Tendon injuries of hand by Dr Saumya Agarwal
101
Tendon Injuries of Hand Dr Saumya Agarwal Junior resident MS Ortho Dept of Orthopaedics J.N.Medical College and Dr. Prabhakar Kore Hospital and MRC, Belgaum
-
Upload
kles-jn-medical-college-and-dr-prabhakar-kore-hospital-and-medical-research-centre -
Category
Health & Medicine
-
view
1.625 -
download
0
Transcript of Tendon injuries of hand by Dr Saumya Agarwal

Tendon Injuries of Hand
Dr Saumya AgarwalJunior resident MS Ortho
Dept of Orthopaedics J.N.Medical College and Dr.
Prabhakar Kore Hospital and MRC, Belgaum

muscle to the bone
glistening structurebetween muscle
& bone whichtransmit force from
“”


Loose areolar
tissue
encasing
tendon in low
mechanical
stress area
Paratenon..?

Tendon Sheath..? a dense fibrous tissue tunnel enclosing tendon in high mechanical stress area

Tendon Morphology
• 70% collagen (Type I)
• Extracellular components• Elastin• Mucopolysaccharides (enhance water-
binding capability)
• Endotenon – around collagen bundles• Epitenon – covers surface of tendon• Paratenon – visceral/parietal adventitia
surrounding tendons in hand.

Tendon Nutrition
• Longitudinal vessels Enter in palm Enter at proximal synovial fold• Segmental branches from digital
arteries• Long and short vinculae• Vessels at osseous insertions• Synovial fluid diffusion• Imbibition (pumping mechanism)

Tendon Nutrition
• Avascular zones• FDS(over proximal
phalanx)• FDP (over middle
phalanx)• Nutrition vital for rapid
healing, minimization of adhesion and restoration of gliding


ANATOMY

Abbreviation Full Name Function
FPL Flexor pollicis longus Thumb flexion
PL Palmaris longus Flexion of wrist
FCU Flexor carpi ulnaris Flexion and adduction of hand
FDP Flexor digitorum profundus flexion of distal interphalangeal joints and helps wrist flexion
FDS Flexor digitorum superficialis Flexion of proximal interphalangeal joints and
flexion of proximal phalanges at metacarpophalangeal joints
FCR Flexor carpi radialis Flexion and abduction of hand at wrist

Abbreviation Full Name Function
APL Abductor pollicis longus Abduction of thumb
EPB Extensor pollicis brevis Extension of thumb proximal phalanx
ECRL
ECRB
Extensor carpi radialis longus/brevis Extends and abducts hand
EPL Extensor pollicis longus Extends thumb IP joint
ED
(4 tendons: II - V)
Extensor digitorum Extends digits II - V
EI Extensor indicis Extends digit II
EDM (EDC) Extensor digitorum minimi (quinti) Extends digit V
ECU Extensor carpi ulnaris Extends and abducts hand

Flexor Tendon Injury Zones
1: flexor digitorum profundus distal to insertion of flexor digitorum superficialis
2: insertion of flexor digitorum superficialis to proximal edge of A1 pulley (“No Man’s Land”)
3: proximal edge of the A1 pulley to distal edge of carpal tunnel
4: within the carpal tunnel
5: proximal to the carpal tunnel

Extensor Tendon Injury Zones
O Extensor tendons are divided into 8 zones
O Zones 1,3 and 5 lie over the DIP, PIP and MCP joints

PULLEYS

• ONLY FPL• CONTAINS 2
ANNULAR PULLIES AND ONE OBLIQUE PULLIES
THUMB SHEATH


Camper’s Chiasma


ETIOLOGY Common mechanisms of injury include
Osharp object direct laceration (broken glass, kitchen knives or table saws)
Ocrush injuryOavulsionsOburnsOanimal or human bitesOsuicide attemptsOmotor vehicle accidents

Flexor tendon healing
• 2 forms:– Intrinsic healing: occurs without direct blood
flow to the tendon – Extrinsic healing: occurs by proliferation of
fibroblasts from the peripheral epitendon; adhesions occur because of extrinsic healing of the tendon and limit tendon gliding within fibrous synovial sheaths

Phases of Intrinsic healing
1.Inflammatory (0-5 days) : strength of the repair is reliant on the strength of the suture itself
2.Fibroblastic (5-28 days) : or so-called collagen-producing phase
3.Remodelling (>28 days)

FLEXOR TENDON INJURIES

• Region b/w middle aspects of middle phalanx to finger tips
• Contains only one tendon-fdp• Tendon laceration occurs close to its insertion• Tendon to bone repair is required than tendon
repair
ZONE 1: ZONE OF FDP AVULSION INJURIES

Leddy classification of zone I flexor tendon injuries!!
Type I: tendon retracted into palm (fullness in palm)
Type II: tendon trapped in the sheath at PIP (unable to flex PIP)
Type III: tendon trapped in A4 pully

Type I injury!!

Type II injury!!

• From metacarpal head to middle phalanx• Called so because initial attempts for tendon
repair here produced poor results• FDS and FDP within one sheath• Adhesion formation risk is amplified at
campers chiasma
ZONE II-NO MANS LAND

• B/w transverse carpal ligament and proximal margin of tendon sheath formation
• Lumbricals origin here prevents profundus tendons from over acting
• Delayed tendon repairs are succesfull even after several weeks of injury
ZONE III-DISTAL PALMAR CREASE

• Lies deep to deep transverse ligament
• Tendon injuries are rare
ZONE IV-TRANSVERSE CARPAL LIGAMENT

• LIES PROXIMAL TO TRANSVERSE CARPAL LIGAMENT
ZONE V-PROXIMAL

SIGNS & SYMPTOMS• Unable to bend one or more finger joints
• Pain when bending finger/s
• Open injury to hand (e.g., cut on palm side of hand, particularly in area where skin folds as fingers bend)
• Mild swelling over joint closest to fingertip
• Tenderness along effected finger/s on palm side of hand

Complain of numbness preceeded by execissive bleed
Consider neurovascular insult!!

INSPECTION
• There is a normal arcade to hand with index finger showing least and little finger showing max flexion
• If affected finger shows more extension than other digits, chance of tendon injuries are high
EXAMINATION



• Stabilise the MCP joint
• Ask the pt to flex IP joint
FPL

DETECTION• History and physical
• Examination of wound
• Use of bedside ultrasonography in ER (more sensitive and specific than physical examination)
• Wound exploration techniques or MRI.
• 3-view x-ray must be done (except most benign) to rule out foreign bodies or bony injury.
• Radiographs to evaluate for possible fractures or dislocations (blunt trauma cases)

DICTUM
• Flexor tendon repair is not a surgical emergency. It is proved that equal or better results can be achieved by delayed primary repair.
• Better to repair both FDP & FDS tendons rather than FDP alone

Goals of reconstruction:
•Coaptation of tendons
• anatomical repair
• multiple strand repair to permit active range of motion rehabilitation
•Pully reconstruction to minimize bow-stringing
• atraumatic surgical technique to minimize adhesions
• strict adherence to rehabilitation protocol.

What can we provide?
• Minimal dissection and handling • Tendon apposition without gapping• Early protected mobilization

Timing of flexor tendon repair:
Primary: repair within 24 hours (contraindicated in case of high grade condtamination i.e. human
bites, infection)
Delayed Primary: 1-10 days when the wound can be still pulled open without incision
Early Secondary: 2-4 weeks.
Late Secondary : after 4 weeks

No repair if less than <25% laceration,
only epitenon repair in 25-50% lacerations,
.core suture plus epitenon repair when
>50% laceration
Dorsal blocking splint for 6-8 weeks as conservative measure

Bunnell stitch Crisscross stitch
Mason-Allen stitchRobertson and Al-Qattan Interlock stitch
Core Suture Techniques

Kessler stitch Modified Kessler
Tajima modificationOf kessler stitch withdouble loop at repair site

Sheath repair
• Advantages:– barrier to the formation of extrinsic adhesions– quicker return of synovial nutrition– better tendon-sheath biomechanics

Sheath repair
• Disadvantages:– technically difficult– may narrow and restrict tendon gliding

Suture Materials
• Core Non-absorbable 4/0 suture • Different configurations• 6/0 monofilament running epitenon suture.• As noted by Singer MD et al. 1998, 3-0
prolene or mersilene suture may be suture of choice

• WOUND EXTENDED PROXIMALLY AND DISTALLY• PROXIMAL TENDON RETRIEVED,CORE SUTURES
ARE PLACED• KEITH NEEDLES USED TO PASS THE SUTURES
AROUND THE DISTAL PHALANX EXITING THROUGH NAIL PLATE DISTALLY
• REMAINING DISTAL END OF TENDON SUTURED TO THE RE-ATTACHED PROXIMAL PORTION
ZONE 1 REPAIR

Direct repair: if laceration is more than 1 cm from FDP insertion
Tendon advancement: if the laceration is less
then 1 cm from insertion

• REPAIR BOTH TENDON LACERATIONS• TENDON SHEATH MAY BE OPENED FOR
EXPOSURE BUT A2 AND A4 ARE PRESERVED AS MUCH AS POSSIBLE
• FDS IS REPAIRED FIRST FOLLOWED BY FDP
ZONE II REPAIRS

• If both tendons are lacerated, both are repaired, end to end withcircumferential re-enforcing sutures• May affect lumbricals in addition to flexor
tendons• Damaged lumbrical is either repaired or
excised depending on severity of injury and the location of the laceration
ZONE III REPAIRS

• Lacerations of flexor tendons within the carpal canal are typically associated with partial or complete laceration of median nerve
• Here median nerves should be repaired first and the tendons last
ZONE IV REPAIR

• In this area there may be concomitant ulnar nerve & artery damage as well as radial artery & median nerve damage.
• Primary repair of the arteries is usually indicated
• If wound is contaminated, arteries are repaired and delayed repair of tendons and nerves is planned
ZONE V REPAIR


Brunner incision !!

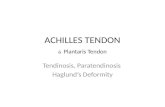
Tendon-to-bone attachment!!

One method of attaching tendon to bone. A, Small area of cortex is raised with osteotome. B, Hole is drilled through bone with Kirschner wire in drill. C, Bunnell crisscross stitch is placed in end of tendon, and wire suture is drawn through hole in bone. D, End of tendon is drawn against bone, and suture is tied over button.
Wilson

Kleinert method of Tendon advancement!!


Repair both tendons:
Because the blood supply to the FDP tendon is
jeopardized if the FDS is not fixed (due to the vinculae anatomy)

Lumbrical muscle bellies usually are not sutured because this can increase the tension of these
muscles and result in a “lumbrical plus” finger (paradoxical proximal
interphalangeal extension on attempted active finger flexion).
Zone 3 injuries

Lumbrical plus!!

Quadriga effect!!
Tendon advancement shortens the FDP & completes the grip before the normal fingers, if the tension on tendon graft is set too high, and limit their flexion and
thus week grip

THREE BASIC
TYPES


Silfverskiöld

Fish-Mouth End-to-End Suture (Pulvertaft)

End-to-Side method tendon repair!!

Postoperative Management

Newer Protocols
Most of them involve active motion exercises. Then the suture strength has to
increase

Different Methods
1. Active Extention-Rubber Band Flexion Method: e.g. Kleinert , and Brooke-Army
2. Immobilization
3. Controlled Passive Motion Methods: e.g. Duran’s protocol
4. Strickland: Early active ROM

Kleinert Protocol• Combines dorsal extension block with rubber-
band traction proximal to wrist
• Originally, included a nylon loop placed through the nail, and around the nail is placed a rubber band
• This passively flexes fingers, & the patient actively extends within the limits of the splint

Active range of motion rehabilitationKleinert !!

Duran protocol
• At surgery, a dorsal extension-block splint is applied with the wrist at 20-30° of flexion, the MCP joints at 50-60° of flexion, and the IP joints straight

Post-operative passive exercisesDuran’s

Differential passive exercises for FDP & FDS!!

Position of Immobilization for Flexor Tendon Injury
•Wrist – 30 degree flexon •MP joint 60-70 degree flexon •Slight flexon of PIP & DIP

Complications
• Joint contracture• Adhesions • Rupture • Bowstringing • Infection

Complications:
Adhesions & stiffness requires tenolysis in 18-25%
cases
Tenolysis is indicated after 3 months if no improvement is
noted
For 1-2 months extensive physiotherapy.

DONOR TENDONS FOR GRAFTING:
Palmaris Longus: Tendon of choice (fulfils requirement of length, diam & availability)
Plantaris Tendon: Equally satisfactory & advantage of being almost twice as long, but is not accessible.
Others: FDS, EDC

Summary
• Meticulous technique– Minimal handling– Appropriate suture configuration– Minimal resection of tendon sheath
• Postoperative mobilization• Supervision!

Extensor Tendon Injury
• Extensor apparatus– Extrinsic muscles
(ED, EI, EDM)– Intrinsic Muscles ( Lumbricals and
Interossei) – Fixed fibrous
structures.

Injury : Zone- I
– Mallet finger – persistent flexon of distal phalanx
• Closed: splinting 6-8 weeks
• Open: suture repair, Soft tissue reconstruction

Zone II injury- Middle Phalanx Level:
– Repair by interrupted suture. – Immobilization for 5-6 weeks– DIP joint in extension – PIP joint left free

Zone III injury- PIP joint level
– Most complex anatomically and physiologically– Causes two deformities • Boutonniere
• disruption of central tendon Closed: splinting MCP and PIP in hyperextension for 6
weeks Open: suture repair (figure of 8 suture)
• Swan Neck –excessive traction of central tendon–Closed : splinting DIP –Open : suture repair

Zone IV injury- shaft of proximal phalanx level
– Repair relatively easy– Adhesion is the
problem

Zone V injury – MP joint level
• Closed: splinting, 45 extension at wrist and 20 flexion at MCP
• Open: suture repair by 5.0 prolene

Zone VI injury- Metacarpal level
Better prognosis than in fingers
All structures, even intertendinous band should be repaired.
Core type suture possible.
Delayed suture is possible

Zone VII- wrist level
– Extensor tendons are under dorsal retinaculum –Retinaculum should be repaired or partially
preserved.–Adhesion is the problem –Grasping core suture should be used. – Immobilization for 5-6 weeks.

EXTENSOR TENDON MANAGEMENT
3 current treatment approaches to extensor tendon rehabilitation are
ImmobilizationEarly controlled passive mobilization Early active motion

Position of Immobilization for Extensor Tendon Injury
•The finger should remain parallel to forearm with wrist in full extension
•PIP & DIP – Neutral

IMMOBILIZATION
• Keep the tendon in a shortened position through splinting or casting
• Tendons immobilized for 3 weeks
• In week 4, gentle active motion of the repaired tendon is introduced
• Rehabilitation depends on zone of injury

IMMOBILIZATION
INJURIES IN ZONES PROXIMAL TO MCPs
INJURIES IN ZONES DISTAL TO MCPs
• May be immobilized for 3 weeks.
• Afterwards, finger may be placed in removable volar splint between exercise periods for 2 weeks
• Progressive ROM after 3 weeks
• If full flexion is not regained rapidly, dynamic flexion may be started after 6 weeks
• Require a longer period of immobilization (usually 6 weeks)
• A progressive exercise program is initiated
• Dynamic splinting during day and static splinting at night to maintain extension

EARLY PASSIVE MOTION
• Extensors are held in extension by dynamic, gentle rubber band traction, and the patient is allowed to actively flex the fingers—passively moving repaired extensor tendons

EARLY ACTIVE MOTION
• Early active short arc program (developed by Evans) allows tendon to actively move 3 days after surgery
• Therapist must take care to ensure stress applied by early active motion does not overpower strength of surgical repair
• Splinting program is complex and specific and requires a skilled occupational therapist

What is Manchester Short Splint?
• Wrist– Finishes at dorsal wrist crease– Allows 45 degrees extension
• MCPJ– 30 degrees flexion
• Exercises– Commence 4th or 5th day – Motion initiated at DIPJ


Proposed changes for Zone II
Day 1 post op–splint, oedema management–Splint : wrist 30degrees extension, MCPJ 40degrees
flexion
Day 3-5 start AROM –PROM exercise always prior to AROM –Isolated DIPJ ROM to at least 35degrees, with
lateral joint support

–Focus on initiating AROM with DIPJ rather than flat fist –Focus on IPJ extension exercises
• Avoid full composite flexion until 4wks