Tendon Rehabilitation Pyramid
1
Click here to load reader
-
Upload
mohsen-eslampanah -
Category
Health & Medicine
-
view
238 -
download
4
Transcript of Tendon Rehabilitation Pyramid

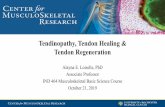
Tendon Rehabilitation Pyramid
Passive protected extension
Exercise Originator: Duran and Houser 1979
Rehabilitation stage: First post op visit
Duration: continues for the duration of protective splinting Frequency: >four times daily, 10 repetition
Function: provides a delivery of motion stress and maintains
finger mobility Description: Passive flexion and extension of the PIP and
DIP joints are performed independently.
the position of the wrist varies in a synergistic pattern. Wrist flx => low force-low Excursion
Wrist Ext=> high force-high excursion
It may be useful to remove the protective splint to allow wrist flexion/extension while the client is in the clinic or for home
Place and hold
Exercise Originator: Evans and Thompson 1993
Rehabilitation stage: used with 2 and 4 strand
solid repairs during first post op visit Duration: continues until just after progression to
next pyramid level
Frequency: 3‐5 times daily, but dependent on
individual situation Hold 3-7 sec
Function: allows for early detection of suboptimal
response to motion stress. Allows for early and careful tailoring of exercise and education
programs based on individual response
Description: Clients should complete a warm up of slow repetitious passive flexion and protected
extension with wrist in 20 degrees of extension.
The active hold position reduces viscoelastic drag on the tendon juncture. The metacarpophalangeal
(MP)/PIP/DIP digital joints are subsequently
actively held in a moderately flexed position.
Active composite fist
Rehabilitation stage: Prescribed for cli-
ents with an unresponsive active tendon lag
from second
week or at the 8 post‐op week Duration: continues until discharge
Frequency: 3‐5 times per day Function: excessive load application at the tendon
juncture is presented and high level of
tendon gliding resistance is overcome in those with binding adhesions Description: This level combines the
performance of active digital flexion to the distal palmar crease with wrist in slight
extension.
Maximum FDP excursion metacarpophalangeal (MP)/PIP/DIP digital
joints are subsequently actively held in a
moderately flexed position.
Hook and straight fist
Exercise Originator: Wehbe and
Hunter(1985) Rehabilitation stage: Prescribed for clients with an unresponsive active
tendon lag Frequency: 2:1 frequency ratio for the hook fist and straight fist. Function: provides greater stress in
the finger flexion positions, maintain-ing the wrist in neutral or slight flexion
minimizes the motion stress delivered Description: The hook fist position causes maximum differential excursion
between tendons up to 23–33 mm.
The straight fist position causes maxi-
mum FDS gliding between the sheath
and the bone and causes excursion that
varies from 17 to 30 mm. It may be useful to remove the protective splint
to allow wrist flexion/extension while
the client is in the clinic or for home exercises.
Isolated joint motion
Rehabilitation stage: Prescribed
for clients with an unresponsive
active tendon lag Function: maximizes motion stress
to adhesions. Description: External stabilization of the proximal and middle phalan-
ges allows for isolated DIP joint
motion and FDP function. External stabilization of the proximal phal-
anx allows for DIP and PIP joint
motion while blocking the MP joint and lumbrical function.
The prescription of isolated PIP
joint exercise is often overlooked in
the patient with a single laceration
to the FDP tendon.
Discontinuation of protective splinting. Significant increases in functional use.
A useful clinical technique is to grade the
discontinuance of protective splinting over a week to reduce sudden motion stress on
the hand.
Resistive composite fist
Function: maximizes motion stress to adhesions, finger exten-
sion exercise can also assist to reduce intrasynovial adhesions. Description: active composite digit flexion with an external mode of resistance such as with putty or a gripper ball.
Resisted hook and straight fist
Rehabilitation stage: Prescribed for clients with an unresponsive active tendon lag.
Description: This level uses the hook and straight fist described in level 4, but uses an external mode of resistance
to maximize force application.
Resisted isolated joint motion This level applies an external mode of resistance
to previously described positions.
creates a minimum of 12 exercise positions for the digit: four for the DIP joint (wrist/MP
flexed/extended) and eight for the PIP joint
(wrist/MP flexed/ extended, DIP blocked/free). If active lag remains unresponsive within two
weeks after the prescription of the exercise,
Groth suggests that the client be discharged as the maximum benefit from supervised therapy
has been reached.
Reference: Groth, G. (2004). Pyramid of progressive force exercises to
the injured flexor tendon. Journal of Hand Therapy, 17, 31-
42.
تهیه کنندگان:
محمد صادق فدایی، زینب اکبری، محسن اسالم پناه
![Design of a Hand Tendon Injury Rehabilitation System using ...based tendon-driven wearable robotic hand [22] Characterisation and evaluation of soft elastomeric acuators for hand assistive](https://static.fdocuments.us/doc/165x107/60b7d0894b1269644e0a4ff0/design-of-a-hand-tendon-injury-rehabilitation-system-using-based-tendon-driven.jpg)