Enclosure 2, Biological Monitoring of the Tennessee River ...

TENNESSEE RIVER DERMATOLOGY 2471 Helton Drive Florence, AL 35630 256.765.2000 www.tennriverderm.com Thank you for choosing Tennessee River Dermatology. Enclosed please find the required forms for our new patients and our patients who have not been to our office within the last three (3) years. Please complete all forms and bring them with you on the day of your visit. Please also remember to bring your insurance card(s) and a picture ID for the patient or guarantor. Please refrain from wearing scented products on the day of your visit. Dr. Hanson is extremely allergic to these. We ask that anyone who enters an exam room is not wearing perfume, cologne, body sprays or scented lotions. Thank you for your cooperation in this matter.
You will receive an automated reminder call a few days before your appointment requesting you to confirm or cancel your scheduled visit. If you are unable to keep your appointment kindly cancel using this reminder system or call our office at (256)765-2000 at least 24 hours prior to your appointment and we’ll be happy to reschedule at a time that is more convenient for you. Once again we thank you for choosing Tennessee River Dermatology and we look forward to providing you with a pleasant office visit. Sincerely, The Physicians and Staff Tennessee River Dermatology, P.C.

Tennessee River Dermatology New Patient Medical Information Form
Please place a check in front of any of the following conditions or symptoms you have:
CONSTITUTIONAL: Fever Weight Loss Change in Sexual ActivityChills Weight Gain FatigueSweats Change in Appetite Dizziness
NEUROLOGICAL: Headache Trauma to Head NumbnessSeizures Loss of Sensation ParalysisStroke Paresthesia
EYES:Acuity change Infection Dry ___Styes BurningGrittiness Glaucoma Decrease night vision SorenessIrritation Blurred vision Cataracts Problem with Tears
INTEGUMENTARY: Rash Blue Pigmentation Acne changes FoliculitisGrowths Photosensitive Sensitive Hands/Feet ErythemaDryness Hypertrichosis Dry/Peeling Lips IrritationScaling Premature Graying Peeling soles/feet VitiligoPigment Changes Blistering Pigmented lesion ScarsAthletes Foot Scleroderma Hyperpigmentation BurningThinning Hair Lymphoma BruisingPhototherapy Yes Subcutaneous nodule Itching
GENITOURINARY: Frequency Pain DysuriaUrgency Discharge Recurrent Yeast InfectionBurning w/urination Distress STD ________________________________Lesions/Sores Menopause Menses: Age ______ ___Regular ___Irregular Blood in urine Recent Pregnancy Birth Control:_________________________
PSYCHIATRIC: Anxiety Self-conscious Suicidal ThoughtsApprehension Stressful Events Depression Distress
MUSCULOSKELETEL: Aches Pain WeaknessCramps Spasm Arthritis Arthralgia
CARDIOVASCULAR: Coronary Artery Disease Congestive Heart FailurePalpitations Varicose Veins Chest Pain Deep Vein ThrombosisClaudication Atrial Fibrillation Heart MurmurPeripheral Edema Dyspnea w/Exertion PacemakerOrthopnea Hypertension Thrombophlebitis
ENT: Epistaxis (Nose Bleeds) Sore Throat Tooth PainNasal Obstruction Strep Throat Sinus Pain Mouth UlcersSinus Infection Vertigo Itchy Throat Sore MouthDry Nose Itching Ears Tooth Abscess
GASTRO- Nausea Constipation Melena ("Black" stools) Hepatitis AINTESTINAL: Vomiting Abdominal Pain Sensitive stomach Hepatitis B
Diarrhea Flatulence Hepatitis C
Continued on Back

Tennessee River Dermatology New Patient Medical Information Form
RESPIRATORY: Cough Wheezing Hx of TB COPDHemoptysis Difficulty Breathing SOB
ENDOCRINE: Diabetes Heat Intolerance HirsutismCold Intolerance Alopecia
ALLERGIC/ Eczema Hives LupusIMMUNOLOGIC: Hay Fever Thyroid Disease Rheumatoid Arthritis
Asthma HIV Chemotherapy
HEM/LYMPH Anemia Bleeding Enlarged lymph nodes/glands:______________Leukemia Lymphoma Cancer Type: __________________________
Derm History:Skin Type: Have you or a blood relative had the following:
Alcohol? Always burns, never tan Exposure To:Smoke? Always burns, sometimes tans Melanoma ArsenicBleeds Easily? Sometimes burns, always tans Skin Cancer RadiationNovacaine? Never burns, always tans Pigmented Lesions/Moles PUVA
Never burns, tans mod. Pigmented Unusual Moles Albinism?Never burns, always tans black Pre-Skin Cancer Vitiligo?
MEDICINE ALLERGIES:1. 3. 5. 7.
2. 4. 6. 8.
PLEASE LIST YOUR CURRENT MEDICATIONS (INCLUDING OVER-THE-COUNTER):
Aspirin? 1. 3. 5. 7.Coumadin?Plavix? 2. 4. 6. 8.Vitamin E?
PLEASE LIST ALL CREAMS AND LOTIONS (INCLUDING OVER-THE-COUNTER) THAT YOU HAVE USED ON YOUR SKIN:CIRCLE THE ONES YOU ARE CURRENTLY USING:
1. 3. 5. 7.
2. 4. 6. 8.
TO PROVIDE YOU WITH THE BEST CARE, WE RECOMMEND A COMPLETE SKIN EXAM FOR MOST NEW PATIENTS.PLEASE INDICATE YOUR PREFERENCE BELOW:
I DO want to have a complete skin exam I DO NOT want to have a complete skin exam.
I attest that I have provided the above information to the best of my ability:
Patient Signature: Date:


Tennessee River Dermatology
In accordance with the American Recovery and Reinvestment Act of 2009, Healthcare Providers are required to obtain
the following additional patient information:
RACE: ETHNICITY: PREFERRED LANGUAGE: __ Black/African American __White __Latino __English
__American Indian __Asian __Non‐Latino __Spanish
__More than one race __Native Hawaiian __Other ethnicity __Other language
__Other race
CURRENT TOBACCO USE: SMOKING STATUS: __Chewing __Current, every day smoker
__Cigarettes __Current, occasional smoker
__Cigars __Current status unknown
__Pipe __Former smoker
__Smokeless __Former status unknown
__Snuff __Never smoked
YES NO
1. If you are 50 years old or older, have you received a flu shot this season? ___ ___
2. If you are 65 years or older, have you EVER received a pneumonia vaccination? ___ ___
3. If you are between the ages of 50 and 75, have you EVER been screened for colorectal cancer? ___ ___
4. If you are a female between the age of 40 and 69, have you EVER had a mammogram? ___ ___
5. What is your preferred method of receiving appointment reminders? __Phone __Mail __Email
6. Email Address: _________________________________________________________________________________
Signature of Patient/Guardian Date

Tennessee River Dermatology
Page 1 of 2
NOTICE OF PRIVACY PRACTICES
This notice describes how medical information about you may be used and disclosed and how you can gain access to this information. Please review it carefully.
USES AND DISCLOSURES
Treatment: Your health information may be used by staff members or disclosed to other health care Professionals for the purpose of evaluating your health, diagnosing medical conditions, and providing Treatment. For example, results of laboratory tests and procedures will be available in your medical record to all health professionals who may provide treatment or who may be consulted by staff members.
Payment: Your health information may be used to seek payment from your health plan, from other sources of coverage such as an automobile insurer, or from credit card companies that you may use to pay for services. For example, your health plan may request and receive information on dates of service, the services provided, and the medical condition being treated.
Health Care Operations: Your health information may be used as necessary to support the day-to-day activities and management of Tennessee River Dermatology. For example, information on the services you received may be used to support budgeting and financial reporting, and activities to evaluate and promote quality.
Law Enforcement: Your health information may be disclosed to law enforcement agencies, without your permission, to support government audits and inspections, to facilitate law-enforcement investigations, and to comply with government mandating reporting.
Public Health Reporting: Your health information may be discussed to public health agencies as required by law. For example, we are required to report certain communicable diseases to the state’s public health department.
Appointment reminders: Your health information will be used by our staff to send you appointment reminders.
Information about treatments: Your health information may be used to send you information on the treatment and management of your medical condition that you may find to be of interest. We may also send you information describing other health-related goods and service that we believe may interest you.
Other Uses and Disclosures Require Your Authorization: Disclosure of your health information or its use for any purpose other than those listed above requires your specific written authorization. If you change your mind after authorizing use of disclosure of your information you may submit a written revocation of the authorization. However, your decision to revoke the authorization will not affect or undo any use or disclosure of information that occurred before you notified us of your decision.
Tennessee River Dermatology
Page 2 of 2
NOTICE OF PRIVACY PRACTICES
INDIVIDUAL RIGHTS
You have certain rights under the federal privacy standards including:
The right to request restrictions on the use and disclosure of your protected health information
The right to receive confidential communication concerning your medical condition and treatment
The right to inspect and copy your protected health information
The right to receive an accounting of how and to whom your PHI has been disclosed
The right to receive a printed copy of this notice
TENNESSEE RIVER DERMATOLOGY’S DUTIES: We are required by law to maintain the privacy of your protected health information and to provide you with this notice of privacy practices. We also are required to abide by the privacy policies and practices that are outlined in this notice.
RIGHT TO REVISE PRIVACY PRACTICES As permitted by law, we reserve the right to amend or modify our privacy policies and practices. These changes in our policies and practices may be required by changes in federal and state laws and regulations. Whatever the reason for these revisions, we will provide you with a revised notice on your next office visit. The revised policies and practices will be applied to all protected health information that we maintain.
REQUEST TO INSPECT PROTECTED HEALTH INFORMATION As permitted by federal regulation, we require that request to inspect or copy protected health information be submitted in writing. You may obtain a form to request access to your records contacting Receptionist or Privacy Official.
COMPLAINTS If you would like to submit a comment or complaint about our privacy practices, you can do so by sending a letter outlining your concerns to: Privacy Official, Tennessee River Dermatology, 2471 Helton Drive, Florence, Alabama 35630
Effective Date: This notice is effective April 16, 2003
TENNESSEE RIVER DERMATOLOGY 2471 HELTON DRIVE FLORENCE, AL 35630
256.765.2000 1.866.MOH.SURG
www.tennriverderm.com
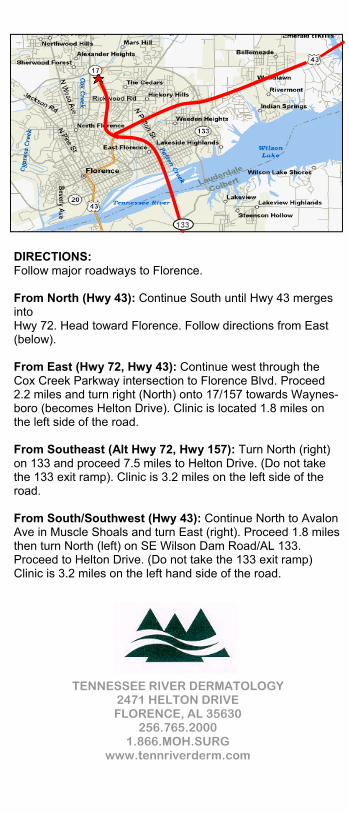
DIRECTIONS: Follow major roadways to Florence. From North (Hwy 43): Continue South until Hwy 43 merges into Hwy 72. Head toward Florence. Follow directions from East (below). From East (Hwy 72, Hwy 43): Continue west through the Cox Creek Parkway intersection to Florence Blvd. Proceed 2.2 miles and turn right (North) onto 17/157 towards Waynes-boro (becomes Helton Drive). Clinic is located 1.8 miles on the left side of the road. From Southeast (Alt Hwy 72, Hwy 157): Turn North (right) on 133 and proceed 7.5 miles to Helton Drive. (Do not take the 133 exit ramp). Clinic is 3.2 miles on the left side of the road. From South/Southwest (Hwy 43): Continue North to Avalon Ave in Muscle Shoals and turn East (right). Proceed 1.8 miles then turn North (left) on SE Wilson Dam Road/AL 133. Proceed to Helton Drive. (Do not take the 133 exit ramp) Clinic is 3.2 miles on the left hand side of the road.
133
TENNESSEE RIVER DERMATOLOGY 2471 HELTON DRIVE FLORENCE, AL 35630
256.765.2000 1.866.MOH.SURG
www.tennriverderm.com
DIRECTIONS: Follow major roadways to Florence. From North (Hwy 43): Continue South until Hwy 43 merges into Hwy 72. Head toward Florence. Follow directions from East (below). From East (Hwy 72, Hwy 43): Continue west through the Cox Creek Parkway intersection to Florence Blvd. Proceed 2.2 miles and turn right (North) onto 17/157 towards Waynes-boro (becomes Helton Drive). Clinic is located 1.8 miles on the left side of the road. From Southeast (Alt Hwy 72, Hwy 157): Turn North (right) on 133 and proceed 7.5 miles to Helton Drive. (Do not take the 133 exit ramp). Clinic is 3.2 miles on the left side of the road. From South/Southwest (Hwy 43): Continue North to Avalon Ave in Muscle Shoals and turn East (right). Proceed 1.8 miles then turn North (left) on SE Wilson Dam Road/AL 133. Proceed to Helton Drive. (Do not take the 133 exit ramp) Clinic is 3.2 miles on the left hand side of the road.
133
TENNESSEE RIVER DERMATOLOGY 2471 HELTON DRIVE FLORENCE, AL 35630
256.765.2000 1.866.MOH.SURG
www.tennriverderm.com
DIRECTIONS: Follow major roadways to Florence. From North (Hwy 43): Continue South until Hwy 43 merges into Hwy 72. Head toward Florence. Follow directions from East (below). From East (Hwy 72, Hwy 43): Continue west through the Cox Creek Parkway intersection to Florence Blvd. Proceed 2.2 miles and turn right (North) onto 17/157 towards Waynes-boro (becomes Helton Drive). Clinic is located 1.8 miles on the left side of the road. From Southeast (Alt Hwy 72, Hwy 157): Turn North (right) on 133 and proceed 7.5 miles to Helton Drive. (Do not take the 133 exit ramp). Clinic is 3.2 miles on the left side of the road. From South/Southwest (Hwy 43): Continue North to Avalon Ave in Muscle Shoals and turn East (right). Proceed 1.8 miles then turn North (left) on SE Wilson Dam Road/AL 133. Proceed to Helton Drive. (Do not take the 133 exit ramp) Clinic is 3.2 miles on the left hand side of the road.
133