi said. “This needs to be carefully managed because if it fails, they have no other option than a gastric resection.”
Drs. Jayanthi, Sarela and Zehetner reported no disclosures. Dr. Lipham is a consultant for Medtronic.
24 In the News GENERALSURGERYNEWS.COM / GENERAL SURGERY NEWS INTERNATIONAL EDITION 2012
‘Lacking other tools, tGES is less invasive and shows that in selected patients, it can improve GES success rate.’—N.V. Jayanthi, MD, FRCS

International Panel Issues Statement on Sleeve GastrectomyExperts Stress That
Recommendations Are Not aStandard of Care; Based on
Opinion, Not Randomized Data
BY CHRISTINA FRANGOU
An international panel of surgeons with expertise in laparoscopic sleeve AA
gastrectomy has issued a consensus state-ment on best practices, intended to foster standardization and improve safety for this increasingly popular technique.
“Standardization of the technique of laparoscopic sleeve gastrectomy (LSG) is paramount to improving the safe-ty and maintaining the minimal mor-
bidity and high weight loss efficacy y gte the authors in rates,” wroteport, published their re
in rgery for Obesity SurRelated Diseases and 12;8:8-19).(20
This marks the Tt attempt to firstdardize a bariat-stand
metabolic surgical ric/mdure with respect proced
to patient selection, to pattechnique and complication
management based on concurrent best practices, said Kelvin Higa, MD, one of the panelists and clinical professor of sur-gery, University of California, San Fran-cisco, and director of minimally invasive and bariatric surgery at the Fresno Heart and Surgical Hospital, in California.
“It is intended to serve as a guide for both experienced surgeons and surgeons new to the procedure,” he said.
He cautioned, however, that the doc-ument was intended to serve as a guide, and not to dictate standard of care.
The field is changing so rapidly that already some of the recommendations in the statement are outdated. And among recommendations that haven’t been affected by newer data, there was wide variation, in opinions on many items.
“This represents a snapshot in time and even now, I suspect, some of the conclu-sions reached remain controversial,” said Dr. Higa. “For example, Barrett’s esoph-agus was felt to be an absolute contrain-dication (81%); one might argue as to the severity of Barrett’s in relation to other
patient factors such as age and cardiopul-monary risk.”
In recent years, LSG has morphed from its original role as the first step in a two-stage operation for patients with super-morbid obesity to a standalone restrictive bariatric procedure in people with less severe obesity.
Early studies of the procedure as a standalone operation have been “encour-aging” but the operation is poor-ly standardized; long-term results and
randomized studies are lacking.In March 2011, 27 of the world’s most
experienced surgeons in the procedure (all have performed at least 500 LSGs) met to develop a consensus statement that could improve safety and standardization.
Led by Raul J. Rosenthal, MD, pro-fessor of surgery and chair of minimal-ly invasive surgery and the bariatric and metabolic institute, Cleveland Clinic Florida, the panel agreed on 69 key rec-ommendations for best practices, based
on their collective experience of more than 12,000 cases.
Consensus was determined by greater than 70% agreement. On most areas of consensus, 90% or more of surgeons sup-ported the statement. The panel could not come to consensus on 26 questions, many on technical areas of stapling and on the role of LSG as a conversion procedure.
Among the recommendations, the panel found that LSG is a valid standalone
25GENERALSURGERYNEWS.COM / GENERAL SURGERY NEWS INTERNATIONAL EDITION 2012 In the News
see CONSENSUS PAGE 27
‘This represents a snapshot in time and even now, I suspect, some of the
conclusions reached remain controversial.’
—Kelvin Higa, MD
EAES MembershipIf you are interested to
become an EAES Member,
please complete and
return this reply card.
Reply Card to obtain membership applications
To register your interest in the congress simply return the form below to the EAES Offi ce
Name
Address
City + ZIP Code
Country
Phone Fax
Physician Resident in Training
Last Name
Firt Name
Address
City + ZIP Code
Country
Phone Fax
Fax or send it to:
EAES Offi ce
P.O. Box 335
5500 AH, Veldhoven
The Netherlands
Phone: +31(0)40 252 5288
Fax: +31(0) 40 252 3102
Email: [email protected]
Internet: www.eaes.eu
21st InternationalCongress of the EAES
Vienna, Austria19 - 22 June 2013
HOFBURG Vienna Convention Centre
Congress President: Prof. Selman Uranues
Program Committee Chair: Prof. Nicola di Lorenzo
Deadlines:
Abstract submission deadline:
15 January 2013
Early registration deadline:
15 April 2013
HIGHLIGHTS- Postgraduate courses
- Hands-on training
- New technologies
- “How I do it” video session
- Challenges in colorectal surgery
- Laparoscopic surgery of solid
organs
- Diverticular disease
- Management of complications
- Pro and contra discussions
- Role of laparoscopy in advanced
rectal cancer
- Robotic surgery
- Single vs. reduced port surgery
- Laparoscopy in emergencies
- Free paper sessions: oral, video
and poster
- Special awards and grants
- Technical exhibition

of Düssseldorf, added that POEM still is considered investigational and many questions need to be answered before it is widely adopted.
Other achalasia experts, however, are more cautiousabout adopting this treatment, stating that the excite-ment over the procedure is outstripping the results.
“What I am concerned about is the widespread use of POEM as it is currently being observed without appro-priate evaluation of its place in the therapeutic arma-mentarium for achalasia,” said Carlos Pellegrini, MD,Henry N. Harkins Professor and Chair, Department of Surgery, University of Washington School of Medicine,after results of a new study were presented at the annu-al meeting of the American Surgical Association (ASA)this spring. “All too often, we have seen rapid adoption of new procedures simply because they are new, proceduresthat eventually fade away from practice after [a] consid-erable price has been paid by society.”
The Rise of POEM In 2007, Pankaj Jay Pasricha, MD, and colleagues
reported that they had performed an endoscopic meth-od of esophageal myotomy in animal studies (Endoscopy2007;39:761-764). Soon after, Japanese surgeon Haruhi-ro Inoue, MD, performed a peroral endoscopic myotomy in humans who had achalasia and other spastic esoph-ageal motility disorders (Endoscopy 2010;42:265-271).ySince then, the procedure has been picked up around the world and the video presentations usually create a stir when presented at surgical meetings.
To date, the exact numbers of patients who have undergone POEM worldwide are unknown. Published reports suggest about 300 patients in China, 200 in Japan, 70 in Europe and 100 in the United States have had the procedure. Additionally, many surgeons and gastroenterologists worldwide have undergone some training in POEM even if they do not yet perform it in their practice. Training programsare available in Japan, the UnitedStates and Europe.
Techniques around the worldvary but most follow the same prin-ciple: After the patient goes under general anesthesia, the endoscopist makes a small incision in the muco-sa of the esophagus, approximately 15 cm above the gastroesophagealjunction. The endoscopist then cre-ates a tunnel into the submucosal space, reaching downto the gastroesophageal junction. A long endoscopicmyotomy of inner circular muscle bundles is carried out,leaving the outer longitudinal muscle layer intact. Whenthe procedure is finished, the small opening in the muco-sal lining is clipped.
Only about eight reports of POEM have been pub-lished, most of them small and from single centers. The largest series comes from China and includes 119 patients. In the studies to date, there are no reports of patient deaths. But unconfirmed reports have circulated that a 19-year-old woman in the United States may have died following a POEM procedure. The woman died in a Baltimore hospital from mediastinal sepsis second-ary to a perforation. Before her death, she told hospital staff that three days earlier she underwent an endoscop-ic Heller myotomy. The hospital has released no further details. It’s not known if the woman indeed underwent POEM or if she had a laparoscopic Heller myotomy.
The New Research
This spring, several of the centers most experienced with POEM around the world presented their updat-ed results. In one trial, European investigators present-ed early data from the first prospective international trial of POEM, which included 51 patients with pri-
mary achalasia (29 men; mean age, 43 years) who underwent POEM at centers in Germany, Switzer-land, the Netherlands and Canada. POEM was successfully performed in all patients with a mean operative time of 105 minutes. A transmural esophageal perforation at the muco-sal entry site occurred in one patient; the perforation was addressed intra-operatively and the patient had no
further sequelae. Two patients developed ulcerations (one at the esophagus and one at the cardia) within a month of the procedure. These complications also resolved without sequelae.
The investigators provided some data on three-month outcomes, in the longest follow-up yet avail-able for POEM. In 35 patients followed for at least three months postoperatively, 94% had an Eckhardt score drop of three points or greater, which investi-gators defined as a treatment success. Mean lower esophageal sphincter pressure dropped from 27.4 mm Hg pretreatment to 10.2 mm Hg post-treatment (P<0.001).
However, POEM also appeared to be associated with an increased risk for reflux at a rate similar to that for other conventional achalasia treatments; 20% of patients developed symptoms of gastroesophageal reflux post-treatment.
This finding may contradict one of the chief
arguments for POEM, namely that it may avoid therisk for reflux commonly associated with conventionalachalasia treatments because it leaves intact the anato-my of the lower esophageal sphincter. This study sug-gests that the reflux rate after POEM is comparable tothat of balloon dilation and perhaps even laparoscopicHeller myotomy with fundoplication. Although many experts usually cite reflux rates of 10% to 15% after Heller myotomy with fundoplication, some large pub-lished studies indicate that between 21% and 42% of patients experience post-treatment reflux (Surg Endosc2012;26:18-26; Arch Surg 2005;140:827-833). Addi-gtionally, 17% of patients had erosive esophagitis onfollow-up esophagogastroduodenoscopy.
If POEM does not reduce reflux rates comparedwith laparoscopic Heller myotomy, there is little rea-son to pursue it, said Marco Patti, MD, professor of surgery and director of the Center for EsophagealDiseases, University of Chicago Pritzker School of Medicine. “In my mind, what do you gain? You avoidthe four 4-mm incisions that you use for a laparoscop-ic Heller myotomy with a fundoplication. That’s all.And for a procedure that only has very short-termfollow-up.”
He said he is not surprised by the high rate of reflux.“When you do a POEM, you just cut all the musclesand you open completely the valve, so whatever else isin the stomach will actually reflux.”
The investigators, however, said that the resultssuggest there is a role for POEM in the treatment of achalasia. “POEM is a promising treatment for acha-lasia with adequate symptom relief in 90% of cases,” said lead author Daniel von Renteln, MD, of theDepartment of Interdisciplinary Endoscopy, Universi-ty Medical Center Hamburg-Eppendorf in Hamburg,Germany, adding that further studies are warranted toevaluate long-term efficacy.
In a single-center study, presented at the ASA’sannual meeting, Lee Swanstrom, MD, a surgeon inthe minimally invasive surgery division at The Ore-gon Clinic, in Portland, and colleagues looked at six-month results in 18 patients who underwent POEM.The group included nine women and nine men withmanometrically defined achalasia who were eligible for laparoscopic myotomy. The cohort had a median ASA of 2, experienced symptoms for a median of 25 monthsand lost a median of 12 pounds prior to POEM. Tenpatients had advanced achalasia (Eckhardt score great-er than 6) and 11 had prior endoscopic interventions.The procedures lasted a median of 146±44 minutesand the median length of the myotomy was 9 cm witha median six clips used for mucosotomy closure.
Like the European investigators, Dr. Swanstromand colleagues reported high rates of reflux, this timereaching 46%, based on 24-hour pH tests. The refluxwas categorized as mild to moderate in all patients.
The implications of the acid reflux on long-termresults are not yet determined, said Dr. Swanstrom.Patients who were shown to have reflux were startedon peptic medications even if they were asymptomatic.
The study also showed that POEM was associatedwith a significant reduction of achalasia symptoms. Inpost-procedural exams, patients experienced improve-ments in dysphagia and lower esophageal sphincter pressure, measurable one month after surgery and stillpresent up to six months after POEM. Additionally,patients had very low pain levels after treatment; only two of 18 (11%) required any pain medication follow-ing POEM. They returned to full activities within amean of three days, investigators reported.
26 In the News GENERALSURGERYNEWS.COM / GENERAL SURGERY NEWS INTERNATIONAL EDITION 2012
POEMContinued from page 1
‘POEM is a promising treatment for achalasia with adequate symptom relief in 90% of cases.’
—Daniel von Renteln, MD
Peroral endoscopic myotomy is a potentially promis-ing approach to treat achalasia and esophageal motility disorders, but some experts warn that it is not yet ready for widespread adoption. Image courtesy of Haruhiro Inoue, MD

One patient did experience a major complication, a full-thickness entry incision. Surgeons recognized the problem immediately and placed a single endo-scopic suture to close at the end of the procedure. The patient experienced no ill effects as a result, said Dr. Swanstrom. Minor complications included five cases of capnoperitoneum, one capno-thorax and four mucosotomies.
The study provides “the first objective evidence that thePOEM procedure is a safe andeffective surgical treatment for achalasia palliation,” said Dr.Swanstrom. He stressed that theprocedure is a surgical treatment performed endoscopically, andshould be performed by surgeonsexperienced with endoscopy andachalasia.
In another study, presented at Digestive Disease Week 2012, Chinese surgeons unveiled a new approach to POEM in which they performed a water-jet hydrodissection. They used a HybridKnife (Erbe, Ger-many), a single instrument that combines an ultrafine high-pressure water jet with an electrocautery needle. The surgeon used the water-jet function to perform a needleless submucosal injection, and switched to the electrosurgical function for submucosal tunneling and endoscopic myotomy of inner circular muscle bundles.
In the randomized controlled study of 43 patients who underwent water jet–assisted POEM or conven-tional POEM, the authors found that water jet–assist-ed POEM was associated with a significantly shorter operating time, lower bleeding rate and a reduced use of coagulation forceps. Operating time decreased by 15 minutes with the water-jet approach, from 36.9±10.0 to 21.8±7.1 minutes (P<0.0001). The bleeding rate fell by two-thirds (4.8±1.3% vs. 12.5±4.9%;
P<0.0001), and use of forceps also declined by two-thirds (0.96±1.4% vs. 2.4±2.5; P=0.045).PP
The investigators, led by Zhou Pinghong of the Endoscopy Center, Zhongshan Hospital of Shanghai’s Fudan University, reported no perforations or surgical intervention in either group. The length of the muco-
sa cut, the length of the circu-lar muscle cut and the number of hemostatic clips used were similar between the two groups.
Future for POEMAchalasia experts want more
long-term and well-designed stud-ies before the procedure gains further acceptance. Dr. Pellegri-ni said that past experiences with botulinum toxin and other treat-ments demonstrate the need for
long-term follow-up. Botulinum toxin had excellent results at six months but was later found to fail with-in two to five years (Nat Rev Gastroenterol Hepatol2011;8:311-319).
“It is not until we have a follow-up of at least several years that we can say that a treatment modality is effec-tive in this disease,” Dr. Pellegrini said.
Dr. Patti said he is concerned that the technique is being widely adopted prematurely. In recent months, he received phone calls from other physicians looking for referrals so they can perform POEM on patients. Dr. Patti said he has refused to refer patients to sur-geons and gastroenterologists who do not have a prov-en record with both achalasia and POEM.
“Unfortunately, outside of the centers where it is done with IRB [institutional review board] approval, centers are not explaining that this is experimental and that we really don’t know the results. Dr. Swanstrom is a very skilled endoscopist and surgeon, and yet even
he has a high rate of complications,” Dr. Patti said. “My gut feeling is that it is absolutely unethical to do this procedure outside of IRB protocols in tertia-ry care centers, where they will have long-term follow-up. Second, it should be done by a multidisciplinary group that involves a surgeon, a gastroenterologist and a radiologist.”
Dr. Neuhaus believes that it’s too early to make a decision about POEM but it may yet have a role in future achalasia treatment. He said that POEM may eventually prove most effective for patients who have failed more conventional treatments for achalasia and those likely to have poor results with laparoscop-ic myotomy or pneumatic dilation, primarily younger patients or patients with type III achalasia.
But he too cautioned that many important ques-tions must be answered in clinical trials before POEM is broadly accepted. The predictive factors for failure have to be determined; long-term outcomes must be studied; and the sequelae of reflux after POEM need to be investigated. Even if POEM results hold up in the long term, he said, “these procedures should be limited to centers with expertise in advanced therapeutic endo-scopic and/or laparoscopic surgery, and should be done on an interdisciplinary level with well-chosen patients in carefully designed clinical trials.”
Dr. Renteln reported no relevant disclosures. Other investigators involved with the European trial
reported relationships with Olympus, Torax Medical, Boston Scientific Corporation, Cook, Inc., Movetis
NV, AstraZeneca, Erbe GmbH and Karl Storz. Dr. Swanstrom reported relationships with Boston Scientific
and Olympus Medical. No other surgeon quoted in this article reported having relevant disclosures.
procedure and a valid option for high-risk patients, transplant candidates, morbidly obese patients with metabolic syndrome,patients with a body mass index of 30 to35 kg/m2 with associated comorbidities,patients with inflammatory bowel diseaseand adolescent morbidly obese patients.
The panel just missed agreement onthe statement “LSG will become themost frequently performed [bariatric/metabolic] procedure,” although 67%supported the position.
Panelists were highly divided onmany issues regarding revisions. They did not agree that LSG is a valid optionto convert a failed laparoscopic adjust-able gastric band (67%). Consensus wasreached on the point that Roux-en-Y gastric bypass, not LSG, is the best option to convert a failed gastric bandbut with only 71% of surgeons in agree-ment. Most members of the panel, 95%,said that LSG is an “acceptable optionto convert a successful but complicatedgastric band” but only 72% said that it can be done in a single step.
The panel came to agrree-ment on optimal bouggiesize, saying that a bouu-gie between 32 and 36 FFr(87%) is ideal. They cauu-tioned that a bougie less than 32 Fr might increaase complications and a boougielarger than 36 Fr could lead to a lack d l kof long-term restriction and possible dila-tion of the sleeve.
Studies presented since the panel’s consensus suggest that bougie size can be larger than 36 Fr, said Michel Gag-ner, MD, clinical professor of surgery in Montreal. Two meta-analyses presented at the International Federation for the Surgery of Obesity and Metabolic Disor-ders meeting in September 2011 showed that bougie size below 40 Fr resulted in higher rates of leaks and bioabsorbable buttress material had decreased the rate of leaks by threefold.
“I would suggest surgeons should use a bigger bougie size than in the consensus statement,” said Dr. Gagner.
The panel agreed that staple-line rein-forcement reduces bleeding along the sta-ple line (100%). And 95% of the panel said
ceptable to oversew andit is accsaid it is acceptable to 77% ress the staple line.buttrccording to the panel,Ace heights are still up stapleebate. They agreed that for des should not be used staplesclosed height less than with a c
that of a blue load (1.5 mm) on h f blany part of a sleeve gastrectomy (81%). They suggested that nothing less than a green load up to the incisura angula-ris, nothing less than blue from the inci-sura angularis to the angle of His and nothing less than green when perform-ing revisions should be used.
The authors stressed that it is impor-tant to completely mobilize the fundus before transection (96%) and to take down short gastric vessels before resec-tion (82%).
On the issue of leaks, the panel widely agreed that Roux-en-Y reconstruction is a valid treatment option in proximal chron-ic leaks (90%), while stenting has limited utility for chronic leaks (86%). Stents can be used for an acute proximal leak (93%).
Dr. Gagner warned that the state-ment represents expert opinion, and not
randomized data. Expert opinion is ratedas the lowest level of evidence-based med-icine at level 5, he said. “An expert opin-ion is just an expert opinion and an expert opinion of 20 experts is just an expert opinion of 20 people.”
“This statement is out there just to help practitioners know what the expertsare thinking about sleeve gastrectomy at aparticular moment.”
He added, “I would suggest that sur-geons don’t need to concentrate on mak-ing the most perfect sleeve and aiming for radical weight loss for their patients; Ithink they should concentrate on making the sleeve in the safest way possible, not getting any strictures and avoiding leaksshould be their No. 1 concern.”
Dr. Rosenthal said he and his col-leagues are working on a second publica-tion on LSG that will be based on datafrom the 12,799 cases submitted to theconsensus panel.
The Centers for Medicare & Med-icaid Services (CMS) currently restrictscoverage for LSG. In fall 2011, CMS announced it is reviewing available evi-dence on the use of LSG for the treat-ment of morbid obesity.
27GENERALSURGERYNEWS.COM / GENERAL SURGERY NEWS INTERNATIONAL EDITION 2012 In the News
‘My gut feeling is that it is absolutely unethical to do this procedure outside of
IRB protocols in tertiary care centers, where they will
have long-term follow-up.’—Marco Patti, MD
CONSENSUSContinued from page 25

Find out more about Atrium’s hernia repair solutions at www.atriummed.com/solutions© Atrium Medical Corporation 2012. All rights reserved. Atrium, C-QUR Mesh, C-QUR V-Patch, C-QUR TacShield, C-QUR FX, C-QUR CentriFX,
C-QUR Film, ProLite, ProLite Ultra and ProLoop are trademarks of Atrium Medical Corporation, a MAQUET GETINGE GROUP company.
Handling. Healing. Reinforcement.
TM
Atrium’s full line of products for soft tissue repairempowers the surgeon to choose an appropriate implant withboth mechanical durability and enhanced biocompatibility.

Supported by
Brought to You by
REPORT
July 2012
Benefi ts of GORE® DUALMESH® Biomaterial in Hernia Repair:
A Case-based Presentation
Introduction from the Faculty Chair
Karl LeBlanc, MDBaton Rouge, Louisiana
Considered one of the most common types of surgery, hernia repair remains an ongoing challenge for surgeons because
of the risk for recurrence and other complications.1 As a long-standing material used for hernia repair, expanded polytetrafluorethylene (ePTFE) has made strides to max-imize the outcomes and address the risks. The use of ePTFE has evolved significantly since its introduction in 1983.2 With early iterations, such as the GORE-TEX® Soft
Faculty
Alfredo M. Carbonell, DOChief of Minimal Access
and Bariatric SurgeryCo-Director, The Hernia
CenterAssociate Professor of
Clinical SurgeryGreenville Hospital
System University Medical Center
University of South Carolina School of Medicine
Greenville, South Carolina
Carl R. Doerhoff, MDGeneral SurgeonSurgiCare of MissouriJefferson City, Missouri
Birgitta Hansson, MDDepartment of SurgeryCanisius-Wilhelmina
HospitalNijmegen, The Netherlands
Antonio Iuppa, MDChief, Department of
SurgeryIstituto Oncologico del
MediteraneoViagrande, Italy
Srdjan Rakic, MDStaff SurgeonDepartment of SurgeryTwenteborg HospitalAlmelo, The Netherlands
Songzhang Ma, MDProfessor of General
SurgeryBeijing Redcross
Chaoyang HospitalCapital Medical SchoolBeijing, China
Chair
Karl LeBlanc, MD Associate Medical DirectorSurgeons Group of Baton
Rouge/Our Lady of the Lake Physician Group
Director and Program Chair of the Fellowship Program
Minimally Invasive InstituteAdjunct ProfessorPennington Biomedical
Research CenterBaton Rouge, LouisianaClinical Professor of SurgeryLouisiana State UniversityNew Orleans, Louisiana

2
REPORT
Tissue Patch (GORE®, W.L. Gore & Associates, Inc.), surgeons could apply a solid, microporous sheet of ePTFE to enhance tissue incorporation while minimizing the risk for recurrence.3
With more recent configurations of ePTFE, particularly GORE®
DUALMESH® Biomaterial and GORE® DUALMESH® PLUS Bio-material (GORE®, W.L. Gore & Associates, Inc.), hernia repair has become more innovative, improving fixation to the abdom-inal wall and tissue ingrowth, while minimizing adhesion forma-tion and the risk for recurrence.4 Despite these developments, there are several misconceptions regarding its use and long-term outcomes, as well as the costs associated with the ePTFE material. In the past, several publications provided relevant information on the use of ePTFE, but as with many maturing prosthetic materials, surgeons may be overlooking the benefits of this long-standing material when compared with other pros-thetics, such as polypropylene and polyester mesh.5 Yet, with studies demonstrating an increased risk for recurrence as well as biomaterial-related complications—adhesion formation and tissue ingrowth—and bowel obstruction when using polypro-pylene and polyester mesh, understanding how to use ePTFE in hernia repair for different types of patients will increase awareness of the features that continue to make ePTFE the most effective option.6,7
This report will discuss the benefits of using GORE®
DUALMESH® Biomaterial in hernia repair and provide evidence based on recent studies as well as clinical experience.
Understanding the Mechanism Behind ePTFE
ePTFE is a fluorocarbon polymer with favorable properties—chemical inertness, a high strength-to-weight ratio, thermal resistance, and biocompatibility—that can be expanded and manipulated to modulate tissue response.8 The fluorine atoms shield the carbon atoms, resulting in a low level of reactivity with other chemicals. Consequently, there cannot be chemical cleavage of the bonds or covalent chemical interactions.9 The strength of the fluorocarbon bonds is an underlying characteris-tic of ePTFE mesh. The mesh can be placed either by laparosco-py or by an open surgical approach. Unlike sutures, mesh repair minimizes the risk for recurrence and postoperative pain, and is associated with greater patient satisfaction.10 If adhesions occur, the bowel easily can be dissected free from the prosthesis with-out affecting other tissue or neighboring organs.11,12
Although conventional ePTFE mesh is pliable and can provide effective tissue ingrowth while minimizing inflammation and adhe-sion formation,5,13 the GORE® DUALMESH® Biomaterial product possesses a smooth surface on the visceral side that mitigates against the development of adhesions to the material. The COR-DUROY surface allows for rapid tissue ingrowth. Every surgeon is concerned about the risk for developing a prosthetic infection. The GORE® DUALMESH® PLUS Biomaterial product is the only product on the market that has antimicrobial agents impregnat-ed within it. This has been proven to be an effective agent against methicillin-resistant Staphylococcus aureus (MRSA)14 for up to 14 days postoperatively.
Characteristics of the GORE®
DUALMESH® BiomaterialThe GORE® DUALMESH® Biomaterial currently is used
in hernia repair—open and laparoscopic—and temporary
bridging of fascial defects.15 Unlike its ePTFE predecessors, as well as other meshes—polypropylene- and polyester-based—the GORE® DUALMESH® Biomaterial possesses a 2-sided design with one side to promote ingrowth, while minimizing adhesions on the other.4,16 The GORE® DUALMESH® Bioma-terial features a visceral interface side with pores less than 3 microns in size that minimize tissue attachment, and a fascial side—the CORDUROY surface—that includes ePTFE ridges that stimulate tissue fixation on the abdominal wall to create a neoperitoneal surface.4 The GORE® DUALMESH® Biomateri-al is soft and supple, allowing it to roll up tightly enough to be inserted into the abdominal cavity with or without the use of a trocar.17,18 In the event that the patient requires radiation thera-py subsequent to the hernia repair, ePTFE is able to withstand therapeutic irradiation.19 The GORE® DUALMESH® Biomaterial is the only consistently visible mesh on computed tomograph-ic (CT) scans, which provides a benefit for future evaluations of the abdominal wall to assess the need for any additional surgi-cal interventions.20
Minimizing Adhesion Formation in Hernia Repair
The barrier surface of the GORE® DUALMESH® Biomate-rial is permanent and proven. One study evaluated the sever-ity of adhesions using GORE® DUALMESH® Biomaterial at reoperation (N=65), and found that 91% of patients had filmy, avascular adhesions if they had any at all.12 If one has had the opportunity to reoperate on a patient who had undergone mesh implantation, the challenge of minimizing adhesion for-mation to these materials is not widely publicized. These have proven to be most difficult in many patients regardless of the “tissue-separating” product being used; however, this is not the case with the GORE® DUALMESH® Biomaterial. In cases where patients require reoperation, clinicians are able to see the neoperitoneum on the visceral surface of the material.12
This layer is easily penetrated to expose the underlining ePTFE surface that will appear as pristine as the day of implantation. This layer can be dissected from the mesh so that there is min-imal risk for bowel injury.12 This represents a unique quality of the material that is largely unrecognized.
Improving Recurrence Rate With GORE® DUALMESH® Biomaterial
Recurrence is considered the most important end point in hernia repair.20 With recurrence rates as high as 58%,21 sur-geons have benefited from the use of laparoscopy in ventral and incisional hernia repair. Heniford et al evaluated the safety and efficacy of laparoscopic ventral hernia repair in 850 patients of which 34% were recurrent hernias. GORE® DUALMESH® Bio-material was used in 97% of patients, and the results showed a recurrence rate of 4.7% in patients at mean follow-up time of 20 months.22 Additionally, patients experienced a shorter hos-pital length of stay (LOS, 2.3 days) and a low conversion rate to open surgery (3.4%).22 Similarly, Cobb et al conducted a ret-rospective study (N=270) to evaluate laparoscopic ventral and incisional repairs using GORE® DUALMESH® Biomaterial.17 The average patient was obese and had a large hernia (143 cm2).17
Results showed that the recurrence rate for ventral hernias was 4.7% and that laparoscopic ventral hernia repair was associ-ated with shorter LOS (3 days) and a low rate of conversion to open surgery (2.5%).17

REPORT
3
The strength of the ingrowth of the collagen into the prod-uct is considered critical to the prevention of recurrence of herniation following the repair of these hernias with GORE®
DUALMESH® Biomaterial. This has been confirmed in the lab-oratory. One study evaluated the use of GORE® DUALMESH®
Biomaterial versus polypropylene mesh in 12 rabbits and assessed adhesions, and found that it had greater attachment strength (P=0.02).4 Additionally, the study showed that 12% of the rabbits in the GORE® DUALMESH® Biomaterial group developed adhesions on the visceral side compared with 88% of rabbits in the polypropylene group.4
Minimizing Infection With GORE® DUALMESH®
PLUS BiomaterialIn addition to hernia recurrence, one of the ongoing con-
cerns of using prosthetic materials is the infection rate associ-ated with hernia repair. Hospital-acquired infections, including surgical site infections, continue to be challenging, and result in increased patient pain and discomfort, longer hospital LOS, and a higher mortality rate; thus, it is imperative to identify strat-egies that will minimize the risk for infection while optimizing the outcomes.23 Hernia repair and the use of biomaterials presents a higher potential for infection and, consequently, an increased recurrence rate. Studies show that although infection rates vary depending on whether procedures are open or laparoscop-ic, rates can be as high as 18%.24 In cases where patients are more susceptible to infection, GORE® DUALMESH® PLUS Bio-material has been proven effective in inhibiting bacterial col-onization, while maximizing rapid tissue attachment. GORE®
DUALMESH® PLUS Biomaterial is the only prosthetic mate-rial for hernia repair that incorporates an antimicrobial agent within the product.17 The GORE® DUALMESH® PLUS con-tains both silver carbonate and chlorhexidine diacetate, which have been shown to be bactericidal to 10 different strains of organisms including MRSA, S. epidermidis, Escherichia coli,Pseudomonas aeruginosa, Klebsiella pneumoniae, and Candi-da albicans.25 Harrell et al tested MRSA resistance in 9 types of mesh, including GORE® DUALMESH® PLUS Biomaterial,
Parietex® Composite (polyester/polypropylene/glycol), Mar-lex® (polypropylene), and Composix® (ePTFE/polypropylene), and found that GORE® DUALMESH® PLUS Biomaterial was the only mesh without detectable adherence by MRSA.14 The impregnation of these agents into the biomaterial provides pro-tection against the risk for an infection by inhibiting microbial colonization and initial biofilm formation for up to 14 days fol-lowing repair.14
Clinical Evidence on Lack of Shrinkage For GORE® DUALMESH® Biomaterial
GORE® DUALMESH® Biomaterial continues to be a main-stay of laparoscopic incisional and ventral hernia repairs. Yet, there has been criticism of the material in that there is a per-ception that it shrinks more than other materials used for this type of procedure. Recent studies have provided data on adult patients that address this misconception. Because ePTFE is the only prosthetic consistently visible using CT imaging,26
Carter and colleagues were able to measure the size of the mesh after implantation in 65 patients undergoing CT scan-ning following laparoscopic incisional hernia repair with GORE®
DUALMESH® Biomaterial.27 It was possible to determine the actual size of the mesh after implantation using specialized software, which showed an average shrinkage rate of 7.9%.27
Similarly, Schoenmaeckers et al reported that shrinkage of ePTFE in 656 patients undergoing laparoscopic hernia repair was only 7.5% when measured by CT scan.26
Since the introduction of the ePTFE, a number of studies have outlined its characteristics and demonstrated its use for hernia repair in optimizing outcomes in different types of patients. This report will address many of the current uses of GORE® DUALMESH® Biomaterial, including parastomal hernia repair, re-operative procedures in the presence of mesh, and complex abdominal wall repairs. Certainly, there are many sur-geons who do not believe that a product is better just because it is new. More importantly, however, the science as well as a product’s track record should provide guidance when selecting a prosthetic material to repair any and all hernias.
Case 1An 85-year-old man undergoing parastomal hernia repair.
Al fredo M. Carbonell, DO
T he patient had a history of invasive bladder carcinoma. Twelve years ago, the patient
had undergone a radical cystoprostatectomy with an ileal conduit urinary stoma. He pre-sented with both a midline incisional and a
recurrent parastomal hernias. He had undergone 2 failed open non-mesh attempts at parastomal hernia repair in the past ( Figure 1). After discussing open and laparoscopic options, the patient chose laparoscopy.
A laparoscopic Sugarbaker repair was performed. Taking into account the midline incisional defect, the hernia defect area measured 11 x 9 cm (Figure 2). The GORE® DUALMESH®
Figure 1. Computed tomographic scan image demonstrating both the parastomal and midline incisional hernia defects.

4
REPORT
Biomaterial was chosen for the repair as it is the most proven mesh for the laparoscopic repair of parastomal hernias, and its laminar mesh structure prevents an aggressive mesh–bowel inflammatory reaction, thus preventing bowel erosion.28 The GORE® DUALMESH® Biomaterial was trimmed to a size mea-suring 18 x 21 cm. Cardinal sutures were placed along the edges of the mesh and paired sutures were placed along the side of the mesh where the bowel would exit (Figure 3). The mesh was positioned against the abdominal wall using both permanent sutures and tacks (Figures 4 and 5). Total operative time was 98 minutes, and postoperatively the patient did very well and was discharged home after a 4-day hospital stay. At the 4-year follow-up, the patient remained free of cancer and without any recurrence.
DiscussionThe laparoscopic Sugarbaker parastomal hernia repair is a
durable hernia repair option. The physical properties of GORE®
DUALMESH® Biomaterial with its laminar construction make it the safest mesh to use for this technique and this has been borne out in the clinical literature.16,28 Parastomal hernias pose a unique problem for general surgeons because unlike other types of hernias of the abdominal wall, the defect needs to be covered completely while still allowing a functional portion of the intestine to exit the abdominal wall through that very same defect. The Sugarbaker parastomal hernia repair technique accomplishes this task by positioning the mesh directly against the abdomi-nal wall, while allowing the bowel segment to course in between the mesh and the abdominal wall. The bowel then re-enters the peritoneal cavity through a sling or shower curtain deformity between the mesh and the abdominal wall. Because the bowel essentially is draped over the edge of the mesh, the mesh has to have certain properties to avoid mesh–bowel erosion.
ConclusionFor years, GORE® DUALMESH® Biomaterial has been the
most consistently used type of mesh for laparoscopic incision-al hernia repair as well as parastomal hernia repair, particularly,
Figure 2. Intraoperative photo demonstrating the parastomal hernia defect.
Figure 5. Immediate postoperative photo demonstrating the laparoscopic incisions and the transabdominal fascial suture site incisions.
Figure 4. GORE® DUALMESH® Biomaterial in position against the abdominal wall.
Figure 3. GORE® DUALMESH® Biomaterial with cardinal sutures in place prior to implant.

REPORT
5
the Sugarbaker technique.28,29 GORE® DUALMESH® Bioma-terial is a nonporous, laminar mesh structure, which allows for adequate mesh ingrowth, without the dense adhesions seen with other mesh types.30,31 Although the macroporous or corduroy side of the mesh is placed in direct contact with the bowel, the mesh does not erode into the bowel. Despite its many years of use, there have been no reported events of spontaneous GORE® DUALMESH® Biomaterial–bowel erosion as have been seen with both polyester and polypropyl-ene-based meshes.32 Its laminar structure prevents the mesh from growing into the bowel, despite the continuous peristalsis of the bowel across the mesh edge.
Q&ADr. LeBlanc: Do you prep the bowel in these patients?Dr. Carbonell: No. A bowel prep is traditionally used to decrease the chance of wound infection or anastomotic leak-ing at the time of bowel resection or reanastomosis. Not only have studies demonstrated the opposite to be true, but we also
are not opening the bowel during parastomal hernia repair. If one was to injure the bowel during the repair, it would be inad-visable to proceed with mesh implantation anyway. Hence, bowel prep is not useful.Dr. LeBlanc: How far apart are the sutures placed?Dr. Carbonell: We have traditionally used a spacing of every 5 cm or so for standard laparoscopic incisional hernia repair, the thought being that if the mesh stays where you place it, the hernia is unlikely to recur. The only way to ensure that the mesh stays where you place it is to use multiple, permanent, trans-abdominal fascial sutures.Dr. LeBlanc: Do you place an abdominal binder on these patients postoperatively? If so, how long do you make them wear it?Dr. Carbonell: Binders have not been shown to decrease seroma, but in some patients it helps them feel like they have support of their abdomen while they ambulate. If the binder is comfortable for them, I have these patients wear it for support for approximately 6 weeks.
Case 2A 39-year-old man with a large recurrent midline incisional hernia.
Carl R. Doerhoff, MD
T he patient was morbidly obese with a body mass index (BMI) of 40 kg/m2 (height: 68
inches, weight: 120 kg). A construction work-er, the patient was on medical disability. Sig-nificant past medical history included a prior
colostomy and subsequent subtotal colectomy with J-Pouch for ulcerative colitis in 1998. He reported having 15 abdomi-nal operations with multiple attempts at hernia repair, includ-ing multiple mesh failures. In 2009, he underwent a repair using the components separation technique with polypropylene but he developed yet another recurrence. He had a second repair using the components separation technique in early 2010 using biologic mesh. Following this operation, he developed a large wound infection that was treated with damp-to-dry dressings and healed by secondary intention.
When the patient was referred and first examined in July 2010, he had a large abdominal wall defect, an exceedingly thin, weeping re-epithelialized wound, and a central “mass” of contracted polypropylene measuring 2 x 8 inches. His CT scan showed a meshoma with surrounding inflammation.
In August 2010, the patient underwent operation to remove the infected polypropylene and biologic mesh and excise the thin re-epithelialized skin. The patient’s midline incision-al defect and left-sided colostomy hernia were closed using a No. 1 absorbable monofilament. The incision was left open; however, despite negative pressure wound therapy and damp-to-dry dressings, the wound continued to have a draining sinus tract. In November 2010, the patient underwent oper-ation to remove an infected polypropylene stitch. This time, his wound healed with damp-to-dry dressings. A follow-up CT scan showed no residual mesh or inflammation but did show an abdominal wall defect measuring 22 x 32 cm. The residual
abdominal wall could not be medialized to decrease the size of his defect. Consequently, the defect had to be bridged with a piece of mesh that could withstand significant intraabdominal pressure and protect abdominal viscera.
In February 2011, the patient’s hernia was repaired lapa-roscopically, using 2 pieces of GORE® DUALMESH® PLUS Biomaterial, each measuring 26 x 34 cm. The first 2.5 hours of the procedure required extensive adhesiolysis. The falci-form ligament was taken down and the urinary bladder was mobilized posteriorly. Outside the abdomen, the 2 pieces of GORE® DUALMESH® PLUS Biomaterial were oriented trans-versely, overlapping by 5 cm, and affixed to one another with 22 interrupted stitches of CV-0 GORE-TEX® Suture (Figure 6).
Figure 6. Large recurrent midline incisional hernia repaired using 2 pieces of GORE® DUALMESH® PLUS Biomaterial (26 x 34 cm).

6
REPORT
Cardinal stitches of CV-0 GORE-TEX® Suture were placed at 6 locations on the mesh. The conjoined pieces of mesh were introduced into the abdomen through a 15-mm trocar site. Car-dinal stitches were brought transabdominally, using a GORE®
Suture Passer. The edge of the mesh was then positioned using an absorbable tacker. The caudal portion of mesh was affixed to the pubis and Cooper’s ligaments with a nonabsorb-able tacker. Next, 25 transfascial CV-0 GORE-TEX® Sutures were placed circumferentially around the 2 pieces of mesh using a GORE® Suture Passer. Last, a double crown of 300 nonabsorbable tacks was placed circumferentially. All skin incisions were closed using running nonabsorbable sutures. The entire operation was completed in 5 hours. The patient had an uneventful hospital course and was discharged on post-operative day 5.
ConclusionThis operation demonstrates that bridging is still a viable
alternative even for the largest of multiple recurrent hernias.
Q&ADr. LeBlanc: Do you attempt to make the obese patients lose weight prior to surgery?Dr. Doerhoff: Typically, yes. Especially if they have failed more
than one repair or if their BMI is greater than 45 kg/m2. Studies have shown that the recurrence rate in the obese population can be as high as 50%. Although some patients refuse to lose weight, a durable laparoscopic repair can be done.Dr. LeBlanc: Why did you choose the laparoscopic approach rather than an open approach to this hernia?Dr. Doerhoff: I’m not a personal fan of open repair because of increased risk for infection, seroma, and wound complications. The laparoscopic repair allows me to visualize the complete abdominal wall and identify any additional smaller hernias, as well as “Swiss cheese” defects. Therefore, I do a better job of overlapping a defect laparoscopically. Additionally, studies of incisional hernias have shown that covering the entire prior inci-sion may reduce recurrence. Dr. LeBlanc: Do you think that the PLUS product was the ideal product for this individual and why?Dr. Doerhoff: I always feel better adding an antimicrobial bar-rier (silver and chlorhexidine) to the mesh in a patient who has had a previous mesh infection. Additionally, studies have shown a higher incidence of wound infections in the obese population. The antimicrobial technology has been shown to be effective against both gram-positive and gram-negative bacteria as well as MRSA for up to 14 days postoperatively.
Case 3A 66-year-old obese woman undergoing parastomal hernia repair.
Birgitta Hansson, MD
T he patient had a BMI of 33 kg/m2 and suf-fered from rheumatoid arthritis. The lat-
ter was treated with steroids. Five years ago, a Hartmann’s procedure was performed to manage acute diverticular disease with perfo-
ration and peritonitis. The patient complained of pain caused by the stretching of the abdominal wall and poor fitting of the appliance, resulting in leakage and peristomal skin irritation. Furthermore, she reported to have cosmetic problems that caused her quality of life to decrease significantly since the hernia became symptomatic. Clinical examination showed a huge parastomal hernia in the left lower abdomen. The hernia could not be reduced.
A CT scan was performed to measure the hernia and rule out concomitant incisional hernias because these could not be palpated at clinical examination. The results showed a hernia of more than 5 cm with herniation of the small bowel and an inci-sional hernia in the lower abdomen (Figure 7). Because of her growing complaints, a laparoscopic approach was determined to be optimal, and both hernias were repaired using 2 separate pieces of GORE® DUALMESH® Biomaterial. The parastomal hernia was repaired using the Sugarbaker technique, by which the mesh covered the hernia opening with an overlap of 4 cm on each side once the stoma loop was lateralized. The double crown technique was used for the incisional hernia. The post-operative course was uneventful. Figure 8 shows the postop-erative result after the Sugarbaker technique.
Discussion A parastomal hernia is a common complication after stoma
formation. Risk factors are obesity, chronic cough, or when the created size of the stoma opening is too wide. A symptomatic parastomal hernia can be treated by relocating the stoma, or by local reinforcement of the abdominal wall with a prosthet-ic mesh. Stoma relocation involves relaparotomy and replace-ment of the stoma to the contralateral side. In addition to the risk for developing an incisional hernia at the midline or at the old ostomy site (20%-30% of all cases), this technique carries a recurrence rate of up to 36%.33,34
Mesh repair has a lower recurrence rate. Depending on tech-nique and placement, recurrence rates vary between 6.9% and 17.8%, and the overall mesh infection rate is 2.3%.28 The mesh can be placed in an onlay, retromuscular, or intraperitoneal posi-tion, either by laparoscopy or open approach. A review of the literature finds no significant advantage of one approach over the other, while randomized controlled trials have proven to be lacking.28 The laparoscopic approach is safe and feasible and causes minimal damage to the insufficient abdominal wall.35
GORE® DUALMESH® Biomaterial is used to reinforce the abdominal wall. GORE® DUALMESH® Biomaterial is the most often used prosthetic material in parastomal hernia surgery because it is soft and pliable and easy to handle. It results in less severe adhesions to the viscera compared with polypro-pylene meshes.16 If adhesions occur, the bowel can easily be dissected free from the prosthesis.11 A potential drawback of

REPORT
7
GORE® DUALMESH® Biomaterial is risk for infection.13 In the only prospective series reporting on the laparoscopic repair of 55 parastomal hernias with an ePTFE patch, prosthetic infec-tion was found in 3.6%.35 Once the mesh is infected, it should be removed. In general, infection of the mesh is not a major issue in a laparoscopic ventral or parastomal hernia surgery because it is considered to be a clean operation. Although when a bowel injury with fecal spill occurs, we recommend postponing mesh implantation for at least 6 weeks.
Conclusion When performing a parastomal hernia repair, surgeons can
use a mesh with or without a slit. The former technique also is called the “keyhole technique.” Unfortunately, this technique has a high recurrence rate caused by progressive widening of the central keyhole. Recurrence rates of more than 30% have been reported.28,36 In 1985, Sugarbaker described the non-slit technique by which a mesh is used to cover the hernia open-ing with an overlap of 4 cm on each side, after the stoma loop is lateralized (Figure 8).37 A considerably lower recurrence rate of 11.6 % was reported.28 Recently, the use of biologic grafts in parastomal hernia repair has been published. Review of the literature, however, does not show better outcomes with the more expensive biologic materials.38
Therefore, the Sugerbaker technique with GORE®
DUALMESH® Biomaterial is an effective technique.
Q&ADr. LeBlanc: Do you ever use transfascial sutures for these procedures? If so, when do you decide to do so? Dr. Hansson: Yes, I always use 2 nonresorbable sutures (Prolene 2.0) at the most lateral border of the mesh, at the left and right side of the “lateralized” bowel. Besides this, the mesh is fixed with titanium tacks (ProTack).Dr. LeBlanc: Do you make an attempt to close the hernia defect in these cases?Dr. Hansson: Nowadays, I don’t close the defect anymore. I did in my study on the keyhole technique and after a while we noticed that the sutures disrupted. Since then, I prefer a tension-free repair. In the study, we operated on 55 consec-utive patients with a symptomatic parastomal hernia using the keyhole technique (see also references). We closed the defect using a non-resorbable suture 0. We reoperat-ed on 9 out of 55 patients because of a recurrent symptom-atic hernia. During reoperation, we found that the sutures were disrupted and the mesh was everted due to the high intraabdominal pressure. We concluded that suturing the defect only has temporary result, after a while sutures dis-rupt. That’s why we believe that a tension-free repair is best.
Case 4A 62-year-old woman with cirrhosis and massive hepatitis C virus–related (Child B) ascites undergoing intraperitoneal incisional hernia repair.
Antonio Iuppa, MD
T he patient underwent colon resection for a perforation resulting from diverticulitis 10
years ago. She developed a giant incisional her-nia with skin ulceration and high risk for spon-taneous evisceration (Figure 9). On admission
to the hospital, the patient’s bilirubin and albumin levels were 2.5 mg/dL and 2.8 g/dL, respectively. The antithrombin III level was normal, and there was no previous history of bleeding.
Initial management included sterile occlusive dressing, fluid repletion, and antibiotic administration. The attempt to reduce ascites with medications failed. A peritoneovenous shunt was implanted 1 week before the repair with satisfactory results with a significant reduction of the ascites.
The initial plan was to perform a suprafascial extraperitone-al repair in order to avoid the opening of the peritoneum; how-ever, the preservation of the peritoneum was impossible thus requiring an intraperitoneal approach. The procedure started
Figure 7. Preoperative CT scan of obese patient with parastomal hernia.
Figure 8. Postoperative CT scan with ePTFE patch.

8
REPORT
with the creation of a plane between the muscular fascia and the subcutaneous tissue so that the mattress stitches would not have to pass through the skin. The hernia sac was opened but not resected so that it could cover the mesh at the end of the operation. A posterior plane was created on the posteri-or face of the abdominal wall, detaching the adhesions, the falciform ligament, and the bladder. Once this posterior sup-port area was created, the size of the defect was measured. It was determined that the prosthesis should be 4 to 5 cm larg-er than the defect, enabling gentle retraction of the margins without causing excessive tension. In this case, the GORE®
DUALMESH® PLUS Biomaterial, measuring 26 x 36 cm, was used to avoid leakage of ascitic fluid.
The fixation of the mesh was performed with nonresorbable monofilament material. The suture was passed in U-shape from the abdominal wall to the mesh about 4 cm from the margin of the defect, covering the entire circumference of the defect. After ensuring that the tension was uniform across the entire mesh, the residual hernial sac covered the mesh using inter-rupted reabsorbable stitches. This step separated the mesh from the subcutaneous tissue and supported the migration of fibroblasts into the mesh (Figure 10).
The patient had an uneventful recovery except for the appearance of a subcutaneous hematoma that did not require surgical intervention.
ConclusionOne of the most challenging situations in patients with inci-
sional hernias is the presence of cirrhosis and ascites. Abdom-inal wall repair in a patient with advanced cirrhosis presents an operative risk of great magnitude and may pose a considerable technical problem when complicated by the leakage of ascitic
fluid, necrosis of the abdominal wall with ulceration, rupture, strangulation, or infection.
Management of umbilical hernias in patients with cirrho-sis and ascites remains difficult as these patients often have advanced liver disease and are at greater risk for complications following any surgical intervention. Elective surgical repair pre-vents complications, whereas morbidity after emergency sur-gery is up to 30%.39-41 Repair should be performed after optimal management of ascites, which includes fluid and salt restriction, diuretics, and possibly undergoing a transjugular intrahepatic portosystemic shunt procedure before surgery, if the ascites are difficult to control with medical therapy.
Q&ADr. LeBlanc: What type of antibiotic coverage did you admin-ister to this patient?Dr. Iuppa: I administered vancomycin hydrochloride (2 g daily for 3 days), a nonabsorbable antibiotic that is effective against anaerobic gram-negative rods. It is useful in controlling portal systemic encephalopathy in patients with cirrhosis. It also has been shown that changes in blood ammonia concentrations correspond very well with changes in the number of anaerobic gram-negative rods in feces.Dr. LeBlanc: Are the antimicrobial agents in the PLUS materi-al essential in cases such as this one?Dr. Iuppa: The GORE® DUALMESH® PLUS Biomaterial is the only 2-sided, prosthetic material with antimicrobial agents (chlorhexidine and silver) that act synergistically to inhibit bac-terial colonization and resist initial biofilm formation on the bio-material for up to 14 days following implantation. This is of great importance when used in immunodepressed or debili-tated patients such as those with cirrhosis.
Figure 9. Preoperative CT scan showing the ascites and the hernia.
Figure 10. Postoperative CT scan showing the position of the mesh and the shunt.

REPORT
9
Case 5A 48-year-old man undergoing continuous ambulatory peritoneal dialysis after ventral hernia repair.
Srdjan Rakic, MD, FACS
T he patient had undergone open sublay repair of a midline suprapubic incisional
hernia using a polypropylene mesh (15 x 10 cm), and a laparoscopic repair of a large inci-sional hernia at midline incision using GORE®
DUALMESH® Biomaterial measuring 20 x 30 cm.42 Because the patient refused hemodialysis and kidney transplantation was not an option given the patient’s poor vascular status, continuous ambulatory peritoneal dialysis (CAPD) was indi-cated.42 Being aware of the potential risk for infection, it was essential to avoid compromising the GORE® DUALMESH® Bio-material while inserting the CAPD catheter. A CT scan was used to determine the precise position of the mesh (Figure 11) and, consequently, to preoperatively draw a sketch of the mesh on the abdominal wall of the patient (Figure 12). With the mesh outlined, the CAPD catheter was implanted laparoscop-ically using 2 trocar ports that were positioned left laterally in the abdomen, while avoiding the GORE® DUALMESH® Bio-material.42 Intraoperatively, the mesh was completely covered with intact neoperitoneum and omental adhesion.42 The pro-cedure was carried out uneventfully. During the next 2 years, the patient experienced occasional episodes of CAPD-related peritonitis, requiring removal (3 times) or reinsertion (2 times) of the catheter.42 The latter procedures were performed using the same technique as the initial insertion of the CAPD cathe-ter: left or right (Figure 13). In all instances, the mesh was left undisturbed and remained uninfected.
Conclusion This case highlights the importance of a radiopaque mesh
for subsequent insertion of a catheter for CAPD. Abdominal surgery after laparoscopic ventral or incisional hernia repair (LVHR) can be challenging and requires careful planning and
execution. A detailed preoperative assessment of the position and size of the previously implanted mesh is highly desirable. ePTFE mesh has the unique property of being revealed by CT scan due to its density and structure.
Reoperations in patients with a previous LVHR carry a risk for mesh contamination and infection. Therefore, it is impera-tive to avoid an incision through a mesh or coming into con-tact with it whenever possible, in order to minimize the risk for contamination. In this specific case, the ability to radiologically visualize the existing mesh provided the ability to safely insert a CAPD catheter 3 times and at 3 different sites, despite only having access to a relatively small portion of the abdominal wall during the procedure.
Q&ADr. LeBlanc: Is it true that this is the only product that is truly “visible” on CT scans?Dr. Rakic: Yes. Visibility of meshes or the property of being revealed by high-resolution imaging techniques such as CT or MRI is determined by 2 factors: predominantly by specif-ic properties of mesh itself and, to a lesser degree, by a host inflammatory reaction generated by implanted prosthesis.
The most important properties of a mesh that determine its radiologic visibility are the density, structure, and thick-ness of the material used to produce a mesh. The only mesh-es that are always visible are GORE® DUALMESH® and GORE®
DUALMESH® PLUS because of the high density of the materi-al (ePTFE), its homogenous structure (nonwoven/not knitted), and its thickness (1, 1.5, or 2 mm). This feature allows for very precise and reliable measurements of mesh dimensions, posi-tion, and overlap.
Figure 11. Preoperative CT scan showing position of the mesh.
Figure 12. Preoperative sketch of the mesh on the abdominal wall of the patient.

10
REPORT
The visibility of composite meshes containing ePTFE com-ponent (Composix, Ventralex, Intramesh T1, Dulex) is less consistent: Because the ePTFE component is much thin-ner (≤0.20 mm, they sometimes are clearly visible, whereas at other times they are not. As a general rule, these meshes easily can remain unrecognized when not specifically sought after and vice versa. Less reliable and less consistent vis-ibility of these meshes do not allow for precise radiologic measurements compared with the first group.
All other meshes in general are not visible due to their iso-attenuity relative to surrounding structures. Indirect evidence of mesh presence occasionally can be recognized, especially with MRI, due to the intense inflammatory response surround-ing and incorporating the mesh (eg, scar tissue, meshoma). However, precise and reliable measurements of mesh dimen-sion, position, and overlap are impossible.Dr. LeBlanc: In your mind, does the fact that this material did not become infected despite the episodes of peritonitis prove that there is no more susceptibility to infection with this mate-rial compared with other prosthetic materials?Dr. Rakic: Possibly. I assume that every mesh placed into the abdominal cavity will be covered with some sort of neoperito-neum within a relatively short period. Complete neoperitoneal-ization of mesh might well be crucial in protection against mesh infection. If this is really true, it is probably irrelevant as to which mesh is lying under neoperitoneum.
Case 6Two patients undergoing giant abdominal wall desmoid resection and abdominal wall reconstruction.
Songzhang Ma, MD
A 31-year-old woman was diagnosed as having a giant desmoid tumor measur-
ing 25 cm in diameter infiltrating the thickness of the abdominal wall (Figure 14). A com-plete tumor excision was performed and the
abdominal wall was reconstructed using GORE® DUALMESH®
Biomaterial measuring 20 x 30 cm (Figure 15). A 25-year-old woman had undergone an abdominal wall
desmoids resection 3 years prior to reoperation. Myocutaneous
flaps covered the defect. The tumor was recurrent in situ from the previous year and quickly developed a mass measuring 12 cm in diameter (Figure 16). The tumor was resected care-fully and completely, and the abdominal wall was reconstruct-ed using GORE® DUALMESH® Biomaterial measuring 18 x 24 cm (Figure 17).
GORE® DUALMESH® Biomaterial was secured to the deep fascial elements using interrupted 1-0 Prolene sutures, and subcutaneous closed suction drains were placed.
With both patients, the procedures were done successfully. The postoperative period of both patients was uneventful and without any serious complications (eg, seroma or infection).
Figure 14. A giant desmoid measuring 25 cm in diameter infiltrating the thickness of the abdominal wall.
Figure 15. GORE® DUALMESH® Biomaterial was used to reconstruct the abdominal wall.
Figure 13. Plain x-ray of the abdomen show-ing the continuous ambulatory peritoneal dialy-sis catheter introduced on the right side of the abdomen. Tacks used for fixation of the mesh also are visible.

REPORT
11
Postoperative treatment included sulindac 200 mg twice daily and tamoxifen 20 mg daily. At the 24-month follow-up, there was no desmoid recurrence on the abdominal wall. Inspira-tion and expiration tests were used to measure the patients’ abdominal wall compliance, and the results showed that the abdominal wall was functioning well without any feeling of stiffness in both patients. At 6 months, however, a CT scan indicated a newly developed tumor on the mesentery in the 25-year-old patient.
ConclusionGORE® DUALMESH® Biomaterial was selected for abdomi-
nal wall reconstruction based on its following features consid-ered ideal for the repair:
• Mesh pliability and compliance• Tensile strength• Biocompatibility• Minimal adhesion with tissue and organs to the material• Firm tissue attachment and ingrowth
Superficial desmoid tumors should be resected before they become large. The reconstruction of the abdominal wall with large soft tissue defects is usually very complicated and can be performed immediately using myocutaneous flaps or syn-thetic meshes. Because positive margins were associated with a 2-fold increased risk for local tumor recurrence, additional resection on surrounding tissue should be completed. Patho-logic examination of the specimens of our patients confirmed
the presence of 2 to 3 cm margins of normal tissue around the tumor.
Q&ADr. LeBlanc: How long were the drains left in place?Dr. Ma: The time at which to pull the drainage tube is deter-mined by the amount of drainage. If drainage is less than 20 mL per day, it can be considered. In case 1, the drainage tube was retained for 7 days. In case 2, it was retained for only 3 days. Because of the large surgical wound, tube retainment depends on the clinical signs. After pulling the tube out, an ultrasound or CT scan may be necessary. If any fluid remains in the abdominal cavity around the mesh, additional treatment may be required. In case 1, a CT scan showed a small amount of fluid but did not require further treatment.Dr. LeBlanc: If you have to reoperate on patients such as these, what do you recommend for closure of the DUALMESH®?Dr. Ma: This is a good question. In my opinion, if abdomi-nal surgery is required, the conventional method to open and close the abdominal wall is acceptable. If the reoperation is for recurrence of tumor, removal of the tumor is performed first, and then repair the subsequent abdominal defect with a new mesh. It is easy to separate the adhesion between the GORE®
DUALMESH® Biomaterial and the organ surface; the healed area with mesh in the abdominal wall can still be closed by using continuous sutures.
References1. Zografos GN, Mitropapas G, Vasiliadis F, et al. Open and laparo-
scopic approach in incisional hernia repair with ePTFE prosthesis. J Laparoendosc Adv Surg Tech A. 2007;17(3):277-281.
2. W.L. GORE & Associates, Inc. GORE DUALMESH Biomaterial. Flagstaff, AZ. 2010.
3. W.L. GORE & Associates, Inc. GORE-TEX soft tissue patch. http://www.GOREmedical.com/stp. Accessed April 3, 2012.
4. LeBlanc KA, Bellanger D, Rhynes KV 5th, Baker DG, Stout RW. Tissue attachment strength of prosthetic meshes used in ventral and incisional hernia repair. A study of the New Zealand White rab-bit adhesion model. Surg Endosc. 2002;16(11):1542-1546.
5. Bauer JJ, Salky BA, Gelernt IM, Kreel I. Repair of large abdominal wall defects with expanded polytetrafluoroethylene (PTFE). Ann Surg. 1987;206(6):765-769.
6. Matthews BD, Pratt BL, Pollinger HS, et al. Assessment of adhe-sion formation to intra-abdominal polypropylene mesh and polytet-rafluoroethylene mesh. J Surg Res. 2003;114(2):126-132.
7. Novitsky YW, Harrell AG, Cristiano JA, et al. Comparative eval-uation of adhesion formation, strength of ingrowth, and textile properties of prosthetic meshes after long-term intra-abdominal implantation in a rabbit. J Surg Res. 2007;140(1):6-11.
8. W.L. GORE & Associates, Inc. Proprietary ePTFE technology from GORE. http://www.GORE.com/en_xx/products/venting/packag-ing/eptfe_membrane.html. Accessed April 3, 2012.
9. “Material Matters” in Surgery. http:www.GOREmedical.com/news-letters/clsoing-remarks/issue-6/featured-topic.html. Accessed April 4, 2012.
Figure 16. A recurrent desmoid tumor 3 years prior to reoperation.
Figure 17. GORE® DUALMESH® Biomaterial is used to reconstruct the abdominal wall with interrupted 1-0 Prolene sutures.

12
REPORT
10. Burger JWA, Luijendijk RW, Hop WCJ, Halm JA, Verdaasdonk GG, Jeekel J. Long-term follow-up of a randomized controlled trial of suture versus mesh repair of incisional hernia. Ann Surg. 2004;240(4):578-585.
11. Wassenaar EB, Schoenmaeckers EJP, Raymakers JFTJ, Rakic S. Subsequent abdominal surgery after laparoscopic ventral and inci-sional hernia repair. Hernia. 2010;14(2):137-142.
12. Koehler RH, Begos D, Berger D, et al. Adhesion formation to intraperitoneally-placed mesh: reoperative clinical experience after laparoscopic ventral incisional hernia repair. JSLS. 2003;7(4):335-340.
13. Bleichrodt RP, Simmermacher RK, van der Lei B, et al. Expanded poly-tetrafluoroethylene patch versus polypropylene mesh for the repair of contaminated defects of the abdominal wall. Surg Gyne-col Obstet. 1993;176(1):18-24.
14. Harrell AG, Novitsky YW, Kercher KW, et al. In vitro infectability of prosthetic mesh by methicillin-resistant Staphylococcus aureus. Hernia. 2006;10(2):120-124.
15. A legacy of innovation in hernia repair: CORDUROY tissue ingrowth surface. GORE DUALMESH Plus. Flagstaff, AZ: W.L. GORE & Associates, Inc.; 2007.
16. Simmermacher RK, Schakenraad JM, Bleichrodt RP. Reherniation after repair of the abdominal wall with expanded polytetrafluoro-ethylene. J Am Coll Surg. 1994;178(6):613-616.
17. Cobb, WS, Kercher, KW, Matthews, et al. Laparoscopic ventral hernia repair: a single center experience. Hernia. 2006;10(3): 236-242.
18. LeBlanc KA. A new method to insert the DUALMESH prosthesis for laparoscopic ventral herniorrhaphy. JSLS. 2002;6:349-352.
19. Boyce B. Physical characteristics of expanded polytetrafluoroeth-ylene grafts. (Stanley JC, ed). In: Biological and Synthetic Vascular Prostheses. New York: NY: Grune and Stratton; 1982:553-561.
20. Wassenaar EB, Schoenmaeckers EJ, Raymakers JT, Rakic S. Recurrences after laparoscopic repair of ventral and incisional hernia: lessons learned from 505 repairs. Surg Endosc. 2009;23(4):823-832.
21. Luijendijk RW, Hop WC, van den Tol MP, et al. A comparison of suture repair with mesh repair for incisional hernia. N Engl J Med. 2000;343:392-398.
22. Heniford BT, Park A, Ramshaw BJ, Voeller G. Laparoscopic repair of ventral hernias: nine years’ experience with 850 consecutive hernias. Ann Surg. 2003;238(3):391-399; discussion 399-400.
23. Engemann JJ, Carmeli Y, Cosgrove SE, et al. Adverse clinical and economic outcomes attributable to methicillin resistance among patients with Staphylococcus aureus surgical site infection. Clin Infect Dis. 2003;36(5):592-598.
24. Rios A, Rodriguez JM, Munitz V, Alcaraz P, Pérez Flores D, Parilla P. Antibiotic prophylaxis in incisional hernia repair using a prosthesis. Hernia. 2001;5(3):148-152.
25. W.L. GORE & Associates, Inc. GORE DUALMESH Plus Biomaterial. Flagstaff, AZ. 2010.
26. Schoenmaeckers E, van der Valk S, van den Hout H, Raymakers JF, Rakic S. Computed tomographic measurements of mesh shrinkage
after laparoscopic ventral incisional hernia repair with an expanded polytetrafluoroethylene mesh. Surg Endosc. 2009;23(7):1620-1623.
27. Carter PR, LeBlanc KA, Hausmann MG, Whitaker JM, Rhynes VK, Kleinpeter KP, Allain BW. Does expanded polytetrafluoroethylene mesh really shrink after laparoscopic ventral hernia repair? Hernia. 2012;16(3):321-325.
28. Hansson BM, Slater NJ, van der Veldon, et al. Surgical techniques for parastomal hernia repair: a systemic review of the literature. Ann Surg. 2012;255(4):685-695.
29. Carlson MA, Frantzides CT, Shostrom VK, Laguna LE. Minimal-ly invasive ventral herniorrhaphy: an analysis of 6,266 published cases. Hernia. 2008;12(1):9-22.
30. Matthews BD, Mostafa G, Carbonell AM, et al. Evaluation of adhesion formation and host tissue response to intra-abdominal polytetrafluoroethylene mesh and composite prosthetic mesh. J Surg Res. 2005;123(2):227-234.
31. Jenkins ED, Yom V, Melman L, et al. Prospective evaluating of adhesion characteristics to intraperitoneal mesh and adhesiolysis-related complications during laparoscopic re-exploration after prior ventral hernia repair. Surg Endosc. 2010;24(12);3002-3007.
32. Foda M, Carlson MA. Enterocutaneous fistula associated with ePTFE mesh: case report and review of the literature. Hernia. 2009;13(3):323-326.
33. Carne PW, Robertson GM, Frizelle FA. Parastomal hernia. Br J Surg. 2003;90(7):784-793.
34. Allen Mersh TG, Thomson JP. Surgical treatment of colostomy complications. Br J Surg. 1988;75(5):416-418.
35. Hansson BM, de Hingh IH, Bleichrodt RP. Laparoscopic hernia repair is safe and feasible: early results of a prospective clinical study includ-ing 55 consecutive patients. Surg Endosc. 2007;21(6):989-993.
36. Hansson BM, Bleichrodt RP, de Hingh IH. Laparoscopic parasto-mal hernia repair using a keyhole technique results in a high recur-rence rate. Surg Endosc. 2009;23(7):1456-1459.
37. Sugarbaker PH. Peritoneal approach to prosthetic mesh repair of parastomy hernias. Ann Surg. 1985;201(3):344-346.
38. Slater NJ, Hansson BM, Buyne OR, Hendriks T, Bleichrodt RP. Repair of parastomal hernias with biological grafts: a systematic review. J Gastrointest Surg. 2011;15(7):1252-1258.
39. Carbonell AM, Wolfe LG, DeMaria EJ. Poor outcomes in cirrhosis-associated hernia repair: nationwide cohort study of 32,033 patients. Hernia. 2005;9(4):353-357.
40. Choi SB, Hong KD, Lee JS, et al. Management of umbilical hernia complicated with liver cirrhosis: an advocate of early and elective herniorrhaphy. Dig Liver Dis. 2011;43(12):991-995.
41. Ahmad TAA, Ali SM, Zaghloul N, El-Minshawy O. Complicated umbilical hernia in cirrhotic patients with ascites. Egyptian J Surg. 2004;23(2):167-171.
42. Schoenmaeckers E, Woittiez AJ, Raymakers J, Rakic S. Continu-ous ambulatory peritoneal dialysis after intra-abdominally placed synthetic mesh for ventral hernia repair. J Laparoendosc Adv Surg Tech A. 2011;21(8):741-743.
SR
123
RP
1564
Disclaimer: Gore products referenced within, if any, are used within their FDA approved/cleared indications. Gore does not have knowledge of the indications and FDA approval/clearance status of non-Gore products. Gore makes no representations as to the surgical techniques, medical conditions or other factors that may be described in this article. The reader is advised to contact the manufacturer for current and accurate information. AQ0106-EN1
This monograph is designed to be a summary of information. While it is detailed, it is not an exhaustive clinical review. McMahon Publishing, GORE, and the authors neither affirm nor deny the accuracy of the information contained herein. No liability will be assumed for the use of this monograph, and the absence of typographical errors is not guaranteed. Readers are strongly urged to consult any relevant primary literature.
Copyright © 2012, McMahon Publishing, 545 West 45th Street, New York, NY 10036. Printed in the USA. All rights reserved, including the right of reproduction, in whole or in part, in any form.
Financial Disclosures:
Dr. LeBlanc reported that he is a consultant and on the speakers’ bureau for W.L. GORE, CR Bard, and Covidien. He also is on the medical advisory board for Via Surgical. Dr. Carbonell reported that he is a consultant and on the speakers’ bureau for W.L. GORE and a consultant for Ethicon Endo-Surgery and Bard Davol. Dr. Doerhoff reported that he is on the speakers’ bureau for W.L. GORE, Ethicon Endo-Surgery, and Covidien. Drs. Hansson, Iuppa, Rakic, and Ma reported no relevant financial conflicts of interest.

Supported by
Brought to You by September 2012
REPORT
Surgeons’ views are based on individual experiences and are not to be construed as claims made by EES.
Technological Advancements in Tissue-Sealing Devices
Introduction
Laparoscopic surgery began to gain ground in the operating rooms (ORs) of the 1990s. Since then, this minimally invasive approach has amassed substantial evidence to support its equivalence and/or superiority to open techniques in terms of blood loss, pain, hospital length of stay, return to normal activities, cosmesis, and a host of other factors.1-3 Laparoscopy is now considered the standard of care for the majority of procedures for
which it is indicated. Although researchers continue to explore its utility, few would dispute its overall advantages for patients.
Laparoscopic surgery still presents challenges to the surgeon in terms of access, visualization, and tactile feedback, as well as ergonomic compromises that result in an occupational injury rate similar to that of symphony musicians.4,5 Hemostasis, one of the basic components of surgery, is particularly demanding during
Faculty
David Arrese, MDSurgical OncologistRiverside Methodist HospitalColumbus, Ohio
Matthew Kalady, MDAssistant Professor of SurgeryCleveland ClinicCleveland, Ohio
James Dana Kondrup, MDMinimally Invasive SurgeonLourdes HospitalBinghamton, New York
Benyamine Mizrahi, MDColorectal SurgeonColorectal Surgical Associates, PCKansas City, Missouri
Sharon L. Stein, MDDirector, Acute Intestinal Failure ClinicCase Western Reserve University
Medical CenterCleveland, Ohio
Sonia Ramamoorthy, MDAssociate Professor of SurgeryChief, Section of Colon
and Rectal SurgeryRebecca and John Moores
Cancer CenterUniversity of California, San Diego
Health SystemLa Jolla, California

2
REPORT
laparoscopic procedures due to the limitations of vessel-sealing methods that solely rely on compression, such as sutures, clips, and staples. Thus, as technology has evolved to propel the adoption of laparoscopy, surgeons have come to depend on energy-based vessel-sealing devices that offer reliable seals within the confines of a laparoscopic port.
But not all energy-based devices are created equal. In bipolar energy devices, the current only passes through tissue that is located between the instrument’s electrodes. This offers potential advantages over monopolar devices regarding safety and precision related to the unintended dispersal of current.6 Even bipolar energy devices do not perform the same, as they can vary in measures such as burst pressure and thermal damage to vessels.7
The ENSEAL® System, marketed by Ethicon Endo-Surgery, Inc., was developed to meet and exceed the demands of vessel sealing while also offering the ability to perform other functions. Specifically, ENSEAL® Devices provide reliable hemostasis, are designed to minimize thermal spread, and can be used to grasp and dissect tissue,8 which can offer flexibility and efficiency to surgeons. In 2003, the FDA cleared the bipolar ENSEAL® Device to seal vessels up to 7 mm in diameter.9 Since then, ENSEAL® Technology has been modified and refined, largely based on surgeon feedback. Today, ENSEAL® Devices are indicated for an array of procedures, including general, colorectal, gynecologic, bariatric, thoracic, and urologic surgeries.9 The latest additions to the ENSEAL® Portfolio include the G2 Curved and Straight Tissue Sealers for laparoscopic surgery and the G2 Super Jaw Tissue Sealer for open procedures, which expand the ENSEAL® Line with superior sealing and a superior sealing experience.
Considerations for the ENSEAL® System
James Dana Kondrup, MD, a minimally invasive surgeon at Lourdes Hospital in Binghamton, New York, has been practicing minimally invasive surgery for 24 years. He began using the ENSEAL® System 3 years ago to bolster his armamentarium (rather than to replace his existing devices). “In the early years, I was using the tri-polar electric cautery, then I started using the HARMONIC®,” he said. “I travel around the world and teach internationally, and I always come across surgeons using different energy sources. I knew it was important for all surgeons to be familiar with at least 2 energy sources, so when ENSEAL® came out, it was an excellent opportunity to add it to my regimen of surgical tools.”
There were several features that Dr. Kondrup liked in particular about the ENSEAL® System. “The first was that the energy inside the device had minimal thermal spread, only a few millimeters from the instrument,” he said. Dr. Kondrup also
liked the fact that he could tell where the cutting blade was at all times. “The ENSEAL® I-BLADE™ has a gold square that tells you exactly where it is during the surgical procedure,” he added (Figure 1).
“Finally, another feature I like is the learning curve. As I travel all over the world, I have to teach residents and new surgeons how to use ENSEAL® on demand. I find the learning curve to be very manageable,” said Dr. Kondrup.
Sonia Ramamoorthy, MD, associate professor of surgery, chief, Section of Colon and Rectal Surgery, Rebecca and John Moores Cancer Center, University of California, San Diego Health System in La Jolla, performs approximately 80% of her cases laparoscopically. The majority of these cases are cancer- and inflammatory bowel disease–related procedures. Dr. Ramamoorthy described herself as a former diehard user of LigaSure™ devices. However, she noticed that many of her colleagues—including those recognized as pioneers and innovators of minimally invasive surgery and laparoscopy—were using ENSEAL® Devices in videos of laparoscopic procedures presented at surgical meetings. “I wondered what the difference was,” she said. “So I thought I’d give it a try and see how I liked it.”
It took Dr. Ramamoorthy a few cases to get used to the ENSEAL® System, especially when training residents. “But once I started, I really found it to be very reliable in terms of getting at mesenteric vessels,” she said. “I think LigaSure™ and ENSEAL® are both good devices, but the reliability of one over the other is what really matters to me. When I am
Figure 1. Additional compression is achieved by advancing the I-BLADE™ during coagulation.Image courtesy of James Dana Kondrup, MD.

REPORT
3
going through difficult or inflamed mesenteries, or [performing surgery on] obese patients, I find ENSEAL® does a good job of sealing the tissue.”
This reliability also may have been the factor that influenced her peers. “I asked quite a few of them why they use ENSEAL®, and they said they just thought it was reliable in sealing the vessels. They felt confident about the hemostasis, and I would agree with that,” said Dr. Ramamoorthy.
ENSEAL® Vessel-Sealing Technology
Advancing Superior Sealing
ENSEAL® Devices use a patented temperature-controlled, bipolar energy delivery system in the jaw and a unique cutting mechanism, the I-BLADE™, to produce minimal thermal spread and strong, uniform compression across the entire length of the seal.8 Teeth located along the jaw of each instrument serve to facilitate the handling and grasping of tissue. Surgeons also can combine different shaft lengths and jaw configurations (ie, straight or curved) to accommodate a variety of procedures.10 Together, these features allow for the safe and thorough transection of large tissue bundles, multifunctionality, and superior sealing.
Excessive thermal spread from bipolar instruments is a major concern for laparoscopic surgeons.11 The nature of laparoscopy limits surgeons’ ability to assess the degree to which potentially traumatizing heat is being transferred beyond its intended target. Surgeons usually cannot feel it themselves, so they need to be able to understand the thermal spread and capabilities of their energy device.
“During an open procedure, if it’s getting too hot I can adjust appropriately to make sure any tissue is far enough away,” said David Arrese, MD, a surgical oncologist at Riverside Methodist Hospital in Columbus, Ohio. “But when I’m operating laparoscopically, I don’t have my hand in there. I’m concerned about thermal spread because I’m dissecting close to ureters, the small bowel, or the colon, and I’m really concerned about injuring these structures.”
ENSEAL® uses sophisticated technology to measure the temperature of the instrument and to modify the energy flow so that the temperature is high enough to seal vessels, but low enough to minimize lateral thermal spread. “The thermal spread is very minimal with ENSEAL®,” Dr. Arrese said. “It has carbon fibers within the jaw that deactivate when the tissue reaches 100οC, so that limits the thermal spread.”
ENSEAL® Devices use positive temperature coefficient (PTC) technology to achieve closely regulated energy with a minimal degree of thermal spread. The PTC polymer located in the instrument’s top jaw contains chains of conductive particles that continuously modulate energy throughout
the activation cycle. As the temperature in the jaw reaches 100οC, the polymer expands and the chains break apart. The disconnection of the chains results in a discontinuation of conductivity, which prevents the flow of electric current, ultimately reducing the temperature. When temperatures fall below 100οC, the conductive particle chains come back together, thus restoring the flow of electricity and bringing the temperature back up.12
This back-and-forth, hot–cold cycle continuously relays while the instrument is in use, and it is sensitive along the entire length of the jaw. This is important because tissues can be highly heterogeneous and can vary in density. “The PTC in the ENSEAL® Jaw has sensing particles, so it does a good job in making sure the temperature is uniform throughout rather than having a portion where, for example, if it’s just spreading from a middle line toward the sides, the temperature might not be as uniform and you might not get the same kind of seal in all places,” said Sharon L. Stein, MD, director, Acute Intestinal Failure Clinic, Case Western Reserve University Medical Center in Cleveland, Ohio.
Dr. Ramamoorthy appreciates being able to rely on the designed minimal thermal spread of the ENSEAL®. “The lateral spread is minimal in either direction, and I think that is very important, especially as you’re doing work around neurovascular bundles,” she said. “You want to make sure you are treating only the vessel you want to treat and not, perhaps, the nerves that are sitting around it. Otherwise, you could injure or damage someone’s nerve supply for bladder or sexual function, as we see in colorectal surgery.”
Dr. Kondrup feels confident in how ENSEAL® functions. “ENSEAL® only goes up to 100οC. It will not go above that, and other instruments will go well above that,” he said. “Tissue damage can result from direct cautery from the electricity and from heat damage, when the temperature goes so high it actually damages the tissue laterally. So I feel it’s important to keep heat down so that you don’t cause any additional damage to the tissue.”
Advantages of the I-BLADE™
For Dr. Stein, the most important feature of any vessel-sealing device is its ability to provide sound, reliable hemostasis. “The most important thing is the security of the vessel transection. I don’t typically use staplers to transect vessels; for the inferior mesenteric artery or ileocolic artery, I typically use an advanced-energy device,” she said. “Having the security that the device is going to seal and seal well every time is imperative—a no brainer. If you start to have leaks or bleeding afterward, that is completely unacceptable.”
ENSEAL® uses tissue compression along with heat to seal vessels, and its cutting mechanism, the I-BLADE™,

4
REPORT
thoroughly and cleanly transects tissue. It offers strong, uniform compression along the entire length of the jaw,7
and it delivers appropriate doses of energy to each tissue thickness within it. The cutting blade is located within the instrument’s teeth, which enables the blade to stay in place. “Being [located] within the teeth, it’s sort of like the I-BLADE™ is between railroad tracks. The knife cannot jump out of the teeth of the instrument,” said Dr. Arrese.
“With a lot of other devices now, the cutting already happens or you just push a button and it’s an automated process. But the ENSEAL® gives you a little more visual and physical control over how quickly your tissue is cut,” explained Dr. Ramamoorthy. “The way the ENSEAL® works is that you first grasp the tissue and then apply the compression. As you apply compression, you activate energy; you advance the I-BLADE™ forward and energy delivery moves with the blade because you’re compressing. The I-BLADE™ is nice because you can see how fast or slow you are cutting the tissue; that’s under your control.”
Although competing energy devices may lose compression as the surgeon moves distally,a ENSEAL® is designed to provide durable, consistent, and reliable compression throughout the entire length of the instrument (Figure 2).13
Matthew Kalady, MD, assistant professor of surgery at the
Cleveland Clinic in Ohio, noted that during both his surgical residency and fellowship, he and most of his peers used LigaSure™ devices. “But I tried ENSEAL® because its technology is a little bit different,” he said. “[ENSEAL®] has the I-BLADE™ Technology, and I think there is a bit more uniform distribution of the energy and compression on the vessels. I think it gives a good seal, and [the compression] goes all the way out to the end of the vessel as well.”
ENSEAL® Devices can seal tissue of all sizes, up to and including vessels that are 7 mm in diameter.8 “It’s a very consistent instrument when it comes to hemostasis,” said Dr. Kondrup. “That’s one of the advantages of ENSEAL®, the reliable hemostasis when I’m doing more difficult cases. It’s very user friendly as far as controlling blood vessels.” In a benchtop comparison of seal strengths across 52 device activations, porcine arteries sealed with ENSEAL® displayed superior burst strengths versus those sealed with LigaSure™ (P<0.05; Figure 3).13
Dr. Ramamoorthy also is confident that the ENSEAL® will reliably perform the tasks for which it is indicated. “I think any device I use has to be able to seal a large amount of tissue. Being able to reliably seal 5- and 7-mm vessels is important,” she said. The ability of the ENSEAL® to seal large vessels may reduce reliance on other instruments,
Figure 2. Compression analysis of 2 laparoscopic energy-delivery devices.a a In side-by-side benchtop testing, average compression at distal 0.11 in of jaw: 187 psi (SD=81 psi) for ENSEAL® TRIO vs 40 psi (SD=9 psi) for LigaSure™.
From reference 13.
0
50
100
150
200
250
Proximal third Medial third Distal third
Jaw Position
■ ENSEAL® G2 Curved
■ LigaSure™ 5 mm Blunt Tip
Ave
rag
e C
om
pre
ssio
n,
psi
a In side-by-side benchtop testing, average jaw compression was 201 psi (SD=42 psi) for ENSEAL® TRIO versus 96 psi (SD=9 psi) for LigaSure™. Data on file. Ethicon Endo-Surgery, Inc.

REPORT
5
and may improve efficiency in the OR by reducing the number of instruments needed.
Versatility and Customization
The ENSEAL® System is designed not only to provide consistent, reliable hemostasis in vessel sealing, but also can serve as a tissue grasper and dissector. “These days we’re trying to find instruments that are multifunctional, that don’t just deliver energy, but that also can help us to do a little dissection or pick things up, and I think ENSEAL® allows us to do things like that,” Dr. Ramamoorthy said. “It’s a nice device for us to use in terms of not having to switch multiple devices in and out of the patient’s abdomen. I can dissect with it, I can seal vessels with it, and then I can keep going with my dissection. I don’t have to switch out to a grasping device. It works pretty well for several different applications in the abdomen.”
Dr. Ramamoorthy suspects that being able to use an energy device that fits through a 5-mm port, unlike a large stapler that would require a 12-mm port, allows surgeons to reduce the size of the incision needed to achieve reliable vessel sealing. “This really facilitates laparoscopic cases,” she added.
Dr. Kondrup finds that the multifunctionality of ENSEAL®
Devices improves his operating efficiency (Figure 4). “There are some instruments on the market that just cauterize, but don’t cut,” he said. “With ENSEAL® you have the ability
to activate the cautery and then quickly cut; when you’re moving along and cutting adhesions, it’s very rapid. You don’t have to take the instrument out and get a hemostatic device, because it is a hemostatic device.”
A study by Person and colleagues investigated several parameters of vessel sealing in porcine vessels and compared
Figure 3. Strength of tissue seals across multiple device activations.a
a Benchtop study using 5-mm porcine carotid arteries. Burst pressure was measured over 52 activation cycles (P<0.05).
From reference 13.
Figure 4. An ENSEAL® Device coagulating and cutting the mesoappendix during an appendectomy.Image courtesy of James Dana Kondrup, MD.
600
700
800
900
1,000
1,100
1,200
1,300
1,400
1,500
1,600
2 9 16 23 30 37 44 51
ENSEAL® G2 Curved ENSEAL® G2 Straight LigaSure™ 5 mm
Ve
sse
l B
urs
t P
ress
ure
, m
m H
g

6
REPORT
ENSEAL® with the LigaSure™ V and LigaSure Atlas™.7 They found that ENSEAL® offered faster seal times, comparable seal quality, and higher burst pressure versus LigaSure™. ENSEAL® also created less radial thermal damage to the adventitial collagen than LigaSure™.7
Several risk factors are associated with time on the operating table and shorter times on the operating table offer better patient outcomes.14 “So it’s nice to be able to save some time, save the patient money, save the hospital money, and reduce risk by getting patients off the table,” said Dr. Kondrup.
ENSEAL® also offers surgeons a greater degree of ergonomic flexibility. It can be used by right- or left-handed surgeons and is available in shaft lengths of 14, 25, 35, and 45 cm.10 Surgeons can choose a straight or curved tip, the latter of which Dr. Ramamoorthy prefers. “I think having a curved tip allows me to get around certain vessels at the proper angle, so I like having that option,” she noted.
“We’re able to do a lot of different things with ENSEAL®. It used to be very difficult to take a fatty mesentery with an energy device, and I don’t think that’s the case any more—we don’t have to convert to do the mesentery extracorporeally,” said Dr. Ramamoorthy. “In some ways, I think ENSEAL®
has really facilitated what we can do laparoscopically or robotically, allowing us to complete more of the operation with a minimally invasive approach.”
The ENSEAL® G2 Platform
In September 2011, Ethicon Endo-Surgery invited an experienced group of surgeons to try out the latest generation
of ENSEAL® Technology: The ENSEAL® G2 Platform (Figure 5) and the ENSEAL® G2 Super Jaw Tissue Sealer. Both of these devices, along with HARMONIC® Devices, are compatible with the Ethicon Endo-Surgery Generator G11. The surgeons who attended this workshop included both dedicated ENSEAL®
users and those who use competing devices.Dr. Stein felt that the ENSEAL® G2 Platform is a major
improvement over other devices because of its intuitive nature. “Before, I felt like I was about to cut when I wanted to be burning, and vice versa,” she said. “For most of us, we cut when we’re pulling something. But [before], that was the burning device and to me, that was very counterintuitive and backward.”
As a user of a competing device, Dr. Stein found the new ENSEAL® G2 Device did not challenge her muscle memory or make her ponder her every move. “Every time you do a case, you can’t be thinking, for example, ‘I have to burn, then I have to cut—clamp, burn, cut, open.’ [Instead,] you want it to be fluid and easy,” she said.
Dr. Arrese was particularly pleased with the ENSEAL® G2 Super Jaw, which is indicated for use in open procedures. “This is where I really see the big difference between ENSEAL® and LigaSure™. Also, the blade will never come out of the curve of the teeth,” he said.
Most modifications to the new ENSEAL® G2 Platform were meant to provide a superior sealing experience8 through enhanced ergonomics, tactile feedback, and safety, while retaining the positive characteristics of the older ENSEAL®
Portfolio. Dr. Kondrup was among the first to test the ENSEAL® G2 Platform when it was first approved for human
Figure 5. The ENSEAL® G2 Advanced Bipolar Tissue Sealer.

REPORT
7
cases. “The first thing I noticed about it was the handle,” he said. “It was extremely comfortable compared with the orig-inal ENSEAL® Device, similar to the HARMONIC®; very user friendly and very easy to advance the blade. The reduction in finger fatigue is just amazing.”
The second thing that Dr. Kondrup noticed were the changes to the instrument’s jaw. “The positive electrode is now welded to the lower jaw, so there is 1 piece, as opposed to 2 separate pieces. I believe it’s sturdier,” he said.
Some features, however, are hard to improve on. “The hemostasis is just as reliable as the original. [But] it’s hard to imagine an improvement in hemostasis when you’ve had good hemostasis to start with,” noted Dr. Kondrup.
“They made a few changes from the prior instruments. In one prior edition, you could cut through the tissue without sealing it first—the previous edition did not have a mechanical stop to prevent you from cutting the tis-sue without sealing it first,” said Dr. Kalady. “I work with fellows every day, and if they’re not familiar with how to handle the instrument they could actually cut through a vessel or through tissue before it’s sealed. There were safety controls on the handle of that instrument, but I found it cumbersome to go between the safety mode and the [working mode].”
Dr. Kalady also found the noise produced by the previous ENSEAL® Generator to be bothersome. “When the machine was activated, it made a very annoying tone,” he said. “They changed that to make a much more pleasing background noise [with the Ethicon Endo-Surgery Generator G11]. Now there is one tone when it is activated to work, another tone when you’re at the point where you start to cut, and a final, single tone that goes off to indicate that you’re safely through everything.”
Benyamine Mizrahi, MD, a colorectal surgeon at Colorectal Surgery Associates, PC, in Kansas City, Missouri, has used LigaSure™ devices since his surgical residency. This con-tinued through his 2 fellowships and his past 2 years as a practicing surgeon. But he is open to the possibility of using another instrument. “I think there is room to make things bet-ter in an energy device. I’m not committed to one product over another, I just want the best tool to make surgery go smoother and faster,” he said. “If ENSEAL® has what it takes, then I’d love to use it.”
All vessel-sealing devices have their pros and cons, explained Dr. Mizrahi. “One thing ENSEAL® does better is the compression it provides, because of the I-BLADE™ Technology.a You have a better, tighter seal and closure from the beginning of the blade to the end,” he said.
ENSEAL® G2 Devices (G2 Straight, G2 Curved, and G2 Super Jaw) offer more than twice the compression at
the distal tip of the jaws than the LigaSure™,8,b and this characteristic can pay off in many ways. “The better the seal, the less bleeding you get and the less often you need to coagulate, so that makes the procedure go faster,” said Dr. Mizrahi. “That means less time in the OR, less time the patient is under anesthesia, and the more cases you can do—everyone is happy.”
In addition to its superior compression, Dr. Mizrahi believes that the ability to see exactly where he is burning and cutting gives ENSEAL® an edge over LigaSure™. “With the Ligasure™, you close, you burn, it lets you know when it’s done, and then you cut. You don’t see the blade. With ENSEAL®, you’re sealing and you can see right where you’re sealing, and you can bring the blade up to that point. Essentially, you control what you’re cutting,” he said.
Although LigaSure™ is the device with which he is the most familiar and comfortable, Dr. Mizrahi sees room for ENSEAL® in his OR. “ENSEAL® definitely has promise. If I’m able to do the case more efficiently and with less fatigue and can get the same job done, then I’m definitely going to be using it,” he said.
Dr. Kondrup estimated that surgeons who are unfamiliar with ENSEAL® would be able to quickly adjust to it. “I find the learning curve to be very manageable and I think that most surgeons will be able to adapt from other energy devices,” he said. “There are no adjustments to be made, no numbers to turn on and off. You simply plug it into the generator, the generator tests the instrument, and you’re ready to go.”
He does recommend that surgeons exercise caution with any new instrument before trying it out on a case. “I think it’s important to use the instrument in a benchtop demonstration first—don’t take it right into the OR,” said Dr. Kondrup. “The only real concern I have is that surgeons get to know how the instrument operates.”
Dr. Stein always takes a cautious approach when she uses a new instrument on a case for the first time. “I’ll start off on something that is not imperative, like a little piece of omentum, to make sure I’m comfortable with what I’m doing,” she said. “With the G2 [Device], once I’d used it a handful of times, I saw that what I needed to do was very intuitive and I could just go on with my case.”
Conclusion
ENSEAL® Devices deliver strong seals while providing a superior sealing experience. Their multifunctionality and cus-tomization provide surgeons with a high level of flexibility with minimal thermal spread. The availability of the ENSEAL®
G2 Portfolio gives surgeons another option for performing a variety of surgical procedures.
a Average jaw compression: 110 psi ENSEAL® G2 Super Jaw versus 91 psi LigaSure Impact™ and 80 psi LigaSure Atlas™, P<0.0000. Test conducted on an inanimate model. Data on file. Ethicon Endo-Surgery, Inc.b In side-by-side benchtop testing, average jaw compression was 201 psi (SD=42 psi) for TRIO versus 91 psi (SD=13 psi) for Impact™. Data on file. Ethicon Endo-Surgery, Inc.

8
REPORT
Financial Disclosures: Drs. Arrese and Kalady reported that they have received honoraria from Ethicon Endo-Surgery. Dr. Kondrup reported that he has served as a consultant and member of the speakers’ bureaus for Ethicon Endo-Surgery, Ethicon Women’s Health & Urology, and PALL Medical. Dr. Mizrahi reported that he has received honoraria from Ethicon Endo-Surgery. Dr. Ramamoorthy reported that she has served as a consultant for and has received honoraria from Ethicon Endo-Surgery. She also has served as a consultant for Covidien. Dr. Stein reported that she has received honoraria from Covidien and Ethicon Endo-Surgery.
Disclaimer: This monograph is designed to be a summary of information. Although it is detailed, it is not an exhaustive clinical review. McMahon Publishing, Ethicon Endo-Surgery, and the authors neither affirm nor deny the accuracy of the information contained herein. Ethicon Endo-Surgery has participated in the editorial process. No liability will be assumed for the use of this monograph, and the absence of typographical errors is not guaranteed. Readers are strongly urged to consult any relevant primary literature.
Copyright © 2012, McMahon Publishing, 545 West 45th Street, New York, NY 10036. Printed in the USA. All rights reserved, including the right of reproduction, in whole or in part, in any form.
“The new ENSEAL® G2 Platform is an amazing improve-ment in the design of the handle, and the addition of the Ethicon Endo-Surgery Generator G11, which provides feedback as you use the instrument, is extremely helpful, especially for new surgeons,” said Dr. Kondrup. “I don’t think anything else on the market comes close to allowing you to see where the blade is, cut and cauterize, and dissect. I’m extremely happy with that instrument, and I’m also happy to be able to choose either the ENSEAL® or HARMONIC® Tech-nology, as indicated for a particular case.”
For complete product information, please refer to the instructions for use in the package insert.
References1. Reza MM, Blasco JA, Andradas E, Cantero R, Mayol J.
Systematic review of laparoscopic versus open surgery for colorectal cancer. Br J Surg. 2006;93(8):921-928.
2. De U. Laparoscopic versus open appendicectomy: An Indian perspective. J Minim Access Surg. 2005;1(1):15-20.
3. Jin C, Hu Y, Chen XC. Laparoscopic versus open myomec-tomy—a meta-analysis of randomized controlled trials. Eur J Obstet Gynecol Reprod Biol. 2009;145(1):14-21.
4. Raymond DM, Romeo JH, Kumke KV. A pilot study of occupational injury and illness experienced by classical musicians. Workplace Health Saf. 2012;60(1):19-24.
5. Park A, Lee G, Seagull FJ, Meenaghan N, Dexter D. Patients benefit while surgeons suffer: an impending epidemic. J Am Coll Surg. 2010;210(3):306-313.
6. Massarweh NN, Cosgriff N, Slakey DP. Electrosurgery: history, principles, and current and future uses. J Am Coll Surg. 2006; 202(3):520-530.
7. Person B, Vivas DA, Ruiz D, Talcott M, Coad JE, Wexner SD. Comparison of four energy-based vascular sealing and cut-ting instruments: a porcine model. Surg Endosc. 2008; 22(2):534-538.
8. Ethicon Endo-Surgery. ENSEAL® G2 Tissue Sealer (Curved/Straight) Product Fact Sheet. http://www.ees.com/node/43144. Accessed July 30, 2012.
9. ENSEAL® 510(k) submission. www.accessdata.fda.gov/cdrh_docs/pdf4/KO43008.pdf. Accessed July 30, 2012.
10. Ethicon Endo-Surgery. ENSEAL® G2 Curved and Straight Tissue Sealers–Description and Specs. http://www.ees.com/Clinician/Product/energy/enseal-g2-tissue-sealers#!Description%20&%20Specs. Accessed July 29, 2012.
11. Newcomb WL, Hope WW, Schmelzer TM, et al. Comparison of blood vessel sealing among new electrosurgical and ultrasonic devices. Surg Endosc. 2009;23(1):90-96.
12. Ethicon Endo-Surgery. Energy Devices Portfolio. http://www.ees.com/sites/default/files/generalsurgery_EES_Energy_Devices_Portfolio.pdf. Accessed July 30, 2012.
13. Data on file. Ethicon Endo-Surgery, Inc.
14. Jackson TD, Wannares JJ, Lancaster RT, Rattner DW, Hutter MM. Does speed matter? The impact of operative time on outcome in laparoscopic surgery. Surg Endosc. 2011;25(7):2288-2295.
SR
1123
/SR
1228
D
SL#
12-
065
3
OS
S#
EC
P61
5