
Teleneurology - Florida Osteopathic Medical Association · 2Efficacy of site-independent...
51
Teleneurology SCOTT PEARLMAN, D.O. NEUROHEALTH OF SOUTH FLORIDA TELENEUROLOGIST FOR SPECIALISTS ON CALL
Transcript of Teleneurology - Florida Osteopathic Medical Association · 2Efficacy of site-independent...
Teleneurology
SCOTT PEARLMAN, D.O.
NEUROHEALTH OF SOUTH FLORIDA
TELENEUROLOGIST FOR SPECIALISTS ON CALL
Telemedicine Benefits And
Challenges
2
“It is an amazing invention, but who would ever want to
use one”
Rutherford Hayes, 1882 on the using telephone for the first time
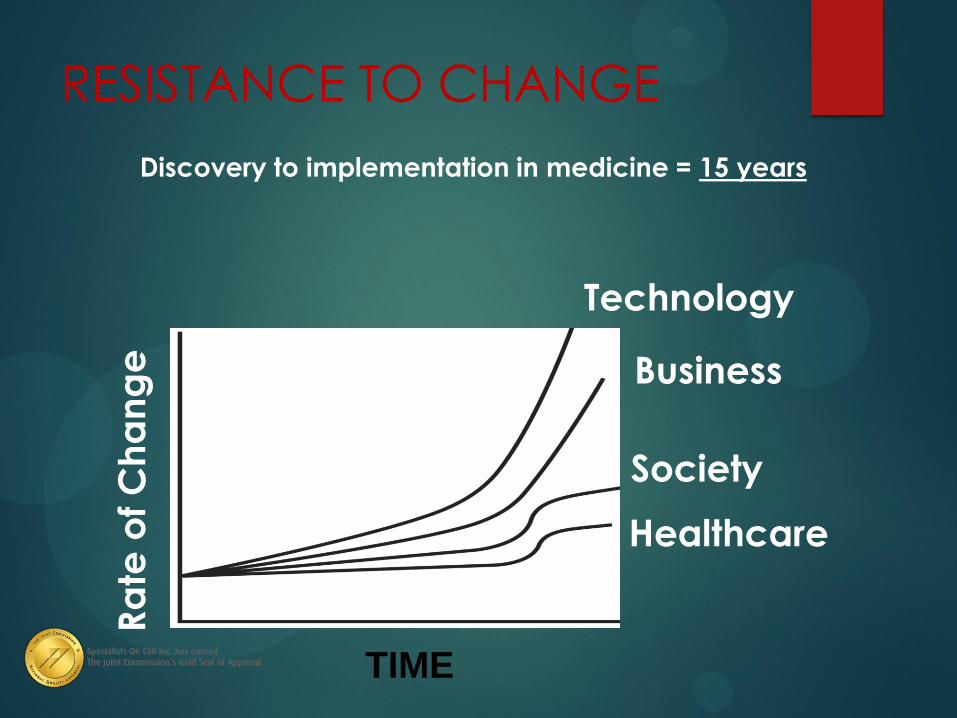
RESISTANCE TO CHANGE
Discovery to implementation in medicine = 15 years
TIME
Ra
te o
f C
ha
ng
e
Society
Business
Technology
Healthcare
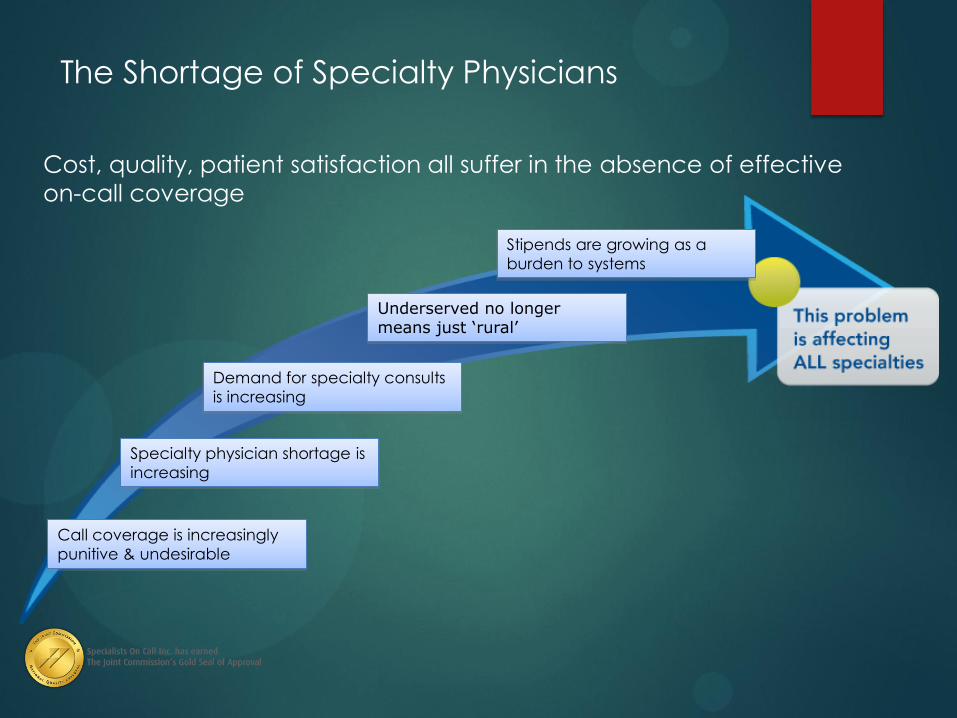
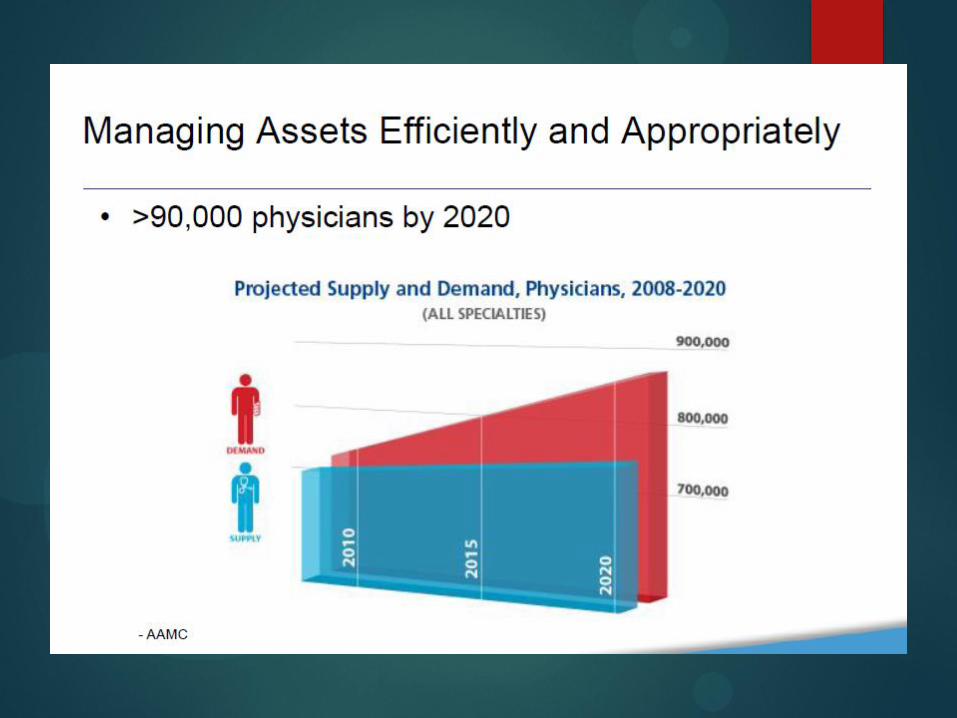
The Shortage of Specialty Physicians
Cost, quality, patient satisfaction all suffer in the absence of effective
on-call coverage
Call coverage is increasingly
punitive & undesirable
Specialty physician shortage is
increasing
Underserved no longer means just ‘rural’
Demand for specialty consults
is increasing
Stipends are growing as a
burden to systems

Telemedicine + Stroke
The U.S. has ~4 neurologists per 100,000 persons
800,000 strokes per year
Increasing numbers of stroke neurologists opting out of call coverage Increasing numbers of underserved patients
State/local regulations require emergency call coverage
in order for center to be recognized as stroke-capable
facilities or primary stroke centers
The Rationale
Just-in-time Care
Improved Quality
Enhanced Efficiency
Better Professional Communication
Patient Satisfaction
Enlarged Catchment Area
Cost Savings?
Advantages of telemedicine:
Decreased response time
High patient satisfaction scores for telemedicine consults
Reduced geographic disparity in neurological care
Improved access for remote or underserved areas
Easy recruitment of patients for clinical trials
Decreased travel time and expense for patients and doctors
Telemedicine is Good for
patients
Access to specialists in a timely manner
Increased response time
Quicker treatment plan
TIME IS BRAIN
Acutely ill patients get acute evaluation
Shorter hospital stay as earlier evaluation and thus
test ordered earlier
Teleneurology is Good for
Hospitals
Allows hospitals to treat stroke patients with confidence &
clinical consistency
Eliminates EMS diversions
Reduces unnecessary patient transfers
Satisfies staffing requirement for Primary Stroke Center certification
Supports ER staff & improves department efficiency
Provides a competitive advantage in local marketplace
Relieves the burden of on-call coverage for local neurologists/physicians
Serves as a recruiting advantage for physicians
HISTORY OF TELEMEDICINE
Early History of Telemedicine
1950s and 1960s
Nebraska Psychiatric Institute - UN & state mental hospital & Interact System - Dartmouth and UVM Medical Schools [Microwave]
STARPAHC [Space Technology Applied to Rural Papago Advanced Health Care - Papago Indian Reservation & Public Health Hospital in Arizona
Alaska Satellite Biomedical Demonstration Project used NASA technology to link 26 sites across Alaska.
HISTORY OF TELEMEDICINE Boston Logan Airport to Massachusetts General
Hospital 1967
HISTORY OF TELEMEDICINE STARPAHC – On the Papago Indian Reservation
1975
History & Development
Health care via remote services
Not a new concept
What IS new – technology
Levine & Gorman, 1999
First detailed description of potential use of telemedicine in
acute stroke via video teleconferencing (VTC)
As of 2012 survey, there were 56 confirmed active telestroke
programs in the U.S. (Silva et al, 2012)
16
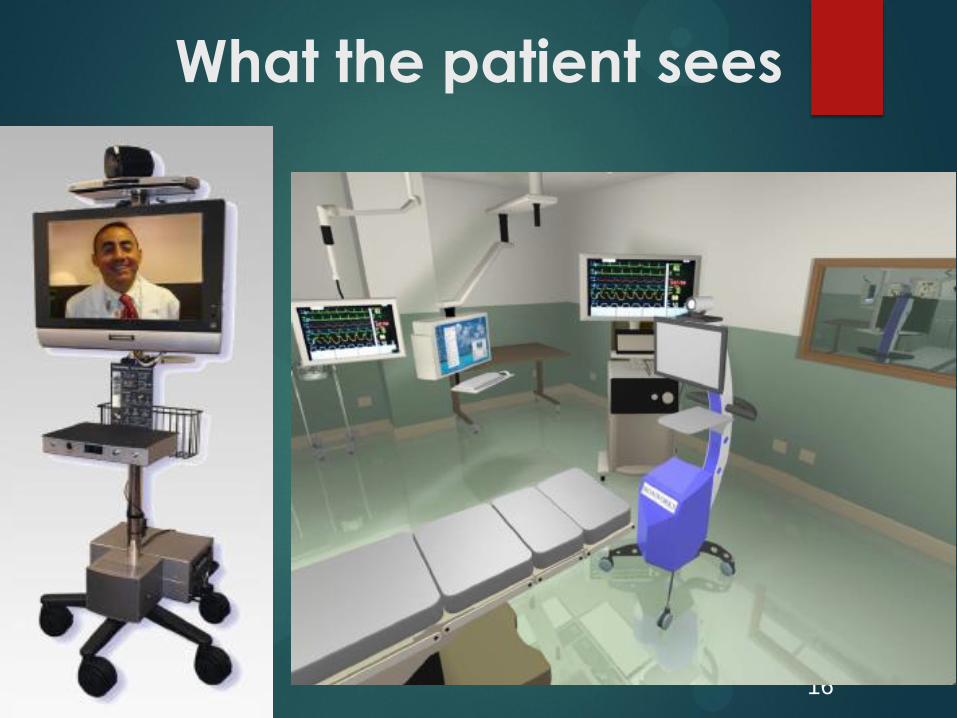
What the patient sees

17
What I see
Youtube Patient video
https://www.youtube.com/watch?v=nB4joFD7MR
0
Equipment
Minimum quality standards, including transmission rates
and ability to support high resolution and high frame
rates
Teleradiology - Review of imaging at appropriate
resolution using DICOM (digital imaging and
communications in medicine), which is a standardized digital format.
Must be FDA-approved in order to receive Medicare or
Medicaid reimbursement
Equipment
High quality video
teleconferencing (HQ-VTC) –
interactive audiovisual systems, coupled with the use of
teleradiology for remote review
of brain images (Schwamm et
al, 2009)
Pt & provider can see and hear
each other in full color
Cameras have various degrees
of remote control connected to
a display screen
Telemedicine models:
Do it yourself: technology purchase with consults by local physician
Hub – Spoke: consults provided by hub facility physicians
Independent: consults provided by independent telephysicians
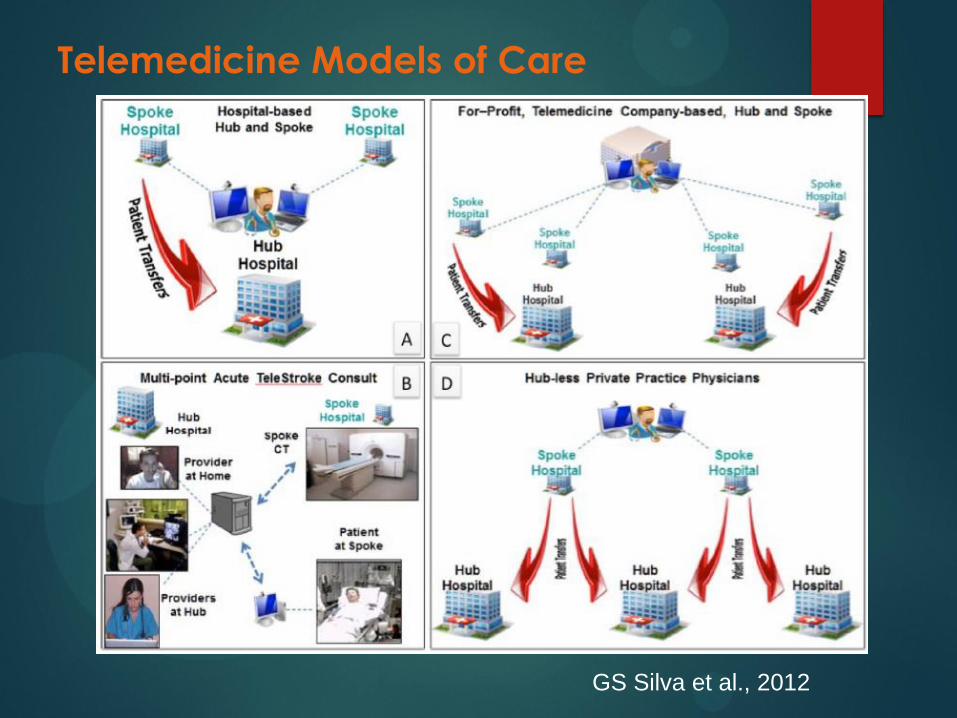
Telemedicine Models of Care
GS Silva et al., 2012
Why is Telemdicine
important?
-TIME
-NEED
-TPA WINDOW
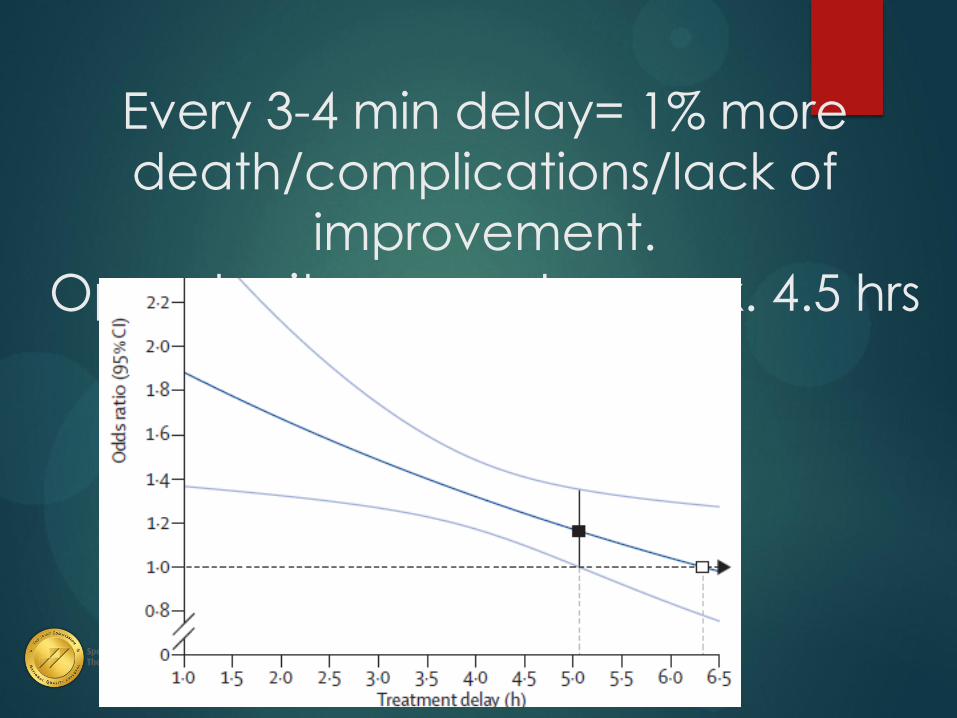
Every 3-4 min delay= 1% more
death/complications/lack of
improvement.
Opportunity gone at approx. 4.5 hrs
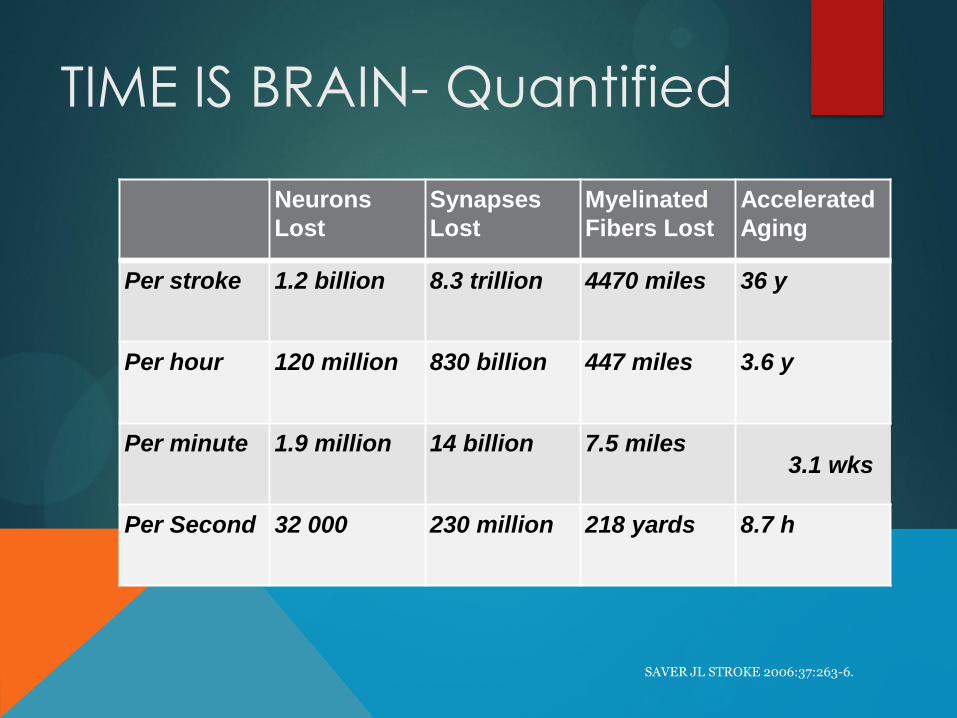
TIME IS BRAIN- Quantified
Neurons
Lost
Synapses
Lost
Myelinated
Fibers Lost
Accelerated
Aging
Per stroke 1.2 billion 8.3 trillion 4470 miles 36 y
Per hour 120 million 830 billion 447 miles 3.6 y
Per minute 1.9 million 14 billion 7.5 miles 3.1 wks
Per Second 32 000 230 million 218 yards 8.7 h
SAVER JL STROKE 2006:37:263-6.
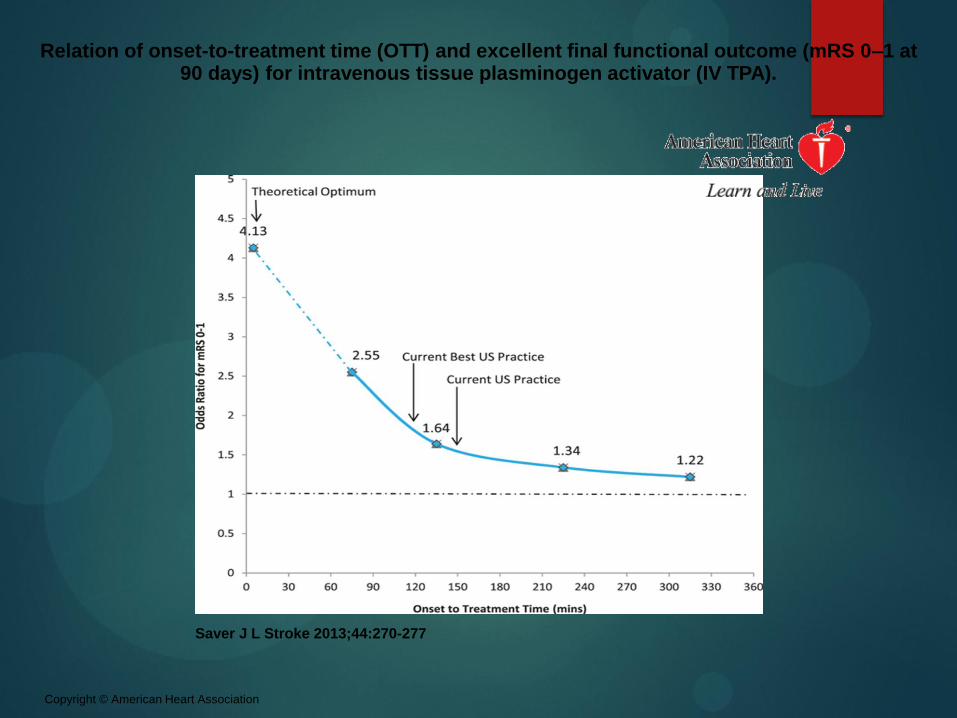
Relation of onset-to-treatment time (OTT) and excellent final functional outcome (mRS 0–1 at 90 days) for intravenous tissue plasminogen activator (IV TPA).
Saver J L Stroke 2013;44:270-277
Copyright © American Heart Association
Is Telestroke a good idea?
Televideo Stroke care improves patient outcomes1
Televideo: more correct treatment decisions than Telephone2
High Telestroke satisfaction among skeptical ED docs (100%) and demanding patients (86%) 3
American Stroke Association guidelines require Telestroke in most/many cases4
27
1Effects of the implementation of a telemedical stroke network: the Telemedic pilot project for integrative stroke care (TEMPIS) in Bavaria, Germany Lancet Neurology
2006; 5:742-48
2Efficacy of site-independent telemedicine in the stroke doc trial: a randomized, blinded, prospective study. Lancet Neurology 2008; 7 (9):787-795
3 Virtual Telestroke support for the Emergency department evaluation of acute stroke Academic Emergency Med Nov 2004
4 A Review of the evidence for the use of telemedicine within stroke systems of care Stroke. 2009; 40
Telemedicine + Stroke
• By certain estimates the misdiagnosis rate by primary care and ER physicians may be as high as 30% compared with stroke team final diagnoses (Harbison et al, 2003)
• Non-stroke specialists often reluctant to administer tPA in absence of specialist expertise significant delays or withholding of treatment
– In one survey, 40% of ER physicians indicated they would not use IV tPA, usually due to risk of ICH
– However, most lawsuits involving tPA were associated with failure to treat rather than adverse events from tPA
Medical Liability
As of the 2009 review of telestroke (Schwamm et
al.), no specific evidence to suggest that telemedicine consultations increase risk of
malpractice claims, compared to providing local
consultations
In general, physicians are at greater liability risk
whenever tPA is involved (whether it is delivered
or withheld)
Most tPA-related lawsuits arise when tPA is withheld
More thorough stroke care documentation by
telestrokologists may reduce such issues
Feasibility & Effectiveness (IV tPA)
Safety of telestroke-guided tPA administration assessed by major safety outcome of symptomatic ICH and in-hospital mortality
Audebert et al (2006)
Nonsignificantly higher rates of symptomatic ICH (7.8% vs 2.7%, p=0.14)
Similar rates of PH2 parenchymal hemorrhages (4.3% vs 2.7%, p=0.72)
Similar in-hospital mortality (3.5% vs 4.5%, p=0.74)
TEMPiS study (2007)
Compared to patients receiving conventional tPA delivery,
telestroke patients had similar long-term mortality and functional
outcomes (at 3 and 6 months)
Feasibility & Reliability (acute stroke)
Wang et al (2003)
20 patients, NIHSS vs NIHSS-telestroke
No difference of >3 points between the 2 scoring
systems
Handschu et al (2003)
German study
Excellent reliability for all 13 items of the NIHSS in 41
patients examined within 36 hours of onset
AHA/ASA Recommendation
Class I, Level of Evidence A
“The NIHSS-telestroke examination, when
administered by a stroke specialist using HQ-VTC, is
recommended when an NIHSS-bedside assessment
by a stroke specialist is not immediately available
for patients in the acute stroke setting, and this
assessment is comparable to an NIHSS-bedside
assessment.”
AHA/ASA Recommendation
Class I, Level of Evidence A
“HQ-VTC [high quality video teleconference] systems are
recommended for performing an NIHSS-telestroke
examination in nonacute stroke patients, and this is
comparable to an NIHSS-bedside assessment. Similar
recommendations apply for the European and
Scandinavian Stroke scales”
Feasibility studies (non-acute stroke)
• STRokE DOC (UCSD) – Stroke Team Remote Evaluation using a Digital Observation Camera (Meyer et al, 2005)
– Public internet connection, “site independent”
– 25 patients examined both at bedside and via telemedicine by 2 NIHSS-certified neurologists
– Feasibility – all 25 patient exams performed successfully with wireless telemedicine
– Reliability - 67% of NIHSS items and 82% of modified NIHSS items had excellent agreement
• Comparable to in-person assessments
• Wiborg et al, 2005
– European Stroke Scale
– Scandinavian Stroke Scale
Feasibility studies (non-acute stroke)
NIHSS – 13-item neurological exam
Demonstrated to be reliable amongst neurologists, non-
neurologists physicians, nonphysician staff
Shafqat et al. (1999)
First assessment of interrater agreement between NIHSS-
bedside and NIHSS-telestroke
Stroke neurologists, assisted by bedside nurse during telestroke
assessment
NIHSS-bedside and NIHSS-telestroke scores were strongly
correlated (r=0.97, p<0.001)
Telestroke examination times were longer (9.70 vs 6.55
minutes, p<0.001)
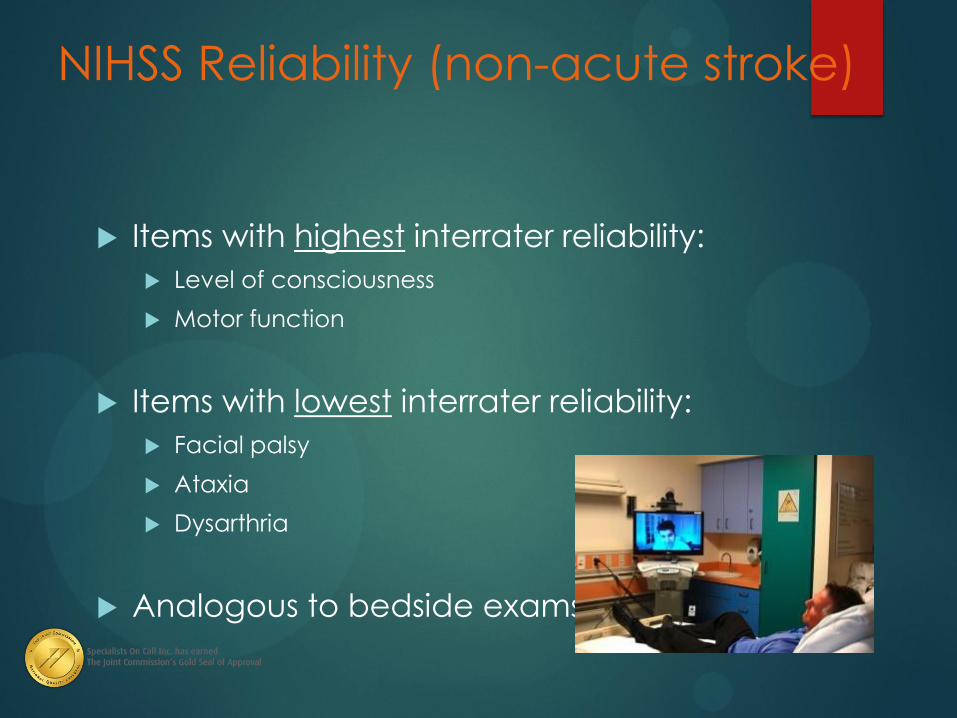
NIHSS Reliability (non-acute stroke)
Items with highest interrater reliability:
Level of consciousness
Motor function
Items with lowest interrater reliability:
Facial palsy
Ataxia
Dysarthria
Analogous to bedside exams
Barriers to telemedicine:
Limited neurological evaluation: cannot evaluate muscle tone, strength, sensation, reflexes, funduscopic exam
Physician reluctance to accept novel technology
Licensing and credentialing issues
Limited billing and reimbursement
Malpractice concerns
Licensure & Credentialing • Each state has own rules regarding medical practice
– A physician in state A providing telemedicine services to a patient in state B is considered to be practicing in state B telestroke
specialist must be licensed in all states in which potential patients
are located
• Physicians must be credentialed at sites where they provide
telemedicine services
Case Study #1: small/CAH
• Small community hospital
– <100 beds
– 1 private practice neurologist
– System standard is PSC status for acute facilities
• Barriers
– 24/7 neurology coverage for ED
– Consistent response to ED
– CT & lab services
Case Study #2: limited neurology
• Community hospital
– 220 beds
– Stipend to private practice neurology
– Large stroke volume/current PSC status
• Barriers
– Limited utilization of rt-PA for acute stroke
– Significant variability in ED response to stroke
– Difficulty employing dedicated neurology practice
Case Study #2: limited neurology
• Actions
– Termed private practice stipends
– Implemented TN for 24/7/365 ED coverage
• Results
– Reduced variability in ED response to acute stroke
– Easily acquire new neurologists for out-patient practice and in-patient consultation
– Rt-PA utilization increased immediately
– Continued PSC certification
Case Study #3
Large county hospital
>500 bed
Staff neurologists
Active Neurointerventionalists
Results
Improved door to need time- aim <60 minutes
Improved communication between interventional
and teleneurologist
-still comes down to if no neurologist in house, takes
extended period of time to get to the patient
“Connect to Quality”
Case 3: IV Tpa &Thrombectomy
55 year old man presented to hospital with an acute onset of left sided hemiplegia, right gaze preference and neglect, global aphasic
He was last known normal at 4:30 pm, and his wife attempted to wake him up at 5:15 pm and contacted EMS
He was brought to hospital at 5:30 and a CT of the brain was negative for hemorrhage
I saw the patient on camera at 5:45, reviewed films, lab results and reviewed tpa criteria. NIH 19
Tpa administered at 5:55
Partial improvement, but still with significant aphasia, 30 min into tpa disdcussed case with NIR, pt went for intervention
Connect to Quality 43
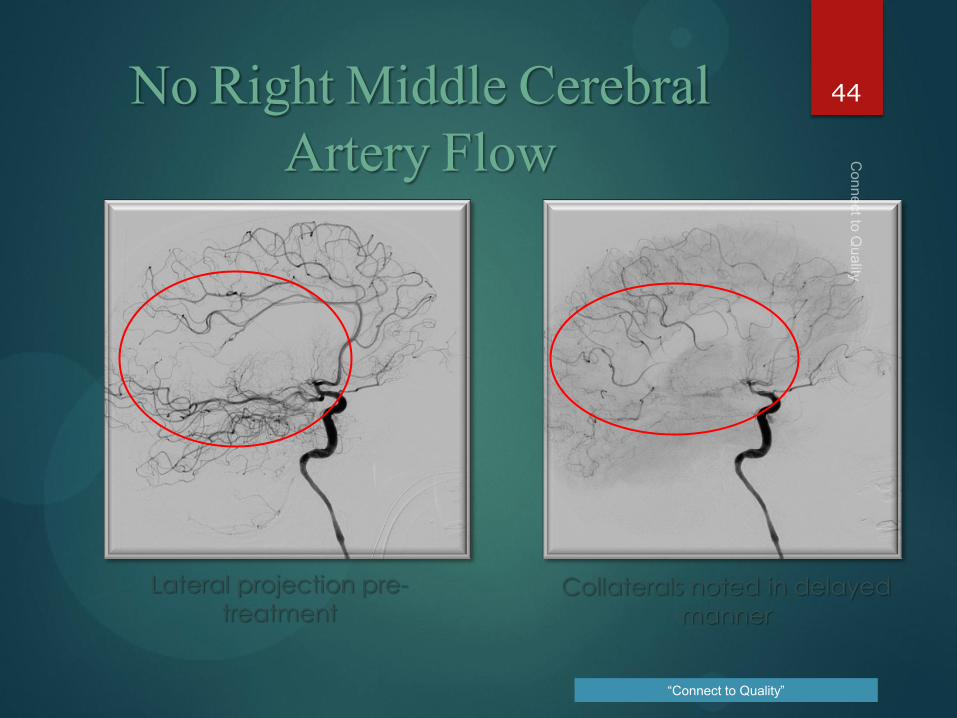
Lateral projection pre-
treatment Collaterals noted in delayed
manner
“Connect to Quality”
No Right Middle Cerebral Artery Flow
44
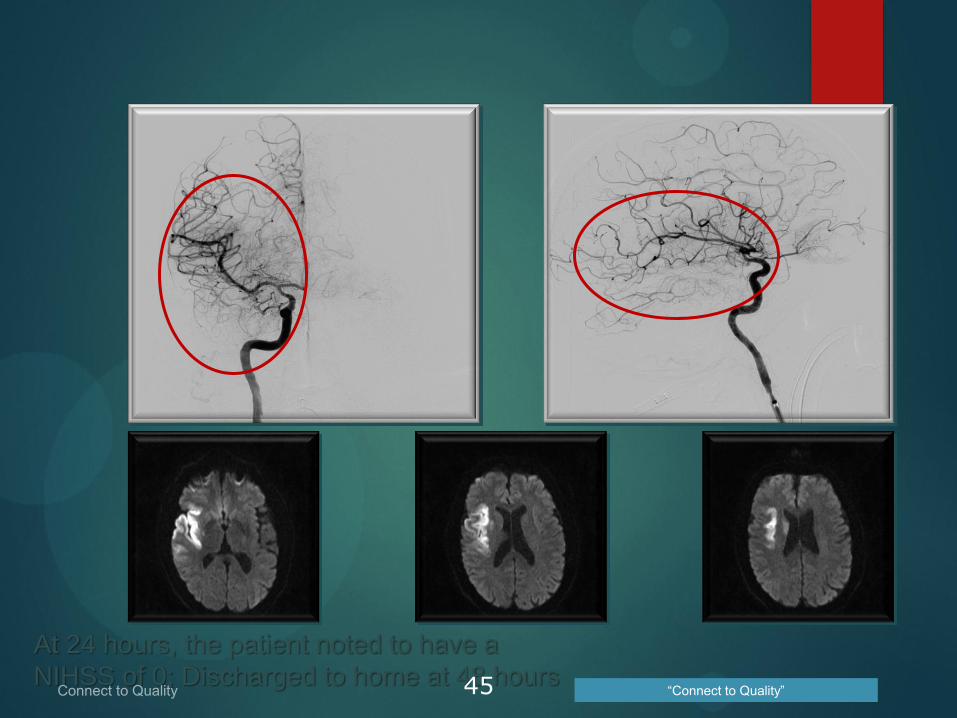
At 24 hours, the patient noted to have a
NIHSS of 0; Discharged to home at 48 hours “Connect to Quality” 45
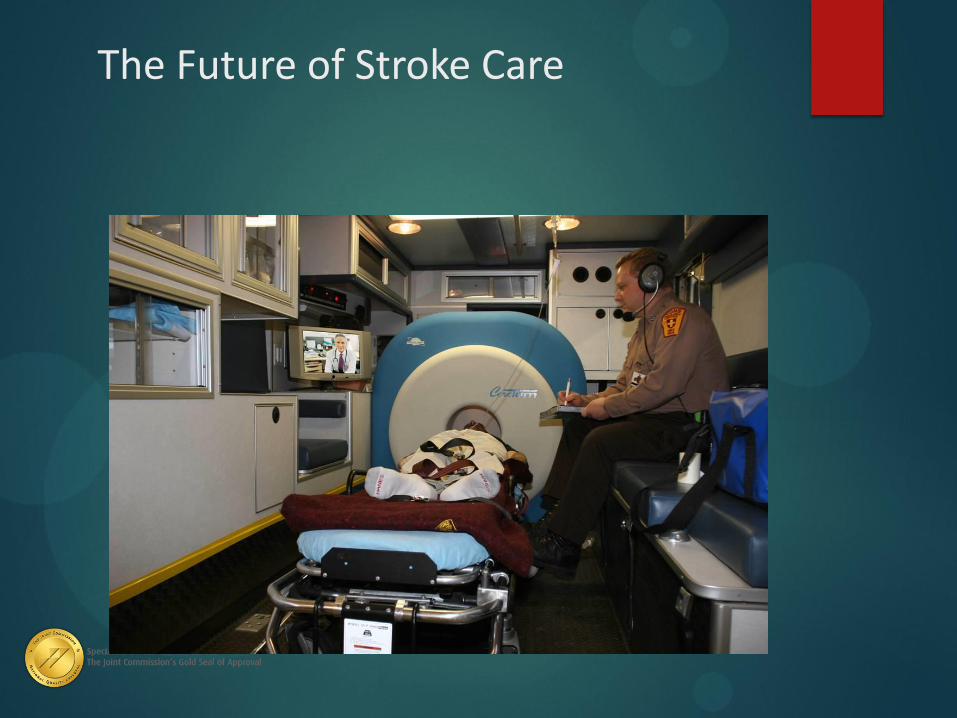
The Future of Stroke Care
The Mobile Stroke unit
CT scanner capable of advanced vascular imaging (CTA/CTP)
Teleneurology
Point of care labs
Being done in Houston and Germany
Cost: $400,000
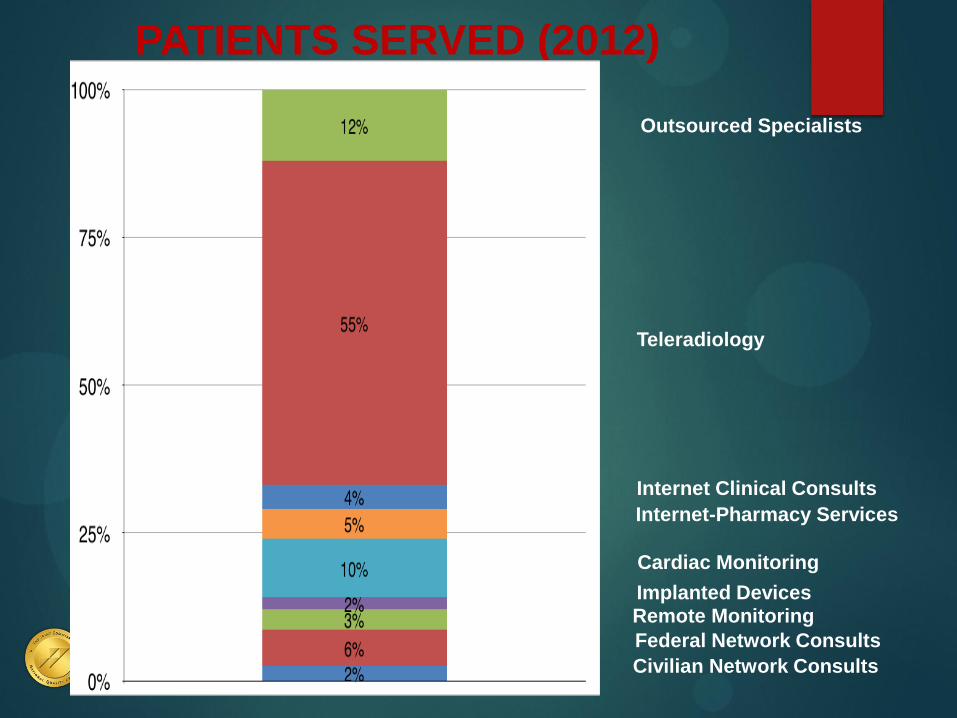
PATIENTS SERVED (2012)
Civilian Network Consults
Federal Network Consults
Remote Monitoring Implanted Devices
Cardiac Monitoring
Internet-Pharmacy Services
Internet Clinical Consults
Teleradiology
Outsourced Specialists
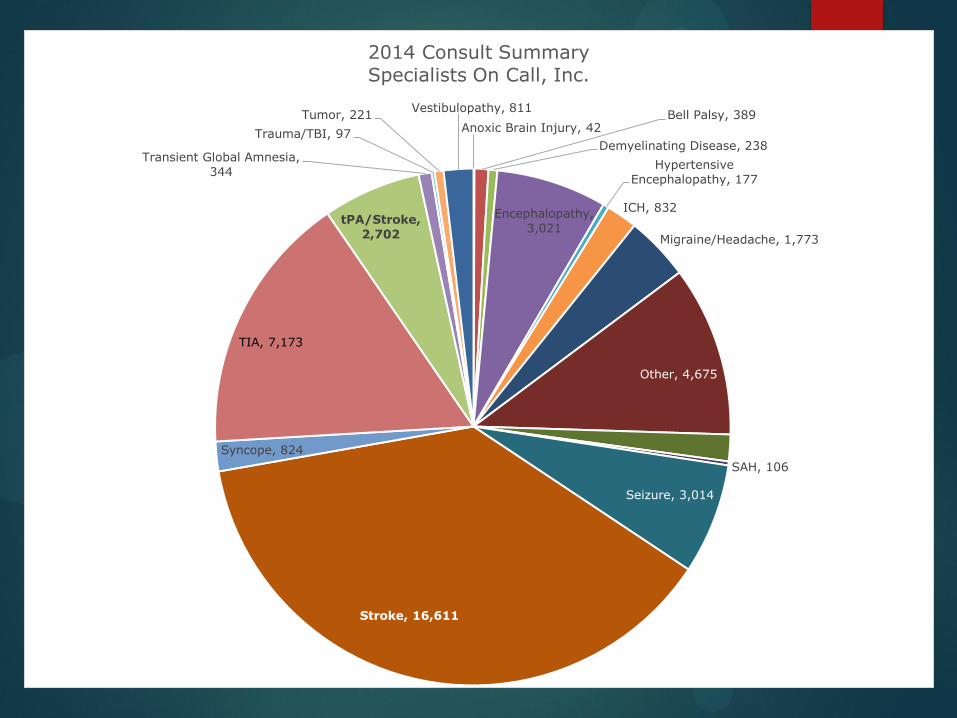
Anoxic Brain Injury, 42 Bell Palsy, 389
Demyelinating Disease, 238
Encephalopathy,
3,021
Hypertensive
Encephalopathy, 177
ICH, 832
Migraine/Headache, 1,773
Other, 4,675
Psychogenic, 752
SAH, 106
Seizure, 3,014
Stroke, 16,611
Syncope, 824
TIA, 7,173
tPA/Stroke,
2,702
Transient Global Amnesia,
344
Trauma/TBI, 97
Tumor, 221 Vestibulopathy, 811
2014 Consult Summary
Specialists On Call, Inc.
Specialists On Call’s
tPA Administration Rate
tPA / tPA + ischemic stroke = tPA administration rate
2,702 / 19,313 = 14%
When do we ‘NOT’ use
telemedicine?
51

















