Terapia antitrombotica dopo stenting nel in terapia ...tigulliocardio.com/slide/Rubboli.pdf ·...
28
Terapia antitrombotica dopo stenting nel paziente in terapia anticoagulante orale Andrea Rubboli Unità Operativa di Cardiologia & Laboratorio di Emodinamica Ospedale Maggiore, Bologna Key points: 1. triplice terapia è il trattamento antitrombotico ottimale 2. triplice terapia è associata ad aumentato rischio emorragico 3. impianto di stent medicati da evitare/limitare
Transcript of Terapia antitrombotica dopo stenting nel in terapia ...tigulliocardio.com/slide/Rubboli.pdf ·...

Terapia antitrombotica dopo stenting nel paziente in terapia anticoagulante orale
Andrea Rubboli
Unità Operativa di Cardiologia & Laboratorio di EmodinamicaOspedale Maggiore, Bologna
Key points:1. triplice terapia è il trattamento antitrombotico ottimale2. triplice terapia è associata ad aumentato rischio emorragico3. impianto di stent medicati da evitare/limitare

p<0.05 p=NS p<0.05 p<0.05 p=NS
(%)
Rubboli A et al. Cardiology 2005;104:101-6
Meta-analysis of ISAR, STARS, FANTASTIC e MATTIS (total pts. 2436)
TAO(+ ASA) e stent coronarico

CAPTA study
200 pts. with mechanical aortic valve
no adjunctive risk factors
ASA 100 mg + Clopidogrel 75 mg vs. OAC (INR 2.5-3.5)
Schlitt A et al. Thromb Res 2003; 109:131-5
Trombosi di protesi: 9.1 vs 0%Trombosi di protesi: 9.1 vs 0%
ACTIVE W study
6706 pts. with atrial fibrillation
≥ 1 risk factors
ASA 75-100 mg + Clopidogrel 75 mg vs. OAC (INR 2.0-3.0)
The ACTIVE Investigators. Lancet 2006; 367:1903-12
Valve thrombosis: 9.1 vs 0%
ASA + clopidogrel quando indicata TAO

+

Armstrong PW & Welsh RC, Edmonton, CDN
Bassand JP, Besançon, FRA
Bates ER, Ann Arbor, MI, USA
Belardi J, Buenos Aires, ARG
Bourassa MG & Farah B, Montrel, CDN
Chevalier B, Saint Denis, FRA
Danchin N, Paris, FRA
Di Mario C, London, GB
Eeckhout E, Lausanne, CH
Grip L, Göteborg, SWE
Grube E, Siegburg, GER
Kleiman NS, Houston, TX, USA
Meier B, Berne, CH
Morice M-C, Paris, FRA
Neumann F-J, Bad Krozingen, GER
Popma JJ, Boston, MA, USA
Rutsch W, Berlin, GER
Sanborn TA, New York, NY, USA
Schömig A, Munich, GER
Serruys PW, Rotterdam, NL
Sigwart U & Camenzind E, Geneve, CH
Sousa EMR, Sao Paulo, BRA
Urban P, Geneve, CH
Verheugt FWA, Nijmegen, NL
All casesSelected
casesNo cases
OAC + ASA 1 (4%) 5 (21%) 18 (75%)
OAC + thienopyridine 2 (8%) 1 (4%) 21 (88%)
OAC + dual antiplatelet 15 (62%) 5 (21%) 4 (17%)
83%
Rubboli A et al. Ital Heart J 2004;5:851-6
Antithrombotic treatment after coronary artery stenting in patients on chronic oral anticoagulation: an international survey of current clinical practice.

ACC/AHA/SCAI 2005 guideline update for
percutaneous coronary intervention(J Am Coll Cardiol 2006;47:216‐235)
OAC+ASA+clopidogrel
ACC/AHA/ESC 2006 guidelines for the management
of patients with atrial fibrillation(J Am Coll Cardiol 2006;48:854‐906)
OAC+clopidogrel
Guidelines on the management of valvular
heart disease(Eur Heart J 2007;28:230‐268)
OAC+ASA+clopidogrel
Anticoagulants in heart disease: current status
and perspectives(Eur Heart J 2007;28:880‐913)
OAC+ASA+clopidogrel
Management of acute myocardial infarction in patients
presenting with persistent ST‐segment elevation(Eur Heart J 2008;29:2909‐45)
OAC+ASA+clopidogrel
Raccomandazioni attuali (livello evidenza C!!)

trombosi protesi valvolare
trombembolia arteriosa
tromboembolia venosa
trombosi di stent
emorragia
Rapporto rischio/beneficio?

1. Orford JL et al. Am J Cardiol (2004)
2. Mattichak SL et al. J Interven Cardiol (2005)
3. Khurram Z et al. J Invasive Cardiol (2006)
4. Porter A et al. Catheter Cardiovasc Interv (2006)
5. Lip GYH & Karpha M. Chest (2006)
6. Karjalainen PP et al. Eur Heart J (2007)
7. DeEugenio D et al. Pharmacotherapy (2007)
8. Rubboli A et al. Coron Artery Dis (2007)
9. Nguyen MC et al. Eur Heart J (2007)
10. Wang TY et al. Am Heart J (2008)
11. Ruiz‐Nodar JM et al. J Am Coll Cardiol (2008)
12. Rogacka R et al. J Am Coll Cardiol Intv (2008)
ANDREA RUBBOLI1, JONATHAN L. HALPERIN2, K.E. JUHANI AIRAKSINEN3, MICHAEL BUERKE4, ERIC EECKHOUT5, SAUL B. FREEDMAN6, ANTHONY H. GERSHLICK7, AXEL SCHLITT4, HUNG-FAT TSE8, FREEK W.A. VERHEUGT9 & GREGORY Y.H. LIP10
Ann Med 2008;40:428-36

Rubboli A et al. Ann Med 2008;40:428-36
Triplice terapia con TAO, ASA & tienopiridine vs. altri regimi:
meno stroke &
più emorragie (maggiori)(quanto più la terapia si prolunga)
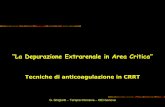
2.26% DES vs 1.19% BMS p = 0.03
Ruiz-Nodar JM et al. Eur Heart J 2009;30:932-9

Gilard M et al. Am J Cardiol 2009;104:338-42
p = 0.2 p = 0.04 p = 0.3
% major bleeding

% patientsw
ithbleeding
p<0.001 p=0.64 p<0.0001
Early and late increased bleeding rates after angioplasty and stenting due tocombined antiplatelet and anticoagulant therapyChristophe Hälg, MD; Hans Peter Brunner‐La Rocca, MD; Christoph Kaiser, MD; Raban Jeger, MD; Stefan Osswald, MD; MatthiasPfisterer, MD; Andreas Hoffmann*, MD; for the BASKET investigators
da Eurointervention 2009;5:425-31

…. what proportion of these major hemorrhagicevents can actually be attributed to triple therapy?In other words, might triple therapy be safer than itappears?
Rubboli A & Halperin JL. Thromb Haemost 2008;100:752-3

Variabile RR 95% IC Autori
Uso di inibitori GP IIb/IIIa 5.1 1.3‐20.6 Lahtela H et al.Thromb Haemost 2009; 102:1227‐33
Approccio radiale vs. femorale 0.27 0.16‐0.45 Jolly SS et al. Am Heart J 2009; 157:132‐40
Anticoagulazione “bridge” 3.9 1.0‐15.3 Karjalainen PP et al. Eur Heart J 2008; 29:1001‐10
emorragie precoci

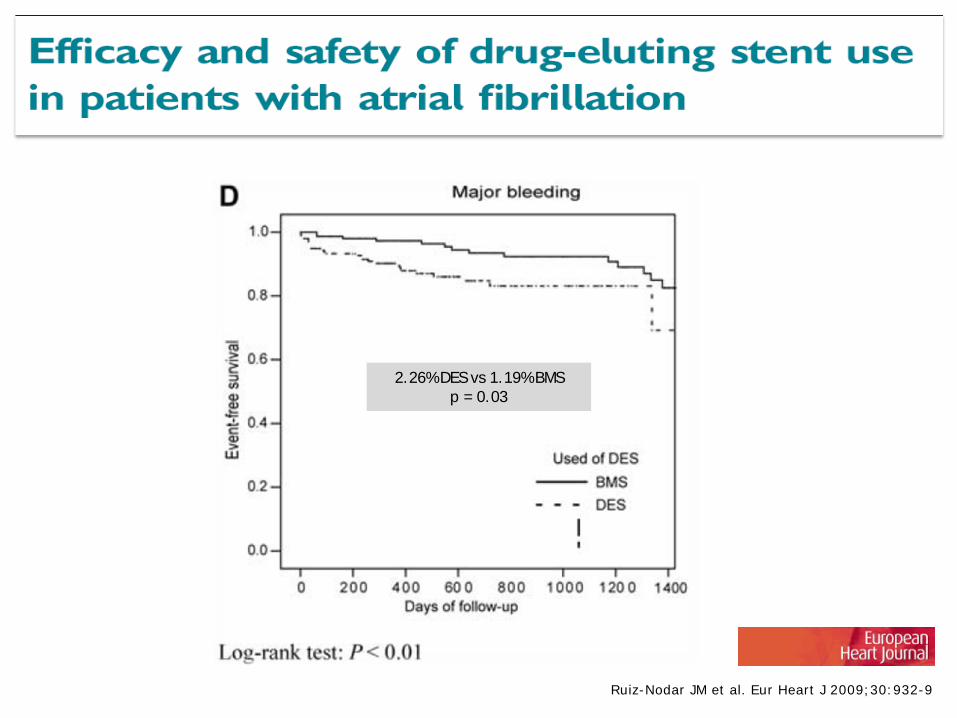
ANDREA RUBBOLI, M.D.,1 MAURO COLLETTA, M.D.,1 JOSE’ VALENCIA, M.D.,2 ALESSANDRO CAPECCHI, M.D.,3 NICOLETTA FRANCO, M.D.,4
LUISA ZANOLLA, M.D.,5 LUIGI LA VECCHIA, M.D.,6 GIANCARLO PIOVACCARI, M.D.,4 and GIUSEPPE DI PASQUALE, M.D.,1 for the WARfarin and coronary STENTing (WAR-STENT) Study Group
Rubboli A et al. J Interv Cardiol 2009;22:390-7
Ospedale degli Infermi, Rimini, ITA
(N Franco, G Piovaccari)
Coordinating Center
Ospedale Maggiore, Bologna, ITA
(A Rubboli, M Colletta, G Di Pasquale)
Ospedale Civile, Bentivoglio, ITA
(A Capecchi, LG Pancaldi)
Ospedale S. Bortolo, Vicenza, ITA
(L La Vecchia, A Fontanelli)
Hospital Universitario, Alicante, ESP
(J Valencia)
(%)
Rubboli A et al. J Interv Cardiol 2009;22:390-7

Author Design N° Comparison
Orford JL et al. (2004) Retrospective, 1‐center 66 none
Mattichak SL et al. (2005) Retrospective, 1‐center 82 pts. receiving ASA+clop
Khurram Z et al. (2006) Retrospective, 1‐center 214 pts. receiving ASA+clop
Porter A et al. (2006) Retrospective, 1‐center 180 none
Lip GYH & Karpha M (2006) Retrospective, 1‐center 35 within population
Karjalainen PP et al. (2007) Retrospective, multi‐center 239 pts. receiving ASA+clop
DeEugenio D et al. (2007) Retrospective, 1‐center 97 pts. receiving ASA+clop
Rubboli A et al. (2007) Retrospective, 1‐center 49 within population
Nguyen MC et al. (2007) Prospective, multi‐center (post‐hoc) 800 within population
Wang TY et al. (2008) Prospective, multi‐center (post‐hoc) 1247 within population
Ruiz‐Nodar JM et al. (2008) Retrospective, 2‐center 426 within population
Rogacka R et al. (2008) Retrospective, 2‐center 127 none
Rubboli A et al. Ann Med 2008;40:428-36

2.26% DES vs 1.19% BMS p = 0.03
Ruiz-Nodar JM et al. Eur Heart J 2009;30:932-9
only ~ 50% pts. discharged on TT
TT duration?
TT ongoing @ bleeding?

% patientsw
ithbleeding
p<0.001 p=0.64 p<0.0001
from Hälg C et al. Eurointervention 2009;5:425-31

Rubboli A et al. Eurointervention 2010; 5:105

Rossini R et al. Am J Cardiol 2008;102:1618-23

FINLAND
1. University Hospital, Turku(KE Juhani Airaksinen, MD, FESC)
2. University Hospital, Helsinki3. University Hospital, Oulu4. Central Hospital, Satakunta5. University Hospital, Kuopio6. Central Hospital, Lappi7. Central Hospital, Keski‐Suomen8. University Hospital, Tampere9. Central Hospital, Keski‐Pohjanmaa
ITALY
1. Maggiore Hospital, Bologna(Andrea Rubboli, MD, FESC)
2. S. Bortolo Hospital, Vicenza
GERMANY
1. Martin Luther University, Halle‐Wittenberg(Axel Schlitt, MD)
2. Herzzentrum, Leipzig3. Universitätklinikum, Münster4. Heart Center, Kerckhoff
GREAT BRITAIN
1. City Hospital, Birmingham
SPAIN
1. University Hospital, Alicante
A. F. C. A. S.
Management of patients withAtrial Fibrillation undergoing
Coronary Artery Stenting: a multicenter, prospective registry

Thromb & Haemost 2010;103:13-28

Triplice terapia (TAO + ASA + clopidogrel):
1. indicata nei pz. a rischio TE medio‐elevato dopo impianto di stent
2. (verosimilmente) associata ad aumentato rischio emorragico
3. da condurre con INR ai limiti inferiori del range terapeutico
4. da protrarre per il più breve tempo possibile , e quindi no stent medicati

CYPHER® TAXUS® ENDEAVOR XIENCE V
Photos on file at Abbott Vascular.

F-up Clopidogrel= 2 months
Pts Clopidogrel> 2 months
Pts
30 days 97.71% (97.71 - 99.14) 171 99.69% (99.69 - 99.96) 324
6 months 97.71% (97.71 - 99.14) 147 97.47% (97.47 - 98.73) 251
12 months 96.94% (96.94 - 98.73) 95 97.02% (97.02 - 98.45) 146
Stent ThrombosisAcute 0.2%
Sub‐acute 0%Late 0% MATRIX Registry (12-month interim analysis)
Piscione F et al. GISE 2008/TCT 2008/JIM 2009

Karjalainen PP et al. Eur Heart J 2007;28:726-32

Sørensen R et al. Lancet 2009;375:1967-74